Tessa Hart, PhD Moss Rehabilitation Research Institute Elkins Park, PA.
70
Advances in Brain Injury Rehabilitation Research Tessa Hart, PhD Moss Rehabilitation Research Institute Elkins Park, PA
-
Upload
liliana-hunt -
Category
Documents
-
view
218 -
download
1
Transcript of Tessa Hart, PhD Moss Rehabilitation Research Institute Elkins Park, PA.

Advances in Brain Injury Rehabilitation
ResearchTessa Hart, PhD
Moss Rehabilitation Research InstituteElkins Park, PA

The Traumatic Brain Injury Model System: A study (collection of studies) that spans acute care rehabilitation long-term outcome
Recent example of a TBI treatment study at Moss that focuses on a major problem in post-acute phase of recovery
Overview: 2 Parts

The Traumatic Brain Injury Model System

The Traumatic Brain Injury Model System (TBIMS) A multi-center, longitudinal project on the
short- and long-term outcomes of TBI, and how to improve them
The TBIMS program has been funded since 1987 by the National Institute on Disability and Rehabilitation Research, US Department of Education
Moss has been a TBIMS center since 1997

Mission Statement
“The Traumatic Brain Injury Model Systems program seeks to improve the lives of persons who experience traumatic brain injury, their families and their communities by creating and disseminating new knowledge about the course, treatment and outcomes of their condition.”

Definition of TBI◦TBI is defined as damage to brain tissue
caused by an external mechanical force as evidenced by medically documented loss of consciousness or post traumatic amnesia (PTA) due to brain trauma or by objective neurological findings that can be reasonably attributed to TBI on physical examination or mental status examination.

How the Mission is Accomplished Prospective, multi-center longitudinal
research on people with TBI and their families and communities◦ Determine long-term outcomes, and what affects
them◦ What are most common and important problems?
Treatment research◦ Pilot studies to develop promising treatments◦ Larger collaborative studies to test their effects

Not All Research The TBIMS program supports other projects
designed to fulfill the mission:◦ Conferences, seminars, networking opportunities
for people with brain injury & their families◦ Websites and materials for dissemination of new
knowledge◦ Collaborations between TBIMS centers and others
with similar missions: Brain Injury Association (national & state chapters) HRSA projects within states

Who Are the TBI Model Systems? 16 ‘centers of excellence’ for TBI treatment
and research Clinical excellence: Must have state-of-the-
art care for TBI from the time of injury, through emergency and acute care, to inpatient rehabilitation
Research excellence: Must be able to conduct innovative research to create new knowledge about TBI

Current Traumatic Brain Injury Model Systems
Currently Funded
Follow-up Center
Previously Funded

Types of Research National Database
◦ All 16 centers collect same data on patients enrolled in TBIMS From emergency/ acute care From rehab hospital: all patients in the database
receive inpatient TBI rehabilitation From follow-up at years 1, 2, 5, 10, 15, 20…… after
the TBI◦ Currently >9000 patients in the National
Database (since 1989…. starting 20 yr follow-ups)

NIDRR TBI National Database Form I – 8,775 cases (as of 3/31/2009) Form II – 26,352 follow-ups* - 22% attrition
(6%**)◦ Year 1 – 8,085 – 16% attrition (3%**)◦ Year 2 – 6,931 – 19% attrition (6%**)◦ Year 5 – 4,382 – 22% attrition (13%**)◦ Year 10 – 1,172 – 27% attrition (9%**)◦ Year 15 – 418 – 21% attrition (14%**)◦ Year 20 – 9 – 22% attrition (0%**)
*There are some follow-ups in database that were performed at 3, 4, and 6 years post-injury.
**Additional percent attrition due to loss of center funding.

Unique Research Opportunity
To see how people with TBI and their caregivers do over time… a long time
To identify the most persistent and pressing problems that require long-term treatment and support
To examine the factors that predict who will do well, who not so well

What (Who) Are We Missing? Mild TBI
◦ TBIMS enrollment is from inpatient TBI rehab units; most are moderate/ severe (this is a moving target due to changes in policy over 20+ years)
Non-traumatic BI Children: TBIMS includes ages 16 and up Uninsured or under-insured
◦ If no funding for inpatient rehab, can’t be enrolled (this varies by state)
People who do not get rehab (i.e., no “control group”

What Information Is In the National Database? Basic information about person’s
background-- age, race, gender, education & occupation, drug & alcohol history, family, etc.
Injury information--cause, severity, CT scan findings, etc.
Status & improvement during rehabilitation◦ FIM◦ Disability Rating Scale (DRS)

Follow-Up Information After discharge from rehab, person and/ or
family are telephoned at 1, 2, 5, 10, 15, 20….. years after injury
Moss is following >800 people with TBI Structured interview to assess long term
outcomes:◦ Work, social life, other community participation◦ Health issues (rehospitalization)◦ Emotional status, quality of life

Demographic Data[Includes data from 01/01/1989 – 12/31/2008]

Age
mean = 39; n = 8779

Growth in Older Adults Admitted for TBI Rehab (eRehab, N=35,423)
Age at Admission to Rehab

Gender
n = 8778

Race
n = 8777

Etiology of Injury
n = 8749

Level of Education At Injury
n = 8575

Blood Alcohol LevelAt Emergency Department Admission*
* excludes cases not tested = 23%
mean = 68.7; n = 6461

TBI Severity

Amount and location of brain damage is hard to visualize
Typical damage is to the frontal and temporal poles, and diffuse axonal injury (DAI)
Focal injury may show up on brain scans, but DAIoften does not.
The best gauge of theamount of DAI is the depth & duration of impaired consciousness after the TBI.
Severity of TBI Hard to Measure

Indices of TBI Severity
TIME
Normal conscious-ness
Depth of coma at time of TBI (GCS score)
(Coma ) Disorientation Normal or impaired conscious-ness
*Post-Traumatic Amnesia
Retro-grade Amnesia
Duration of Unconsciousness

Glasgow Coma Scale ScoreAt Emergency Department Admission*
mean = 9.4; n = 6668

Duration of Unconsciousness
mean = 8.6 days; n = 8358

Duration of PTA
<17% 1 Thru 7
15%
8 Thru 2843%
>=2935%
mean = 24.9 days; n = 6536
(Moderate/Severe)
(Very Severe)
(Extremely Severe)

Mean Length of Stay

Outcomes at 1 Year+

Functional Independence Measure
Complete
Independence
Modified Independence
Supervision
Minimal Assistance
Moderate Assistance
Maximal Assistance
Total Assistance
Mean Scores converted to 7-point scale

Living Situation

Improvement and Decline (GOS-E)

Work Work is one of the most important– and best
studied– outcomes TBI affects many young people in (or just
starting) productive years Costs of people with TBI not working are
enormous◦ To injured individuals (financial & personal)◦ To families who must support another person◦ To family members who have to quit work to care
for injured person◦ To society

Employment Status

Predictors of Return to Work The consequences of TBI are important
(especially cognitive/ behavioral problems), but pre-injury factors may be even more so
Being employed at the time of TBI◦ But even if you are, risk of unemployment 3-5
years after TBI is 5x greater than general population for men… 3x for women
What “level” of job you have◦ Professional/ managerial vs blue collar vs
unskilled “Vicious cycle” of pre-injury disadvantages:

Risk Factors for Poor Work Outcome
…how should we intervene in this cycle to improve outcomes?
Poor education
Poor employment history
Substance abuse
Violent injuryLow income/ poor insurance
More needs unmet by services
Non-white

www.tbindsc.org/syllabus
To view all variables in the TBIMS National Database

TBI Model Systems National Data and Statistical Center Websitewww.tbindsc.org/syllabus

Online TBI Model Systems National Database Syllabus

www.tbims.org/combiCenter for Outcome Measurement in
Brain Injury




Model System Knowledge Translation Center Center at University of Washington that is
working with all TBIMS centers (+ SCI, Burn Model Systems) to help translate research information for clinicians, and consumers affected by disability www.msktc.washington.edu
“Knowledge Translation” refers to the newer models of active transfer from research to usable clinical information… older models (“dissemination”) were more passive



Anger Self-Management
Training for TBI

Anger/ irritability is an important problem after TBI:◦ Frequent complaint (up to 1/3 of survivors)◦ Range of symptoms from irritability,
“crankiness” to verbal and physical aggression◦ Occurs across spectrum of injury severity, from
mild to severe◦ Persistent problem, may even worsen over time◦ Important problem-- contributes to family
burden, social isolation and vocational failure◦ Difficult to treat– may exclude people from
therapy programs
Background

Very few Some medications may be used, but little
evidence base; and meds may not be acceptable to patients
We set out to develop a testable, non-drug treatment for TBI-related anger that could stand alone or be incorporated into outpatient therapy programs.
Treatment Options

In designing a new treatment, it’s often helpful to build in ‘active ingredients’ that get at the (hypothesized) root causes of a problem, e.g.:◦ Attention problems are caused by certain
neurotransmitter deficiencies◦ Methylphenidate (Ritalin) boosts levels of those
neurotransmitters◦ Therefore, it should alleviate attention problems
Where To Begin?

Primary/ organic◦ Damage to frontal/ temporal areas, limbic system;
neurochemical changes Secondary to brain injury
◦ Cognitive deficits such as ↓ attention, language, memory, reasoning can frustration & anger
Secondary to life changes◦ Loss of independence◦ ↓ social life, ↓ income, etc., etc.
Premorbid factors Can’t pinpoint/ measure the relative
magnitude of these for a given patient
But Anger Has Multiple Causes

No matter what other causes exist, we reasoned that 2 characteristic aspects of executive dysfunction contribute to anger after TBI:
(1) Impaired self awareness, especially of behavioral/ emotional problems and their impact on others
-- reduced ability to monitor anger episodes-- tendency to blame others when things go
wrong
Find a “Common Treatable Cause”

(2) Impaired Problem Solving Loss of cognitive and behavioral flexibility Difficulty in appreciating consequences of actions Anger or irritability can become a stereotyped
response to threat (change, confusion, any problem situation) after TBI
Anger is gratifying in an immediate sense, but highly maladaptive in the long run
Even if person recognizes need for change, he/ she lacks the problem-solving ability to modify behavior

Built around 2 main ingredients:◦ Self-Awareness/ Self-Monitoring training◦ Training of specific methods for Problem Solving
in anger situations Designed for people with brain injury
◦ At a range of cognitive levels ◦ With or without participating SOs
Fully manualized◦ Standardized therapist-workbook format for
replication across centers, therapists, patients
Anger Self-Management Training (ASMT)

8 ~weekly sessions, 1:1; Significant Other (if any) attends portions of 3 sessions
‘Psycho-educational model’ with:◦ Didactic material on anger, its relationship to TBI,
etc…… “normalization”◦ Skill training in the 2 main ingredients:
Self-monitoring of anger, triggers, consequences, characteristic behaviors, patterns, etc.
Problem-solving using simplified and modified “anger management” methods successful in the general population
◦ “Outside Practice” (never homework!)
ASMT

Pre-post test design (no control group) Is it feasible?
◦ Will people understand it? It is acceptable?
◦ Will people like it? --hate it?◦ Will they show up? Will they drop out?
Will it reduce self-reported anger?◦ Or will the focus on anger monitoring have the
opposite effect? Estimate effect size for larger trial If changes observed, are they clinically
meaningful?
Pilot Study of ASMT

8 Male, 2 Female 6 White, 4 African-American Age: 23 – 59 (mean, 44) Time post-TBI: 6 months – 20 years (median, 4
yr) 4 MVA, 4 assault (1 GSW), 2 fall PTA duration: Median 51 days (11 days – “2
years”) Severe cognitive deficits, especially in memory No severe emotional disturbances other than
anger problems
Participants

Self-report and SO (proxy) report pre and post treatment
State-Trait Anger Expression Inventory-2 (STAXI-2): 2 subscales◦ Trait Anger: measures general tendency toward
anger, “hot headedness,” whether expressed or not◦ Anger Expression-Out: Outward expression:
sarcasm, hostility, verbal/ physical aggression Brief Anger Aggression Questionnaire (BAAQ)
◦ Captures more extreme “acting-out” or passive aggression
Anger Measures
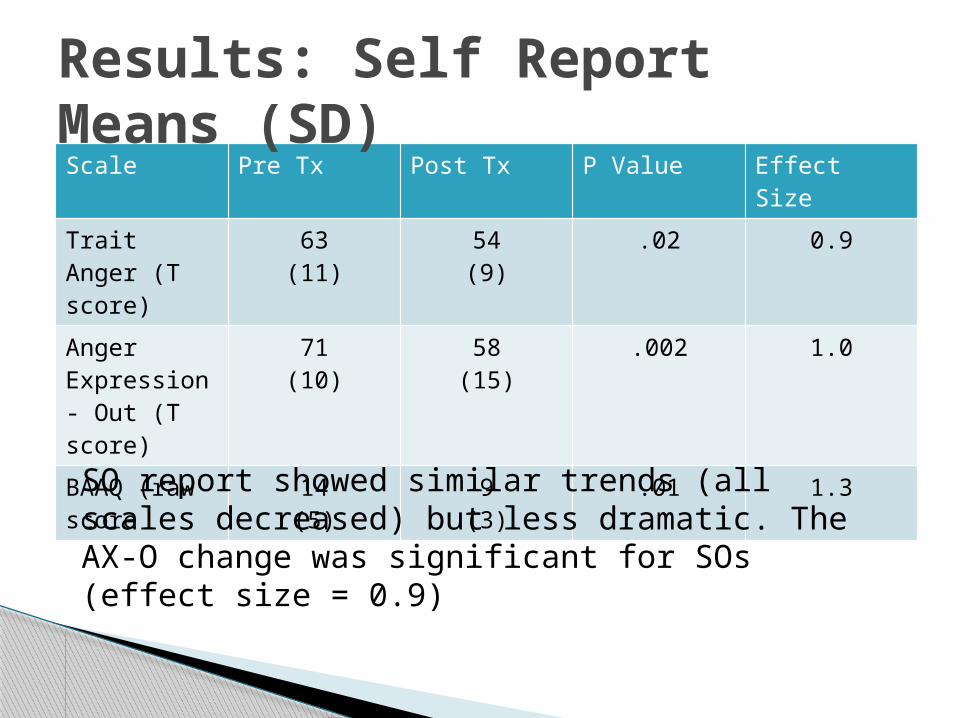
Scale Pre Tx Post Tx P Value Effect Size
Trait Anger (T score)
63(11)
54(9)
.02 0.9
Anger Expression- Out (T score)
71(10)
58(15)
.002 1.0
BAAQ (raw score
14(5)
9(3)
.01 1.3
Results: Self Report Means (SD)
SO report showed similar trends (all scales decreased) but less dramatic. The AX-O change was significant for SOs (effect size = 0.9)

Trait Anger Changes
Pre-treatment Post-treatment15
25
35
45
55
65
75
85
ST
AX
I-2
Tra
it T
Sco
re

Anger Expression-Out Changes
Pre-treatment Post-treatment15
25
35
45
55
65
75
85
ST
AX
I-2
AX
-O T
Sco
re

BAAQ Changes
Pre-treatment Post-treatment0
5
10
15
20
25B
AA
Q T
ota
l S
co
re

All participants rated themselves “a little better” or “a lot better” overall at handling their anger
SOs rated participants as “a little better” or “a lot better” except for 1 (no change)
7/10 participants and 6/ 8 SOs rated anger as having less impact on daily life (relationships, mood, community function) after treatment
Cognitive deficits seemed to have little impact on ability to improve with treatment
Clinical Significance
“I didn’t think this was going to do a damn thing for me, but it helped me a lot”
“I give this study an A+” Program is not long enough– there is so
much more to learn (several comments) Many specific suggestions for how to
improve program, such as ◦ More SO involvement◦ More repetition / reminders between sessions or
sessions closer together◦ Support / booster group for program “graduates”
Subject & SO Debriefing

3-center study (with control group) has just been funded by NIH to begin summer 2011
Trajectory of treatment effects◦ Do we need all 8 sessions to get an effect? Would
4 sessions work just as well?◦ Do positive effects persist after treatment?
Are there broader effects on other aspects of daily living?
For whom does it work? Do people benefit more at a given level of cognitive ability, time post TBI, etc?
What’s Next?