Technology Innovations from Devices for Dignity (Avril McCarthy)
20
Healthcare science in action – how scientific and technological innovations are supporting service personnel on their return from combat Avril McCarthy, Lead Clinical Scientist & MedTech Lead for D4D Technology Innovations from “Devices for Dignity” (D4D) Healthcare Technology Co-operative (HTC) HTCs: “National resources embedded in the NHS, intended to accelerate new treatments and technologies into practice to improve healthcare quality and well-being for patients.”
-
Upload
ahcs -
Category
Health & Medicine
-
view
45 -
download
0
Transcript of Technology Innovations from Devices for Dignity (Avril McCarthy)

Healthcare science in action – how scientific and technological innovations are supporting service personnel on their return from combat
Avril McCarthy, Lead Clinical Scientist & MedTech Lead for D4D
Technology Innovations from “Devices for Dignity” (D4D) Healthcare Technology Co-operative (HTC)
HTCs: “National resources embedded in the NHS, intended to accelerate new treatments and technologies into practice to improve healthcare quality and well-being for patients.”

Outline
• Overview of Devices for Dignity (D4D)
• Relevance of D4D to Injured Combatants
• Challenges / opportunities for Healthcare Science

Mick Brennan, ex Royal Signals from Doncaster, Sochi 2014
To deliver innovative healthcare technologies
that preserve dignity and promote independence
for people of all ages living with long term conditions
D4D Mission:
Clinicians
Academia
Businesses
Patient
focus Patients and
Public

Relevance of D4D to Injured Combatants
• D4D focuses on functional limitations that impact dignity & independence irrespective of cause – holistic approach
• Dignity: core value of Geneva Convention
– human dignity of all individuals must be respected at all times
• 4.8M veterans in UK ( estimate)
– 2.9M > 65yrs
– 52% of veterans have a long-term illness, disability or infirmity (compared to 35% for non-veterans)
Paralysed ex-serviceman “Terry” using an environmental control system to open his front door remotely

Urinary Continence Management (UCM) Major reason for loss of self-esteem/social isolation 2nd most common reason for need for institutional care
Renal Technologies (RT) 0.05% of population on dialysis but 2% of NHS budget
14% of older population with CKD
Assistive and Rehabilitative Technologies (ART) 11 million people in the UK with disabilities
Three areas of focus (Themes):

Functional Limitations & Causes
Stroke
Traumatic Brain Injury
Loss of
Mobility
Limb deficiencies
from amputation
Impaired:
Swallowing
Speech
Cognition /
memory
Impaired
muscle
control
Meningitis Trauma
Incontinence
Spinal Cord Injury
Diabetes
Impaired Senses

Functional Limitations & Causes
Stroke
Traumatic Brain Injury
Loss of
Mobility
Limb deficiencies
from amputation
Impaired:
Swallowing
Speech
Cognition /
memory
Impaired
muscle
control
Meningitis Trauma
Incontinence
Spinal Cord Injury
Diabetes
Impaired Senses

Functional Limitations & Causes
Stroke
Traumatic Brain Injury
Loss of
Mobility
Limb deficiencies
from amputation
Impaired:
Swallowing
Speech
Cognition /
memory
Impaired
muscle
control
Meningitis Trauma
Incontinence
Spinal Cord Injury
Diabetes
Impaired Senses

D4D Project Portfolio
22 MedTech Projects:
• ART: Postural support, mobility aids, swallowing, communication aids
• RT: Monitoring & self-management technologies
• UCM: Catheter design, treatments for incontinence, early diagnosis of urinary infections
And importantly - we are open to suggestions for new unmet needs
Example D4D Technologies

Banter, Bevvies & Bathrooms…
Communication difficulties – no banter
– Giving or restoring a voice to those who have lost their own – common in TBI
1. Improved communication aids in ICU for those mechanically ventilated , willing but unable to speak
2. Improved text-to-speech prediction app with choice of voices
3. Self-directed speech therapy for retraining vocal muscles
• NIHR i4i Project about to start
Ben Parkinson with his voice output aid – he then progressed so donated it to a Veteran
who’d had a stroke

Banter, Bevvies & Bathrooms…
Swallowing difficulties TBI dysphagia incidence: 38%-65%
– High risk of aspiration pneumonia
Electrical stimulation (ES) therapy
– Stimulation + exercise to improve swallow function
– Randomised pilot trial: 1mth+ post-stroke
• 75% ES with significantly improved swallow v 57% on normal treatment (control)
• Significant improvement in ES QoL (SwalQol)
– Fully powered trial in planning
Nutrition in a bag
Banter, Bevvies & Bathrooms…
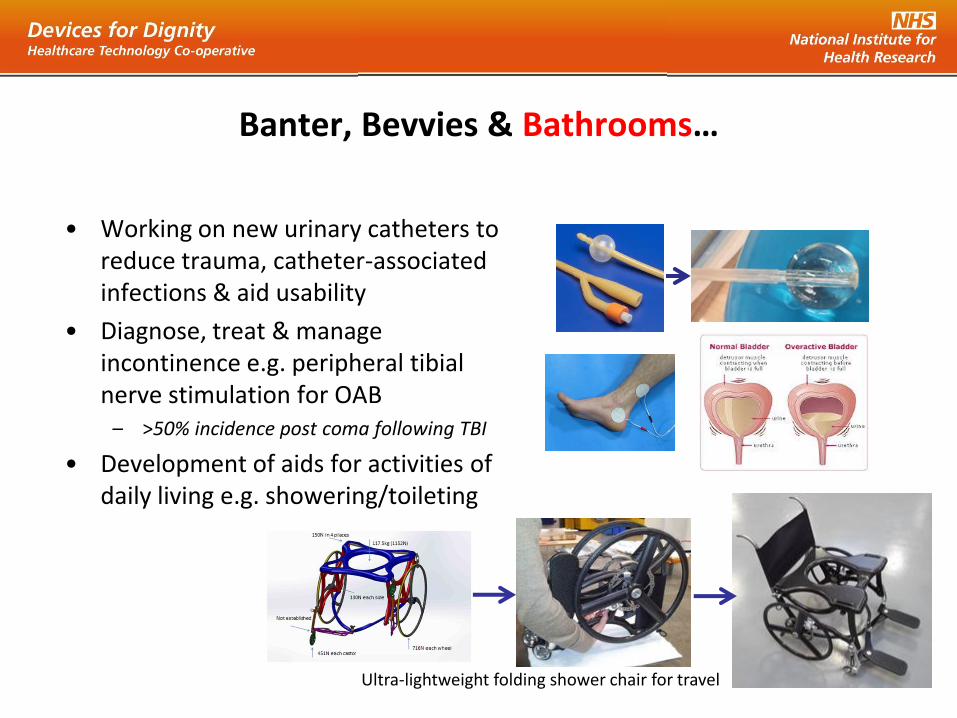
• Working on new urinary catheters to reduce trauma, catheter-associated infections & aid usability
• Diagnose, treat & manage incontinence e.g. peripheral tibial nerve stimulation for OAB
– >50% incidence post coma following TBI
• Development of aids for activities of daily living e.g. showering/toileting
Ultra-lightweight folding shower chair for travel
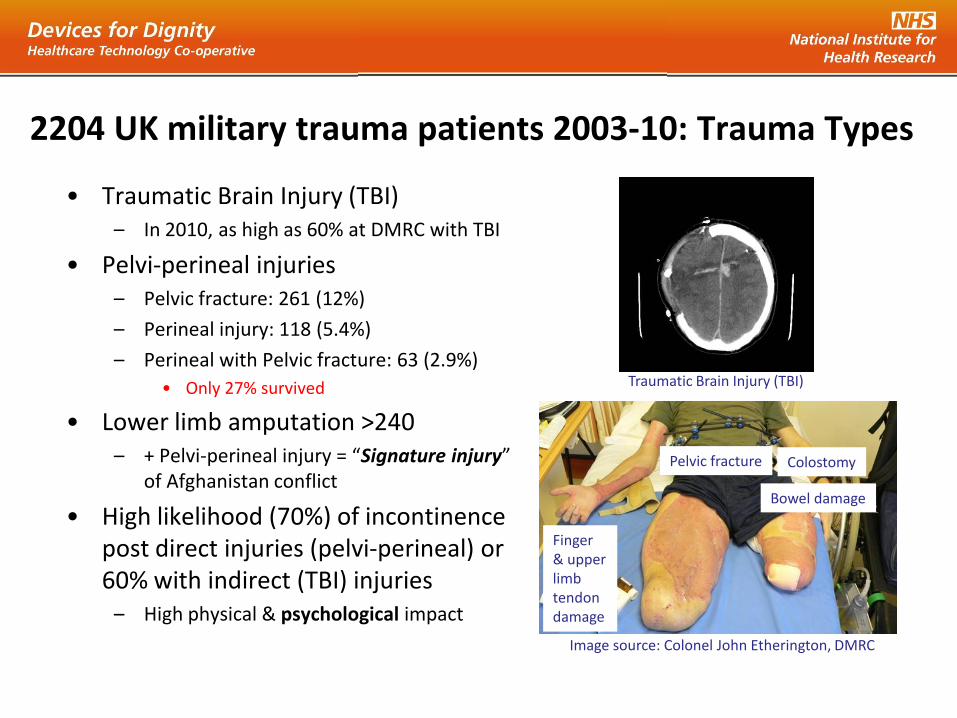
2204 UK military trauma patients 2003-10: Trauma Types
• Traumatic Brain Injury (TBI) – In 2010, as high as 60% at DMRC with TBI
• Pelvi-perineal injuries – Pelvic fracture: 261 (12%)
– Perineal injury: 118 (5.4%)
– Perineal with Pelvic fracture: 63 (2.9%)
• Only 27% survived
• Lower limb amputation >240 – + Pelvi-perineal injury = “Signature injury”
of Afghanistan conflict
• High likelihood (70%) of incontinence post direct injuries (pelvi-perineal) or 60% with indirect (TBI) injuries
– High physical & psychological impact
Image source: Colonel John Etherington, DMRC
Colostomy
Bowel damage
Pelvic fracture
Finger & upper limb tendon damage
Traumatic Brain Injury (TBI)

Rehabilitation Challenges: Prosthetic
• Number / Complexity of other injuries
– e.g. Donning & doffing prosthetics one-handed or with missing digits
– Spasticity related to TBI/SCI
– Sensory loss
• Complex stump/socket interface
– Achieving a stable fit
– Risk of further injuries if a poor fit (pressure ulcers etc )
– Heterotopic ossification (uncontrolled remodelling)
• Upper limb devices
– > degrees of freedom needed so more challenging control problem
Genium X3 “bionic” waterproof, above knee lower limb prosthesis (left) in action
Heterotopic ossification
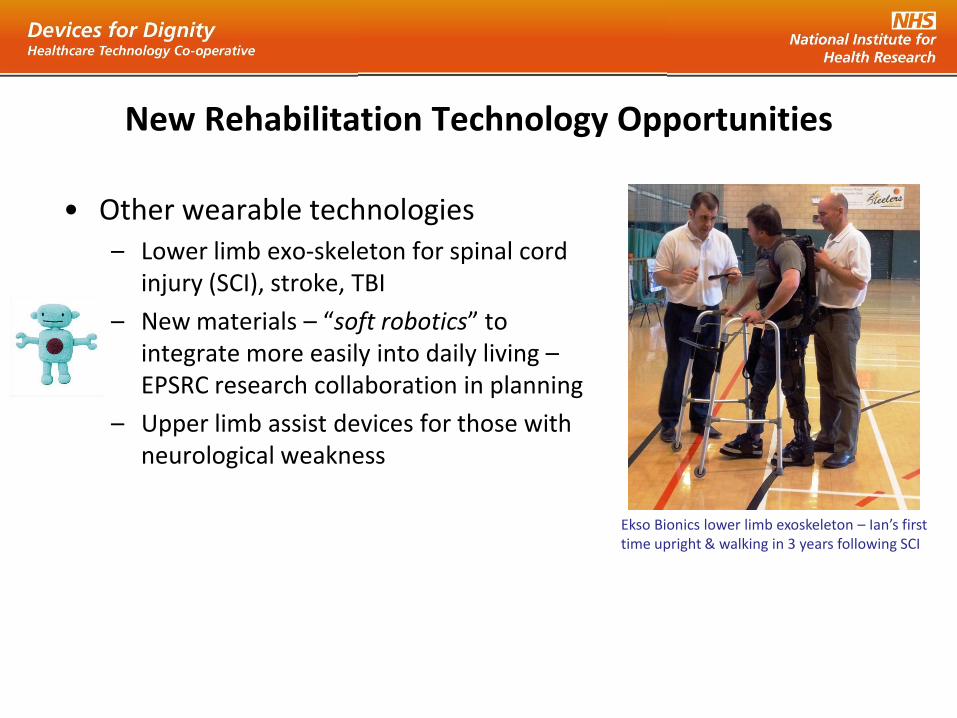
New Rehabilitation Technology Opportunities
• Other wearable technologies – Lower limb exo-skeleton for spinal cord
injury (SCI), stroke, TBI
– New materials – “soft robotics” to integrate more easily into daily living – EPSRC research collaboration in planning
– Upper limb assist devices for those with neurological weakness
Ekso Bionics lower limb exoskeleton – Ian’s first time upright & walking in 3 years following SCI


Evolving challenges for Healthcare Science (& Society)
Conflicts have led to accelerated advances in emergency medicine / rehab that also benefit non-military patients.
• However, leads to number / complexity / severity of now survivable injuries
• Resulting in long-term support challenges
– Requiring a comprehensive integrated approach (including psychological)
• Including planning for long-term care of ageing survivors
– Those with life-changing injuries will also begin to experience age-related conditions

We should view the survivors’ experiences as a valuable resource & invite them to help co-develop medical technologies for the future
Opportunities for Healthcare Science (& Society)
D4D Innovation Model

8 NIHR HTCs: Direct/indirect relevance to combatants
NIHR HTC Name Host NHS Trust Research Theme/s
Brain Injury Cambridge
University Hospitals Acquired & developmental brain injury across acute care pathway
Cardiovascular Guy’s and St
Thomas’ Atherosclerosis, Arrhythmias, Heart failure & structural heart disease
Colorectal Therapies Leeds Teaching
Hospitals Minimally invasive therapies for colorectal disease
Devices for Dignity Sheffield Teaching
Hospitals
Urinary incontinence management, renal technologies, assistive &
rehabilitative technologies
Enteric Barts Health Stoma complications, neuromodulation for faecal incontinence, novel
diagnostics for chronic GI disease, improved GI surgery
MindTech Nottinghamshire Mental Health and neuro-developmental disorders
Trauma Management University Hospitals
of Birmingham
Trauma: Immediate Care, Secondary Care, Regeneration,
Rehabilitation
WoundTec Bradford Teaching
Hospitals Wound management

Lest we forget…
“Treat your men/women as you would your own
beloved sons/daughters.
And they will follow you into the deepest valley.”
Sun Tzu, c 510BC, “The Art of War”,
Submit an unmet need: www.devicesfordignity.org.uk