
Technology, Expectations, and Adjustment to Hearing … · Technology, Expectations, and Adjustment...
16
J Am Acad Audiol 12 : 64-79 (2001) Technology, Expectations, and Adjustment to Hearing Loss : Predictors of Hearing Aid Outcome J. Christopher K . Jerram* Suzanne C. Purdy*t Abstract This study examined the influence of technology, demographic factors, and prefitting expec- tations, attitudes, and adjustment to hearing loss on hearing aid outcome . Clients obtaining new hearing aids completed questionnaires measuring personal adjustment to hearing loss, expectations of and attitudes toward hearing aids, and hearing aid benefit . Eighty-one per- cent of the 200 subjects completing the prefitting questionnaires returned questionnaires evaluating hearing aid outcome. Factors affecting hearing aid use, overall satisfaction, and benefit were investigated using regression analyses . Higher use time was associated with higher prefitting expectations and greater acceptance of hearing loss . Greater benefit in easy and difficult listening situations was predicted by higher prefitting expectations . Multiple- memory hearing aids produced higher satisfaction . Benefit was greater for multiple-memory, multiple-channel, and wide dynamic range compression aids . Findings were consistent with previous studies showing positive outcomes for newer technologies but also showed that two subjective factors, prefitting hearing aid expectations and acceptance of hearing loss, sig- nificantly influenced hearing aid outcome . Key Words : Attitude, benefit, expectations, hearing aid, hearing aid use, personal adjust- ment, questionnaire, satisfaction, technology Abbreviations : APHAB = Abbreviated Profile of Hearing Aid Benefit, BTE = behind the ear, CIC = completely in the canal, CPHI = Communication Profile for the Hearing Impaired, HAPI = Hearing Aid Performance Inventory, HARQ = Hearing Attitudes in Rehabilitation Questionnaire, HHIE = Hearing Handicap Inventory for the Elderly, HPI = Hearing Performance Inventory, ITC = in the canal, ITE = in the ear, MAPHAB = Modified Abbreviated Profile of Hearing Aid Benefit, MELLI = multiple environmental listening utility, MPAS = Modified Personal Adjustment Scale, PHAB = Profile of Hearing Aid Benefit, SADL = Satisfaction with Amplification in Daily Living, WDRC = wide dynamic range compression A vaiiety of measures have been developed to assess hearing aid outcome including aided performance and benefit, satis- faction with hearing aids, and amount of hear- ing aid use (Brooks, 1990 ; Dillon et al, 1999 ; Humes, 1999). Hearing aid benefit can be defined as an increase in hearing ability after provision of an aid. Objective benefit measures do not require the wearer to express an opinion or *Audiology Section, Department of Physiology, The University of Auckland, Auckland, New Zealand ; tNational Acoustic Laboratories, Sydney, Australia Reprint requests : Chris Jerram, Audiology Section, Department of Physiology, The University of Auckland, Faculty of Medicine and Health Sciences Private Bag 92019, Auckland, New Zealand judgment regarding the hearing aids . There are many objective speech recognition tests that can be used to assess benefit (Levitt and Resnick, 1978) and purely acoustic tests of hearing aid function in a coupler or on the person's ear (Wet- zell and Harford, 1983 ; Mueller, 1992) . Subjec- tive measures of benefit require a judgment or opinion, such as loudness or quality judgments using rating scales (e.g ., Arlinger and Biller- mark, 1999 ; Jenstad et al, 1999) . Subjective hearing aid benefit also has been measured as reduction in perceived disability or handicap (Weinstein, 1990) . The International Classification of Impairments, Disabilities, and Handicaps developed in 1980 by the World Health Organization defines disability as the degree to which a physical impairment causes 64
Transcript of Technology, Expectations, and Adjustment to Hearing … · Technology, Expectations, and Adjustment...
J Am Acad Audiol 12 : 64-79 (2001)
Technology, Expectations, and Adjustment to Hearing Loss : Predictors of Hearing Aid Outcome J. Christopher K. Jerram* Suzanne C. Purdy*t
Abstract
This study examined the influence of technology, demographic factors, and prefitting expec-tations, attitudes, and adjustment to hearing loss on hearing aid outcome. Clients obtaining new hearing aids completed questionnaires measuring personal adjustment to hearing loss, expectations of and attitudes toward hearing aids, and hearing aid benefit. Eighty-one per-cent of the 200 subjects completing the prefitting questionnaires returned questionnaires evaluating hearing aid outcome. Factors affecting hearing aid use, overall satisfaction, and benefit were investigated using regression analyses . Higher use time was associated with higher prefitting expectations and greater acceptance of hearing loss . Greater benefit in easy and difficult listening situations was predicted by higher prefitting expectations . Multiple-memory hearing aids produced higher satisfaction . Benefit was greater for multiple-memory, multiple-channel, and wide dynamic range compression aids . Findings were consistent with previous studies showing positive outcomes for newer technologies but also showed that two subjective factors, prefitting hearing aid expectations and acceptance of hearing loss, sig-nificantly influenced hearing aid outcome.
Key Words: Attitude, benefit, expectations, hearing aid, hearing aid use, personal adjust-ment, questionnaire, satisfaction, technology
Abbreviations: APHAB = Abbreviated Profile of Hearing Aid Benefit, BTE = behind the ear, CIC = completely in the canal, CPHI = Communication Profile for the Hearing Impaired, HAPI = Hearing Aid Performance Inventory, HARQ = Hearing Attitudes in Rehabilitation Questionnaire, HHIE = Hearing Handicap Inventory for the Elderly, HPI = Hearing Performance Inventory, ITC = in the canal, ITE = in the ear, MAPHAB = Modified Abbreviated Profile of Hearing Aid Benefit, MELLI = multiple environmental listening utility, MPAS = Modified Personal Adjustment Scale, PHAB = Profile of Hearing Aid Benefit, SADL = Satisfaction with Amplification in Daily Living, WDRC = wide dynamic range compression
A
vaiiety of measures have been developed to assess hearing aid outcome including aided performance and benefit, satis-
faction with hearing aids, and amount of hear-ing aid use (Brooks, 1990 ; Dillon et al, 1999; Humes, 1999). Hearing aid benefit can be defined as an increase in hearing ability after provision of an aid. Objective benefit measures do not require the wearer to express an opinion or
*Audiology Section, Department of Physiology, The University of Auckland, Auckland, New Zealand ; tNational Acoustic Laboratories, Sydney, Australia
Reprint requests : Chris Jerram, Audiology Section, Department of Physiology, The University of Auckland, Faculty of Medicine and Health Sciences Private Bag 92019, Auckland, New Zealand
judgment regarding the hearing aids . There are many objective speech recognition tests that can be used to assess benefit (Levitt and Resnick, 1978) and purely acoustic tests of hearing aid function in a coupler or on the person's ear (Wet-zell and Harford, 1983; Mueller, 1992). Subjec-tive measures of benefit require a judgment or opinion, such as loudness or quality judgments using rating scales (e .g ., Arlinger and Biller-mark, 1999 ; Jenstad et al, 1999).
Subjective hearing aid benefit also has been measured as reduction in perceived disability or handicap (Weinstein, 1990). The International Classification of Impairments, Disabilities, and Handicaps developed in 1980 by the World Health Organization defines disability as the degree to which a physical impairment causes
64

dysfunction and handicap as the psychosocial
sequelae of this (Badley and Lee, 1987a, b; Badley et al, 1987 ; Arnold and MacKenzie, 1998).
Many different self-assessment scales have been developed to measure hearing disability and
handicap (Noble, 1998), including the Profile of Hearing Aid Benefit (PHAB, Cox et al, 1991) and
the Hearing Handicap Inventory for the Elderly (HHIE, Ventry and Weinstein, 1982), which
have been used extensively to measure hearing
aid benefit in the realms of disability (PHAB) and
handicap (HHIE) . Humes (1999) identified several components
of hearing aid outcome including aided perfor-mance measured by speech recognition scores and the HHIE, hearing aid use time, loudness and sound quality ratings, and satisfaction . Sat-isfaction is an internalized construct that can be measured as a single global measure (Brooks, 1985 ; Kuk and Pape, 1993 ; Dillon et al, 1999) or as separate components (Kochkin, 1993, 1995 ; Cox and Alexander, 1999) . Although overall sat-isfaction is related to benefit, satisfaction and benefit are separate dimensions of hearing aid success (Kochkin, 1995 ; Purdy and Jerram, 1998 ; Humes, 1999) .
The psychosocial effects of hearing aids have also been studied . Mulrow et al (1990) reported
improved cognitive function and reduced depres-sion in clients fitted with hearing aids compared with a control group of waiting list clients .
Bridges and Bentler (1998) found higher ratings of life satisfaction in successful hearing aid
wearers . Garstecki and Erler (1998) found fewer
depressive tendencies among hearing aid wear-ers than hearing aid nonwearers, and Crandell (1998) found that hearing aids have a positive impact on functional health status in elderly
listeners . In a recent large study of hearing-impaired listeners and their family and friends,
Kochkin and Rogin (2000) reported many posi-
tive effects of hearing aids on quality of life .
Predicting Hearing Aid Outcome
Many variables have been investigated as possible predictors of success with hearing aids .
For example, Mulrow et al (1992) found that
greater baseline perceived handicap, younger
age, lower education level, greater degree of
high-frequency hearing aid gain, better near
visual acuity, and fewer number of medications all positively influenced hearing aid outcome .
The present study investigated the effects on hearing aid outcome of demographic, hearing aid technology, and subjective predictor variables .
Predictors of Hearing Aid Outcome/Jerram and Purdy
A number of previous studies have examined these variables.
Age, Hearing Loss, and Gender
Deterioration in central auditory function in
older hearing aid wearers can adversely affect hearing aid outcome (Kricos et al, 1987 ; Gate-
house, 1990 ; Stach et al, 1991) . General ill
health, loss of mobility, and social isolation
(Welzl-Miiller and Stephan, 1986 ; Stephens and
Meredith, 1991 ; Evenhuis, 1995 ; Cohn, 1999)
also reduce success with hearing aids in elderly hearing aid wearers . This is consistent with reports of reduced hearing aid performance with increasing age (Crowley and Nabelek, 1996 ; Jer-ram and Purdy, 1997) .
People with greater hearing loss wear their hearing aids more often (Brooks, 1985 ; Sather-ley, 1992). The reported relationship between audiometric thresholds and hearing aid benefit is variable, ranging from nonsignificant (Schum, 1992) to significant (Kochkin,1995), with greater benefit usually being associated with greater loss . As expected, poorer hearing aid perfor-mance is associated with worse hearing thresh-olds (Purdy and Jerram, 1998).
Garstecki and Erler (1998) found differ-
ences between the sexes when they compared
hearing aid wearers and nonwearers using the Communication Profile for the Hearing Impaired
(CPHI) inventory. Significant gender differences were present for 6 of the 25 CPHI scales (Prob-
lem Awareness, Social Communication Impor-
tance, Nonverbal strategies, Anger, Stress, and Denial) . Women were more likely to admit to communication problems, use nonverbal strate-gies to remedy difficult communication situa-tions, and report feelings of anger, stress, and negative emotions than men. Crowley and Nabelek (1996) found no effect of gender on rat-ings of hearing aid performance, but Garsteki and Erler's (1998) results suggest that gender may affect some hearing aid outcome measures .
Hearing Aid Technology
Choice of monaural or binaural hearing aid fitting affects outcome, with greater success found for binaural fittings (Brooks, 1984 ; Day et al, 1988 ; McKenzie and Rice, 1990), particu-larly for directional hearing aids (Leeuw and Dreschler, 1991).
A variety of new hearing aid technologies are currently available that aim to enhance per-
ception of speech, particularly in background
65

Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
noise. This includes digital circuitry, multiple memories, multiple microphones, multiple-frequency channels, and various forms of com-pression . Kochkin (1996) found that outcomes were consistently better for newer "high-performance" hearing aids (higher overall sat-isfaction, perceived improvement in quality of life and benefit, etc.) . Modern digital hearing aids generally provide clearer sound than older ana-log aids (Kates and Weiss, 1996 ; Kiessling, 1996 ; Arlinger et al, 1998 ; Valente et al, 1998). Mul-tiple-memory hearing aids have proved an effec-tive way of adjusting amplification for specific listening situations (Keidser, 1995; Berninger and Nordstrom, 1997). Dual-microphone sys-tems result in improved speech perception in noise (Valente, 1999). Overall satisfaction with hearing aids is highly related to the number of listening situations in which wearers' needs are met (Kochkin, 1996). Kochkin (1996) found that multiple-memory and multiple-microphone hear-ing aids, allowing different amplification char-acteristics in different listening situations, provide the highest satisfaction.
Channelling of the incoming signal into more than one frequency band allows indepen-dent adjustment according to the degree of hear-ing loss in that frequency region . Many modern hearing aids have multiple channels, allowing compression parameters to vary across fre-quency. Kochkin (1996) found higher "usage sat-isfaction" among users of multiple-channel hearing aids compared with single-channel aids .
It is still not clear whether new nonlinear compression circuits, in which amplification is reduced for loud sounds, are better than linear (equal amplification for loud and soft sounds) for speech understanding in noise (Byrne, 1996 ; Verschuure et al, 1996). Dillon (1996) reviewed the compression literature and concluded that for speech in quiet at a comfortable level, no com-pression scheme yet tested offers better intelli-gibility than individually selected linear amplification.
Variable results have been found regard-ing the relative advantages of the four main hearing aid styles : behind the ear (BTE), in the ear (ITE), in the canal (ITC), and, recently, com-pletely in the canal (CIC). Smaller ITE and CIC hearing aids are less associated with the stigma of hearing loss than the more conspicuous BTE style (Brooks, 1994) . ITE hearing aids can pre-sent handling problems in older hearing aid users (Meredith and Stephens, 1993) but not con-sistently (Upfold and May, 1990). The latter study found no difference in performance
between ITC, ITE, and BTE hearing aids in elderly hearing aid wearers. CIC hearing aids appeal to younger, less impaired individuals, but wearers rate CIC hearing aids lower on reli-ability, ease of adjusting, and performance rel-ative to cost (Kochkin, 1995).
Psychosocial Factors
Several studies have examined the effects of personality on hearing aid outcome (Gate-house, 1994 ; Scott et al, 1994 ; Cox et al, 1999). Cox et al (1999) found that a more outward-looking personality gained higher benefit in the Easy Listening, Reverberant, and Background Noise subscales of the abbreviated version of the PHAB (APHAB). Gatehouse (1994) found that depression was associated with less hearing aid use and lower reports of hearing aid benefit and satisfaction . Other aspects of personality mea-sured with the Crown-Crisp Experiential Index were also highly correlated with hearing aid outcome (Gatehouse, 1994 ; Noble, 1998).
Several studies have examined the influence of attitudes toward hearing loss and hearing aids on hearing aid outcomes (Hickson et al, 1986, 1999 ; Brooks, 1989 ; Gatehouse, 1994 ; Hal-lam and Brooks, 1996). Using the Hearing Atti-tudes in Rehabilitation Questionnaire (HARQ), Hallam and Brooks (1998) found that clients who were least distressed by their hearing dif-ficulties and reported not wanting or needing a hearing aid used their aids least frequently and evaluated them less highly in listening situa-tions. Gatehouse (1994) and Hickson et al (1986, 1999) found a significant positive relationship between attitudes toward hearing aids and their use.
Personal adjustment to disability also has been associated with rehabilitation outcome (Brown and Munford, 1984 ; Corso, 1987 ; Burke et al, 1988) and is seen as important in offering guidelines for aural rehabilitation (May, 1986 ; Stephens, 1996). Crowley and Nabelek (1996) found that personal adjustment to hearing loss measured using the CPHI was predictive of hear-ing aid performance in difficult listening situations measured using the Profile of Hearing Aid Per-formance (Cox and Gilmore,1990) . In contrast, Cox and Rivera (1992) found that CPHI composite scores were not predictive of PHAB benefit.
Counselling to ensure that hearing aid wear-ers make informed choices, have realistic expec-tations, and know how to use hearing aids has been found to influence hearing aid success in adults (Brooks and Johnson, 1981 ; McCarthy et
66
Predictors of Hearing Aid Outcome/Jerram and Purdy
al, 1990; Rose and Pool, 1994; Kapteyn et al,
1997 ; Kochkin, 1999) . Kricos et al (1991) devel-oped a 48-item expectations checklist and found
that 87 percent of participants had high expec-
tations of hearing aids . Schum (1999) found that candidates for amplification tend to expect
more benefit than they will typically achieve,
especially when listening to speech in noise or without visual cues . In contrast, Bentler et al's (1993) results suggested that performance
exceeded expectations . Schum (1999) concluded
that hearing aid benefit could not be reliably pre-
dicted from perceived need or expectation . Brooks and Johnson (1981) reported that prefitting counselling had a positive effect on hours of
hearing aid use and satisfaction with hearing
aids, which suggests that realistic expectations should improve hearing aid outcomes .
The present study was designed to evaluate
which, if any, of a number of the predictor vari-
ables discussed above influence three measures of hearing aid outcome, perceived hearing aid
benefit, overall satisfaction, and daily hours of hearing aid use .
METHOD
Subjects
A total of 12 private and 7 public hospital audiology clinics participated in the study. Over an approximately 18-month period, adult prospective hearing aid wearers undergoing their initial hearing aid evaluation were intro-duced to the study by their audiologist . Consent forms were received from 225 potential partic-ipants . Each was sent questionnaires examin-ing personal adjustment to hearing loss, hearing aid expectations, attitudes to hearing aids (Appendix), and unaided hearing ability, to be completed and mailed to the researcher prior to fitting of hearing aids . Complete sets of ques-tionnaires were received from 200 individuals (89% response rate). These 200 individuals received a copy of the aided version of the Mod-ified APHAB (MAPHAB) and the satisfaction questionnaire for completion and return approx-imately 10 weeks after their final hearing aid follow-up appointment.
Completed aided questionnaires were received from 162 subjects (81% return rate), 81 males and 81 females. Seventy-six of these sub-jects (47%) attended public hospital clinics, and 86 (53%) attended private clinics. Ages ranged
from 31 to 88 years (mean = 70.5 years, SD =10.8).
Twenty-five were fully employed, 13 were partially employed, and 124 were not employed outside the
home . Sixty-one subjects were new hearing aid
users, and 101(62%) had some prior hearing aid
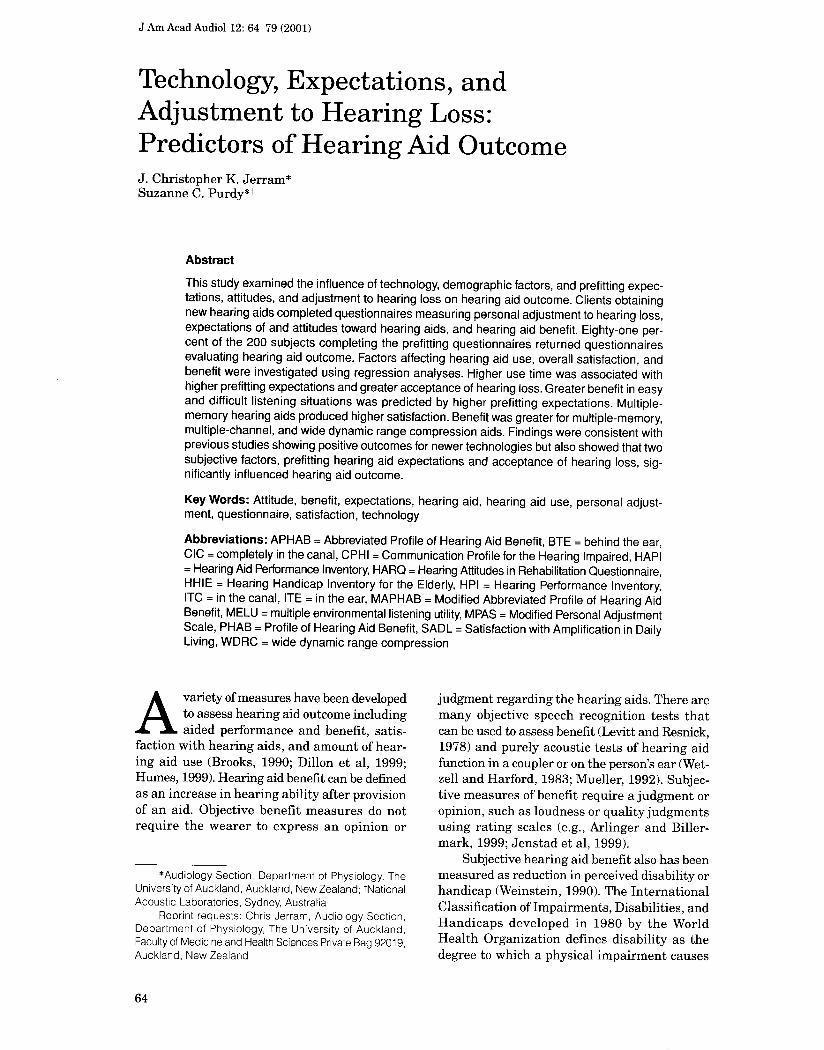
experience . Figure 1 shows the subjects' mean
right and left ear pure-tone thresholds in the fre-
quency range of 0.5 to 4 kHz . All had sensorineural
hearing loss .
Outcome Measures
Hearing aid outcome was measured in three
ways : daily hearing aid use time, hearing aid benefit, and overall satisfaction . Overall hear-
ing aid satisfaction was measured using a sin-
gle 20-point rating scale ranging from "very,
very dissatisfied" (1) to "very, very satisfied"
(20) . Subjects were asked to indicate the amount
of hearing aid use (0-1, 1-4, 4+ hours per day) . Hearing aid benefit was measured using a mod-ified version of the APHAB questionnaire (Cox
and Alexander, 1995), which evaluates unaided and aided hearing performance in 24 listening situations . Hearing aid benefit is measured as
the difference in hearing performance with and
without a hearing aid. A positive difference in scores between unaided and aided versions indi-
cates that hearing aids are beneficial . The
APHAB measures benefit in four types of lis-tening environment: Ease of Communication,
Reverberation, Background Noise, and Aver-
siveness of Sounds . Factor analysis of the aided
version of the APHAB for New Zealand listen-
-10
10
30
50
70
90
110 0 .5 1 2 4
Frequency (kHz)
Figure 1 Mean left and right ear audiometric thresh-
olds (dB HLl of the 162 subjects completing the study.
Error bars show standard deviations .
67

Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
ers (Purdy and Jerram, 1998) revealed three factors that roughly matched the four scales of Cox and Alexander (1995) . These factors repre-sent easy and difficult listening situations and listening to aversive environmental sounds . Purdy and Jerram (1998) dropped two items from the questionnaire due to poor response rates. The resulting 22-item questionnaire, the MAPHAB, was used in the present study as a measure of hearing aid outcome. The APHAB response scale was altered from the original to be an equal-interval scale (Keller et al, 1998), with a scale ranging from never (0%) to always (100%) with 10 percent increments marked on the scale.
Client and Hearing Aid Predictor Variables
For subjects who completed the study, clin-icians provided information on subject age; pure-tone hearing thresholds at 0.5, 1, 2, and 4 kHz ; type of hearing loss ; monaural or bin-aural fitting, hearing aid style; and type of hearing aid technology (peak clipping, output, input, and wide dynamic range compression [WDRC]; multiple microphone ; multiple mem-ory; multiple channel). When they completed the final hearing aid questionnaires, subjects were asked to indicate the duration of hearing aid experience (<6 weeks, 6 weeks-11 months, >1 year) and employment status (full time, part time, not employed outside the home).
The adjustment factor of the CPHI, consist-ing of 100 items comprising 13 of the 25 origi-nal CPHI subscales (Demorest and Erdman, 1986, 1987, 1989), has been used to measure per-sonal adjustment to hearing loss in a range of domains (Crowley and Nabelek, 1996 ; Erdman and Demorest, 1998; Jerram and Purdy, 1999). Jerram and Purdy (1999) obtained high (> 0.8) alpha internal consistency values (Cronbach, 1951) for New Zealand listeners with hearing impairment for 7 of the 13 adjustment factor sub-scales . Three of the adjustment subscales with high internal consistency (Jerram and Purdy, 1999), Acceptance of Loss, Stress, and Denial, were used to assess personal adjustment to hearing loss in the present study. The 25-item questionnaire containing the three adjustment subscales was called the Modified Personal Adjustment Scale (MPAS) .
Items in the Acceptance of Loss and Stress subscales are negatively worded, with a 5-point rating scale ranging from "strongly disagree" (1) to "strongly agree" (5). A high score indicates
poor personal adjustment in coping with the statement described. According to the analysis procedure of Demorest and Erdman (1987), scores are reversed, and after reversal, a high score is indicative of a good level of personal adjustment . For items in the Denial subscale, a low score indicates denial of a negatively worded statement. Persistent disagreement with com-mon emotional reactions experienced by listen-ers with hearing impairment represents an unwillingness to admit that a problem exists-thus, a poor personal adjustment to the problem. Items in the Denial subscale are therefore not reversed to keep scoring for this subscale par-allel to that of the other subscales.
Prefitting attitudes toward hearing aids were measured using the factor 1 ("hearing aid stigma") items in the hearing aid section of the HARQ (Hallam and Brooks, 1996). The HARQ subscale consists of eight negatively worded items (e.g ., "It would make me feel old to wear a hearing aid") and one positively worded item (item 9, "I think the BTE hearing aids are really quite small and inconspicuous"). Scoring ranges from "true" (1) to "not true" (3). Scoring is reversed for item 9; thus, a high score represents a positive attitude toward hearing aids .
Prefitting hearing aid expectations were measured using the expectations questionnaire developed by Seyfried (1990) . Seyfried's ques-tionnaire contains 12 items, 7 of which are pos-itively worded (e.g ., "My hearing aids will fit comfortably") and 5 of which are negatively worded (e.g ., "I will adjust slowly to my hearing aids") . Scoring ranges from "strongly agree" (1) to "strongly disagree" (6) for all items . For analysis, scoring is reversed for the negatively worded items so that a low score represents high expectations .
RESULTS
Hearing Aid Characteristics
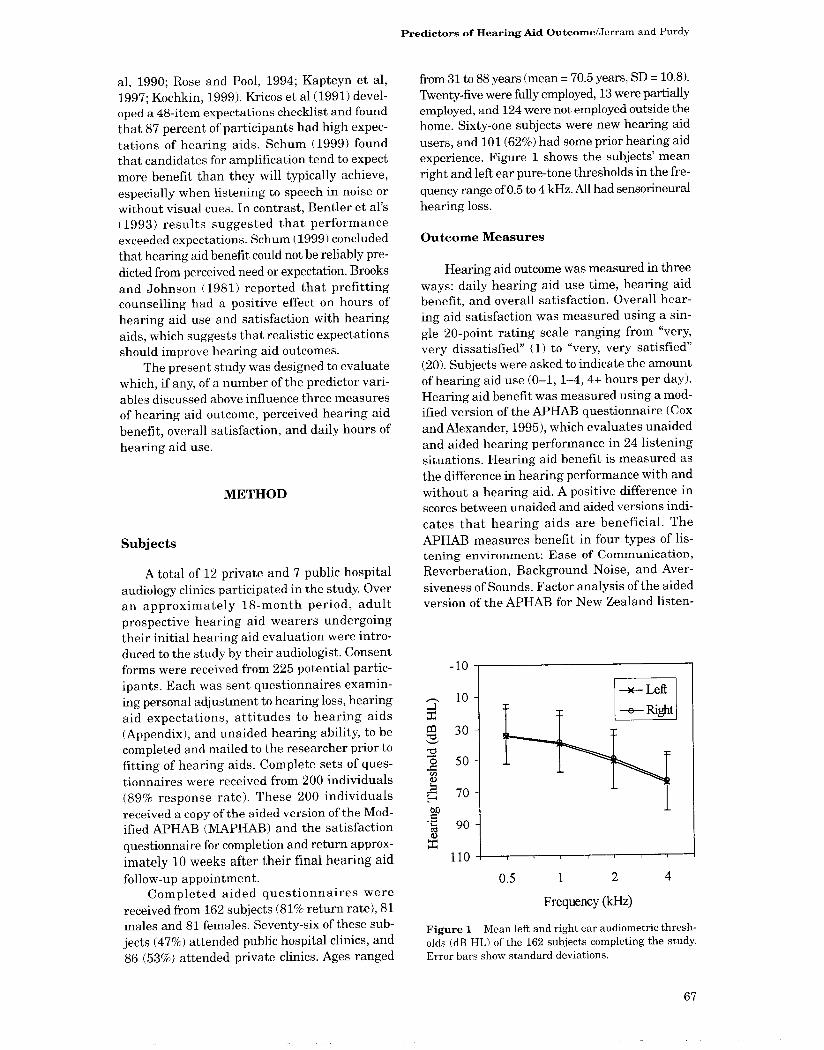
Ninety-five subjects (59%) were binaurally fitted, and 67 (41%) were monaurally fitted . Figure 2 shows numbers of subjects wearing hearing aids with each of the hearing aid tech-nologies that were examined as predictors of outcome. The most widely prescribed technology was WDRC. Very few subjects wore linear peak-clipping hearing aids . Multiple-memory and multiple-frequency channel aids were prescribed more often than multiple-microphone aids .
68
Predictors of Hearing Aid Outcome/Jerram and Purdy
WDRC
63 0
U U E~ b a .Cd `0 x
Other C
P-clip
M-band
M-mem
M-mic
items in the expectations questionnaire had very poor item-total correlations (9, 11, and 12) and were not included in subsequent analyses . With these three items excluded, Cronbach's alpha was 0.60 for the expectations questionnaire (n = 171) . Bentler et al (1993) analyzed subsets of Seyfried's (1990) expectations questions and derived a subset of five items yielding a higher alpha value (0.74) . This subset resulted in a poor alpha value (0.45) in the present study, lower than that obtained when all 12 items were included (0.49) .
0 20 40 60 80 100
Subjects Using Technology
Figure 2 Numbers of subjects using each type of hearing aid technology : wide dynamic range compres-sion (WDRC), other types of input or output compres-
sion (Other C), peak clipping (P-Clip), multiple channels (M-band), multiple memories (M-mem), and multiple microphones (M-mic). These results are based on the
audiologists' reports for the 162 subjects who returned the aided questionnaires .
Item Analysis of Prefitting Questionnaires
Item analyses were performed to determine internal reliability of the personal adjustment, expectations, and hearing aid attitudes ques-
tionnaires completed by the 200 subjects who responded to the first mail-out . Only question-naires with no missing values were included in the analysis . Reliability was excellent (Cron-bach's alpha = 0 .90-0 .92) for the WAS per-sonal adjustment subscales, Acceptance of Loss
(n = 153), Stress (n = 152), and Denial (n = 144) . Item 9 of the HARQ attitudes scale was poorly correlated with the other items in the ques-tionnaire. Cronbach's alpha for the HARQ, excluding item 9, was 0 .81 (n = 189) . Three
Results for Subjects Completing Aided Questionnaires
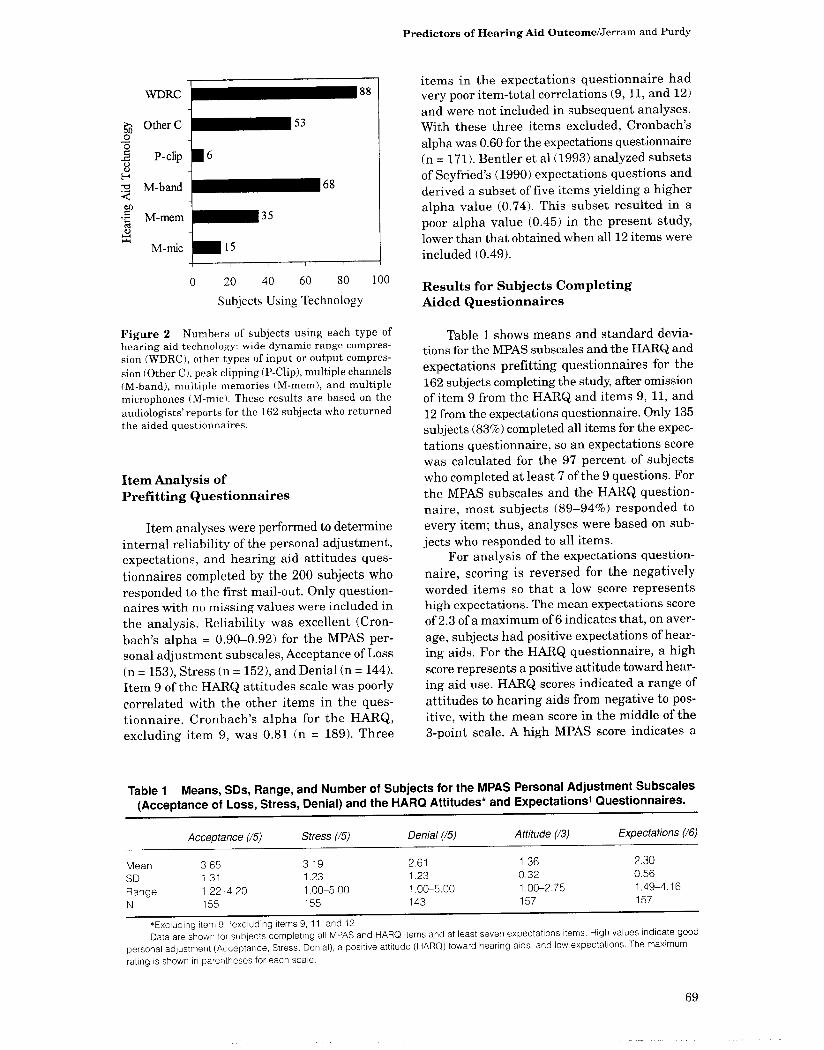
Table 1 shows means and standard devia-tions for the MPAS subscales and the HARQ and expectations prefitting questionnaires for the 162 subjects completing the study, after omission of item 9 from the HARQ and items 9, 11, and 12 from the expectations questionnaire. Only 135 subjects (83%) completed all items for the expec-tations questionnaire, so an expectations score was calculated for the 97 percent of subjects who completed at least 7 of the 9 questions. For
the MPAS subscales and the HARQ question-naire, most subjects (89-94%) responded to every item ; thus, analyses were based on sub-
jects who responded to all items. For analysis of the expectations question-
naire, scoring is reversed for the negatively worded items so that a low score represents high expectations . The mean expectations score of 2.3 of a maximum of 6 indicates that, on aver-
age, subjects had positive expectations of hear-ing aids . For the HARQ questionnaire, a high score represents a positive attitude toward hear-ing aid use. HARQ scores indicated a range of attitudes to hearing aids from negative to pos-itive, with the mean score in the middle of the 3-point scale. A high WAS score indicates a
Table 1 Means, SDs, Range, and Number of Subjects for the WAS Personal Adjustment Subscales
(Acceptance of Loss, Stress, Denial) and the HARQ Attitudes* and Expectationst Questionnaires .
Acceptance (15) Stress (15) Denial (15) Attitude (13) Expectations (16)
Mean 3 .65 3 .19 2.61 1 .36 2 .30 SD 1 .31 1 .23 1 .23 0.32 0.56
Range 1 .22-4.20 1 .00-5.00 1 .00-5.00 1 .00-2.75 1 .49-4.16 N 155 155 143 157 157
*Excluding item 9, 'excluding items 9, 11, and 12, Data are shown for subjects completing all WAS and HARQ items and at least seven expectations items. High values indicate good
personal adjustment (Acceptance, Stress, Denial), a positive attitude (HARQ) toward hearing aids, and low expectations . The maximum
rating is shown in parentheses for each scale.
69

Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
high level of personal adjustment . The WAS mean data showed a moderately high accep-tance of hearing loss and adjustment to stress related to hearing loss and a moderate level of awareness of communication problems .
Only two subjects wore their aids 1 hour or less per day, 48 (26%) wore their aids 1 to 4 hours, and 112 (69%) wore their aids 4+ hours per day. For the 162 subjects completing the study, rat-ings of overall hearing aid satisfaction ranged from 2 to 20 . Only 5 subjects had satisfaction scores below 10 . Mean satisfaction was 15.33 (SD = 3.33) or 77 percent of the entire scale. Thus, on average, people were very satisfied with their hearing aids .
Only 58 percent of subjects completed all of the unaided and aided MAPHAB items. Ninety percent of subjects (n = 146) completed at least 80 percent of the MAPHAB items (i .e ., >_17 of 22). For these subjects, item 16 ("The sounds of con-struction work are uncomfortably loud") had the poorest response rate (78%) of the individ-ual items. Response rates for the other individ-ual MAPHAB items ranged from 92 to 100 percent. Means and standard deviations for MAPHAB benefit scores are shown in Table 2 for subjects who responded to at least 80 percent of the MAPHAB items. On average, benefit scores were slightly higher for the difficult listening than for the easy listening factor and were low-est for the aversiveness of sounds factor.
Relationships between Outcome Measures
The relationship between the satisfaction and benefit outcome measures was investigated by calculating Pearson correlation coefficients for the 146 subjects completing at least 80 percent of the MAPHAB items. Satisfaction was corre-lated with factors 1 (r = .224, p = .007) and 2 (r = .312, p < .001) but not factor 3 (r = .072, p = .387) benefit scores . The strongest relationship between satisfaction and benefit scores was for difficult listening situations (factor 2) . Figure 3
Satis F1 F2 F3
Figure 3 Mean satisfaction rating and MPHAB factors 1, 2, and 3 scores for subjects wearing their hearing aids <4 hours (n = 51) and 4+ hours (n = 111) . Error bars show standard errors .
shows satisfaction ratings and MAPHAB bene-fit as a function of hearing aid use time . On average, subjects who wore their aids more had higher satisfaction ratings and higher factors 1 and 2 MAPHAB benefit scores .
Effects of Predictor Variables on Outcome Measures
Ordinal logistic regression analyses were used to investigate whether demographic, hear-ing aid technology, or subjective factors had an effect on hours of hearing aid use, satisfaction, and benefit. Factors that were investigated included age, gender, employment status, type of clinic (public vs private), prior hearing aid experience, four-frequency pure-tone average (combined and separate ears), monaural ver-sus binaural fitting, hearing aid style (BTE, ITE, ITC, CIC), hearing aid input-output char-acteristic (WDRC, input compression, output limiting compression, peak clipping), "high-performance" hearing aid features (multiple channel, multiple memory, multiple microphone),
Table 2 Means, SDs, and Range for the Satisfaction Ratings (Using a 20-Point Scale) and MAPHAB Factors 1 (Easy Listening), 2 (Difficult Listening), and 3 (Aversive Sounds)
Satisfaction Factor 1 Factor 2 Factor 3
Mean 15.33 24 .4 25.3 -5 .1 SD 3.33 24 .1 18 .5 24.5 Range 2-20 -45.2-81 .8 -21 .1-82 .5 -71 .5-76 .3
Percent hearing benefit is shown for MAPHAB factors 1 to 3. Data are shown for the subjects who completed at least 80% of the MAPHAB unaided and aided items (n = 146) .
70
personal adjustment to hearing loss (MPAS Acceptance of Loss, Stress, and Denial sub-scales), attitudes to hearing aids (HARQ), and expectations of hearing aids . Only subjects with complete information were included in each regression analysis .
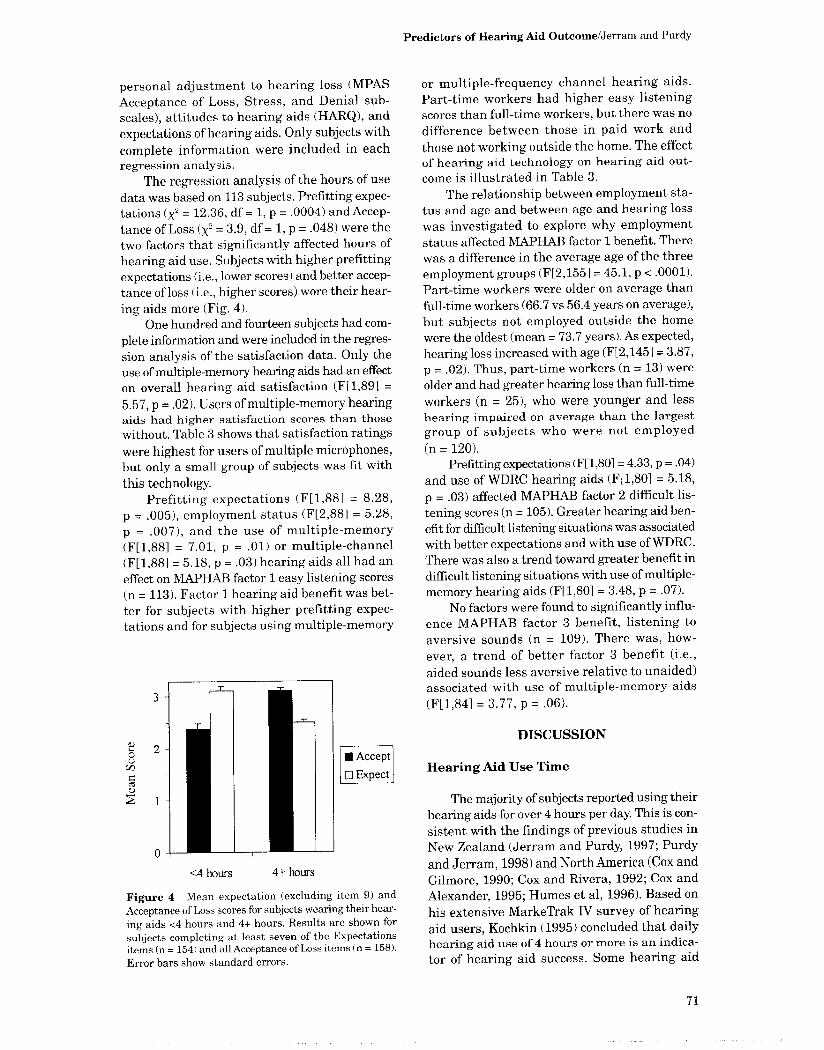
The regression analysis of the hours of use data was based on 113 subjects . Prefitting expec-tations (X2 = 12 .36, df = 1, p = .0004) and Accep-tance of Loss (X2 = 3 .9, df = 1, p = .048) were the two factors that significantly affected hours of hearing aid use. Subjects with higher prefitting expectations (i .e ., lower scores) and better accep-tance of loss (i.e ., higher scores) wore their hear-ing aids more (Fig . 4) .
One hundred and fourteen subjects had com-plete information and were included in the regres-sion analysis of the satisfaction data . Only the use of multiple-memory hearing aids had an effect on overall hearing aid satisfaction (F[1,89] =
5.57, p = .02) . Users of multiple-memory hearing aids had higher satisfaction scores than those without. Table 3 shows that satisfaction ratings
were highest for users of multiple microphones, but only a small group of subjects was fit with this technology.
Prefitting expectations (F[1,88] = 8.28, p = .005), employment status (F[2,88] = 5 .28, p = .007), and the use of multiple-memory (F[1,88] = 7 .01, p = .01) or multiple-channel (F[1,881 = 5.18, p = .03) hearing aids all had an effect on MAPHAB factor 1 easy listening scores (n = 113) . Factor 1 hearing aid benefit was bet-ter for subjects with higher prefitting expec-tations and for subjects using multiple-memory
<4 hours 4+ hours
" Accept O Expect
Figure 4 Mean expectation (excluding item 9) and
Acceptance of Loss scores for subjects wearing their hear-
ing aids <4 hours and 4+ hours. Results are shown for
subjects completing at least seven of the Expectations items (n = 154) and all Acceptance of Loss items (n = 158) .
Error bars show standard errors .
Predictors of Hearing Aid Outcome/Jerram and Purdy
or multiple-frequency channel hearing aids . Part-time workers had higher easy listening scores than full-time workers, but there was no difference between those in paid work and those not working outside the home . The effect of hearing aid technology on hearing aid out-come is illustrated in Table 3 .
The relationship between employment sta-tus and age and between age and hearing loss
was investigated to explore why employment status affected MAPHAB factor 1 benefit. There was a difference in the average age of the three
employment groups (F[2,155] = 45 .1, p < .0001) .
Part-time workers were older on average than
full-time workers (66.7 vs 56.4 years on average), but subjects not employed outside the home were the oldest (mean = 73.7 years) . As expected, hearing loss increased with age (F[2,145] = 3 .87, p = .02) . Thus, part-time workers (n = 13) were
older and had greater hearing loss than full-time
workers (n = 25), who were younger and less hearing impaired on average than the largest group of subjects who were not employed
(n = 120) . Prefitting expectations (F[1,801= 4.33, p = .04)
and use of WDRC hearing aids (F[1,80] = 5.18,
p = .03) affected MAPHAB factor 2 difficult lis-
tening scores (n = 105) . Greater hearing aid ben-
efit for difficult listening situations was associated
with better expectations and with use of WDRC.
There was also a trend toward greater benefit in
difficult listening situations with use of multiple-memory hearing aids (F[1,801 = 3.48, p = .07) .
No factors were found to significantly influ-ence MAPHAB factor 3 benefit, listening to aversive sounds (n = 109) . There was, how-ever, a trend of better factor 3 benefit (i .e ., aided sounds less aversive relative to unaided) associated with use of multiple-memory aids (F[1,84] = 3 .77, p = .06) .
DISCUSSION
Hearing Aid Use Time
The majority of subjects reported using their hearing aids for over 4 hours per day. This is con-
sistent with the findings of previous studies in New Zealand (Jerram and Purdy, 1997 ; Purdy
and Jerram,1998) and North America (Cox and Gilmore, 1990 ; Cox and Rivera, 1992; Cox and Alexander, 1995 ; Humes et al, 1996). Based on
his extensive MarkeTrak IV survey of hearing aid users, Kochkin (1995) concluded that daily hearing aid use of 4 hours or more is an indica-tor of hearing aid success. Some hearing aid
71

Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
Table 3 Means and SDs for Satisfaction and MAPHAB Factors 1, 2, and 3 Benefit for the Different Hearing Aid Technologies Used by Subjects in the Study
Technology n
Satisfaction
Mean (SD)
Factor 1
Mean (SD)
Factor 2
Mean (SD)
Factor 3
Mean (SD)
WDRC 88 15 .2 (3 .6) 24 .4 (21 .4) 26 .3 (18 .4) -5 .8 (25 .2) Other C 53 15 .1 (3 .2) 23 .6 (24 .3) 25.3 (18 .5) -5 .1 (24 .5) PC 6 15 .1 (2 .8) 16 .8 (34 .8) 18 .6 (33 .4) 2 .78 (18 .8) Multiband 68 14 .8 (3 .5) 27 .6 (20 .5) 25 .5 (17 .3) -3.6 (26 .0) Multiple memory 35 15 .9 (2 .9) 19 .7 (25 .5) 24 .5 (17 .2) -2.7 (23 .5) Multiple microphone 15 16 .3 (3 .7) 28 .1 (20 .6) 20 .1 (12 .3) -12.3 (17 .9)
To enable comparison with Table 2, data presented are for subjects who completed at least 80% of the MAPHAB (n = 146) . Other C = other compression circuits (input or output).
users with very specific and limited hearing aid listening needs may be successful users, how-ever, despite using their aids very little . Self-reporting of hearing aid use can be misleading (Humes et al, 1996 ; Taubman et al, 1999), since subjects tend to exaggerate actual hearing aid use time . Despite this limitation, self-report of hear-ing aid use appears to be a valuable and widely recognized dimension of hearing aid outcome (Humes, 1999).
Hearing Aid Benefit
Hearing aid benefit was measured using the MAPHAB (Purdy and Jerram, 1998). As seen previously, benefit was slightly greater for difficult than for easy listening situations (e .g ., Cox and Alexander, 1995 ; Valente et al, 1995, 1998). Studies investigating older versus newer hearing aid technologies typically report mean APHAB benefit values in the range of 20 to 35 percent for the three APHAB listening subscales (e.g., Valente et al, 1995, 1998; Preves et al, 1999), although, occasionally, benefit over 40 percent is obtained . Mean benefit scores for the easy and difficult listening factors in the present study fall within the range of values previously reported, despite the use of a different scale.
Many subjects were unable to complete the MAPHAB. We have noted previously that older clients in particular may have difficulty with some of the APHAB questions (Purdy and Jerram, 1998). The reversal of a number of the items to prevent bias is one source of confusion (Noble, 1998), and our use of a more detailed 100-point scale also may have made the questionnaire too complex for some clients. A recent study showed that, based on respondent preference and test--retest reliability, a 10-point scale is optimal (Preston and Colman, 2000).
As seen in other studies (Cox and Alexan-der, 1995 ; Valente et al, 1995, 1998 ; Preves et al, 1999), hearing aids were not beneficial for lis-tening to aversive environmental sounds . The amount of "negative benefit" was considerably less, however, than values reported previously, presumably reflecting the greater loudness com-fort provided by the WDRC technology that the majority of subjects were using. WDRC has gained popularity because it provides better speech intelligibility in quiet compared with linear amplification (Humes et al, 1999; Walden et al, 1999) and greater listening comfort across a wide range of situations (Jenstad et al, 1999). Superior performance has not been found con-sistently in noisy environments, however (Kam and Wong, 1999 ; Souza and Turner, 1999).
Previous studies have shown that the APHAB can distinguish between different types of high-performance hearing aids (Valente et al, 1995, 1998 ; Arlinger et al, 1998; Berninger and Karlsson, 1999 ; Preves et al, 1999). Con-sistent with Kochkin's (1996, 2000) reports of the listening advantages provided by higher-performance hearing aids, benefit was signifi-cantly greater in easy listening situations for multiple-memory and multiple-channel hear-ing aids . This is not surprising, since these tech-nologies allow greater fitting and user flexibility. Benefit in difficult listening situations was greater for WDRC hearing aids . Although some studies have failed to find speech reception ben-efits of WDRC in noise (Kam and Wong, 1999 ; Souza and Turner, 1999), other studies have seen WDRC advantages in noise compared with linear technology (e.g., Humes et al, 1999). In the present study, it is possible that clients using WDRC hearing aids experienced greater hear-ing aid benefit in difficult listening situations because of the way their audiologists selected the
72

Predictors of Hearing Aid Outcome/Jerram and Purdy
technology. Clients using WDRC had milder
hearing losses (by 5 dB on average) than clients
fitted with non-WDRC aids ; thus, they may
have experienced greater benefit in noise due to
having less cochlear pathology. The advantages
of multiple-microphone hearing aids in noise
are well documented and have been demon-strated using the APHAB (e.g ., Valente et al,
1995 ; Preves et al, 1999) . Therefore, it was sur-prising that multiple-microphone technology
was not a predictor of MAPHAB factor 2 bene-
fit . This could be due to the small number of sub-
jects fitted with multiple-microphone hearing
aids . It is also possible that audiologists only pre-
scribed this technology for clients with more
severe speech in noise problems .
Satisfaction
In general, the subjects were very satisfied with their hearing aids . The mean rating of
76 percent was slightly higher than the value of
71 percent found by Purdy and Jerram (1998) using the same scale. Subjects in the present
study had new hearing aids, and there was a rel-atively high proportion of high-performance hearing aids fitted . Kochkin (1995, 1996) found that satisfaction is greater for newer hearing aids and newer technologies . Mean scores reported
by Cox and Alexander (1999) for the Satisfaction with Amplification in Daily Living (SADL) ranged from 43 to 91 percent for the individual items in their satisfaction profile. Although derived in quite different ways, the 70 percent global satisfaction value obtained by Cox and Alexander for the SADL questionnaire and Kochkin's (1996) reported satisfaction values of
71 to 75 percent for new and high-performance
hearing aids are consistent with the satisfaction results obtained in the present study.
There were statistically significant positive correlations between satisfaction and the two MAPHAB listening factors. Similar to Purdy and Jerram (1998), the strongest correlation between hearing aid benefit and satisfaction was for difficult listening situations, and satis-faction was higher in subjects who wore their
aids more often. This is consistent with Kochkin's (1993, 1996) finding that satisfaction is highly
related to the number of listening situations in which the wearer's needs are met. Kochkin
(1999, 2000) has used the term "multiple envi-
ronmental listening utility" (MELD) to refer to
the ability of hearing aids to provide good lis-
tening satisfaction in a range of environments, including noise. Consistent with Kochkin's
MELU concept, users of multiple-memory hear-
ing aids were significantly more satisfied with their hearing aids .
Hyde and Riko (1994) criticized global mea-
sures of overall satisfaction on the basis that they
confound features of hearing aid performance,
convenience, aid physical characteristics, and stigma . This could explain why only one of the
factors investigated (multiple memories) was predictive of satisfaction . Future research in
this area may be more successful if a more spe-
cific, differentiated satisfaction scale such as
the SADL (Cox and Alexander, 1999) is used .
Demographic Factors
Part-time workers had higher easy listening
hearing aid benefit scores than full-time workers .
This is probably explained by the greater degree of hearing loss seen in older subjects, who made
up the majority of part-time workers . Previous
hearing aid experience (Pawing and Philip, 1991),
age (Mulrow et al, 1992 ; Crowley and Nabelek, 1996 ; Jerram and Purdy, 1997), and degree of
hearing loss (Brooks, 1985 ; Kochkin, 1995) have
been found previously to affect hearing aid out-
come but were not significant factors in the pre-
sent study. Differences in subject groups across
studies could account for these differences .
Attitudes
With the exception of one item, internal
reliability of the HARQ hearing aid stigma fac-
tor was very good, as was found by Hallam and
Brooks (1996) . Hallam and Brooks (1996) also
obtained a relatively low item loading for item
9, which was excluded from the present analy-
sis . In contrast to previous studies (Hickson et
al, 1986, 1999 ; Brooks, 1989; Brooks and Hal-
lam, 1998), attitudes toward hearing aids were
not predictive of hearing aid outcome. Brooks
(1989) investigated attitude with a single ques-
tion that was similar in content to item 9 of the
HARQ, and found that subjects with a more
positive attitude wore their hearing aids more
when they were evaluated 4 months after the
fitting . Brooks and Hallam (1998) assessed atti-
tudes to hearing loss and hearing aids using
the 40-item HARQ, which has seven subscales, including the Hearing Aid Stigma subscale used
in the present study. In agreement with the pre-
sent study, an attitude that wearing a hearing
aid is stigmatizing was not predictive of hear-ing aid outcome. Attitudes to hearing loss and
73

Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
hearing aids measured by other subscales (feel-ings of personal distress/inadequacy due to hear-ing loss, minimization of hearing impairment, and not wanting/needing hearing aids) were predictive of outcome. Two of these factors (dis-tress/inadequacy and minimization) are similar in content to the CPHI personal adjustment subscales. Stigma associated with hearing loss and hearing aids is a barrier to hearing aid use (Kochkin, 1993 ; Hetu, 1996 ; Arnold and MacKen-zie, 1998). Hetu (1996) has shown that adults who develop a hearing loss are reluctant to acknowledge hearing difficulties because of fear of stigmatization and embarrassment. The find-ing of no relationship between the perception of hearing aids as stigmatizing and hearing aid out-come suggests that, in general, individuals who accept hearing aids have generally overcome this fear. The range of responses to the HARQ (see Table 1) indicates that some individual sub-jects did have very poor attitudes toward hear-ing aids ; thus, for some subjects, concerns about stigma may have still been a problem.
Expectations
The poor internal reliability of the 12 items of Seyfried's (1990) expectations questionnaire also was seen by Bentler et al (1993) . We were not able to replicate the good reliability reported by Bentler et al for a subset of five expectations items and instead obtained moderately good reliability for a different subset of nine items.
Higher prefitting expectations were associ-ated with higher daily hearing aid use time . Expectations also influenced hearing aid bene-fit in easy and difficult listening situations . On average, subjects had positive expectations (mean = 2.3 ± 0.6) . The mean expectations score plus 1 SD falls in the middle of the 6-point scale. An expectations score greater than 3, indicating low expectations, could be used as an indicator for a potentially poorer outcome . Further research is needed to determine whether addi-tional prefitting counselling (e.g., Brooks, 1979, 1985 ; Brooks and Johnson, 1981) would improve hearing aid outcomes for these individuals with low expectations .
Higher expectations scores predicted greater hearing aid benefit in noisy and in quiet listen-ing situations . In contrast, Schum (1999) found a modest negative correlation between prefitting expectations measured using the Hearing Aid Needs Assessment questionnaire and speech in noise scores on the Hearing Aid Performance Inventory (HAPI, Walden et al, 1984). Thus, in
contrast to the present study, higher expectations of listening performance were associated with poorer listening outcome. Seyfried (1990) found no relationship between expectations (measured using Bentler et al's [ 1993] subset of items) and hearing aid benefit measured using the Under-standing Speech subsection of the Hearing Per-formance Inventory (HPI, Giolas et al, 1979). The HAPI and HPI directly assess aided perfor-mance and thus differ from the subtractive ben-efit measure obtained using the MAPHAB in the present study. Another difference between stud-ies is that Schum only examined expectations of aided listening ability, whereas Seyfried's expec-tations questionnaire assesses a range of expec-tations including the ability to handle hearing aids and physical comfort.
Personal Adjustment
As has been found previously (Demorest and Erdman, 1987, 1989; Jerram and Purdy, 1999), the CPHI Acceptance of Loss, Stress, and Denial subscales had excellent internal relia-bility. Acceptance of Loss subscale scores were related to hours of use. Crowley and Nabelek (1996) also found a predictive relationship between CPHI Personal Adjustment scores (13 subscales including Acceptance of Loss) and hearing aid performance. Although hearing aid performance and hours of use are not the same, they are related (Purdy and Jerram, 1998). The original CPHI is a very long questionnaire that examines many aspects of hearing loss (Demor-est and Erdman, 1986). Using the whole scale, Cox and Rivera (1992) found no relationship between CPHI and PHAB results. This is con-sistent with our findings of no relationship between MAPHAB benefit and CPHI Accep-tance of Loss, Stress, or Denial scores .
A high CPHI score indicates good personal adjustment to hearing loss . Thus, the mean score of 3.7 - 1.3 for the Acceptance of Loss scale indicates that the subjects in this study were generally "well adjusted" to their hearing loss. This is probably not surprising for subjects who were willing to participate in hearing aid research requiring a reasonable time commit-ment, some of whom had worn hearing aids pre-viously. Similar Acceptance of Loss scores have been reported in other studies (Demorest and Erdman, 1989; Cox and Rivera, 1992; Garsteki and Erler, 1998; Erdman and Demorest, 1998 ; Jerram and Purdy, 1999). Forty-four percent of subjects had low Acceptance of Loss scores of 2 or less . Pre- and/or postfitting counselling
74

Predictors of Hearing Aid Outcome/Jerram and Purdy
might improve hearing aid outcomes for these
individuals (Brooks, 1989) .
SUMMARY AND CONCLUSIONS
T his study evaluated the effects of a num-ber of predictor variables on three mea- sures of hearing aid outcome, hours of use, subjective benefit, and overall satisfaction .
Subjects completed three questionnaires prior to hearing aid fitting that examined personal adjustment to hearing loss, attitudes to hear-ing aids, and expectations of hearing aids . These questionnaires had good internal relia-
bility after exclusion of some items from the attitudes and expectation scales . On average, subjects had a moderate level of personal adjustment and positive attitudes and expec-tations, but there was considerable variability
across individuals . Subjects were generally satisfied with their hearing aids and had good subjective benefit . The majority of subjects reported using their aids more than 4 hours per day. Subjects who used their aids more had higher benefit and satisfaction ratings . Satis-
faction was related to benefit, particularly for difficult listening situations .
Demographic factors did not affect hearing aid outcome. Multiple-memory hearing aids increased satisfaction and benefit. Multiple-channel and WDRC instruments were associated with greater hearing aid benefit, but the WDRC effect may have resulted from audiologists using WDRC in subjects with lesser degrees of hear-ing loss . On average, satisfaction was highest for multiple-microphone aids, but this effect was not significant, presumably due to the small num-ber of subjects fitted with this technology. The results support the use of newer hearing aid technologies in order to maximize hearing aid outcomes .
Subjects with better prefitting expectations of hearing aids and better personal adjustment to hearing loss measured using the CPHI Accep-tance of Loss subscale used their hearing aids more . Expectations also positively influenced benefit in easy and difficult listening situations . The predictive influence of prefitting expecta-
tions and acceptance of hearing loss on hearing aid use and benefit suggests that these factors should be regularly assessed prior to hearing aid fitting. Prefitting and follow-up counselling may be beneficial in cases where expectations of hearing aids and acceptance of hearing loss are poor.
Acknowledgments. The authors would like to acknowl-edge the support for this study provided by New Zealand public hospital and private audiology clinic staff and clients. Funding for this research was provided by the Deafness Research Foundation of New Zealand. We also thank Elizabeth Robinson from the University of Auckland's Biostatistical Unit for her support and sta-tistical analysis of the data .
REFERENCES
Arlinger S, Billermark E . (1999) . One year follow-up of users of a digital hearing aid. Br J Audiol 33:223-232 .
Arlinger S, Billermark E, Oberg M, Lunner T, Hellgren J. (1998) . Clinical trial of a digital hearing aid. Scand Audiol 27:51-61 .
Arnold P, MacKenzie I. (1998) . Rejection of hearing aids : a critical review. J Audiol Med 7:173-199.
Badley EM, Lee J. (1987a). Impairment, disability, and the ICIDH (International Classification of Impairments, Disabilities, and Handicaps) model. I : the relationship between impairment and disability. Int Rehabil Med 8:113-117 .
Badley EM, Lee J. (1987b). Impairment, disability, and the ICIDH model. III: underlying disease, impairment, and disability. Int Rehabil Med 8:174-181 .
Badley EM, Lee J, Wood PH . (1987) . Impairment, dis-ability, and the ICIDH (International Classification of Impairments, Disabilities, and Handicaps) model. II : the nature of the underlying condition and patterns of impair-ment . Int Rehabil Med 8:118-124 .
Bentler RA, Niebuhr DP, Getta JP, Anderson CV. (1993) . Longitudinal study of hearing aid effectiveness II . Sub-jective measures . J Speech Hear Res 36:820-831 .
Berninger E, Karlsson KK . (1999) . Clinical study of Widex Senso on first-time hearing aid users. Scand Audiol 28:117-125 .
Berninger E, Nordstrom I. (1997). Multiple memory hear-ing aid-consistency of program-usage in real-world listening situations . Scand Audiol 26:252-256 .
Bridges JA, Bentler RA . (1998) . Relating hearing aid use to well-being amongst older adults. Hear J 51 :39-44 .
Brooks DN . (1979) . Hearing aid use and the effects of counselling . Aust J Audiol 1:1-6 .
Brooks DN . (1984) . Binaural benefit-when and how much? Scand Audiol 13:237-241 .
Brooks DN . (1985) . Factors relating to the under-use of postaural hearing aids . Br J Audiol 19:211-217.
Brooks DN. (1989) . The effect of attitude on benefit obtained from hearing aids . Br JAudiol 23:3-11.
Brooks DN . (1990) . Measures for the assessment of hear-ing aid provision and rehabilitation . Br J Audiol 24:229-233 .
Brooks DN . (1994) . Some factors influencing choice of type of hearing aid in the UK : behind-the-ear or in-the-ear. Br JAudiol 28:91-98 .
75
Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
Brooks DN, Hallam RS . (1998) . Attitudes to hearing dif-ficulty and hearing aids and the outcome of audiological rehabilitation . Br J Audiol 32:217-226 .
Dillon H. (1996) . Compression? Yes, but for low or high frequencies, for low or high intensities, and with what response times? Ear Hear 17:287-307 .
Brooks DN, Johnson DI . (1981) . Pre-issue assessment and counselling as a component of hearing aid provision . Br JAudiol 15:13-19 .
Brown MA, MunfordA. (1984) . Rehabilitation of post-MI depression and psychological invalidism : a pilot study. Int J Psychiatr Med 13:291-298 .
Burke W Wesolowski M, Zencius A . (1988) . Long term programs in head injury rehabilitation . Cogn Rehabil 6:38-41 .
Byrne D . (1996) . Hearing aid selection for the 1990's-where to? J Am Acad Audiol 7:77-97 .
Cohn ES. (1999). Hearing loss with aging : presbycusis . Clin Geriatr Med 15:145-161 .
Corso JF. (1987) . Sensory-perceptual processes and ageing. Ann Rev Gerontol Geriatr 7:29-55 .
Cox RM, Alexander GC . (1995) . The Abbreviated Profile of Hearing Aid Benefit . Ear Hear 16:176-186 .
Cox RM, Alexander GC . (1999) . Hearing satisfaction in daily life : the SADL scale . Ear Hear 20:306-320 .
Cox RM, Alexander GC, Gray G. (1999) . Personality and the subjective assessment of hearing aids . J Am Acad Audiol 10:1-13.
Cox RM, Gilmore C . (1990) . Development of the Profile of HearingAid Performance (PHAP) . J Speech Hear Res 33:343-357 .
Cox RM, Gilmore C, Alexander GC . (1991) . Comparison of two questionnaires for patient-assessed hearing aid benefit . J Am Acad Audiol 2:134-145 .
Cox RM, Rivera IM. (1992) . Predictability and reliabil-ity of hearing aid benefit measured using the PHAB . J Am Acad Audiol 3:242-254 .
Crandell C . (1998) . Hearing aids : their effect on func-tional health status . Hear J 5:22-30 .
Cronbach LJ . (1951) . Coefficient alpha and the internal structure of tests . Psychometrika 16:297-334.
Crowley HJ, Nabelek IV (1996) . Estimation of client-assessed hearing aid performance based upon unaided variables. J Speech Hear Res 39:19-27 .
Day GA, Browning GG, Gatehouse S. (1988) . Benefit from binaural hearing aids in individuals with a severe hear-ing impairment. Br J Audiol 22:273-277 .
Demorest ME, Erdman SA . (1986) . Scale composition and item analysis of the Communication Profile for the Hearing Impaired . J Speech Hear Res 29:515-535 .
Demorest ME, Erdman SA . (1987). Development of the Communication Profile for the Hearing Impaired . J Speech Hear Disord 52 :129-143 .
Demorest ME, Erdman DA. (1989). Factor structure of the Communication Profile for the Hearing Impaired . J Speech Hear Disord 54:541-549 .
Dillon H, Birtles G, Lovegrove R . (1999) . Measuring the outcomes of a national rehabilitation program : norma-tive data for the Client Oriented Scale of Improvement (COSI) and the Hearing Aid User's Questionnaire (HAUQ) . J Am Acad Audiol 10:67-79 .
Erdman SA, Demorest ME . (1998) . Adjustment to hear-ing impairment II : audiological and demographic correlates . J Speech Lang Hear Res 41:123-136 .
Evenhuis HM. (1995) . Medical aspects of ageing in a population with intellectual disability: II . Hearing impair-ment . J Intellect Disabil Res 39:27-33 .
Garstecki DC, Erler SF. (1998) . Hearing loss, control, and demographic factors influencing hearing aid use among older adults . J Speech Lang Hear Res 41:527-537 .
Gatehouse S. (1990) . Factors that influence the benefit from amplification in the elderly. Acta Otolaryngol Suppl (Stockh) 47:262-268 .
Gatehouse S. (1994) . Components and determinants of hearing aid benefit. Ear Hear 15 :30-49 .
Giolas TG, Owens E, Lamb SH, Schubert ED . (1979) . Hearing Performance Inventory. J Speech Hear Res 44:169-195 .
Hallam RS, Brooks DN. (1996) . Development of the Hearing Attitudes in Rehabilitation Questionnaire. Br JAudiol 30:199-213 .
Hetu R. (1996) . The stigma attached to hearing impair-ment . Scand Audiol 25(Supp143):12-24 .
Hickson L, Hamilton L, Orange SP. (1986) . Factors asso-ciated with hearing aid use. Aust JAudiol 8:37-41 .
Hickson L, Timm M, Worral L. (1999) . Hearing aid fit-ting : outcomes for older adults . Aust JAudiol 21:19-23 .
Humes LE . (1999) . Dimensions of hearing aid outcome . JAm Acad Audiol 10:26-39 .
Humes LE, Halling D, Coughlin M. (1996) . Reliability and stability of various hearing aid outcome measures in a group of elderly hearing aid wearers. J Speech Hear Res 39:923-935 .
Humes LE, Christenson L, Thomas T, Bess FH, Hedley-Willams A, Bentler R . (1999). A comparison of the aided performance and benefit provided by a linear and a two channel hearing aid . J Speech Hear Res 42:65-79 .
Hyde ML, Riko K. (1994) . A decision-analytic approach to audiological rehabilitation . J Acad Rehabil Audiol Monogr 27:337-374 .
Jenstad LM, Seewald RC, Cornelisse LE, Shantz J. (1999) . Comparison of linear gain and wide dynamic range com-pression hearing aid circuits : aided speech perception measures . Ear Hear 20:117-126.
Jerram JCK, Purdy SC . (1997) . Evaluation of hearing aid benefit using the Shortened Hearing Aid Performance Inventory. J Am Acad Audiol 8:18-26 .
Jerram JCK, Purdy SC . (1999) . Measuring personal adjustment to hearing loss using a shortened version of
76
Predictors of Hearing Aid Outcome/Jerram and Purdy
the Communication Profile for the Hearing Impaired . Aust JAudiol 21:1-8 .
Kam CS, Wong LN . (1999) . Comparison of performance with wide dynamic range compression and linear ampli-fication . J Am Acad Audiol 10:445-457 .
Levitt H, Resnick SB . (1978). Speech reception by the hearing impaired: methods of testing and development of materials. Scand Audiol Suppl 6:107-129 .
May J. (1986) . Personal adjustment to hearing loss . Hear Rehabil Q 11:12-13 .
Kapteyn TS, Wijkel D, Hackenitz E. (1997) . The effects of involvement of the general practitioner and guidance of the hearing-impaired on hearing-aid use. Br JAudiol 31:399-407 .
Kates JM, Weiss MR . (1996) . A comparison of hearing aid array processing techniques . J Acoust Soc Am 99:138-148 .
Keidser G. (1995) . The relationship between listening conditions and alternative amplification schemes for mul-tiple memory hearing aids . Ear Hear 16:575-586 .
Keller SD, Ware JE Jr, Gandek B, Aaronson NK, Alonso J, Apolone G, Bjorner JB, Brazier J, Bullinger M, Fukuhara S, Kaasa S, Leplege A, Sanson-Fisher RW, Sullivan M, Wood-Dauphinee S. (1998) . Testing the equiv-alence of translations of widely used response choice labels : results from the IQOLA Project. International Quality of Life Assessment . J Clin Epidemiol 51:933-944.
Kiessling J. (1996) . Hearing instruments: a look into the future . Folia Phoniatr Logop 48:156-162 .
Kochkin S. (1993) . MarkeTrak III identifies key factors in determining customer satisfaction . Hear J 46:39-44 .
Kochkin S. (1995) . MarkeT!rak IV Norms: Subjective Measures of Satisfaction and Benefit. Presented at the American Academy of Audiology Annual Convention, Dallas, TX.
Kochkin S. (1996) . Customer satisfaction and subjective benefit with high performance hearing aids . Hear Rev 3:16-26 .
Kochkin S. (1999) . From Customer Satisfaction to Customer Bliss. Presented at Phonak Small Business Seminar, Fiji .
Kochkin S. (2000) . MarkeTrak V: "Why my hearing aids are in the drawer": the consumers' perspective . Hear J 53 :34-42 .
Kochkin S, Rogin CM . (2000) . Quantifying the obvious: the impact of hearing instruments on quality of life . Hear Rev 7:6-34.
Kricos PB, Lesner SA, Sandridge SA, Yanke RB . (1987) . Perceived benefits of amplification as a function of cen-tral auditory status in the elderly. Ear Hear 8:337-342 .
Kricos PB, Lesner SA, Sandridge SA. (1991) . Expectations of older adults regarding the use of hearing aids . J Am Acad Audiol 2 :129-133 .
Kuk FK, Pape NM. (1993) . Relative satisfaction for fre-quency responses selected with a Simplex procedure in different listening conditions . J Speech Hear Res 36:168-177 .
Leeuw AR, Dreschler WA . (1991) . Advantages of direc-tional hearing aid microphones related to room acoustics. Audiology 30:330-344 .
McCarthy PA, Montgomery AA, Mueller HG . (1990) . Decision making in rehabilitative audiology. J Am Acad Audiol 1:23-30 .
McKenzie AR, Rice CG. (1990) . Binaural hearing aids for high-frequency hearing loss . Br J Audiol 24:329-334 .
Meredith R, Stephens D. (1993) . In-the-ear or behind-the-ear hearing aids in the elderly. Scand Audiol 22 : 211-216 .
Mueller HG . (1992) . Insertion gain measurements . In : Mueller HG, Hawkins DB, Northern JL, eds. Probe Microphone Measurements Hearing Aid Selection and Assessment. San Diego: Singular, 113-143.
Mulrow CD, Aguilar C, Endicott JE, Tuley MR, Velez R, Charlip WS, Rhodes MC, Hill JA, DeNino LA . (1990) . Quality-of-life changes and hearing impairment . A ran-domized trial. Ann Intern Med 113 :188-194 .
Mulrow CD, Tuley MR, Aguilar C. (1992) . Correlates of successful hearing aid use in older adults . Ear Hear 13 : 108-113.
Noble W. (1998). Self-Assessment ofHearingand Related Functions. London: Whurr.
Parving A, Philip B. (1991) . Use and benefit of hearing aids in the tenth decade and beyond. Audiology 30:61-69 .
Preston CC, Colman AM. (2000) . Optimal number of response categories in rating scales : reliability, validity, discriminating power, and respondent preferences. Acta Psychol104 :1-15.
Preves DA, Sammeth CA, Wynne MK. (1999) . Field trial evaluations of a switched directional/omindirectional in-the-ear microphone . JAm Acad Audiol 10:273-284 .
Purdy SC, Jerram JCK. (1998) . Investigation of the Profile of Hearing Aid Benefit in experienced hearing aid users. Ear Hear 19:473-480 .
Rose DE, Pool AF . (1994) . In search of effective means to reduce hearing aid returns. Hear J 47:29-31 .
Satherley NA. (1992). A Survey of HearingAid Users and the Establishment and Evaluation of a Hearing Aid Rehabilitation Program in the Christchurch Region . Unpublished master's thesis, University of Canterbury, Christchurch, New Zealand.
Schum DJ . (1992) . Responses of elderly hearing aid users on the Hearing Aid Performance Inventory. J Am Acad Audiol 3:308-314.
Schum DJ. (1999) . Perceived hearing aid benefit in rela-tion to perceived needs . J Am Acad Audiol 10:40-45 .
Scott B, Lindberg P, Melin L, Lyttkens L. (1994) . Control and dispositional style among the hearing-impaired in communication situations . Audiology 33:177-184 .
Seyfried DA . (1990) . Use of a Communication Self-Report Inventory to Measure Hearing Aid Counselling Effects.
77
Journal of the American Academy of Audiology/Volume 12, Number 2, February 2001
Unpublished doctoral thesis, University of Iowa, Iowa City, IA .
Souza PE, Turner CW (1999) . Quantifying the contri-bution of audibility to recognition of compression-amplified speech . Ear Hear 20:12-20.
Stach BA, Loiselle LH, Jerger JF. (1991) . Special hear-ing aid considerations in elderly patients with auditory processing disorders. Ear Hear 12(Suppl):131S-138S .
Stephens D . (1996) . Hearing rehabilitation in a psy-chosocial framework . Scand Audiol 43(Suppl):57-66 .
Stephens SD, Meredith R . (1991) . Quantitative reports of hearing benefit . Clin Rehabil 5:225-229 .
Taubman LB, Palmer CV, Durrant JD, Pratt S. (1999) . Accuracy of hearing aid use time as reported by experi-enced hearing aid users. Ear Hear 20:299-305 .
Upfold LJ, May AE . (1990) . Hearing aid manipulation skills in an elderly population : a comparison of ITE, BTE and ITC aids. Br JAudiol 24:311-318 .
Valente M. (1999) . Use of microphone technology to improve user performance in noise. Trends Amplif 4:112-135 .
Valente M, Fabry DA, Potts LG. (1995). Recognition of speech in noise with hearing aids using dual microphones. J Am Acad Audiol 6:440-449 .
Valente M, Fabry DA, Potts LG, Sandlin RE . (1998) . Comparing the performance of the Widex SENSO digi-tal hearing aid with analog hearing aids . J Am Acad Audiol 9:342-360 .
Ventry I, Weinstein B . (1982) . The Hearing Handicap Inventory for the Elderly : a new tool . Ear Hear 3:128-134 .
Verschuure MA, Stikyvoort E, de Jong RM, Goedegebure A, Dreschler WA. (1996). Compression and its effect on the speech signal . Ear Hear 17:162-175 .
Walden BE, Demorest M, Hepler E . (1984) . Self-report approach to assessing benefit derived from amplification. J Speech Hear Res 27:49-56 .
Walden BE, Surr RK, Cord MT. (1999) . A clinical trial of the Resound IC4 hearing device . J Am Acad Audiol 8:65-78 .
Weinstein BE . (1990). The quantification of hearing aid benefit in the elderly: the role of self-assessment mea-sures. Acta Otolaryngol Suppl (Stockh) 476:257-261 .
Welzl-Miiller K, Stephan K. (1986). The benefit of hear-ing aids : influence of hearing loss and age. Scand Audiol 15:115-119 .
Wetzell C, Harford ER. (1983) . Predictability of real ear hearing aid performance from coupler measurements. Ear Hear 4:237-242 .
APPENDIX
Seyfried (1990) Expectations Checklist
10. 11 . 12 .
I will have difficulty operating the controls on my hearing aid(s) . My hearing aids will fit comfortably. My hearing aids will make speech more distinct . My family believes my hearing aids will help me communicate better. I will have difficulty inserting and removing my hearing aid(s) . I will adjust slowly to my hearing aids . In some noisy situations, my hearing aids will be helpful. I will need my hearing aids in most listening situations in which I find myself. When I am using my hearing aid(s), I will need to watch speakers' faces and ask them for repeti-tions occasionally. When I am speaking to others in a quiet room, my hearing aid(s) will be helpful. When I am using my hearing aid(s), some sounds will be uncomfortably loud . I will feel self-conscious when I am wearing my hearing aids .
Hearing Attitudes in Rehabilitation Questionnaire (HARQ)
1. 1 think that if you wear a hearing aid people tend to ignore you. 2. I would stand out in a crowd wearing a hearing aid. 3. Many people don't know how to react to you when you have a hearing aid. 4. It would make me feel old to wear a hearing aid. 5. If I wear a hearing aid, people will probably think I'm a bit stupid . 6. It would embarrass me to have to wear a hearing aid. 7. I think people react differently to you when you are wearing a hearing aid.
78

Predictors of Hearing Aid Outcome/Jerram and Purdy
8 . From what I know, hearing aids don't help a great deal . 9 . I think the behind-the-ear aids are really quite small and inconspicuous .
Communication Profile for the Hearing Impaired (CPHI) Subscales
(Items 1-9 = Acceptance of Loss, 10-17 = Stress, 18-25 = Denial) 1 . 1 try to give the impression of normal hearing. 2. I try to hide my hearing problem. 3. Sometimes I'm ashamed of my hearing problems . 4. I'm sensitive about my hearing loss . 5. I find it difficult to admit to others that I have a hearing problem. 6. It bothers me to admit that I have a hearing loss . 7. I can't talk to people about my hearing loss . 8. I have a hard time accepting the fact that I have a hearing loss . 9 . I'd rather miss part of a conversation than admit that I have a hearing loss .
10 . I feel threatened by many communication situations due to difficulty hearing . 11 . I'm not very relaxed when conversing with others . 12 . I'm not very comfortable in most communication situations . 13 . I get very tense because of my hearing loss . 14 . When I have trouble hearing, I become nervous. 15 . I worry about looking stupid when I can't understand what someone has said . 16 . Straining to hear upsets me . 17 . When I can't understand what's being said, I feel tense and anxious. 18 . Sometimes I feel left out when I can't follow the conversation of those I'm with . 19 . I sometimes get annoyed when I have trouble hearing. 20 . When I have trouble hearing, I feel frustrated . 21 . It's frustrating when people refuse to repeat what they've said . 22 . Sometimes when I misunderstand what someone has said, I feel foolish. 23 . I sometimes get angry with myself when I can't hear what people are saying. 24 . Sometimes I feel tense when I can't understand what someone is saying. 25 . 1 sometimes feel embarrassed when I misunderstand what someone has said .


















