Targeted prophylaxis with amphotericin B lipid complex in liver transplantation
8
Targeted Prophylaxis With Amphotericin B Lipid Complex in Liver Transplantation Saket Singhal, * Richard W. Ellis, Stephen G. Jones, Sarah J. Miller, ‡ Neil C. Fisher, * J.G. Mark Hastings, and David J. Mutimer * The purpose of this study is to prospectively evaluate a strategy in which prophylaxis with amphotericin B lipid complex at 3 different dosages was targeted to liver trans- plant recipients at high risk for the development of inva- sive fungal infection (IFI). High risk was defined as a postoperative requirement for prolonged (>5 days) inten- sive care unit (ICU) treatment. Consecutive high-risk pa- tients were administered prophylaxis with amphotericin B lipid complex from day 5 after orthotopic liver transplan- tation (OLT) until ICU discharge or death. The first 10 eligible patients were administered 5 mg/kg/d, the next 10 patients were administered 2.5 mg/kg/d, and a final 10 patients were administered 1 mg/kg/d. Drug safety and efficacy were assessed before each dosage reduction. Dur- ing the study period, 130 adult patients underwent 137 OLTs. Thirty patients fulfilled the entry criteria and were administered prophylaxis with amphotericin B lipid com- plex. No patient developed proven IFI during prophy- laxis. Cultures from normally sterile sites (blood and ab- dominal drain fluid) always showed negative results. All fungal isolates were sensitive in vitro to amphotericin B. There was no significant difference in colonization scores among the groups of patients administered different dos- ages of amphotericin B lipid complex. No death, serious adverse reaction, or nephrotoxicity was attributed to am- photericin B lipid complex. We conclude that prophylaxis with amphotericin B lipid complex targeted to patients requiring prolonged ICU treatment after OLT appears to be well tolerated and may prevent IFI. Our current policy is to use amphotericin B lipid complex, 1 mg/kg/d, as antifungal prophylaxis in this high-risk group. (Liver Transpl 2000;6:588-595.) I nvasive fungal infection (IFI) has a high mortality after orthotopic liver transplantation (OLT). In early studies, the incidence of IFI in this setting ranged from 18% to 42%, and the associated mortality rates were 50% to 78%. 1-6 Candida species accounted for the majority of infections, and many patients infected with Candida organisms survived. In contrast, infections caused by Aspergillus species were nearly always fa- tal. 2,3,6 We showed that in liver transplant recipients considered high risk for IFI, fluconazole prophylaxis reduced the incidence of invasive candidiasis 7 but was complicated by the emergence of fluconazole-resistant fungi and failed to prevent invasive aspergillosis. 8 A recent randomized, placebo-controlled trial of liver transplant recipients showed that prophylaxis with flu- conazole was associated with a decrease in fungal colo- nization and fewer deaths related to IFI, but did not improve overall survival. 9 Amphotericin B formulations are the agents of choice for the treatment of infections caused by As- pergillus species. Concerns about toxicity related to con- ventional amphotericin B 10 have inhibited its use as antifungal prophylaxis in OLT. The development of new lipid-based formulations of amphotericin B that are less toxic than the conventional form of the drug has led to renewed interest in the potential prophylactic use of this agent. 11-14 In 1 study, prophylaxis with liposo- mal amphotericin B (AmBisome; Nexstar, San Dimas, CA) at 1 mg/kg/d from the time of OLT reduced the incidence of IFI compared with placebo. 15 However, another group observed systemic mycosis in 4 of 58 liver transplant recipients treated according to a similar prophylactic schedule with AmBisome. 16 Amphotericin B lipid complex (Abelcet; The Lipo- some Co Ltd, London, England) is a lipid formulation with a high amphotericin B–lipid ratio (1:1), 17 and pharmacokinetic studies indicate that this formulation achieves lower peak plasma concentrations but greater tissue levels than the other lipid formulations of am- photericin B. 18 Furthermore, the in vitro activity of Abelcet against isolates of both Aspergillus and Candida organisms has recently been shown to be similar to that achieved by conventional amphotericin B but signifi- cantly greater than that achieved by AmBisome. 19 A randomized, prospective multicenter trial con- firmed that Abelcet was as effective as but less nephro- toxic than conventional amphotericin B for the treat- ment of invasive candidiasis in immunosuppressed patients (including solid-organ transplant recipients). 20 From the *Liver and Hepatobiliary Unit and the Departments of Clinical Microbiology and ‡Pathology, Queen Elizabeth Hospital, Edg- baston, Birmingham, UK. Laboratory work was supported in part by an educational grant from The Liposome Company Ltd, London, England. Address reprint requests to Dr Saket Singhal, Liver Research Labo- ratories, Clinical Research Block, Queen Elizabeth Hospital, Edgbaston, Birmingham B15 2TH, UK. Telephone: 44-121-6841236; E-mail: [email protected] Copyright © 2000 by the American Association for the Study of Liver Diseases 1527-6465/00/0605-0111$3.00/0 doi:10.1053/jlts.2000.7572 588 Liver Transplantation, Vol 6, No 5 (September), 2000: pp 588-595
-
Upload
saket-singhal -
Category
Documents
-
view
213 -
download
1
Transcript of Targeted prophylaxis with amphotericin B lipid complex in liver transplantation

Targeted Prophylaxis With Amphotericin B LipidComplex in Liver Transplantation
Saket Singhal,* Richard W. Ellis,† Stephen G. Jones,† Sarah J. Miller,‡
Neil C. Fisher,* J.G. Mark Hastings,† and David J. Mutimer*
The purpose of this study is to prospectively evaluate astrategy in which prophylaxis with amphotericin B lipidcomplex at 3 different dosages was targeted to liver trans-plant recipients at high risk for the development of inva-sive fungal infection (IFI). High risk was defined as apostoperative requirement for prolonged (>5 days) inten-sive care unit (ICU) treatment. Consecutive high-risk pa-tients were administered prophylaxis with amphotericin Blipid complex from day 5 after orthotopic liver transplan-tation (OLT) until ICU discharge or death. The first 10eligible patients were administered 5 mg/kg/d, the next 10patients were administered 2.5 mg/kg/d, and a final 10patients were administered 1 mg/kg/d. Drug safety andefficacy were assessed before each dosage reduction. Dur-ing the study period, 130 adult patients underwent 137OLTs. Thirty patients fulfilled the entry criteria and wereadministered prophylaxis with amphotericin B lipid com-plex. No patient developed proven IFI during prophy-laxis. Cultures from normally sterile sites (blood and ab-dominal drain fluid) always showed negative results. Allfungal isolates were sensitive in vitro to amphotericin B.There was no significant difference in colonization scoresamong the groups of patients administered different dos-ages of amphotericin B lipid complex. No death, seriousadverse reaction, or nephrotoxicity was attributed to am-photericin B lipid complex. We conclude that prophylaxiswith amphotericin B lipid complex targeted to patientsrequiring prolonged ICU treatment after OLT appears tobe well tolerated and may prevent IFI. Our current policyis to use amphotericin B lipid complex, 1 mg/kg/d, asantifungal prophylaxis in this high-risk group. (LiverTranspl 2000;6:588-595.)
Invasive fungal infection (IFI) has a high mortalityafter orthotopic liver transplantation (OLT). In
early studies, the incidence of IFI in this setting rangedfrom 18% to 42%, and the associated mortality rates
were 50% to 78%.1-6 Candida species accounted for themajority of infections, and many patients infected withCandida organisms survived. In contrast, infectionscaused by Aspergillus species were nearly always fa-tal.2,3,6 We showed that in liver transplant recipientsconsidered high risk for IFI, fluconazole prophylaxisreduced the incidence of invasive candidiasis7 but wascomplicated by the emergence of fluconazole-resistantfungi and failed to prevent invasive aspergillosis.8 Arecent randomized, placebo-controlled trial of livertransplant recipients showed that prophylaxis with flu-conazole was associated with a decrease in fungal colo-nization and fewer deaths related to IFI, but did notimprove overall survival.9
Amphotericin B formulations are the agents ofchoice for the treatment of infections caused by As-pergillus species. Concerns about toxicity related to con-ventional amphotericin B10 have inhibited its use asantifungal prophylaxis in OLT. The development ofnew lipid-based formulations of amphotericin B thatare less toxic than the conventional form of the drug hasled to renewed interest in the potential prophylactic useof this agent.11-14 In 1 study, prophylaxis with liposo-mal amphotericin B (AmBisome; Nexstar, San Dimas,CA) at 1 mg/kg/d from the time of OLT reduced theincidence of IFI compared with placebo.15 However,another group observed systemic mycosis in 4 of 58liver transplant recipients treated according to a similarprophylactic schedule with AmBisome.16
Amphotericin B lipid complex (Abelcet; The Lipo-some Co Ltd, London, England) is a lipid formulationwith a high amphotericin B–lipid ratio (1:1),17 andpharmacokinetic studies indicate that this formulationachieves lower peak plasma concentrations but greatertissue levels than the other lipid formulations of am-photericin B.18 Furthermore, the in vitro activity ofAbelcet against isolates of both Aspergillus and Candidaorganisms has recently been shown to be similar to thatachieved by conventional amphotericin B but signifi-cantly greater than that achieved by AmBisome.19
A randomized, prospective multicenter trial con-firmed that Abelcet was as effective as but less nephro-toxic than conventional amphotericin B for the treat-ment of invasive candidiasis in immunosuppressedpatients (including solid-organ transplant recipients).20
From the *Liver and Hepatobiliary Unit and the Departments of†Clinical Microbiology and ‡Pathology, Queen Elizabeth Hospital, Edg-baston, Birmingham, UK.
Laboratory work was supported in part by an educational grant fromThe Liposome Company Ltd, London, England.
Address reprint requests to Dr Saket Singhal, Liver Research Labo-ratories, Clinical Research Block, Queen Elizabeth Hospital, Edgbaston,Birmingham B15 2TH, UK. Telephone: 44-121-6841236; E-mail:[email protected]
Copyright © 2000 by the American Association for the Study ofLiver Diseases
1527-6465/00/0605-0111$3.00/0doi:10.1053/jlts.2000.7572
588 Liver Transplantation, Vol 6, No 5 (September), 2000: pp 588-595

A more recent study found that Abelcet was safe andeffective for the treatment of IFI in liver transplantrecipients in whom treatment with conventional am-photericin B had failed,21 but concluded that the resultscould have been improved by earlier initiation of ther-apy. We recently reported low toxicity with Abelcet, 5mg/kg/d, in 30 patients, 18 of whom had undergoneOLT (this report included 10 patients from the currentstudy).22
Risk factors for IFI after OLT can be identified andinclude a requirement for prolonged intensive care unit(ICU) treatment postoperatively.4,6,23 We performed aprospective audit of a strategy in which Abelcet wasadministered to patients requiring ICU treatment for 5days or greater post-OLT. This was achieved by inten-sive mycological surveillance of patients administeredAbelcet (before and during prophylaxis) followed by invitro fungal speciation and antifungal susceptibilitytesting. Clinical, laboratory, and postmortem data werealso recorded.
Patients and Methods
Approval for this prospective audit was obtained from thelocal research ethics committee, and informed consent wasobtained from patients or their next of kin.
Patients
All consecutive adult OLTs performed between November17, 1996, and December 31, 1997 (inclusive), were includedon the study. After OLT, all patients were administered tripleimmunosuppressive therapy with corticosteroids, azathio-prine, and either cyclosporine or tacrolimus. All patients wereadministered prophylactic antibacterial therapy with intrave-nous ceftazidime, 1 g 3 times daily, and coamoxiclav, 1.2 g 3times daily, for 48 hours after OLT (beta-lactam–allergicpatients were administered ciprofloxacin, 400 mg twice daily,and metronidazole, 500 mg 3 times daily).
Standard Antifungal Prophylaxis
According to unit protocol, oral (or nasogastric) nystatin pro-phylaxis, 500,000 U 3 times daily, was administered to allpatients for 3 months after OLT, and intravenous (or oral)fluconazole prophylaxis, 100 mg/d, was administered to pa-tients with identifiable pre-OLT risk factors for IFI (thosewho underwent transplantation for fulminant hepatic failureor retransplantation or required ICU treatment before OLT).
Targeted Abelcet Prophylaxis
All patients requiring ICU treatment (defined as a need formechanical ventilation or renal support in the form of con-tinuous venovenous hemofiltration [CVVH]) for 5 days orgreater after OLT were administered prophylaxis with Abel-
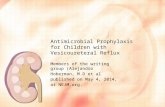
cet. This was started day 5 post-OLT and continued untilICU discharge or death. We used a protocol involving astepwise reduction in Abelcet dosage, starting with 5 mg/kg/d(high dosage [HD]) for the first 10 eligible patients, then 2.5mg/kg/d (medium dosage [MD]) for the next 10 eligiblepatients, and finally 1 mg/kg/d (low dosage [LD]) for another10 patients (Fig. 1). Safety and preliminary efficacy wereassessed before each dosage reduction to derive comparativedata on fungal colonization and drug safety and tolerability.All patients were administered a test dose of 1 mg over 15minutes before the first dose and were closely monitored forthe development of adverse reactions.
Clinical Data Analysis
For all patients administered Abelcet, demographic data wererecorded, including sex and risk factors for IFI. Clinical de-tails included duration of ICU treatment after OLT, durationand dosage of Abelcet therapy, adverse reactions to Abelcet,renal function before and during Abelcet prophylaxis (in par-ticular, the need for CVVH), concomitant medication duringAbelcet prophylaxis, and outcome at 12 months (with post-mortem details when this was performed).
Mycological Surveillance
For patients administered Abelcet prophylaxis, the followingclinical samples were collected, when possible, for fungal cul-ture before starting Abelcet therapy and twice weekly duringprophylaxis: throat swab, stool specimen (or rectal swab),urine specimen, sputum specimen (or endotracheal aspirate),
Figure 1. Strategy for targeted prophylaxis with Abelcet.
589Prophylaxis With Amphotericin B Lipid Complex

and abdominal drain fluid. Blood was collected specifically forfungal culture if 1 or more of the following features werepresent: unexplained pyrexia or leukocyte count greater than30 3 109/L, respiratory sepsis, or neurological deterioration.
Mycological Laboratory Analysis
Specimens were incubated for 48 hours on Sabouraud’s agar,and fungal growth was documented as absent, light, moder-ate, or heavy. Isolated yeasts were speciated by the API ID32Cyeast identification system (Bio-Merieux, Marcy L’Etoile,France), and sensitivities to fluconazole and amphotericin Bwere determined by the Etest method (AB Biodisk, Solna,Sweden).24 Strains were designated according to their mini-mum inhibitory concentrations (MICs) as fully sensitive,partly sensitive, or resistant to each antifungal agent. Forfluconazole, the MICs for these 3 categories were less than 16mg/L, 16 to 32 mg/L, and greater than 32 mg/L, respectively,and for amphotericin B, the MICs were less than 1 mg/L, 1 to2 mg/L, and greater than 2 mg/L, respectively.25
Mycological Definitions
Each isolate was assigned a score of 1 to 3 according towhether colonization by that species was light, moderate, orheavy, respectively; the sum of these scores for all isolates in anindividual patient was defined as the number of colonies forthat patient. A semiquantitative colonization score was thencalculated for each patient by the following formula:
no. of colonies 3 no. of sites colonized
total no. of specimens
In this way, overall colonization could be comparedamong patients treated with HD, MD, and LD Abelcet. Onthe basis of previous studies,2,3,5,6,23,26,27 proven IFI was de-fined as (1) histological evidence of fungal invasion (organbiopsy or postmortem histological evaluation) or (2) isolationof fungus from a single, normally sterile site (blood or abdom-inal drain fluid). In addition, isolation of Candida organismssimultaneously from 3 or more nonsterile sites (throat, rec-tum, urine, or sputum), which is regarded by some investiga-tors as highly predictive for the development of invasive in-fection, was defined as possible IFI. Colonization was definedas the isolation of fungus from 1 or 2 nonsterile sites. Negativesurveillance culture results obtained in a patient who hadpreviously shown colonization and/or IFI was defined as fun-gal clearance.
Statistical Analysis
Statistical analysis was performed using Statistical Packagesfor Social Sciences (SPSS Inc, Chicago, IL). Chi-squared testand Kruskal-Wallis test were used to compare the rates ofcolonization and colonization scores among groups of pa-tients, respectively. The t-test for paired samples was used tocompare the means of the serum creatinine values in patientsat the start and end of prophylactic therapy.
Results
All adult liver transplant recipients during the studyperiod were followed up for 12 months. During thisperiod, 130 adult patients received 137 liver trans-plants. Thirty patients (31 transplants) required ICUtreatment for 5 days or greater from the time of OLTand were administered Abelcet according to the strategypreviously described and shown in Figure 1. Accordingto previously published analyses of risk factors for thedevelopment of IFI,2-4,6-8,23,26-30 these 30 patients wereclearly at high risk (Table 1). IFI was not observed in the100 patients (106 transplants) who achieved ICU dis-charge before day 5 post-OLT.
Table 1. Patients Requiring Abelcet With Each RiskFactor for IFI
Risk Factors for IFI(n 5 15*)
No. of PatientsRequiring Abelcet
With Each Risk Factor(n 5 30)
PreoperativeRetransplantation 3Transplantation for fulminant
liver failure 8Inpatient at the time of trans-
plantation 16Requirement for ICU (for
mechanical ventilation) 7Requirement for hemodialysis 6
IntraoperativeRoux-en-Y (choledochojejunos-
tomy) biliary anastomosis 5Blood transfusion $10 units 8
Postoperative (within 12 wk)ICU stay $5 days 30†Requirement for reintubation 16Requirement for tracheostomy 11Bacterial infection requiring
parenteral antibiotic treat-ment 25
Cellular rejection episode(s)requiring steroid treatment 7
Requirement for repeatedlaparotomy 7
Requirement for hemodialysis 20Vascular complications 4
*Fifteen different risk factors were recorded; there were 173identifiable risk factors in the 30 patients, with a median of 6risk factors (range, 1 to 9 risk factors) per patient.†By definition, all 30 patients required ICU stay for 5 days orgreater.
590 Singhal et al

Clinical and Mycological Outcome
For these 30 patients (12 men, 18 women), the medianICU stay post-OLT was 14 days (range, 6 to 45 days),median duration of Abelcet prophylaxis was 7 days(range, 1 to 37 days), and median total dosage of Abel-cet administered was 0.9 g (range, 0.1 to 9.3 g) perpatient. Six of 30 patients died, and 3 of these patientsunderwent postmortem examination, including Gro-cott staining for fungal infection. None showed histo-logical evidence of fungal infection (Table 2). Only 1 of24 survivors had evidence of possible IFI during Abelcettherapy. In this patient, Candida species were isolatedsimultaneously from 3 nonsterile sites during Abelcetprophylaxis, but the patient did not develop clinicallysignificant infection, fungal clearance was achieved be-fore ICU discharge, and the patient was well 2 yearspost-OLT. No patient developed proven IFI before orduring Abelcet prophylaxis.
Fungal Speciation and Sensitivity Testing
Four hundred seven samples were examined (median,10 samples per patient; range, 2 to 42 samples perpatient), of which 69 samples (16.5%) yielded fungi(Table 3). The 69 isolates were from 21 patients. Ninepatients (3 patients at each dosage) always showed neg-ative culture results. No fungi were isolated from nor-mally sterile sites (blood or abdominal drain fluid) inany patient. Candida albicans and Candida glabrataaccounted for 54 of 69 isolates (78%). The greatestnumber of fungal isolates were obtained from throatswabs and stool specimens (46% and 35% of isolates,respectively). Twenty-one of 30 patients showed fungalcolonization at some stage before or during prophylaxis;throat and/or stool specimens yielded fungi in 20 of 21patients (95%).
Thirty-nine isolates were fully sensitive both to flu-conazole and amphotericin B. One isolate was fully
Table 2. Cause of Death in Patients Who Fulfilled Study Entry Criteria and Were Administered Abelcet
Patient No. Abelcet Dosage ICU Days (post-OLT) Day of Death (post-OLT) Cause of Death*
1 HD 23 23 Hemorrhagic necrotizing pancreatitis2 HD 24 24 Multiorgan failure3 HD 36 42 Cytomegalovirus pneumonitis4 MD 15 15 Primary nonfunction of graft (no postmortem)5 MD 16 50 Cytomegalovirus pneumonitis (no postmortem)6 LD 9 11 Gram-negative septicemia (no postmortem)
NOTE. Patients administered all dosages of Abelcet, n 5 6. Median ICU stay in these patients was 19.5 days (range, 9 to 36 days) afterOLT; median day of death post-OLT was day 23.5 (range, days 11 to 50).*No fungi were identified (by Grocott staining) on postmortem histological examination.
Table 3. Breakdown of Isolates by Fungal Species, Site of Colonization, and Sensitivity to Fluconazole and Amphotericin B
Species
Site FluconazoleSensitivity
Amphotericin BSensitivityT Sp St U D Total
Candida albicans 21 6 9 0 0 36 36 S 36 SCandida glabrata 5 0 12 1 0 18 1 S, 15 P/S, 2 R 17 S, 1 P/SCandida tropicalis 0 1 0 2 0 3 3 S 3 SCandida parapsilosis 1 0 2 1 0 4 4 P/S 4 SSacharomyces cerevisiae 2 1 0 0 0 3 3 P/S 3 SAspergillus fumigatus 3 1 1 0 0 5 5 R 5 STotal 32 9 24 4 0 69 40 S, 22 P/S, 7 R 68 S, 1 P/S
NOTE. (1) No fungi were isolated from drain fluid specimens (or blood cultures, not shown), (2) all isolates of C albicans were fullysensitive to both fluconazole and amphotericin B, and (3) no isolates were resistant to amphotericin B.Abbreviations: T, throat; Sp, sputum; St, stool; U, urine; D, abdominal drain fluid; S, fully sensitive; P/S, partly sensitive; R, resistant.
591Prophylaxis With Amphotericin B Lipid Complex

sensitive to fluconazole and partly sensitive to ampho-tericin B. Twenty-two isolates were partly sensitive tofluconazole and fully sensitive to amphotericin B. Sevenisolates were resistant to fluconazole and fully sensitiveto amphotericin B. Thus, all isolates were sensitive toamphotericin B (68 fully, 1 partly), but 29 of 69 isolateswere resistant or only partly sensitive to fluconazole.
Aspergillus fumigatus was isolated from 5 specimensin 3 patients and was always resistant to fluconazole. Calbicans was always fully sensitive both to fluconazoleand amphotericin B, but the majority of C glabrataisolates were resistant or only partly sensitive to flucon-azole. Seven of 30 patients were colonized with newspecies during Abelcet prophylaxis (Table 4).
Colonization Scores
The colonization score was calculated for each patient(see Methods; Table 5). There was no significant differ-ence in colonization scores among the groups of pa-tients administered HD, MD, or LD Abelcet (P 5 .56,Kruskal-Wallis test).
Safety
No deaths were attributed to Abelcet, and the drug wasnot stopped in any patient because of an adverse reac-tion. Seven of 30 patients started renal support (in theform of CVVH) during Abelcet prophylaxis, but allwere administered concomitant nephrotoxic medica-tion, and in 2 of these 7 patients, renal function recov-ered during Abelcet prophylaxis, allowing cessation ofCVVH. Ten of 30 patients never required CVVH(mean serum creatinine levels for these 10 patients werenot significantly different between the onset (98 6 11[SEM] mmol/L) and end (99 6 16 mmol/L) of Abelcettherapy (P 5 .99, t-test for paired samples). The other13 of 30 patients were undergoing CVVH before start-ing Abelcet therapy, reflecting the critically ill nature ofthe targeted population.
Discussion
The aim of this study is to evaluate a strategy in whichprophylaxis with Abelcet (at 3 different dosages) wastargeted to patients at high risk for the development ofIFI after OLT.
Early IFI is rarely observed in the technicallystraightforward transplant recipient who achieves earlyICU discharge. IFI was not observed in the 100 patientson this study who achieved ICU discharge before day 5
Table 5. Semiquantitative Colonization Scores forPatients Administered HD, MD, and LD Abelcet
Patient No. HD Abelcet MD Abelcet LD Abelcet
1 3.27 0.29 12 0.75 0 0.543 0.03 2 1.54 2.25 0.25 2.55 0.43 0.8 0.16 0 0.06 07 1.04 0.25 0.578 0 0 5.59 0 0.16 0
10 0.95 0 0Mean 6 SEM* 0.87 6 0.3 0.38 6 0.2 1.17 6 0.5
*Kruskal-Wallis test confirmed no significant difference incolonization scores among groups (P 5 .56).
Table 4. Patients Newly Colonized During Abelcet Prophylaxis
PatientNo.
AbelcetDosage Fungal Species Site(s) Colonized
FluconazoleSensitivity
Amphotericin BSensitivity
1 HD Candida glabrata Sputum, stool, throat Fully sensitive Partly sensitive2 HD Candida tropicalis Urine Fully sensitive Fully sensitive3 MD Aspergillus fumigatus Throat Resistant Fully sensitive4 LD Aspergillus fumigatus Stool, throat Resistant Fully sensitive5 LD Candida glabrata Stool Partly sensitive Fully sensitive6 LD Candida albicans Throat Fully sensitive Fully sensitive7 LD Sacharomyces cerevisiae Sputum, throat Partly sensitive Fully sensitive
NOTE. Six of these 7 patients were colonized by species other than C albicans, but none of these isolates was resistant to amphotericinB and none of these patients developed clinically significant fungal infection. Patients 3 and 6 died, but fungal infection was not acontributing factor.
592 Singhal et al

post-OLT and who therefore were not administeredAbelcet prophylaxis. In contrast, the 30 patients whorequired prolonged ICU treatment post-OLT had mul-tiple risk factors for the development of IFI (Table 1).Thus, the strategy of targeting prophylaxis to this groupappears to identify patients at risk for IFI with excellentsensitivity and specificity.
From a historical perspective, it is remarkable thatno patient in this consecutive series of 137 liver trans-plants developed proven IFI. An analysis of the Bir-mingham Liver Unit database (personal communica-tion, B. Gunson, January 1998), showed that 952patients underwent OLT at this center before the startof this study (January 19, 1982, to November 16, 1996[inclusive]). Of these, 49 patients (5.1%) developed IFIand 36 of 49 patients (73.5%) died of IFI. These figuresare similar to those reported in previous analyses ofincidence of and mortality from IFI in OLT.1-6 A fur-ther analysis of this database showed that the medianpostoperative ICU stay for the 495 consecutive OLTsperformed immediately before the current group was 3days (range, 0 to 124 days), and that 30% of thesetransplants required prolonged ($5 days) postoperativeICU treatment. The liver transplant recipients in thecurrent study are a similar population in that a similarproportion (30 of 130 patients; 23%) required pro-longed ICU treatment and therefore fulfilled the entrycriteria for prophylaxis with Abelcet.
Did early administration of Abelcet to high-risk pa-tients prevent clinically significant fungal infection?Postmortem studies of liver transplant recipients haveshown that IFI is often cryptic during life, and thatinvasive disseminated infection with Aspergillus speciesis frequently persistent despite prolonged HD therapywith amphotericin B.2,6,8,26,27,30,31 We recently re-viewed our use of AmBisome in 30 patients post-OLT.31 Of 5 patients administered AmBisome (medi-an dosage, 3.2 mg/k/d; range, 2.8 to 3.5 mg/kg/d for amedian of 14 days; range, 6 to 20 days) for presumedinvasive aspergillosis, 4 patients died. Postmortem ex-amination was performed in 3 of these 4 patients, andinvasive aspergillosis was confirmed in each case. In ourcurrent study of targeted Abelcet prophylaxis, 6 of 30patients died and none had premortem evidence of IFI.Three of these 6 patients underwent postmortem exam-ination and there was no histological evidence of fungalinvasion (Table 2). Thus, there was no proven mortalityfrom IFI, and we suggest that an antifungal strategybased on prophylaxis targeted to high-risk cases may bepreferable to empirical treatment.
In this study, all isolates of C albicans were fullysensitive to fluconazole. This is in keeping with the
findings of an earlier prospective study of fluconazoleprophylaxis for patients with acute liver failure.8 Thatstudy also showed that fluconazole-resistant species (Afumigatus, Candida krusei, Candida inconspicua, and Cglabrata) emerged in 4 of 8 patients who underwenttransplantation. The potential importance of emergentfluconazole-resistant species in liver transplant recipi-ents has been recognized by others. Fortun et al32 de-scribed the emergence of fluconazole-resistant C gla-brata and associated IFI in 4 liver transplant recipients.In the present study, we identified a number of fungalspecies that were resistant or only partly sensitive tofluconazole. They include 18 isolates of C glabrata, 17of which had reduced sensitivity to fluconazole. Allwere fully sensitive to amphotericin B (Table 3).
Although we confirmed the in vitro sensitivity offungal isolates to amphotericin B, many patients re-mained colonized with fungus despite the systemic ad-ministration of Abelcet, and a controlled randomizedstudy would be required to convincingly show the su-periority of amphotericin B over fluconazole. We ac-knowledge that the current study did not have a place-bo-treated or fluconazole-treated control group, but wehave identified from our unit a historical comparisongroup of patients who were not administered prophy-laxis with amphotericin B. Eight liver transplant recip-ients required ICU treatment for 5 days or greater andunderwent the same mycological surveillance protocolas the patients in the current study. Five of these 8patients were administered prophylaxis with flucon-azole (previously published8), whereas 3 patients werenot administered antifungal prophylaxis (personalcommunication, N. Fisher, Birmingham Liver Unit,October 1996). From these 8 patients, 88 specimenswere collected (median, 10.5 specimens; range, 6 to 16samples per patient), of which 33 yielded fungi(37.5%). In the current study, fungi were isolated from69 of 407 specimens (17%), and this difference ishighly significant (P , .001, Chi-squared test). Threeof the 8 historical patients developed IFI, and 2 of these3 patients died. We acknowledge, however, that com-parison with historical data is limited by factors thatcould independently impact on the development offungal infection, such as advances in surgical techniquesand ICU practices and the modification of posttrans-plantation drug regimens in favor of strategies that uselower dosages of immunosuppressive agents.
Previous investigators have reported their experiencewith LD amphotericin B. In a randomized, placebo-controlled study, Tollemar et al15 suggested that Am-Bisome prophylaxis, 1 mg/kg/d, for 5 days from thetime of OLT was effective in preventing IFI in trans-
593Prophylaxis With Amphotericin B Lipid Complex

plant recipients. However, 5 patients (including 2 pa-tients administered AmBisome prophylaxis) were with-drawn from the study at an early stage because ofsuspected fungal infection, and all 5 patients were thenadministered HD systemic antifungal therapy. An ad-ditional 2 patients administered AmBisome prophy-laxis subsequently developed suspected IFI and re-quired further AmBisome treatment, but died. In thestudy of Tollemar et al,15 5 of 37 placebo-treated pa-tients developed proven IFI with C albicans, and 1placebo-treated patient developed infection caused byAspergillus organisms. This latter patient is likely theonly one who would have benefited from AmBisome(in preference to fluconazole) prophylaxis because wehave shown that fluconazole prophylaxis is sufficient forpreventing invasive candidiasis in liver transplant recip-ients.7
In a more recent study (not placebo controlled),AmBisome prophylaxis at 1 mg/kg/d for 7 days fromthe time of OLT was administered to 58 transplantrecipients. Despite prophylaxis, 4 patients developedsystemic mycoses; 3 of these patients died of invasiveaspergillosis, and it was suggested that a dosage of 1mg/kg/d may be suboptimal as prophylaxis.16 Mora etal33 reviewed their experience using amphotericin Bprophylaxis at 10 mg/d for 10 to 14 days after OLT.Prophylaxis was considered for patients according topre-OLT criteria (those patients with encephalopathy,requiring ICU treatment, or with a positive fungal cul-ture result), and the incidence of IFI was 7.5% with noepisodes of aspergillosis. However, 7 patients who diedwithin the first 2 weeks post-OLT were excluded, andthe investigators do not report either the number ofpatients administered prophylaxis or the number ofinfected patients who died. Last, Singh et al34 described3 transplant recipients administered amphotericin B,0.5 to 1 mg/kg/d, for candidemia post-OLT; all 3 pa-tients subsequently developed invasive and fatal as-pergillosis.
None of these reports compared different dosageregimens. In the current study, we used a therapeuticdosage of Abelcet, 5 mg/kg/d, for the initial cohort ofeligible patients and proceeded to the lower dosage reg-imens only after showing acceptable safety and likelyefficacy. Comparison of the groups administered HD,MD, and LD Abelcet showed no clear relationship ofAbelcet dosage to colonization scores (P 5 .56,Kruskal-Wallis test). Our data therefore suggest thatLD Abelcet, 1 mg/kg/d, may be as effective as the higherdosages at limiting fungal colonization and preventingIFI.
At the 3 dosages studied, Abelcet was well tolerated
with no apparent renal toxicity. During the study pe-riod, no patient died of IFI or developed proven IFIduring Abelcet prophylaxis, and all fungal isolates weresensitive in vitro to amphotericin B. Patients adminis-tered LD Abelcet did not have a worse clinical outcomeand were not colonized more heavily than those admin-istered greater dosages. We therefore conclude that pro-phylaxis with Abelcet appears to be safe and may pre-vent IFI in this complex high-risk patient group.
We recommend that patients requiring prolongedICU treatment after OLT should be administered tar-geted prophylaxis with LD lipid-based amphotericin B,and our current policy is to use Abelcet, 1 mg/kg/d, inthese patients. We undertake surveillance mycologicalcultures in all patients administered Abelcet prophy-laxis and histological examination for fungi, when indi-cated. Detection of breakthrough infection would ne-cessitate an increase in dosage to therapeutic levels.
Acknowledgment
The authors thank their medical and nursing colleagues fortheir cooperation in specimen collection and Dr Desley Neiland Bridget Gunson for their assistance with statistical anal-ysis.
References1. Schroter GPJ, Hoelscher M, Putnam CW, Porter KA, Starzl TE.
Fungus infection after liver transplantation. Ann Surg 1977;186:115-122.
2. Wajszczuk CP, Dummer JS, Ho M, Van Thiel DH, Starzl TE,Iwatsuki S, et al. Fungal infections in liver transplant recipients.Transplantation 1985;40:347-353.
3. Kusne S, Dummer JS, Singh N, Iwatsuki S, Makowka L, Es-quivel C, et al. Infections after liver transplantation: An analysisof 101 consecutive cases. Medicine 1988;67:132-143.
4. Colonna JO II, Winston DJ, Brill JE, Goldstein LI, Hoff MP,Hiatt JR, et al. Infectious complications in liver transplantation.Arch Surg 1988;123:360-364.
5. Tollemar J, Ericzon B-G, Homberg K, Andersson J. The inci-dence and diagnosis of invasive fungal infections in liver trans-plant recipients. Transplant Proc 1990;22:242-244.
6. Castaldo P, Stratta RJ, Wood P, Markin RS, Patil KD, ShaeferMS, et al. Clinical spectrum of fungal infections after orthotopicliver transplantation. Arch Surg 1991;126:149-156.
7. Kung N, Fisher NC, Gunson B, Hastings M, Mutimer DJ.Fluconazole prophylaxis for high-risk liver transplant recipients[letter]. Lancet 1995;345:1234-1235.
8. Fisher NC, Cooper MA, Hastings JGM, Mutimer DJ. Fungalcolonization and fluconazole therapy in acute liver failure. Liver1998;18:320-325.
9. Winston DJ, Pakrasi A, Busuttil RW. Prophylactic fluconazolein liver transplant recipients. A randomized, double-blind, pla-cebo-controlled trial. Ann Intern Med 1999;131:729-737.
10. Warnock DW. Amphotericin B: An introduction. J AntimicrobChemother 1991;28(suppl B):S27-S38.
594 Singhal et al

11. de Marie S, Janknegt R, Bakker-Woudengerg JM. Clinical use ofliposomal and lipid-complexed amphotericin B. J AntimicrobChemother 1994;35:907-916.
12. Tollemar J, Ringden O. Lipid formulations of amphotericinB—Less toxicity but at what economic cost? Drug Saf 1995;13:207-218.
13. Hiemenz JW, Walsh TJ. Lipid formulations of amphotericin B:Recent progress and future directions. Clin Infect Dis 1996;22(suppl 2):S133-S144.
14. Richardson MD. Lipid complexes of amphotericin B: The com-petitive picture. J Med Microbiol 1997;46:185-187.
15. Tollemar J, Hockerstedt K, Ericzon BG, Jalanko H, Ringden O.Liposomal amphotericin B prevents invasive fungal infections inliver transplant recipients. Transplantation 1995;59:45-50.
16. Braun F, Ruechel R, Lorf R, Canelo R, Muller A, Sattler B, et al.Is liposomal amphotericin B (AmBisome) an effective prophy-laxis of mycotic infections after liver transplantation? TransplantProc 1998;30:1481-1483.
17. Janoff AS, Perkins WR, Saletan SL, Swenson CE. AmphotericinB lipid complex: A molecular rationale for the attenuation ofamphotericin B-related toxicities. J Liposome Res 1993;3:451-471.
18. Mehta J. Do variations in molecular structure affect the clinicalefficacy and safety of lipid-based amphotericin B preparations?Leuk Res 1997;21:183-188.
19. Johnson EM, Ojwang JO, Szekely A, Wallace TL, WarnockDW. Comparison of in vitro antifungal activities of free andliposome-encapsulated nystatin with those of four amphotericinB formulations. Antimicrob Agents Chemother 1998;42:1412-1416.
20. Anaissie EJ, White MH, Uzun O, Singer C, Bodey GP, AzarniaN, et al. Amphotericin B lipid complex vs amphotericin B fortreatment of haematogenous and invasive candidiasis: A pro-spective, randomized, multicentre trial [abstract]. Proc 35thIntersci Conf Antimicrob Agents Chemother 1995;LM21:330.
21. Merhav H, Mieles L. Amphotericin B lipid complex in thetreatment of invasive fungal infections in liver transplant pa-tients. Transplant Proc 1997;29:2670-2674.
22. Singhal S, Hastings JGM, Mutimer DJ. Safety of high-doseamphotericin B lipid complex. Bone Marrow Transplant 1999;24:116-117.
23. Collins LA, Samore MH, Roberts MS, Luzzati R, Jenkins RL,Lewis WD. Risk factors for invasive fungal infections compli-cating orthotopic liver transplantation. J Infect Dis 1994;170:644-652.
24. Chen SCA, O’Donnell ML, Gordon S, Gilbert GL. Antifungalsusceptibility testing using the Etest: Comparison with the brothmacrodilution technique. J Antimicrob Chemother 1996;37:265-273.
25. Pfaller MA, Messer SA, Bolstrom A, Odds FC, Rex JH. Multi-site reproducibility of the Etest MIC method for antifungalsusceptibility testing of yeast isolates. J Clin Microbiol 1996;34:1691-1693.
26. Brown RS, Lake JR, Katzman BA, Ascher NL, Somberg KA,Emond JC, et al. Incidence and significance of Aspergillus cul-tures following liver and kidney transplantation. Transplanta-tion 1996;61:666-669.
27. Rolando N, Harvey F, Brahm J, Philpott-Howard J, AlexanderG, Casewell M, et al. Fungal infection: A common, unrecog-nized complication of acute liver failure. J Hepatol 1991;12:1-9.
28. Paya CV, Hermans PE, Washington JA II, Smith TF, Anhalt JP,Wiesner RH, et al. Incidence, distribution, and outcome ofepisodes of infection in 100 orthotopic liver transplantations.Mayo Clin Proc 1989;64:555-564.
29. Patel R, Portela D, Badley AD, Harmsen WS, Larson-Keller JJ,Ilstrup DM, et al. Risk factors of invasive Candida and non-Candida fungal infections after liver transplantation. Transplan-tation 1996;62:926-934.
30. Boon AP, Adams DH, Buckels J, McMaster P. Cerebral as-pergillosis in liver transplantation. J Clin Pathol 1990;43:114-118.
31. Fisher NC, Singhal S, Miller SJ, Hastings JGM, Mutimer DJ.Fungal infection and liposomal amphotericin B (AmBisome)therapy in liver transplantation: A 2-year review. J AntimicrobChemother 1999;43:597-600.
32. Fortun J, Lopez-San Roman A, Velasco JJ, Sanchez-Sousa A, deVicente E, Nuno J, et al. Selection of Candida glabrata strainswith reduced susceptibility to azoles in four liver transplantpatients with invasive candidiasis. Eur J Clin Microbiol InfectDis 1997;16:314-318.
33. Mora NP, Klintmalm G, Solomon H, Goldstein RM, GonwaTA, Husberg BS. Selective amphotericin B prophylaxis in thereduction of fungal infections after liver transplant. TransplantProc 1992;24:154-155.
34. Singh N, Mieles L, Yu VL, Gayowski T. Invasive aspergillosis inliver transplant recipients: Association with candidemia andconsumption coagulopathy and failure of prophylaxis with low-dose amphotericin B. Clin Infect Dis 1993;17:906-908.
595Prophylaxis With Amphotericin B Lipid Complex