Tailoring Pediatric Procedural Sedation and Analgesia in the Emergency Department: Choosing a...
8
Tailoring Pediatric Procedural Sedation and Analgesia in the Emergency Department: Choosing a Regimen to Fit the Situation Jonathan Bennett, MD, Andrew DePiero, MD, Susanne Kost, MD P rocedures performed on children in the emergency department (ED) can be anxiety-producing, painful, or both. Many procedures require relative or complete immobility to be performed safely, both for the practi- tioner and the patient. In addition to ensuring safety, relief of anxiety and pain, and control of motion, the practitioner providing sedation in the ED must keep in mind “big picture” issues. These bigger issues include using bed space and staff Abstract: Practitioners of procedural sedation and analgesia for children in an emergency department setting must balance the needs of individual patients, including safety and effi- cacy, with the needs of the depart- ment as a whole, including efficiency and appropriate use of resources. Individual patient needs will vary depending on the age and develop- mental stage of the patient, the anticipated level of pain and dis- tress, the degree of immobility required, and the duration of the procedure. The ability to accurately predict the need for sedation, the level of sedation and degree of analgesia required for patient com- fort, and the best sedative agent to accomplish these goals without undesirable consequences is a skill that requires knowledge and experi- ence. This review presents 6 case scenarios illustrating various seda- tion options, from an evidence-based perspective whenever possible, for common pediatric presenting complaints. Keywords: procedural sedation analgesia; pediatrics; tailoring sedation Division of Emergency Medicine, Procedural Sedation Service, Nemours/ A.I. duPont Hospital for Children, Wilmington, DE. Reprint requests and correspondence: Susanne Kost, MD, Division of Emergency Medicine, Procedural Sedation Service, Nemours/A.I. duPont Hospital for Children, 1600 Rockland Rd. Wilmington, DE 19899. [email protected] 1522-8401/$ - see front matter © 2010 Elsevier Inc. All rights reserved. 274 VOL. 11, NO. 4 • TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST
-
Upload
jonathan-bennett -
Category
Documents
-
view
225 -
download
5
Transcript of Tailoring Pediatric Procedural Sedation and Analgesia in the Emergency Department: Choosing a...

Abstract:Practitioners of procedural sedationand analgesia for children in anemergency department setting mustbalance the needs of individualpatients, including safety and effi-cacy, with the needs of the depart-ment as a whole, including efficiencyand appropriate use of resources.Individual patient needs will varydepending on the age and develop-mental stage of the patient, theanticipated level of pain and dis-tress, the degree of immobilityrequired, and the duration of theprocedure. The ability to accuratelypredict the need for sedation, thelevel of sedation and degree ofanalgesia required for patient com-fort, and the best sedative agent toaccomplish these goals withoutundesirable consequences is a skillthat requires knowledge and experi-ence. This review presents 6 casescenarios illustrating various seda-tion options, from an evidence-basedperspective whenever possible,for common pediatric presentingcomplaints.
Keywords:procedural sedation analgesia;pediatrics; tailoring sedation
Division of Emergency Medicine,
Procedural Sedation Service, Nemours/
A.I. duPont Hospital for Children,
Wilmington, DE.Reprint requests and correspondence:Susanne Kost, MD, Division of EmergencyMedicine, Procedural Sedation Service,Nemours/A.I. duPont Hospital for Children,1600 Rockland Rd. Wilmington, DE [email protected]
1522-8401/$ - see front matter© 2010 Elsevier Inc. All rights reserved.
274 VOL. 11, NO. 4 • TAILORING PEDIATRIC PROCE
TailoringPediatricProceduralSedation and
Analgesia in theEmergencyDepartment:Choosing a
Regimen to Fitthe Situation
DURAL SEDATION / ANALGESIA IN
Jonathan Bennett, MD,Andrew DePiero, MD, Susanne Kost, MD
rocedures performed on children in the emergencydepartment (ED) can be anxiety-producing, painful, or
Pboth. Many procedures require relative or completeimmobility to be performed safely, both for the practi-tioner and the patient. In addition to ensuring safety, relief ofanxiety and pain, and control of motion, the practitionerproviding sedation in the ED must keep in mind “big picture”issues. These bigger issues include using bed space and staff
THE ED / BENNETT, DEPIERO, AND KOST

TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST • VOL. 11, NO. 4 275
efficiently, as well as heeding institutional andnational regulatory requirements. The ability tochoose a sedation regimen that optimizes all of thesefactors is an invaluable skill in creating an idealprocedural environment for the patients and provi-ders. The following case scenarios will illustrateapproaches to sedation of pediatric patients in theED and provide a practical, evidence-based ap-proach to common ED problems.
CASE 1An 18-month-old boy presents to the ED after
falling from a shopping cart. He had a brief loss ofconsciousness but no vomiting. The episode oc-curred approximately 1 hour ago. He is previouslyhealthy. The patient's vital signs are normal, but heis somewhat fussy during physical examination. Hehas a large, boggy parietal hematoma. You order acomputerized tomography (CT) study of the head.What are your sedation options?
This case provides an example of a brief, painlessprocedure that may require sedation to obtain high-quality diagnostic images. In many situations, thisstudy could be completed without sedation. Thechild may be able to be briefly calmed anddistracted by a parent, child life practitioner, ordesign features in the scanning room, such aspictures on the ceiling. The increased speed ofnew CT scanners has decreased the number ofpatients needing sedation. The use of multisectionalhelical CT compared with single-section helical CTwas shown to decrease the need for sedation 3-fold.1
Another study noted that sedation was only re-quired in 8.6% of all pediatric patients but in 36.4%of patients between 12 and 30 months of age.2
If distraction and immobilizer devices fail, mid-azolam is commonly used as a first-line agent in thissetting. Although it can be administered in a numberof routes, most literature related to the abovevignette has considered its intravenous use. Morethan 90% of children ages 6 months to 6 years wereable to complete a CT scan with a single dose ofintravenous midazolam (0.2 mg/kg).3 Adverseeffects were minimal and included mild desatura-tion (SpO2 90%-95%) in 7% of patients, and therewere no airway complications among the 516patients enrolled in the study.
An alternative to midazolam is pentobarbital. Ithas long been used for pediatric CT, with successrates as high as 97% and with few failures orcomplications.4,5 In 2000, Moro-Sutherland et al6
compared the use of intravenous midazolam withpentobarbital for sedation for head CT imaging. Inthis prospective, randomized clinical trial, 55
patients were enrolled. In the pentobarbital group,97% of patients were successfully sedated andscanned as opposed to 19% of patients who receivedmidazolam. Oral pentobarbital has been shown tobe as effective as chloral hydrate in sedating patientsyounger than 1 year for imaging studies, with feweradverse events.7
A number of other agents have been comparedwith pentobarbital. In a prospective study ofpediatric patients undergoing diagnostic CT, propo-fol was found to require more airway manipulationsto relieve obstruction (23% vs 0%) and to have moreadverse respiratory events (12% vs 0%).8 Etomidatehas also been compared with pentobarbital insedation for CT scans.9 In a cohort from aprospectively gathered database, fewer unsuccess-ful sedations were noted in the etomidate group.Adverse events were more common in the pento-barbital group, whereas both groups had few apneicevents. A prospective double-blinded study showedthe rate of successful sedations in the etomidategroup to be 76% as compared with 97% forpentobarbital.10 Use of etomidate does have amuch shorter recovery time compared withpentobarbital.9,10
Dexmedetomidine is a newer sedative with morelimited data pertaining to its use in pediatricpatients. Its use was first reported prospectively in2006.11 In a pilot program, 62 patients undergoingCT were sedated with dexmedetomidine. Somedecreases in heart rate and blood pressure werenoted initially, but no changes were noted inrespiratory rate or end-tidal CO2. Further workdemonstrated that the use of dexmedetomidine wasassociated with transient sinus arrhythmias in 12%of patients and modest but unpredictable hemody-namic fluctuations.12
For brief painless procedures such as head CT,there are a number of safe and efficacious sedativeoptions. Intravenous access may be an importantconsideration. In this scenario, an agent with a shorthalf-life may be most efficient and will provide theopportunity to more accurately monitor thepatient's mental status.
CASE 2A 4-year-old boy presents to the ED with abdom-
inal pain. He was well until 2 days ago when hedeveloped diffuse abdominal pain. The pain has nowworsened. He has fever and anorexia. He vomitedonce approximately 6 hours ago. On examination, heis uncomfortable but not toxic-appearing. His vitalsare stable. He has significant diffuse abdominal pain.You order a complete blood count, which shows a

276 VOL. 11, NO. 4 • TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST
white blood cell count of 17 000 with left shift. Yourequest surgical consultation. As there is concern forappendicitis, the surgeon requests a CT. What is thebest sedative choice?
Although seemingly similar, this scenario doesvary importantly from that in case 1. Although newCT technology continues to decrease study time,this study is still much longer than a noncontrasthead CT. The other consideration is the injection ofcontrast. Contrast will often result in a “flushed” oruncomfortable sensation that may cause a child tomove. Given the concerns for radiation exposureand the issues with redosing contrast, a carefulselection of sedative agent is indicated to maximizesuccessful imaging on the initial attempt.
In this scenario, the current literature is lesshelpful. Many studies have considered sedation ofpediatric patients for CT, but none have addressedthis more complex CT case scenario. Most sedationregimens that were considered in case 1 primarilyaddressed the issue of noncontrast head CT alone.In addition to contrast studies, other examples ofmore complex CT studies requiring more completeimmobility include studies with fine cuts, such asCT of the temporal bones; studies with theanticipated need for 3-dimensional reconstruction,as in maxillofacial trauma; and studies that requirecrucial timing in the injection of contrast, such aswith CT angiography.
With these considerations, short-acting agentsmay not be the ideal choice. Whereas the patientmay be sedated, they must also be still. Anabdominal CT will require that the patient be stillfor a longer period than in the case of a noncontrasthead CT. As always, the clinical scenario and thepatient's level of cooperation will help guide thesedation choice.
The use of oral contrast poses a challenge tosedation providers because, by definition, it is inconflict with the patient's “NPO status.” A retro-spective study with pentobarbital noted com-plications in almost 15% of patients.13 Thesecomplications included desaturation, vomiting, air-way secretions, airway obstruction, coughing, andbronchospasm. A larger retrospective study consid-ered a similar question in patients receiving pento-barbital or chloral hydrate.14 Most patients in thestudy were sedated with pentobarbital, and none ofthe 367 patients had any complications related tothe administration of the oral contrast material.
As in the previous case, a number of safe andefficacious sedative options exist. Very short-actingagents may not be appropriate for a number ofpatients. Use of a somewhat longer-acting agent,such as propofol via repeated “mini-bolus” or by
infusion, dexmedetomidine infusion, or ketamine,may be most efficient in the scenario given thehigher radiation doses and the issues associatedwith the readministration of intravenous contrast.
CASE 3A 6-year-old girl presents to the ED with leg
weakness. She has had mild weakness for severaldays and is now having some difficulty withambulation. She also reports some mild back pain.She has no upper extremity weakness or breathingdifficulty. Part of the ED diagnostic evaluationincludes lumbar spine radiographs that areconcerning for a mass. A magnetic resonanceimaging (MRI) study of the spine is indicated, andyou are asked to provide the sedation. What areyour alternatives?
This is an example of a long painless procedurethat will require sedation. The patient is havingsome back pain, the degree to which that may affectthe sedation strategy. Ideally, the MRI could beperformed without sedation; however, several obsta-cles exist. The noise generated by the machine andnarrow space contribute to anxiety for manychildren (and adults). As in the case vignette, thepatient may be experiencing pain. The family willhave had little time to speak to their child to helpprepare her for the procedure. Also of importance isthe length of the study itself. An MRI of the spine is amuch longer procedure than an MRI of the brain,with an average “table time” of 60 to 90 minutes.
Alternatives to sedation have been investigated. Aprotocol that used a mock scanner with trainingsessions was successful in allowing functional MRIstudies to be accomplished without sedation in 90%of cases overall and in more than 88% of patientsyounger than 7 years.15 In the acute setting, thisapproach may not be practical. Audiovisual systemsmay have more benefit in the acute setting. In theambulatory setting, alternatives such as these havebeen shown to decrease the need for sedation.16
Intravenous pentobarbital has been used success-fully for this purpose, with a success rate greaterthan 90% and few adverse events.17,18 However,pentobarbital's success rate in children older than12 years or in those greater than 50 kg isdecreased.18
Another frequently used sedative for MRI ispropofol. In a larger multicenter study in childrenundergoing MRI, both pentobarbital and propofolwere found to provide an equal number ofsuccessful sedations (96%). Patients receiving pro-pofol had more apneic events, but the rate of apneaand airway complications combined was similar in

TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST • VOL. 11, NO. 4 277
the 2 groups. Pentobarbital was associated withmore failed sedation, unplanned admissions, andprolonged recovery and vomiting.19 In anotherstudy comparing propofol to a regimen of pento-barbital/fentanyl/midazolam, propofol had fasteronset and recovery with a similar or superiorsuccess rate.20 The rate of adverse events wasalso similar. Propofol is typically administered as aconstant infusion after an initial bolus, but somehave reported success with intermittent smalldoses21 or a single dose for shorter studies.22
As in the case of CT, dexmedetomidine has beenused for pediatric MRI. The largest study is aretrospective analysis of 747 patients.23 At higherdoses, the success rate for completing the MRI was97.6%. Bradycardia and hypotension were noted,but there were no adverse events.
The sedation options in this setting may be morelimited, but they are safe and efficacious. Agentssuch as propofol may require physician presenceand may not represent efficient use of time for abusy ED physician.
CASE 4A 23-month-old boy was chasing his 4-year-old
brother around the living room. He tripped over atoy dump truck and fell, striking his forehead on thecoffee table. He sustained a 3-cm laceration to hismid-forehead. It is sufficiently long and deep suchthat it will require sutures. The injury occurred 3hours ago, and he has been acting normally since.The result of his examination is otherwise unre-markable. He last ate at breakfast time (6 hours ago)and drank some apple juice 2 hours ago. The motherdescribes him as “wild,” and she asks for somethingto “knock him out” for the repair.
Simple facial lacerations are extremely commoninjuries thatmay require suturing in theED. Althoughthese typically can be repaired without significantdiscomfort because of topical anesthetic preparationssuch as LET (lidocaine, epinephrine, tetracaine) gelthey frequently cause significant anxiety in toddlersand school-aged children. In addition, althoughcomplete immobility is not necessary, relative immo-bility is required. This can be achieved with restraintdevices, such as soft papoose board, or additionalpersonnel; but restraint itself can cause additionalfear and anxiety. In children where routine comfortmeasures and distraction are not adequate, mild tomoderate sedation is helpful to provide the necessaryprocedure environment.
Given the goal of reducing fear and anxiety,midazolam, a short-acting benzodiazepine, is anexcellent choice for mild-to-moderate sedation in
children undergoing simple laceration repair. Itprovides anxiolysis, sedation, and antegrade am-nesia. It can be given by various nonparenteralroutes including oral, intranasal, and rectal, andhas been shown to decrease fear and anxietysignificantly.24-26 Recommended dosing ranges formidazolam are 0.2 to 0.4 mg/kg intranasally and0.5 to 0.7 mg/kg orally. Intranasal administrationcan be facilitated by use of an atomizer, althoughmore than 5 mg in a single dose is difficult toadminister. Onset of action is route dependent.Intranasal is the fastest, with an onset in less than5 minutes; and oral is the slowest, with onset in 20to 30 minutes. Typically, there are minimaladverse effects with nonparenteral administration.Pulse oximetry should be performed, but respira-tory depression is extremely unusual with the useof nonparenteral midazolam alone. Duration ofaction is usually about an hour. Paradoxicalagitation is the most disturbing adverse effect,and in one study, occurred in 12.5% of patients.25
It is our practice to warn parents of this adverseeffect, as at times it may occur after discharge.
An alternative to midazolam, if available, isnitrous oxide (NO). This inhalational agent canprovide anxiolysis, sedation, and analgesia. It isavailable in commercial units that can providecontinuous flow of up to 70% NO (30% 02) througheither a nasal mask or a full face mask. Thesecommercially available units have combined deliv-ery/scavenger systems that are necessary to isolateexposure to the patient. Nitrous oxide use has beenstudied by Luhmann et al27 for simple faciallacerations and was shown to decrease distress andimprove provider satisfaction compared with mid-azolam or standard care. There were no respiratorycomplications in their study, although there wasvomiting in about 10% of patients receiving NO.Nitrous oxide is advantageous because the desiredeffects resolve within minutes of its discontinuation,it has significantly less adverse effects in thefollowing 24 hours, and it has significantly shorterrecovery times compared with midazolam.27
CASE 5A 10-year-old boy has suffered a distal radius and
ulna fracture in a fall on his right arm. The fracturesare angulated 45° dorsally and displaced. He hassustained no head or abdominal injuries. Theorthopedist requests “conscious sedation” so thathe can reduce the fracture.
Extremely painful short procedures such as thisone (others in this category include large jointdislocation, abscess drainage, and burn debridement)

278 VOL. 11, NO. 4 • TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST
are generally best performed under proceduralsedation with ketamine or deep sedation withpropofol. The term conscious sedation is not applicable,as the goal is to not have the patient conscious forthe procedure.
Ketamine, a dissociative anesthetic, is in manyways the ideal agent for such procedures. It placesthe patient in a trance-like state of sedation, alsoproviding significant analgesia, immobility, andamnesia. This state is accomplished while usuallymaintaining upper airway muscle tone, protectiveairway reflexes, and spontaneous respiration. Sig-nificant respiratory complications are extremelyuncommon.28 Duration of peak action when givenintravenously is 5 to 10 minutes, allowing forfracture reduction, casting, and molding to beaccomplished with a small number of doses.Although it may be given intramuscularly, thepotential need for repeat dosing and higher ratesof adverse effects make the intramuscular route lessdesirable for this procedure. The most commonadverse effect of ketamine is postprocedure vomit-ing, occurring in 8% of patients. Larger doses andintramuscular administration are associated withincreased rates of emesis.29 The most fearedadverse effect, laryngospasm, is exceedingly rareand usually relieved with positive pressure ventila-tion.30 Midazolam has traditionally been used withketamine to prevent emergence reactions, which,when severe, can be frightening for parents anddisruptive to care. Two randomized trials havespecifically looked at the emergence phenome-na.31,32 Wathen et al31 showed no difference ineither overall emergence or “severe emergence”between all patients receiving ketamine comparedwith patients receiving ketamine and midazolam forsedation. Similarly, Sherwin et al32 showed nodifference in recovery agitation, severe hallucina-tions, or nightmares. However, in the Wathen et alstudy for patients older than 10 years, there was anonsignificant trend toward a lower incidence of“severe emergence” and less vomiting in patientsreceiving ketamine and midazolam. The combina-tion of ketamine/midazolam has been shown to besuperior to fentanyl/midazolam in sedation fororthopedic procedures.33 In cases where ketaminemay be contraindicated (increased intracranialpressure, increased ocular pressure, hypertension),fentanyl/midazolam is an alternative.
Propofol is another option in this case. Byproviding deep sedation, propofol can allow forpainful procedures to be performed. Propofol itself,unlike ketamine, does not provide analgesia andtherefore may require an analgesic agent such asfentanyl or sufentanil. Combination of propofol with
a narcotic agent may increase respiratory depres-sion and apnea. Propofol has been shown to beeffective in one study of brief orthopedic proceduresin a pediatric ED.34 Patients in that study showedslightly more distress with propofol/fentanyl com-pared with ketamine/midazolam. Parental scoring ofperceived pain, orthopedist satisfaction, and patientrecall of the procedure were not different for the 2groups. Propofol/fentanyl allowed significantly fasterrecovery times (20.8 vs 54.2 minutes). However,propofol/fentanyl did cause more frequent oxygendesaturations and required more minor airwayinterventions (jaw thrust and supplemental oxy-gen). Given the increased risk of potential airwaycomplications, propofol should only be used bypractitioners skilled in pediatric airway manage-ment. When used for brief painful procedures,propofol is typically given in 0.5 to 1 mg/kgincrements titrated to the desired effect. In theGodambe et al34 study, the mean propofol dose overthe duration of the procedure was 4.5 mg/kg.Although not extensively studied in the pediatricemergency setting, the combination of ketamineand propofol may also provide adequate deepsedation. The addition of ketamine theoreticallyprovides analgesia effects that propofol does not,without the increased respiratory depression ofnarcotic agents. The combined sedative effectsmay allow for smaller doses to be used than if eitherwere used alone. In a large case series using thisregimen of propofol and ketamine mixed 1:1 in asingle syringe for primarily orthopedic procedures,sedation was effective and well tolerated withaverage doses of 0.8 mg/kg of each agent.35
Finally, in cases where there is a desire or necessityto avoid deep sedation, the use of NO combined withhematoma block is a sedation alternative for pediat-ric forearm fracture reductions. Luhmann et al36
compared 50% NO combined with lidocaine hemato-ma block (NO was given for both hematoma blockand fracture reduction) to ketamine (1 mg/kg)/midazolam for middle to distal forearm fractures inpatients aged 5 to 17 years. They found that bothgroups had very little distress with the procedure; andin fact, those receiving NO/hematoma block hadslightly less distress. In addition, recovery time wasremarkably shorter with NO/hematoma block, 16minutes compared with 83 minutes with ketamine/midazolam. The groups had similar rates of vomitingin the ED, but the ketamine/midazolam group self-reported more adverse effects in the 24 hoursfollowing the procedure. It should be noted that, inthis study, all patients received an oral narcotic asroutine care for presumed fractures. Nitrous oxide'seffectiveness in this setting implies that it may be

TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST • VOL. 11, NO. 4 279
useful for other moderately to severely painfulprocedures where local anesthesia can be used,such as abscess drainage.
CASE 6A 4-year-old boy was bitten on the lip by his
grandmother's dog. He has sustained a complexlaceration to the upper lip that causes significantdisruption to the vermillion border and will requiremultiple layers to close. The plastic surgeon on callhas agreed to perform the repair, but wants the childsedated so he “will not be moving at all” for the 25minutes he estimates the repair will take.
Prolonged procedures that require significantimmobility such as this may require deeper sedationthan is possible with midazolam or NO. In this case,either procedural sedation, with ketamine (with orwithout midazolam), or deep sedation with propofolmay be used. Ketamine would need to be given in anumber of intermittent doses (0.5-1 mg/kg) over theduration of the procedure. As discussed earlier,larger doses may increase the incidence of post-procedure emesis. Propofol may be the idealsedation agent for procedures such as this. Pain ofthe procedure can be managed with either topicalanesthetics before sedation or local injection ornerve block during sedation. However, topicals maynot be practical on a mucosal surface or advisablenear the vermillion border because of systemicabsorption of the agent. A propofol bolus of 1 to 3mg/kg followed by an infusion of 100 to 300 µg/kg/min can then be used to achieve deep sedation forthe duration of the procedure. Propofol may be usedsimilarly in procedures where ketamine may becontraindicated such as ophthalmologic examina-
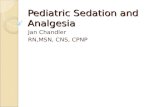
Figure 1. A 3-dimensional approach to tailoring sedation. CH chloral hinfusion; KET ketamine; MDZ midazolam; N2O nitrous oxide; PENT pen
tions (because of concern of elevated intraocularpressure) or lumbar puncture (because of concernof elevated intracranial pressure).37
Sedation is an invaluable tool in the ED forperforming procedures on children. As discussed,there are various agents that can be used dependingon the length of the study and the degree of sedationrequired. For anxiety-producing, but relativelypainless procedures, both midazolam and NO havebeen shown to be extremely safe and effective. Forintensely painful procedures or prolonged proce-dures, ketamine (with or without midazolam) andpropofol are effective. Ketamine may provide a verysmall, perhaps clinically irrelevant, benefit insedation level, whereas propofol provides morerapid recovery and less postprocedure vomiting.Propofol has a narrower therapeutic range and islikely to require more minor airway positioningmaneuvers and supplemental oxygen. Nitrous oxide,when available and when combined with oralnarcotic and local anesthesia, is an alternative thatdoes not require intravenous access for evenmoderately to severely painful procedures.
SUMMARYThe pharmacologic and nonpharmacologic
options for the provision of pediatric proceduralsedation and analgesia have expanded dramaticallyover the past 2 decades. With experience, emergen-cy care providers can begin to use finesse in thedecision of when to provide pharmacologic seda-tion, which agent(s) to use, and how best to deliverthe medications. Figure 1 provides a 3-dimensionalillustration of this concept, with an approximationof where various sedative agents fall when
ydrate; DEX dexmedetomidine; ETOM etomidate; FENT fentanyl; INFtobarbital; PROP propofol.

280 VOL. 11, NO. 4 • TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST
considering control of pain, need for immobility,and the duration of the procedure.
Sufficiently powered studies involving large numb-ers of patients attest to the safety of current practicegiven modern monitoring standards.28,29,38,39 As wemature as a specialty, we should continue to broadenprocedural sedation and analgesia research andclinical policy to include other aspects of qualitybesides safety, such as efficacy, efficiency, andpatient- and family-centered sedation care. We arestarting to recognize additional opportunities toalleviate suffering, exemplified by a recent studylooking at the cumulative stress of multiple “minor”procedures over the course of an ED visit.40 Inanother recent study, preliminary research intointraprocedure agitation as a sedation complicationsuggests that even in procedures that are considered“successful,” 8% of the patients experienced someperiod of agitation.41 Much progress has been made,but we continue to strive for ideal methods forrelieving procedural pain and stress.
REFERENCES1. Pappas JN, Donnelly LF, Frush DP. Reduced frequency of
sedation of young children with multisection helical CT.Radiology 2000;215:897-9.
2. Sacchetti A, Carraccio C, Giardino A, et al. Sedation forpediatric CT scanning: is radiology becoming a drug-freezone? Pediatr Emerg Care 2005;21:295-7.
3. Singh R, Kumar N, Vajifdar H. Midazolam as a sole sedativefor computed tomography imaging in pediatric patients.Paediatr Anaesth 2009;19:899-904.
4. Strain JD, Harvey LA, Foley LC, et al. Intravenouslyadministered pentobarbital sodium for sedation in pediatricCT. Radiology 1986;161:105-8.
5. Pereira JK, Burrows PE, Richards HM, et al. Comparison ofsedation regimens for pediatric outpatient CT. Pediatr Radiol1993;23:341-4.
6. Moro-Sutherland DM, Algren JT, Louis PT, et al. Comparisonof intravenous midazolam with pentobarbital for sedation forhead computed tomography imaging. Acad Emerg Med 2000;7:1370-5.
7. Mason KP, Sanborn P, Zurakowski D, et al. Superiority ofpentobarbital versus chloral hydrate for sedation in infantsduring imaging. Radiology 2004;230:537-42.
8. Zgleszewski SE, Zurakowski D, Fontaine PJ, et al. Is propofola safe alternative to pentobarbital for sedation duringpediatric diagnostic CT? Radiology 2008;247:528-34.
9. Baxter AL, Mallory MD, Spandorfer PR, and the PediatricSedation Research Consortium. Etomidate versus pentobar-bital for computed tomography sedations: report from thePediatric Sedation Research Consortium. Pediatr Emerg Care2007;23:690-5.
10. Kienstra AJ, Ward MA, Sasan F, et al. Etomidate versuspentobarbital for sedation of children for head and neck CTimaging. Pediatr Emerg Care 2004;20:499-506.
11. Mason KP, Zgleszewski SE, Dearden JL, et al. Dexmedetomi-dine for pediatric sedation for computed tomography imagingstudies. Anesth Analg 2006;103:57-62.
12. Mason KP, Zgleszewski SE, Prescilla R, et al. Hemodynamiceffects of dexmedetomidine sedation for CT imaging studies.Paediatr Anaesth 2008;18:393-402.
13. Sanderson PM. A survey of pentobarbital sedation forchildren undergoing abdominal CT scans after oral contrastmedium. Paediatr Anaesth 1997;7:309-15.
14. Ziegler MA, Fricke BL, Donnelly LF. Is administration ofenteric contrast material safe before abdominal CT inchildren who require sedation? Experience with chloralhydrate and pentobarbital. Am J Roentgenol 2003;180:13-5.
15. de Bie HM, Boersma M, Wattjes MP, et al. Preparing childrenwith a mock scanner training protocol results in high qualitystructural and functional MRI scans. Eur J Pediatr 2010;169:1079-85.
16. Lemaire C, Moran GR, Swan H. Impact of audio/visualsystems on pediatric sedation in magnetic resonanceimaging. J Magn Reson Imaging 2009;30:649-55.
17. Bloomfield EL, Masaryk TJ, Caplin A, et al. Intravenoussedation for MR imaging of the brain and spine in children:pentobarbital versus propofol. Radiology 1993;186:93-7.
18. Greenberg SB, Adams RC, Aspinall CL. Initial experiencewith intravenous pentobarbital sedation for children under-going MRI at a tertiary care pediatric hospital: the learningcurve. Pediatr Radiol 2000;30:689-91.
19. Mallory MD, Baxter AL, Kost SI, and the Pediatric SedationResearch Consortium. Propofol vs pentobarbital for sedationof children undergoing magnetic resonance imaging: resultsfrom the Pediatric Sedation Research Consortium. PaediatrAnaesth 2009;19:601-11.
20. Pershad J, Wan J, Anghelescu DL. Comparison of propofolwith pentobarbital/midazolam/fentanyl sedation for magneticresonance imaging of the brain in children. Pediatrics 2007;120:e629-36.
21. Chen YL, Chen CC. Intermittent small doses of propofol forsedation of pediatric patients undergoing magnetic reso-nance imaging. Acta Paediatr Taiwan 2007;48:305-8.
22. Cho JE, Kim WO, Chang DJ, et al. Titrated propofolinduction vs. continuous infusion in children undergoingmagnetic resonance imaging. Acta Anaesthesiol Scand 2010;54:453-7.
23. Mason KP, Zurakowski D, Zgleszewski SE, et al. High dosedexmedetomidine as the sole sedative for pediatric MRI.Paediatr Anaesth 2008;18:403-11.
24. Hennes HM, Wagner V, Bonadio WA, et al. The effect of oralmidazolam on anxiety of preschool children during lacera-tion repair. Ann Emerg Med 1991;20:713-6.
25. Shane SA, Fuchs SM, Khine H. Efficacy of rectal midazolamfor the sedation of preschool children undergoing lacerationrepair. Ann Emerg Med 1994;24:1170-2.
26. Theroux MC, West DW, Corddry DH, et al. Efficacy ofintranasal midazolam in facilitating suturing of lacerations inpreschool children in the emergency department. Pediatrics1993;91:624-7.
27. Luhmann JD, Kennedy RM, Porter FL, et al. A randomizedclinical trial of continuous-flow nitrous oxide and midazolamfor sedation of young children during laceration repair. AnnEmerg Med 2001;37:20-7.
28. Green SM, Roback MG, Krauss B, et al. Predictors of airwayand respiratory adverse events with ketamine sedation in theemergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med 2009;54:158-70.
29. Green SM, Roback MG, Krauss B, et al. Predictors of emesisand recovery agitation with emergency department ketaminesedation: an individual-patient data meta-analysis of 8,282children. Ann Emerg Med 2009;54:171-80.

TAILORING PEDIATRIC PROCEDURAL SEDATION / ANALGESIA IN THE ED / BENNETT, DEPIERO, AND KOST • VOL. 11, NO. 4 281
30. Green SM, Kupperman N, Rothrock SG, et al. Predictors ofadverse events with intramuscular ketamine sedation inchildren. Ann Emerg Med 2000;35:35-42.
31. Wathen JE, Roback MG, Mackenzie T, et al. Does midazolamalter the clinical effects of intravenous ketamine sedation inchildren? A double-blind, randomized, controlled, emergen-cy department trial. Ann Emerg Med 2000;36:579-88.
32. Sherwin TS, Green SM, Khan A, et al. Does adjunctivemidazolam reduce recovery agitation after ketaminesedation for pediatric procedures? A randomized, dou-ble-blind, placebo-controlled trial. Ann Emerg Med 2000;35:229-38.
33. Kennedy RM, Porter FL, Miller JP, et al. Comparison offentanyl/midazolam with ketamine/midazolam for pediatricorthopedic procedures. Pediatrics 1998;102:956-63.
34. Godambe SA, Elliot V, Matheny D, et al. Comparison ofpropofol/fentanyl versus ketamine/midazolam for brief or-thopedic procedural sedation in a pediatric emergencydepartment. Pediatrics 2003;112:116-23.
35. Andolfatto G, William M. A prospective case series ofpediatric procedural sedation and analgesia in the emergencydepartment using single-syringe ketamine-propofol combi-nation (ketofol). Acad Emerg Med 2010;17:194-201.
36. Luhmann JD, Shootman M, Luhmann SJ, et al. A randomizedcomparison of nitrous oxide plus hematoma block versusketamine plusmidazolam for emergency department forearmfracture reduction in children. Pediatrics 2006;118:e1078-86.
37. Ben Yehuda Y, Watemborg N. Ketamine increases openingcerebrospinal pressure in children undergoing lumbarpuncture. J Child Neurol 2006;21:441-3.
38. Cravero JP, Beach ML, Blike GT, et al. The incidence andnature of adverse events during pediatric sedation/anesthesiawith propofol for procedures outside the operating room: areport from the Pediatric Sedation Research Consortium.Anesth Analg 2009;108:795-804.
39. Cravero JP, Blike GT, Beach M, et al. Incidence and nature ofadverse events during pediatric sedation/anesthesia forprocedures outside the operating room: report from thePediatric Sedation Research Consortium. Pediatrics 2006;118:1087-96.
40. Sacchetti A, Baren J, Carraccio C. Total procedural require-ments as indication for emergency department sedation.Pediatr Emerg Care 2010;26:209-11.
41. Lightdale J, Valim C, Mahoney LB, et al. Agitation duringprocedural sedation and analgesia in children. Clin Pediatr2010;49:35-42.