9 Analgesia and Sedation in Mechanical Stoltenberg
25
Lecture 9 Feb 27, 2018 ©AllinaHealthSystem 1 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE • Nothing to disclose
Transcript of 9 Analgesia and Sedation in Mechanical Stoltenberg

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 1
ANALGESIA AND SEDATION IN MECHANICAL VENTILATIONErik Stoltenberg, MDAbbott Northwestern Hospital
February 27, 2018
DISCLOSURE
• Nothing to disclose

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 2
OBJECTIVE
To apply knowledge of the pharmacology of analgesics and sedatives to better care for patients requiring mechanical
ventilation to decrease the duration of mechanical ventilation and improve patient survival.
Case: 55 year old man with sepsis from pneumonia –traditional management• Past Medical History
• Smoking
• Diabetes
• On multiple neuroactive home medications (citalopram, PRN hydrocodone-acetaminophen, trazodone)
• ED Course• Initial VBG pH 7.15 pCO2 55mmHg HCO3 19mEq/L, placed on BiPAP
• CVC placed, given 8L IV crystalloid, ceftraixone
• ICU Course• Arrives to ICU, RR has increased to 40, FiO2 100%, intubated
• Intensivist writes sedation orders (morphine gtt, lorazepam gtt), no clear RASS goal
• Continues on morphine 4mg/h and lorazepam 2mg/hour

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 3
Case: 55 year old man with sepsis from pneumonia –traditional management• ICU Day 2:
• ABG is pH 7.33 pCO2 45mmHg O2 70mmHg HCO3 24 mEq/L, patient is occasionally breathing over the set ventilator rate and is occasionally “dyssynchronous” with the ventilator
• Physician determines patient is “not ready yet” and continues morphine and lorazepaminfusions at 4mg/h and 2mg/h
• ICU Day 3: • ABG improved to normal, infusions are decreased (but not stopped)
• ICU Day 5: • Patient wakes enough to follow commands intermittently, but is confused, clonazepam per
feeding tube is started for “benzodiazepine withdrawal”
• ICU Day 6: • Despite confusion, spontaneous breathing trial (SBT) is attempted and patient fails
Case: 55 year old man with sepsis from pneumonia –traditional management• ICU Day 7:
• Sedation infusions changed to intermittent dosing
• Patient passes a spontaneous breathing trial and is extubated
• Continued to struggle with delirium
• ICU Day 9:• Eventually able to transfer to acute care floor, weaning clonazepam
Lecture 9 Feb 27, 2018
©AllinaHealthSystem 4
Outline
• PAD Framework• Pain analgesia
• Agitation sedation
• Delirium numerous strategies
• Sedation pharmacology
• Selected evidence to support a different sedation paradigm
• Recommended strategy within PAD Framework
Purpose of analgesia and sedation in the ICU
• To…• Reduce discomfort
• Increase tolerance of intubation and mechanical ventilation
• Prevent accidental removal of instrumentation
• Decrease metabolic demands during cardiorespiratory instability
• NOT to• Provide sleep
• Decrease unpleasant memories
• Avoid/treat tachypnea
• Decrease nursing workload*

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 5
Pain in the ICU
• Common – the majority of ICU patients have pain• Post-cardiac surgery, women experience more pain then men
• Negative patient-centered effects• Significant source of stress (sometimes the MOST significant source)
• Can increase risk of PTSD
• Decrease quality of life of ICU survivors
• Can lead to chronic pain
• Negative physiologic effects• Increase plasma catecholamine levels
• Increase myocardial oxygen demand
• Increase oxygen consumption
• Increase vasoconstriction
Objective Pain Assessments (CPOT)

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 6
Objective Pain Assessments (BPS)
Multi-modal Analgesia

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 7
OpioidsOpioid IV dose
(mg)PO dose
(mg)Time to
Peak effectDuration of effect
Infusion rate Elimination half life
Notes
Morphine 5 15 30 min (IV) 3-4 h 2-30 mg/h 1.5-2 h Histamine release may be important from a cardiovascular and pulmonary perspective. Caution in renal failure.
Hydromorphone 0.7 4 30 min (IV) 4-5 h 0.5-3 mg/h 2-3 h Accumulation with hepatic dysfunction.
Fentanyl 0.05 N/A <5 min 30-60 min 25-300+ mcg/hr
3-4 h Significant increase in context-sensitive half-time with infusions >12h.
Remifentanil N/A N/A <3 min <10 min 0.05-0.3 mcg/kg/hr
10-20 min Abrupt discontinuation of analgesia.
Oxycodone N/A 10 <1h 3-4 h N/A 3-4 h Oxycodone is a prodrug
Methadone (variable) 10-20 min (IV), 30-60 min (PO)
3-6 h (longer with repeat dosing)
N/A 8-59 h NMDA receptor-antagonist, unpredictable pharmacokinetics (risk for accumulation). Multiple drug-drug interactions. Can prolong qtc
Context-Sensitive half time
https://www.e-jnc.org/journal/Figure.php?xn=jnc-8-2-53.xml&id=f1-jnc-8-2-53&number=199&p_name=0333_199

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 8
Analgesic Adjunct MedicationsDrug IV or PO dose Half-life Metabolism Notes
Ketamine IV: 0.1-0.5mg/kg bolus, then 0.05-0.4mg/kg/hr
2-3h CYP450: 2B6, 2C9, 3A4, urinary excretion
Attenuates opioid-induced hyperalgesia, may decrease persistent postoperative pain
Acetaminophen IV/PO: 650-1000 mg q4-6 h (<4000 mg per day)
2-4 h CYP450: 1A2, 2E1, urinary excretion
Use caution in hepatic impairment
Ketorolac IV: 15-30 mg q6 h up to 5 days 2.4-8.6 h CYP450. Less than 50% metabolized. 90% excreted in the urine, 6% in bile/ feces
Avoid use in patients with aspirin allergy. Caution with renal dysfunction, patients at high risk for bleeding, and in elderly patients.
Ibuprofen PO: 400 mg q 4 h 1.8-2.5 h CYP450: 2C9, urinary excretion Same caution as with ketorolac, IV formulation also available.
Gabapentin PO: 100 mg TID, can titrate up to maximum dose 1800 mg/day
5-7 h Minimal. Excreted intact in urine.
May cause sedation. Abrupt discontinuation may cause seizures.
Pregabalin PO: 50 mg TID, may increase to 100mg TID
5.5-6.7 h Minimal metabolism (2%). Renally excreted.
Lidocaine IV: 1.5 mg/kg loading dose, 1-2 mg/kg/h
1.5-2 h Hepatic CYP450 (1A2 and 3A4), 10% unchanged in the urine
Active metabolites may accumulate in hepatic or renal failure
Principles of Sedation
• The first step in treatment of agitation – assess the cause• Pain, delirium, hypoxemia, hypoglycemia, hypotension, withdrawal from substances
• Use an objective scale
• Use non-pharmacologic methods first• Analgesia, re-orientation, re-positioning, normalize sleep
• Choice of sedative is extremely important• Myth: doses of sedation infusions are constant for each patient over time

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 9
Richmond Agitation Sedation Scale (RASS)
Benzodiazepines
• Pharmacodynamics via GABAAreceptors in the brain• Anxiolysis• Sedation• Hypnosis• Anticonvulsant effect• Paradoxical agitation in elderly
• Midazolam Pharmacokinetics• Long and variable context-sensitive
half-time (especially in elderly)• Hepatic metabolism: caution in liver
dysfunction and with cP450 inhibitors (common)

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 10
Benzodiazepines Myths
• Myth: BZDs protect patients from bad memories
• Myth: BZD sedation is required in all patients in the ICU
Propofol• Pharmacodynamics unknown! (probably
GABAA)• Sedation• Hypnosis• Amnesia• Anticonvulsant• Anti-emetic • no analgesia!
• Adverse effects• Hypotension
• Vasodilation and myocardial depression
• Potentially allergenic• Egg (lecithin)• Soybean oil
• Propofol Infusion Syndrome (PRIS)• Hypertriglycerideemia, rhabdomyolysis, ECG changes,
cardiovascular collapse
Lecture 9 Feb 27, 2018
©AllinaHealthSystem 11
Dexmedetomidine (Precedex)• Unique pharmacodynamics
• α2 adrenergic receptor agonist• Similar to clonidine, but 8x more specific for CNS• Decreases sympathetic tone• Mild analgesia
• Potentially ideal ICU sedative• Light sedation (with apparent ceiling)• Minimal respiratory depression• FDA approved at doses up to 0.7 μg/kg/hr for
24h• Compared with other sedatives, decreased
ventilator days• Adverse effects
• Hypotension (at rates similar to propofol!)• Bradycardia (asystole with bolus dosing)• Withdrawal can be a problem (little literature on
this)
Chen K, Lu Z, Xin YC, Cai Y, Chen Y, Pan SM. Alpha-2 agonists for long-term sedation during mechanical ventilationin critically ill patients. Cochrane Database of Systematic Reviews 2015, Issue 1. Art. No.: CD010269. DOI: 10.1002/14651858.CD010269.pub2.
Ketamine
• N-methyl D-asparate (NMDA) antagonist
• Historically a dissociative anesthetic
• Only analgesic effects at low doses
• Can avoid “chronicization” of pain• Adverse effects
• Tachycardia, hypertension• Salivation• Hallucinations

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 12
Sedation OptionsDrug IV Loading
DoseInfusion rate
Time to Onset Elimination Half-life*
Active Metabolites
Notes
Midazolam 0.01-0.05 mg/kg
0.02-0.1 mg/kg/hr
2-5 min 1.7-2.6 h Yes (α-hydroxy-midazolam and conjugated α-hydroxy-midazolam)
Active metabolites especially important in renal failure; adverse effects – hypotension, respiratory depression
Lorazepam 0.02-0.04 mg/kg
0.01-0.1 mg/kg/hr
15-20 min 11-22 h No Propylene glycol (carrier solution) can cause acidosis; adverse effects – hypotension, respiratory depression
Propofol 0.1-0.3 mg/kg
5-50 μg/kg/min
1-3 min 4-23 h No Soybean oil and lecithin carrier (avoid with egg allergy) Adverse effects: hypotension, respiratory depression, propofol-related infusion syndrome (PRIS), pain on injection, hypertriglyceridemia, pancreatitis
Dexmedetomidine 1 μg/kg over 10 min
0.2-0.7 μg/kg/hr
5-10 min 1.8-3.1 h No Adverse effects – bradycardia and hypotension, hypertension with loading dose; difficult to achieve deep sedation
Context-Sensitive half time
https://www.e-jnc.org/journal/Figure.php?xn=jnc-8-2-53.xml&id=f1-jnc-8-2-53&number=199&p_name=0333_199
Lecture 9 Feb 27, 2018
©AllinaHealthSystem 13
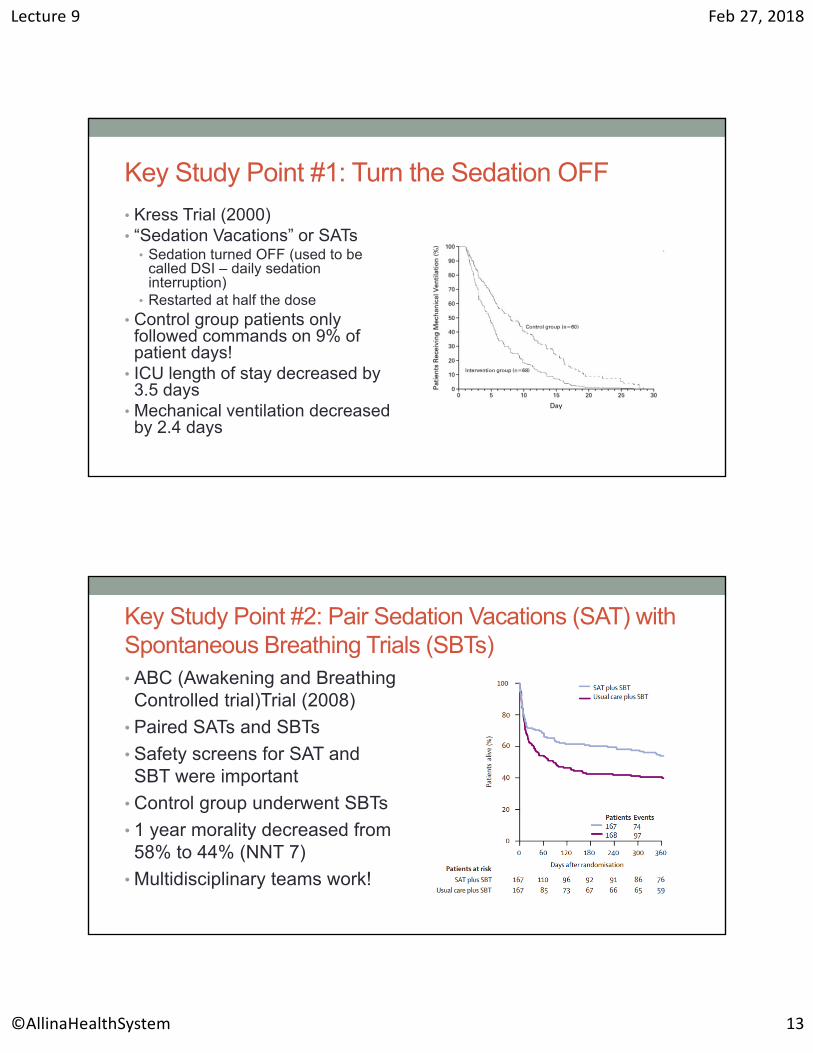
Key Study Point #1: Turn the Sedation OFF
• Kress Trial (2000)• “Sedation Vacations” or SATs
• Sedation turned OFF (used to be called DSI – daily sedation interruption)
• Restarted at half the dose• Control group patients only followed commands on 9% of patient days!
• ICU length of stay decreased by 3.5 days
• Mechanical ventilation decreased by 2.4 days
Key Study Point #2: Pair Sedation Vacations (SAT) with Spontaneous Breathing Trials (SBTs)• ABC (Awakening and Breathing Controlled trial)Trial (2008)
• Paired SATs and SBTs
• Safety screens for SAT and SBT were important
• Control group underwent SBTs
• 1 year morality decreased from 58% to 44% (NNT 7)
• Multidisciplinary teams work!

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 14
Key Study Point #3: Lighter Sedation is Safe, and May be Equal to Sedation Vacations (SATs)• Light vs. deep sedation (2010)• Goal RASS 0 to -3• Similar ICU LOS• Similar self-extubation rate• Similar delirium rate• Daily sedation interruption increased:1. Total midazolam dose2. Total fentanyl dose3. Sense of nursing workload
Key Study Point #4: PRN Opioids Alone can be OK
• Protocol:• PRN morphine IV + 1:1 sitter
• Restraints were never used
• PRN haloperidol for delirium
• Results• 4 fewer days with mechanical
ventilation
• No differences in accidental extubation

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 15
Studies are well and good, but this is reality in the ICU, and…
…physicians need nurses’ help!
Lecture 9 Feb 27, 2018
©AllinaHealthSystem 16
Selected Sedation Myths
Myth: But our patients aren’t deeply sedated!
“…many intensive-care practitioners have the perception that their patients are not oversedated, even though observational studies in Europe and the US found that nearly half of intensive-care patients are deeply sedated and unarousable.”
Girard, T. D. et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet 371, 126–134 (2008).
Myth: lighter sedation leads to more re-intubations
• Although in one study it increased risk of self-extubation
In summary, lighter sedation…
• Decreased ICU LOS• Decreased ventilator time• Decreased disturbing memories
• Decreased PTSD• Decreased nursing workload (compared to daily sedation interruptions)
• Decreased mortality (when paired with SAT/SBT)

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 17
Delirium Assessment and Management
• Delirium definition: • “syndrome with acute onset…change
in baseline mental status, inattention, disorganized thinking and/or altered level of consciousness.”
• Hallucinations and delusions are not required
• Affects up to 80% of patients with mechanical ventilation
• Overall Management:• Predict• Prevent• Detect• Treat
• Use a validated screening tool• Intensive Care Delirium Screen
Checklist (ICDSC)• Confusion Assessment Method for
ICU (CAM-ICU)• Non-pharmacologic methods• Risks
• Age• Benzodiazepines (lorazepam)
• Consequences• 3x higher mortality• Longer mechanical ventilation time
Delirium Risks

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 18
Delirium is Frustrating
• There are no well-validated treatments to reduce the duration of delirium
• Quetiapine may reduce duration, but it was in one small study (36 patients)
• There is severe, but rare, risk with antipsychotic medications
• Antipsychotic medications are therefore not recommend to prevent delirium
Synthesizing Sedation into Modern Critical Care: ABCDEF

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 19
ABCDEF
• Result from PAD Guidelines (Barr 2013)
• Recommended sedation strategies instead of agents
• After implementation of this ABCDEF bundle, mortality decreased approximately 10% for each bundle element followed
Lecture 9 Feb 27, 2018
©AllinaHealthSystem 20
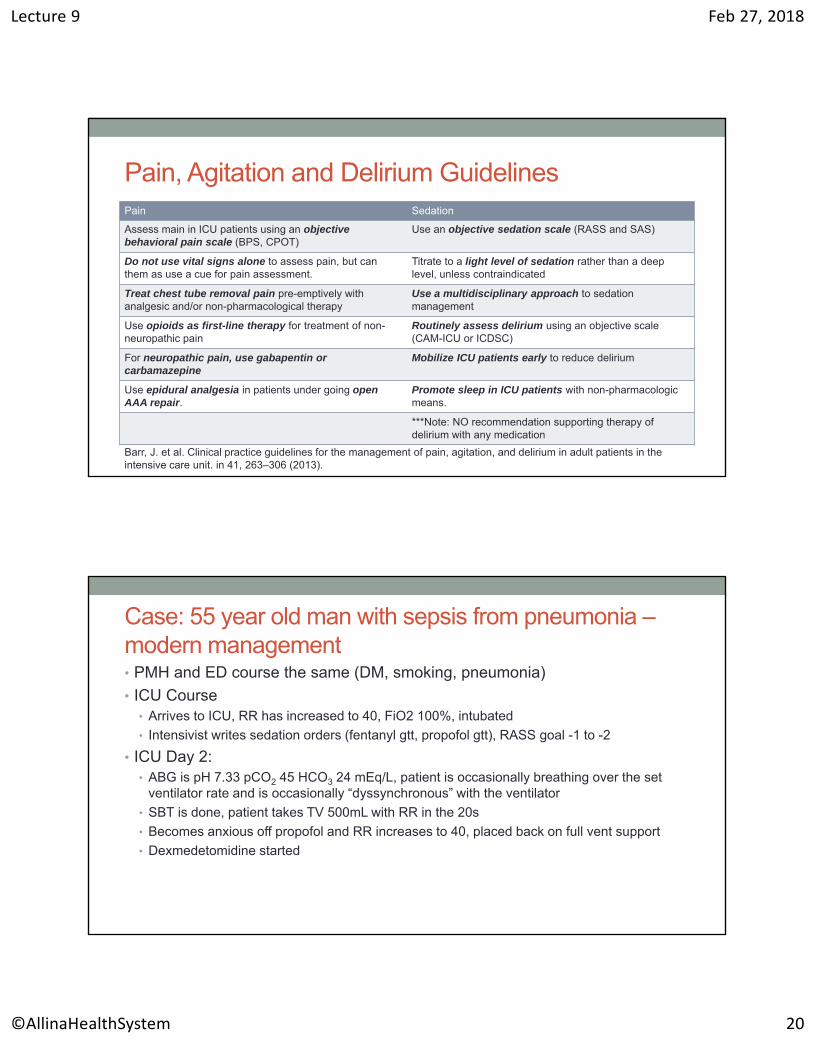
Pain, Agitation and Delirium GuidelinesPain Sedation
Assess main in ICU patients using an objectivebehavioral pain scale (BPS, CPOT)
Use an objective sedation scale (RASS and SAS)
Do not use vital signs alone to assess pain, but can them as use a cue for pain assessment.
Titrate to a light level of sedation rather than a deep level, unless contraindicated
Treat chest tube removal pain pre-emptively with analgesic and/or non-pharmacological therapy
Use a multidisciplinary approach to sedation management
Use opioids as first-line therapy for treatment of non-neuropathic pain
Routinely assess delirium using an objective scale (CAM-ICU or ICDSC)
For neuropathic pain, use gabapentin or carbamazepine
Mobilize ICU patients early to reduce delirium
Use epidural analgesia in patients under going open AAA repair.
Promote sleep in ICU patients with non-pharmacologic means.
***Note: NO recommendation supporting therapy of delirium with any medication
Barr, J. et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. in 41, 263–306 (2013).
Case: 55 year old man with sepsis from pneumonia –modern management• PMH and ED course the same (DM, smoking, pneumonia)
• ICU Course• Arrives to ICU, RR has increased to 40, FiO2 100%, intubated
• Intensivist writes sedation orders (fentanyl gtt, propofol gtt), RASS goal -1 to -2
• ICU Day 2: • ABG is pH 7.33 pCO2 45 HCO3 24 mEq/L, patient is occasionally breathing over the set
ventilator rate and is occasionally “dyssynchronous” with the ventilator
• SBT is done, patient takes TV 500mL with RR in the 20s
• Becomes anxious off propofol and RR increases to 40, placed back on full vent support
• Dexmedetomidine started

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 21
Case: 55 year old man with sepsis from pneumonia –modern management• ICU Day 3:
• Repeat SBT in the morning on dexmedetomidine results in patient with RASS -1, is not anxious with SBT, and is extubated
• ICU Day 4:• Transferred to the acute care floor.
Effect of Improving Sedation Practices:Victims of our own success• Paradigm shifts in ICU care –especially sedation – have significantly improved patient outcomes
• This has resulted in numerous “negative trials” This lack of difference can be explained by “lower-than-expected mortality,” a phenomenon we can all be proud of
Trial Expected Mortality
Observed Mortality
ProCESS 30-46% 18.9%
ARISE 38% 18.8%
ProMISe 40% 30%

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 22
More Multidisciplinary Victories…
• Infection• Sepsis bundles
• VAP Bundles
• Antibiotic Stewardship
• CVC Bundles
• Nutrition• Early Enteral nutrition
• Enteral over TPN
• Mechanical Ventilation• SAT/SBT
• NIPPV
• Monitoring• Less reliance on invasive catheters
• Others• Increased intensivist staffing
• More restrictive blood product management
• Early rehabilitation/mobility
• Lighter Sedation
• Appropriate DVT prophylaxis
• Checklists
• Multidisciplinary Practice
Myths, compiled
• Benzodiazepine sedation is required in the ICU
• Deep sedation protects patients from bad memories
• Doses of sedation infusions are constant for each patient
• Lighter sedation increases nursing workload
• Lighter sedation leads to more re-intubations

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 23
Pearls, compiled
• Many patients in the ICU have pain which requires treatment
• Context-sensitive half time = drug infusions build up
• Sedation is directly related to mechanical ventilation• The primary reason for sedation is for mechanical ventilation tolerance
• Pair sedation strategy (or sedation vacations) with SBTs
• Light sedation without sedation vacations is probably equal to light sedation with sedation vacations (and decreases nurses’ sense of workload)
• In selected ICU patients with appropriate staffing, opioid-only “sedation” may be safe and desirable
Summary
• Appropriate sedation techniques saves lives!
• Objective assessments are required to individualize treatment
• Use an analgesia-first approach
• Remember the context-sensitive half-time
• Optimal PAD care requires multidisciplinary teamwork• Nurses, physicians, CNSs, NPs, RTs, PT, OT, SLP, rehab physicians
• Nurses are the tip of the spear
• Nurses input should always be welcome (and is essential)
• Appropriate treatment of PAD is arguably the most important work we can do!

Lecture 9 Feb 27, 2018
©AllinaHealthSystem 24
REFERENCESBarr, J. et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. in 41, 263–306 (2013).Sessler, C. N. et al. The Richmond Agitation–Sedation Scale. Am J Respir Crit Care Med 166, 1338–1344 (2012).Ely, J. et al. Monitoring Sedation Status Over Time in ICU Patients: Reliability and Validity of the Richmond Agitation-Sedation Scale (RASS). JAMA. 289, 2983–2991 (2003).Stoltenberg, E. et al. Analgesia, Sedation, and Neuromuscular Blockade in Critical Care / John M. Oropello, Stephen M. Pastores, Vladimir Kvetan, editors. McGraw Hill Medical (2017).Strøm, T., Martinussen, T. & Toft, P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet 375, 475–480 (2010).Pandharipande, P. et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 104, 21–26 (2006).Girard, T. D. et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet 371, 126–134 (2008).
REFERENCESMehta, S. et al. Daily sedation interruption in mechanically ventilated critically ill patients cared for with a sedation protocol: a randomized controlled trial. JAMA: The Journal of the American Medical Association 308, 1985–1992 (2012).Treggiari, M. M. et al. Randomized trial of light versus deep sedation on mental health after critical illness. Critical Care Medicine 37, 2527–2534 (2009).Jakob, S. M. et al. Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA: The Journal of the American Medical Association 307, 1151–1160 (2012).Barnes-Daly, M. A., Phillips, G. & Ely, E. W. Improving Hospital Survival and Reducing Brain Dysfunction at Seven California Community Hospitals: Implementing PAD Guidelines Via the ABCDEF Bundle in 6,064 Patients. Critical Care Medicine 45, 171–178 (2017).Kress, J. P., Pohlman, A. S., O'Connor, M. F. & Hall, J. B. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med 342, 1471–1477 (2000).Pun, B. T., Balas, M. C. & Davidson, J. Implementing the 2013 PAD guidelines: top ten points to consider. Semin Respir Crit Care Med 34, 223–235 (2013).PRISM Investigators. Early, Goal-Directed Therapy for Septic Shock - A Patient-Level Meta-Analysis. N Engl J Med 376, 2223–2234 (2017).