Syncope Wm. W. Barrington MD FACC Wm. W. Barrington MD FACC Associate Professor of Medicine...
29
Syncope Syncope Wm. W. Barrington MD FACC Wm. W. Barrington MD FACC Associate Professor of Associate Professor of Medicine Medicine University of Pittsburgh University of Pittsburgh Medical Center Medical Center aACC Fellows in Training Program May 2008
-
Upload
kelsie-mercier -
Category
Documents
-
view
216 -
download
0
Transcript of Syncope Wm. W. Barrington MD FACC Wm. W. Barrington MD FACC Associate Professor of Medicine...

SyncopeSyncope Wm. W. Barrington MD FACCWm. W. Barrington MD FACC
Associate Professor of MedicineAssociate Professor of Medicine
University of Pittsburgh Medical CenterUniversity of Pittsburgh Medical Center
PaACC Fellows in Training Program May 2008

What is syncope?What is syncope?Sudden, temporary loss of consciousness Sudden, temporary loss of consciousness
associated with the inability to maintain associated with the inability to maintain postural tone, followed by spontaneous postural tone, followed by spontaneous recoveryrecovery..
Also referred to as:Also referred to as:• ““Fainting” Fainting” • ““Passing out”Passing out”

SyncopeSyncope
• Affects 1 million Americans each year. Affects 1 million Americans each year. (1)(1)
• Accounts for 3% of ED visits and 6% of Accounts for 3% of ED visits and 6% of hospital admissions. hospital admissions. (1)(1)
• Prevalence of syncope in general population Prevalence of syncope in general population is between 15% and 40%. is between 15% and 40%. (2)(2)
• 39% of medical students have “passed out” at 39% of medical students have “passed out” at least once. least once. (2)(2)
1. Shukla GJ and Zimetbaum PJ Circulation (2006) 113; 715-172. Sheldon RS, Sheldon AG, Connolly SJ et al J Cardiovasculatr Electrophysiology (2006) 17 ;49-54.
Significant Medical ProblemSignificant Medical Problem
EtiologyEtiology
SyncopeSyncope
Cardiac NonCardiac Unknown

EtiologyEtiology
CardiacCardiac• BradycardiaBradycardia• TachycardiaTachycardia• Aortic StenosisAortic Stenosis• Aortic dissectionAortic dissection• Hypertrophic Hypertrophic
cardiomyopathycardiomyopathy• Long QT SyndromeLong QT Syndrome
UnknownUnknown• ? Unknown? UnknownWe will focus today We will focus today
on the noncardiac on the noncardiac causes of syncope.causes of syncope.

Etiology Etiology (3)(3)
NonCardiac
Reflex Syncope
POTSAutonomic
Failure
3. Grubb B Circulation (2005) 111;2997-3006
X

Reflex syncope is a sudden failure of the autonomic nervous system (ANS) to maintain adequate vascular tone during orthostatic stress

Reflex syncope
Neurocardiogenic SituationalCarotid
Hypersensitivity

Neurocardiogenic Neurocardiogenic SyncopeSyncope
• Typically occurs in younger patients Typically occurs in younger patients and has and has 3 distinct phases:3 distinct phases:• Prodrome of lightheadedness, Prodrome of lightheadedness,
diaphoresis, diaphoresis, nauseanausea• Sudden loss of consciousness (LOC)Sudden loss of consciousness (LOC)• Rapid recoveryRapid recovery
• In older patients, prodromal In older patients, prodromal symptoms less symptoms less common, but LOC common, but LOC still suddenstill sudden
Neurocardiogenic Neurocardiogenic SyncopeSyncope
• A comprehensive history and physical is the most important aspect of the evaluation
• Supine, sitting and upright blood pressures may be helpful
• Head up Tilt Table (HUTT) testing is often employed to confirm or establish the diagnosis
Evaluation of Neurocardiogenic Syncope

Neurocardiogenic Neurocardiogenic SyncopeSyncope
• 60° to 70° HUTT removes the effect of 60° to 70° HUTT removes the effect of the lower extremity “muscle pump”the lower extremity “muscle pump”
• Consciousness is thus maintained by Consciousness is thus maintained by appropriate interaction of the appropriate interaction of the sympathetic and parasympathetic limbs sympathetic and parasympathetic limbs
of the ANSof the ANS
Head up Tilt Table (HUTT) testingHead up Tilt Table (HUTT) testing is a is a method of examining the effect method of examining the effect of the of the autonomic autonomic nervous system nervous system on heart rate on heart rate and BPand BP

Neurocardiogenic Neurocardiogenic SyncopeSyncope
• Specificity 90% (without provocation) Specificity 90% (without provocation)
• Short term reproducibility is 80% to Short term reproducibility is 80% to 90%90%
• Individuals with NCS demonstrate a Individuals with NCS demonstrate a “sudden” drop in BP that is frequently “sudden” drop in BP that is frequently followed by a drop in heart ratefollowed by a drop in heart rate
• Commonly, we see one of 3 abnormal Commonly, we see one of 3 abnormal responsesresponses
Head up Tilt Table (HUTT) testingHead up Tilt Table (HUTT) testing

Vasodepressor Response

12.4 seconds
Continuous recording
Syncope
After 15 minutes of HUTT testing
60 bpm 30 bpm
18 bpm

Mixed Vasodepressor/Cardioinhibitory Response
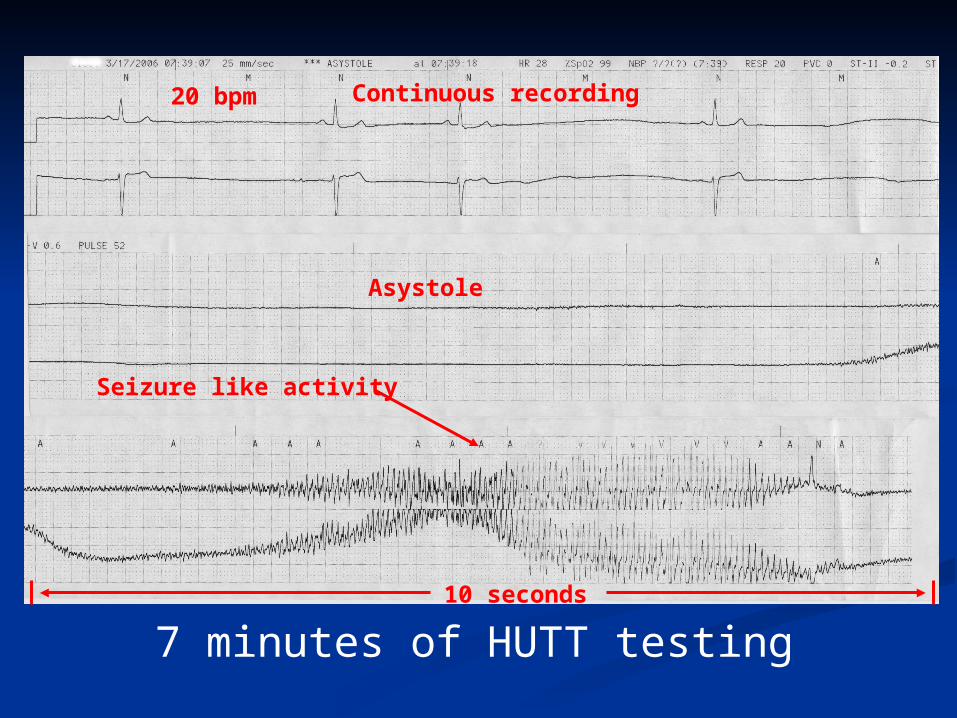
10 seconds
Continuous recording
Seizure like activity
7 minutes of HUTT testing
20 bpm
Asystole

Cardioinhibitory Response

Situational SyncopeSituational Syncope• Syncope that occurs under a specific Syncope that occurs under a specific
set of set of circumstances:circumstances:• MicturitionMicturition• DefecationDefecation• CoughCough
• Patients are typically free of Patients are typically free of symptoms at other symptoms at other timestimes
• Sudden activation of Sudden activation of mechanoreceptors at an mechanoreceptors at an affected affected “site” may activate the ANS leading “site” may activate the ANS leading
to hemodynamic collapseto hemodynamic collapse

Carotid Sinus Carotid Sinus HypersensitivityHypersensitivity
• Pressure on the carotid sinus is Pressure on the carotid sinus is thought to thought to “mimic” hypertension “mimic” hypertension leading to bradycardialeading to bradycardia
• The symptoms are very similar to The symptoms are very similar to those seen those seen with NCSwith NCS
Postural Orthostatic Postural Orthostatic Tachycardia Syncope Tachycardia Syncope
(POTS)(POTS)• Hallmark of syndrome is Hallmark of syndrome is
persistent persistent tachycardia while tachycardia while uprightupright
• Severe fatigueSevere fatigue• Exercise intoleranceExercise intolerance• PalpitationsPalpitations• Syncope and near syncopeSyncope and near syncope

Postural Orthostatic Postural Orthostatic Tachycardia Syncope Tachycardia Syncope
(POTS)(POTS)• Pathophysiology appears to be Pathophysiology appears to be
failure of failure of peripheral vascular peripheral vascular resistance to resistance to increase in the increase in the face of orthostatic stress, face of orthostatic stress, thus the thus the heart rate and inotropic state heart rate and inotropic state increase to compensate.increase to compensate.
• Tilt Table TestingTilt Table Testing• >30 bpm increase in heart rate>30 bpm increase in heart rate• Heart increases to > 120 bpm Heart increases to > 120 bpm (in first 10 minutes)(in first 10 minutes)

POTS Response

Therapeutic ApproachTherapeutic Approach
• Avoid precipitating circumstancesAvoid precipitating circumstances• DehydrationDehydration• Extreme heatExtreme heat
• Increase Fluid intake (possibly salt)Increase Fluid intake (possibly salt)• Lay or sit down when prodromal Lay or sit down when prodromal
symptoms symptoms beginbegin• Encourage moderate aerobic and Encourage moderate aerobic and
isometric isometric exerciseexercise
Therapeutic ApproachTherapeutic Approach
• Tilt table training may be helpfulTilt table training may be helpful• Elastic support hose (effective if waist Elastic support hose (effective if waist
high high and provide >30 mm Hg ankle and provide >30 mm Hg ankle pressure) pressure)
• Elevation of head of bedElevation of head of bed• Isometric “counter maneuvers” such as Isometric “counter maneuvers” such as
leg or leg or arm tensing may abort episodes arm tensing may abort episodes that are that are detected early.detected early.
• Many individuals finally need Many individuals finally need pharmacotherapypharmacotherapy

From Grubb B Circulation (2005) 111;2997-3006

Beta blockersDisopyramide
Fluids/saltStockingsFludrocortisone
Anticholenergics
Selective serotoninRe-uptake inhibitors
Midodrine

Therapeutic ApproachTherapeutic Approach
• Early studies showed single chamber VVI Early studies showed single chamber VVI pacing was ineffective.pacing was ineffective.
• Original, non-blinded studies showed a Original, non-blinded studies showed a benefit benefit with dual chamber pacingwith dual chamber pacing
• Two recent randomized, blinded studies Two recent randomized, blinded studies failed failed to show a benefit with pacingto show a benefit with pacing
• Vasovagal Pacemaker Study (VPS) II Vasovagal Pacemaker Study (VPS) II (4)(4)
• Vasovagal Syncope and Pacing Trial Vasovagal Syncope and Pacing Trial (5)(5)
Is there a role for cardiac pacing?
4. Connolly sj et al JAMA (2003) 289;2224-9 5.Raviele A et al European Heart Journal (2004)25;1741-48

Therapeutic ApproachTherapeutic Approach
• In patients with recurrent syncope In patients with recurrent syncope where no where no other therapy is other therapy is effective, pacing may have a effective, pacing may have a role role in reducing the frequency of in reducing the frequency of syncope or syncope or prolonging the time prolonging the time from onset of from onset of symptoms to frank symptoms to frank syncope, allowing the syncope, allowing the patient to patient to avoid injury.avoid injury.
Cardiac pacing is not routinely first line therapy.

Thank you for your Thank you for your attention.attention.
I would be happy to take I would be happy to take any questions.any questions.