Symptoms Gradient Besides left - hcmny.org for Left Ventricular...showing left ventricular outflow...
13
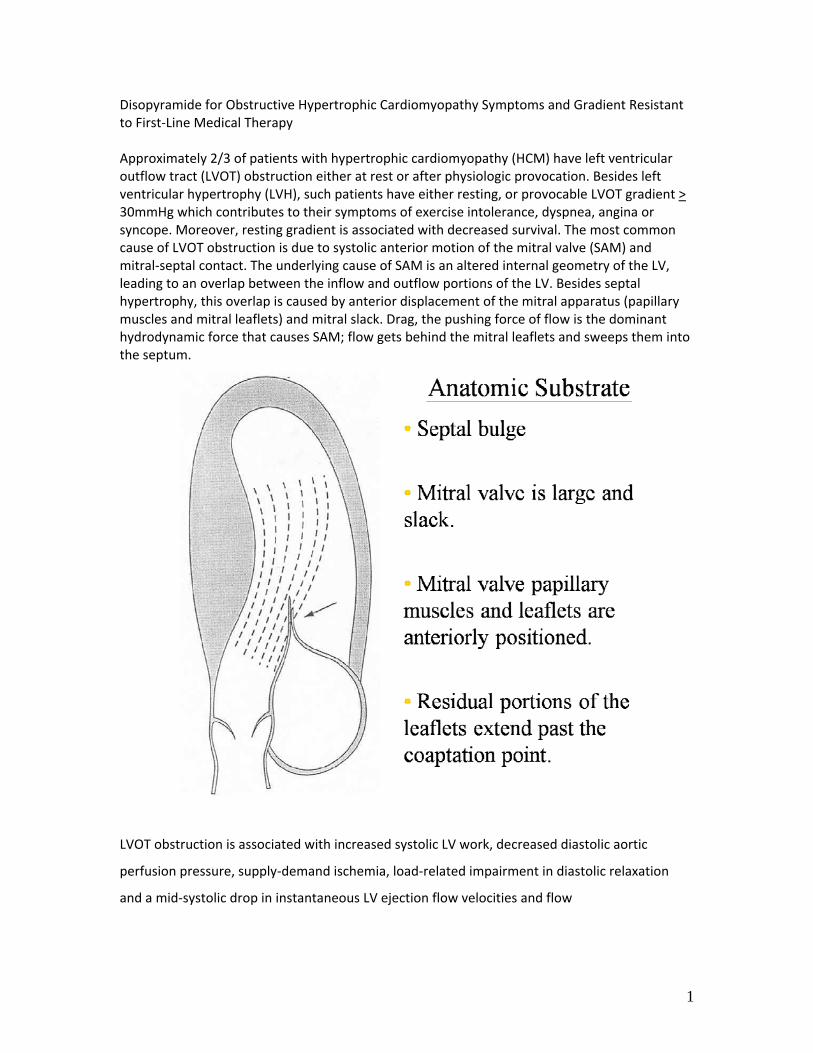
1 Disopyramide for Obstructive Hypertrophic Cardiomyopathy Symptoms and Gradient Resistant to First‐Line Medical Therapy Approximately 2/3 of patients with hypertrophic cardiomyopathy (HCM) have left ventricular outflow tract (LVOT) obstruction either at rest or after physiologic provocation. Besides left ventricular hypertrophy (LVH), such patients have either resting, or provocable LVOT gradient > 30mmHg which contributes to their symptoms of exercise intolerance, dyspnea, angina or syncope. Moreover, resting gradient is associated with decreased survival. The most common cause of LVOT obstruction is due to systolic anterior motion of the mitral valve (SAM) and mitral‐septal contact. The underlying cause of SAM is an altered internal geometry of the LV, leading to an overlap between the inflow and outflow portions of the LV. Besides septal hypertrophy, this overlap is caused by anterior displacement of the mitral apparatus (papillary muscles and mitral leaflets) and mitral slack. Drag, the pushing force of flow is the dominant hydrodynamic force that causes SAM; flow gets behind the mitral leaflets and sweeps them into the septum. LVOT obstruction is associated with increased systolic LV work, decreased diastolic aortic perfusion pressure, supply‐demand ischemia, load‐related impairment in diastolic relaxation and a mid‐systolic drop in instantaneous LV ejection flow velocities and flow
Transcript of Symptoms Gradient Besides left - hcmny.org for Left Ventricular...showing left ventricular outflow...
1
Disopyramide for Obstructive Hypertrophic Cardiomyopathy Symptoms and Gradient Resistant to First‐Line Medical Therapy Approximately 2/3 of patients with hypertrophic cardiomyopathy (HCM) have left ventricular outflow tract (LVOT) obstruction either at rest or after physiologic provocation. Besides left ventricular hypertrophy (LVH), such patients have either resting, or provocable LVOT gradient > 30mmHg which contributes to their symptoms of exercise intolerance, dyspnea, angina or syncope. Moreover, resting gradient is associated with decreased survival. The most common cause of LVOT obstruction is due to systolic anterior motion of the mitral valve (SAM) and mitral‐septal contact. The underlying cause of SAM is an altered internal geometry of the LV, leading to an overlap between the inflow and outflow portions of the LV. Besides septal hypertrophy, this overlap is caused by anterior displacement of the mitral apparatus (papillary muscles and mitral leaflets) and mitral slack. Drag, the pushing force of flow is the dominant hydrodynamic force that causes SAM; flow gets behind the mitral leaflets and sweeps them into the septum.
LVOT obstruction is associated with increased systolic LV work, decreased diastolic aortic
perfusion pressure, supply‐demand ischemia, load‐related impairment in diastolic relaxation
and a mid‐systolic drop in instantaneous LV ejection flow velocities and flow
2
A unique feature of obstructive HCM is the provocable gradient. Obstruction worsens
after physiologic stimuli that reduce preload and afterload and increase contractility such as
Valsalva maneuver, standing, after eating and particularly after exercise. Unfortunately, the
more widely used cardiac medications, such as ACE‐inhibitors, ARBs, vasodilators, and nitrates
are deleterious in exactly this way and increase gradient because of their vasodilatory
properties.
Vasodilatation exacerbates existing or latent obstruction. However, the provocable
increase in gradient provides a tantalizing prospect: would a pharmacologic reduction in
afterload decrease, or even abolish gradient? Preventing or delaying SAM and mitral‐septal
contact is the goal.
A general principle of HCM treatment is that patients are first given a trial of
pharmacotherapy before consideration of septal reduction therapy. All pharmacologic agents
for obstructive HCM are negative inotropes. These drugs decrease the hydrodynamic force on
the mitral leaflets early in systole delaying mitral‐septal contact and attenuating gradient. In
obstructive HCM there is a tug‐of‐war between the anterior displacing force of flow and the

3
restraint of the papillary muscles and chordae. Pharmacologic decrease of ejection acceleration
displaces the equilibrium point towards restraint. Another analogy: the mitral valve acts as an
open door in a windy corridor, snapping shut in a gusty breeze. Negative inotropes decrease
ejection acceleration ‐ gentling the breeze – slamming the door later, or allowing it to remain
open altogether. The first line of pharmacotherapy is beta‐blockade; but while such therapy
may improve symptoms and decrease exercise gradient, beta‐blockade is not expected to lower
resting gradients. We favor metoprolol, bisoprolol, or atenolol and avoid beta blockers with
vasodilatory properties, like labetalol, and carvedilol. While there is considerable experience
with verapamil, this agent has intrinsic vasodilatory activity and a lower negative inotropic effect
than either beta‐blockade or disopyramide. It may paradoxically increase gradient when its
vasodilatory properties outstrip its negative inotropic effect. In Espstein and Rosing’s paper
there were 7 deaths early after verapamil initiation, and they warned against its use in patients
suspected of having high left atrial pressure. However, these are exactly the sort of highly
symptomatic patients one would like to treat with pharmacotherapy. Investigators from Tokyo
have compared sequentially the gradient‐lowering effects of intravenous disopyramide, inderal
and verapamil. They found a 59% reduction with disopyramide, a 19% reduction with inderal
and only 8% reduction with verapamil.

4
Though there are no long term randomized trials, many investigators believe
disopyramide, given in combination with beta‐blockade, is the best pharmacologic therapy for
obstruction. If there is a contraindication to beta‐blockers, verapamil may be given with
disopyramide instead. We will discuss the process of initiating and maintaining therapy, and will
summarize our published experience.
Disopyramide in obstructive HCM
If patients are symptomatic after beta‐blockade we generally add disopyramide.
Disopyramide is a type I anti‐arrhythmic with potent negative inotropic effect, that was
introduced for use in HCM by investigators from Toronto showing efficacy of intravenous
disopyramide in the catheterization laboratory. Subsequent investigations demonstrated the
efficacy of oral disopyramide in the echocardiography laboratory.
A representative series of Doppler tracings performed on 1 patient over a period of 5 weeks,
showing left ventricular outflow tract flow before and after treatment with disopyramide. The
first 2 tracings are before treatment. The third tracing is 2.5 hours after the first oral dose of
300mg disopyramide. The fourth tracing is 3 weeks later, on maintenance oral disopyramide.
The fifth tracing is after drug washout, 72 hours after discontinuing disopyramide.
In a multicenter study of disopyramide from 4 institutions we found that 2/3 of patients
could be successfully managed without the need for septal reduction. In these patients resting
gradients were reduced by half with a concomitant relief of symptoms.

5
In contrast, 1/3 of patients needed intervention because they had persistent gradients
or drug side effects. Moreover, there was a trend toward better survival in disopyramide treated
patients. We believe this is because of lower gradients. Sudden death in the disopyramide
treated patients was very low, 1% per year.
In a more recent single center study of disopyramide in obstructive HCM we treated
>250 patients with disopyramide, usually in association with beta blockade. Average dose of
disopyramide was 500 mg/day. Again, drug therapy was successful in controlling symptoms in
2/3 of patients but was unsuccessful in a third. These patients were referred for surgical
myectomy. Sudden death rate or potentially lethal arrhythmias were very low, <0.5% /year.

6
Disopyramide is an antiarrhythmic and had been widely used for prevention of atrial fibrillation
in the 80’s and 90’s. As such, it is often selected to prevent atrial fibrillation in HCM. It also
frequently decreases symptomatic ventricular premature contractions or bursts of non‐
sustained ventricular tachycardia improving the quality of life of patients who may experience
palpitations. However, disopyramide alone cannot be recommended as sole protection against
sudden death. Patients may inadvertently skip doses, and protection will necessarily be inferior
to that provided by the implantable defibrillator (ICD). Thus, all patients with HCM obstructed or
not, should undergo formal risk stratification for sudden death. In patients where the benefits
appear to outweigh risks of the device, ICD should be discussed, recommended and implanted.
Initiation and maintenance
As a class I antiarrhythmic, there is a theoretic risk that disopyramide might induce
serious, proarrhythmic ventricular arrhythmia. This concern has been relieved by the
multicenter registry, previously described, where sudden death trended lower in the
disopyramide treated patients, and overall was quite low (1%/year). Though disopyramide has
been started in the outpatient setting for years in Canada and in London, we have initiated the
drug in the hospital. Generally, patients are admitted in the morning and undergo an

7
echocardiogram and EKG to establish baseline parameters. Pre‐admission labs are checked to
assure normal renal function and potassium. The optimum starting dose is disopyramide
controlled‐release 250 mg Q12H. In the United States this is given as Norpace CR 150 mg + 100
mg Q12H. In Europe a 250 mg single pill preparation is available for control release dosing. Two
studies have previously shown a dose‐response relationship for lowering gradient.
Consequently, at our institution we give higher doses now (500mg/day), than in the multicenter
efficacy registry (432mg/day). In certain cases, we now lower the starting dose to 200 mg Q12H
‐ for patients with mild renal failure, creatinine <=2.0 or for patients < 100 lbs weight. We
continue the beta blocker or verapamil with disopyramide but generally will not give all 3 drugs
together unless the patient has a permanent pacemaker as protection against heart block.
For the duration of the 3 day hospitalization the patient is monitored on telemetry, and
daily EKG’s are performed for checks of the QTc interval. Patients with ICDs may have a shorter,
24 hour, admission. Modest prolongation of the QTc interval is expected and is a marker that
drug effect is occurring. We continue regular dosing unless QTc interval of 525 msec is exceeded
in patients with a normal QRS complex, or a QTc interval of 550 msec in patients with an initially
wide initial QRS complex. In our experience in 230 patients, during disopyramide initiation no
ventricular tachycardia has occurred. However, one patient had complete heart block requiring
a permanent pacemaker. Routinely, on the third day of hospitalization, a follow‐up
echocardiogram is performed to ascertain effect of disopyramide. If the resting gradient is > 40
mm Hg the dose of disopyramide is up‐titrated to 300 mg Q12H. Not infrequently, a marked
reduction of systolic murmur may be appreciated by the third day of hospitalization. While short
acting disopyramide is also effective it is difficult for patients to comply to 3‐4x/day dosing. Also,
frequent peaks and valleys of drug levels do not contribute to stable and controlled
maintenance of symptom relief. Even with the controlled release preparation some patients
report a worsening of symptoms at the end of dose intervals. Virtually all will notice a difference
if they inadvertently skip a dose.
Follow‐up care begins with an office visit 3 weeks post‐initiation for EKG monitoring (see
QTc parameters above), symptom evaluation, and re‐discussion about benefits and side effects
(current and potential), and discussion of medications to avoid. As disopyramide may prolong
QT interval, other medications with QT prolongation potential should be strictly avoided, such as
other antiarrhymics, some antipsychotics, tricyclic antidepressants, erythromycins, and certain
quinolones for example. For a complete list one can check http://www.qtdrugs.org/. Most

8
important is to strictly avoid concomitant antiarrhythmic use with disopyramide (including
amiodarone and sotalol). From a practical point of view the greatest difficulty with drug
interactions centers on antibiotic use and avoiding the popular erythromycin class and certain
quinolones. We discuss with patients that penicillins, cephalosporins, tetracyclines, vancomycin,
and metronidazole are acceptable and permitted. On rare occasions disopyramide must be
stopped to allow antibiotic (transient hiatus) or other antiarrhythmic to be started (permanent
discontinuation). Such discontinuation is often marked by an increase in symptoms.
We perform an echocardiogram 3 months after drug initiation. EKG and clinical
response is monitored every 4 months. Disopyramide levels are not measured routinely but can
be useful in patients with mild renal failure or to confirm drug compliance, or adequate dosing
in a patient with symptoms. We uptitrate to 300 mg Q12H in patients who have suboptimal
response, and often will check a drug level first. Usually, the highest dose we will use is 300mg
PO Q12H of disopyramide CR.
Side effects of disopyramide
We avoid disopyramide in patients who have LV systolic dysfunction, though almost all
of these patients will have lost their obstruction concomitant with systolic dysfunction. The
efficacy of disopyramide cannot be based on gradient reduction alone. Symptom improvement
and occurrence of side effects must be considered to assess the impact of this intervention.
Disopyramide does not cause organ toxicity (except rarely) which makes it suitable for long‐term
use. However, bothersome side effects may occur due to anticholinergic vagolytic effects.
Disopyramide may cause dry mouth, constipation, urinary hesitancy and blurry vision. We do
not use disopyramide in patients who have significant prostatism symptoms, hesitancy or
dribbling, out of concern we might cause urinary retention or urinary infection. While vagolytic
side effects are generally transient and occur in the beginning of therapy, they may persist.
Intermittent blurred vision is generally a temporary condition. Dry mouth may persist and may
be alleviated with hydration, chewing gum, or using commercial mouth washes for dry mouth.
Constipation may be transient or if it persists may be addressed with use of supplemental bulk
in the diet. Urinary retention and prostatism are more significant reactions and in these cases
disopyramide may be decreased or even stopped.
Pyridostigmine is a well known cholinesterase inhibitor which thoroughly counteracts all
the vagolytic effects of disopyramide while preserving its therapeutic effects. It is marketed in
the US as Mestinon Timespan 180 mg and has been safely used for myasthenia for decades. Its

9
dosing is flexible and may be titrated to relieve disopyramide side effects. Dosing varies
anywhere from 90mg (1/2 tab) twice daily to 180mg twice daily. Care must be taken so that
pyridostigmine does not do its job too well, causing diarrhea or intestinal cramps.
The most dreaded side effect of disopyramide is torsades de pointes, drug induced
ventricular tachycardia. In over 230 cases treated we have had one episode of torsades de
pointes in an 83 year old female who, after 2 years on disopyramide for a 92 mm Hg resting
gradient and severe symptoms, developed torsades which was terminated by her implanted
defibrillator. The arrhythmia was precipitated by hypokalemia from a concurrent single episode
of prolonged diarrhea. After correcting hypokalemia the arrhythmia stopped. She has never had
diarrhea again and because of severe symptoms she requested disopyramide again. It was
restarted in the same dose with no recurrence of arrhythmia after 3 years.
Hypertension may occur in the initial period after drug initiation most prominently in
patients who have underlying hypertension in addition to their obstructive HCM. Hypertension
may be related to the sudden reduction in LVOT gradient. Over time blood pressure tends to
normalize. However, if hypertension persists, up‐titration of the patient’s other medications
(beta‐blockers or verapamil) may reduce pressure; or, clonidine may be introduced. Occasionally
low dose hydrochlorothiazide ‐ 12.5 mg plus triamterene is tolerated without increase in
gradient but only if disopyramide is administered as well. As mentioned above, ACEI, ARBs,
vasodilators, nitrates and the dihydropyridine calcium channel blockers are not an option in
obstructive HCM. Medium and high dose diuretics are also not acceptable options since they
decrease preload.
We have reported a synergistic effect of disopyramide and dual chamber pacing with
short atrioventricular delay for gradient reduction. We cannot recommend this as primary
therapy for gradient because of the unpredictable reduction in gradient with DDD pacing that
may occur from patient to patient. However, we have observed sustained benefit in many
patients and favor this approach in the elderly or frail patient with severe medical co‐morbidity.

10
Obstruction may occur elsewhere in the LV. Anomalous papillary muscle heads may
insert into the middle of the anterior mitral valve leaflet without intervening chordae and cause
obstruction. In these cases the papillary muscle itself may impact the septum causing
obstruction at the mid‐LV level; or, the anomalous muscle may elevate the mitral valve in the LV
chamber and thereby pre‐position the mitral valve anteriorly into the flow stream where it is
subject to drag and SAM. We have observed that such patients also may respond to
pharmacologic management.
Rarer still is mid‐LV obstruction. In these cases, the greatest degree of hypertrophy is in
the mid‐LV walls and obstruction occurs due to systolic apposition of the walls. Blood is trapped
in the apex, often causing a mid‐systolic cessation of flow. Such patients may develop an apical
akinetic chamber due to supply demand mismatch and afterload mismatch. Symptoms from this
variant of obstruction are the most difficult to manage in the HCM domain and beyond the
scope of this paper. There is a paucity of data about the utility of disopyramide in non‐
obstructive HCM. The preponderance of data indicates that disopyramide lowers diastolic filling
pressures in patients with outflow gradients, but that it may not help diastolic relaxation in the
purely non‐obstructed patient.

11
As indicated above 2/3 of patients with obstructive HCM may expect a successful
outcome from starting disopyramide and 1/3 will fail to achieve gradient reduction or symptom
relief. In the multicenter registry 5% of patients were intolerant of disopyramide and had to stop
the medication. In such patients surgical septal myectomy is considered the gold standard for
gradient reduction and improving symptoms and quality of life. Both interventions have their
own side effects and rare attendant mortality. However, improved understanding of the
physiology of obstruction and improved surgical technique have allowed much lower current
operative morbidity, and mortality at experienced centers should be < 1%, with a success rates
in excess of 95%. For patients of advanced age or with medical co‐morbidities, alcohol septal
ablation provides a less invasive route to septal reduction. Thus, patients should not be allowed
to linger too long with refractory symptoms and gradients. Patients who truly have failed
comprehensive pharmacotherapy should be expeditiously offered septal reduction. In this
category often fall young patients <45 years of age with high resting gradients > 80 mmHg and
long floppy anterior leaflets. Patients with the combination of all 3 of these findings infrequently
have sustained benefit from pharmacologic therapy.
Conclusions
The utility of disopyramide for selected patients with obstructive HCM has been shown
over a period of 30 years since its introduction. It is primarily used in patients who are
symptomatic after beta blockade, and may preclude the need for surgical intervention or
alcohol septal ablation. As such, its use should always be considered before such interventions
are undertaken. As with any other potent pharmacologic agent the general cardiologist should
become familiar with this medication and be clear about its indications, use, and side effects.
Finally, initiation of disopyramide should be based on a thorough discussion between physician
and patient focusing on anticipated benefit and potential side effects.
References
Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA 2002;287:1308‐20. Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011;124:2761‐96. Joshi S, Patel UK, Yao SS, et al. Standing and exercise Doppler echocardiography in obstructive hypertrophic cardiomyopathy: the range of gradients with upright activity. J Am Soc Echocardiogr 2011;24:75‐82. Sherrid MV. Pathophysiology and treatment of hypertrophic cardiomyopathy. Prog Cardiovasc Dis 2006;49:123‐51. Maron MS, Olivotto I, Zenovich AG, et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation 2006;114:2232‐9.
12
Shah JS, Esteban MT, Thaman R, et al. Prevalence of exercise‐induced left ventricular outflow tract obstruction in symptomatic patients with non‐obstructive hypertrophic cardiomyopathy. Heart 2008;94:1288‐94. Maron MS, Olivotto I, Betocchi S, et al. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med 2003;348:295‐303. Levine RA, Vlahakes GJ, Lefebvre X, et al. Papillary muscle displacement causes systolic anterior motion of the mitral valve. Experimental validation and insights into the mechanism of subaortic obstruction. Circulation 1995;91:1189‐95. Jiang L, Levine RA, King ME, Weyman AE. An integrated mechanism for systolic anterior motion of the mitral valve in hypertrophic cardiomyopathy based on echocardiographic observations. Am Heart J 1987;113:633‐44. Sherrid MV, Chaudhry FA, Swistel DG. Obstructive hypertrophic cardiomyopathy: echocardiography, pathophysiology, and the continuing evolution of surgery for obstruction. Ann Thorac Surg 2003;75:620‐32. Sherrid MV, Chu CK, Delia E, Mogtader A, Dwyer EM, Jr. An echocardiographic study of the fluid mechanics of obstruction in hypertrophic cardiomyopathy. J Am Coll Cardiol 1993;22:816‐25. Sherrid MV, Gunsburg DZ, Moldenhauer S, Pearle G. Systolic anterior motion begins at low left ventricular outflow tract velocity in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol 2000;36:1344‐54. Sherrid MV, Wever‐Pinzon O, Shah A, Chaudhry FA. Reflections of inflections in hypertrophic cardiomyopathy. J Am Coll Cardiol 2009;54:212‐9. Cannon RO, 3rd, Schenke WH, Maron BJ, et al. Differences in coronary flow and myocardial metabolism at rest and during pacing between patients with obstructive and patients with nonobstructive hypertrophic cardiomyopathy. J Am Coll Cardiol 1987;10:53‐62. Cannon RO, 3rd, McIntosh CL, Schenke WH, Maron BJ, Bonow RO, Epstein SE. Effect of surgical reduction of left ventricular outflow obstruction on hemodynamics, coronary flow, and myocardial metabolism in hypertrophic cardiomyopathy. Circulation 1989;79:766‐75. Sherrid MV, Pearle G, Gunsburg DZ. Mechanism of benefit of negative inotropes in obstructive hypertrophic cardiomyopathy. Circulation 1998;97:41‐7. Flamm MD, Harrison DC, Hancock EW. Muscular subaortic stenosis. Prevention of outflow obstruction with propranolol. Circulation 1968;38:846‐58. Stenson RE, Flamm MD, Jr., Harrison DC, Hancock EW. Hypertrophic subaortic stenosis. Clinical and hemodynamic effects of long‐term propranolol therapy. The American journal of cardiology 1973;31:763‐73. Cabrera‐Bueno F, Garcia‐Pinilla JM, Gomez‐Doblas JJ, Montiel‐Trujillo A, Rodriguez‐Bailon I, de Teresa‐Galvan E. Beta‐blocker therapy for dynamic left ventricular outflow tract obstruction induced by exercise. International journal of cardiology 2007;117:222‐6. Epstein SE, Rosing DR. Verapamil: its potential for causing serious complications in patients with hypertrophic cardiomyopathy. Circulation 1981;64:437‐41. Kajimoto K, Imai T, Minami Y, Kasanuki H. Comparison of acute reduction in left ventricular outflow tract pressure gradient in obstructive hypertrophic cardiomyopathy by disopyramide versus pilsicainide versus cibenzoline. Am J Cardiol 2010;106:1307‐12. Sherrid MV, Barac I, McKenna WJ, et al. Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol 2005;45:1251‐8. Sherrid MV, Shetty A, Winson G, Kim B, Musat D, Alviar CL, Homel P, Balaram SK, Swistel DG. Treatment of obstructive hypertrophic cardiomyopathy symptoms and gradient resistant to first‐line therapy with beta‐blockade or verapamil. Circulation Heart Failure 2013. In press. Wigle ED, Rakowski H, Kimball BP, Williams WG. Hypertrophic cardiomyopathy. Clinical spectrum and treatment. Circulation 1995;92:1680‐92. Elliott PM, Gimeno JR, Thaman R, et al. Historical trends in reported survival rates in patients with hypertrophic cardiomyopathy. Heart 2006;92:785‐91.

13
Pollick C. Muscular subaortic stenosis: hemodynamic and clinical improvement after disopyramide. The New England journal of medicine 1982;307:997‐9. Kimball BP, Bui S, Wigle ED. Acute dose‐response effects of intravenous disopyramide in hypertrophic obstructive cardiomyopathy. Am Heart J 1993;125:1691‐7. Pollick C, Kimball B, Henderson M, Wigle ED. Disopyramide in hypertrophic cardiomyopathy. I. Hemodynamic assessment after intravenous administration. Am J Cardiol 1988;62:1248‐51. Sherrid M, Delia E, Dwyer E. Oral disopyramide therapy for obstructive hypertrophic cardiomyopathy. Am J Cardiol 1988;62:1085‐8. Pollick C. Disopyramide in hypertrophic cardiomyopathy. II. Noninvasive assessment after oral administration. Am J Cardiol 1988;62:1252‐5. Maron BJ, Shen WK, Link MS, et al. Efficacy of implantable cardioverter‐defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med 2000;342:365‐73. Maron BJ, Spirito P, Shen WK, et al. Implantable cardioverter‐defibrillators and prevention of sudden cardiac death in hypertrophic cardiomyopathy. JAMA 2007;298:405‐12. Teichman SL, Ferrick A, Kim SG, Matos JA, Waspe LE, Fisher JD. Disopyramide‐pyridostigmine interaction: selective reversal of anticholinergic symptoms with preservation of antiarrhythmic effect. Journal of the American College of Cardiology 1987;10:633‐41. Minami Y, Kajimoto K, Kawana M, Hagiwara N, Sherrid MV. Synergistic effect of dual chamber pacing and disopyramide in obstructive hypertrophic cardiomyopathy. Int J Cardiol 2010;141:195‐7. Klues HG, Roberts WC, Maron BJ. Anomalous insertion of papillary muscle directly into anterior mitral leaflet in hypertrophic cardiomyopathy. Significance in producing left ventricular outflow obstruction. Circulation 1991;84:1188‐97. Sigwart U, Maron BJ, Nishimura RA, Danielson GK. Pitfalls in clinical recognition and a novel operative approach for hypertrophic cardiomyopathy with severe outflow obstruction due to anomalous papillary muscle. Circulation 1999;100:e99. Minami Y, Kajimoto K, Terajima Y, et al. Clinical implications of midventricular obstruction in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 2011;57:2346‐55. Fifer MA, O'Gara PT, McGovern BA, Semigran MJ. Effects of disopyramide on left ventricular diastolic function in hypertrophic cardiomyopathy. Am J Cardiol 1994;74:405‐8. Matsubara H, Nakatani S, Nagata S, et al. Salutary effect of disopyramide on left ventricular diastolic function in hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol 1995;26:768‐75. Balaram SK, Tyrie L, Sherrid MV, et al. Resection‐plication‐release for hypertrophic cardiomyopathy: clinical and echocardiographic follow‐up. Ann Thorac Surg 2008;86:1539‐44; discussion 44‐5. Smedira NG, Lytle BW, Lever HM, et al. Current effectiveness and risks of isolated septal myectomy for hypertrophic obstructive cardiomyopathy. Ann Thorac Surg 2008;85:127‐33. Schaff HV, Dearani JA, Ommen SR, Sorajja P, Nishimura RA. Expanding the indications for septal myectomy in patients with hypertrophic cardiomyopathy: results of operation in patients with latent obstruction. J Thorac Cardiovasc Surg 2012;143:303‐9. Fifer MA, Vlahakes GJ. Management of symptoms in hypertrophic cardiomyopathy. Circulation 2008;117:429‐39.