Symposium of Clinical Endocrinology fileSymposium francophone d’endocrinologie de IASI Symposium...
28
Symposium francophone d’endocrinologie de IASI Symposium of Clinical Endocrinology 6 – 8 may 2009, IASI Pregnancy and Hypothyroidism: Disadvantages for Mother and Child P.Bottermann, Munich
Transcript of Symposium of Clinical Endocrinology fileSymposium francophone d’endocrinologie de IASI Symposium...
Symposium francophone
d’endocrinologie de IASI
Symposium of Clinical Endocrinology
6 – 8 may 2009, IASI
Pregnancy and Hypothyroidism:
Disadvantages for Mother and Child
P.Bottermann, Munich
Pregnancy and Hypothyroidism
Disadvantages for Mother and Child
-------------------------------------------
general prevalence in pregnant women
- overt hypothyroidism 0,3 – 0,5 %
autoimmune thyreoiditis ~ 80 %
- subclinical hypothyroidism 2 – 3 %
autoimmune thyreoiditis ~ 55 %
--------------------------------------
Thyroid autoantibodies (TPO) at all
in pregnant women: 5 – 15 %
Chapter 1 – Mother
Pregnancy and Hypothyroidism
Disadvantages for Mother and Child
----------------------------------------------
Decreased fertility
34% become pregnant
11% in case of overt hypothyroidism
89% in case of subclinical hypothyroidism
Increased risk for early and late complications
Abortion
Anemia
Gestational hypertension
Placental abruption
Postpartal hemorrhages
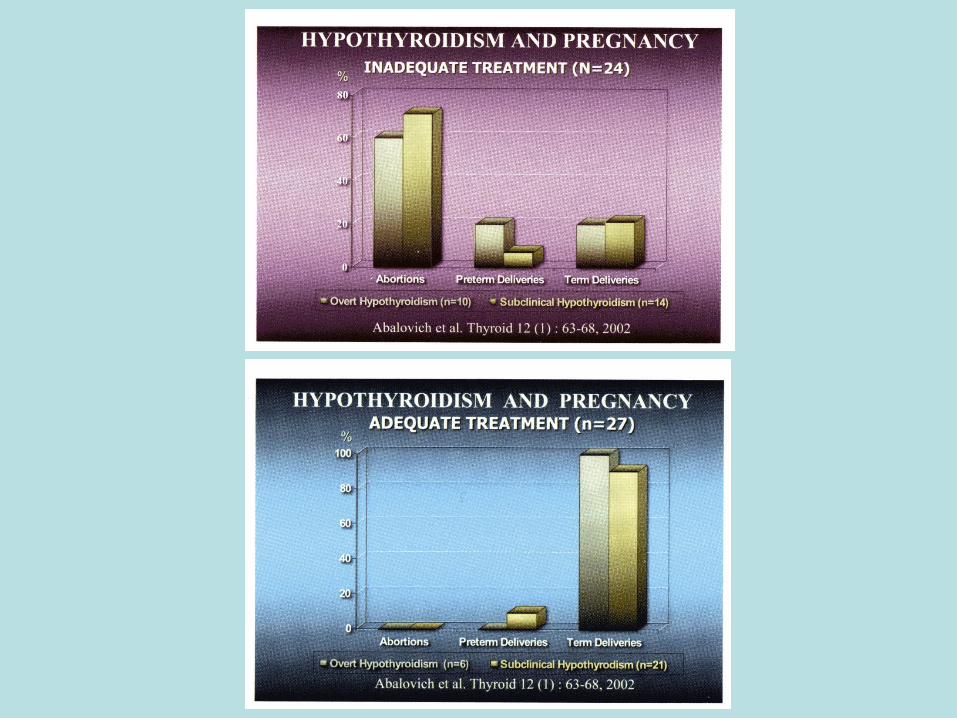
! Adequate thyroxine treatment decreases these risks !
Hypothyroidism - known before pregnancy
Optimal substitution with thyroxine
-------------------------------------------------
During pregnancy thyroxine dosage has to be elevated at 30 – 50 %
The increase of estrogen secretion after conception induces an increase in
TBG production.
The TBG- and therefore the TBG-T4 compartment become enlarged.
The euthyroid pregnant women increases the T4 production until a new
steady state/ balance.
The daily need for iodine increases from 150 µg to 250 µg.
But why it is necessary to elevate the substitution dosage?
What happens in euthyroid women during pregnancy ?
Pregnancy and Hypothyroidism
Disadvantages for Mother and Child
---------------------------------------------
What can we learn from the
pathophysiology of the mother for the child
First, let us look to the fetal development
Chapter 2 - Child
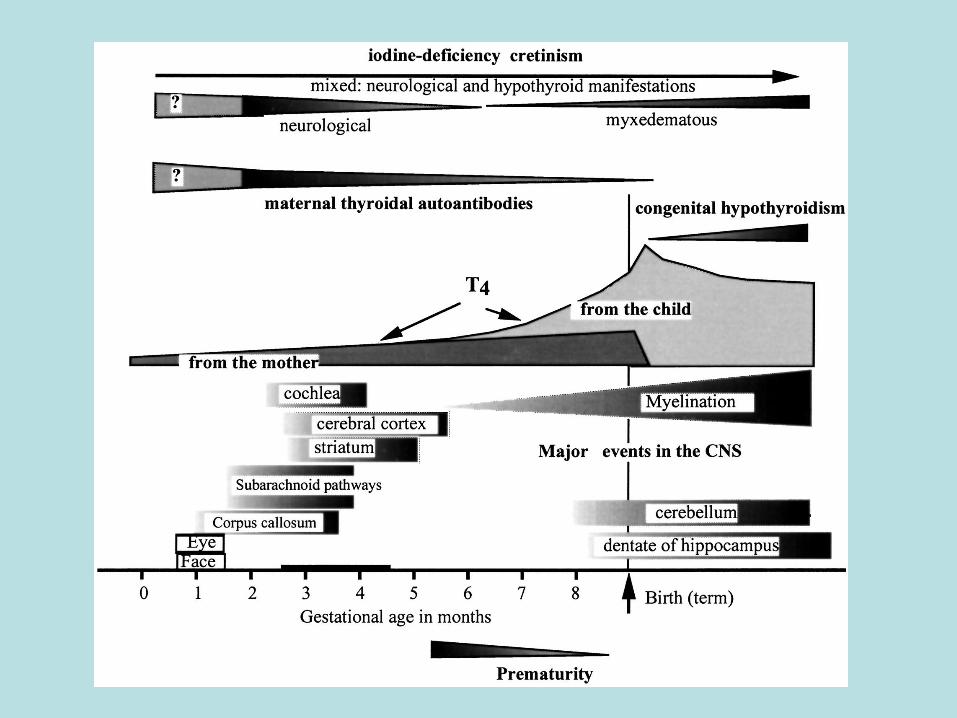
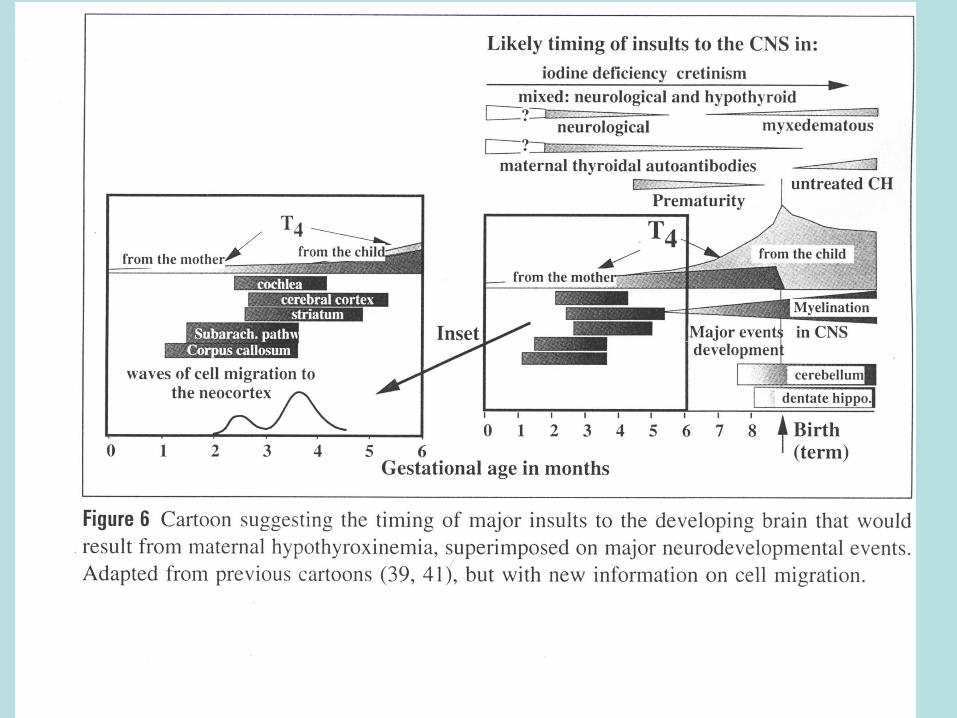
Fetal Brain and Thyroid Development
The fetal thyroid begins to work during the second trimester of
pregnancy.
In the first half of pregnancy thyroid hormone (T4) comes from the
mother; in the second half more and more thyroid hormone (T4) is
added from the fetal thyroid.
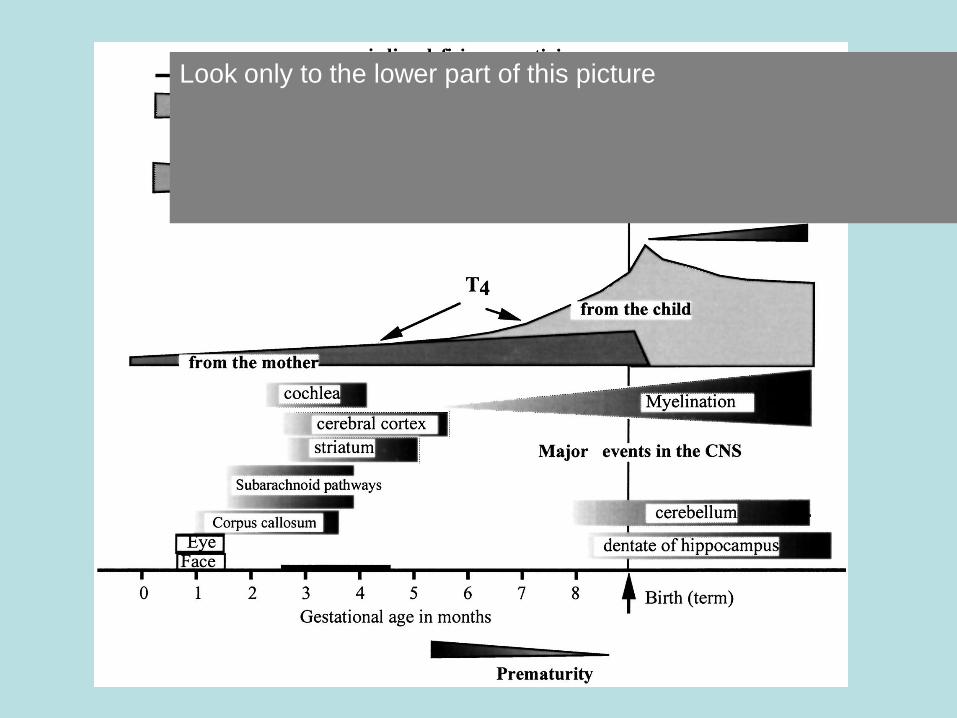
Look only to the lower part of this picture
Fetal Brain and Thyroid Development
The fetal thyroid begins to work during the second trimester of
pregnancy.
In the first half of pregnancy thyroid hormone (T4) comes from the
mother; in the second half more and more thyroid hormone (T4) is
added from the fetal thyroid.
It is important to note that for the developing organs (brain included) T3
is necessary.
For sufficient fetal generation of T3 sufficient maternal T4 must be
supplied.
Very early during fetal life deiodinases are detectable for local
generation of T3 (intracellulary) from T4
Early maternal hypothyroxinemia J. Clin. Invest. 111:1073–1082 (2003)
alters histogenesis and cerebral cortex
cytoarchitecture of the progeny Rosalía Lavado-Autric,1 Eva Ausó,2 José Victor García-Velasco,2 María del Carmen Arufe,1
Francisco Escobar del Rey,1 Pere Berbel,2 and Gabriella Morreale de Escobar1
…that maternal hypothyroxinemia clearly results in an alteration of neuronal
migration during neocorticogenesis…
…… availability to the developing brain of maternal T4 is of greater
importance than that of T3, because T3 in the fetal brain is almost entirely
dependent on its local generation from T4 and not on the uptake of
circulating T3….
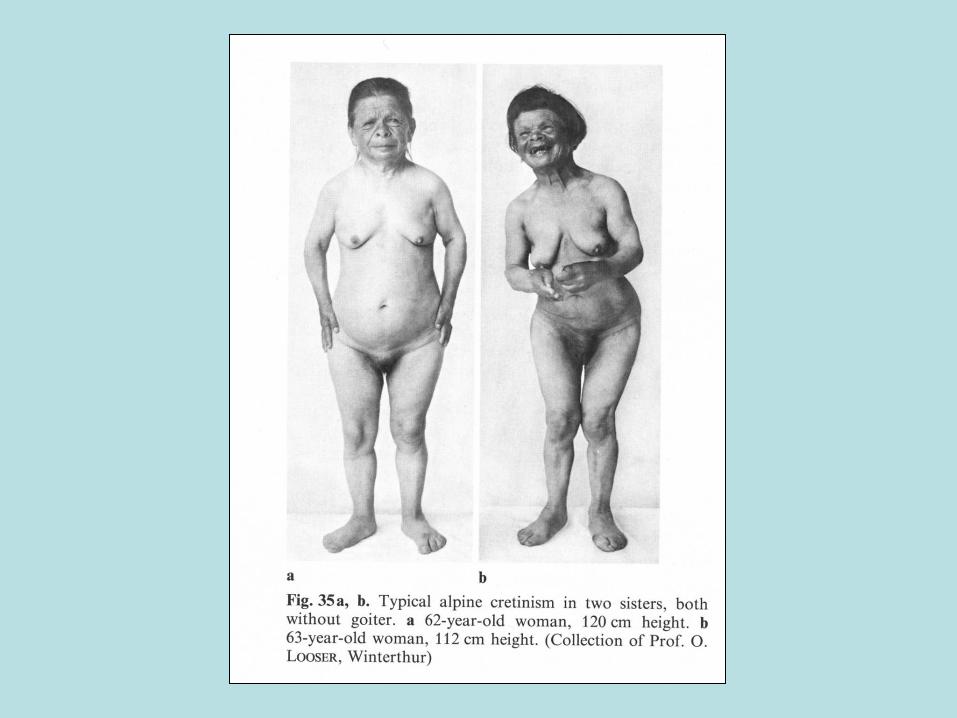
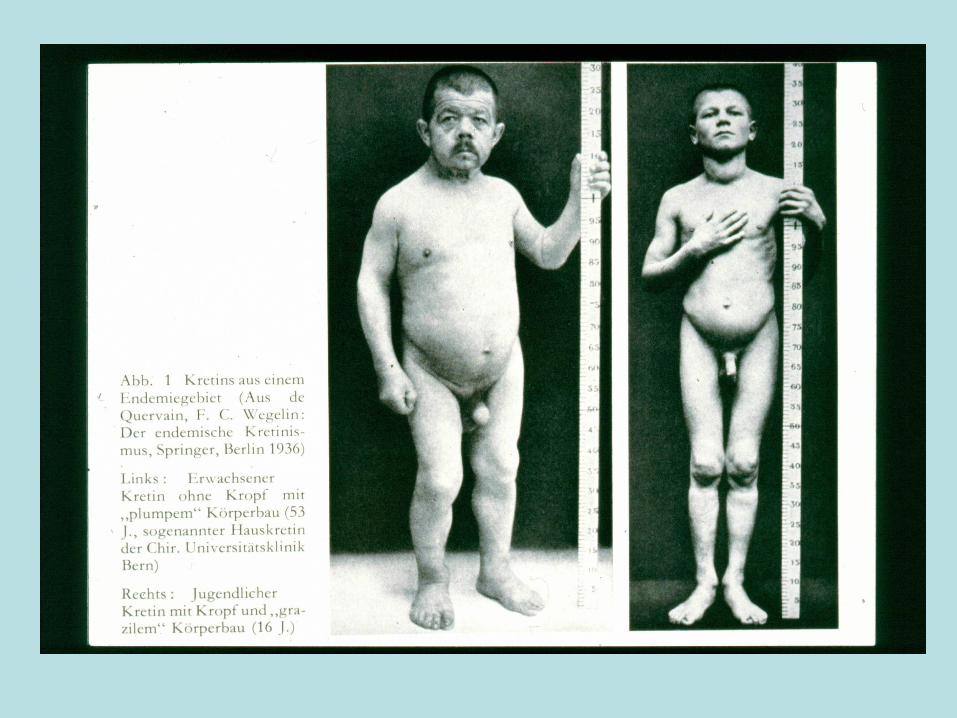
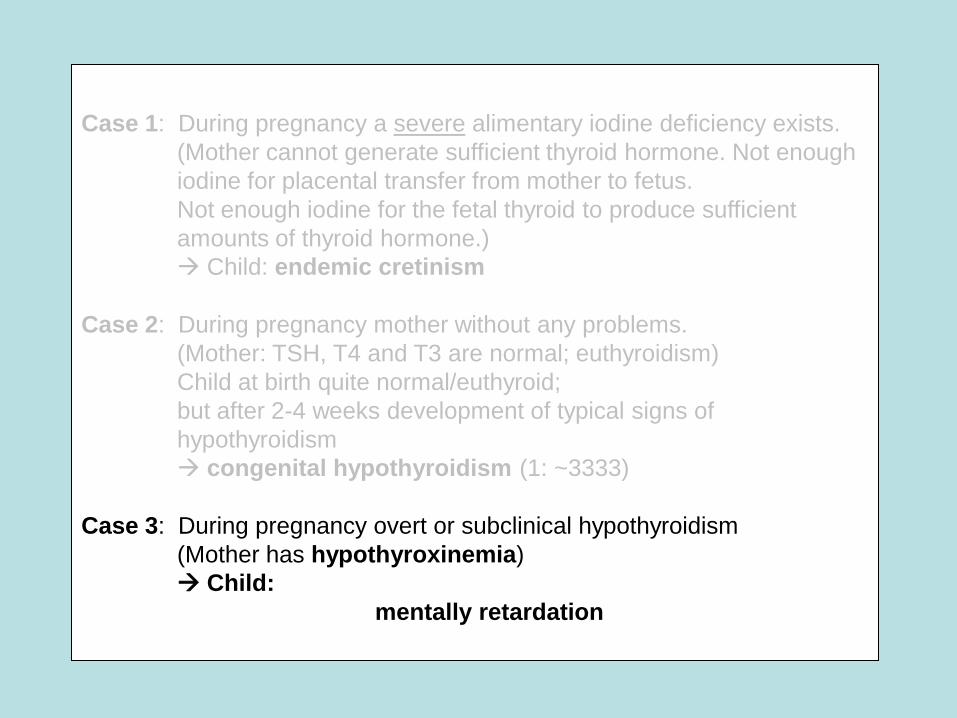
Case 1: During pregnancy a severe alimentary iodine deficiency exists.
(Mother cannot generate sufficient thyroid hormone. Not enough
iodine for placental transfer from mother to fetus.
Not enough iodine for the fetal thyroid to produce sufficient
amounts of thyroid hormone.)
Child:
endemic cretinism
What happens?
Case 1: During pregnancy a severe alimentary iodine deficiency exists.
(Mother cannot generate sufficient thyroid hormone. Not enough
iodine for placental transfer from mother to fetus.
Not enough iodine for the fetal thyroid to produce sufficient
amounts of thyroid hormone.)
Child: endemic cretinism
Case 2: During pregnancy mother without any problems.
(Mother: TSH, T4 and T3 are normal; euthyroidism)
Child at birth quite normal/euthyroid;
but after 2-4 weeks more and more development of typical signs
of hypothyroidism
congenital hypothyroidism (1: ~3333)
Case 1: During pregnancy a severe alimentary iodine deficiency exists.
(Mother cannot generate sufficient thyroid hormone. Not enough
iodine for placental transfer from mother to fetus.
Not enough iodine for the fetal thyroid to produce sufficient
amounts of thyroid hormone.)
Child: endemic cretinism
Case 2: During pregnancy mother without any problems.
(Mother: TSH, T4 and T3 are normal; euthyroidism)
Child at birth quite normal/euthyroid;
but after 2-4 weeks development of typical signs of
hypothyroidism
congenital hypothyroidism (1: ~3333)
Case 3: During pregnancy overt or subclinical hypothyroidism
(Mother has hypothyroxinemia)
Child:
mentally retardation
Early maternal hypothyroxinemia J. Clin. Invest. 111:1073–1082 (2003)
alters histogenesis and cerebral cortex
cytoarchitecture of the progeny Rosalía Lavado-Autric,1 Eva Ausó,2 José Victor García-Velasco,2 María del Carmen Arufe,1
Francisco Escobar del Rey,1 Pere Berbel,2 and Gabriella Morreale de Escobar1
…that maternal hypothyroxinemia clearly results in an alteration of neuronal
migration during neocorticogenesis…
……also supports previous conclusions that availability to the developing
brain of maternal T4 is of greater importance than that of T3, because T3 in
the fetal brain is almost entirely dependent on its local generation from T4
(4, 44) and not on the uptake of circulating T3….
Click on image to view larger version.
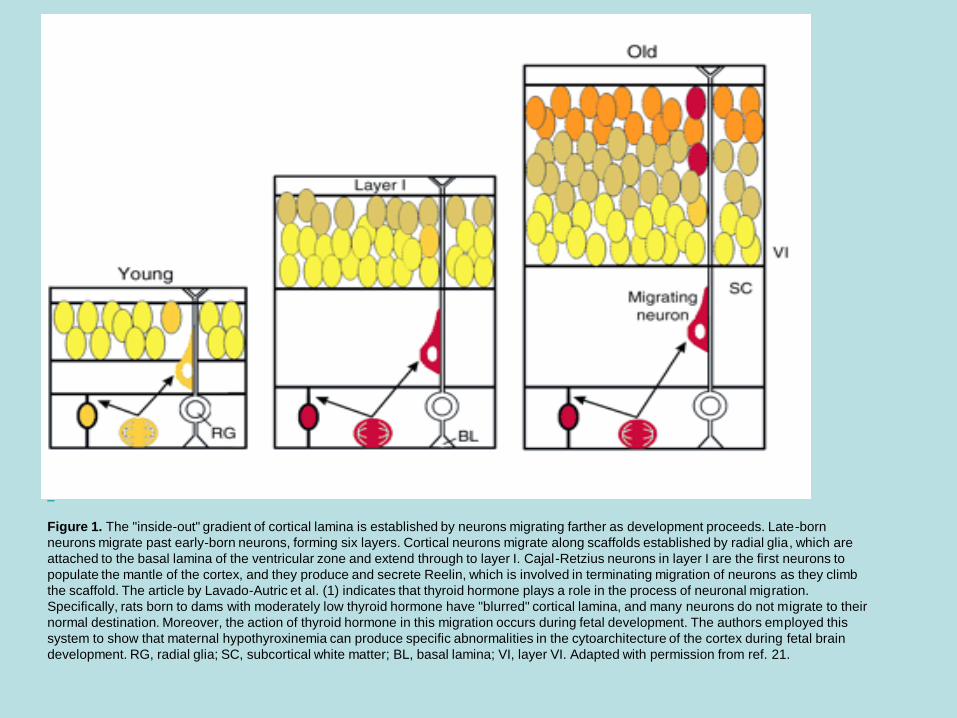
Figure 1. The "inside-out" gradient of cortical lamina is established by neurons migrating farther as development proceeds. Late-born
neurons migrate past early-born neurons, forming six layers. Cortical neurons migrate along scaffolds established by radial glia, which are
attached to the basal lamina of the ventricular zone and extend through to layer I. Cajal-Retzius neurons in layer I are the first neurons to
populate the mantle of the cortex, and they produce and secrete Reelin, which is involved in terminating migration of neurons as they climb
the scaffold. The article by Lavado-Autric et al. (1) indicates that thyroid hormone plays a role in the process of neuronal migration.
Specifically, rats born to dams with moderately low thyroid hormone have "blurred" cortical lamina, and many neurons do not migrate to their
normal destination. Moreover, the action of thyroid hormone in this migration occurs during fetal development. The authors employed this
system to show that maternal hypothyroxinemia can produce specific abnormalities in the cytoarchitecture of the cortex during fetal brain
development. RG, radial glia; SC, subcortical white matter; BL, basal lamina; VI, layer VI. Adapted with permission from ref. 21.
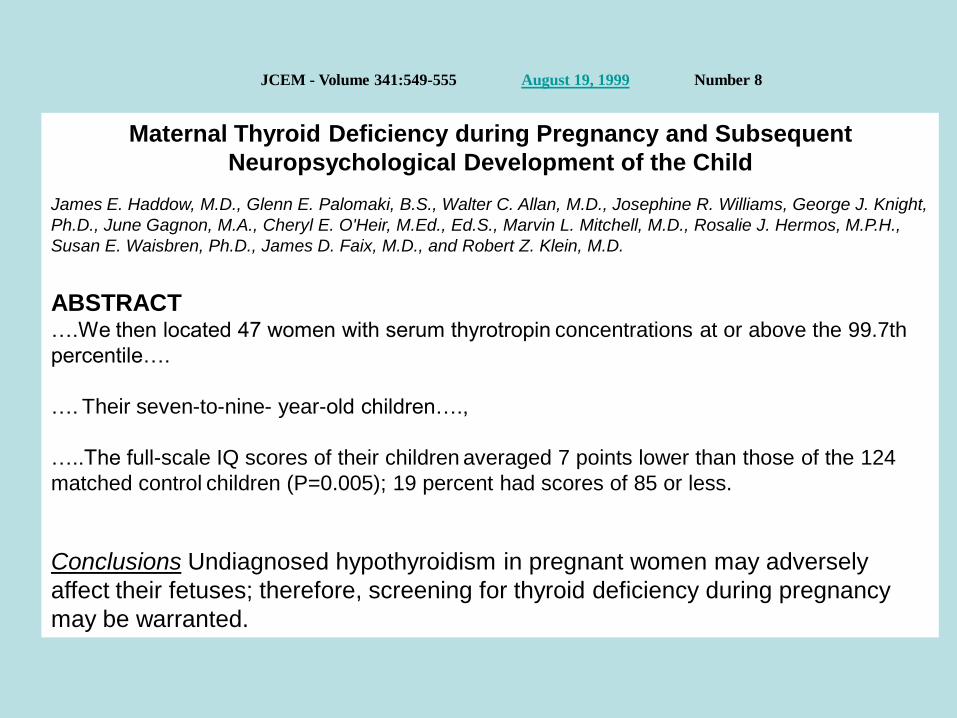
Maternal Thyroid Deficiency during Pregnancy and Subsequent
Neuropsychological Development of the Child
James E. Haddow, M.D., Glenn E. Palomaki, B.S., Walter C. Allan, M.D., Josephine R. Williams, George J. Knight,
Ph.D., June Gagnon, M.A., Cheryl E. O'Heir, M.Ed., Ed.S., Marvin L. Mitchell, M.D., Rosalie J. Hermos, M.P.H.,
Susan E. Waisbren, Ph.D., James D. Faix, M.D., and Robert Z. Klein, M.D.
ABSTRACT
….We then located 47 women with serum thyrotropin concentrations at or above the 99.7th
percentile….
…. Their seven-to-nine- year-old children….,
…..The full-scale IQ scores of their children averaged 7 points lower than those of the 124
matched control children (P=0.005); 19 percent had scores of 85 or less.
Conclusions Undiagnosed hypothyroidism in pregnant women may adversely
affect their fetuses; therefore, screening for thyroid deficiency during pregnancy
may be warranted.
JCEM - Volume 341:549-555 August 19, 1999 Number 8
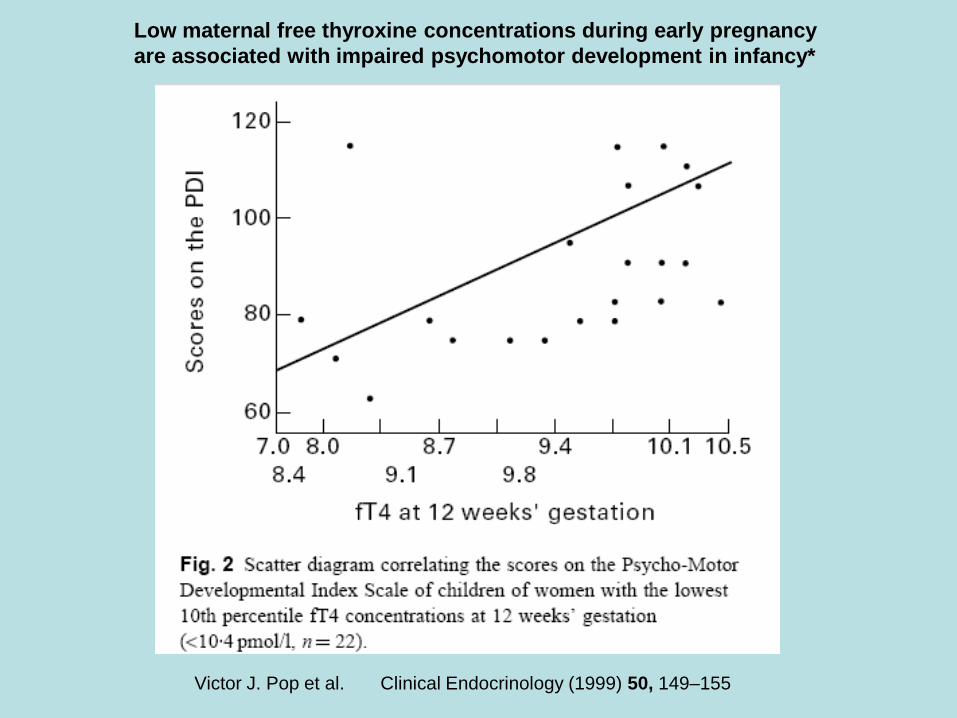
Low maternal free thyroxine concentrations during early pregnancy
are associated with impaired psychomotor development in infancy*
Victor J. Pop et al. Clinical Endocrinology (1999) 50, 149–155
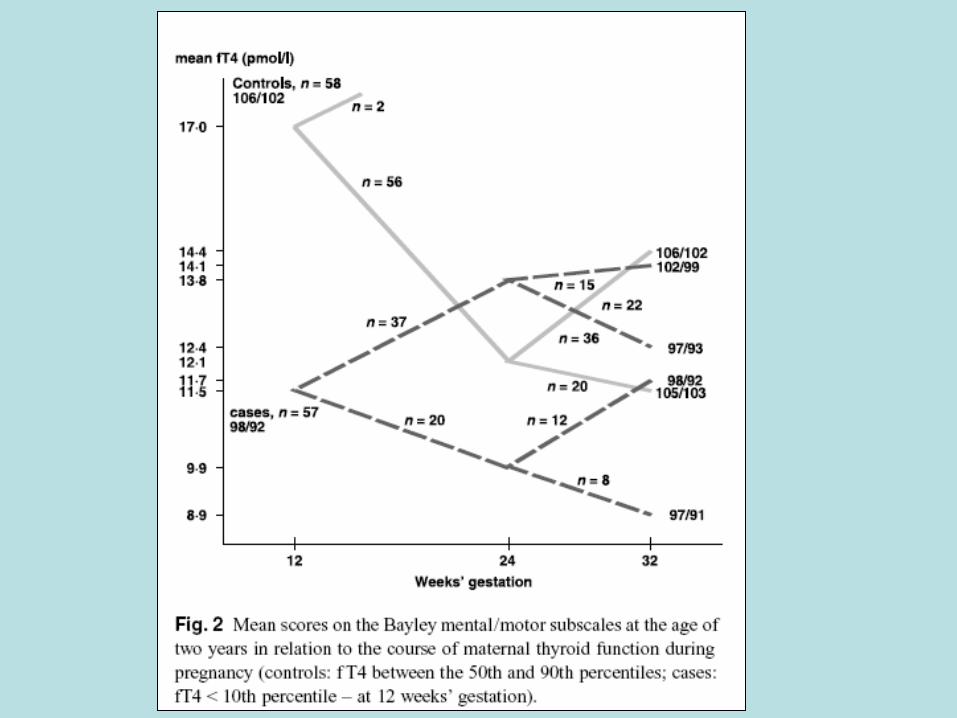
Clinical Endocrinology (2003) 59, 282–288,
Maternal hypothyroxinaemia during early pregnancy and
subsequent child development: a 3-year follow-up study Victor J. Pop*, Evelien P. Brouwers*, Huib L. Vader†,
Thomas Vulsma‡, Anneloes L. van Baar§ and Jan J. de Vijlder¶
Summary
OBJECTIVE
To evaluate the impact of maternal hypothyroxinaemia
during early gestation (fT4 below the lowest tenth percentile
and TSH within the reference range: 0·15–2·0 mIU/l) on infant
development, together with any subsequent changes in fT4 during
gestation.
RESULTS
Children of women with hypothyroxinaemia
at 12 weeks’ gestation had delayed mental and motor
function compared to controls: …..
CONCLUSIONS
Maternal hypothyroxinaemia during
early gestation is an independent determinant of a
delay in infant neurodevelopment. However, when fT4
concentrations increase during pregnancy in women
who are hypothyroxinaemic during early gestation,
infant development appears not to be adversely affected.
Chapter 3:
What shall we do tomorrow
CLINICAL PRACTICE GUIDELINE
Management of Thyroid Dysfunction during Pregnancy
and Postpartum: An Endocrine Society Clinical Practice Guideline Marcos Abalovich, Nobuyuki Amino, Linda A. Barbour, Rhoda H. Cobin, Leslie J. De Groot,
Daniel Glinoer, Susan J. Mandel, and Alex Stagnaro-Green
Conclusions: Management of thyroid diseases during pregnancy requires
special considerations because pregnancy induces major changes
in thyroid function, and maternal thyroid disease can have adverse
effects on the pregnancy and the fetus. Care requires coordination among
several health care professionals. Avoiding maternal (and fetal) hypothyroidism
is of major importance because of potential damage to fetal
neural development, an increased incidence of miscarriage, and preterm
delivery. Maternal hyperthyroidism and its treatment may be accompanied
by coincident problems in fetal thyroid function. Autoimmune
thyroid disease is associated with both increased rates of miscarriage, for
which the appropriate medical response is uncertain at this time, and
postpartum thyroiditis. Fine-needle aspiration cytology should be performed
for dominant thyroid nodules discovered in pregnancy. Radioactive
isotopes must be avoided during pregnancy and lactation. Universal
screening of pregnant women for thyroid disease is not yet
supported by adequate studies, but case finding targeted to specific
groups of patients who are at increased risk is strongly supported. (J Clin Endocrinol Metab 92: S1–S47, 2007)
Messages for the daily practice
Look for women at risk, especially in childbearing age,
- History of thyroid diseases as hyper- or hypothyrodism, goiter,
struma resection, family history of thyroid diseases,
infertility or preterm delivery,
Risk of thyroid diseases in other autoimmune diseases.
antiTPOAb during or after a former pregnancy (PPTD)
- for overt or subclinical hypothyroidism
Treat with thyroxine
Look for compensatory T3 overproduction as a sign of a relative
iodine deficiency.
(TSH normal; imbalance in the normal range between T3 (higher)
and T4 (lower.)
Treat with iodine – or perhaps, to be on the safe side, with tyroxine.
at all:
Be aware of a possible alimentary iodine deficiency
Treat with 200 µg iodine during pregnancy and breast feeding.

Multumesc frumos