Switram kc020 hyd
213
A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH” IN THE MANAGEMENT OF SWITRAM (VITILIGO) 1 INTRODUCTION The aim of medicine is to safeguard and rescue men from the consequences of their vices. Since its inception Ayurveda emphasizes on maintenance of positive health and alleviation of the diseases pestering humankind, among which skin diseases are one. Switra is a dermatological disorder having its references cited in the Vedas. The term is derived from “Sweth Varne” meaning white colour. It is basically a disease related to hypopigmentation. Switra is also known as “Sweta Kustam” or “Kilasam”. Switra emerges as a sequel to irregular dietary habits, life style changes, and genetic predisposition. Constant use of chemicals, cosmetics, plastic, rubbers, and pollution may accelerate the attack of the disease. The disease involves the skin and does not cause pain, ulceration or any secretions. Switra inflates an inferiority complex in the persons affected. Skin is the vital organ involved in this disease. Skin being the largest organ of the body and on the surface is continually exposed to injury. The colour of the skin plays an important role as high cosmetic value is attributed to it. Colouring, tattooing, adorning with jewellery are all part of skin appeal. The general state of the health is reflected in the appearance and condition of the skin and the earliest signs of many systemic diseases may be observed by inspecting it. As the skin is on the surface and it is on display patient with skin diseases are always in public eye. The greatest handicap of all is to be unwelcome and isolation by the community. The functions of the skin are impaired in skin diseases making those more affected, more vulnerable and less able to reconstitute themselves after damage. 20-30% of skin diseases require serious attention. (Davidson) The disease Switra is one among them, as it causes immense mental agony and social embarrassment.
-
Upload
ayurmitra-ksrprasad -
Category
Documents
-
view
1.810 -
download
7
description
A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO), K.NAMRATA, Department of Kayachikitsa, PG unit Dr.BRKR Govt. Ayurvedic College, HYDERABAD
Transcript of Switram kc020 hyd

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
1
INTRODUCTION
The aim of medicine is to safeguard and rescue men from the consequences of their
vices. Since its inception Ayurveda emphasizes on maintenance of positive health and
alleviation of the diseases pestering humankind, among which skin diseases are one.
Switra is a dermatological disorder having its references cited in the Vedas. The
term is derived from “Sweth Varne” meaning white colour. It is basically a disease
related to hypopigmentation. Switra is also known as “Sweta Kustam” or “Kilasam”.
Switra emerges as a sequel to irregular dietary habits, life style changes, and
genetic predisposition. Constant use of chemicals, cosmetics, plastic, rubbers, and
pollution may accelerate the attack of the disease. The disease involves the skin and does
not cause pain, ulceration or any secretions. Switra inflates an inferiority complex in the
persons affected.
Skin is the vital organ involved in this disease. Skin being the largest organ of the
body and on the surface is continually exposed to injury. The colour of the skin plays an
important role as high cosmetic value is attributed to it. Colouring, tattooing, adorning
with jewellery are all part of skin appeal.
The general state of the health is reflected in the appearance and condition of the
skin and the earliest signs of many systemic diseases may be observed by inspecting it.
As the skin is on the surface and it is on display patient with skin diseases are always in
public eye. The greatest handicap of all is to be unwelcome and isolation by the
community.
The functions of the skin are impaired in skin diseases making those more
affected, more vulnerable and less able to reconstitute themselves after damage. 20-30%
of skin diseases require serious attention. (Davidson) The disease Switra is one among
them, as it causes immense mental agony and social embarrassment.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
2
Based on the clinical features of switra, it can be correlated to vitiligo of the
modern medicine. Vitiligo on the face is ranked 17th by WHO in world’s most Disabling
diseases. Vitiligo is also an ancient malady having references cited in Bible and other
contemporary Texts. It is defined as a common acquired discolouration of the skin
characterized by well circumscribed, ivory or chalky white macules which are flush on to
the surface. Sometimes systemic, Cutaneous, ocular associations may be present. The
hair over the patch may be white or normal.
Vitiligo occurs world wide with an overall prevalence of 1%. The higher
incidence of the condition has been recorded in India from Asia, followed by Mexico and
Japan. The incidence is 6% in Calcutta, 4% in Vellore, 8% in Amaravati, 2.9% in Goa,
8.8% in Delhi. The difference of its incidence may be due to higher reporting of vitiligo
in a population where an apparent colour contrast and stigma attached to the condition
may force them to seek early consultation. Both males and females are equally affected
with no predilection of sex. The age of first onset is below 20 years and the lower limbs
are generally the site of first onset.
The imperatives of its epidemiology both in rural India and in global are
reckoning and have been highlighted. In spite of the latest advancements made in modern
medicine the etiology of vitiligo remains unknown. It is expected to be of autoimmune
origin as it is associated to some of the autoimmune disorders. Occasionally it may be
possible to identify the triggering factors.
An effective panacea for the disease could not be found till date. Generally topical
corticosteriod therapy, topical PUVA, Oral Psoralen Photo chemotherapy or oral PUVA,
Surgical techniques like skingrafting, other techniques like tatooing, camouflage creams
are employed to manage vitiligo. But all the above mentioned methods are associated
with high risk factors, are expensive, and unsuitable for people living in different
climatic conditions and the success rate is not commendable.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
3
Ayurveda offers absolution to many diseases among which switra is one.
Innumerable yogas have been described to combat the disease.
One such comprehensive formula is “Dhatri- Khadira Kwath” from Bhaishajya
Ratnavali, contemporary text of 19 A.D.
A total of 30 patients were taken for this study and all the patients received the
treatment for 45 days. The medicine was administered in kwath form, followed by honey
as anupana. The main aim was to assess the efficacy of the formula in causing
pigmentation in the white patches of switra. And three Clinical parameters – colour of the
patch, number of patches and size of the patches were taken into consideration to assess
the result.
Present study is divided into five parts. The first part deals with review of
literature of the disease, second part deals with drug review, third part deals with clinical
study – observations and results, fourth part deals with discussion, conclusion, summary
and fifth part deals with references, bibliography and annexure.
Thus a humble step has been made to probe into various aspects of switra and its
management with the trial drug.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
4
HISTORICAL REVIEW
Switra is an ancient malady and a historical background will facilitate continuity with
current research .Many earliest references of switra dating back to Vedic kala are found
and the contribution of our ancestors in combating the disease is known.
For convenience sake time period is divided into:
1. PRACHEENA KALA (5000 BC- 7 A.D )
2. MADHYAMA KALA ( 8 A.D –15 A.D )
3. ADHUNIKA KALA (16 A.D ONWARDS )
PRACHEENA KALA (5000 BC- 7 A.D):
VEDIC PERIOD: includes description of the disease in Rig, Yajur, Sama &Atharvavedas.
RIG VEDA:
a) Old looking unmarried princess Ghosa, the daughter of Kaksivana was cured of
kusta roga and was made young and beautiful, and was married .1
b) Sujava was cured of kusta and rejuvenated and was married to a good looking
girl .2
c) Diseases like kilasa and Palithya were described .3
d) Application of Bringraj, Harida , Neelika , Indravaruni in kusta ,palitya rogas
.Here Sayanu interprets kusta as Svetha kustam.4
YAJUR VEDA:
There is a reference of moon being affected by the disease.5

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
5
ATHARVA VEDA:
a) There is a refernce in Atharva Veda that white coloured patches appear in a
disease called Sweta kusta, and when it penetrates into deeper dhatus it is called
Kilasa
kusta .6
In this context “ASIKINI “and “RAJINI” are the drugs used which are very
important in the disease.
SAMA VEDA : No references found in this veda
.Aitheraya Aranyaka: Sage Bharadwaja mentioned twak, mamsa .rakta are derived from
mother and in a stage all the three are affected
During Uanishad period Asvatayana mentioned maharogas .Narayana interprets Kusta
as one among them.7
In Mahabharata (400 B.C) mentioning of many twag doshas are found but no special
reference of Switra is found.
Puranas (500 B.C) were influenced by the medical concepts and description of many
diseases are found in them.
Padmapurana mentions kusta and Switra as diseases caused due to the imbalance of the
tridoshas.8
Markandeya purana mentioned two girls suffered with this disease and were eventually
cured 9It is regarded by this purana that all twag rogas are due to past life sins.
Vayu purana regarded kusta and kilasa to have evolved due to faulty practice of yoga10.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
6
Vishnu purana mentioned a wide variety of skin diseases in sharirika rogas 11.In
anatomical chapters a detailed description of embryological development of organs is
found and seven layers of skin have been described in this context.
Itihasa purana mentioned switra among several diseases caused due to derangement of
the doshas .Sins or the papakarmas are considered to play a major role in causing the skin
diseases in particular .12.
Brahma vaivartha purana mentioned many skin diseases under the heading GALITHA
VYADHIS 13among which switra is one.
Agni purana mentioned kusta as a broad term to describe all the skin diseases including
switra.
In Yagnavalkya smriti skin or the twacha has been described having six layers and all
the diseases arise from these layers .14
Manu smriti (200B.C-200 A.D) has clearly mentioned that a stealer of clothes suffers
from switram .It is aquainted as hereditary disease and people suffering with this disease
are not eligible for marriage .15
OTHER LITERATURE DURING VEDIC PERIOD:
Other than the Indian literature, earliest references of the condition can be traced back to
the period of Aushooryan (2200 B.C) in the classic TARIKH –E-TIL-IRAN.16
Pharaonic medicine in the ebers papyrus (1500B.C) described two types of diseases
affecting the colour of the skin. a) With tremors probably leprosy b) with colour change
probably Vitiligo .The latter was said to treatable .17
In Arabic medicine the terms “BOHAK “BAHAK” ‘BARAS’ are the terms mentioned to
denote a similar condition like Vitiligo.18
In Bible the term “ZORAAT”denotes Vitiligo.19

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
7
In Japanese literature (1200BC) SHIRABITO is the term used for the condition like like
switra .20
SAMHITA KALA:
Charaka samhita: In this treatise switra is described in the kusta roga chapter .A
detailed description of the disease is found in this text.A special etiology is mentioned for
switram, types and treatment has been vividly described .21
Sushruta samhita: Has also described switra in a detailed fashion.In nidana Stan 5th
chapter description of the disease is found .22
Bhela samhita; Bhela included switra in eleven kshudra kustas and mentioned it as
asadya roga .23
Harita samhita :did not give a detailed description of the disease but mentioned a stealer
of clothes and money is prone to get this disease .And arista lakshanas of kusta rogas are
mentioned and said to be applicable to switra also.24
Kashyapa samhita: included switra in eleven types of kshudra kustas .Five types are
mentioned but no names and clinical features are found .it is said to be a asadya vyadhi.25
SANGRAHA KALA;
Astang Sangraha: switra as a bahya vikruti and in sutra Stan mentions that using a
poisonous jalouka for rakta mokshanam shall cause the disease 26.
Astang Hrudayam: describes switra as a separate disease .Etiology, types, clinical
features, prognosis and treatment are clearly mentioned .Vagbatta has considered switra
to a medical emergency as delayed medical intervention may lead to complete
depigmentation.27

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
8
MADHYAMA KALA (8 A.D. - 15 A.D):
Vangasena: a text book of 10 A.D describes about the etiological factors responsible for
the disease. Specially seven dietary factors are mentioned which cause kusta rogas.The
etiology of kusta and switra are considered same .28
Madhava Nidan: a special text on etiology of different diseases describes switra in
49thchapter .complete description of the disease is found vividly in this book.29
Sharangdhara samhita :( 11-12 A.D) has mentioned the etiology of kusta and switra to
be same and mentioned three types of the disease based on the involvement of the
dhatus .30
BhavaPrakash: written by Bhavmisra has given a detailed description about the disease
the etiology, types ,clinical features ,prognosis and treatment have been in the text.31
BUDDHIST LITERATURE:
Tripitika literature is the oldest source to have a glimpse of Indian medicine in
Buddhist tradition. It is mentioned that kusta, kilasa, ganda, sosa, apasmara, are five
prevalent abadhas.
Vinaya pitam mentioned the disease kilasa i.e spotted deer 32.
Sardulakarnavadana: In this book Ayurveda is mentioned along with four vedas.
Kushta and kilasa are mentioned seperately33.
Lalithavistara: One among the nine important texts deals with the advent of Lord
Buddha and his teachings. In this context those diseases caused by vata, pitta, sleshma
and sannipata diasease of kushta and kilasa34
Saddharmapundarika: Diseases like kusta and kilasa are mentioned seperately35
JAIN TRADITION: 16 diseases are enumerated among which leprosy is one.
Kalyanakaraka: By Vugraditycharya. 20 chapters are present. From 8 th chapter onwards
diseases are mentioned. Kusta is one among mahamayas.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
9
OTHER NON-MEDICAL SOURCES:
Panini (7th B.C): Sutras were annotated by patanjali in 2nd B.C. Kusta and Kilasa are
mentioned separately.
Kautilya’s Arthasastra: (321-297 B.C) In a chapter on secret means, a number of
diseases has been mentioned among which kusta is one. In this disease this physician’s
certificate is honoured.36
Bana Bhatta (606-648 A.D): In Harsacharitra and Kadambari mentioned the concept of
health and described Switra separately.37
Amarakosha (600 A.D): Has mentioned switra separately and terms like “Padasphota”,
“Twak pushpi” are mentioned in this context.38
ADHUNIKA KALA (16 A.D ONWARDS):
Yogaratnakar: mentioned switra as kilasa and described it in kusta chapter.
Bhaishajya Ratnavali: switra is described in kusta roga adhikar. Treatment of switra is
described with various formulations .39
RESEARCH WORKS DONE IN VARIOUS INSTITUTIONS :
1. Dr.Sheela ratna M.V, Switra roga and its management Mysore 1979.
2. Dr.Patil A.K, Survey of Switra in Jamnagar and Vicinity in reference to its nidana
and Chikitsa .Jamnagar 1984.
3. Dr.Upadhyaya R.K, Therapuetic assessment of some Ayurvedic drugs in
treatment of Vitiligo.Varnasi 1985.
4. Dr.Shankaran.K, Managament of Switra with special reference to Bakuchi
Trivendrum 1986.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
10
5. Dr.Lahiri P.K, Clinical studies and management of Switra kusta (leucoderma)
with Ayurvedic drugs, Calcutta 1987.
6. Dr.PrithviRaj, Concept of switra and its management in Ayurveda, varnasi1988.
7. Dr.ThakoreS.R, Switra mein Kakodumbara ka Prayogika Adhyayan.
Ahmedabad1989.
8. Dr.Srikanth Babu, Evolution of Kakodumbaradi yoga in management of Switra.
Mysore 1992.
9. Dr.Sharada C.L, Clinical study of Switra (leucoderma) and its management with
kakodumbara and manahshiladi lepa.Jamnagar 1993.
10. Dr.Kambale.S, Switra kustavar nidana parivarjana aushadhi (bavanchi) ani
aharacha parinama.Nanded 1996.
11. Dr.Prabhakar.Shinde, A Clinical study of the effect of Somarajyadi churnam (int)
and Somarajyadi lepa (ext) in Switra .Hyderabad 1996.
12. Dr Seeta Devi.P .A clinical study on the effect of lepa in Switra .Mysore 2003.
13. Dr.Venugopal CH, A clinical study on the effect of kaseesabadda ras (int) with
and without chitraka lepa in Switra (VITILIGO) Hyderabad 2003.
14. Dr.Mahantesh P.M, A Comprehensive management of kilasa kusta Vitiligo).Hubli
2006.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
11
NIRUKTI
The term switra is derived from “swith” dhatu meaning white colour. Rak pratyaya is
added and letter “kha” is deleted.It belongs to napunsaka gender.
Swith +ra = Switra40
Switra =Sweth varne switra
The term indicates a disease where white coloured patches appear on the skin.
Switra is analogous to the disease vitiligo in the contemporary medicine .The
term Vitiligo is derived from latin word “vitium” meaning defect .41 Documentation of
the word is present in the book De-Meedicina by the Roman Physician Celsus42.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
12
PARIBHASHA
The definition of Switra is given by all the ancient classics .The acharyas who have
defined switra primarily suggested that this is a disease related to impairment of colour.
The term Switra is derived from “sweth varne switra” meaning white colour.
Amarkosha defined switra as “Swetate twaganena Switram”43 meaning ‘white colour
of the skin’.
Shabda kalpa drumam defined it as “Swetate itihi” meaning white colour .44
Kashyapa samhita defined Switram as “Sweta bhavamicchanti switram” meaning
reflection of white colour .45
Sushruta defined it as “Twagatam eva aparisravi “one which involves only the skin and
has no oozing tendency.46
The essence of all the above mentioned, indicate Switra as a disease in which
hypopigmentation is a cardinal feature.
Vitiligo is defined as a dermatological disorder characterized by milky white patches
devoid of melanocytes .It bears resemblence in having a progressive tendency and
genetic predisposition.47

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
13
SHAREERA RACHANA
Introduction: “Twak’ or the “Twacha” are the analogous names to identify the skin in
Ayurveda. It is one of the largest organs which cover the entire external surface area of
the body.
Twak is aptly defined as “Twach Samvarne” 48 meaning the one which covers. It
covers the entire external surface of the body protecting the underlying rakta, mamsa,
medo dhatus49. The skin forms a self renewing, self repairing interface between the body
and the environment.
Embryonic Development of Twak:- A perfect combination of healthy sukra and
sonitha leads to the formation of an healthy embryo50. The pancha maha bhutas act
accordingly on the embryo leading to the formation of various anga – pratyangas.
Amongst the five, Vayu helps in the division of the cells, and Tejo maha bhuta helps in
the maturation and specialization of the cells forming different layers of cells of different
organs. Sushruta opined that as the cream is formed over the boiling milk, the various
layers of the skin are also formed and deposited on the rapidly forming product of the
combination of sukra & sonitha.51
Vagbatta described that during the process of cooling (Processing) of the blood,
the layers of twak are formed, and the purity of the skin lies in the purity of blood.52
Sushruta described seven layers of the skin, Charaka53 and Vagbatta54 described six
layers of skin.
Twak is derived predominantly from vayu and akash mahabhutas and its
adhistana devata is vayu55. Twak is one of the pancha gnanedriyas56 and its indriyartha is
Sparsha57, its indriya buddi is Sparshana58.
The entire body is a combination of three doshas, Sapta dhatus and three malas59.
Skin also being a part of this body is composed of vata, pitta and kapha. It is an upadhatu
of mamsa dhatu. Sweda is excreted through the skin.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
14
The tridoshas have their respective role to play in the twak. The skin being the
seat of vata it does the sparsha grahana, 60 pitta helps in imparting the colour and luster51.
Kapha gives the mrudutwa and snigdatwa to the skin.62
In the process of formation of various dhatus, the mamsa dhatu is derived from
rakta dhatu.63 The prasada bhagha of mamsa dhatu is subdivided into vasa & twak.64
These two are nourished by the mamsa dhatu. Apart from receiving nourishment from its
parent dhatu, twak is also nourished by numerous rasavahinis. Sometimes the rasa and
twak become analogous, twak Sara person is considered as rasa Sara also65.
Twak is considered to be a rasaja bhava by the virtue of its property to reflect the
varna.66
LAYERS OF THE SKIN:
1st Layer: is named as “udakadhara”67 by charaka and is believed to contain watery
substance such as rasa or lasika (body lymph). Sushruta named it as ‘avabhasini’ which
measures 1/18vreehi; this layer reflects the colour and complexion of the skin68.
Vagbhatta named it as “bhasini”. It is the site for manifestation of sidma and
padmakantakam.
2nd Layer: is named as ‘asrgdhara’ by charaka as it contains blood capillaries. Sushruta
named it as “Lohita”. It measures 1/16 vreehi. Vagbhatta named it as “Lohini”.
Cutaneous infections like Tilakalaka, Nyaccha, and Vyanga are manifested here.
3rd Layer: Unnamed by charaka, Sushruta named it as “sweta” it measures 1/12 vreehi.
It is the site for manifestation of Charmadala, Ajagillika, and Mashaka.Charaka described
this layer to be the seat for Sidma & Kilasa.
4th Layer: Not named by charaka & Vagbhatta but explained it to be the site for all
varieties of kusta and dadru. Sushruta named it as ‘Tamra’ measuring about 1/8 th vreehi
and seat for various types of kusta and kilasa.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
15
5th Layer: Not named by Charaka and Vagbatta but explained diseases like alaji, and
vidradhi being manifested here. Sushruta named this layer “vedini” measuring about 1/6 th
of vreehi. And diseases like kusta and visarpa are explained here.
6th Layer: Not named by Charaka but Vagbhatta named it as “pranadhara” the supporter
of life and seat for diseases like arumshi. Excision of which leads to tremors and entering
to darkness. Any manifestations are deep rooted here and difficult to treat. Sushruta
named this layer as ‘Rohini’ which measures 1 vreehi. Grandhi, arbudas, apache, slipada,
galaganda are manifested here. All muscular outgrowths are noted here.
7th Layer: Named by sushruta as “Mamsadhara”. The deepest layer, thickness is double
the vreehi, and diseases like Bhagandara, Vidradhi are manifested here. All the diseases
involving mamsa and rakta dhathu are explained here.
According to Charaka69:
Table -1
S.No. Name of the Layer Function Diseases
1. Udaka dhara Protects the loss of body fluids -
2. Asragdhara Reservoir of blood -
3. Tritiya - Sidma, kilasa
4. Chaturtha - Dadru, Kusta
5. Panchami - Alaji, Vidradi
6. Shasti - Tremors anddarkness before eyes.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
16
According to Sushruta70:
Table -2
S.No. Name ofthe layer
Thickness Function Diseases
1. Avabhasini 1/18 Vreehi Reflection ofcolour &
complexion
Sidma, Padma Kantakam
2. Lohita 1/16 Vreehi - Tilakalaka, Nyaccha,Vyanga
3. Swetha 1/12 Vreehi - Charmadala, Ajagallika,Mashaka
4. Tamra 1/8 Vreehi - Kilasa & Kusta5. Vedini 1/6 Vreehi - Kusta & visarpa6. Rohini 1 Vreehi - Granthi, Apacchi, Arbuda,
Galaganda, Sleepada7. Mamsadara 2 Vreehi - Bhagandara, Vidradi,
Arsas
According to Astangahrudaya71:
Table -3
S.No. Nameof the layer
Function Diseases
1. Bhasini Expresses Colour and fiveshades of complexion
-
2. Lohini - -3. Swetha - -4. Tamra - -5. Vedini - -6. Rohini - -7. Mamsadhara - -

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
17
ANATOMY OF THE SKIN
Among the three primary germ layers of the embryo, the epidermis is derived
from the ectoderm-the outer most primary germ layers. At the beginning of the second
month the ectoderm consists of simple cuboidal epithelium. These cells flatten and are
known as Periderm.
By the end of fourth month, all layers of the epidermis are formed and each layer
assumes its characteristic structure.
The dermis is derived from wandering mesodermal cells. The mesenchyme
becomes arranged in a zone beneath the ectoderm and there undergoes changes in the
connective tissues that form the dermis.
Nails develop during third month from ectoderm. Hairfollicles develop between
third & fourth month from the ectoderm. By the fifth and sixth month follicles produce
delicate hair called lanugo which usually shed before birth.
The secretory portions of sebaceous and sudoriferous glands are derived from
ectoderm. The connecting tissues and blood vessels associated with the glands develop
from mesoderm.
Microstructure of the Skin:
Epidermis: is a compound tissue consisting mainly of continuously self replacing
stratified keratinized squamous epithelium. The principle cells of which are called
Keratinocytes. Other Cellular elements of different developmental orgin within the
mature epidermis includes melanocytes or the pigment forming cells from embryonic
neural crest. Langercells are immunocompetent antigen presenting cells derived from
bone marrow. Other cells are Lymphocytes. These disparate cells are collectively
known as non-keratinocytes or epidermal immigrants. Neurally associated Merkel cells
are now thought to be modified Keratinocytes.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
18
Sensory nerve endings are also sparsely present within the epidermis. Each
component has an individual primary function, but the fact of there intimate spatial
associations and of functional interactions has led to the concept of epidermal symbionts.
The population of keratinocytes undergoes continuous renewal through out the
life a mitotic layer of cells at the base replacing those shed at the surface. As they move
away from the base of the epidermis, the keratinocytes undergo progressive changes in
shape and content full of protein keratin, a process known as keratinisation.
It is usual to divide the epidermis into number of strata from deep to superficial as
follows, S.basale, S.spinosum, S.granulosum, S.lucidum and S.corneum. The first three
of these layers are metabolically active and often grouped together as the stratum
malpighi. The more superficial strata of cells achieving terminal keratinazation
constitute the cornified zone.
1. Stratum basale: This includes the deepest layer of cells adjacent to the dermis and
appears to rest upon a continuous narrow ‘basement membrane’ which includes the basal
plasma membrane of the cell, a basal lamina consisting of lamina lucida and lamina
densa, and a dermal reticular lamina. This area is also known as epidermal – dermal
junction. The cytoplasm contains the common cellular organelles, melanosomes and
many cytoskeletal intermediate filaments. The plasma membranes of the opposed cells
are connected by desmosomes and the basal plasma membrane has hemidesmosomes.
Melanocytes, Langerhans cells and Merkelcells are interspread among the basal
keratinocytes.
2. Stratum spinosum (Prickle Cell Layer): This contains several layers of mature
keratinocytes packed closely and inter digitating by means of numerous projections and
indentations of the cell membrane which are linked by many desmosomes giving then
spiny appearance, hence also called as Prickle cell layer. The cytoplasm contains the
common organelles including some lysosomes and melanosomes. Langerhans cells and

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
19
the occasional associated lymphocytes are the only non -keratinocytes present in the
stratum spinosum.
3. Stratum granulosum: In this stratum three to four layers of flattened cells with
extensive changes in Keratinocyte structure occurs . The nuclei become pycnotic and
began to disintegrate, the membraneous organelles such as mitocondria, golgi membranes
and ribosomes degenerate, and keratin filament bundles become more compact and
associated with Keratohyalin granules. Small round granules with a lamellar internal
structure also appear in the cytoplasm. The lamellar granules are concentrated deep to the
plasma membrane of the granular cell with which they fuse liberating their predominantly
lipid content in to the intercellular space not only of this stratum, but also into the space
between it and the stratum corneum. They form an important component of the
permeability barrier of the epidermis, langerhans cells may occasionally be seen at lower
levels of stratum granulosum.
4. Stratum lucidum: Only found in thick glabrous palmo-plantar skin, this layer
represents poorly understood stage in Keratinocyte differentiation. Ultrastructurally
resembles the transitional cell, an incompletely keratinized cell occasionally seen in the
innermost layer of the statum corneum of non-glabrous skin.
5. Stratum corneum: This stratum is the final product of epidermal differentiation or
Keratinazation. It consists of closely packed layers of flattened Polyhedral Corneocytes.
These cells overlap at their lateral margins and interlock with cells of opposed layers by
ridges, grooves and microvilli. In this skin the statum may be only a few cells deep, but in
thick skin it may be more than 50 cells deep. The interior of this corneocyte is devoid of
nucleus and membraneous organelles, consisting solely of a dense array of keratin
filaments embedded in an interfilmentous matrix partly composed of filaggrin derived
from keratohyalin granules.
Desquamation of the outer layers of the stratum corneum involves a poorly
understood loosening of attachments (desmosomes and inter cellular substances) between
the cells, probably involving enzyme action and is normally imperceptible, when

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
20
execessive, it appears in hairy regions as dandruff and more massively in certain diseases
as peeling, scaling, and exfoliation. Langerhans cells are not present in the stratum
corneum and therefore are not desquamated.
Melanophages are macrophages which have ingested performed melanin and
melanphores or dermal melanocytes, within which melanin can be rapidly aggregated or
dispersed to change body colour in adaptation to environmental backgrounds.
Embryonic precursors of melanocytes migrate from the neural crest to enter the
epidermis as melanocytes from about eight gestational weeks. It is estimated that a single
melanocyte may be in functional intact via its dendrites with up to 30 Keratinocytes to
form an entity called the epidermal melanin unit. Melanocytes decrease significantly
in number in old age and are absent from grey hair.
EPIDERMAL MELANOCYTES AND SKIN PIGMENTATION
Melanocytes are melanin pigment forming cells derived from the neural crest and
widely distributed throughout the body in vertebrates. In humans they are present in the
epidermis and its appendages, in oral epithelium, some mucous membranes, the uveal
tract of the eyeball, parts of the middle and internal ear and in the leptomeninges at the
base of the brain. The cells of the retinal pigment epithelium, developed from the outer
wall of the optic cup, also produce melanin, and neurons in different locations within the
brain stem synthesize a variety of melanin called neuromelanin.
True melanins are complicated,high molecular weight polymers attached to a
structural protein (to form melanoproteins) and in humans there are two classes, the
brown black eumelanin and redyellow Phaeomelanin both derived from tyrosine
catalysed by the enzyme tyrozinase . The dermis is for the survival of the epidermis and
important morphogenetic signals are exchanged at the interface between the epidermal-
dermal junction during development and postnatally. The dermis can be divided into
superficial papillary layer, and a deeper reticular layer.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
21
Dermis: The dermis is an irregular, moderately soft connective tissue, with a matrix
composed of an inter woven collageneous and elastic network in an amorphous ground
substance of glycosamino glycans, glycoproteins and bound water, which accommodates
nerves, blood vessels, lymphatics, epidermal appendages and a changing population of
cells. The dermis provides considerable strength to skin by virtue of the number and
arrangement of its collagen fibres, which give it tensile strength and it has elastic recoil,
because of its elastic fibres.
Layers of dermis:
1. Papillary Layer:- This is immediately deep to the epidermis and is specialized to
provide mechanical anchorage, metabolic support and trophic maintainance to the
overlying tissue as well as housing rich networks of sensory nerve endings and
blood vessels. Its superficial surface is marked by numerous papillae which
interdigitae with recesses in the base of the epidermis and form the dermal-
epidermal junction at the interface. The papillae have round or blunt apices which
may be divided into several cusps. In skin especially in regions with little
mechanical stress and minimal sensitivity, papillae are few and very small, while in
thick skin of the palm and sole of the foot, they are much larger, closely integrated,
and arranged in curved parallel lines following the pattern of ridges and grooves
typical of these surfaces. Lying under each epidermal ridge are two longitudinal
rows of papillae or either side of epidermal retepegs through which the sweat ducts
pass on the way to the surface. Each papilla contains dense collagen fibres, elastic
fibrils, microfibrils, attached to the basal lamina. Also present in thick hairless skin
meissner’s corpuscular nerve endings.
2. Reticular Layer: This merges with the deep aspect of the papillary layer. Its
bundles of collagen fibres are thick than those in the papillary layer and interlace
with them and with each other form a strong yet deformable three dimensional
lattice in which many fibres are parallel to each other and within which lies a
variable number of elastic fibres. The Orientation of the collagenfibres may be
related to the direction of action of the mechanical forces to which the dermis is
subjected and may be involved in the development of the skin surface lines.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
22
ULTRASTRUCTURE OF MELANOGENESIS:
Melanocyte is a dendrite non-keratinocyte, lacking desmosomal contacts with
apposed keratinocytes. The nucleus is large round and euchromatic.
In the cytoplasm are intermediate filaments, a prominent golgi complex and
vesicles, associated granular endoplasmic reticulum, mitochondria and coated vesicles
together with a characteristic marker organelle, the melanosome.
The melanosome is a membrane bound structure which undergoes a sequence of
four developmental stages during which melanin is synthesized and deposited within it by
the tyrosine – tyrosinase reaction.
Stage –I Stage I melanosome is spherical vacuole, derived probably from the rough
endoplasmic reticulum, and containing filamento - amorphous structural protein and
vesiculo globular bodies.
Stage-II Stage II Eumelanosomes become spherical or ellipsoid and the inner
matrix becomes organized into filamentous sheets exhibiting a 9nm periodicity.
Stage-III At Stage III melanin begins to be deposited on the innersheets, gradually
observing their arrangement, until densely pigmented.
Stage-IV is reached, exhibiting no other internal structures apart from non-
melanized vesiculo globular bodies. Phaeomelanosomes retain their spherical shape
throughout all stages.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
23
In most active melanocytes, melanosomes of the four stages are present. When
mature, stage IV melanosomes move into the dendrites along the surfaces of
microtubules and are transferred to keratinocytes by a special type of phagocytosis, with
subsequent liberation of melanosomes into the keratinocytes cytoplasm.
Hence colour of the skin plays a vital role in protecting the humans from various
physical, chemical agents and harmful effect of sunlight.
APPENDAGES OF THE SKIN:
Organs that develop from the embryonic epidermis – hair, sweat glands,
sebaceous glands, nails ceruminous glands, have a host of important functions to
perform. Hair and nails protect the body. The sweat glands help regulate body
temperature. The sebaceous glands produce an oily substance the sebum and ceruminous
glands provide waxy secretion in the ear canal. Skin along with its appendages forms the
integumentary system72-73.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
24
SHAREERA KRIYA
Ayurveda defines “Shareera” as “Sheeryate iti Shareeram” means the one which
constantly undergoes wear and tear. This applies to all the organs which constitute the
shareera, particularly the skin.
As defined by Shabdakalpadrumam. “Twachati Samvrunoti medo shonithadikam
iti”74 Twak covers the underlying rakta, mamsa, medo dhatus. Twak not only covers the
entire body area but also forms a strong physical barrier against microbial invasion. It
protects the body against mechanical, chemical, thermal, osmotic and photo damage. It is
major site of inter communication between the body and environment.
Second vital function of the twak is to impart Varna or the colour to the body and
its structures. It reflects the luster and brilliance present in it.
The Varna of an individual is determined in the embryonic stage of life. It is a
rasaja bhava75. The tejomahabhuta is the main factor in determining the varna76. The kind
of food taken during pregnancy also determines the colour. The four prakrut varnas
formed by the combination of different mahabhutas.
Tejo+Jala = Gouravarna
Tejo+Prithvi = Krishna varna
Prithvi + Akash = Krishna – Shyama
Jala + Akash = Goura – Shyam
Charaka has attributed the Varna aspect to the udana vata (one among
panchavidha vatas). 77 The vital functions of Pitta are mentioned as production of normal
and abnormal temperature in the body as well as normal or abnormal colour of the
Skin 78.
Among the five types of Pitta, imparting colour to the skin is a specialized
function of the Bhrajakapitta79. As pitta is involved in the above said function, kapha
builds the texture of the skin making it supple, shiny and strong.80

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
25
There are two major aspects of varna-(i) Prabha (brilliance of the skin) (ii) Chaya
(Substratum of the colour) Prabha is of 7 types- rakta, Peeta, Sita, Syava, Harita,
Pandura, Asita. Prabha specifies the colour of an individual. Chaya is of 5 types,
according to the panchamahabutas 81. Nabhasi, Vayavi, Agneeyi, Ambasi, Parthivi and is
the substratum of the colour. Prabha is reflected to farther distance but chaya can be
appreciated only from a close view. Prabha and chaya are inseparable aspects of Varna
and their reflection is the vital function of Prakrit pitta. In a deranged state, pitta exhibits
abnormal colours.
Amongst the dhatus, twak is closely related to rasadhatu. It derives nutrition from
the rasadhatu through its channels. The texture of the skin is depended on the quality of
nutrition provided 82
Sweda, which is a mala of medodhatu, is expelled out through skin. But in normal
state it acts like a dhatu. It is held in the skin, thereby moisturizing it83.
Tridoshas have their own specific properties by the virtue of which they perform
various functions. “Ushma” 84 is the inherent property of pitta, which enables it perform
thermoregulation and helps in eliciting the lustre of the skin85
Applied aspect:
In ksheena avastha of pitta “Prabhahani” is noticed 86
If pitta prahopakara diet is consumed it vitiates pitta causing digestion of the cells
producing colour to the hair leading to a condition called “Palityam”87
In a vitiated state vata, pitta and kapha exhibit black, yellow and white colour
respectively.88

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
26
BHARAJAKA PITTA & ITS FUNCTIONS:
It has been specified by sushruta that production of colour, exhibition of luster of
skin are the functions of Bhrajakapitta 89
The word Bhrajaka is derived from “Bhraj Dhatu meaning “Deepti” or “Kanti”
‘Sushruta’ mentioned that Bhrajaka pitta resides in the skin. ‘Dalhana’ Commented that
Bhrajakapitta resides in the bahyatwak i.e. avabhasini. 90 Hence it is mentioned in the
reference of avabhasini that its main function is reflection of colour & luster.
Vagbatta also stated that Bhrajaka pitta is located in the skin and reflects the
radiance of the skin.91 Arunadutta commented that Bhrajaka pitta performs functions like
“deepana” “Pachana” of the substances used for abhyanga, lepa, Parisheka92
Chakrapani mentioned that variations in the body temperature and colour are the
functions of bhrajaka pitta93.
Dalhana stated absorption and digestion of the substances used together with oils
and decoctions used for sprinkling over the body is also done by the Bhrajakapitta.
Bhela Samhita has also described the function of Bhrajakapitta as providing
ushma and Prabha to the body94 .Hence it can be concluded that Bhrajaka pitta resides in
the avabhasini the first layer of twak and performs vital function like.
Providing luster and brilliance to the skin.
Helps in thermoregulation of the body.
Capable fo presystemic metabolism of drugs and other substances applied
topically through the process of “abhyanga” “parisheka” “avagahana” & “lepa”.
Applied aspect: Any derangement in the Bhrajakapitta functions leads to alteration of
skin colour and impaired thermo regulation. In the present disease switram, pathology is
noted due to the impairment of this pitta.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
27
The third vital function of twak is thermo regulation. By the virtue of pitta
(Bhrajaka) located in the skin this function is performed. “The Ushma” property of pitta
aides in this function. Any derangement of pitta leads to “mandoanala” condition and
“Sheetam” 95 abnormal cold sensation to the body.
The fourth important function of twak is being a sensory organ. Twak is one
among the pancha gyanendriyas97. It is seat for the vata97. And “Sparsha” or the tactile
sensation is the inherent property of vata98 among the panchavidha vatas; the Pranavata
controls all the indriyas99. All kinds of sensations like touch, temperature, pain, pleasure
are perceived by the skin.
The fifth function of the skin is excretion. It is the channel for the excretion of
sweda which is considered as a mala of the body. If sweda is not generated sufficiently it
leads to bad odour, Cracks in the skin and hairfall.100
Sixth function of the twak is to act like channel or marga. Twak is categorized
under shakha101 along with other dhatus and shakha is classified under bahyaroga
marga102 .This rogamarga help in manifestation of the diseases and prognosis can be
known. Certain shodhana procedures are done to transfer the dhoshas from shaka to
kosta. Hence skin or twak also acts as a channel. It also lodges the nakha and smashru
which are the malas of asthi.
Hence, it can be said that the twak is a tridoshaja bhava in which vata acts as a
initiative principle pitta acts a metabolic principle and kapha is a preservative principle.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
28
PHYSIOLOGY OF THE SKIN
The skin is the largest organ of the body, being on the surface and continually
exposed to injury. It has to be both strong and supple to resist the wear and tear. It forms
the integumentary system along with its derivatives like hair, nails, sweat and sebaceous
glands.
It forms about 8% of the total body mass and its surface area varies with height
and weight.
Functions of the skin:
1. Protection: The skin covers the entire body. It forms self renewing and self
repairing interface between the body and its environment it is major site of inter
communication in both directions between the two. Within limits it forms an
effective barrier against microbial invasion, and has properties which can protect
against mechanical, chemical, osmotic, thermal and photo damage.
2. Thermoregulation:- In response to high environmental temperature of strenuous
exercise, the evaporation of the sweat from the skin surface lowers an elevated
body temperature to normal. In response to low environmental temperature
production of sweat is decreased, which helps to conserve heat. Apart from this,
changes in the blood flow also regulate body temperature. The rich vasculature of
the skin has a generous rescue to meet the requirements of wounding and repair,
so common on surface. Dilatation can increase the flood flow 100 fold, assisting
the thermo regulation.
3. Sensation: Skin is a major sense organ, richly supplied by nerve terminals and
specialized receptors for touch, temperature, pain, pleasure stimuli.
4. Excretion: Besides removing heat and some water from the body, sweat is also a
vehicle for excretion of small amounts of salts and several organic compounds.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
29
5. Synthesis of Vitamin D: It can be regarded as endocrine organ as it carries out
many biochemical synthetic processes (Boyce 1994) including formation of
vitamin D. It can synthesize vitamin D from calciferol in the presence of sunlight.
Apart from synthesizing vitamin D it also helps in the synthesis of cytokines and
growth factors. Cytokines include inter leukins, interferons.
6. Immunity: It is an important site of immuno-surveillance against the entry of
antigens and initiation of primary immune response.
7. Frictional property: Skin has good frictional properties, assisting in locomotion
and manipulation by its texture. It is elastic, and can be stretched and compressed
within limits. It is capable of absorption and excretion and selectively and
regionally permeable to a variety of chemical substances.
8. Skin Colour: The colour of human skin derives from and varies with the amount
of blood (and its degree of oxygenation) in the cutaneous circulation, the
thickness of the stratum corneum and the certainty of specialized cells producing
the pigment melanin. Melanin has protective role against ultraviolet radiation, and
acts as a scavenger of harmful free radicals produced under this and other
circumstances. Racial variations in the colour are mainly due to the differences in
the amount, type, distribution of melanin and are genetically determined.
The anterior pituitary gland or the adeno hypophysis secretes hormones that
regulate a wide range of bodily activities including skin pigmentation. Some cortiotrophs
of remnants of pars intermedia secrete MSH – melanocytes stimulating hormone which
effects the skin pigmentation. MSH increases skin pigmentation by stimulating the
dispersion of melanin granules in melanocytes in amphibians. Its exact role in humans is
unknown.
Three pigments, melanin, carotene and haemoglobin give colour to the skin.
Melanin is located mostly in the epidermis, carotene in dermis and haemoglobin in the
red blood corpuscles.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
30
The amount of melanin varies the skin colour. Melanocytes are most plentiful in
the nucous membrane, penis, nipple of the breast, areola, face and he extremities. The
numbers of melanocytes are same in all the races but the amount of melanin produced
decides the colour.
Melanocytes synthesize melanin from the amino acid tyrosine, in the presence of
an enzyme tyrosinase in an organelle melanosome. Exposure to ultraviolet radiation
increases the enzymatic activity leading to the darkness of the skin which further protects
the body from ultraviolet radiation.
In this condition called VITILIGO there is partial or complete loss of melanocytes
from patches of skin thereby producing hypopigmented spots. The colour of the hair is
also due to the substance melanin, absence of which causes white colour of the hair. The
cells melanocytes are scattered in the matrix of the bulb of the hair.
TYROSINASE, AND SYNTHESIS OF MELANINS:
Tyrosinase is a copper containing metallo enzyme, present in the form of several
isozymes, which catalyses initial stages of the synthesis of tyrosine – melanin.
It is formed by ribosomes on the granular endoplasmic reticulum, conveyed to the
golgi complex, glycosylated and incorporated into coated vesicles which attach to
the limiting membrane of the stage I melanosome, liberating active enzyme.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
31
ILLUSTRATION-1:
The first two steps include oxidation of tyrosine to DOPA
OXIDATION
TYROSINE DOPA
TYROSINASE
Oxidation of DOPA to Dopaquinone
OXIDATION
DOPA DOPAQUINONE
TYROSINASE
In eumelanin synthesis, dopachrome is formed converted into dihydroxyindoles
and 5-6 dihydroxy indoles, 2-dicarboxylic acid.
The final stages in the pathway to melanin essentially involves complex
polymerizations in which tyrosinase may again be involved.
In phaeo melanin synthesis, the amino acid cysteine is added to dopaquinone to
form 5-S cysteinyldopa.
Most natural melanins are mixture of eumelanins and phaeomelanin
Dopaquinone Dopachrome
dihydroxyindoles
Dopachrome Oxidoreductase
Dopachrome tautomerase
5-6 dihydroxy indoles and2-dicarboxylic acid

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
32
FUNCTIONS OF MELANINS:
Melanin has biophysical and biochemical properties related to its functions in the
skin.
It protects against the damaging effects of the ultra violet radiation on DNA
through its special absorptive electron-photon coupling and amorphous
semiconductor properties, whereby it can absorb any different types of energy and
dissipate them in the form of vibrational modes or heat.
Its redox capacity makes it an efficient scavenger of damaging free radicals,
however generated, and its ability to bind to a variety of metal ions and drugs
suffest it can act as an anti toxic agent.
However, if the energy input is too great, these properties can be expressed in the
output of toxins activated, chemical species which can be damaging.
Another disadvantage is that a high concentration of melanin in relation to
incident solar UV may adversely affect synthesis of vitamin D.
DETERMINATION AND CONTROL OF MELANIN PIGMENTATION:
Melanin Pigmentation of human skin can be analysed in two bases (1)
Constitutive (2) facultative
Constitutive pigmentation is the intrinsic level, genetically determined.
Facultative pigmentation comprises reversible changes induced by environmental
agents eg: UV and X-radiation, chemicals and hormonal influences.
Genetics: Specific genes can influence differentiation of neural crest cells into
melanoblasts, and also melano blast migration to the skin, their differentiation
with melanocytes and morphological features of these such as shape, size, and

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
33
length of dendrites, which in turn determine the size of the pool of keratinocytes
to which each cell transfers its melanosomes.
Other genes acting primarily within the melanocyte control the synthesis of
tyrosinase, its type and activity, the type of melanin synthesized the size, shape,
protein structure and number of melanosomes, their degree of melanization and
their rate of transfer to keratinocytes.
Constitutive melanin pigmentation in man is probably under similar precise
genetic control.
Racial variations in pigmentation are due to differences in melanocyte
morphology and activity of melanocytes than to numerical differences.
In heavily pigmented skins the cells tend to be larger, more dendritic and to
contain more and larger Stage III and IV melanosomes than melanocytes.
Ultraviolet radiation: The response of the melanin pigmentary system to
ultraviolet varies with genetic and constitutional factors. It includes immediate
tanning, or pigment darkening, which can occur within few minutes due to photo
oxidation of preexisting melanin.
Delayed tanning occurs after about 48hrs and involves stimulation of new
melanogenesis within the melanocytes, and transfer of additional melanosomes to
keratinocytes. There may also be some increase in size of active melanocytes and
their numbers.
Lower frequency UV band induces synthesis of keratinocytes of b-FGF, as well
as inter leukin I which induces them to produce melanocyte stimulating
hormone a known stimulant of melanogenesis.
Hormonal Influences: In amphibians MSH from the anterior lobe of the
hypophysis and melatonin, a skin lightening hormone secreted by the pineal, are
involved in pigmentary alterations.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
34
Their importance as normal regulatory factors in man is unclear.
In pregnancy, higher levels of circulating Oestrogens and progesterone are
responsible for the increased melanization of the face, abdominal and genital skin
and the nipple and areola.
A number of other factors operating within the epidermis such as interleukins,
arachidonic acid, prostaglandins and various cytokines, also affect melanogenesis.
Level of pigmentation at anytime represents a balance between a large number of
competing influences between constitutive and facultative, and these must be
taken into account in the analysis and diagnosis of hypo and hyperpigmentary
disorders103.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
35
NIDANA
Nidana is defined as the etiological factors responsible for causing the disease104
All the diseases affecting the skin in particular are described under one heading “kusta
rogas”. As switra also affects the skin it is described in this chapter.
All the acharyas have mentioned a common nidana for kusta and switra.105
Acharya charaka has mentioned a vishesha nidana for switra.106
The etiological factor can be sub divided into
a. Aharaja nidana
b. Viharaja nidan
c. Chikista sambandhi
d. Anyaja
a. Aharaja nidan:
Vagbatta mentioned, a pregnant women consuming excessive kaphakara ahara,
the baby shall be affected with switra.107
Viruddha ahara
Mithyahara
Asatmya bhojana
Ahita bhojana
Adhika matra Bhojana
Ajeerna anantara bhojanam
Vidhi viruddha ahara sevanam
Kuvidhi of langhana
Sheetala – ushna ahara sevanam
Drava, snigdha, guru padarthas
Gramya, anupa, jaleeyamamsa sevanam, anantharam dugda sevanam
Navanna, dadhi, matsya, lavana, amla, masha, mulaka, pisti, tila, ksheera, Guda
sevanam

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
36
Tila, guda, dudga sevanam
Chilachima variety of fish108.
Seven dietery factors (7) specially mentioned by vangasena109
Tila, Taila, Kulatthi, Valmika roga, Lingaroga, Mahisha dadhi, Vruntakam.
b. Viharaja Nidan
Chardi, Mala-mutradi vegadharana
Ati vyayamam
Ati Santapasevanam
Vyayamam in ajeernaavastha
Mithya vihara
Diva swapnam
Garma srama, Bhayarthanam sheethambu sevanam.
c. Chikista sambandhi Nidana:
Vagbatta mentioned usage of savisha jalouka in rakta mokshana leads to switra at
that site 110
Snehapana anantaram doing vyayamama,or vyavayam leads to skin diseases111
Suppression of vamana vegas or doing vyayamam or maithuna after vamana leads
to skin diseases112.
Panchakarma apacharas specifically produces skin diseases113
Taking apakwa Vajra, Vaikrantha, Nag, Loha, Hingula, Rasakarpur, Tutha leads
to skin diseases114.
Apakwa Hartal bhasma and Vanga bhasma leads to switra specifically.115
Vaidya Nimittija:
Snehapan after attaining samyak snigdha lakshnas causes sneha vyapat which
leads to kustarogas116.
Doing dushita rakta stambana leads to kilasa and kusta117

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
37
d. Anya nidana:
In adibala pravrutti Sukra – shonitha beeja doshas leads to kusta rogas in the
progeny118
Manasika causes like bhaya, krodha leads to skin diseases119
Dadga and kshatas produce switra120
Bhoja mentioned vrana and parasparsha to be the cause for switra121
Manu smriti described stealing of clothes and wealth leads to switra122
Harita samhita mentioned stealing of silver leads to switra123
Kashyapa mentions abstinence from yagnas, yagas, Homas, Bali, Improper athidi
sevana leads to switra.124
Papakarmas of previous births
Brahmana, Stri, Sajjana, go hatya
Disrespecting parents, insulting Gods
Having died of skin disease in the previous birth125
Vishesha Nidana specially mentioned by charaka126
Viruddha annapana sevana
Vacham asatyam
Papakarmas
Krutagna bhavas
Ninda suranam
Guru garshanam
Poorva kruta karmas

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
38
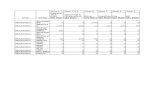
Aharaja Nidana:
Table – 4
S.No. Nidana C.S. S.S A.H M.Ni B.P Va.S
1. Garbhini consuming excessivekaphakara ahara
- - + - - -
2. Virudha ahara + + + + + +
3. Mithyahara - + + - - +
4. Asatmya Bhojan - + - - - -
5. Ahita Bhojan - + - - - -
6. Adhika matra Bhojan - - - + - +
7. Ajeernam anantara Bhojanam - + - + + +
8. Vidhi virudha ahara sevana - - - - + -
9. Kuvidhi of Langana - - - - - +
10. Sheetala – Ushna Ahara Sevanam - - - + + +
11. Drava – Snigdha – Guru padartha - + - + + +
12. Tila guda – dugda sevanam - - - + + +
13. Chilachima variety of fish + - - - - -
14. Gramya, anupa, jaleeyamamsasevanam,Anantaram dugda sevanam
- + - - - -
15. Navanna, dadhi, Matsya Lavana, Amla,Masha, Mulaka, Pisti, tila, Ksheera,Gud sevanam.
- - - + + +
Viharaja Nidana:Table - 5S.No. Nidana C.S. S.S A.H M.Ni B.P Va.S
1. Chardi, Mala-mutradi vegadharana - + - + + +2. Ati vyayayam - - - - - +3. Ati santapasevanam - - - + + +4. Vyavayam in ajeernavastha - - - - + +5. Mithya vihara - - + - - -6. Diva swapnam - - - + + +7. Garma, Srama, Bhayarthanam
sheethambu sevanam- + - + + +

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
39
Chikitsa Sambandhi Nidan:
Table - 6
S.No. Nidana C.S. S.S A.H M.Ni B.P Va.S1. Savisha Jalouka Prayog - - + + - -2. Snehapana anantaravyayamam or
maithun- + - - - -
3. Suppression of vamanadi vegas - - - + - +4. Doing vyayama or maithun after
vamana- + - - - -
5. Panchakarma apacharas - - - + + -6. Snehapana after attaining samyak
snigdha lakshanas+ - - - - -
7. Dushitha raktha stambhana + - - - - -
Anya Nidan:
Table - 7
S.No. Nidana C.S. S.S A.H M.N B.P Va.S M.S B.J Ka
1. Sukra shonitha beejadoshas
- + - - - - - - -
2. Bhaya, Krodha - - - + + - - - -
3. Kshata, Dagda - - + - - - - - -
4. Vranas - - - - - - - + -
5. Para sparsha - - - - - - - + -
6. Stealing of clothes &
Wealth
- - - - - - + - -
7. Abstinence fromyagna, homa, bali
- - - - - - - - +
8. Papakarmas ofprevious births
+ + + - - - - - -
9. Brahmana, Stri,Sajjana go Hatya
- + + + - - - - -
10. Vipra guru garshana + - - - + + - - -
11. Vacham asatyam + - - - - - - - -
12. Ninda suranam + - + - - - - - -
13. Having died of skindiseases in previousbirth
- + - - - - - - -

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
40
ETIOLOGY
The etiology of vitiligo is unknown but triggering / precipitating factors areidentified.
Triggering / Precipitating factors:
It is difficult to precisely define the triggering factors for vitiligo. Neverthless it
is essential to elicit the details of history of emotional stress, drug intake, infections,
trauma / injury (Koebner’s phenomenon) 127 existant prior to the development of vitiligo
lesions .128-130
It is believed that major oxidative stress occurs in vitiligo skin, which is
evidenced by low catalase levels and cellular vacuolization in the epidermis .131-132
several factors may contribute to the oxidative stress, thus leading to the accumulation of
epidermal hydrogen peroxide. The presence of the hydrogen peroxide can be
demonstrated invivo by using non-invasive Fourier transform Raman Spectro
Scopy133-134
ILLUSTRATION-2:
VITILIGO TRIGGERING / PRECIPITATING FACTORS ,
THEIR ROLE IN PATHOGENESIS135-138
Triggering Molecular level Genetic factorsFactors Changes
1. Nutritional Deficiency
2. Emotional stress Biochemical changes Normal Skin
3. Drugs
4. Infections Enzymatic Disturbances Previtiligo
5. Focal sepsis and toxins Auto Immunity and VitiligoImmune dysfunction
6. Exposure to chemical
7. Oxidative stress Epidermal hydrogen peroxide VITILIGOaccumulation

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
41
POORVARUPAS
Poorvarupas are defined as the prodromal symptoms of a disease to bemanifested.
Madhukosh commentary defined poorvarupas as Bhavi Vyadhi Prabodhakas139
Generally the poorvarupas are only indicators of a particular disease to be manifested.
Some times they are avyaktam not present at all and at times they are minimally
exhibited.140. The disease switram does not exhibit any poorvarupas, but as it has the
same causative factors like that of kusta141, the poorva rupas exhibited by kusta rogas can
be considered for switram occasionally.
Kusta Poorvarupas:
Sparsha Agnanam142
Atiswedam
Aswedam
Vivarnyam
Loma harsha
Kharatwam
Kandu
Toda
Srama143
Klama
Shula in vrana
Sheegrautpatti
Chira Stithiti
Daha
Suptata
Ruksham
Pipasa

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
42
Gouravam
Doubalyam
Vepathu
Pidaka
Arunshi
Ativedana
Kota utpatti
Ati bhrama
Ati kopanam 144
Asruja Karshanyam

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
43
RUPA
Rupa can be defined as the clinical features of the manifested disease. They are
the subjective evidences of a disease. They are exhibited only after the complete
manifestation of a disease. In the Shatkriyakalas the rupas are exhibited in the
vyaktavasta145. Dalhana commented that the rupas are exhibited after the completion of
Dosha – dushya samurchana and the pratyatmaka lingam or the cardinal symptom is first
exhibited.
Eswarasena’s commentary on Madhava nidan defined rupam146
“Vyadhi hi Swarupam…….
Tad Vyaktam Tadrupam.
Madhukosh defined rupam as147
“Utpanna vyadhi bodhakameva lingam rupam”
In switram, according to definition of kashyapa 148 expressions of white colour
patches on the body is the Pratyatmaka linga of switram.
Sushruta defined the rupas as “Twagtam eva aparisravi”149. The patch involves
the skin and has no oozing tendency
Vishista dosha lakshanas:
According to classical texts the vataja, pittaja, sleshmaja types of switram have
been mentioned. The tridoshas invade rakta, mamsa, and medodhatus respectively and
produce lakshanas accordingly.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
44
Vataja:
Mandala
Aruna varnam or rakta varnam
Ruksham
Sparsha katinatvam
Parusham
Keshanashanam
Paridwamsi (Romapatrari)
Pittaja
Tamra Varnam
Kamala Patravat
Daham
Roma Vidwamsam
Sleshmaja
Swetavarnam
Snigdam
Stulam
Kandu yuktam
Guru
Ghanam
Charaka mentioned three varieties of the disease by the virtue of involvement of
dhatus150.
Daruna: When rakta dhatu is invaded by vata dosha it exhibits raktavarna151
Aruna: Mamsadhatu invaded by Pitta dosha it exhibits tamravarna
Switra: Medodhatu invaded by kapha dosha it exhibits swethavarna

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
45
Rupas:
Table -8
S.No. Lakshanas C.S S.S152 A.H153 M.Ni154 Sha.Sha B.P
Vataja
1. Mandalam - + - + - -
2. Arunavarnam - + + + - -
3. Raktavarnam + - - - - +
4. Rooksham - - + - - +
5. Sparsha katinatvam - + - + - -
6. Parusham - + - + - -
7. Keshanashanam - + - + - -
8. Paridwamsi - + - + - -
Pittaja
1. Tamravarnam + - + - - +
2. Kamalapatravat - + + + - +
3. Daham - + + + - +
4. Romavidvamsam - - + - - +
Sleshmaja
1. Swetavarnam + + + + - +
2. Snigdam - + - + - -
3. Stulam - + - + - -
4. Kandu yuktam - + + + - +
5. Guru - - + - - +
6. Ghanam - - + - - +

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
46
CLINICAL FEATURES
EPIDEMIOLOGY:
Vitiligo occurs world wide with an overall prevalence of 1%. However, its
incidence ranges from 0.1 >to 8.8% 155-161. The highest incidence of the condition has
been recorded in India followed by Mexico & Japan.
Behl et.al162-163 had organized camps in rural areas and industrial pockets in India
to evaluate the status of vitiligo. Its incidence was found to be higher in villagers living
near dyeing, printing, carpet industries. A higher incidence of vitiligo in such areas may
be due to inclusion of cases with chemically induced depigmentation by industrial
phenols, quinone’s which might have a completely different pathomechanism. Its
incidence however was relatively low amongst those residing adjoining copper mines.
SEX INCIDENCE:
Adults and children of both sexes are equally affected although the greater
number of reports among females is probably due to the greater social consequences to
women and girls affected by this condition164-171
AGE INCIDENCE:
Almost half the patients present before the age of 20 years and nearly 70-80%
before the age of 30 years.172-176
FAMILY HISTORY:
The proportion of patients with positive family history varies from one part of the
world to another. In India, in particular, it ranges from 6.25-18%. In some studies it is as
high as 40%. The mode of transmission of vitiligo is quite complex. It is probably
polygenic with a variable penetrance177-181

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
47
PERCENTAGE OF INCIDENCE:
1947 - Calcutta / India - 6%
1958 - Vellore / India - 4%
1969 - Amaravati/ India - 8%
1972 - Delhi / India - 8.8%
1974 - Goa / India - 2.9%
1988 - Delhi / India - 1.25%
The difference in its incidence may be due to higher reporting of vitiligo in population
where apparent colour contrast may force them to seek an early consultation.
CLINICAL FEATURES:
Vitiligo is characterized by the appearance of patchy discolouration evident in the
form of typical chalky – white or milky white macules.
The macules are round and oval in shape with scalloped margins 182-183
The size of the macules may vary from few mm to several cms with the lesions
affecting the skin and or mucous membrances.
The lesions are asymptomatic although itching, burning may precede or
accompany the onset of lesions in few patients .184-185
Vitiligo is a slow and progressive disease and may have remissions and
exacerbations correlating with trigerring events 186-187
Occassionally the lesions of vitiligo may begin to form around a pigmented
naevus188(Sutton’s nevus, Leucoderma aquisitum centrifugum) and then go on to affect
distant regions 189.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
48
Although any part of the skin or mucous membrane is amenable to develop
vitiligo, the disease has a predilection for normal hyperpigmented regions such as the
face, groin, axillae, areola, and genitalia.
Furthermore lesions may develop in areas like, ankles, elbows, knees, which are
subjected to repeated trauma / friction, an outcome of koebner’s phenomenon190.
In the event of extensive disease the lesions are symmetrically distributed 191-193
with an exclusive dermatomal distribution or mucous membrane involvement 194-196
Lip-tip syndrome, another variant of vitiligo is characterized by depigmentation
fo the terminal phalanges and the lips.
CLINICAL VARIANTS:
1. Trichrome Vitiligo: Recognized by the presence of a narrow to broad
intermediate colour zone between vitiligo macule and normal pigmented
surrounding skin. It is a variant of unstable vitiligo 197.
2. Quadrichrome Vitiligo: It is well documented fourth colour in vitiligo lesions,
usually seen in darker skin types. A macular perifollicular or marginal hyper
pigmentation is its salient feature and denotes a repigmentating disease.
3. Penta chrome vitiligo: Infrequently encountered variant in which there is a
sequential display of white, tan, brown, blue-gray hyperpigmentation and normal
skin. Black Skinned individual are predisposed to have this disorder198
4. Blue vitiligo: It usually corresponds to vitiligo macules occurring at the site of
post inflammatory hypermelanosis 199.
5. Inflammatory Vitiligo: It is an entity which may reveal an erythematous, raised
border in a vitiligo macule with frequent itching / oozing. These can be induced
by aggressive therapy200-202.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
49
CLINICAL FEATURES OF VARIOUS TYPES OF VITILIGO:
1. Localized:
Focal: One or more macules in one area, but not clearly as in segmental or
Zosteriform distribution.
Segmental: One or more macules in quasidermatomal pattern.
Mucosal: Involvement of mucosal membranes alone.
2. Generalized
Acrofacial: Involvement of distal extremities and face.
Vulgaris: Scattered macules over the body.
Mixed: Acrofacial and vulgaris involvement or segmental and acrofacial.
3. Universal: Complete or nearly complete depigmentation.
According to progression and prognosis
Segmental: Has an early onset in life, spreads rapidly in affected area. The cause may arrest
and depigmented patches can persist unchanged for the life.
Vitiligo Zosteriformis: Macules distributed along a dermatome or lines of body
cleavage.
Non Segmental:
Shows poor prognosis. Includes all types of vitiligo, except segmental type.
Vitiligo _areata: 1 or 2 macules (Focal, Localized or partial).
Vitiligo acrofacialis : Macules affecting face and tips of hands and feet.
Vitiligo vulgaris: Scattered macules over the body.
Vitiligo mucosal: Involvement of mucosal membranes alone.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
50
According to clinical stages:
Progressive Vitiligo: Developing new lesions .
Increasing old lesions
Ill defined border of lesion
Quiescent stage: No appearance of new lesions
Stationary old lesions
Well defined, hyperpigmented borders
ASSOCIATIONS OF VITILIGO:
Cutaneous associations203-210
Premature graying of hair
Leucotricha
Halo nevus
Lichen planus
Alopecia areata
Occasionally other skin disorders like Dermatitis herpetiformis, Giant congenital
melanocytic nevus, Chronic urticaria, Malignant melanoma have been seen in association
with vitiligo.
Other interesting autoimmune associations include Morphea, and Hashimoto’s
thyrioditis 211.
While presenting strong direct and indirect evidence of auto immune etiology of
alopecia areata, Hordinsky and Ericson212 stressed its association with vitiligo in many
patients.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
51
Occular associations:
Vogt-Koyanagi-Harada syndrome213-218 refers to full constellation of vitiligo,
Poliosis and Alopecia with pan uvetis and auditory and neurological manifestations.
However iris, retinal pigmentary abnormalities may be present as isolated
findings in vitiligo patients. Choroidal abnormalities and irites may also be present 219-221
Systemic associations:
Hypo / hyper thyroidism, Diabetes mellitus, Addisions disease, Pernicious
anaemia, Lymphoma, Leukemia, HIV, Autoimmune poly endocrinopathy ,Candidiasis
,Ectodermal dystrophy.
CHILDHOOD VITILIGO:
Morphological characteristics in childhood vitiligo are more or less identical to
those of adult onset vitiligo. Interestingly there has been steady increase in the evidence
of child hood vitiligo during past two decades222.
CONTACT VITILIGO:
Contact vitiligo is an acquired leucoderma as a result of repeated topical or
systemic exposure to variety of chemicals223. These chemicals are mainly alley phenols,
catechols used in manufacturing plastics, resins, synthetics, rubber, paints, petroleum,
deodorants, germicides, insectides, photographic chemicals, varnishes etc., These
chemicals are also present in certain objects like footware, plastic watch strap and
bindis.224-225

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
52
SAMPRAPTI
Samprapti is defined as the phenomenon of dosha-dushya samurcchana226. The
complete process of manifestation of a disease is explained in this context.
The nidana and samprapti for kusta and switra are similar 227. The whole process
of samprapti can be understood through shatkriyakalas228
Sanchaya
Prakopa Dosha Prakopa avastha
Prasara
Stanasamshryam Dosha – dusya samurcchana
Vyakti Vyadhi utpatti avastha
Bheda
The knowledge of samprapti is essential to break the chain of pathogenesis to
prevent further progression of the disease and to implement specific treatment at different
stages of pathogenesis229.
1. SANCHAYAM: is the accumulation of vitiated doshas in their respective places230.
The doshas remain in equilibrium, unless disturbed by external causes.
Viruddha ahara-vihara, Manasika karanas like Bhaya, krodha, papakarnas, sadvrut
apacharas are the endogenous causes.
Kshata, dagda, vranas, Savishajaloukaprayoga are the exogenous causes. The
exogenous and endogenous causes are responsible for the vitiation of doshas.
Viruddha ahara produces amavisha which is antagonistic to the dhatus, there by
leads to various disease.231
Adhika amla, lavana, ushna, teekshana dravyas cause pitta prakopa leading to
rakta dusti 232

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
53
Virudha vihara, diwaswapnam, atisantapasevanam causes pitta prakopa233
Suppression of natural urges causes vitiation of apanavata and it travels in
pratilomagati disturbs samanavata which in turn disturbs udana vata (responsible
for Varna).
Bhaya, kroda increase rajogunam in the body, which in turn causes vata-pitta
prakopa
Papakarmas, sadvrut apacharas leads to psycho-somatic disturbances, leads to
vitiation of vata pitta doshas234.
In agantuja karanas, directly twakdusti occurs and lakshanas are exhibited, later
on the doshas are vitiated.235
2. PRAKOPA: Prakopa the next stage of sanchaya. The accumulation of vitiated doshas
continues and the doshas are ready to rise above their respective stanas236.
Nidana Factors
Sanchaya Prakopa
Are continued
3. PRASARA: This is the stage where the vitiated doshas get dislodged from their
respective places and start spreading all over the body through siras or channels. In
switra, the vitiated vata, pitta, kapha spread in the body through “Tiryagata Siras” 237
which implies urdwa, adho, tiryak Siras. The doshas spread in all the directions238.
4. STANA SAMSHRAYAM: The most important phase of shatkriyakalas where the
major event “Samprapti” occurs239. Dosha – dushya samurcchana and vyadhi purvarupas
are exhibited in this stage

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
54
Doshas implies the vitiated vata, pitta, kapha and dushyas are twak, rakta, mamsa,
and lasika in kusta, and rakta, mamsa, medo dhatus in switra.
Switra is considered as “Tridhatu Samshrayam”240 which means involvement
of tridoshas and tridhatus (rakta, mamsa, and medodhatus) in the pathogenesis of the
disease241.
The vitiated doshas while moving in the body reach particular dhatus, by the
virtue of obstruction of that particular srotas. They get lodged in that dhatus.242.
The doshas cause “Shithilatwam” of rakta, mamsa, medodhatus and are
expressed out on to the surface i.e. twak. The term “Bahirnischarantou” (bahya desha
prasarantou) is used to denote the mechanism of outward movement of vitiated doshas.243
Charaka mentioned “doshopaghata”244 (being affected by the vitiated doshas) in this
context. The doshas reach “Twak” where they get settled. The twak becomes the place
for stanasamshrayam.
The fourth layer “Tamra” is the site for switra roga.245
No purva rupas are mentioned but as nidana is same for kusta and switra, some
purvarupas of kusta may occasionally appear.
5. VYAKTAVASTHA: The stage of exhibiting the lakshanas of the manifested
disease246. “Mandalas” and “Twak vivarnyam” are seen at the site of manifestation of
vitiated doshas in the skin.
In switra “Sweta Varnam” of twak is seen as a pratyatmaka lingam247.
Switra Produces discolouration of skin only, it does not cause destruction,
putrifaction of dhatus or exudation hence it is “aparisravi” and this feature differentiates
it from Kusta.248
In agantuja karanas like dagdas, kshata, vrana, directly twak dusti occurs causing
“Twak Vaivarnyam” and after that doshas get vitiated.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
55
6. BHEDAVASTHA: The stage of complications or upadravas. If timely intervention is
not done leads to complete depigmentation of the body. Vagbhatta considered switra as
medical emergency as, if not treated on time spreads all over the body and makes it
asadya249.
The disease may go beyond medodhatu, and makes it asadya if not treated
timely.250
Three types of switra are present due to particular dosha predominance and
produce their respective colour on the patch 251
Vataja Involves raktadhatu Raktavarnam
Pittaja Involves mamsadhatu Tamra varnam
Sleshmaja Involves medodhatu Sweta Varnam
Types of Samprapti
Sankhya - 3
Vikalpa - Though sannipatika vyadhi, Ekadoshaja bhedas are alsomentioned
Pradhanya - Switra is a swatantravyadhi
Bala - Depending upon the state of nidana, dosha, dushyas in each
case
Kala - Vyadhi kala not mentioned

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
56
SAMPRAPTI GHATAKAS
Doshas : Pittapradhana tridosha
Dushya : Rakta, mamsa, medo dhatus
Agni : Jataragni, dhatwagni
Ama : Agnimandyam, dhatwagni mandyam
Udbhavastan : Amapakwashyam
Sanchara : Tiryakgata siras
Srotas : Rasa, rakta, mamsa, medo
Srotodusti : Sanga
Adhistana : 4th Layer of twak “Tamra”
Vyaktastana : Twak
Rogamarga : Bahya
Vyadhi Swabhava : Chirakari

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
57
ILLUSTRATION-3:
FLOW CHART
NIDANA
BEEJADOSHAS AHARAJA VIHARAJA MANSIKA PAPAKARMAS VRANA
DAGDA
KSHATAS
BEEJA BHAJA AGNIMANDYAM
AFFECTED
AMA UTPATTI
DOSHA DUSTI
VATA, PITTA, KAPHA
BEEJA BHAGA
AVAYAVA TIRYAKGATA SIRAS
RAKTA, MAMSA, MEDO DHATUS
BAHYAMARGA GAMANTOU
STANASAMSHRAYAM
TWAK DUSTI
BHRAJAKA PITTA DUSTI
SWETA VARNAM
SWITRAM

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
58
PATHOGENESIS OF VITILIGO
There are several diseases marked by lack of pigment in the skin that is grossly
referred to as leucoderma. Some are caused by an inability of melanocytes to produce
melanin, while others are caused by melanocytes either not being present or being
destroyed. The latter are the pathology for the disease VITILIGO.
Vitiligo is a progressive disease in which the melanocytes are gradually destroyed
causing unpigmented areas on the skin. The exact etiology of vitiligo is unknown, but
four main theories exist to explain the pathogenesis of it.
a. Autoimmune hypothesis
b. The neural hypothesis
c. The self destruct hypothesis
d. The growth factor defect hypothesis
It is believed that vitiligo is a polygenic trait and that a convergence theory,
combining elements of different theories is the most accurate etiology.
Vitiligo is not a physically damaging disease. But effects are social and
psychological especially for dark skinned races
a. Auto - immune theory: There is great anecdotal evidence that an auto immune
disorder cause the destruction of melanocytes, and this is accepted as the common cause
of vitiligo
Vitiligo appears in conjunction with several other auto immune disorders, such as
Juvenile diabetes, Addisions disease, Pernicious anaemia and additionally organ specific
antibodies.
If the immune system raises antibodies or cytotoxic T-cells to damage
melanocytes, the mode of action the cells take against the melanocytes could be apoptosis
induction directly against melanocytes or Ig induced Compliment.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
59
There is histological evidence in vitiligo patients that apoptosis is occurring in
unpigmented skin lesions. There is damage to melanocytes and keratinocytes.
Melanocytes exhibit nuclear shrinking, vacuolization, loss of dendrites, and
detachment.
b. Neural Theory: The Peripheral nerve endings may secrete substance that is cytotoxic
to melanocytes and cause their destruction.
This is supported by segmental variety of vitiligo which occurs in specific
dermatomes, indicating the skin is possibly affected by nerves of specific dermatomes.
Vitiligo appears with certain neurological disorders such as encephalitis, trauma
that cause peripheral nerve damage.
Nerve endings in depigmented areas were seen to produce abnormal neuro
peptides, nerve growth factors, and displayed axonal degeneration, these abnormal
chemicals may be toxic to melanocytes.
Depigmented areas showed some abnormal autonomic functions, such as
increased adrenergic toxins, increased norepinepherine, and an increased concentration of
catecholamines. These data then suggested that neurotransmitter release could, have an
affect on melanocyte destruction and depigmentation.
c. Self destruct theory: It is known that some of the intracellular pre-melanogenesis
metabolites are toxic to melanocytes such as dopa, and dopachrome. Normally
melanocytes possess cellular measures to counteract these toxic substances and are
destroyed by leakage of metabolites into the cytoplasm and eventually cell lysis.
There is evidence, that certain hydroquinone derivatives that are similar to these
intra cellular metabolites cause leucoderma.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
60
d. Growth factor Defect hypothesis : It was noted that growth defects of melanocytes
were partially corrected by adding a growth factors to their culture suggesting that growth
defects may be part of pathology of vitiligo.
e. Genetic Influences: There does appear to be a strong genetic influence in vitiligo. A
positive family history has been reported in about 20% of patients.
It does not progress via simple Mendelian pattern but more likely is coded
polygenically.
There is some evidence both proving and disproving involvement of HLA system
in occurrence of vitiligo.
Hence, it is believed that genetic factors play a key role in the pathogenesis of
vitiligo.
f. Convergence Theory: Researchers have begun to lean towards multifaceted etiology,
for vilitigo. This theory states that genetic influences have a role in causing vitiligo in
addition to other elements, such as stress, accumulation of toxic compounds, infection,
auto immunity, mutations, impaired melanocytes proliferation.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
61
SWITRA – BHEDAS
The classification of switra gives the information about of the types of the disease.
It is an attribute of Sankhya samprapti. Classifications are based on different criteria like
Nidan Doshas, Ashraya dhatus and Sadya – asadyata.
I. Based on Nidan: 252 Bhoja classified switra into two types.
1. Doshaja: (endogenous Origin) again sub divided into
a. Atmaja
b. Paraja
2. Vranaja (Exogenous Origin)
II. Based on Doshas: 253
1. Vataja
2. Pittaja
3. Sleshmaja
III. Based on Ashraya Dhatus: 254
1. Accroding to charaka Baluki tantra255
Rakta ashrita Daruna Daruna
Mamsa ashrita Aruna Varuna
Medo ashrita switra switra
IV. Based on Sadhya – asadhyata: 256
1. Sadhya-Curable
2. Asadhya-incurable
Kashyapa257 mentioned 5 types of switra but has not mentioned names or clinical
features. Bhela 258 has mentioned switra to be one among eleven kshudra kustas.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
62
Switra Bhedas:
Table -9
S.No. Types C.S. S.S A.H M.Ni Sa.s B.P B.J Ka.S B.S Bh
3 3 3 3 3 3 2 5 - 3
1. Doshaja - - - - - - + - - -
2. Vranaja - - - - - - + - - -
3. Vataja - + + + + + - - - -
4. Pittaja - + + + + + - - - -
5. Sleshmaja - + + + + + - - - -
6. Raktashrita + - - - - - - - - +
7. Mamsashrita + - - - - - - - - +
8. Midho asshrita + - - - - - - - - +
9. Sadya + + + + + + - - - -
10. Asadya + + + + + + - - - -

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
63
CLASSIFICATION OF VITILIGO
The classification system is important because of special significance assigned to
each type of vitiligo
I. Based on distribution:
1. Localised259: a) focal
b) Segmental
c) Mucosal
2. Generalized: a) Acrofacial
b) Vulgaris
c) Mixed
3. Universal
II.Based on Progression and prognosis: 260
1. Segmental: a) Vitiligo zosteriformis
2. Non Segmental: a) Vitiligo areata
b)Vitiligo acrofacialis
c) Vitiligo Vulgaris
d) Vitiligo mucosal
III. Based on Clinical Stages:261
1. Progressive Vitiligo
2. Quiescent Vitiligo

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
64
SAPEKSHA NIDAN
Sapeksha nidan, otherwise called has vyadhi vyavacchedaka nidan is the
differential diagnosis aspect of the disease. The knowledge is essiential to diagnose a
disease and to implement specific treatment.
In all the classics, the nidana of switra and kusta rogas are mentioned to be
same,262 but they differ in the symptomatic aspect.
Arunadutta specified that, the vitiated doshas affects the dhatus, eats up the hair,
skin, ligaments and cartilages in the kustarogas but these sequential events do not take
place in switra263.
Switra has to be differentiated from sidma kusta which is one of the mahakusta264
because of its close resemblance with the former.
Sapeksha Nidana:
Table - 10
S.No. Features Switra Sidma
1. Classified into Independent Mahakustas
2. Doshas involved Vata, Pitta, Kapha265` Vata-kapha266
3. Dhatus affected Rakta, mamsa, medo dhatus Twak, rakta, Mamsa,lasika
4. Skin layer involved 4th layer Tamra 1st layer avabhasini
5. Poorvarupas Not present Present
6.
a.
Roopas (Clinical features
Colour
White colour patches White, reddish brownpatches(Alabu-Pushpavarnam267
b. Areas involved Anywhere through out thebody
Mainly found on chestand back
c. Extent of layers involved “Twagatam only thesuperficial epidermis isinvolved
Dermis is involved
d. Appearance Centrally hypopigmentedwith hyperpigmented border
External margins arethin, fissured with

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
65
reddish brown or whitecolour centrally
e. Elevation Patch at the skin level, notelevated
Mildly elevated margins
f. Scales Not present When rubbed produce adust like material (RajoGrushtam)
g. Pain Not present Mild pain present onrubbing
h. Itching Not present Present when in contactwith sweat
i. Hair involved The hair of the patch mayturn white (Leucotrichia)
Hair not involved
j. Oozing tendency “Aparisravi” no oozingtendency.
Little purulentdischarges present inchronic stages
k. External causes May be Produced by dagda,vrana, kshatas also
Not due to these factors
l. Symmetry Symmetrical andasymmetrical patchespresent
Mostly asymmetricalpatches present
m. Sensation Not altered Sensation may bealtered
n. Prognosis The deeper the dhatuinvolved, the diseasebecomes incurable
Sadya roga268

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
66
DIFFERENTIAL DIAGNOSIS OF VITILIGO
Generalised vitiligo must be distinguished from Piebaldism, Waarden burg’s
syndrome, Woolf’s syndrome and Ziprokowski-margolis syndrome.
Piebaldism:
Is congenital
Stable and spares the dorsal spine
Hyperpigmented macules are present in white patches
A white forlock is also present on forehead
Characteristic distribution pattern
Waarden burg’s syndrome:
Autosomal disorder
Includes hearing defects
Has characteristic eye features, fundi may be hypopigmented
Along with white forelock, premature graying of scalp, hair, eyebrows, cilia and a
dappled appearance of the skin is seen.
Forehead, neck, chest, abdomen, anterior knees, arms, dorsa of hands are
commonly involved
Woolf’s syndrome:
Piebalism
Deafness
Ziprokowski-margolis syndrome:
Rare congenital syndrome
Occurs in males only
Deaf – mutism
Heterochromic irides
Piebald like hypomelanosis of skin

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
67
Round, oval or geographic hypopigmented macules
Occurs mainly on extremities and trunk
Segmental vitiligo must be distinguished from Nevus depigmentosus, Tuberous
sclerosis, Hypomelanosis of Ito.
Nevus depigmentosus:
Rare, congenital, non familial
Stable quasidermatomal leucoderma
Unilateral macules of varied size
Lesions are white to tan colour with regular or serrated margins
Lesions mostly on trunk, lower abdomen, proximal extremities but may involve
face and neck
Quasinevoid macules with irregular, serrated, feathered margins
Tuberous sclerosis:
Uncommon neurocutaneous syndrome
Appears during early life
Classical triad – adenoma sebaceum, seizures, mental retardation preceded by the
appearance of white macules
White macules, polygonal and lance ovate in shape.
White macules appear on trunk, lower extremities upper extremities, head and
neck.
CNS, heart, kidney, liver, thyroid, testes and gastrointestinal systems involved
Hypomelanosis of Ito:
Bilateral irregularly shaped leucoderma
Mainly on trunk and extremities
Randomly distributed with whorled or streaked configuration
Margins are serrated and blurred
Hypopigmentation may be progressive

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
68
A solitary vitiligo lesion must be distinguished from, Tinea versicolor, Pitryriasis alba,
Idiopathic guttate hypomelanosis, Post inflammatory hypomelanosis, Chemical
depigmentation, Vagabond leucoderma, Vogt-koyanagi-Harada syndrome,
Scleroderma
1. Tinea versicolor:
Occurrence on the upper chest, not amelanotic, scaling positive for fungi.
Lesions raised with hyperpigmented borders.
2. Pitryriasis alba:
Not amelanotic, faint margins, erythema and scaling.
3. Idiopathic guttate hypomelanosis:
Small, sharp margins, usually on arms, legs
4. Post inflammatory hypomelanosis:
History of presence of characteristic rash
5. Chemical depigmentation:
History of industrial exposure and small white macules at the site of contact
6. Vagabond leucoderma:
Is a leucoderma of older ill-kept men with history of poor hygiene, poor diet and
chronic alcohol abuse.
Depigmented patches are found in diffuse, light brown hypopigmented patches
around waist and groin.
The arms, legs, face are less involved
Attributed to multiple ectoparasitic infections.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
69
7. Vogt-koyanagi-Harada syndrome:
Rare multi system disease
Characterised by uveites, alopecia, poliosis
The first stage is the meningo encephalitic phase
Second is the ophthalmic stage
Third stage is vitiligo, poliosis, alopecia which marks the convalescent stage
8. Scleroderma:
A vitiligo like hypomelanosis
Lesions primarly on the upper trunk and distal extremities
Lesions amelanotic, with perfollicular spearing which resembles repigmenting
vitiligo269

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
70
SADHYA –ASADHYATA
Sadhya – asadhyata is the prognostic aspect of a disease. They are the prabhava
bheda of a roga270. Prognosis is determined by the lakshnas of the disease exhibited by
the patient.
Switra involves rakta mamsa and medhodatus. The deeper the involvement of
the dhatus the prognosis becomes worse. In this context, Acharya vagbatta has specified
the sadhya - asadhyata based on the colour of the patch. Rakta Varna or Aruna Varna are
sadhya, Tamra Varna becomes kasta sadhya and Sweta Varna becomes atishaya asadhya.
As the disease penetrates the deeper dhatus it becomes asadhya.271
Charaka mentioned a person who has followed vamana – virechana, rakta
mokshana regime completely, who takes sattu regularly and whose papakarmas are over,
such case is sadhya.272
Kashyapa273 and Bhela 274 have mentioned switra to be asadhya vyadhi.
Sadhya lakshnas:
Nutana or recent onset (less than one year)
Hair not dis coloured into Rakta varna 275
Patch which is very superficial – Tanu
White in colour or panduvarna
Mild elevation in the centre of the patch276
If the disease is still present in the twak, rakta and mamsa 277
Patch small in size 278
Less in number
Patches not adjoining each other
Hair not turned into white colour279

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
71
Asadhya lakshnas:
If the disease is present for more than one year280
Hair discoloured into rakta varna, sweta varna
Patches large in size
Numerous patches all over the body
Patches adjoining each other
If the disease enters beyond medodhatu281
If guhyastan i.e. genitals involved, palms and soles, osta ie lips involved
If the patch is due to dagda, vranas, kshata282
Sadhya lakshnas:
Table -11S.No. Lakshnas C.S. S.S A.H M.Ni B.P
1. Nutana or recent onset (less than one year) + - + + +
2. Hair not dis coloured into Rakta varna + - + - -
3. Patch which is very superficial – Tanu + - + - +
4. White in colour or panduvarna + - - - -
5. Mild elevation in the centre of the patch + - - - -
6. If the disease is still present in the twak, rakta andmamsa
- + - - -
7. Patch small in size - - + - -
8. Less in number - - + + -
9. Patches not adjoining each other - - + + +
10. Hair not turned into white colour - - + + +

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
72
Asadhya lakshnas:
Table -12
S.No. Lakshnas C.S
.
S.S A.H M.Ni B.P
1. If the disease is present for more than one year + - - + -
2. Hair discoloured into rakta varna, sweta varna + - - - -
3. Patches large in size + - - + -
4. Numerous patches all over the body + - - + -
5. Patches adjoining each other + - - + -
6. If the disease enters beyond medodhatu - + - - -
7. If guhyastan i.e. genitals involved, palms and soles,osta ie lips involved
- - + + +
8. If the patch is due to dagda, vranas, kshata - - - + +

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
73
PROGNOSIS
a. Positive family history: A positive family history is associated with progression and
shows poor signs of prognosis.
b. Mucosal involvement: The site affected most commonly on the limbs and mucosae.
The next affected sites are face and trunk. Bad prognosis was observed in patients having
mucosal involvement. In mucosal involvement lip involvement is very high. The order of
occurance in lips, genetalia, nipple, buccal mucosa, gingivae, alveolar margins. It is
worth while to state that mucosal vitiligo is of poor prognostic value.
c. Koebner’s phenomenon: A trauma leading to hypopigmented patch defines this term.
Subjects with Isomorphic Koebner’s phenomenon showed poor prognosis.
d. Non - Segmental vitiligo: Among this, vitiligo vulgaris is the commonest type
followed by acro-facial and mucosal. The non-segmental type of vitiligo is considered to
be of autoimmune origin. Hence this type is a poor prognostic indicator that portends
disease progression. Amongst all forms V. Vulgaris is more predominant.
e.Trichrome sign: Has an intermediate zone of hypochromia, located between the
achromic centre and peripheral unaffected skin. Shows poor prognosis.
f. Leucotrichia: leucotrichia may indicate poor prognosis in regard to repigmentation.
There has been good prognosis in segmental type of vitiligo. The age at
presentation does not have much significance. But the mean age of presentation is around
26-30 years. It may also start at young age in subjects with strong family history.283

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
74
CHIKISTA
Chikista is defined as roga nidana pratikara charya284. It is vyadhi harana kriya285.
The Phenomenon which restores the normalcy in the equilibrium among the doshas,
dhatus and malas286.
The primary step, in treatment of a disease is the prevention or abstinence from
the etiological factors287. The nidana of switra suggests viruddha ahara – vihara,
papakarmas, and misconduct to be the vital causes for the manifestation of disease.
The treatment aspect includes three types of therapies to combat the disease288
1. Daiva Vyapashray chikista – spiritual therapy
2. Yukti vyapashray chikista - rational therapy
3. Satvavajaya chikista – psychological therapy
Vagbhatta mentioned switra to be a medical emergency due to its bheebhatsa
nature and tendency to turn asadya at the earliest, hence timely medical intervention is
necessary. 289
1. Daiva Vyapashray chikista – spiritual therapy:
The spiritual therapy consists of recitation of mantras, wearing roots and gems290
Performing auspicious acts, offering gifts, oblations to the fire God.
Following religious precepts, atonement, fastings, invoke blessings, falling on the
feet of Gods, pilgrimages.
Spiritual therapies have empirical powers to eradicate diseases instanteously.
Such therapies are related to the blessings and influence of the Gods.
All the items enumerated under the spiritual therapy are effective in eradication of
diseases only the to divine influences

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
75
2. Yukti vyapashray chikista - rational therapy: consists of wise administration of
diet and drugs. This is sub – divided into
a. Antah parimarjan chikista:
The drugs or diet taken internally to alleviate the disease.
In switra roga, a person is made to undergo all the shodhana procedures first.
After patient is fully evacuated, samsrama karma is done as primary step of
treatment by giving malapu ras (Kakodumbara) along with gudam291.
The mixture should be given according to the balam of the rogi. After that he
should be exposed to the sun. This procedure to be continued for 3 days.
During this event if patient feels thirsty, peya is given to quench his thirst .292
By doing the above patient develops blisters on the patches all over the body.
The blisters should be pricked with kantakam to release the fluid in it.
After all the blisters are opened, a kwath prepared from bark of kakodumbara,
priyangu, asan, and shatapushpa should be given early in the mornings for 15
days 293
Otherwise, Phanitham prepared from palasa kshara can also be given294
All the yogas beneficial in kusta rogaas, are recommended in switra also
Sprinkling khadira kwatha externally on the body or taking it internally or
even drinking khadira udaka is very beneficial in switra295
A person should be exposed to sun continuously for 1 week after taking
Bakuchi churnam internally, pathya being dugda sevanam296

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
76
Gomutram is very useful in switra roga. Trikatu, Chitraka, madhu added in
gomutram and stored in a jar of ghee for 15 days and then taking it is very
beneficial297
b. Bahirparimarjana chikista: Applications over the body are included in this category
Manahsilaadi lepam298
Burnt bone of as mixed with kadali kshara, cow’s blood and applied as a
paste299
Kshara of Jati (Malathi) flowers mixed with elephant’s ichor, applied
externally300
Nilotpala, kusta, saindhavalavana mixed in elephant’s urine
Seeds of Bakuchi and mulaka grounded in ‘Cow’s urine
Kakodumbara, bakuchi, chitraka, powdered with cow’s urine301
Manashila powdered with peacock’s bile makes an effective paste in switra
The seeds of bakuchi, cow’s bile, loha bhasma, rasanjana, souveeranjana,
pippali, together made into paste and applied externally 302
c. shastra pranidhan: all the surgical therapies are included here
Doing rakta mokshana is one therapy advised in switra
3. Satvavajaya chikista – psychological therapy: The satwavajaya chikista
includes virteous conduct of a person. The psychological therapy is restraint of
mind from the ahita or unwholesome objects.
Normally the mind, including the sensefaculties remains undisturbed.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
77
In order to retain this condition one should make efforts to maintain a healthy
mind. This is achieved invariably by examining with intellect, not deviating from
the generally approved principles, not breaking the code of conduct or sadrut303
Respecting Gods,, Brahmins, preceptors, elderly people
Offering oblation to fire
Performing sandhya twice
Observing personal hygiene
Having faith and devotion towards teachers, gurus, and those who have
accomplished spiritual knowledge or perfection.
Be friendly to all creatures
Reconcile the angry
Controller of intolerance
Be of peaceful disposition
Conquer the roots of attachment
All the above acts help to maintain the psycho – somatic equilibrium, thus giving
health to a person304. The importance of these therapies is evident by the statement “a
person who has undergone shodhana procedures by vamana, virechana, raktamokshana,
who has been taking sattu as his regular diet, whose body is roughened and whose
papakarmas are decreasing by following the spiritual and virteous conduct, the disease
gets cured in such person305

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
78
TREATMENT
The main goal of treating vitiligo is to improve appearance. Therapy for vitiligo
takes a long time; it is usually continued for 6 to 18 months. The choice of therapy
depends on the number of white patches, their size, and location and how widespread
they are. Each patient responds differently to therapy and a particular treatment may not
work for everyone.
Current treatment options for vitiligo include:
1. Medical
2. Surgical
3. Adjuvant therapies
1. Medical therapies: Include most of which are applied topically
a) Topical Steroid therapy: Steroid creams are helpful in repigmentation, particularly if
they are applied in the initial stages of the disease. Cortico steroids are a group of drugs
similar to hormones which are produced by adrenal glands.
Mild topical steroid creams are prescribed for children under 10 years and
stronger for adults. They should be applied for 3 months to expect results and this is
simplest and safest treatment for vitiligo but not as effective as Psoralen
photochemotherapy.
There are side effects like skin shrinkage and skin striae in areas particularly
where skin is thin. They can be minimized by using weaker formulations of steroid
creams in these areas.
b. Psoralen Photochemotherapy: also known as Psoralen and ultraviolet A Therapy or
PUVA therapy.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
79
The most effective treatment for vitiligo available. The goal of PUVA is to
repigment the white patches. Though time consuming yields better results but care must
be taken to avoid side effects which some times can be severe.
Psoralen is a drug that contains chemical that react with ultraviolet light to cause
darkening of the skin.
The treatment involves taking Psoralen by mouth (Oral) or by applying it on the
skin (topically) this is followed by carefully timed exposure to sunlight.
Topical Psoralen therapy: is used for small number of patches affecting a limited part
of the body, it is also used for children 2 yrs old or older who have localized patches of
vitiligo.
Oral Psoralen therapy: used for people with extensive vitiligo and for people who do
not respond to topical PUVA treatment. Advised for children above 10 years as young
children have the risk of developing cataracts.
c. Depigmentation: This treatment involves fading the rest of the skin on the body to
match the areas that are already white. For more than 50% involvement depigmentation is
the best treatment options.
Patients apply the drug monobenzyl ether of hydroquinone twice a day to
pigmented areas until they match the already depigmented areas.
2. Surgical therapies: All surgical therapies are considered only after proper medical
therapy is provided. These therapies are time consuming and expensive. They are
appropriate only for carefully selected patients.
a. Autologous skin Grafts: The doctor removes skin from one area of your body and
attaches it to another area. This type of skin grafting is useful for small patches.
Treatment with grafting takes time, and is costly.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
80
b. Skin grafts using blisters: In this procedure the doctor creates blisters on your
pigmented skin by using heat suction or freezing cold. The tops of the blisters are then
cut out and transplanted to a depigmented skin area.
c. Micropigmentation: (Tatooing) : This procedure involves implanting pigment into
the skin with a special surgical instrument. This works best for lip area.
d. Autologous melanocyte transplants: In this procedure, the doctor takes a sample of
your normal pigmented skin and places it in a laboratory dish containing a special cell
culture solution to grow melanocytes. When the melanocytes in the culture solution have
multiplied, the doctor transplants them into depigmented areas.
3. Adjuvant therapies: In addition to medical and surgical therapies, there are many
things you can do to minimize the appearance of white patches and cope with emotional
aspects of vitiligo.
a. Sunscreens: People who have vitiligo, particularly those fair skinned should use
sunscreens to protect from both UVA and UVB forms of ultraviolet light. Sunscreens
also minimize tanning which makes the contrast between normal and depigmented skin
less noticeable.
b. Cosmetics: Some patients cover the depigmented patches with stains, makeup,
selftanning lotions. These cosmetic products are effective for people whose vitiligo is
limited to exposed areas of the body. Self tanning lotions have an advantage over makeup
in that the colour will last for several days and will not come off with washing.
c. Counselling and support groups: many people with vitiligo find it helpful to get
counselling from a mental health professional. A mental health counselor can also offer
support and help in coping with vitiligo.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
81
PATHYA – APATHYA
Pathya – apathyas are the list of indicative and preventive measures to be
followed by a person afflicted by a disease. Pathya – apathyas are of great importance to
the patient to stay healthy and avoid further progression of the disease. In the ayurvedic
classics, acharyas have mentioned pathya – apathya for all the diseases. As the nidana is
same for kusta and switra, the pathya – apathyas also remain same.
Pathya:
1. Ahara:
Shali rice (Oriza sativa)
Shastik rice (Oriza sativa)
Yava ( Barly)
Godhuma (Wheat)
Koradoosh ( Paspalum scrobiculatum)
Shyamak (Echinochlova frumentacea)
Uddalaka ( wild variety of Paspalum scrobiculatum
The above mentioned grains should be one year old and matured
Mudga (Phaseolus radiatus)
Adaki arhar (Cajanus cajan)
Soups to be prepared from the above two
Flesh of Jangala animals devoid of fatty matter
2. Vihara:
To be sincere and to be dutiful to God, Teachers, Gurus,
To offer prayers, perform yagna, homas, give donation to poor and needy.
3. Aushadha:
Nimba
Bhalltaka

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
82
Manduka parni (Centella asiatica)
Avalaguja (Psorhalia Corylifolia)
Adusa (Adathoda vasica)
Flowers of Arka (Calotropis procera)
Medicated oil prepared from sarshapa (Brassica nigra)
Medicated ghee prepared from chakramarda (Cassia tora), Patola (Trichosanthes
dioca)
Body of the patient can be anoinated with vajraka taila, Khadira kashaya,
Argwadhadi group fo drugs, power or paste.306
Apathya:
1. Ahara:
Mamsa (Flesh of birds)
Vasa (Oily part of flesh)
Dugdha (Milk)
Dadhi (Curd)
Tila taila (Seasame oil)
Kulatta (Dolichos biflorus)
Masha (Phaseolus mungo)
Nishpav (Dolichos lablab)
Preparations of sugar and Jaggery
Pisti
Amla (Articles having sour taste)
Viruddha ahara (incompatible food)
Vidahi (Food which can cause obstruction to channels)
Vidagda (food which cause acidic eructations)307
Arundutta mentioned that prohibition from aetiological factors constitutes the actual
treatment of disease. Although meat of all kinds may be prohibited but meat if not
incompatible may be permitted.308

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
83
2. Vihara:
Adhika matra bhojanam
Food taken during ajeernam
Diva swapnam
Vegadharana
Ativyayamam
Ativyavayam
Abusing elders, gurus, teachers

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
84
CRITERIA FOR DRUG SELECTION
The present drug “Dhatri-Khadira Kwatham” has been taken from
“Kustarogadhikar” of “Bhaishajya Ratnavali”, a contemporary textbook of 19th 309
century A.D.
The compound has two drugs – Khadira and Amlaki, Madhu as anupana.
Both the above mentioned drugs are non-controversial, unadulterated, easily
available, and economical
It is a simple combination and easy to prepare and use.
Both are sheeta Virya dravyas hence best pitta shamakas, and indicated in
kustarogas.
“Khadira” is mentioned as “Kustagnanam”310. It is equally beneficial in swithra
also.
The use of Khadira Kashaya or Khadira udaka internally and externally is highly
recommended in swithra311. Hence to know its action, on pigmentation in the present
disease is the main purpose for the selection.
Amlaki, the best rasayanam312, easy to use highly beneficial for the body to
restore health and improve immunity.
Apart from this, it has mild laxative effect which is very beneficial in the
treatment.
Regular use of amlaki destroys diseases like Swithra and Prameha313
Ultimately the principle “Swasthasya Swasthya rakshanam, aturasya vikara
prashamanam” is achieved through these two drugs.
Khadira helps in treating the disease, amlaki helps in restoring the health.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
85
DESCRIPTION OF INDIVIDUAL DRUGS
KHADHIRA:
Latin Name : Acacia catechu
Family : Leguminosae – Mimosaceae - (Vatadi Varga)
Charaka : Kustagna, Kashayaskanda
Sushruta : Salasaradi Gana
VERNACULAR NAMES:
English : Black Catechu, Cutch Tree
Hindi : Katha, Khair, Khair babul
Telugu : Kasu, Khadiramu, Mallasandra, Podala Manu, Sandra,
Sundara
Sanskrit : Bahushalya, Balapatra, Bala putra, Balatanaya,
Dantadhavana, Gayatri, Homa, Hima Shalya, Khadira,
Karkati, Kantaki, Kusthari, Kustarahita, Medya, Tiktasara,
Saradruma, Sushalya, Pathidruma, Vakrantaka, Yagnanga,
Yagnika, Yapadru
Morphology: A moderate sized tree of 9-12 mts hight. Bark is dark coloured, rough.
Young shoots are dark brown or purple glaborous. Leaves 2-pinnate.
Bark: The part used in the present study. The bark is bitter and acrid, cooling, astringent
to the bowls, antihelmenthic, antidysentric, antipyretic, cures itching, sore throat,
bronchitis, indigestion, heaviness, ulcers, boils, Psoriasis, inflammations, leprosy,
anemia, Leucoderma, also given in elephantiasis, urinary discharges, strengthens teeth.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
86
PROPERTIES:
Rasa : Tikta, Kashaya
Guna : Laghu, Ruksha
Virya : Sheeta
Vipaka : Katu
Karma : Kapha-Pittahara, Medogna, Dipana, Dantya
MAJOR CHEMICAL CONSTITUENTS:
Heart wood : Catechani, Catechutannic acid
Wood : I-epicatchin, Afzelchin, Gossypetin, Procyanidin, taxifolin
Gum : L-Arabinose, D-galactose, D-Rhamnose
RESEARCH WORK DONE ON ACACIA CATECHU:
1. A Medicinal extract of Acacia Catechu and Scutelleria baicalensis at as a dual
inhibitor of cyclooxygenase and 5-lipooxygenase to reduce inflammation
Ref: Burnett BP JiaQ.ZhaoY.levy RM.
J.Med Food 2007 Sep; 10 (3) 442-51
2. Medicinal Plant extra acts as anti-Escheria coli 0157: H7 agents and their effects
on bacterial cell aggregation.
Ref: Voravunthikunchai SP.Linsuwan S.
J.Food Prot 2006 Oct; 69(10) : 2336-41
3. Determination of the predominant catechins in Acacia Catechu by liquid
Chromatography / electrospray ionization – mass spectrometry.
Ref: Shen.D. WuQ. Wang M. Yang Y. Lavoie E J. Simon JE
J. Agric Food Chem 2006 May; 3 54(9): 3219 -24
4. Final report of the safety assessment of Acacia Catechu Gum.
Ref: Int.J.Toxicol 2005; 24 suppl. 3:75-118.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
87
5. Effective Medicinal plants against enterohaemorrghic eschercia Coli.0157:H7.
Ref: J.Ethnopharma col.2004 Sep; 94(1) 49-54
6. Antimicrobial Evaluation of some medicinal plants for their anti – enteric
potential against multi – drug resistant salmonella typhi
Ref: Rani P. Khullar N. Phytother Res 2004 Aug; 18(8) : 670-3
7. In vitro plantlet regeneration from seedling nodal explant of Acacia Catechu.
Ref: Sahani.R.Guptha Sc.Indian J.Exp Biol 2002 Sep; 04(9):1050-5
8. Preliminary observations on leukemia specific agglutinoins from seeds.
Ref: Agarwal S.Agarwal SS.
Indian J. Med Res 1990 Feb; 92:38-42
9. Antifertility activity of traditional contraceptive pill comprising Acacia Catechu
Ref: Azad Chowdhary A.K
Indian J. Med Res 1984 Sep; 80:372-4
10. Hypotensive action of Acacia Catechu.
Ref: J.S.K. Sham, K.W.Chiu, P.K.T.Pang,
Planta Med 1984; 50:177-180

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
88
AMLAKI:Latin Name : Emblica officinalis
Family : Euphobiaceae (Haritakyadi Varga)
Charaka : Vayasthapana, Virechanopaga
Sushruta ; Triphala, Parushakadi
VERNACULAR NAMES:
English : Emblic myrobalan Tree
Hindi : Amlaki, Amla, Amlika
Telugu : Amlakamu, Amalaki, Usiri, Usirikaya, Nelli, Pullayusirika
Sanskrit : Adiphala, Akara, Amalaki, Amrita, Amrita Phala,
Bahuphali, Dhatri, Dhatrika, Dhatriphala, Shriphala,
Vayastha, Tishya, Sriphali, Vrishya, Rochani, Karshaphala,
Kayastha.
Morphology: A deciduous small or middle sized tree with crooked trunk and spreading
branches, bark greenish grey, peeling off in Conchoidal flakes. Branchlets glaborous
leaves sub-sessile.
Fruit: The part used in the drug given in the present study. The fruit is acrid, sour, bitter,
sweetish, cooling, carminative, alterative, laxative, tonic, antipyretic, and useful in
burning sensations, urinary discharges, thirst, leprosy, piles, and anaemia.
Properties:
Rasa : Amlapradhana Pancharasas (except lavana)
Guna : Guru, Snigdha
Virya : Sheeta
Vipaka : Madhura
Karma : Tridoshahara, Vayasthapana, Rasayana, Chakushya,
Vrusya, Keshya.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
89
Major Chemical Constituents :
Fruit: Vit-C, Phyllembin, Tinolic Acid, indole, acetic Acid, Phyllembic acids & Salts,Ellagic acid, Corilagin.
RESEARCH WORK DONE ON EMBLICA OFFICINALIS:
1. Hypolipidaemic effect and anti atherosclerotic effects of fruit juice of Emblica
Officinalis in cholesterol fed rabbits.
Ref: Ritu Mathur, Arti Sharma, Mira Varma
J. Ethnopharmacology Vol 50 (2) 1996 pgs 61-68
2. Detoxifies the body, regulates digestion, helps to increase lean body mass &
reduce fats. A natural source of vitamin C.
Ref: Dr. Manish, Chakrapani Ayurvedic Clinic & Research Centre
3. Antitumor activity of Emblica Officinalis
Ref: Jeena K. Jose, Girija Kuttana nd Ramadasan Kuttan.
J. Ethnopharmacology vol 75; issues 2-3, May 2001 Pg 65-69
4. Flavinoids from Emblica Officinalis and Mangifera Indica effectiveness for
dyslipidemia
Ref: L. Anila and N.R. Vijayalakshmi
J. Ethnopharmacology vol 79 issue:1, Feb 2002 pg 81-87.
5. Hepatoprotective activity of Emblica Officinalis
Ref: Jeena K. Jose and Ramadasan Kuttan
J. Ethnopharmacology vol.72 (1-2) Sep 2002 pg 135-140
6. Cytoprotective and immuno modulating properties of Amla (Emblica Officinalis)
on lymphocytes and in-vitro study.
Ref: M. Saiam; D Neetu Yogesh B. Anju P.
J. Ethnopharmacology vol.81 (1) June 2002 Pg 5-10

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
90
MADHU:
There are 8 types of Madhu - Makshika, Bhramara, Ksaudra, Pauthika chatra,
Ardya, Audalaka, and Dalam.
Best anupana, has good yogavahi nature
Properties: Sheeta, Laghu, Swadu, Ruksha, Gnahi, Lekhana, Netrahitakara,
Agnideepaka, Swarakara, Vrana Sodhana, Ropana, Srotoshodhaka, Varnya, Medhya,
Vrishya, Visada, Ruchikara, Kusta-arsas, Raktapitta, Kapha, Prameha, Klama, Krimi,
Medohara, Swasa, Kasa, Hikka, Malabaddahara, Alpavatakara,
Rasa : Madhura Rasa, Kashaya anurasa
Guna : Laghu, Ruksha
Veerya : Sheeta Virya
Vipaka : Katu

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
91
METHOD OF DRUG PREPARATION
The present yogam is a combination of Khadira and Amlaki
The bark of Khadira, fruits of Amlaki are used in the preparation
Barks of Khadira, fruits of amlaki are collected, through the herb collector; they
are dried under shade, to restore their medicinal properties.
Khadira bark is pounded into coarse powder & weighed. Equal quantity of amlaki
fruit is pounded and added to it.
The powder is made into kwath churam. It is stored in a neat, dry container and
packed accordingly.
The Kwath form is administered to the patient.
Dose : 30ml Tid
Madhu as anupana

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
92
METHODOLOGY
The study was conducted in the Department of Kayachikitsa, Govt. Ayurvedic
Hospital, Erragadda,Hyderabad between 6-3-07 to 31.1.08
Aim: To assess the efficacy of Dhatri – Khadira kwath in causing pigmentation in white
patches of switra.
Source of Data : Patients of either sex aged between 5-70 years diagnosed as switra
were selected from OPD of Govt.Ayurvedic Hospital, Erragadda, Hyderabad.
Sampling Method and Research Design: The study was conducted as an open trial
study with randomized selection of 30 patients of either sex within age groups 5-70 years
suffering from switra were included.
Informed consent from all patients was obtained prior to the study. A complete
history was taken through a special proforma including age of onset, duration, family
history of switra, H/o consangnious marriage of parents, any personal or family history of
systemic diseases. A thorough dermatological examination was conducted on the
patients.
Inclusion criteria:-
Patients of either sex with sweta varna mandalas (i.e. milky white patches,
centrally hypopigmented with sharp circumscribed borders).
Patients aged between 5-70 years
Chronicity less than 6 years.
Exclusion criteria: as per ICD-10, L00-L99 skin and sub-cutaneous diseases,
L80-Vitiligo
Patients below 5 years and above 70 years
Certain conditions originating in the perinatal period (P00-P96)

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
93
Certain infectious and parasitic diseases – (B00-B99)
Complications of pregnancy and childbirth (O00-O99)
Endocrinal, nutritional and metabolic diseases (E00-E90)
Congenital malformations, deformities and chromosomal abnormalities (Q00-Q99)
Neoplasms (C00-D48)
Systemic connective tissue disorders (M30-M36)
With other skin diseases like Psoriasis, Eczema which interfere with the treatment.
With Psychiatric problems like Psychosis, mania, OCD, Schizophrenia
Investigations: Following investigations were done prior to the study.
CBP
ESR
RBS
CUE
Diagnostic Criteria: Swetavarna mandalas with or without other features of switra
Intervention:
Drug: Dhatri – Khadira kwath
Dose: 30ml tid, followed by madhu as anupana
Route: Oral
Duration: 45 days
Followup: 2 months
Assessment criteria:
The assessment was made on the colour, number and size of the mandalas which were
observed before starting the treatment, during and after the treatment.
Change in the colour of mandalas
Change in number of mandalas
Change in the size of mandalas
To assess the improvement in the colour the following grading was given

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
94
C0 – Normal skin colour
C1 – Tanned brown
C2 – Light brown
C3 – Dark pink
C4 – Light pink
C5 – White colour
The data obtained before and after treatment were analysed. The complete results
of treatment were ascertained in terms of,
I. Colour of the mandalas:
1-25% - Mild Response
26-50% - Moderate Response
51-75% - Marked Response
76-100% - Excellent Response
0 - No Response
II. Number of Mandalas:
1-25% - Mild Response
26-50% - Moderate Response
51-75% - Marked Response
76-100% - Excellent Response
0 - No Response
III. Size of Mandalas:
1-25% - Mild Response
26-50% - Moderate Response
51-75% - Marked Response
76-100% - Excellent Response
0 - No Response

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
95
Overall effect of therapy was assessed based on the following groups
1-25% - Mild Response
26-50% - Moderate Response
51-75% - Marked Response
76-100% - Excellent Response
0 - No Response
In this study subjects were classified into 5 groups mild, moderate, marked
excellent and No response groups. If the symptoms of a patient decrease by 1-25% he is
put in mild group, if the patient has decrease in symptoms by 26-50% he is placed in
moderate group, subject with relief of symptoms by 51-75% he is placed in marked
group. If patient has relief by more than 75% he is placed in excellent group. There are
patients with no relief of symptoms who are placed in no response group.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
96
OBSERVATIONS
ACCORDING TO THE INCIDENCES
Table – 13 Showing incidence of age:
Sl.No. Age(in years) No. of Patients %
1. 0-10 yrs 6 20%
2. 11-20 yrs 7 23.33%
3. 21-30 yrs 6 20%
4. 31-40 yrs 4 13.33%
5. 41-50 yrs 1 3.33%
6. 51-60 yrs 4 13.33%
7. 61-70 yrs 2 6.66%
Among 30 patients taken for the study maximum number of patients fall under
11-20 yrs group.
Highest percentage of study population includes females 56.66%
Table – 15 Incidence of Habitat:
Sl.No. Habitat No. of Patients %
1. Rural 2 6.6%
2. Urban 23 76.6%
3. Town 5 16.66%
Majority of the subjects came from urban areas 76.6%

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
97
6
7
6
4
1
4
2
0
1
2
3
4
5
6
7
NO OF PATIENTS
0 TO 10 11 TO 20 21 TO 30 31 TO 40 41 TO 50 51 TO 60 61 TO 70YRS
AGE OF THE PATIENT
Series1
INCIDENCE OF SEX
MALES43%
FEMALES57%
MALES FEMALES
2
23
5
0
5
10
15
20
25
NO OF PATIENTS
RURAL URBAN TOWNHABITAT
INCIDENCE OF HABITAT
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
98
Table – 16 Incidence of Religion:
Sl.No. Religion No. of Patients %
1. Hindu 21 70%
2. Muslim 6 20%
3. Christian 3 10%
Majority of the subjects belong to Hindu community 70%.
Table – 17 Incidence of Marital Status:
Sl.No. Marital Status No. of Patients %
1. Married 13 43.33%
2. Un-married 17 56.66%
Most of the patients taken for clinical study were un-married 56.66%.
Table – 18 Incidence of Diet:
Sl.No. Diet No. of Patients %
1. Mixed 23 76.66%
2. Veg 7 23.33%
Veg: Vegetarian diet
Majority of the subjects had mixed diet 76.66%
Table – 19 Incidence of Socio - Economic Status:
Sl.No. Age(in years) No. of Patients %
1. LIG 13 43.33%
2. MIG 17 56.66%
3. HIG 0 0
LIG: Low income group (below 10,000/-),
MIG: Middle income group (10,000/- to 20,000/-),
HIG: High income group (20,000/- and above)
Majority of the subjects belong to middle income group

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
99
21
6
3
0
5
10
15
20
25
NO OF PATIENTS
HINDU MUSLIM CHRISTIANRELEGION
INCIDENCE OF RELEGION
Series1
MARITAL STATUS
MARRIED43%
UNMARRIED57%
MARRIED UNMARRIED

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
100
INCIDENCE OF DIET
MIXED77%
VEG23%
MIXED VEG
13
17
0
0
2
4
6
8
10
12
14
16
18
NO OF PATIENTS
LIG MIG HIG
SOCIO -ECONOMIC STATUS
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
101
Table – 20 Incidence of Occupation:
Sl.No. Occupation No. of Patients %
1. Agriculture 1 3.33%
2. Private Employees 2 6.6%
3. Business 2 6.66%
4. Electrician 1 3.33%
5. Student 16 53.33%
6. Housewife 6 20.00%
7. Carpenter 1 3.33%
8. Watchman 1 3.33%
Majority of the patients belonged to student community 53.33%
Table – 21 Incidence of Colour of the patients:
Sl.No. Colour of pt No. of Patients %
1. Fair 9 30%
2. Wheatish 14 46.66%
3. Black 7 23.33%
Majority of the subjects were wheatish skinned people 46.66%.
Table – 22 Incidence of Origin of the disease:
Sl.No. Origin No. of Patients %
1. Doshaja 28 93.33%
2. Vranaja 2 6.66%
The origin of the disease due to external causes were found in two subjects 6.66% and in
majority of subjects the cause was endogenous 93.33%

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
102
1
2 2
1
16
6
1 1
0
2
4
6
8
10
12
14
16
NO OF PATIENTS
AGRICULTURE BUSINESS STUDENT CARPENTEROCCUPATION
INCIDENCE OF OCCUPATION
Series1
9
14
7
0
2
4
6
8
10
12
14
NO OF PATIENTS
FAIR WHEATISH BLACK
COLOUR OF THE PATIENT
Series1
ORIGIN OF DISEASE
DOSHAJA93%
VRANAJA7%
DOSHAJA VRANAJA

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
103
Table – 23 Incidence of Prakriti:
Sl.No. Prakriti No. of Patients %
1. VP 9 30%
2. PK 5 16.66%
3. KV 1 3.33%
4. PV 9 30%
5. VK 3 10%
6. KP 3 10%
VP= Vata pitta, PK= Pitta kapha, KV= Kapha vata, PV= Pitta vata, VK= Vata Kapha,KP= Kapha pitta.Among 30 patients, majority of them belonged to vatapitta and Pitta vata prakruti 30%.
Table – 24 Incidence of Family History:
Sl.No. Family History No. of Patients %
1. Present 1 3.33%
2. Absent 29 96.66%
Majority of the patients did not present with a family history 96.66%.
Table – 25 Incidence of Stress:
Sl.No. Stress No. of Patients %
1. Present 7 23.33%
2. Absent 23 76.66%
Majority of the patients did not present with history of stress 76.66%.
Table – 26 Incidence of Consangnious Marriage of parents:
Sl.No. Cong.Marriage No. of Patients %
1. Presnet 6 20%
2. Absent 24 80%
Majority of patients did not present with history of consangious marriage of parents 80%.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
104
9
5
1
9
3 3
0
1
2
3
4
5
6
7
8
9
NO OF PATIENTS
VP PK KV PV VK KP
PRAKRUTI
Series1
FAMILY HISTORY
present3%
absent97%
present absent
STRESS
PRESENT23%
ABSENT77%
PRESENT ABSENT

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
105
Table – 27 Incidence Chronicity:
Sl.No. Chronicity No. of Patients %
1. 1month – 1 yr 20 66.66%
2. 2 -3 yrs 6 19.99%
3. 4-5 yrs 3 10%
4. 6-7 1 3.33%
Majority of the patients taken for the study had chronicity of disease from 1 month to 1
year 66.66%.
Table – 28 Incidence of Old/New cases:
Sl.No. Old/New cases: No. of Patients %
1. Old 15 50%
2. New 15 50%
Among 30 cases taken for the study 15 patients were new and 15 patients were old who
already received treatment else were.
Table – 29 Incidence of age of first onset:
Sl.No. Age(of first onset) No. of Patients %
1. 0-10 yrs 7 23.33%
2. 11-20 yrs 8 26.66%
3. 21-30 yrs 4 13.33%
4. 31-40 yrs 4 13.33%
5. 41-50 yrs 1 3.33%
6. 51-60 yrs 4 13.33%
7. 61-70 yrs 2 6.66%
In majority of patients disease started before the age of 20 yrs 49.99%

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
106
H/O CONSANGNIOUS MARRIAGE
PRESENT20%
ABSENT80%
PRESENT ABSENT
20
6
3
1
0
2
4
6
8
10
12
14
16
18
20
NO OF PATIENTS
1MON-1YR 2YR-3YR 4YR-5YR 6YR-7YR
CHRONICITY OF THE DISEASE
Series1
OLD/NEW CASES
OLD50%
NEW50%
OLD NEW

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
107
Table – 30 Site of first onset:
Sl.No. Site (of first onset) No. of Patients %
1. Scalp 0 0
2. Face 11 36.66%
3. Neck 0 0
4. Chest 1 3.33%
5. Abdomen 2 6.66%
6. Back 4 13.33%
7. Upper limbs 2 6.66%
8. Lower limbs 9 30%
9. Genitals 1 3.33%
In majority of subjects face was the site of first onset 36.66% followed by lower limbs
30%
Table – 31 Nidanam:
Sl.No. Ahara nidanam No. ofPatients
%
1. Adika ushna, teekshana ahara sevana 1 3.33%
2. Amla, lavana, katurasa sevana 5 16.66%
3. Madura rasa sevana 3 10%
4. Adhika dadhi 4 13.33%
5. Adika mamsa 5 16.66%
6. Dumrapana 1 3.33%
7. Masha and mulakas 1 3.33%
8. Dadi and mamsa 1 3.33%
9. Nothing particular 9 30%
Among 30 subjects 9 patients did not have any particular eating habits in excessive 30%.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
108
7
8
4 4
1
4
2
0
1
2
3
4
5
6
7
8
NO OF PATIENTS
0 TO 10 11 TO 20 21 TO 30 31 TO 40 41 TO 50 51 TO 60 61 TO 70
AGE IN YEARS
AGE AT FIRST ONSET
Series1
0
11
0
1
2
4
2
9
1
0
2
4
6
8
10
12
NO OF PATIENTS
SCALP NECK ABDOMEN UPP.LIMB GENITALS
SITE
SITE OF FIRST ONSET
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
109
Table – 32 Types:
Sl.No. Types No. of Patients %
1. Localized 26 86.66%
2. Generalized 4 13.33%
3. Universal 0 0
Among 30 subjects taken for the study 26 of them presented with localized type of
vitiligo 86.66%
Table – 33 Nature of spread:
Sl.No. Spread No. of Patients %
1. Gradual spread 29 96.66%
2. Sudden spread 1 3.33%
3. Stable 0 0
Among 30 subjects 29 of them presented with gradual spread of the disease 96.66%.
Table – 34 Symmetry of the patches:
Sl.No. Symmetry No. of Patients %
1. Symmetrical 15 50%
2. A symmetrical 15 50%
Among 30 subjects 15 patients presented with symmetrical patches and 15 presented with
asymmetrical patches 50%
Table – 35 Leucotrichia:
Sl.No. Leucotrichia No. of Patients %
1. Present 5 16.66%
2. Absent 25 83.33%
Among 30 subjects 25 of them did not have leucotrichia (hair not involved) 83.33%

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
110
26
40
0
5
10
15
20
25
30
NO OFPATIENTS
LOCALIZED GENERALIZED UNIVERSAL
TYPES OF VITILIGO
Series1
29
10
0
5
10
15
20
25
30
NO OF PATIENTS
GRADUAL SUDDEN STABLENATURE OF SPREAD
NATURE OF SPREAD
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
111
Table – 36 Colour of the patches:
Sl.No. Colour of the patches No. of Patients %
1. White colour (C5) 23 76.66%
2. Light Pink (C4) 5 16.66%
3. Dark pink (C3) 2 6.66%
4. Light Brown (C2) 0 0
5. Tanned brown (C1) 0 0
Among 30 subjects 23 of them presented with white coloured patches 76.66%
Table – 37 Number of patches:
Sl.No. Number of patches No. of Patients %
1. 1-5 27 90%
2. 6-10 1 3.33%
3. Above 10 2 6.66%
Among 30 subjects 27 of them had 1-5 number of patches on them 90%
Table – 38 Size of patches (for 24 patients only):
Sl.No. Size of patches No. of Patients %
1. 1-15cm 19 82.6%
2. 16-30cm 2 8.68%
3. 31-45cm 1 4.34%
4. 46-60cm 0 0
5. 61-75cm 1 4.34%
6. 76-90cm 0 0
7. Above 90cm 1 4.34%
Among 30 subjects 19 of them presented with patches between 1-15cm size 82.60%

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
112
19
2
1
0
1
0
1
0
2
4
6
8
10
12
14
16
18
20
NO OF PATIENTS
1-15 cms 16-30 cms 31-45 cms 46-60cms 61-75 cms 76-90 cms above 90 cmsSIZE IN CMS
SIZE OF THE PATCHES
Series1
23
5
2
0 0
0
5
10
15
20
25
NO OF PATIENTS
C5 C4 C3 C2 C1
COLOUR OF THE PATCHES
27
12
0
5
10
15
20
25
30
NO OF PATIENTS
1 TO 5 6 TO 10 ABOVE 10NO OF PATCHES
NO OF PATCHES

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
113
Table – 39 Aggravating factors:
Sl.No. Aggravating factors No. ofPatients
%
1. Exposure to sun 4 13.33%
2. Contact with chemicals 1 3.33%
3. Application of Cosmetics 0 0
4. Intake of milk 1 3.33%
5. Intake of curd 2 6.66%
6. Non-veg diet 2 6.66%
7. Nothing particular 20 66.66%
Among 30 subjects 20 of them had no specific aggravating factors 66.66%
Table – 40 History of Allergy:
Sl.No. History of Allergy No. ofPatients
%
1. Food 1 3.33
2. Drugs 0 0
3. Dust 1 3.33
4. Nothing particular 28 93.33
Among 30 subjects 28 of them had no specific History of Allergies 93.33%

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
114
RESULTS
Table – 41 Responded / Not responded:
Sl.No. Parameter Responded % Notresponded
%
1. Colour 24 80% 6 20%
2. Number 3 10% 27 90%
3. Size (for24 Pts) 11 45.8% 13 54.1%
Amont 30 subjects 24 patients responded in colour and 6 did not respond, 3 patients
responded in number and 27 did not respond, out of 24 patients 11 responded in size and
13 did not respond.
Table – 42 Response in the Colour of Patches:
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 11 6 7 0 6
Among 30 subjects 11 showed mild response, 6 moderate, 7 marked and 0 excellent
response in colour. 6 patients showed no response in colour.
Table – 43 Response in the Number of Patches:
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 0 2 1 0 27
Among 30 subjects 0 showed mild response, 2 showed moderate response, 1 showed
marked improvement, 0 showed excellent response. 27 patients showed no response in
the number of patches

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
115
RESPONSE IN COLOUR
RESPONDED80%
NOTRESPONDED20%
RESPONDED NOTRESPONDED
11
6
7
0
0
2
4
6
8
10
12
NO OF PATIENTS
1-25% 26-50% 51-75% 76-100%
% RELIEF
RESPONSE IN COLOUR
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
116
RESPONSE IN NUMBER
RESPONDED10%
NOTRESPONDED90%
RESPONDED NOTRESPONDED
A
0
2
1
0
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
NO OF PATIENTS
1-25% 26-50% 51-75% 76-100%% RELIEF
RESPONSE IN NUMBER
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
117
RESPONSE TO SIZE
RESPONDED46%
NOT.RESPONDED54%
RESPONDED NOT.RESPONDED
3
6
1 1
0
1
2
3
4
5
6
NO OF PATIENTS
1-25% 26-50% 51-75% 76-100%% RELIEF
RESPONSE IN SIZE
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
118
Table – 44 Response in the Size of Patches (for 24 patients only):
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 3 6 1 1 13
Among 30 subjects 3 showed mild Response, 6 showed moderate Response, 1 showed
marked improvement, 1 showed excellent Response. 13 patients showed no Response in
the size of patches
Table – 45 Overall Results:
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 18 4 2 0 6
Among 30 subjects 18 showed mild response ,4 showed moderate response, 2 showed
marked improvement, 0 showed excellent response after the clinical study, and 6 patients
did not respond to the treatment at all.
Table – 46 Results:
VARIABLE MALESN=13
FEMALESN=17
Age (Mean Age) 27.1 yrs 28.58 yrs
Habitat – Urban 76.92 % 76.47 %
Habitat – Town 15.38 % 17.65 %
Habitat – Rural 7.69 % 5.8%
Diet – Vegetarian 38.46 % 11.26 %
Diet - Mixed 61.54 % 88.24 %
Types – Localized 92.31 % 82.35 %
Generalized 7.69 % 17.65 %

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
119
18
4
2
0
6
0
2
4
6
8
10
12
14
16
18
NOOFPATIENTS
1-25% 26-50% 51-75% 76-100% 0RESPONSE%RESPONSE
OVERALLRESULTS
Series1

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
120
Table – 47 Statistical Analysis of the Results :
PARAMETER MEAN MEAN
DIFF.
STD
DEV
STD
ERR
t
Value
p
Value
REMARKS
COLOUR BT 4.44 0.84 0.48 0.08 6.6 < 0.0001 SIGNIFICANT
COLOUR AT 3.6 1.1 0.2
NUMBER BT 1.66 0.28 2.23 0.41 1.7 <0.35 NOTSIGNIFICANT
NUMBER AT 1.38 1.94 0.36
SIZE BT 12.36 0.02 24.4 4.45 2.05 <0.1 NOTSIGNIFICANT
SIZE AT 12.34 24.3 4.2

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
121
DISCUSSION
About the Disease: Switra is an ancient malady due to its references being cited in the
Vedas. It is evident that people suffered from this disease from times unknown. A similar
condition like switra was prevalent in other civilizations across the globe. This is evident
from, the description of the disease available in their respective literature. It was called
“Kilas” in Tibet, “Bohak” in Arabia “Zorak” in Jerusalem, “Shirabito” in Japan,
Hence it can be said that this disease was prevalent across the globe not restricting to
particular country or race. Since ancient times attempts were made to combat the disease.
Switra can be well correlated to VITILIGO in contemporary medicine.
Switra and vitiligo have similar clinical features and presentation of the disease.
Both the diseases are related to hypopigmentation. Vitiligo is the most commonly aquired
hypomelanosis. The prevalence of the disease is 1% World wide.
In a society where attractiveness is positively related to expectations of further
success, happiness and satisfaction in marital relationships, it is not surprising that any
visible illness like switra can make the afflicted person experience high levels of self
conciousness and low self – esteem.
The etiology of vitiligo remains unknown, only the Triggering / Precipitating
factors are identified, among which nutritional deficiency, emotional stress infections,
exposure to chemicals are included. The etiology of Switra is given as incompatible diet,
misconduct, improper life style. The essence of both remains same i.e. misconduct,
improper life style indirectly leads to stress which disturbs the harmony between the body
and mind. Stress plays an important role in dermatological diseases. Incompatible diet
leads to disturbances in the metabolism and causes accumulations of toxins in the body,
in directly leads to nutritional deficiency. Vitiligo (Non - segmental type) is considered of
auto immune origin.
.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
122
During this study no prodromal symptoms are mentioned for both switra and
vitiligo and the same was noticed in the study.
The pratyatmaka linga “Swetavarna mandalas” were clearly evident. Patients
sought medical attention when they noticed white coloured patches on the skin. As per
the definition of Sushruta, 30 switra is “Twagatam” and “Aprasravi”accordingly in
subjects the skin was only involved, no pain or secretions were noticed. Vitiligo is also
presented as milky white patches, centrally hypopigmented with sharp circumscribed
borders and mostly asymptomatic. The clinical features of vataja, pittaja, sleshmaja could
not be found in the patients as described in the texts. The macules were found to be of
round, oval shape and some macules were irregular in shape. The size of macules mostly
varied from 1-15cm. The mucous membranes were affected and lips were mostly among
the affected mucosal surfaces. Although any part of the skin or mucous membrane is
amenable to develop vitiligo the disease has a predilection for normal, hyperpigmented
regions such as face, groin, axillae, areola, and genitalia. The same was observed that the
face was the first site of onset in many patients.
Further, lesions may develop in areas like ankles, elbows, knees, which are
subjected to repeated trauma or friction according to texts and the same has been
observed in the patients whose first site of onset were limbs the areas generally involved
were the knees, or elbows or ankles. Lip – tip syndrome characterized by depigmentation
of terminal phalanges was not encountered during the study.
Clinical variants of vitiligo were not seen in subjects of the study. Among the
various types of Vitiligo, maximum prevalent type was localized – focal and segmental
forms. The non - segmental form, which is a generalized type, was also seen in the
patients in less percentage.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
123
Discussion on Drug Review: The drug taken for the clinical study is “Dhatri – Khadira
Kwath” selected from Baishaijya Ratnavali. It basically contains Dhatri i.e. Amlaki and
Khadira. The main aim for selecting the drug is to find a simple panaceae for a disease
like switra. The form of administration is kwath form which has high efficacy. Both the
drugs are easily available, non-controversial, unadulterated and economical. The kwath
churnam was given to the patients sufficient for every 15 days for a total duration of 45
days. The patients were advised to take 1 tsp (5grms) of honey each time after taking the
medicine. Before starting the treatment patients were advised to take Triphala Churnam
for virechanam. Khadira is the best kustahara dravya. Many instances have quoted
khadira to be beneficial in switra also. Works on Bakuchi, Kakodumbara, Chitraka, and
Kaseesabaddaras have been conducted but efficacy of khadira in causing pigmentation
has not been studied. Moreover Amlaki is the best rasayana, pitta shamaka and improves
the efficacy of the formulation.
Probable mode of action: Khadira is the Sheeta Virya Dravya having tikta, Kashaya
rasas. Has best Pitta Shamaka and rakta shodaka property. As Rakta and pitta
(Interlinked with each other) are both vitiated in switra Khadira acts best in this aspect.
Amlaki also is sheeta virya dravya with pancharasas (Except Lavana). It is the
best source of vitamin C. Helps to build immunity, and may hinder the autoimmune
reaction in the body. It is also best pitta shamaka. Generally the oxidants which are the
outcome of metabolic reactions are accumulated in the skin which can be shown through
Fourier – Raman spectroscopy. These oxidants are responsible for the harmful changes in
the skin. Amlaki has the best anti - oxidant property which can counter the effects of
toxins in the skin.
Discussion on Methodology: The study was conducted in the Dept of Kayachikitsa,
Govt.Ayurvedic Hospital, Erragadda, Hyderabad. The main aim was to assess the
efficacy of Dhatri- Khadira Kwatha in causing pigmentation in white patches of switra.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
124
A total of 34 patients were incorporated, 4 patients were dropouts, 30 patients
completed the treatment schedule. The patients had to come for a review for every 15
days. And the improvement in the condition was assessed accordingly. Patients of either
sex aged between 5-70 yrs were randomly selected into a group, and an open trial was
conducted. Prior to the trial an informed consent from all the patients was obtained. A
thorough dermatological examination and a detailed history were taken through a special
case sheet.
Inclusion Criteria: Patients of either sex were included in the study to know the
incidence of the disease among males and females. Patients aged 5yrs were the lowerlimit
and 70 yrs the higher limit. To know the increase in the incidence of childhood vitiligo
the lower limit was taken and higher limit to know the incidence of switra in elderly
people.
Chronicity less than 6 yrs was taken to assess the response of patches to the
treatment. Generally above 6yrs of chronicity the patches do not respond to the treatment
and in some cases there may be complete depigmentation.(Fitzpatrick)
Exclusion criteria: The exclusion criteria were followed from ICD-10. L00-L99-Skin
and sub-cutaneous disease. L80 vitiligo; shows the exclusion criteria for vitiligo. Patients
below 5yrs are too young to take the medicine and above 70yrs also may not be able to
take the medicine.
Other skin diseases like Psoriasis and Eczema interfere with the treatment hence
they are excluded. The psychiatric problems like psychosis etc makes the patient unfit for
this treatment.
Investigations: There are no special laboratory investigations to diagnose switra. As a
part of routine examination CBP, ESR, RBS, CUE were done prior to the study.
Diagnostic Criteria: Swetavarna mandalas on the skin and mucosal surfaces with or
without other features of switra.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
125
Assessment criteria: The assessment was based on three clinical parameters, the colour,
number and size of the mandalas, which was observed before, during and after the
treatment. To assess the improvement in the colour, grading was given. C0- Normal Skin
colour, C1-Tanned Brown Colour, C2 – Light Brown Colour, C3- Dark Pink, C4 – Light
Pink, C5 – White Colour. All the patients did not present with white coloured patches.
Some had light pink, others had darkpink colour in the patches. During the treatment the
improvement was assessed like change of colour from white to light pink and so on. The
grading was given to assess the stepwise changes in the colour.
The complte results of the treatment were ascertained in terms of 5 groups. If the
symptoms of a patient decrease by 1-25% he is put in mild response group, if the patient
had decrease in symptoms by 26-50% he is placed in moderate response group, if the
patient had relief of symptoms by 51-75% he is placed in marked response group. If the
relief is more than 75% he is placed in excellent response group. If no know relief of
symptoms is seen they are placed in no response group.
Discussion on observations: A total of 34 patients were incorporated among whom, 4
were dropouts and 30 completed the treatment schedule. The following discussion on
observations is based on them.
Age groups: Among 30 patients, 6 of them (20%) were below the age of 10 yrs. 7
patients (23.33%) were below the age of 20yrs. From past two decades there is a sharp
rise in the incidence of childhood vitiligo (Behl) and the same was observed in this study.
Sex: Both males and females were taken for the study. The disease affects both the sexes
equally. But the percentage of female patients (56.66) in this study is higher than men. It
can be attributed to the social stigma and embarrassment caused due to depigmentation
and thus making female patients seek medical attention earlier than males.
Religion: Higher percentage of the subjects 70% belonged to Hindu community.
Generally in particular communities the dietary habits vary, which may be the cause for
the disease, to evaluate that, religion was taken into consideration.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
126
Marital Status: Among 30 subjects, unmarried patients were more in number 17,
(56.66%).
Diet: The higher incidence of the disease was found in subjects with mixed diet 23
patients (76.66%). Generally taking non - vegetarian diet may accelerate the onset of the
disease.
Socio Economic Status: The subjects were classified into three groups depending on
their income level. Less thanRs.10,000/- were grouped into Low income group,
Rs.10,000-20,000/- Middle income group and aboutRs.20,000/- High income group.
Majority of subjects 17 (56.66%) belonged to Middle income group.
Habitat: Incidence of the disease is high in the rural population (Behl), among the 30
subjects taken for the study; a high incidence is seen in the urban population -23 patients
(76.6%) Rapid phenomenon of urbanisation which leads to life style changes and dietary
disorders might have resulted in the higher incidence in urban people.
Occupation: Switra may be produced as one of the occupational hazard. Occupation has
a direct influence on the disease. Occupation which includes contact with chemicals, or
printers, dyers, have chance of acquiring switra. In the present study majority of them
were students 16 (53.33%).
Colour of the patients: Generally vitiligo affects all the races equally, but the dark
skinned people are more prone to display due to the colour contrast. India is a tropical
country where we find more of wheatish to dark coloured people. In the study the
incidence of switra was found more in wheatish skinned people 14 (46.66 %.)
Origin of the disease: Switra has a doshaja (Endogenous) origin and vranaja origin
(Exogenous). Generally due to intake of incompatible diet and other factors disease may
be produced and due to external causes likes vranas due to accidents, burns, chemical
contacts or trauma Switra may be produced. Among 30 patients 28 of them (93.33%) are
of endogenous origin and 2 (6.66%) had exogenous origin. Among which 1 patient

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
127
acquired the disease due to burns with spirit and other due to trauma (Koebner’s
phenomenon). The origin of the disease due to trauma also holds significance.
Prakriti: among 30 patients, majority of the patients 9 (30%) with switra belonged to
Vata – Pitta prakriti followed by Pitta-Vata prakriti (30%) The incidence was more in
people with vata and pitta features.
Family History: The proportion of patients with positive family history varies from one
part of the world to another. In India, in particular it ranges from 6.25 – 18%. In some
studies it is as high as 40% (Behl). In the present study the incidence of family history
was 3.33% only. The absence was 96.66% it cannot be generalized, but the polygenic and
variable penetrance of the disease can be known.
History of Consangnious marriage: Among 30 subjects only 6 of them (20%)
presented with a history of consangnious marriage of parents, 24 of them (80%) had no
history.
Stress: Though stress is said to be one of the triggering factors for the disease
(Srivastava), in the present study only 7 of them presented with history of stress (23.33%)
Chronicity: Majority of the subjects, 20 of them (66.66%) had chronicity below 1 year.
The higher the chronicity, it was observed that patients’ response to treatment decreased.
The highest chronicity of the study was 6 yrs. But no severe depigmentation was noticed.
,
Old/New: Among 30 patients’ 15 patients were new cases, who started treatment with
the trial drug and 15 cases were old who previously took treatment elsewhere.
Age of first onset: Almost half the patients presented before the age of 20yrs and nearly
70-80% before the age of 30 yrs (Lerner and Nor Bend). In the present study , 50% of the
patients presented before the age of 20 yrs , 13.33% before the age 30yrs and 13.33%
before 40yrs. It is seen in majority of the patients that the disease presented before the
second decade of life and the incidence decreased in the subjects with age above 50yrs.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
128
Nidanam: As per Ayurvedic texts the ahara – vihara nidana plays an important role in
the disease. Description about the cause of the disease due to adhika amla, lavana, dadhi,
dugda, masha, pisti sevana is mentioned. In the present study majority of them 9 (30%)
did not have any particular dietary habits as mentioned above. But 16.66% patients had
history of excessive consumption of meat and 16.66% had history of excessive curd
intake.
Site of first onset: The disease has a predilection for normal hyperpigmented regions
such as face, groin, axillae, areola, and genetalia. Further lesions may develop in areas
like ankles, elbows, knees, which are subjected to repeated trauma or friction (Behl) and
the same was observed in the clinical study that about 11 patients 36.6% face was the
first site of onset and 9 patients 30% had lowerlimbs as first site of onset. In patients with
lowerlimbs were involved the patches developed at the site of knees, ankles and
bonyprominences of medial malleolus. Very less patients 1 (3.33%) presented genitals as
first site of onset.
Types: There are three types of vitiligo, localized, generalized and universal. The
localized forms includes focal, segmental and mucosal, the generalised includes the non-
segmental, universal where complete depigmentation occurs. In the present study
majority of patients 26 (86.66%) were of localized types 4 patients were of generalized
type(13.33%).No patients with universal type were seen.
Nature of spread : In 29 (96.66%) patients the lesions had gradual spread ,only one
patient had sudden spread of the patches immediately after attaining puberty. Lesions
stable for many years was not found in any patients.
Symmetry of the patches: The shape of the patches was taken into account. Equal
number of patients had symmetrical 50% and asymmetrical patches 50%. Mostly round
and oval were prevalent in symmetrical types.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
129
Leucotrichia: Hair over the patch may or may not turn white (Behl) But if hair turns
white indicates poor prognosis. In the present study only 5 patients presented with
leucotrichia. Among whom only 2 patinets responded to the treatment.
History of Allergy: H/o dust allergy was found in 1 patient 3.33%, 1 patient had food
allergy (particularly to bananas, Brinjalas) majority of them 28 (93.33%) had no H/o
allergy.
Aggravating factors: A couple of observations regarding the aggravating factors were
made during the clinical study. Majority of them 20pts (66.66%) did not have any
aggravating factors, but 4 pts observed redness of patch, burnings sensation when
exposed to sun. 2 pts (6.66%) observed intake of non-veg diet particularly chicken and
fish resulted in increase in the size of the patch, 2 patients observed taking curd caused
intense itching in the patches, the same was observed by 2pts, that taking milk caused
itching in the patches.
Colour of the patches: Among 30 patients 23 (76.6%) of them presented with white
coloured patches. 5 pts presented with light pink coloured patches, 2 pts presented with
dark pink coloured patches. Probably the application of topical creams might have lead to
the change in the colour. Old cases presented with the about two coloured patches.
Number of patches: Among 30 patients 27 (90%) of them had patches between 1-5 in
number only 1 patient had between 6-10, and 2pts had patches above 10 in number.
Size of the patches: The size measurement was possible for only 24 patients. 19
patients (82.6%) had patches ranging between 1-15cms. 2 patients has patches between
16-30 cm, 1 patient presented with patch size between 31-45 cms, 1 patient presented
with 61-75cms, above 90cms – 1 patient.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
130
Discussion on Results: The results were analysed statistically by paired‘t’ test from the
observations made during and after the clinical study. The mean age of the study
population is 28 yrs. Mean age of female population is 28.58yrs. Majority of the subjects
had mixed diet, more than females, males were vegetarians. Highest percentage of the
study population came from urban areas. In females the disease was more of systemic
type.
Colour of the patches: Among 30 patients, 24 patients (80%) responded in colour, 6
patients (20%) did not respond in the colour. The patients who have undergone complete
treatment schedule showed marvelleous improvement in the colour of the patches. The
patient came every 15 days for a review. Each time patient noticed marked changes in the
colour of patch. In the first 15 days the colour changed to light pink, in some it even
turned into darkpink. In patients who have already taken treatment elsewhere presented
with light and darkpink patches initially. In those subjects after 30 days brown
pigmentation spots were noticed .After 45 days the pigmentation improved noticeably.
Two kinds of pigmentation changes were noticed during the study. In some cases
pigmentation started from periphery bringing about changes in the size, such is peripheral
repigmentation. In some case pigmentation spots were seen around the hair follicles in
the center of the patch, gradually growing in size and changing the symmetry of the
patch, such is perifollicular repigmentation. The statistical analysis shows P<0.0001
which is significant.
Among the 24 patients responded, 11 patients showed mild response, 6 showed
moderate response, 7 showed marked response, no patients showed excellent response.
Number of patches: Among 30 patients majority of them, 27 presented with 1-5 no on
their body. 1 patient had patches in between 6-10 and 2 patients had more than 10 patches
on the body. After the treatment schedule, the patients did not show much response in the
number. But patients who responded showed moderate and marked response.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
131
Of 30 patients only 3 responded in number and 27 numbers did not show any
response in change of number of patches. Out of 3, 2 patients showed moderate response,
1 patient showed marked response. No patient showed excellent response.
The statistical analysis shows P<0.35 which is not – significant. There were
changes noticed in the patch but there was no change in the number of patches. The
patients in whom the number decreased were of recent onset and small in size. But
among few who responded in number, their response was remarkable.
Size of the patches: Among 24 patients, 19 patients had patches of size in between 1-15
cms, 2 patients had size in between 16-30 cms. 1 patient had 31-45cms, 1 patient had
patch ranging between 61-75cms, and 1 patient above 90 cms.
After completing the treatment schedule 11 patients (45.8%) responded in size, 13
patients (54.1%) did not respond. Among the 11 patients 3 showed mild response, 6
showed moderate response, 1 showed marked response, 1 patient showed excellent
response.
The change in the size of the patches was depended on the colour changes. The
repigmentation occurring in the white patches brough about the difference in size.
Peripheral repigmentation caused Shrinkage in the size and perifollicular repigmentation
brought about changes in symmetry (shape) which automatically brought difference in
the size
The statistical analysis shows P<0.1 which is not- significant. But the response
seen in the size of the patches in duration of 45 days is commendable.
During the clinical study, in the first 15 days majority of them started showing
changes in the patches. The colour change was prominent, but there was no change in the
number and size.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
132
After 30 days, the colour grading improved; the change in the colour was
even more remarkable. Pigmentation spots in the centre of patch were seen in some
patients and in few, changes from periphery were noticed. No change in the number
noticed.
After completion of 45 days – changes in the colour was even more satisfactory. Size
differences in the patches were clearly evident. Small patches of 1-3 cms disappeared and
some faded due to the pigmentation. They were not as prominent as before. Change in
number but only in 3 patients was noticed. The improvements were noticed in patients
with less chronicity, fresh cases with small sized patches. And the type was more of
localized type. In cases where the buccal mucosa was involved changes in colour was
remarkable.
During the treatment patients noticed many factors that caused irritation, itching,
burning sensation and increase in size. No blisters or oozing was noticed. Initially
patients experienced nausea, while taking the medicine but after a week the feeling
disappeared. Patients were advised for followup of 2 months. Only 12 patients had
regular followup. The changes that took after completion of treatment schedule persisted
after 2 months also. No new findings took place. No patients were Diabetic,
Hypertensive or Asthamatic hence no changes were recorded in those aspects.
Overall, from the clinical study conducted on 30 patients for duration of 45 days
satisfactorily with negligible side effects 18 patients showed mild response, 4 patients
showed moderate response, 2 patients showed marked response, no patients showed
excellent response. 6 patients showed no response to treatment at all. The initial results
are promising depending upon the response in colour, number and size. Some more time
is needed to establish the results.
Limitations of the study:

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
133
1. As the study does not have a control group, any categorical statements about the
success attribution to drug cannot be made.
2. The duration of the study is very short, it would have been better if the duration
was for a longer period to establish the results even more effectively.
3. As the sample size is very small (30pts) any significant findings found in the
study cannot be generalized to the population.
Recommendations for the future study:
1. Study to be conducted on larger samples.
2. To do a comparative study between a control group and test group with medicine
taken internally.
3. To do a comparative study between a control group taking medicine internally
and externally and test group taking medicine only internally.
4. To take a longer duration of time for clinical study.
5. To scientifically probe the action of Khadira on melanocytes.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
134
CONCLUSION
From the discussion based on this study, it becomes nearly conclusive that,
Switra is a pittapradhana tridoshaja, twak vikara. Sweta Varna mandalas appear
on the skin suggestive of the disease.
It has historical background suggestive that many people suffered from this
disease since times unknown.
Based on the clinical features it can be well correlated to vitiligo of contemporary
medicine.
The prevalence of the disease is 1% world wide, affecting males and females
equally, but incidence of females is higher due to the social stigma and
embarrassment attached to the disease.
The incidence of childhood vitiligo is rapidly increasing from past two decades.
In the present study 20% of the patients were below 10 years.
The age of first onset, is before 20yrs, face and lowerlimbs are the site of first
appearance of the disease.
Family history and H/o consangnious marriage of parents had little role to play in
the etiology. Many of the patients had no specific incompatible dietary habits, in
most of the cases etiology was unknown.
Koebner’s Phenomenon was noticed in two patients as etiology. Leucotrichia also
was not seen in majority of patients.
Certain foods caused itching, increase in size of the patches, exposure to sun
caused redness and burning sensations in the patches.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
135
Early detection and short duration of the disease, small sized patches, good
prognosis is seen.
The drug proved to be beneficial as promising results were noticed initially in
response of colour and size. No much change in number was noticed.
Out of 30 patients – 18 patients showed mild response, 4 patients moderate
response, 2 marked response and 6 members did not respond to the treatment.
Better results can be established with “Dhatri-Khadira Kwath” if study is
conducted on larger samples, for a longer duration in a comparative fashion by
enthusiastic scholars.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
136
SUMMARY
A clinical study was undertaken to evaluate or assess the efficacy of ‘Dhatri-
Khadira Kwath’ in the disease switra.
As the colour of the skin plays an important role in the lives of people, any visible
changes in the skin can make the afflicted person experience high levels of self –
conciousness and low self esteem. Patients are subjected to social embarrassment, there
by leading to psychological disturbances. Hence disease switra which is related to
hypopigmentation was selected for the study. Based on the clinical features it is well
correlated to vitiligo of contemporary science.
The etiology of the disease remains unknown. It is expected to develop as a
sequel to irregular dietary habits and life style changes. Genetic predisposition may also
account for the disease.
A comprehensive formula “Dhatri-Khadira Kwath” selected from Bhaishajya
Ratnavali was used in the clinical study. A total of 30 patients fulfilling the inclusion and
exclusion criteria were taken for the study for duration of 45 days.
The present literary work is divided into five parts which gives a detailed picture
of the disease, and clinical study.
Thte first part consists of review of literature where the literary aspect about the
historical background, anatomy, physiology of the affected part, etiology, clinical
features, differential diagnosis, prognosis, treatment and dietary restrictions are
explained.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
137
The second part contains the drug review which includes the criteria for the
selection of drug, description of individual drugs and method of preparation has been
elaborated.
The third parts comprises of methodology, observations of the study and results of
the study.
Fourth part is mainly the discussion, conclusion and summary aspect of the study.
Fifth part relates to references, bibliography, annexure which includes, master
charts and special casesheet of the study.
The present study highlights the fact that, medicine taken orally could be
beneficial in the management of Switra.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
138
REFERENCES
Historical Review:
1. Ibid 1.117.7
2. Ibid 1.117.8,24
3. Ibid 1.23.1-4: 1.24.1-4
4. Sayana on AVS .1.24.2
5. Y.V – 30/21
6. A.V. Kanda – 1: 23-24
7. A.V.S.1.23.
8. Padmapurana 1.81.2
9. Markandeyapurana 16.14
10. 1.11.35-58
11. V.P.2.115, 95
12. I.P 10.33.40
13. B.V.P1.26.26
14. Yagna.Praya.84.91-103
15. Pg.No.42 History of Medicine in India – P.V. Sharma
16. Najamabadi, M.Tarikh-E-Tib-E-Iran. Volume 1, Shamshi Tehran: 1934
17. Ebbel.B.The Papyrus, Ebesscopenhagen.lewin and Meinksgard.1937 Pg.45
18. El. Mofty AM.Vitiligo and Psoralens. Pergamon Press: Oxyford; 1968 p.1147-95
19. Goldman L, Moraites RS, Kitz miller KW White spots in biblical times. A
background for the dermatologist for participation in discussions of current
revisions of the bible. Arch Dermatol 1966; 93:744 – 53
20. ITO.M.Vitiligo.Tohokee .J. Exp.Med.1952: 5 72-6
21. Cha.Chi 7/173
22. Su.Ni 5/17
23. B.S 6th / 35
24. H.S Dwitiya stan; 4 adhyaya

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
139
25. Kashyapa samhita kusta chikitsa
26. A.S.Su 35/3
27. A.H.Ni 14/34
28. Vangasena Kustaroga adhikar/8th sloka
29. M.Ni 49/4
30. Sha.Sa madhyamakanda, kustaroga adhyay
31. B.P. 54/3
32. Srivasthava.G.Vitiligo – Introduction Asian Clinic, Dermatol 1994; 1:1 – 5
33. S.L.V 1-Chapter – 33
34. Lalitha vistara. P.L. Vaidya .Ed Mithila Institute Darbhanga 1960
35. Saddharma Pundarika PLvaidya Ed Mithila Institute Darbhanga 1960
36. K.A.S. (14.177.1)
37. Harsha Charitra – 88 , 399
38. Indian .J. Dermatol / Venerol / Leprol / May – June, 2007 Vol.73 issue 3
39. B.R. 54 Chapter Kustaroga adikar.
Nirukti:
40. Sanskrit Shabdarda Koustubha, Pd. Taranish Jha, Late Sri Chaturvedi
Dwarakaprasad Sharma. 2nd edition.
41. Carter RL, editor, A dictionary of Dermatologic terms 4 th edition, (1992)
Williams and Wilkins: Battimore
42. Nair B.K. Vitiligo retroaspect. Int J. dermatol 1978; 17:755-7
Paribhasha:
43. Amarkosha
44. Shabda Kalpa drumam, 5th vol.
45. Kashyapa samhita kusta roga adikar
46. Su.Ni 5/17
47. Dermatology in General Medicine

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
140
Shareera Rachana:
48. Shabda stoma mahanidhi, 2nd edition by Taranath Tark, Vachaspathi
Bhattacharyena.
49. Shabdakalpa drumam, 2nd Vol. Raja Radhakanth deva
50. Su.Sha 5/3
51. Su.Sha 4/4
52. A.S.Sha 5/17
53. Cha.sha 7/4
54. A.H.Sha 3/8
55. Su.Sha 1/10
56. Su.Sha 1/7
57. Su.Sha 1/26
58. Cha.Sha 7/7
59. A.H. Su 11/1
60. A.H.Su 12/8
61. Su.Su 21/9
62. Cha.Su 1/61
63. Su.Su 14/10
64. Cha.Chi 15/7
65. Cha.Vi 8/103
66. Su.Sha 3/31
67. Cha.Sha 7/4
68. Su.Sha 4/4
69. Cha.Sha 7/7
70. Su.Sha 4/4
71. A.H.Sha 3/8
72. Anatomy and Physiology by Tortora
73. Gray’s Anatomy – Integumentary system

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
141
Shareera Kriya:
74. Shabdakalpa drumam, 2nd vol
75. Su.Sha 3/31
76. Su.Sha 2/37
77. A.H. Su.12/5
78. Cha.Su 12/11
79. Su.Su 21/10
80. A.H.Su1/3
81. Cha.Ind 7/16
82. Cha.Vi 8/103
83. A.H.Su 11/4
84. Cha.Chu 1/16
85. A.H.Su 11/12
86. A.H.Su 11/15
87. Su.I 13/7 – Dal. Commentay
88. A.H.Su 11/5-7
89. Su.Su 21/9-10
90. Su.Su 21/10 – Dal Commentay
91. A.H.Su 12/14
92. A.H.Su 12/14 – Arunadutta commentary
93. Cha.Su 12/11 – Chakrapani Commentary
94. Bhelasamhita.Shareera.Purushanischaya Shareer
95. A.H.Su 11/15
96. Su.Sha 1/6
97. Su.Sha 1/10
98. Su.Sha 1/26
99. A.H. Su 12/4
100. A.H. Su 11/22
101. Cha.Su 11/48
102. Cha.Su 11/49
103. Integumentary system – Gray’s Anatomy

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
142
Nidana:
104. Cha.Ni ½ - Chakrapani Commentary
105. A.H.Ni. 14/1
106. Cha.Chi 7/177
107. A.H.Sha ¼
108. Cha.Su 26/83
109. Vangasena Kustaroga Adikar / 8 sloka
110. A.S.Su 35/3
111. Su.Ni 5/3
112. B.P. 54/4
113. M.Ni. 49/6
114. Anupan Darpan 8 chapter
115. R.T. 18/7
116. Cha.Su 13/76
117. Cha.Chi 4/26
118. Su.Su 24/6
119. Cha.Sha 1/18
120. A.H.Ni 14/1-2
121. Su.Ni 5/17-Bhoja Commentary
122. Manusmriti – History of Medicine in India P.V. Sharma
123. H.S 38/1-3
124. Kashyapa samhita, kusta rogadhikar
125. Su.Ni.5/39-40 – Dalhana Commentary
126. Cha.Chi 7/177
127. Pengun Js. Vitiligo Br.J. Dermatol 1996 : 134:373
128. Shwartz RA, Jannigar CK Vitiligo Cutes 1997; 60: 239-44
129. Behl PN, Agarwal A. Srirastava G. Vitiligo in Behl PN, Srivastava G editors’
practice of Dermatology 9 th edition CBS Publishers: New Delhi 2003.
Pg 238-41

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
143
130. Behl PN Review of Therapeutic measures in the treatment of vitiligo Indian J.
Dermatol venerol 1957 : 23: 17-24
131. Schallreuter KU. Moorej. Behrens – Williams. S. Panske A. Harari .M. Rapid
Initiation of repigmentation in vitiligo with Dead Sea climato therapy in
combination with pseudo catalase. Int .J.Dermatol 2002 : 41.482-7
132. Schallreuter KU. Successful treatment of oxidative stress in vitiligo. Skin
pharmacol App Skin Physiol 1999:12:132-138
133. Ortonne JP. Psoralen therapy in vitiligo. Clinical. Dermatol 1989:7:120-135
134. Orecchia G. Perfett .L. Phototherapy with topical khelllin and sunlight in
vitiligo. Dermatology 1992:184:120-123
135. Ivker R, Goldaber M. Buchness MR, Blue vitiligo. J. Am Acad Dermatol
1994:30:829-31
136. Michaelson G. Vitiligo with raised borders. Report of two cases Acta.Derm
Venerol 1968:48:158-161
137. Fisher AA. Differential diagnosis of idiopathic vitiligo Part III : occupational
leukoderma cutis 1994:53:278-80
138. Koga M. Aango T. Clinical features and course of type A and type B. Vitiligo
Br.J. Dermatol 1988:118:223-8
Purva Rupas:
139. M.Ni 1/6-Madukosh commentary
140. Cha.Ni 1/8 – Chakrapani Commentary
141. A.H.Ni. 14/37

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
144
142. Cha.Chi 7/12
143. Kashyapa Samhita, Kustaroga adikar
144. M.Ni 49/829
Rupa:
145. Su.Su. 21/34-Dalhana Commentary
146. M.Ni.1/7- Eshwarasena Commentary
147. M.Ni.1/7 – Madukosha commentary
148. Kashypa Samhita Kusta chikitsa
149. Su.Ni. 5/17
150. Cha.Chi 7/173
151. Cha.Chi 7/174
152. Su.Ni 5/18
153. A.H.Ni 14/38
154. M.Ni 49/38-39
155. Srivastava G. Vitiligo. Introduction Asian Clinic Dermatol 1994:1:1-5
156. Schwartz RA. Janniger CK. Vitiligo Cutis 1997; 60:239-44
157. Hann SK. Partk YK, Chun Wt. Clinical feature of vitiligo. Clinic Dermatol
1997; 15:891-7
158. Kova CS So vitiligo .J. Am Acad Dermatol 1998:38:647-66
159. Agarwal G. Vitiligo An under estimated problem Fam Pract 1998:15:519-23
160. Handu. S. Kaur.I. Vitiligo Clinical Findings in 1436 Patients .J. Dermatol
Tokyo 1999:26:653-7
161. Alkhateeb A. Fair PR, Thody A. Benett. DC, Spritz RA Epidemiology of
vitiligo and associated auto immune diseases in Caucasian probands and their
families. Pigment cell Res 2003 : 16:208-14
162. Behl PN, Bhatia RK 400 case of vitiligo – A clinico therapeutic analysis. Indian
J. Dermatol 1971:17:51-4
163. Le Poole C, Boissy RE, Vitiligo. Semin cutain Med Surg 1997:16:3-14
164. Hann SK, Lee HJ. Segmental Vitiligo. Clinical Findings in 208 pts.J.Am Acad
Dermatol 1996:35:671-4

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
145
165. Zaima H, Koga M. Clinical Cause of 44 cases of Localised type vitiligo J.
Dermatol 2002:29:15-9
166. Halder RM. Childhood Vitiligo. Cli Dermatol 1997:15:899-906
167. Cho.S.Kang, KC, Halm JH Characteristics of vitiligo in Korean children. Pedia
Dermatol 2000 : 17: 189-93
168. Manda S, Dogna. S, Epidemiology of Childhood vitiligo. A study of 625
patients from North India. Pediator Dermatol 2003:20:207-10
169. Behl PN, Agarwal A, Srivastava G. Vitiligo In. Behl PN Srivastava G. editor
Practive of dermatology 9th edition CBS Publishers: New Delhi 2003 . Pg 238-
41.
170. Herane Ml.Vitiligo and Leukoderma in Children Clinic Dermatol 2003: 21:283-
95
171. Jaigirdar MQ, Alam SM, Mardul A2. Clinical presentation of vitiligo. Mymem
Singh Med J 2002:11:79-81
172. Engel L. What are those white patches in my patients’ skin? Dermotol Nurs
2001:13:292-7
173. Leener HR, Fitz Patrik TB, Halder RM, Haulk JL. Discussion of case of
vitiligo. Photo dermatol. Photo immunol Photomed 1999 ; 15:41-4
174. Norbend .J. Lerner AB, Vitiligo - It is important. Arch Dermatol 1982: 118:5-8
175. Lerner AB, Vitiligo J. Invest Dermotol 1959: 32:285-310
176. Westerhof W.Vitiligo Window in the darkness. Dermotology 1995:190.181-2
177. Goudie BM, Wilkieson C. Goudie RB. Skin maps in vitiligo Scott Med J.
1983:28:343-6
178. Pengum JS. Vitiligo Br.J.Dermatol 1996:134-373
179. Singh P, Singh J. Agarwal US, Bhargava RK. Contact vitiligo : etiology and
treatment Indian J. Dermatol Venerol Leprol 2003; 69:27-9
180. Harder RM, Girmes PE, Cowan CA, Enterline JA, Chakrabarti SG, Kenney JA
Jr. Childhood vitiligo J. Am Acad Dermatol 1987; 16:948-54

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
146
181. Federman DG, Kravetz JD, Ruser CB, Judson PH, Kirsner Rs. Vogt - Koyanagi
Harada syndrome and ulcerative colitis. South Med J. 2004; 97: 169-71
182. Schwartz RA., Jannigar CK. Vitiligo Cutis 1997; 60:239-44
183. Behl PN, Agarwal A, Srivastava G. Vitiligo. IN Behl PN, Srinvastava G. editor
Practice in Dermatology 9th edition CBS Publishers New Delhi, 2003.Pg 238-
41.
184. Arata J, Abe – Mastassura Y. Generalized vitiligo preceded by a generalized
figurate erythemato squamous eruption. J Dermatol 1994; 21:438-41
185. Fisher AA Differential diagnosis of idiopathic vitiligo from contact leucoderma
Part II leucoderma due to cosmetics and bleaching creams. Cutes 1994:53:232-4
186. Adbel Naser MB, Ludwing WD, Goldrick H, Or fornos CE Non – segmental
vitiligo decrease of the CD4 5RA T – Cell subset and evidence for peripheral T
cell activating Int J. Dermatol 1992; 31: 321-6
187. Goudi RB, Spence JC, Markie R. Vitiligo Pattens stimulating autoimmune and
rheumatic disease lancet 1979; 2:393-5.
188. Wayne DM, Hebig EB. Halo Nevi Cancer 1968; 22:69-90
189. Handa S, Dogra S. Epidemiology childhood vitiligo A study of 625 patients
from North India. Pediat Dermatol 2003; 20:207-10
190. Pengum Js. Vitiligo Br J. Dermatol 1996; 134:373
191. Wee TA. A case report of extensive vitiligo. Harvair Med J. 1997; 56:37-40
192. Drake L, Dinchart SM, Farmer FR, Goltz RW, Graham GF, Hordinsky MK.
Et.al Guidelines of care for vitiligo patients. J. Am Acad dermatol 1996;
35:620-6
193. Hann SK, Chun WH, Park YK Clinical Characteristic of Progressive vitiligo
Int.J. Dermatol 1997; 36:353-5
194. Hartmann G, Panconesi E. Vitiligo: A psychologically influencing diseases.
Clinic Dermatol 1997; 15:879-9
195. Mathias CG, Maibach HI, Conant MA. Perioral leukoderma stimulating vitiligo
from use of toothpaste containing cinnamic aldehyde. Arch Dermotol 1980:
116:1172-3

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
147
196. O’ Sullivan JJ. Stevenson CJ. Screening for occupational vitiligo in workers
exposed to hydroquinone monoethyl ether and to para tertiary amyl-phenol
Br.J.Ind Med 1981; 38:381-3
197. Dupre A, Christol B. Cockade – like vitiligo and linear vitiligo a variant of Fitz
patrick’s trichrome vitiligo Arch Dermatol Res 1978; 262: 197-203
198. Ivker R, Goldaber M, Buchness MR, Blue vitiligo J. Am Acad Dermatol
1994:30:829-31
199. Arata.J. Abe-Mastura Y. Generalised vitiligo preceded by a generalized figurate
erythemato squamous eruption J.Dermatol 1994; 21: 438- 41
200. Michaelsson G. vitiligo with raised border –report of two cases. Acta Derm
venevol 1968; 48:158-61
201. Fisher AA. Differential diagnosis of idiopathic vitiligo Part III: occupational
leucoderma cutis 1994; 53:278-80
202. Sehgal VN, Rege VL, Mascarnhas F, Kharangata UN Clinical pattern of
vitiligo amongst Indians J. Dermatol Tokyo 1976; 3:49-53.
203. Ortone JP, Bahadoran P, Fitz Patrick TB. Hypomelanosis and hypermelanosis.
In Freeberg IM, Eisen AZ Wolff K, Austen KF, Gold Smith LA, Katz SI, Fitz
Patrick TB, editors. Dermatology in general medicine MCGraw Hill: New York
1999 Pg.836-47
204. Adams BB, LeukyAW. Colocalization of alopecia areata and vitiligo. Pediats
Dermatol 1999; 16:364 – 6.
205. Smyth Jr.Jr. Mc.Neil M. Alopecia areata and Universalis in the Smyth chicken
model for spontaneous auto immune vitiligo. J. Investigation Dermatol Syrup
Proc 1999;4:211-5
206. Khandpur S, Reddy BS. An association of 20 nails, dystrophy with vitiligo J.
Dermatol 2001; 28:38-42
207. Lee D, LazovaR, Bolognia JL.A figurate papulosquamous variant of
inflammatory vitiligo. Dermatology 2000; 200:270-4
208. Wayte J, Wilkinson JD Unilateral lichen planus sparing the vitiliginous skin
.Br.J.Dermatol 1995; 133:817-8.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
148
209. Anstey A, Marks R. Co-locolization of lichen planus and vitiligo Br. J.
Dermatol 1993; 128:103-4
210. Kang JK, Hann SK. Vitiligo coexistent with nevus depigmentoses .J. Dermatol
Tokyo 1996; 23:187-90
211. Down’s AM; Lear JT. Dunnil MG. Polymorphic light eruption limited to areas
of vitiligo. Clinic Exp.Dermatol 1999;24:379-81
212. Malignant melanoma and vitiligo J. Invest Dermatol 1979; 73:491-4.
213. Nordlund JJ, Albert D, Forget B, Lerner AB, Halo Nevi and Vogt Koyanagi
Harada Syndrome – Manifestation of Vitiligo. Arch Dermatol 1980; 116: 690-2
214. Kumakiri M, Kimura T, Miura Y, Tagana Y. Vitiligo with an inflammatory
erythema in Vogt – Koyanagi Harada disease. Demonstration of fila mentous
masses and amyloid deposits J. cutan pathol 1982; 9:258-66.
215. Barnes L. Vitiligo and Vogt. Koyanagi – Haradasyndrome. Dermatol Clin 1988;
6:229-39.
216. Egli F, Walter R, Images in Clinical Medicine Vitiligo and pernicious anaemia
N. Engl J. Med 2004; 350-2698
217. Okada T. Sakamoto T, Ishi Bashi T, Inomata H. Vitiligo in Vogt – Koyanagi
Harada disease Immunohistological analysis of inflammatory site Gafes Arch
clin Exp Ophthalmol.1996; 234:359-63.
218. Tsurata D, Hamada T, Teramae H, Hito H, Ishii M Inflammatoy Vitiligo in
Vogt – Koyanagi Harada disease J. Am Acad Dermotol 2001, 44:129-31
219. Fournier GA, Albut DM, Wagnoner MD. Choroidal halo nevus occurring in a
patient with vitiligo. Suru Ophthalmol 1984; 28:671-2.
220. Fragnoli MC, Bolognia, JL. Pentachrome vitiligo. J. Am. Acad Dermatol 1995;
33:853-6
221. Federman DG, Kavertz JD, Ruser CB, Judson PH, Kirsner RS. Vogt-Koyanagi
Harada syndrome and Ulcerative Colitis. South Med J. 2004; 97: 169-71.
222. Halder RM, Erimes PE, Cowan CA, Enterline JA, Chakrabarti CG. Kenney JA
Jr. Childhood Vitiligo. J Am Acad Dermatol 1987; 16:948-54.
223,224,225. Singh P, Singh J. Agarwal US, Bhagavan RK. Contact Vitiligo:
Etiology and treatment. Indian J.Dermatol Venerol Leprosol. 2003; 69:27-9

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
149
Samprapti:
226. A.H.Ni.1/8
227. A.H.Ni.14/2
228. Su.Su.21/36
229. Cha.Ni 5/22-23
230. A.H.Ni. 12/22
226. A.S.Su 9/7
227. Cha.Su 24/1-10
228. A.S. Su 9/26
229. Cha.Su 8/18
230. Cha.Su 11/45
231. A.H.Su. 12/23
232. Su.Ni.5/3
233. Su.Ni 5/3 Dalhana Commentary
234. Su.Su.21/23
235. A.H.Ni.14/37
236. A.H.Ni. 14-37 Arunadutta Commentary
237. Su.Su 24/10
238. A.H.Ni 14/1-3
239. Cha.Ni 5/3
240. Su.Sha 4/33
241. Su.Su 21/34 - Dalhana Commentary
242. Amarakosha
243. Su.Ni 5/17
244. A.H.Chi. 20/1
245. Su.Ni.5/28
246. Cha.Chi 7/177
Bhedas:
247. M.Ni 49/37-39
248. Su.Ni 5/17

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
150
249. Cha.Chi 7/174
250. M.Ni 49/37-39 – Bhalukitantra
251. Cha.Chi 7/175-176
252. Kashyapa samhita Kusta Rogadikar
253. Bhela samhita 6th Chapter
254. Fitzpatrick; Elsen; Wolf Dermatology in General Medicine,
255. Behl PN, Agarwal A, Srivastava G. Vitiligo In Behl PN Srivastava G editor,
practice of Dermatology 9th edition Pg 238-41
256. Behl PN, Agarwal A, Srivastava G. Vitiligo In Behl PN Srivastava G editor,
practice of Dermatology 9th edition Pg 238-41
Sapeksha Nidan:
257. M.Ni 49/37
258. A.H.Ni 14/5 – Arunadutta Commentary
259. Cha.Chi 7/13
260. Su.Ni 5/17
261. Cha.Chi 7/28
262. Cha.Chi 7/19
263. Cha.Chi 7/37
264. Fitz Patrick, Eisen, Klaus Disorders of Melanocytes – Dermatology in General
Medicine 3rd edition
Sadya-Asadyata:
265. Cha.Vi 6/3
266. A.H.Ni.14/39
267. Cha.Chi 7/172
268. Kashyapa Samhita Kusta chikitsa
269. Bhela Samhita 6/35
270. Cha.Chi 7/176
271. Cha.Chi 7/177
272. Su.Ni 5/28

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
151
273. A.H.Ni 14/40
274. M.Ni 49/40
275. Cha.Chi 7/175
276. Su.Ni.5/28
277. B.P. 54/47
278. Dermatology General Medicine Vol-1 3rd edition
Chikitsa:
279. Vaidyata Shabda Sindu
280. B.P. Purvakanda, 54th Chapter
281. Cha.Su 9/5
282. Su.utt 1/25
283. Cha.Su 11/54
284. A.H. Chi 20/1
285. Cha.Su 11/55
286. Cha.Chi 7/162
287. Cha.Chi 7/163
288. Cha.Chi 7/164
289. Cha.Chi 7/165
290. Cha.Chi 7/166
291. B.R. 54/56
292. A.H.Chi 20/7
293. Cha.Chi 1/167
294. Cha.Chi 1/168
295. Cha.Chi 1/169
296. Cha.Chi 1/170
297. Cha.Chi 1/171
298. Cha.Su 8/16
299. Cha.Su 8/18
300. Cha.Chi 7/172

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
152
Patya – Apatyas:
306. Su.Ni 9/5 – Dalhana Commentary
307. Su.Chi 9/4
308. A.H.Chi 19/25 – Arunadutta Commentary
Drug Review:
309. B.R 54/53
310. Cha.Su 25/40
311. Cha.Chi 7/166
312. B.P. Nigantu Haritak Kyadi varga/39 sloka
313. Cha.Chi 6/48

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
153
BIBLIOGRAPHY
1. Raja Radhakanth Deva Shabdakalpadrumam 2nd Volume published by
Chaukhamba Sanskrit Bharati Varanasi.
2. Raja Radhakanth Deva Shabdakalpadrumam 5th Volume published by
Chaukhamba Sanskrit Bharati Varanasi.
3. The practical Sanskrit – English dictionary
4. Taranath Tark and Vachaspati Bhattacharyena Shabdastoma mahanidhi - 2nd
edition
5. Late Sri Chaturvedi Dwarakaprasad Sharma, Pd. Taranish Jha, editors Sanskrit
Sabdartha Koustubha 2nd edition published by Ram Narayana Lal Bini Prasad.
6. Sri mad Bhishagvarya Gadhadhara Tanaya Vangasena, Vidusha Virichita, Sri
Lala Shaligramji Vysya 1st edition published by Khemraj Sri Krishna das Setina.
Venkateshwar Steam press Bombay.
7. J.G.G. Ledingham, David .A.Warrel, editors Concise Oxford Text book of
Medicine 4th edition.
8. Late Peter .L. Villiams, editor Gray’s Anatomy 38th edition.
9. Gerard.J. Tortora, Grabowski, Sandra Raynolds Principles of Anatomy and
Physiology 7th edition
10. Guyton and Mall editors Textbook of Medical Physiology 9th edition.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
154
11. K.L. Bhishagratna, Translator and editor Sushruta Samhita (English) Volume 2
published by Choukamba Sanskrit Series.
12. Haritha Samhita 1st edition (1953), published by Choukamba Sanskrit Sansthan.
13. Acharya Girija Dayalu Shukla., Editor Bela Samhita 1st edition (1959)
published by Choukamba Vidya Bhavan.
14. Vriddha Jeevaka, Revised by Vatsya The Kashyapa Samhita. 1st edition (1953)
Sanskrit introduction by Pt. Hemaraj Sharma, with Hindi translation of Sanskrit
introduction by Ayurveda alankar Sri Satyapala Bhisagacharya. Published by
Jaya Krishna Das Hari Das Gupta, Choukamba Sanskrit Sansthan.
15. Vd. Ranjit Rai Desai, Ayurvedeeya Kriya Shareer, 6th edition, published by Shri
Baidyanath Ayurved Bhavan.
16. Carter RL, editor, A Dictionary of Dermatolegic Terms, 4th edition (1992)
Williams and Wilkins: Battimore.
17. Fitz Patrick TB. Hypomelanosis South Med J 1964; 57: 995-1005
18. PV Sharma editor, History of Medicine in India Published by the Indian
Material Science Acadamy.
19. Acharya Raghuveer Prasad Trivedi. Editor, Charmaroganidarshika 2nd edition.
Published by Shri Baidyanath Ayurved Bhavan.
20. R.Marks.Roxburgh’s common skin diseases 17th edition. Published and
distributed by Oxford University Press.Inc.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
155
21. Professor Ramharsh Singh Bruhattar Kayachikitsa. 1st edition. Published by
Varanaseya Sanskrit Samsthan.
22. P.C. Hayes, T.W Markay; E.H. Forrest. Churchill’s pocket book of medicine.
2nd edition. Published by Churchill living stone.
23. Prof K.R. Srikanta Murthy, Astang Sangraha of vagbatta – Sutrastana. 6th
edition. Published by Chaukambha Orientalia.
24. P.D. Gyaras RamSharma, Anupana Darpanam. 1st edition. Published by
Khemraj Sri Krishnadas. Venkateshwar Steam Press, Bombay.
25. Dr. M. Ramasundar Rao, Shareera Kriya Vignanam, 2nd edition. Published by
Metroprinters, Vijayawada.
26. Dr. Ram Karan Sharma, V.D. Bhagvan Das. Charaka Samhita – Sutrastan
(English). 2nd edition. Published by Chaukambha Sanskrit Series.
27. Prof.P.V. Sharma, editor, Translator, Charaka Samhita - Sutrastan (with
English translation) 1st edition. Published by Chaukambha Orientalia.
28. Sehgal Virendra N, Srivastava Govind. Vitiligo – Compendium of Clinico –
epidemiological features. Ind.J. of Dermatology/Venerol/Leprol/ year 2007, Vol
73, issue 3.
29. Singh P, Singh J, Agarwal U.S, Bhargava RK. Contact Vitiligo: Etiology and
Treatment. Ind.J. of Dermatology/Venerol/Leprol/ year 2003, Vol 69, issue 1.
Pg-27-29.
30. Kirtikar and Basu, Indian Medicinal Plants Vol.II, 2nd edition. Published by
Lalith Mohan Basu.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
156
31. Kirtikar and Basu, Indian Medicinal Plants Vol.III, 2nd edition. Published by
Lalith Mohan Basu.
32. Dr. J.L. N. Sastry Illustrated Dravyaguna Vijnanam. Vol.II, 2nd edition (2005)
Published by Chaukamba Orientalia.
33. Vaidya Ratnam P.S. Varier’s Indian Medicinal Plants – A Compendium of 500
Species Vol.I, 1st edition. Published by orient Longman.
34. Vaidya Ratnam P.S. Varier’s Indian Medicinal Plants – A Compendium of 500
Species Vol.IV, 1st edition. Published by orient Longman.
35. Vd. Yadavji Trikamji, Introduction by P.V. Sharma Sushruta Samhita, with
Dalhana Commentry. 7th edition. (2002). Published by Chaukamba Orientalia.
36. Vaidya Visarada V.S. Venkatasubramania Sastri, V.D. Vi.C. RajaRajeshwara
Sharma, editors, Bhela samhita. C.C.R.A.S – Litrerary Research Unit, New
Delhi.
37. Prof K.R. Srikanta Murthy, Sushruta Samhita (Text, English Translation,
Notes) Vol.I, 1st edition (2000) Published by Chaukamba Orientalia.
38. Prof. K.R. Srikanta Murthy Vagbhatta’s Astang Hrudayam (English) Vol.II 4th
edition (2000) Published by Krishnadas Acadamy, Varanasi.
39. Sri Bhaskara Govinda Ghanekar Sushruta Samhita, Shareerastan 2nd edition,
published by Jayakrishna Das Haridas Gupta Chaukamba Sanskrit Series.
40. P.V. Sharma, editor and translator, Sushruta Samhita with English Translation
1st edition, (1999) published by Chaukamba Bharathi Acadamy.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
157
41. Kaviraj Ambika Dutt Sastry Sushruta Samhita (Hindi) 6th edition, published by
Chaukamba Sanskrit Series.
42. Acharya P.V. Sharma Dravyaguna Vignana (Hindi) Vol.II 8th edition, Published
by Chaukamba Bharathi Acadamy.
43. Sri Vishwanath Diwedi Aushadi Vignan Sastra 3rd edition (1986) published by
Shri Baidyanath Ayurved Bhavan Limited.
44. Vd. Laxmipathi Sastri, Bhisagrathna Brahma Shankara Sastri, editor
Yogaratnakar (Hindi) with Vidyotini Commentory 7th edition. Published by
Chaukamba Sanskrit Series.
45. Dr. Vidyadhar Sukla padarth vignan Darpan, 2nd edition (1989) Foreword by
Ach. P.V. Sharma. Published by Chaukambha Surabharathi Prakashan.
46. Vd. Yadavji, Trikamji editor Charaka Samhita by Agnivesa, Revised by
Charaka and Dridabhala of Chakrapani datta. 5th edition. Published by
Chaukamba Sanskrit Series.
47. Bhishagvachaspathi Pd. Durgadutta Sastry Sharangdhara Samhita (Hindi) with
tatwa Dipika. (2002) Published by Chaukamba Vidya Bhavan.
48. Kaviraj Ambika Dutt Sastry Bhaishajya Ratnavali (Hindi) editor by Rajeshwar
Dutta Sastry 16th edition (2002) published by Chaukamba Sanskrit Samsthan.
49. Spring House Hand book of Signs and symptoms.
50. Dr. Seetha Devi. P “A clinical study on the effect of Lepa in Switra”. Mysore
2003

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
158
51. Dr. Mahantesh P.M. “A Comprehensive Management of Kilasa Kusta
(Vitiligo) Hubli 2006.
52. Dr. Prabhakar M. “A clinical Study on the effect of Bakuchi Processed in
vibheetaki and kakodumbara Kashaya (internally) on switra (Vitiligo).
53. Dr. Venugopal Ch. “A Clinical Study on the effect of Kaseesa Badda Ras
(Internally) with and without chitrakalepa in switra (Vitiligo)
54. Dr. Ratna Priyadarshini Y “ A clinical Study on the effect of Eladi kwath in the
management of muthrashmari (Uro lithiasis)
55. Agnivesa Charaka Samhita (Hindi) by Chaukamba Vidyabhavan.
56. Behl P.N, Agarwal A. Srivastava G. Vitiligo In Behl PN, Srivastava. G editors
practice of Dermatology 9th edition CBS publishers New Delhi 2003.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
159
POST GRADUATE DEPT. OF KAYACHIKITSADR.B.R.K.GOVT.AYURVEDIC MEDICAL COLLEGE, HYD-038.
“A CLINICAL STUDY ON THE EFFECT OF “DHATRI- KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
SPECIAL CASE SHEET
Name : OP/IP No:Age : Pt.Code No. :Sex : Sp.Diagnosis:Address : Date of Research:
Drug Given:Occupation : Contact No:Marital Status :Religion / Nationality :
CASE HISTORY
1. Chief Complaint with duration :
2. Associated Symptoms :
3. History of Present Illness :
4. History of Past Illness
a. Medical Past History : DM/HTN/Br. Asthma /Anaemia / Hypo or Hyperthyroidism /koch’s /Any other Skin Disorders.
b. Surgical Past History :
5. Treatment Historya. Regarding Switram :
b. Other Illness :
6. Family Historya. Noint / Nuclearb. No. of Family Members present :c. H/o consangnious marriage in the family.d. Any member suffering with similar complaint.e. Any Psychological disturbance associated with the family.

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
160
7. Personal History:a. Socio-economics Status : LIG/MIC/HIGb. Diet : Veg/Mixed
Staple food:c. Nature of Job : Sedentery/Active/Labourious/Standing/Travellingd. Psychological Stress : Mid/Moderate/Severee. Timings : Day/Night/Late Nights/Shiftf. H/o.Allergy : Food/Drug/or Any otherg. Habits :h. Addictions :
8. Menstrual/Obestetric History:a. Menstrual Cycle :b. Marital Life :c. LCB :d. Any other disorders :
Physical Examinations:a. Height f. RRb. Weight g. Heartc. PR h. Lungsd. BP i. Abde. Temp
DASAVIDHA PARIKSHA:
a. Prakruti f. Satmyab. Vikruti g. Satwac. Saara h. Ahara Shakthi : i. Abhyaharanad. Samhananam ii. Jarana shakthie. Pramananam i. Vyayama Shakthi
j. Vayastah
ASHTASTANA PARIKSHA:
a. Nadi e. Shabdab. Muthram f. Sparshac. Malam g. Drikd. Jihwa h. Akriti
SROTO PARIKSHA:

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
161
EXAMINATION OF THE SKIN
i. AGE AT ONSET :
ii. DURATION :
iii. ETIOLOGY :a. Positive family historyb. Trauma ( Koebner’s Phenomenon )c. Incompatible foodd. Untimely sleeping habitse. Emotional disturbancesf. Stressg. Exposure to hot and cold climatesh. Consangnious marriagei. Any history of autoimmune disorderj. Drug allergy
iv. NATURE OF SPREAD:
a. Gradualb. Stablec. Sudden
v. TYPE OF LESION :
a. Symmetricalb. A symmetrical
vi. ANY H/O itching/oozing/inflammation:
vii. ANY AGGRAVATING/RELIEVING FACTORS:
viii. SITE INVOLVED:a. Faceb. Scalpc. Trunk
i. Chestii. Abdomeniii. Back
d. Limbsi. bony prominencesii. Upper limbsiii. Lower limbs
vi ORIGIN OF LESION:
I. a. Doshaja (endogenous)b. Vranaja (exogenous)

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
162
II.
VATAKA(rakta dhatu )
PITTAJA (mamsa) KAPHAJA(medo)
1. Mandala 1. Kamala parravat 1. Ghana
2. Ruksha 2. Daham 2. Guru
3. Parusham 3. Roma Vidwamsam 3. Kanduyuktam
4. Kesha Nashanam 4. Tamra Varnam 4. Swetavarnam
5. Aruna varnam
vii. TYPES OF DEVELOPMENT:
I Localized
a. Focal
b. Segmental
c. Mucosal
II. Generalized
a. Non-Segmental
b. Universal
INVESTIGATIONS:
a. CBP
B. ESR
C. RBS
TREATMENT SHEDULE:
Drug : Dhatri Khadira Kwatham for 45 days (Ref BR)
Dose : 30ml tid or 45 ml BD

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
163
DURING THE TREATMENT SCHEDULEBEFORE TREATMENT
15 days 30 days 45 daysLOCATION
Colour Number Area Colour Number Area Colour Number Area Colour Number Area
Face
Scalp
Trunk
i. Chest
ii. Abdomen
iii. Back
b. Limbs
i. Upperlimbs
ii. Lowerlimbs
ASSESSMENT OF THE RESULT : RESPONDED/NOT RESPONDED
Sign of the Guide Sign of Co-Guide Sign of PG Scholar

A CLINICAL STUDY ON THE EFFECT OF “DHATRI - KHADIRA KWATH”IN THE MANAGEMENT OF SWITRAM (VITILIGO)
164
CONSENT FORM
I, Smt. / Sri.______________________________aged ___________ years have willingly
Accepted to take the medicine given as a drug trial as a part of research programme
scheduled for 45 days. Hence I shall continue the medicine for above said tenure with
full acceptance.
Signature of the Patient.________________________________________________________________________
NOTES

A CLINICAL STUDY ON THE EFFECT OF“DHATRI-KHADIRA KWATH” IN THE
MANAGEMENT OF “SWITHRAM”(VITILIGO)
BYDr.K.NAMRATA
Guide & SupervisorDr. Prakash Chander
M.D (Ayu)Professor & H.O.D., P.G.Unit (K.C)
Ayurmitra
TAyComprehended

Introduction
Swithra is a dermatological disorder having its referencescited in the Vedas.
The term is derived from “Sweth Varne” meaning whitecolour, & is a disease related to hypopigmentation
20-30% of skin diseases require serious attention & Switra isone among them.
Based on the clinical features, swithra can be correlated toVitiligo.
Vitiligo occurs world wide with an overall prevalence of 1%. Vitiligo on the face is ranked 17th by WHO in world’s most
Disabling diseases.

CONT..
The higher incidence of the condition has been recordedin India from Asia
The etiology of vitiligo remains unknown. It is expectedto be of autoimmune origin.
Dhatri-Khadira Kwath (B.R –kusta rogadikar)has beentaken for the present study to assess the efficacy incausing pigmentation in white patches of swithra.

SHAREERA RACHANA
Twak is defined as “Twach Samvarne” meaning the onewhich covers.
Sushruta mentioned seven layers of skin namely,Avabhasini, Lohitha, Swetha , Tamra, Vedini, Rohini,Mamsadhara.
Tamra is the seat for Kilasa or Swithra.Charaka has mentioned 6 layers of skin namely,
Udakadhara, Asragdhara, Tritiya, Chaturtha, Panchami,Shasti.
Tritiya is the seat for Kilasa or Swithra.

SHAREERA KRIYA
Twak covers the underlying rakta, mamsa, medo dhatus Twak imparts varna to the body. Imparting varna to the body is a specialized function of
the Bhrajakapitta.The third vital function of twak is thermo regulation by
the virtue of pitta . Other functions include –being a sense organ,acting as a
channel to excrete sweda. It belongs to bahya roga marga .

NIDANA
a. Aharaja nidan:Vagbatta mentioned, a pregnant women consuming
excessive kaphakara ahara, the baby shall be affectedwith switra.
Gramya, anupa, jaleeyamamsa sevanam, anantharamdugda sevanam, Navanna, dadhi, matsya, lavana, amla,masha, mulaka, pisti, tila, ksheera, Guda sevana.
b. Viharaja NidanChardi, Mala-mutradi vegadharana ,Ati vyayamam , Ati
Santapasevanam ,Vyayamam in ajeernaavasthaGarma srama, Bhayarthanam sheethambu sevanam.

CONT..
c. Chikista sambandhi Nidana:Vagbatta mentioned usage of savisha jalouka in rakta
mokshana leads to switra at that site 110
Doing dushita rakta stambana leads to kilasa and kustaVishesha Nidana specially mentioned by charakaViruddha annapana sevana ,Vacham asatyamPapa karmas ,Krutagna bhavasNinda suranam ,Guru garshanamPoorva kruta karmas

RUPA
Swetha Varna mandalas on the body is the pratyatmakalinga of switram.
It is Twagtam and aparisravi .vataja, pittaja, sleshmaja types of switram have beendescribed which invade rakta ,mamsa &medo dhatus
If the doshas are present in rakta dhatu they producerakta varna,
when in mamsa dhatu produce tamra varna,and in medodhatu produce swetha varna.

SAMPRAPTI GHATAKAS
Doshas : Pittapradhana tridosha Dushya : Rakta, mamsa, medo dhatus Agni : Jataragni, dhatwagni Ama : Agnimandyam, dhatwagni
mandyam Udbhavastan : Amapakwashyam Sanchara : Tiryakgata siras Srotas : Rasa, rakta, mamsa, medo Srotodusti : Sanga Adhistana : 4th Layer of twak “Tamra” Vyaktastana : Twak Rogamarga : Bahya Vyadhi Swabhava : Chirakari

SADHYA-ASADHYATA
The deeper the involvement of the dhatus the prognosisbecomes worse.
Rakta Varna or Aruna Varna are sadhya, Tamra Varna becomes kasta sadhya andSweta Varna becomes asadhya.Charaka mentioned a person who has followed vamana –
virechana, rakta mokshana regime completely, whotakes sattu regularly and whose papakarmas are over,such case is sadhya.

CHIKITSA
The treatment aspect includes three types of therapiesto combat the disease
Daiva Vyapashray chikista – spiritual therapyYukti vyapashray chikista - rational therapySatvavajaya chikista – psychological therapyCHIKITSA SUTRAM : In switra roga, a person is made to undergo all the
shodhana procedures first. After patient is fully evacuated, samsrama karma is done
as primarily by giving malapu ras (Kakodumbara) alongwith gudam.

CONT….
After that he should be exposed to the sun for 3 days. If patient feels thirsty, peya is given to quench his thirst . patient develops blisters on the patches all over the body. The
blisters should be pricked with kantakam to release the fluid init.
After all the blisters are opened, a kwath prepared from barkof kakodumbara, priyangu, asan, and shatapushpa should begiven early in the mornings for 15 days
Sprinkling khadira kwatha externally & taking it internally ordrinking khadira udaka is very beneficial in switra.
Gomutram is very useful in switra roga..

DRUG REVIEW
The present drug “Dhatri-Khadira Kwatham” has been takenfrom “Kustarogadhikar” of “Bhaishajya Ratnavali”,
The compound has two drugs – Khadira and Amlaki, Madhu asanupana.
The drugs are non-controversial, unadulterated, easilyavailable, and economical
It is a simple combination and easy to prepare and use. Khadira is mentioned as “Kustagnanam” The use of Khadira Kashaya or Khadira udaka internally and
externally is highly recommended in swithra.

CONT…
Khadira is the Sheeta Viryadravya having tikta, Kashayarasas.Tikta rasa has ama pachana &vishagna prop.Khadira has Pitta Shamaka and rakta shodaka property.As Rakta and pitta are both vitiated in switra Khadira actsbest in this aspect.
Amlaki also is sheeta virya dravya ,having best pittashamaka effect.
Amlaki, is the best rasayanam , for rasa and rakta dhatusHelps to build immunity, and may hinder the
autoimmune reactions in the body. Amlaki has the best anti - oxidant property which can
counter the effects of toxins in the skin

CONT
It has a mild laxative effect which is very beneficial inthe treatment.
Regular use of amlaki destroys diseases like Swithra andPrameha.
The form of administration is kwatha which has highefficacy
The bark of Khadira, fruits of Amlaki are used in thepreparation
Khadira bark is pounded into coarse powder & weighed.Equal quantity of amlaki fruit is pounded and added to it.
The powder is made into kwath churam.

KHADIRA BARK

AMLAKI FRUITS

DHATRI KHADIRA KWATH CHOORNAM

CLINICAL STUDY-METHODOLOGY The study was conducted in the Department of Kayachikitsa, Govt.
Ayurvedic Hospital, Erragadda,Hyderabad. Aim: To assess the efficacy of Dhatri – Khadira kwath in causing
pigmentation in white patches of switra. Source of Data : Patients of either sex aged between 5-70 years
diagnosed as switra were selected from OPD of Govt.AyurvedicHospital, Erragadda, Hyderabad.
Sampling Method and Research Design: The study was conductedas an open trial study with randomized selection of patients .
Informed consent from all patients was obtained prior to the study. A complete history was taken through a special proforma including
age of onset, duration, family history of switra, H/o consangniousmarriage of parents, any personal or family history of systemicdiseases.

INCUSION CRITERIA
Patients of either sex with sweta varna mandalas (i.e. milky whitepatches, centrally hypopigmented with sharp circumscribed borders).
Patients aged between 5-70 years Chronicity less than 6 years. Exclusion criteria: as per ICD-10, L00-L99 skin and sub-cutaneous
diseases, L80-Vitiligo Patients below 5 years and above 70 years Certain conditions originating in the perinatal period (P00-P96) Certain infectious and parasitic diseases – (B00-B99) Complications of pregnancy and childbirth (O00-O99) Endocrinal, nutritional and metabolic diseases (E00-E90). Neoplasms (C00-D48)&Systemic connective tissue disorders (M30-M36)

INVESTIGATIONS
Following investigations were done prior to the study.
CBP,ESR ,RBS ,CUEDiagnostic Criteria: Swetavarna mandalas with or
without other features of switra Intervention:Drug: Dhatri – Khadira kwathDose: 30ml tid, followed by madhu as anupanaRoute: OralDuration: 45 days

Assessment criteria
The assessment was made on the COLOUR , NUMBER and SIZE ofthe mandalas which were observed before, during and after thetreatment.
To assess the improvement in the colour the following grading wasgiven
C0 – Normal skin colour C1 – Tanned brown C2 – Light brown C3 – Dark pink C4 – Light pink C5 – White colour The data obtained before and after treatment were analysed.

CONT..
The complete results of treatment were ascertained in terms of, 1-25% - Mild Response 26-50% - Moderate Response 51-75% - Marked Response 76-100% - Excellent Response 0 - No Response If the symptoms of a patient decreased by 1-25% he is put in mild
group, decrease in symptoms by 26-50% he is placed in moderategroup,
Relief of symptoms by 51-75% he is placed in marked group, reliefby more than 75% he is placed in excellent group ,no relief ofsymptoms were placed in no response group.

OBSERVATIONS
INCIDENCE OF AGE: Maximum number of patients 7(23.3%)fall under11-20 yrs group.
INCIDENCE OF SEX : more of females 17(56.6%) INCIDENCE OF HABITAT: Majority of the subjects came from urban
areas 23 (76.6%) INCIDENCE OF RELIGION: Majority of the subjects belong to Hindu
community 21 (70%). INCIDENCE OF MARITAL STATUS: Most of the patients t were un-
married17( 56.66%). INCIDENCE OF DIET: Majority of the subjects had mixed diet 23 (
76.66%) INCIDENCE OF SOCIO-ECONOMIC STATUS: Majority of the subjects
belong to middle income group,17( 56.6%). INCIDENCE OF OCC:Majority of the patients belonged to student community 16(53.33%)

OBSERVATIONS
ORIGIN OF THE DISEASE: The origin of the disease due to externalcauses were found in two subjects 6.66% and in majority of subjectsthe cause was endogenous 28(93.33%)
COLOUR OF THE PT: Majority of the subjects were wheatishskinned people14( 46.66%)
PRAKRITI: Majority of them belonged to vatapitta and Pitta vataprakruti 30%.
FAMILY HISTORY: Majority of the patients did not present with afamily history 29(96.66%)
STRESS: Majority of the patients did not present with history ofstress 25(76.66%).
CONSANGNIOUS MARRIAGE OF PARENTS: Majority of patientsdid not present with history of consangious marriage of parents24(80%).

OBSERVATIONS
CHRONICITY : Most had chronicity of disease from 1 month to 1 year20(66.66%)
Old/New cases: 15 patients were new and 15 patients were old whoalready received treatment else were.
AGE OF ONSET: In majority of patients disease started before theage of 20 yrs 15(49.99%)
SITE OF ONSET: In majority of subjects face was the site of firstonset 11(36.66%) followed by lower limbs 9( 30%)
Nature of spread: Among 30 subjects 29 of them presented withgradual spread of the disease 96.66%
History of allergy: Among 30 subjects 28 of them had no specifichistory of Allergies 93.33%

OBSERVATIONS
Colour of the patches: Among 30 subjects 23 of thempresented with white coloured patches 76.66%
Number of patches: Among 30 subjects 27 of them had 1-5number of patches on them 90%
Size of Patches (for 24 patients only): 19 of them presentedwith patches between 1-15cm size 82.60%

OBSERVATIONS
BEFORE TREATMENT AFTER TREATMENT

BEFORE TREATMENT AFTER TREATMENT

BEFORE TREATMENT AFTER TREATMENT

RESULTSResponded/Not responded
Sl.No. Parameter Responded
% Notresponded
%
1. Colour 24 80% 6 20%
2. Number 3 10% 27 90%
3. Size (for24
Pts)
11 45.8% 13 54.1%

Response in the colour of the patches
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 11 6 7 0 6

Response in the number of patches
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 0 2 1 0 27

Response in the size of the patches
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 3 6 1 1 13

Overall Results
Sl.No. Mild
(1-25%)
Moderate(26-50%)
Marked(51-75%)
Excellent(76-100%)
Noresponse
1. 18 4 2 0 6

Statistical analysis of the results
PARAME
TER
MEAN MEAN
DIFF.
STD
DEV
STD
ERR
t
Value
p
Value
REMARK
S
COLOUR
BT
4.44 0.84 0.48 0.08 6.6 < 0.0001 SIGNIFIC
ANT
COLOUR
AT
3.6 1.1 0.2
NUMBER
BT
1.66 0.28 2.23 0.41 1.7 <0.35 NOTSIGNIFIC
ANT
NUMBER
AT
1.38 1.94 0.36
SIZE BT 12.36 0.02 24.4 4.45 2.05 <0.1 NOTSIGNIFIC
ANT
SIZE AT 12.34 24.3 4.2

DISCUSSION
Switra is an ancient malady due to its references being cited in theVedas.
Switra can be well correlated to Vitiligo as both have similar clinicalfeatures and presentation of the disease. Both the diseases arerelated to hypopigmentation.
The etiology of vitiligo remains unknown, only the Triggering /Precipitating factors are identified, among which nutritionaldeficiency, emotional stress ,infections, exposure to chemicals areincluded. The etiology of Switra is given as incompatible diet,misconduct, improper life style.
No prodromal symptoms were seen. Swetavarna mandalas” were clearly evident,

CONT…
switra is “Twagatam” and “Aprasravi”accordingly in subjects the skin wasonly involved, no pain or secretions were noticed.
The macules were found to be of round, oval and irregular in shape. Among the mucosal surfaces ,lips were commonly involved. There are no special laboratory investigations to diagnose switra. From past two decades there is a sharp rise in the incidence of childhood
vitiligo (Behl) and the same was observed in this study. It was noticed that non –veg diet accelerated the disease progression. The origin of the disease due to trauma also holds significance. The higher the chronicity, it was observed that patients’ response to
treatment decreased. pts observed redness of patch, burnings sensation when exposed to sun.

COLOUR OF PATCH
Two kinds of pigmentation changes were noticed during thestudy
pigmentation started from periphery bringing aboutchanges in the size, such is peripheral repigmentation.
In some cases pigmentation spots were seen around the hairfollicles in the center of the patch, gradually
growing in size and changing the symmetry of the patch,such is perifollicular repigmentation.
The statistical analysis shows P<0.0001 which is significant.

NUMBER OF PATCHES
Among 30 patients , 27 presented with 1-5 no on theirbody. 1 patient had patches in between 6-10 and 2patients had more than 10 patches on the body.
Out of 3, 2 patients showed moderate response, 1patient showed marked response. No patient showedexcellent response.
The statistical analysis shows P<0.35 which is not –significant.

SIZE OF PATCHES
The change in the size of the patches was depended onthe colour changes.
The repigmentation occurring in the white patchesbrough about the difference in size.
Peripheral repigmentation caused Shrinkage in the sizeand perifollicular repigmentation brought about changesin symmetry (shape) which automatically broughtdifference in the size
The statistical analysis shows P<0.1 which is not-significant. But the response seen in the size of thepatches in duration of 45 days is commendable.

CONT.. In the first 15 days majority of them started showing changes in the
patches. The colour change was prominent, but there was no changein the number and size.
After 30 days, the colour grading improved remarkably, but nochange in the number was noticed.
After completion of 45 days – changes in the colour was even moresatisfactory.
Size differences in the patches were evident. Small patches of 1-3cms disappeared and some faded due to the pigmentation.
The improvements were noticed in patients with less chronicity,fresh cases with small sized patches.

LIMITATIONS OF THE STUDY
As the study does not have a control group, anycategorical statements about the successattribution to drug cannot be made.
The duration of the study was short, it wouldhave been better if the duration was for a longerperiod to establish the results even moreeffectively.
As the sample size is very small (30pts) anysignificant findings found in the study cannot begeneralized to the population.

RECOMMENDATIONS
Study to be conducted on larger samples. To do a comparative study between a control
group and test group with medicine takeninternally.
To do a comparative study between a controlgroup taking medicine internally and externallyand test group taking medicine only internally.
To take a longer duration of time for clinicalstudy.
To scientifically probe the action of Khadira onmelanocytes.

CONCLUSION
Switra is a pittapradhana tridoshaja, twak vikara. Sweta Varna mandalas appear on the skin suggestive of the disease. Based on the clinical features it can be well correlated to vitiligo of
contemporary medicine. The prevalence of the disease is 1% world wide, affecting males and
females equally, but more commonly reported by females. The incidence of childhood vitiligo is rapidly increasing from past
two decades. The age of first onset is before 20yrs, face and lowerlimbs are the
site of first appearance of the disease. Family history and H/o consangnious marriage of parents had little
role to play in the etiology.

CONT…
The drug proved to be beneficial as promising results were noticedinitially in response of colour and size. No much change in numberwas noticed.
Out of 30 patients – 18 patients showed mild response, 4 patientsmoderate response, 2 marked response and 6 members did notrespond to the treatment.
Better results can be established with “Dhatri-Khadira Kwath” ifstudy is conducted on larger samples, for a longer duration in acomparative fashion by enthusiastic scholars.

SUMMARY
A clinical study was undertaken to assess the efficacy of ‘Dhatri-Khadira Kwath’ in the disease switra.
Switra is related to hypopigmentation was selected for the study. 30 pts of either sex were taken for the study duration of 45 days
fulfilling the inclusion and exclusion criteria Comprehensive formula “Dhatri-Khadira Kwath” selected from
Bhaishajya Ratnavali was used in the clinical study Three parameters were taken to assess the improvement –colour
,number ,size of the mandalas. The work is divided into five parts which gives a detailed picture of
the disease, and clinical study.

THANK YOU

My commitment increases my level of energy. My energy increases my level of action. Myaction increases my level of success. My success increases my level of commitment.
Research in any field is the most important section of development. Ayurveda is inservice is for ages to the needy mankind to relieve their ailments and recording the factsfor the future generations. At present the Ayurveda research scholar, developing theAyurveda and understanding under the limelight of contemporary scientific backgrounds.The plagiarism is more and more now a day in the scientific community. This ishappening as the researches of the various institutions are not available for the commonresearcher. We wish to control this plagiarism by contributing the dissertations forscientific community. If you find any thesis is a copy of the previous publication, we takethis issue to the university authorities for proper action. The solution to prevent copy catsis … http://ayurvedaresearch.wordpress.com/
Dr. Shiva Rama Prasad Kethamakka