Sustainable tailored integrated care for older people in ... · The SUSTAIN project is funded under...
43
Sustainable tailored integrated care for older people in Europe (SUSTAIN-project) Lessons learned from improving integrated care in Austria
Transcript of Sustainable tailored integrated care for older people in ... · The SUSTAIN project is funded under...

Sustainable tailored integrated care for older people in Europe (SUSTAIN-project)
Lessons learned from improving integrated care in Austria

2
Colophon
Christina HäuslerAustrian Interdisciplinary Platform on Ageing / OEPIA
Georg RuppeAustrian Interdisciplinary Platform on Ageing / OEPIA
Contact: [email protected]@oepia.at
The SUSTAIN project is funded under Horizon 2020 – the Framework Programme for Research and Innovation (2014-2020) from the European Union under grant agreement No. 634144. The content of this report reflects only the SUSTAIN consortium’s views. The European Union is not liable for any use that may be made of the information contained herein.

3
TABLE OF CONTENTS
Key points
• Findings indicate that fostering a more integrated provision of dementia care across different health care sectors can lead to improvements regarding person-centered, prevention-orientated, safe and coordinated care.
• Improvements of integrated care are highly context dependent and there is no one-size-fits-all solution. A tailored approach should be considered that utilizes a variety of key and enabling factors.
• Single individuals/organizations so called champions played a pivotal role regarding integrated care improvements.
• Fragmentation of responsibilities, information flows, financial and personnel resources were recognized as main barriers of establishing integrated care in Austria.
• An overarching approach, including already engaged champions on professional or organizational level as well as steering from outside to provide resources (e.g. policy/decision maker) are needed to support change and sustain improvements within the health care system.

4
CONTENTS
1. INTRODUCTION 61.1 Integrated care in Austria 61.2 The SUSTAIN project 71.3 SUSTAIN sites in AUSTRIA 81.4 Reader’s guide 8
PART 1 GERONTOPSYCHIATRIC CENTRE (GPZ) 10
2. GERONTOPSYCHIATRIC CENTRE (GPZ): CHARACTERISTICS AND IMPROVEMENT PROJECT 11
2.1 General description of the site 112.2 Rationale for improvement project 112.3 Aims and objectives of the
improvement project 122.4 Explanation of the improvement project 12
3. FINDINGS OF THE IMPROVEMENT INITIATIVE IN GERONTOPSYCHIATRIC CENTRE 16
3.1 Introduction 163.2 What seems to work? 163.3 What are explanations for succeeding and
improving integrated care initiatives? 193.4 What are explanations for not succeeding
and improving integrated care initiatives? 20
4. MAIN LESSONS LEARNED FROM GERONTOPSYCHIATRIC CENTRE (GPZ) 23
4.1 Working towards integrated care improvements that could have an impact 23
4.2 Working towards integrated care improvements that could be transferable across the EU 24
4.3 Methodological reflections 254.4 Overall reflections and keypoints 25
PART 2 COORDINATED PALLIATIVE CARE STYRIA (CPC) 26
5. COORDINATED PALLIATIVE CARE STYRIA (CPC): CHARACTERISTICS AND IMPROVEMENT PROJECT 27
5.1 General description of the site 275.2 Rationale for improvement project 275.3 Aims and objectives of improvement project 28
6. FINDINGS OF THE IMPROVEMENT INITIATIVE IN COORDINATED PALLIATIVE CARE STYRIA (CPC) 31
6.1 Introduction 316.2 Reasons for the withdrawal from SUSTAIN 316.3 Barriers and facilitators for improving
integrated care initiatives in Austria 326.4 Reflection and key points 32
PART 3 33
7. OVERALL (NATIONAL) REFLECTIONS 347.1 Conclusion 347.2 Implications of SUSTAIN for integrated care
in Austria 347.3 Policy recommendations 357.4 Recommendations for service providers 35
8. REFERENCES 37
9. ANNEXES 409.1 Practical measures for monitoring outcomes
and progress of the implementation of the improvement plans. 40

TABLE OF CONTENTS

6
TABLE OF CONTENTS
1.1 Integrated care in Austria
In Austria, the integration of care both within the health system and between health and social care has been a major challenge over the past two decades. This is due to the fragmentation of responsibilities, information flows and funding sources (Nolte et al., 2012). However, with the rising number of people with chronic conditions and new patterns of care needs (e.g. due to dementia and other cognitive impairments), problems at the interfaces, e.g. between hospitals and community care, have become evident. Therefore, a number of initiatives have been started in Austria to adapt organizational structures and processes, e.g. information exchange and discharge from hospital, as well as education and training programs. Still, related reforms remain piecemeal, are often discontinued and not systematically evaluated.
The establishment of Regional Health Funds (2006) stipulated so-called ‘reform pools’ with the aim of promoting projects to improve coordination and cooperation between primary care and hospital care. For instance, in Vienna the ‘Patient-oriented, integrated health care’ project (‘Patientenorientierte Integrierte Krankenbetreuung – PIK’) aimed to implement an independent discharge management across the whole city (http://www.pik.or.at 1). Similar projects were started in a few other Austrian regions. Furthermore, integrated planning of health services across sectors was introduced by 2008 to strengthen the implementation of needs- and patient-based pilot projects. As a result, a number of disease management projects (DMP) were developed in various regions and for selected diseases. The results of these projects were however limited. For instance, by 2012, only 32,000 patients and less than 1,000 physicians participated in the DMP “Therapie Aktiv” that had been introduced in six Austrian regions. Additionally, on average only 15.8 % of the funds allocated for the “Reformpool”
were used, with regional variations ranging from 1.5% in Tyrol to 33% in Styria (Schang, Waibel, & Thomson, 2013).
In the area of long-term care (LTC), some improvements supervised by the Ministry of Labour, Social Affairs and Consumer Protection have been made. For instance the ‘National Quality Certificate’ (NQZ, https://www.sozialministerium.at/siteEN 2) for residential and nursing homes was introduced in Austria which aims to provide an objective measure of the quality of care provided by residential and nursing homes. The certificate should promote systematic efforts - above and beyond the fulfilment of legal provisions - to improve the quality of life and care of their residents. Another step towards more integrated care made in 2012, when the Ministry of Labour, Social Affairs and Consumer Protection implemented a universal long-term care allowance program, which subsidize long-term care services for dependent people on a nationwide level (Trukeschitz & Schneider, 2012).
In relation to coordination and integration, no progress has been made, for instance it is still not possible (and even prohibited in some regions) to provide community care services in residential settings, with the exception of some regions where ‘service housing’ has been established. Vice versa, it is also not possible for staff in care homes to provide community care. An exceptional measure to increase integration of social and care services was implemented in two regions (Upper Austria and Styria) where the public administration defined operational districts, each of which was then allocated to a single provider organization. No evaluation has yet been presented to show whether this intervention, on the detriment of consumer choice, has really resulted in the expected increase of cost-effectiveness in home care.
1. INTRODUCTION
1 Last access 28.06.2018, 2 Last access 28.06.2018

7
TABLE OF CONTENTS
Hospice and palliative care are one of the most active and reform-oriented areas in health and long-term care in Austria (e.g. Lynch, Connor, & Clark, 2013). Driven by a dedicated ‘Hospice Association’, important steps to raise awareness for end-of-life care and to establish concepts of palliative care across health and long-term care provision have been made, for example by projects such as ‘Palliative Care in Care Homes’ (e.g. Pelttari & Pissarek, 2013) and the further extension of ‘Mobile Palliative Care Teams’. Indeed, the concepts of palliative care (multi-disciplinary teams, patient-oriented, comprehensive approach) have a potential to serve as a general model for person-centered care, but their integration in mainstream provision of long term care remains to be seen.
1.2 The SUSTAIN project
SUSTAIN, which stands for ‘Sustainable Tailored Integrated Care for Older People in Europe’ (www.sustain-eu.org), is a four-year (2015-2019) cross-European research project initiated to take a step forward in the development of integrated care. SUSTAIN’s objectives were twofold: 1. to support and monitor improvements to established integrated care initiatives for older people living at home with multiple health and social care needs, and in so doing move towards more person-centred, prevention-oriented, safe and efficient care; and 2. to contribute to the adoption and application of these improvements to other health and social care systems, and regions in Europe.
The SUSTAIN-project is carried out by thirteen partners from eight European countries: Austria, Belgium, Estonia, Germany, Norway, Spain, the Netherlands, and the United Kingdom. With the exception of Belgium, in all other countries two integrated care initiatives per country were invited to participate in the SUSTAIN-project. The initiatives were already operating within their local health and social care systems. Criteria for including these initiatives, also referred to as ‘sites’, were defined by SUSTAIN research partners and drawn from the principles of the Chronic Care Model and related models (Epping-Jordan, 2004; Minkman, 2012; Wagner et al., 2005) Accordingly, initiatives should:
• Be willing and committed to improve their current practice by working towards more person-centred, prevention-oriented, safe and efficient care, which, in line with the European Commission’s stipulations, are SUSTAIN’s four key domains.
• Focus on people aged 65 years and older, who live in their own homes and who have multiple health and social care needs.
• Support people to stay in their own homes (or local environments) for as long as possible.
• Address older people’s multiple needs, in other words, they should not be single disease oriented.
• Involve professionals from multiple health and social care disciplines working in multidisciplinary teams (e.g. nurses, social workers, pharmacists, dieticians, general practitioners).
• Be established, i.e. preferably operational for at least two years.
• Cover one geographical area or local site. • Be mandated by one organisation that represents the
initiative and that facilitates collaboration with SUSTAIN research partners.
The fourteen initiatives selected according to these criteria showed great diversity in the type of care services provided (Arrue et al., 2016; De Bruin et al., 2018). Their focus ranged from proactive primary care for frail older people and care for older people being discharged from hospital, to nursing care for frail older people, care for people with dementia, and palliative care.
In the SUSTAIN-project, we adopted an implementation science approach using the Evidence Integrated Triangle(Glasgow, Green, Taylor, & Stange, 2012), in which local stakeholders and research partners co-design and implement improvement plans. In the first phase of the project (starting autumn 2015), SUSTAIN-partners established working relationships with the different sites, and identified relevant local stakeholders related to the initiative (i.e. managers, health and social care professionals, representatives of older people and informal carers, local policy officers). Furthermore, they carried out baseline assessments of each initiative’s principal characteristics and also worked with local stakeholders to identify areas of current practice in the initiative, which might be subject to improvement (e.g. collaboration between formal and informal care providers, involvement of older people in care processes). Findings from the baseline assessments were used as inputs for workshops with key stakeholders related to the initiative at each site. The purpose of the workshops was to discuss outcomes of the baseline assessments and enable sites to determine local improvement priorities.
In the second phase of the project (starting spring 2016), local steering groups were set up. Steering groups consisted of stakeholders who participated in the workshops together with additional local stakeholders considered relevant to the initiative. These steering groups were created to design and implement improvement plans, that is, sets of improvements that apply to local, site-specific priorities. Each steering group agreed to implement their plans over the 18-month period from autumn 2016 to spring 2018. In each initiative, implementation progress and outcomes were monitored by SUSTAIN partners using a multiple embedded case study design, in which each initiative was treated as one case study (Yin, 2014). A hallmark of case study design is the use of several data sources, a strategy which also enhances data credibility (Creswell, 2009). SUSTAIN partners therefore used a set of qualitative and quantitative data collection tools (see Appendix 10.1), allowing us to collect data from different data sources, being: surveys to users, surveys to professionals, interviews with users and carers, professionals and managers, care plans/clinical notes, field notes, notes of steering group meetings, and templates to collect efficiency data from local services, organisations or registries. Data were collected at agreed

8
TABLE OF CONTENTS
and specified times during the 18-month implementation period, using the same procedures and tools for all initiatives. In addition to a core set of data collection tools applied in all initiatives, sites were being encouraged to select site-specific tools tailored to their site-specific context and improvement priorities.
Data were analysed per site, guided by the principles of case study design. There were three steps in our analyses: 1. all data sources were analysed separately using uniform templates for analysis which were generated through a discussion among research partners; 2. for each data source, data were reduced to a series of thematic statements (qualitative data) or summaries (quantitative data); 3. an overarching site-specific analysis was done, in which all qualitative and quantitative data were coupled and underwent a process of pattern-matching across the data. This is the approach of choice for evaluating complex community-based interventions which are context bound and noted for their differences in application and implementation (Billings & Leichsenring, 2014; Craig et al., 2008). In order to be able to do a site-specific overarching analysis, we created an analysis framework which was used by all SUSTAIN partners in order to create uniformity of approach. Data were analysed against the propositions and analytical questions presented in Table 1.
1.3 SUSTAIN sites in AUSTRIA
The two Austrian sites were chosen because they represent examples of innovative practice and characteristic features of the Austrian context for integrated care.
The first site, called “Coordinated Palliative Care Styria” (CPC) in Graz is specialised in a defined area of care at the interface between health and social care, namely end-of-life care. Originating from specific needs of cancer patients
in clinical care, the concept of palliative care has been further developed towards interventions between inpatient and outpatient care, in particular by the establishment of ‘mobile palliative care teams’ that are able to work in clinical and residential settings as well as in the community (i.e. patients’ homes, addressing both the needs of patients at the end of life and their families). With observed changes in health care needs of older people, the model has moved towards serving older people with chronic conditions and multi-morbidity.
The second site, the “Gerontopsychiatric Centre” (GPZ) in Vienna is a unique centre for community-based geronto-psychiatric consultancy (clinical-psychiatry and neurology) and serves as a service centre for patients, their families (carers) and for other stakeholders in health and social care (hospital wards, GPs, health and social care services and facilities). The small multi-professional team running the GPZ in Vienna is thus networking with a wide range of stakeholders to address the needs of older people suffering from cognitive decline, related morbidities and social problems.
1.4 Reader’s guide
The outline of the report is divided in two parts, each presenting one of the two Austrian sites of integrated care. Chapter 2 features characteristics of the Gerontopsychiatric Centre (GPZ) and describes the appendant improvement initiative, its rationale and aims. Findings of the improvement project are presented in chapter 3 and main lessons learned from the improvement initiative of the GPZ are featured in chapter 4.
The Coordinated Palliative Care Styria (CPC) is presented in part two, starting with a site description, and detailed information about the developed initiative in chapter 5.
Table 1 - Propositions and analytical questions against which SUSTAIN data were analysed.
Proposition 1 Integrated care activities will maintain or enhance person-centredness, prevention orientation, safety, efficiency and co-ordination in care delivery.
Proposition 2 Explanations for succeeding in improving existing integrated care initiatives will be identified.
Analytical question 1 What seems to work, in what kind of situation, and with what outcomes when making improvements to integrated care?
Analytical question 2 What are the explanations for succeeding and improving integrated care initiatives?
Analytical question 3 What are the explanations for not succeeding and improving integrated care initiatives?
Analytical question 4 Are there any factors that are particularly strong in the analysis that could be seen as having an impact on integrated care improvements?
Analytical question 5 What factors can be identified in the analysis that could apply to integrated care improvements across the EU, and be transferable?

9
TABLE OF CONTENTS
Since the site did not continue its improvement initiative throughout the whole project phase of SUSTAIN, we conducted a further analysis on barriers and facilitators of integrated care which are described in chapter 6. Chapter 7 summarizes the main lessons learned from the CPC-initiative.
The last chapter (chapter 8) gives an overall national reflection on the sites findings and implications for integrated care in Austria and finally, provide recommendation for policy maker and service provider which closes the final chapter of the national SUSTAIN report.

TABLE OF CONTENTS
PART 1 Gerontopsychiatric Centre (GPZ)

11
TABLE OF CONTENTS
2.1 General description of the site
The basic mission of the GPZ is the support and adequate treatment of older people and their families living at home and suffering from psychiatric problems in most cases cognitive disorders. It is a unique centre for community-based geronto-psychiatric consultancy (clinical-psychiatry and neurology), offering a wide range of information and links to related services for older people and their families. It also includes a ‘Memory Clinic’ and offers counseling (by phone and face-to-face) to GPs, health and social care services and family carers.
The GPZ is affiliated to the ‘Psycho-Social Services’ in Vienna that are run and financed by the municipality of Vienna. After identifying substantial lack of geronto-psychiatric competencies and related services for home dwelling older people in the city of Vienna, the Gerontopsychiatric Centre was founded in 2001. In most cases up to that point, formal and informal care people were seeking support directly at the ‘Psycho-Social Services’ (PSD) that had, however, not been specialized in such cases.
Nowadays the multi-disciplinary team of the GPZ consists of psychiatrists, psychologists, nurses and a social worker. All services are free of charge for the older people. The integrated team is collaborating with a wide range of stakeholders in the health and social care sector including `Fonds Soziales Wien’, which purchases social services for the city of Vienna, all providers of home care, Alzheimer Austria, providers of adult day service, GP’s and specialized doctors.
Funding for GPZ is solely provided by the city of Vienna and not financially supported by the health insurance. If older people need more complex clinical assessments (e.g. magnetic resonance tomography – MRT) that go beyond the capacities of the GPZ (e.g. technical resources), the GPZ collaborates with specialized health
care organizations e.g. hospital units specialized in geriatric psychiatry. These expenditures are however, covered by the health insurance.
2.2 Rationale for improvement project
The GPZ provides dementia care through a multi-professional team and provides already comprehensive and integrated care service on a high level (Psota & Sepandj, 2003). Users as well as collaborating partners of the GPZ that were involved in developing the SUSTAIN project in Austria generally expressed high satisfaction concerning the kind and quality of services provided by the GPZ. However, many ways of working and of integrating these services in the regional health and care system are based on quite informal relationships and vague personal agreements.
The GPZ is a specific example of integrated and coordinated care in a context of rather weakly developed mechanisms for cooperation and coordination between sectors and organizations. With regard to the team, collaboration around the needs of older people has become a daily routine. However, bottlenecks and shortcomings were identified when it comes to trans- and cross-organizational collaboration, in particular with the hospital sector. The lack of time and opportunities for communication, information exchange and procedural agreements, which is also due to restricted personnel resources, were identified as key barriers and thus as a starting-point for improvements.
2. GERONTOPSYCHIATRIC CENTRE (GPZ): CHARACTERISTICS AND IMPROVEMENT PROJECT

12
TABLE OF CONTENTS
Moreover, dementia care is a topical subject and highly relevant for the hospital sector. Older people living with dementia are more frequently admitted to general hospitals than those without dementia, due to their greater risk of physical and mental comorbidity, poorer nutritional status and difficulties managing medication and seeking timely medical care (Shenkin, Russ, Ryan, & MacLullich, 2013). However, a hospital stay can worsen the symptoms of dementia and the (early) use of community-based services is not only more cost effective than hospital care but is also considered to delay institutionalization (Gaugler, Kane, Kane, & Newcomer, 2005; Schwarzkopf, Menn, Leidl, Graessel, & Holle, 2013). In many cases, individuals living with dementia remain undetected throughout their hospital stay because they are admitted due to other clinical reasons and have not been diagnosed so far (e.g. Joray, Wietlisbach, & Büla, 2004; McLean, 1987).
To be transferred from the familiar surrounding at home to a hospital can be a difficult experience not only for older people with dementia but also for their families, who sometimes eyewitness a major change in the behavior of their loved ones, as emphasized by professionals of the hospital. A change of scenery increases the risk for delirium and promotes disruptive behavior which is also considered as challenging by the hospital staff, especially if they are neither specialized in geriatric- nor psychiatric care. Specific knowledge and training is needed in the opinion of the steering group to provide safe and preventive dementia care in the hospital and to support family carers.
2.3 Aims and objectives of the improvement project
In many cases, dementia is diagnosed late which limits the opportunities for older people to decide on their care and treatment at an early stage (Sommerlad et al., 2018) A timely diagnosis is key for a good chance to live at home independently as long as possible. A hospital admission – for whatever reason – provides the opportunity to identify a cognitive disorder in an early stage and to give access to adequate integrated care. However, this requires well-trained staff and clearly defined operational procedures.
Taking the rationale into account, the improvement project pursues three main objectives:
1. to improve the identification of older people living dementia in its early stages and give them and their families access to community-based integrated care (provided by the GPZ).
2. to raise the awareness, -the knowledge and - skills of hospital staff regarding older people with dementia.
3. to establish a sustainable link between hospitals and the integrated care centre GPZ (e.g. enhance collaboration, share medical records)
2.4 Explanation of the improvement project
Two Viennese hospitals Krankenhaus Hietzing (KHH) and Sozialmedizinisches Zentrum Ost – Donauspital (SMZ) as well as the integrated care centre GPZ operationalised the project in a one year implementation period. At hospital SMZ the medical and nursing staff of seven units specialized in internal medicine, cardiology and angiology as well as the casualty department participated in SUSTAIN. Hospital Hietzing (KHH) joined SUSTAIN in March 2017 with one ward specialized in gastroenterology and hepatology. A thematic priority of this specific hospital ward is the management of delirium. Delirium occurs more commonly in older people who are older and have a previously compromised mental status – which is why KHH engaged in SUSTAIN. Each involved health care organization nominated at least 2 representatives who managed the improvement project within their respective organization. Together with ÖPIA, all representatives formed the steering group which managed and coordinated the improvement project.
The GPZ held inter-professional training sessions at the respective hospitals in order to raise the awareness and skills of hospital staff. Particularly the training sessions should enable staff members to identify older people living with dementia at an early stage. Moreover, further education should improve their communication skills in regard of people living with dementia and raise the awareness of medication interaction as well as comorbidities. Further, the GPZ introduced the short screening test Mini-Cog (Kamenski et al., 2009) as a valid and efficient screening instrument that also takes limited time recourses of nurses and physicians into account.
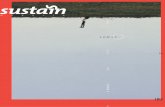
Figure 1 provides an overview on the project procedures. Individuals enter the project when they are identified of being affected by dementia through the Mini-Cog in the hospital, which is conducted by the nursing staff. Next, a physician informs the person about the suspected mental condition and advices the identifies person to use the services of the GPZ. Further, the physician requests consent to inform the family carer and asks permission to share the medical record with the integrated care centre. Only people who signed the consent form were included in the study whereby affected individuals who were not able to give consent were also informed about the screening result and could use the services of the GPZ free of charge. Additionally, both, the identified person and their carer receive an information leaflet describing the services of the GPZ as well as a letter of recommendation at discharge.
After discharge from the hospital the identified people or their caregiver contact the integrated care centre in order to schedule an appointment. Older people, who follow the recommendation, receive care and treatment from a multidisciplinary team. Service users of the integrated care centre are thoroughly examined and diagnosed by the multidisciplinary team to achieve the longest possible life in their familiar surroundings of their own homes. Optional, the GPZ visits the individuals at home to facilitate access

13
TABLE OF CONTENTS
to adequate services. Depending on the people’ needs and background, the GPZ gives advice on organizing home assistance, visiting services and placements in geriatric day centers and day clinics. Family carers receive advice for relieving their burden and obtain information about dementia as a disease. Furthermore, the GPZ shares - with informed consent - the medical record with health care professionals/organizations which are involved in the service users’ care (e.g. GP, formal carer). For further, more complex examination (e.g. magnetic resonance tomography-MRT) the GPZ cooperates with the geronto-psychiatric wards of the hospitals which receive the medical record of the client as well. According to the clients’ needs and health status, further appointments were scheduled with the GPZ.

14
TABLE OF CONTENTS
Figure 1 - Flowchart of the Austrian improvement project ODIWA (Optimization of dementia diagnostics, integrated medical
follow up and awareness).
Flowchart of ODIWA (Optimization of dementia diagnostics, integrated medical follow up and awareness)
Continuing inter-professional training sessions for hospital staff
• (early) Signs of dementia,• Short screening ‘Mini-Cog’• Communication skills regarding older people living with dementia• Comorbidities and medication interaction
Hosital--> First encounter with potential candidates within the
improvement project
• Older people are informed about their suspected condition and referred to the Gerontopsychiatric Centre
• Older people give informed consent to share their medical record with the Gerontopsychiatric Centre and agree to inform their informal carer about the suspected condition
• Informal carer and informed about the suspected condition (e.g. at discharge)
• The medical record is shared with the Gerontopsychiatric Centre by mail
Gerontopsychiatric Centre--> 1st visit of participants within the improvement project
• Multi professional team including psychiatrists, psychologists, social workers, neurologists, nurses• Thorough anamnesis, diagnosis and multi-professional treatment• Home visits or ambulatory treatment• Coordination of care (home care service and informal care)• Counselling for relatives, friends and carers• Collaboration with various health/social services as well as the GP• The medical records are shared with the hospital if service users are in need of further examination
(e.g. MRT), GP and (in-)formal carers are informed about the further care
Gerontopsychiatric Centre--> 2st / 3rd visit of participants within the improvement project
• at least 2 obligatory visits (first visis, visit after on year). Number of visits depend on the service users’ needs
GerontopsychiatricUnit
• Complex cases can be sent back for futher examination (e.g.:MRT...)
Criticalpathway
Pathway of participants
ca. 1 month
max. 12 weeks
at home
at home
doesn’t follow the recommmendation
SUSTAIN evaluationFollow-up survey
SUSTAIN evaluationQuestionnaires,
Interviews
General Practitioner
Social Services
Ongoing

TABLE OF CONTENTS

16
TABLE OF CONTENTS
3.1 Introduction
Besides supporting health care organizations to improve integrated care for older people, SUSTAIN aims to ensure that improvements to integrated care initiatives are applicable to other health systems and regions in Europe. Therefore, researchers monitored the implementation of the SUSTAIN projects for a one year period and tried to identify barriers and success factors for establishing integrated care initiatives. Further, researchers tried to explore what kind of improvements maintain or improve person-centeredness, prevention-orientation, safety, efficiency and co-ordination in care delivery. Outcomes of the Viennese improvement project in the context of SUSTAIN core domains are described in the following chapters.
After developing the improvement project described in the previous chapter, the actual implementation took place in Vienna from May 2017 until April 2018. During this time, SUSTAIN researchers collected data in order to monitor and evaluate progress and outcomes of the improvement project. Table 2 provides an overview of the quantity of data collected per data source. More information about the different types of data collected can be found in Appendix 10.1.
Within the Austrian improvement project (see figure 1) we additionally interviewed older people and their family carers at two critical points in time. Firstly, at home after their hospital stay when participants consider whether they want to use the services of the GPZ or not. And secondly, after participants received care provided by the Gerontopsychiatric Centre (GPZ). Thereby, we aimed to explore the reasons why older people did or did not use the integrated care service of the GPZ after their hospital stay.
3.2 What seems to work?
Characteristics of people using or refusing the initiative Overall, the hospital staff identified 39 older people suspected of suffering from dementia4. The age ranged from 65 to 93 years with a mean age of 79.5 (SD= 7.9). All participants were living with at least one other medical condition and most of them were to some extent care-dependent. Twenty-two percent of the identified people followed the recommendation and used the services of the GPZ, eleven percent deceased or were transferred to a nursing home and twenty-two percent were not available (e.g. due to wrong contact details). However, the majority (38%) refused the hospitals advice and declined the integrated care offer (see Table 3).
Reasons for not using further dementia care varied among the respondents (see Table 4). Involvement of family carers and the quality of how professionals informed identified people about the positive screening result (e.g. time, involvement of carers) were considered as key factor regarding the usage of the integrated care centre. Older people without any informal carer did not visit the GPZ at all. Neither of them remembered the recommendation and some were severely affected and therefore could not arrange further care on their own. Family carers and older people who were well aware of the recommendation mostly refused further care because they mistrusted the screening result.
“ Who do they think they are? They don’t know me at all! I’m certainly not crazy! No, I’m sure the test failed and I remember having a bad day too. No wonder, after surgery…. Everybody would have failed that screening (…) Yes, it’s a good thing that the hospital cares about dementia too. Our health system is an achievement. But that centre is not for me since I’m not suffering [from dementia], you know?!” (Participant 16, who did not follow the recommendation)
3. FINDINGS OF THE IMPROVEMENT INITIATIVE IN GERONTOPSYCHIATRIC CENTRE
4 More than 39 older people were identified by the staff however refused to participate in the study. Furthermore, older people who were not able to sign the consent form due to their mental condition or were directly transferred from the hospital to a nursing home were excluded from the study.

17
TABLE OF CONTENTS
Table 2 - Quantity of data collected per data source.
Data source(Professionals & managers)
NData source(Service users & informal carers)
N
Team Climate Inventory (TCI) Baseline 7Follow-up 8
Interviews users and carers Overall: 39 interviews with
project participants Participants, who used
the integrated care service:8 users;3 carers
Interviews managers 2Person-centered coordinated care questionnaire (P3CEQ)
8 users
Focus group professionals3; with 2 to
3 participantsClient report (Careplan) 8 users
Minutes of meetings and inter-professional-training sessions
7 Meetings; 2 inter-professional-
training sessions
Field notes3 1 document with notes taken
during phase 1 and 2 of SUSTAIN; 1 Document
containing Email traffic
3 Collected since Oct. 2016 – April 2018
Table 3 - Patient pathways after the hospital stay.
Table 4 - Characteristics of people (not) using the Gerontopsychiatric Centre.
Used GPZ DeceasedTransferred to nursing Home
Refused Further Care
Not Available
Percentage 22% 11% 11% 38% 22%
Total number 8 4 4 14 8
Other identified people were not able to follow the hospitals advice because they were already readmitted to the hospital or still recovered from their initial stay. However, all participants highly appreciated the interconnected care between the hospital and the integrated care centre. People who used the service of the GPZ could be characterized as highly interested in
health care in general, well aware of their health status and accompanied by a caring family member or friend. Once again, the quality of informing the person about dementia played a pivotal role in the usage of further dementia care. The more time professionals spent with informing identified individuals and their family carers about dementia the more likely they followed the hospitals advice.
Older people who refused further care (38%) Older people who used the services of the GPZ (22%)
• Denial/mistrust regarding the screening test Mini-Cog• Recovery or readmission to the hospital• Absence of an informal carer• Severely affected: was not able to either comprehend the
recommendation nor organize further care arrangements• Low quality of informing the person about dementia
(time spent, involvement of informal carers)
• Presence of family member• Health-conscious users & carers• Highly interested in healthcare• High quality of informing the person about dementia
(time spent, informal carer present)

18
TABLE OF CONTENTS
SUSTAIN core domainsBefore SUSTAIN, the GPZ already provided comprehensive and integrated dementia care on a high level (Psota & Sepandj, 2003; see also Arrue et al., 2016). New however, was the interconnected care approach between the hospital sector and the community based integrated care centre GPZ, assuming that access to high quality care and collaboration between healthcare sectors foster a person-centred, prevention-oriented, safe and efficient care delivery.
Person-centerednessOlder people and their carers who followed the hospital’s recommendation perceived care provided by the GPZ as person-centered as indicated in the interviews and underlined with an average P3CEQ-score in the upper third (mean= 21.39; SD= 3.94). In the opinion of older people and their carers who used the service of the GPZ, a specific strength of the experienced care was the thorough needs assessment and excellent counselling by the multidisciplinary team. In the users and carers view, the person itself was the centre of attention rather than the disease. Consequently, they felt well treated and involved in their care. “ They [GPZ] were nice. I could talk with them and they listened
(…) They took the assessment really seriously. Wrote everything down on a piece of paper, which was too small. He (GPZ staff) had to continue at the backside of the paper. (…) Yes, I think they know everything about me now. Except that I was bitten by a dog when I was 9 years old.” (User 7)
Furthermore, the inter-professional training sessions fostered a more person-centered care approach as stated by the hospital staff. The professionals appreciated the opportunity of further education and all involved healthcare organizations considered them as a success. In the nursing- and medical staffs’ opinion, the training fostered a more attentive and sensitive care. The staff indicated to be more aware of signs of dementia even if people are in an early stage of the disease which led in their opinion to a more person-centered care. Findings from interviews with older people confirm these statements. However, only people who used the service of the GPZ described the hospital staff as friendly, competent and attentive. The other respondents expressed neutral feelings towards the hospitals’ care.
“ The lectures were the centerpiece. (…) We are much more attentive now than before. Not only the nurses are more sensitive with respect to these early signs but our physicians too. How should I put it…Yes, now, we don’t pass by if something seems strange, we look twice.” (Professional 3)
Prevention-orientationProfessionals of the GPZ as well as service users and their carers stated that an early diagnosis and access to integrated dementia care are closely linked to prevention-oriented care. Despite the consistent positive appraisal in terms of the dementia trainings, only half of the wards (4 out of 8 wards) administered the Mini-Cog on a regular basis and referred people continuously to the integrated care centre. Furthermore, the wards remarkably varied in
the number of referred people, which ranged from 0 to 27, indicating that prevention-orientation was maintained but not improved in all hospital wards.
Service users of the GPZ and their carers were glad to be informed about the diagnosis and to receive immediate treatment and care. In particular, younger people and their carers (under 80 years) indicated that an early diagnosis and treatment empowers those affected to live as long as possible a life they feel worth living. For instance, maintaining their cognitive abilities was associated with living at home for as long as possible and with the ability to participate in social activities with their family members. In their perspective, the integrated care centre supported them to maintain or even raise their quality of life despite the dementia diagnosis.
“ Considering [name of the service user] dementia stage, we are glad to be informed now. Now is better than later when there is nothing you can do, except watch him getting worse. If we are lucky he will still be with us [family] for a long time and join family celebrations or little trips with full consciousness.” (Carer 2)
However, some respondents expressed the opinion that the diagnosis came too late for them and that there is nothing to improve their situation. Most of them were above the age of 80 years and live with functional impairments or other severe diseases (e.g. Parkinson's disease, impaired mobility). Some professionals raised the question if the inter-professional-training sessions were sufficient in order to detect older people at an early stage of dementia since the staff mainly identified people at an advanced stage of dementia (but without pre-existing diagnosis).
“ If I had been younger maybe they [GPZ] would have helped me. But look at me. I’m old and sick... Parkinson [Parkinson’s disease] and bound to a wheel chair with that thing (point at the bladder bag). It is too late. I just want to have my peace and enjoy the little things.” (User 4)
SafetyThe treatment and care of the GPZ were considered from various angles and multidisciplinary perspectives, which is why participants felt safe and well cared for. Most of the participants indicated that a change in their medication helped to improve their well-being. Reviewing the number of medications, medication adherence and addressing medication interaction in regard of older people living with dementia were also associated as key factors by professionals of the GPZ when it comes to delivering safe care. The number and proper use of medication are considered as important health concerns among community-dwelling older people, especially those with dementia, because of their increased potential for medication error, sensitivity to drug effects, and significant risk for nursing home placement (e.g. Lau, Mercaldo, Shega, Rademaker, & Weintraub, 2011). “ Yes. Now I can follow conversations. Before [Care from the
GPZ] I was so tired. Yes, really, really tired. But now I know the pills were to blame.” (User 5)

19
TABLE OF CONTENTS
Sustainability and coordination A sustainable link was established between two wards and the GPZ, one in each participating hospital. These wards integrated the initiative in their daily routines and referred people regularly to the integrated care centre. Moreover, they will engage in further dementia programs in the near future or already established inter-professional case conferences targeting people suffering from mental health conditions like delirium, dementia or depression. However, the cooperation between the remaining wards and the GPZ was not strengthened. Furthermore, the exchange of medical records could not be maintained because no reasonable solution in regard to electronic data transfer was found.
“ Yes, I think committed wards will continue the collaboration and keep testing patients [suspected of dementia]. I agree with my colleague that our care is now more connected or, like you [interviewer] call it, is more integrated than before. Especially, since we haven’t known the GPZ at all before. We got to know them through the project.” (Physician 1)
Findings from the interviews and the Team-Climate-Inventory (TCI) show some variability in the perception of project success depending on the point of views and expectations of the involved organizations. The main success criterion for GPZ representatives was the number of referred people, which was smaller than expected. As a result, the efficiency of the initiative was questioned. Further, the professionals indicated that older people without caregivers cannot take advantage of the initiative since they are not able to arrange further care on their own and consequently are not able to follow the care recommendation made by the hospital staff. These people however are the ones who needed further care at the very most and would benefit from the project. To involve social service providers was considered as possible solution in order to overcome a systematic bias.
“ The training sessions yes [were successful], but apart from that... to refer patients to the GPZ failed. The patient numbers are just too small to speak of an effective collaboration.” (Manager GPZ)
In contrast, hospital representatives regarded the establishment of a formal contact to the GPZ as a benefit in itself and highly valued the advanced training and possibility to refer cases of suspected dementia- regardless of the actual number of eventually referred people. These findings are reflected in the TCI score (ranging from 1 to 5 with larger values indicating better perceived team climate) with an average score of 4.6 (SD=0.6) for hospital representatives and 3.0 (SD=0.6) for representatives of the GPZ. Beside some increase of inter-organizational collaboration, some wards emphasized positive effects on information exchange within and across hospital units. Both hospitals for example collaborated with hospital intern geronto-psychiatric specialists in the care due to the project.
“ The team climate was already good. But still, I think we talk more with each other… More about the patient care. At the beginning of the project for instance, we practiced the “Uhren-Dreier” [Mini-Cog] together. We also discussed what wording fits best when it comes to inform difficult patients about dementia…. And I think it motivated the staff too - to have a common new mission.” (Nurse 3)
3.3 What are explanations for succeeding and improving integrated care initiatives?
The aim of ODIWA is to counter the considerable rate of under-diagnosed cases of dementia among older people, to raise the awareness among professionals and to foster a more integrated provision of care to older people and their relatives. Findings show that some wards implemented the project successfully and reached the project objectives which also resulted in maintaining or improving the SUSTAIN core domains (i.e. person-centeredness, prevention-orientation, safety, efficiency and interconnected care delivery). Other wards however, struggled with the integration of the initiative in their daily routines despite the willingness and motivation to participate in SUSTAIN. This raises the question why some wards struggled with implementing the project and others succeeded. We identified four main drivers which facilitated the project implementation (see Table 5).
Involvement of family carers was considered as key factor regarding the usage of the integrated care centre. Wards, which emphasized informing both identified people and their family report higher numbers of people who followed the hospital’s advice and used the service of the GPZ. In most cases, family carers managed further care arrangements since most of the older people were multi-morbid and dependent on care to some extent, in particular after their hospital stay.
Furthermore, available personnel resources and prior knowledge facilitated the project implementation. For instance, wards which indicated to have sufficient resources involved more likely family carers and spend more time with informing older people about their screening result. One hospital had prior experience and knowledge through a previously completed project on delirium management.
Table 5 - Drivers for Succeeding and improving integrated care.
Drivers for succeeding and improving integrated care
• Involvement of family carers• Availability of personnel resources and prior knowledge• Personal values, attitudes (Champions)• Flat steering arrangements• Internal collaboration

20
TABLE OF CONTENTS
They indicated that the prior experience facilitated the project implementation since they were already familiar with various concepts of delirium which resemble dementia care (e.g. communication). Since symptoms of delirium in older people are often mistaken for dementia (Fick, Steis, Waller, & Inouye, 2013) the staff was already trained and observant regarding disease related behaviors and new knowledge – attained within the inter-professional-training sessions - were easily integrated in their daily working routines. “ I think our previous work on delirium was a great
advantage. We already discussed how to communicate best with the patients and know, how important the involvement of family carers is. You can say, we embedded the project in a well-established structure that was already in place.” (Nurse 4)
Furthermore, some wards received support from a mental health nurse, specially trained in psychiatric diseases, who held case conferences and helped them to screen individuals suspected of having dementia. The opportunity to ask questions and talk with a specialized nurse about dementia related challenges in care was perceived as great relief by the staff. Particularly in the beginning of the project care-related questions arose frequently and some of the hospital staff indicated that it was easier to ask the mental nurse for help than call professionals from the GPZ since they did not want to ‘burden’ professionals of the GPZ with their questions. That changed over time since the involved professionals learned to know each other better, as stated by the hospital manager. “ At the beginning, we had some questions about the analysis
of the Uhren-Dreier [Mini-Cog]. […] We had to become more familiar with it [Analysis of the Mini-Cog] and I have to admit… including my person… I wasn’t sure if I can call [Name of the professional of the GPZ] and bother him with our questions. But now I know that I can turn to him and that he even appreciates questions. So that changed over time.” (Nurse 3)
Other wards which also tested and referred people to the GPZ on a regular basis assigned project-related tasks to single staff members who became responsible for implementing the initiative. The staff emphasized that this was only possible because of available (additional) personnel recourses. Appointing a single person in charge led to a transparent project structure (other staff members knew to whom they can turn to), a feeling of ownership and responsibility as well as to flat steering arrangements associated with short communication lines and the ability to respond quickly to changes regarding the project implementation. However, exclusively relying on single people is risky since the project may stumble or discontinue when they are no longer available (e.g. maternity leave). “ In my opinion, we were successful a) because a permanent
physician is assigned to my unit which is not the case for other wards. And b) I had two pregnant nurses whose main duty was ODIWA [name of the project]. One of them had a relative who is also suffering from dementia, so she was already in favor of the project.” (Nurse 2)
Some wards implemented the project even in situations when time and personnel resources were limited (e.g. flu epidemic, short staffed, internal audit). These wards perceived dementia care as meaningful and a personal matter. Further, they indicated that the objectives are relevant for their daily work e.g. facilitate their working routines, increased their expertise or helped them to cope with difficult situations. These traits were in particular found in Champions. When interview partners were asked about people who played a pivotal role in regard of implementing the initiative, they spoke of single individuals – Champions – who influenced and facilitated change in others through demonstrating commitment, promoting innovation with passion and persistence, bring together groups of different professions and develop informal networks of support.
“ We really want to help patients and their families. During my work, I see how hard it is for family members when their loved ones can’t remember them anymore or seem scared and dismissive – due to a delirium for example. That really moves my heart and I realize, if there is no place they can turn to, we [the hospital department] have to take health care in our own hands- And this is the reason why we are obligated to continue the work [regarding the project] regardless of circumstances [limited resources].” (Hospital Manager 2)
Besides personal attitudes and values, referral of positive screened older people was particularly efficient if nursing- and medical staff worked well together, trusted each other and cooperated on equal level. In one hospital for instance nurses as well as physicians informed individuals affected by dementia and their family carers on dementia which was perceived as more efficient by the hospital staff. Furthermore, good inter-personal relationships were associated with overcoming difficulties regarding the project more easily.
“ We (chief nurse and chief physician) are working really well together that’s why everything ran very smoothly. Our communication is good, we trust each other and come fast to decisions. That’s why it was easy for you [interviewer] to work with us.” (Physician 1)
3.4 What are explanations for not succeeding and improving integrated care initiatives?
Findings suggest four interrelated barriers with respect to succeeding and improving integrated care in regard of the Viennese improvement project (see table 6).
Staff members indicated that severe time constraints and a lack of personnel resources hindered the project implementation. Project-related tasks were merely performed on a voluntary basis and had (due to limited time and no additional resources) low priority compared

21
TABLE OF CONTENTS
to regular care and medical treatment. Moreover, the medical staff emphasized that their main task is medical treatment according to their area of expertise and that their duties issued by the hospital management do not cover (integrated) dementia care.
“ We are an acute hospital. Our main duty is saving lives. That is not my personal interpretation but the hospitals remit within our health care system. However, dementia is not a life-threatening disease. Don’t get me wrong. We are well aware of the demographic change and notice a shift in the total numbers of older patients with geriatric care needs. I personally think the project goals are highly relevant and of importance. But up to date, I haven’t seen a hospital policy on dementia care. So I have to put my duties first. The project is of less priority.” (Physician 3)
To inform identified people and their family carers about dementia requires approximately 40 minutes. Due to time constraints, patient communication was frequently scheduled according to the physicians’ work plan and was therefore often performed without attendance of family carers. They, however, play a pivotal role in managing further care since family members are mostly in charge of arranging the care appointments (see 3.2). On the one hand professionals indicated that a lack of time and staff prevented a successful project implementation because they had to put their official duties (given by the hospital management) first. On the other hand, some professionals argued that resources were not a barrier for integrated care but a missing hospital policy - in a sense of official responsibility e.g. enclosed in the job specification of professionals - was. Some professionals even thought that resources would not have been an issue at all if the hospital management would have officially committed itself to the initiative (e.g. acknowledged as duty).
“ No, resources were not an issue at all. I think this is kind of an excuse. Or not excuse. This is not the right word because I think everyone [means hospital staff] was – and still is- in favor for the project objectives. Maybe it is more a symptom. Yes, it is a symptom of the real problem. I think if a hospital is 100% committed to implement an initiative, barriers are no longer an issue. Time and personnel will automatically follow because if the objectives are written down in our job specification we are obligated to follow up on them. The same applies for the hospital management. If they want to implement the initiative they are responsible for providing the resources.” (Nurse 5)
Rotating staff and changes within the steering group
also hindered the project implementation. Some wards were characterized by a permanent nursing staff but chief physicians rotated over time (several times per month). This led to a lack of project ownership within the medical staff since they were not able to become familiar with the project itself and its related procedures (e.g. informing positive screened older people about dementia). As a result of, they were less engaged in the initiative and prioritized their usual duties.
“ Yes, my ward has no permanent chief physician. They rotate frequently. At peak periods, I have 5 physicians per month. That is not always the case but just to give you a picture of my situation. I can’t blame them. They are not familiar with SUSTAIN and it takes time to explain each physician what the project is and what they have to do. So they do not feel responsible since they leave after a short period. It is just too short to develop a sense of ownership” (Nurse 5)
Furthermore, the SUSTAIN project aimed to design the improvement projects in close collaboration with the sites and their respective partner organizations (i.e. policymakers, commissioners, health insurers, hospitals, health and social care professionals, older people, informal carers) through a fully participatory approach (see also Billings & Leichsenring, 2014). After the Viennese initiative was developed, important key-people, who also designed the initiative and introduced SUSTAIN to their organizations, left SUSTAIN (i.e. change of employment) which caused several delays. Consequently, other steering group members worried about the continuation of the initiative and considered to withdraw from the implementation of the project. Finally, other professionals took their places and implemented the project at their best. However, they experienced difficulties with taking ownership of the project objectives since they were not involved in designing the initiative.
“ I’m honest. I’m only in this project because my former colleague already confirmed our participation in the project. My boss said I have to take over so I did. Otherwise I would not have worked in that project since it is not my field of expertise.” (Steering group member 3)
Table 6 - Barriers of improving integrated care.
Reasons for not succeeding and improving integrated care
• Limited resources • No mandatory assignment (Missing remit) • Absent or not involved caregiver• Lack of project ownership

TABLE OF CONTENTS

23
TABLE OF CONTENTS
4.1 Working towards integrated care improvements that could have an impact
Findings from the Viennese improvement project indicate that fostering a more integrated provision of dementia care across different health care sectors can lead to improvements regarding person-centered, prevention-orientated, safe and efficient care. (see chapter 3) However, a successful implementation depends on the context in which improvements are implemented and must be individually considered.
The Gerontopsychiatric Centre (GPZ) already provided comprehensive and integrated dementia care (Psota & Sepandj, 2003; see also Arrue et al., 2016) and maintained their high quality of care provision, as indicated by service users and informal carers. A specific strength of the experienced care was the thorough needs assessment and counselling by the staff. Further, they felt safe and well cared for since the GPZ listened to them and involved service users and (in-)formal carers in their care. Putting the person in the centre of care rather than the disease was associated with person-centered care. Reviewing the number of medications, medication adherence and addressing medication interaction in regard of older people living with dementia were seen as key factors by the professionals when it comes to delivering safe care. Most of the participants indicated that a change in their medication helped to improve their well-being.
Inter-professional-training sessions were held by professionals of the GPZ and should raise the awareness and knowledge of hospital staff. Moreover, the trainings should enable an early detection of older people living with dementia. Findings indicate that inter-professional-training
sessions can foster a person-centered and prevention-oriented care approach. In the hospital staffs’ opinion, the trainings lead to a more attentive and sensitive dementia care. However, only some wards tested and recommended identified people to the GPZ on a regular basis. It seems that inter-professional training sessions alone are not sufficient to foster prevention-oriented care in all wards and contextual factors must be considered (see chapter 3.3, 3.4 or 4.2)
Due to the project, a sustainable link was established between two wards and the GPZ, one in each participating hospital. These wards integrated the initiative in their daily routines and referred older people continuously to the integrated care centre. Moreover, they will engage in further dementia programs in the near future. However, not all wards implemented the initiative successfully and since only 8 out of 39 identified people (for reasons see chapter 3.2) used the service of the GPZ, efficiency was questioned by some professionals. The family carers played an important role regarding the use of integrated dementia care (see chapter 3.1). Professionals indicated that older people without a caregiver cannot take advantage of the initiative since they are not able to arrange further care on their own, and consequently are not able to follow the care recommendation made by the hospital staff. These people, however, are the ones who needed further care at the very most and would benefit from the project. To involve social service providers was considered as possible solution in order to overcome a systematic bias.
4. MAIN LESSONS LEARNED FROM GERONTOPSYCHIATRIC CENTRE (GPZ)

24
TABLE OF CONTENTS
4.2 Working towards integrated care improvements that could be transferable across the EU
Within the Viennese SUSTAIN project, we identified various drivers and barriers regarding the implementation of the improvement project. Generally speaking, they could be divided in intrinsic factors (e.g. motivation, mission values and attitudes of professionals/wards) and extrinsic factors (e.g. financial and personnel resources) indicating that factors of success lie on the one hand within the professionals itself and on the other hand suggesting that success can be facilitated from outside through creating a favorable environment.
Within the Viennese initiative, influencing factors varied among wards and findings indicate that there is more than one way to implement an initiative successfully. Therefore, we suggest that improvements of integrated care are highly context dependent and there is no one-size-fits-all solution. A tailored approach should be considered that utilizes a variety of key and enabling factors.
A lack of resources was considered as most substantial barrier for implementing the improvement initiative and was perceived as continuous challenge by all involved healthcare organizations. Additional funding was non-existent and the professionals had to complete activities relating to the project on top of their existing workload.
This led in most cases to a restricted project implementation and activities were only partly pursued. This indicates, that available resources and funding must be considered and discussed thoroughly in order to come to a mutual agreement with implementation partners and to prevent operating delays.
However, personal values and attitudes that were collectively shared were important facilitators with the power to overcome limited resources. In the improvement project, success was related to highly motivated professionals, who perceived dementia care as their personal mission regardless of financial, personnel or time resources. Such champions are considered as important factor for implementing integrated care - also across Europe (Shaw et al., 2012). Champions influence and facilitate change in others through demonstrating commitment, promoting innovation with passion and persistence, bring together groups of different professions and develop informal networks of support.
Findings of the Viennese project suggest that depending solely on champions is not enough to sustain large-scale improvements. Both, already engaged champions on professional or organizational level as well as steering from outside to provide resources (e.g. policy/decision maker) are needed to support change and sustain improvements within the health care system (see figure 2).
Figure 2 - Both, motivated champions and governmental leadership is needed to sustainably integrated care initiatives.
(Top Down) Management of integrated care by policy maker
• provide infrastructure• provide resources• official assignment for improving integrated care
(Bottum-up) Champions of integrated care
• highly interested in improving integrated care• personal matter• personal mission
Alignment

25
TABLE OF CONTENTS
4.3 Methodological reflections
As explained in section 1.2, for SUSTAIN we consulted several data sources to evaluate progress and outcomes of the implementation of the improvement project. In the health aand social care initiative in Vienna, we experienced some challenges with data collection.
Firstly, not all hospital wards were able to recruit older people throughout the project phase due to various reasons (see chapter 3) which is reflected in a limited study sample size. Secondly, older people were hesitant or unwilling to participate, because they disapproved the data transfer between the involved organisations (e.g. medical report, contact information); mistrusted the screening result and considered themselves not being afflicted with dementia; or simply did not want to be involved in a scientific study. Furthermore, some older people, who participated in the interviews and surveys, experienced difficulties with understanding the questions and found them too repetitive, or insufficiently aligned with their situation. Also, the retrieval of the client reports (medical reports) appeared to be challenging since most of the participants were not aware of its’ existence.
The SUSTAIN project team also encountered some challenges with data collection regarding the SUSTAIN core domain efficiency. Hours spent on the intervention for instance were not routinely recorded by professionals. All professionals and managers who were asked to participate in interviews and complete the surveys did so. However, numbers were still low due to the small number of professionals and managers partaking in the project. As a consequence of these challenges, the analysis of the case study relied heavily on qualitative data. However, in line with the principles of case study design, we were able to retrieve these data from different types of respondents and therefore to capture different perspectives.
4.4 Overall reflections and keypoints
The improvement project aimed to counter the considerable rate of underdiagnosed cases of dementia among older people in the hospital and provide them and their caregiver with access to community-based integrated care. Therefore, an integrated care agreement was established between two Viennese hospitals and the integrated dementia care centre GPZ.
• Twenty-two percent of the identified older people with suspected dementia used the service of the integrated care centre (38% refused). Influencing factors were - time professionals spend with informing the people about dementia, - involvement of informal carers, - stage of disease - and characteristics of the older people and their carers (e.g. health-consciousness).
• Some wards implemented the initiative successfully and sustain the integrated care agreement. Older people and their carer followed more likely the professionals’ recommendation and described their care as person-centred, prevention-oriented and safe.
• Involvement of family carers, - availability of personnel resources, - prior knowledge, - a cooperative partnership between different staff groups, – and positive personal values and attitudes towards the initiative and dementia care facilitated the project implementation.
• Interrelated barriers which hindered the project implementation were - limited time and personnel resources –lack of project ownership (no mandatory assignment), -absent or not involved caregiver
• Personal values and professional attitudes which were collectively shared were important facilitators with the power to overcome scarce resources. However, they seem not sufficient to sustain large-scale improvements. In addition, steering on policy level is needed to sustain changes within the health care system.

TABLE OF CONTENTS
PART 2 Coordinated Palliative Care Styria (CPC)

27
TABLE OF CONTENTS
5.1 General description of the site
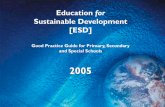
Styria is a state in the southeast of Austria with a population of approximately 1.2 million, 19% of whom are 65 years or older. Against the background that palliative care wards are not sufficient to provide person-centered care at the end of older people’ lives, the main mission of the initiative is to spread the concept of palliative care in Styria and to coordinate palliative care services across all health and social care settings (see figure 3).
Within the SUSTAIN project the Coordinated Palliative Care Styria (CPC) focused on its mobile palliative care teams (MPCTs) which provide integrated care for terminally ill people and offer support for formal and family carers. As a central value, the individual, rather than the symptoms, is in the focus of their working routine. The MPCTs are multi-disciplinary teams including physicians, nurses, social workers, volunteers, coordinators and administrative personnel who support and accompany older people and their families at the end of life.
The initiative started in 2001 with the implementation of the first ‘mobile palliative care team’. By 2005, it succeeded to secure one-stop funding by the ‘Styrian Health Fund’ and was thus able to offer services for older people with foreseeable terminal illness free of charge under the aegis of the Styrian Hospital Holding (KAGES), but across health and social care settings. The mobile palliative care teams in Styria were the first outside Vienna to provide this kind of services on a regular basis (since 2002). They are currently covering the entire region albeit with restricted resources. Formally CPC is an organizational unit of the KAGES (Regional Hospital Holding) which it is accountable to with a budget allocated by the Regional Health Fund. However, the individual MPCTs are organizationally affiliated to three welfare organizations (The Red Cross, Volkshilfe, Hilfswerk) that are providing regular care at home in defined districts of Graz (and Styria Graz).
A wide range of network partners is collaborating in CPC, among others, GPs, specialist doctors, the Hospice Association (which coordinates volunteers supporting the MPCTs, if appropriate), pharmacies and care homes. However, while written agreements were established with all home care providers, networking is based on voluntary commitments.
5.2 Rationale for improvement project
The individual ‘Mobile Palliative Care Teams’ (MPCTs) certainly represented a fully integrated model of care with some degree of coordination between the regional teams. However, the site noticed gaps of coordination and integration with other stakeholders such as the individual hospital wards and general home care services.
A clearer service/task description for the MPCTs and formal carer of general home care services was missing, which sometimes led to an overlap between services provided by the MPCTs and formal carers. The team members of the MPCTs are affiliated to different home care providers (i.e. The Red Cross, Volkshilfe and Hilfswerk). In some cases, the MPCTs and other formal carers were assigned to the same person although some team members of the MPTCs were affiliated to the same home care provider as the other formal carer. Therefore, a clear definition and distribution of service responsibilities for the MPTCs and general home care service regarding people in need for palliative care was required.
Furthermore, non-uniform training and lack of education was making a consistent and sustainable provision of high
5. COORDINATED PALLIATIVE CARE STYRIA (CPC): CHARACTERISTICS AND IMPROVEMENT PROJECT

28
TABLE OF CONTENTS
quality care in all MPCTs difficult. Consultancy skills were necessary to realize what people really need. Therefore, further training was an area that needed improvement as underlined by the CPC.
Another field of improvement was identified in regard to trans- and cross-organizational collaboration. Although written agreements were established with all home care providers, networking was based on voluntary commitments. A more elaborated collaboration between the CPC and respective stakeholders was requested.
5.3 Aims and objectives of improvement project
The aim of this project was to define a set of criteria and improved communication methods for a structured and coordinated care process between the palliative care teams and other social and health care providers. As an important part of this project, participants identified the necessity to enhance the definition of the target group as well as the responsibilities of partners involved in a seamless care process (including informal caregiver). The implementation of the improvement project was planned in three different districts of Graz and its surroundings (i.e. Straßgang, Gries, Kainbach) and should involve three different providers of mobile care services (Red Cross, Volkshilfe and Hilfswerk). Figure 4 gives a visual overview on the envisaged improvement project.
Unfortunately, the site withdrew its participation in SUSTAIN before the improvement project was finalized. To explore the reasons for the drop out and to learn more about barriers and facilitators of integrated care, four interviews were held with the manager of the site, two nursing and care manager of the involved homecare providers Red Cross and Volkshilfe, and the chief physician of KAGES Hospital LKH Graz (palliative unit).
Figure 3 - Hospice- and palliative care system coordinated by CPC. (german version © Hospiz Österreich ÖBIG).
Hospice & Palliative Care
Simple cases More complex cases
Basis Care Support Services Care Services
Acute Care Hospitals
Hospice Teams
Palliative Counselling for Hospital Staff
Palliative ward/unit
Long-Term CareRetirement Home,
Nursing Home
Mobile Palliative Teams
Stationary Hospice
Home CareGP, Specialists,
Therapists, Mobile Services
Daytime Hospice

29
TABLE OF CONTENTS
Figure 4 - Flowchart of the envisaged improvement project “Structured care of palliative-geriatric patients living at home”.
Coordinated Palliative Care Graz/Styria
Basic mission:Provision of adequate (mobile and institutional) palliative care services for older people living at home
Characteristics:• Mobile and flexible
multi-professional teams• Mostly based on cooperation
between regional hospitals and regional welfare organizations
Improvement Project
-> Optimal integration/coordination of palliative care teams with (other) mobile social- and health-care services
• Enhance definition of target group• Define responsibilities of all partners in a seamless care process
(incl. informal caregivers)• Awareness and knowledge transfer between mobile palliative
care teams and other social-/health-care providers
Hospices
‘Structured care of palliative-geriatric patients living at home’
SocialServices
GPAssociation

TABLE OF CONTENTS

31
TABLE OF CONTENTS
6.1 Introduction
The Coordinated Palliative Care Syria (CPC) joined SUSTAIN in 2015 with the vision to improve its integrated care initiative. Together with several stakeholders of the Styrian health care sector they developed the improvement project “Structured care of palliative- geriatric patients living at home”. The aim of this project was to define a set of criteria and improved communication methods for a structured and coordinated care process between the palliative care teams and other social and health care providers (see 5.2;5.3.). To develop the project in more detail, a steering group was appointed which comprised of six representatives from CPC, the three home care providers Red Cross, Volkshilfe and Hilfswerk and the Styrian Hospital Holding KAGES. ÖPIA was designated to observe the meetings and to evaluate the project progress.
Before the first steering group meeting took place, the CPC informed ÖPIA about its withdrawal from SUSTAIN. Their decision was non-revocable. However, they agreed to participate in follow-up interviews and to engage in the Roadmap development of SUSTAIN.
The follow-up interviews indicated that the motivation of the CPC Styria to participate in SUSTAIN was high. The professionals appreciated the interdisciplinary discourse within the SUSTAIN-workshop and were pleased with the initiative they developed. They described the project as relevant to their daily work since it aimed to integrate health care services from different healthcare providers in order to obtain a common frame work of palliative care provision in Styria that is geared to the needs of older people living in their final stage of life. The main reason for participating in SUSTAIN was to empower older people and their caregivers through establishing an easily comprehensible service provision and bring more clarity in the clients care.
“ More clarity for the patients was always our main priority… that they [older people] are able to understand their care, and can distinguish [who is providing what kind of care]. Secondly, it would have improved our collaboration…would have led to a more connected care provision of the mobile care teams. (…) Besides that, I think it would have led to a better understanding of care provided by other professionals…more empathy for other types of professions, and broaden our horizon.” (Steering group representative 2)
6.2 Reasons for the withdrawal from SUSTAIN
Four single follow-up interviews were conducted with key-representatives of the envisaged initiative to explore the reasons for the withdrawal. Overall, there was dissension regarding the reason for withdrawal.
Despite the good premises, ambiguity about the implementation of the project was present from the beginning. Overall, most of the interviewed professionals indicated that the withdrawal was induced by a single person who was key for the project continuation and consequently, did not represent the sentiments of the group. In this case, shortages in personnel and time were discussed as reasons for the withdrawal. Additional resources (personnel, financial) would have been needed to implement the project alongside the regular workload which already included extra hours. One representative assumed that financial support was tied to the project implementation otherwise a smaller initiative would have been developed.
6. FINDINGS OF THE IMPROVEMENT INITIATIVE IN COORDINATED PALLIATIVE CARE STYRIA (CPC)

32
TABLE OF CONTENTS
“ Assuming that we would have financial or personnel support, a completely different project was developed in the workshop. If we were told in advance that this would not be the case, we would have developed different goals for the project.” (Steering group representative 4)
Apart from a clear communication on resources (personnel, financial) and goals that are aligned with the available resources, other reasons for the withdrawal were seen in the individuals (and their backgrounds) involved in the project. According to other interview partners it was more about a lack of goodwill to turn ideas into sustainable actions which always involve extra work and effort.
“ I don’t think that the goals were incorrect but probably the will of those involved to really properly take it up and finish it off.” (Steering group representative 3)
Furthermore, the struggle for power between the nursing and medical staff of the hospital was mentioned as underlying reason in regard of the withdrawal. Thus, a different steering of the project would have been necessary in order to prevent that individual people were in a position to distinguish oneself from the others involved.
“ For me it was a kind of struggle for power between the medical and the care unit that in some way escalated.” (Steering group representative 1)
6.3 Barriers and facilitators for improving integrated care initiatives in Austria
The interview partners were also asked about their opinion on barriers and facilitators of integrated care in Austria. As the “origin of all problems”, the fragmentation of responsibilities, information flows and funding sources were seen as main barriers of establishing integrated care. Still, related reforms remain ad hoc and are often discontinued since an over-arching approach is missing.
Improvements base on motivated professionals who were able to bring relevant stakeholders together. In the respondents view, champions (see chapter 3.3 or 4.2) are key in order to bring all relevant stakeholders together and to overcome particular economic interests. Carefully defined incentives are suggested to ensure that improvements result in economically positive outcomes for all stakeholders. In the view of the interviewed professionals, an external coordinator responsible for implementing integrated care may prevent an adverse group dynamic guided by a struggle of power.
“ Many particular interests of single units and I would say a lack of steering from outside. It needs much more coordination, that is for sure. These things are not fast-selling items.” (Steering group representative 1)
6.4 Reflection and key points
The intended improvement project of Coordinated Palliative Care Styria (CPC) gives insight in the challenges of improving integrated care. Despite initial motivation and goodwill, the developed initiative was not followed through due to the withdrawal of a key-partner of the project. The involved stakeholders hold different views with respect to the underlying reasons. On one side, a lack of time, personnel and financial resources are reported as main barriers for implementing integrated care improvements. On the other side, ulterior motives like a lack of goodwill and a struggle of power were assumed as underlying reasons.
Considering integrated care in Austria, the fragmentation of responsibilities, information flows and funding sources are recognized as main barriers of establishing integrated care. An overarching approach, steered from outside (e.g. policy maker) and accompanied by an appropriate funding system is required in order to facilitate change in the health care system in particular for integrated care improvements within and across health care sectors.
• Single individuals/organizations play a pivotal role regarding integrated care improvements.
• Fragmentation of responsibilities, information flows and funding sources are recognized as main barriers of establishing integrated care in Austria.
• An overarching approach, including an appropriate funding strategy, is needed to establish efficient and sustainable integrated care improvements.
• Steering from outside might overcome power struggles between the different types of professions and across health care providers.

TABLE OF CONTENTS
PART 3

34
TABLE OF CONTENTS
7.1 Conclusion
The two Austrian sites were chosen because they represent examples of innovative practice and characteristic features of the Austrian context for integrated care. Both sites focused on improving integrated care across health care sectors indicating that integration of care is still a challenge with room for improvements.
Findings from the Viennese site show that integrated care improvements can foster a more person-centred, prevention-oriented, safe and efficient care delivery. However, a successful implementation of specific activities depends on the context in which improvements are implemented and must be individually considered. Both sites were highly interested in improving integrated care however, experienced challenges to some extent during the project implementation. A particular barrier of integrating improvements into existing care services was a lack of resources (time, personnel, financial) since both sites had to implement project related tasks on top of their daily work. Consequently, activities were only partly pursued and in case of CPC shortages in staff and finances led to a withdrawal from the project in the end.
Representatives of both initiatives emphasized the pivotal role of single individuals on improving (integrated) care. In case of site one, motivated individuals (champions) who demonstrated personal commitment, passion and persistence towards the initiative objectives facilitated the project implementation, brought together groups of different professionals and succeeded despite of restricted resources. On the other side, CPC was not able to continue its improvement project due to the withdrawal of a key-partner.
Furthermore, findings suggest that champions are not sufficient in order to sustain large-scale improvements.
Beside engaged champions, an overarching approach, steered from outside (e.g. policy maker) and accompanied by an appropriate funding system is required in order to facilitate change in the health care system in particular for integrated care improvements within and across health care sectors.
7.2 Implications of SUSTAIN for integrated care in Austria
Firstly, the scientific partners of SUSTAIN in Austria have conducted a review of national good practice regarding integrated care provision for home-dwelling older people (Arrue et al., 2016). This has given first important insights in daily practice, current care concepts and basic conditions of integrated care in Austria. The related SUSTAIN country report might serve as a basis for future discussions and processes to improve integrated care services in Austria. In the same way, awareness of the challenges of integrated care for older people was raised and expert discussions were stimulated. However, discussions remained limited and attached to specific regions and stakeholders in Austria.
The improvement project realized in Vienna increased the awareness among the involved health care staff in regard of the symptoms and early diagnosis of dementia. Medical and nursing staff became more aware of disease-related challenges for older people and their family carers. Further, integrated dementia care was introduced to the hospital sector as an additional and more interconnected way of care delivery. Eventually, other hospitals and healthcare organizations will follow their model of good practice and
7. OVERALL (NATIONAL) REFLECTIONS

35
TABLE OF CONTENTS
explore new approaches to healthcare delivery that can bridge the boundaries between professions, providers and institutions and consequently improve care for the rising number of people with chronic health problems. However, the positive effects of one improvement project are a small seed that might once contribute to establish more sustainable and large scale integrated care initiatives and a kind of integrated care culture, which is currently not well established in Austria (see chapter 1.1). Even if there is a growing recognition that integrated-/ continuous-/ or seamless-care are of importance for more efficient health care provision, there is no tradition, no adequate framework and no professional or political “lobby” for integrated care in Austria. This situation has not been substantially changed due to SUSTAIN.
7.3 Policy recommendations
- Policy and decision makers have to be aware that necessary financial and structural investments in the development of integrated care systems - similar to investments in healthcare prevention - will usually not bring an immediate return on investment or an easily comprehensible benefit, but have to be seen as a long-term strategy.
- This means that related policy decisions can not only be built on (economic) evidence, but also have to rely on international scientific studies and practice related expertise.
- Nevertheless, it will be worthwhile and important to support future research that can develop business-cases and provide further evidence for cost effective integrated care services.
- Based on respective evidence and scientific insights integrated care needs lobbying in order to become a priority topic on the agendas for national health- and social care planning.
- Adequate and supportive framework conditions (e.g. better inter-organizational collaboration, easier exchange of sensitive information, more financial transparency etc.) have to be established and supported by responsible authorities.
7.4 Recommendations for service providers
- Structural and operational procedures for providing integrated care need to be integrated in the basic mission of the organization as well as the work assignments of staff members. This means, for example, that working time that is specifically dedicated to improve integrated care pathways for patients (e.g. time to give information to patient and relatives, time for communication with
other organizations, time for filling in forms etc.) is acknowledged and accepted as regular work and not as some kind of “extra” duty.
- As the successful implementation of integrated care services widely depends on personal engagement as well as on communication and informal collaboration between staff members it is important to support respective working cultures and organizational environments. This may be done in form of training sessions to improve social skills and communication between staff members or by fostering exchange and joint decision making between professional groups (nursing staff, medical staff and others).

TABLE OF CONTENTS

37
TABLE OF CONTENTS
8. REFERENCES
Arrue, B., Ambugo, E., Baan, C., Barbaglia, G., Billings, J., De Bruin, S., . . . Zonneveld, N. (2016). Integrated care for older people living at home: current situation and ambition of sites participating in the SUSTAIN project. Vienna: Austrian Interdisciplinary Platform on Ageing / OEPIA.
Billings, J., & Leichsenring, K. (2014). Methodological development of the interactive INTERLINKS Framework for Long Term Care. International Journal of Integrated Care, 14(2).
Craig, P., Dieppe, P., Macintyre, S., Michie, S., Nazareth, I., & Petticrew, M. (2008). Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ, a1655. https://doi.org/10.1136/bmj.a1655
Creswell, J. W. (2009). Research design: qualitative, quantitative, and mixed methods approaches (3rd ed). Thousand Oaks, Calif: Sage Publications.
De Bruin, S. R., Stoop, A., Billings, J., Leichsenring, K., Ruppe, G., Tram, N., … Paat-Ahi, G. (2018). The SUSTAIN project: a European study on improving integrated care for older people living at home. International Journal of Integrated Care, 18(1).
Epping-Jordan, J. E. (2004). Improving the quality of health care for chronic conditions. Quality and Safety in Health Care, 13(4), 299–305. https://doi.org/10.1136/qshc.2004.010744
Fick, D. M., Steis, M. R., Waller, J. L., & Inouye, S. K. (2013). Delirium superimposed on dementia is associated with prolonged length of stay and poor outcomes in hospitalized older adults. Journal of Hospital Medicine, 8(9), 500–505.
Gaugler, J. E., Kane, R. L., Kane, R. A., & Newcomer, R. (2005). Early Community-Based Service Utilization and Its Effects on Institutionalization in Dementia Caregiving. The Gerontologist, 45(2), 177–185. https://doi.org/10.1093/geront/45.2.177
Glasgow, R. E., Green, L. W., Taylor, M. V., & Stange, K. C. (2012). An Evidence Integration Triangle for Aligning Science with Policy and Practice. American Journal of Preventive Medicine, 42(6), 646–654. https://doi.org/10.1016/j.amepre.2012.02.016
Joray, S., Wietlisbach, V., & Büla, C. J. (2004). Cognitive impairment in elderly medical inpatients: detection and associated six-month outcomes. The American Journal of Geriatric Psychiatry, 12(6), 639.
Kamenski, G., Dorner, T., BEng, K. L., Psota, G., Rieder, A., Schwarz, F., … Strotzka, S. (n.d.). Detection of dementia in primary care: comparison of the original and a modified Mini-Cog Assessment with the Mini- Mental State Examination, 10.
Kivimaki, M., & Elovainio, M. (1999). A short version of the Team Climate Inventory: Development and psychometric properties. Journal of Occupational and Organizational Psychology, 72(2), 241–246. https://doi.org/10.1348/096317999166644
Lau, D. T., Mercaldo, N. D., Shega, J. W., Rademaker, A., & Weintraub, S. (2011). Functional Decline Associated With Polypharmacy and Potentially Inappropriate Medications in Community-Dwelling Older Adults With Dementia. American Journal of Alzheimer’s Disease & Other Dementiasr, 26(8), 606–615. https://doi.org/10.1177/1533317511432734
Lynch, T., Connor, S., & Clark, D. (2013). Mapping Levels of Palliative Care Development: A Global Update. Journal of Pain and Symptom Management, 45(6), 1094–1106. https://doi.org/10.1016/j.jpainsymman.2012.05.011
McLean, S. (1987). Assessing dementia. Part I: Difficulties, definitions and differential diagnosis. Australian and New Zealand Journal of Psychiatry, 21(2), 142–174.
Minkman, M. M. (2012). Developing integrated care. Towards a development model for integrated care. International Journal of Integrated Care, 12.
Nolte, E., Knai, C., Hofmarcher, M., Conklin, A., Erler, A., Elissen, A., … Vrijhoef, H. J. (2012). Overcoming fragmentation in health care: chronic care in Austria, Germany and The Netherlands. Health Economics, Policy and Law, 7(1), 125–146.
Pelttari, L., & Pissarek, A. (2013). Hospiz Osterreich: advancing end-of-life care in Austria. EUROPEAN JOURNAL OF PALLIATIVE CARE, 20(2), 100–102.
Psota, G., & Sepandj, A. (2003). Das Gerontopsychiatrische Zentrum (GPZ) des PSD Wien. In Multiprofessionelle Altenbetreuung (pp. 251–256). Springer.
Schang, L., Waibel, S., & Thomson, S. (2013). Measuring care coordination: health system and patient perspectives: report prepared for the Main Association of Austrian Social Security Institutions.
Schwarzkopf, L., Menn, P., Leidl, R., Graessel, E., & Holle, R. (2013). Are community-living and institutionalized dementia patients cared for differently? Evidence on service utilization and costs of care from German insurance claims data. BMC Health Services Research, 13(1), 2.
Shaw, E. K., Howard, J., West, D. R., Crabtree, B. F., Nease, D. E., Tutt, B., & Nutting, P. A. (2012). The Role of the Champion in Primary Care Change Efforts: From the State Networks of Colorado Ambulatory Practices and Partners (SNOCAP). The Journal of the American Board of Family Medicine, 25(5), 676–685. https://doi.org/10.3122/jabfm.2012.05.110281
Shenkin, S. D., Russ, T. C., Ryan, T. M., & MacLullich, A. M. (2013). Screening for dementia and other causes of cognitive impairment in general hospital in-patients.

38
TABLE OF CONTENTS
Sommerlad, A., Perera, G., Singh-Manoux, A., Lewis, G., Stewart, R., & Livingston, G. (2018). Accuracy of general hospital dementia diagnoses in England: Sensitivity, specificity, and predictors of diagnostic accuracy 2008–2016. Alzheimer’s & Dementia. https://doi.org/10.1016/j.jalz.2018.02.012
Trukeschitz, B., & Schneider, U. (2012). Long-term care financing in Austria. In Financing Long-Term Care in Europe (pp. 187–213). Springer.
Wagner, E. H., Bennett, S. M., Austin, B. T., Greene, S. M., Schaefer, J. K., & Vonkorff, M. (2005). Finding common ground: patient-centeredness and evidence-based chronic illness care. Journal of Alternative & Complementary Medicine, 11(supplement 1), s-7.
Yin, R. K. (2014). Case study research: design and methods (Fifth edition). Los Angeles: SAGE

TABLE OF CONTENTS

40
TABLE OF CONTENTS
9. ANNEXES
9.1 Practical measures for monitoring outcomes and progress of the implementation of the improvement plans.
Item Data collection tool Short description
DEMOGRAPHIC INFORMATION
Socio-demographics of older people (users)
Demographic data sheet – older people, administered to older people
Survey developed by SUSTAIN researchers requesting information on age, gender, education, marital status, living situation and self-reported medical conditions
Socio-demographics of informal carers
Demographic data sheet – carers, administered to informal carers
Survey developed by SUSTAIN researchers requesting information on age, gender, education, marital status, relationship and distance to older person (user), paid work and caregiving activities
Socio-demographics of professionals
Demographic data sheet – professionals, administered to professionals
Survey developed by SUSTAIN researchers requesting information on age, gender, nationality and occupation
Socio-demographics of managers
Demographic data sheet – managers, administered to managers
Survey developed by SUSTAIN researchers requesting information on age, gender, nationality and occupation

41
TABLE OF CONTENTS
Item Data collection tool Short description
OUTCOMES
Person-centredness
Patient perceptions of quality and coordination of care and support
The Person Centred Coordinated Care Experience Questionnaire (P3CEQ) (Sugavanam et al., under review), administered to older people
Survey measuring older people’s expe-rience and understanding of the care and support they have received from health and social care services
Proportion of older people with a needs assessment
Care plan template (in case sites do not work with care plans, information will be retrieved from clinical notes or other documentation)
Template developed by SUSTAIN researchers for predetermined content analysis of care plans of older peopleProportion of care plans actioned
(i.e. defined activities in care plan actually implemented)
Proportion of care plans shared across different professionals and/ or organisations
Proportion of informal carers with a needs assessment and/or care plan
Perception and experiences of older people, informal carers, professionals and managers with person-centredness
Semi-structured interviews and focus group interviews with older people, informal carers, professionals and managers
Interview and focus group schedules developed by SUSTAIN researchers including interview items on perception and experiences with receiving person-centred care
Prevention orientation
Perceived control in care and support of older people
Perceived Control in Health Care (PCHC) (Claassens et al., 2016), admin-istered to older people
Survey addressing older people’s perceived own abilities to organise professional care and to take care of themselves in their own homes, and perceived support from the social network
Proportion of older people receiving a medication review
Care plan template (in case sites do not work with care plans, information will be retrieved from clinical notes or other documentation)
Template developed by SUSTAIN researchers for predetermined content analysis of care plans of older peopleProportion of older people receiving
advice on medication adherence
Proportion of older people receiving advice on self-management and main-taining independence
Perception and experiences of older people, informal carers, professionals and managers with prevention
Semi-structured interviews and focus group interviews with older people, informal carers, professionals and managers
Interview and focus group schedules developed by SUSTAIN researchers including interview items on perception and experiences with receiving prevention-oriented care

42
TABLE OF CONTENTS
Item Data collection tool Short description
Safety
Proportion of older people receiving safety advice
Care plan template (in case sites do not work with care plans, information will be retrieved from clinical notes or other documentation)
Template developed by SUSTAIN researchers for predetermined content analysis of care plans of older people
Proportion of older people with falls recorded in the care plan
Perception of older people, informal carers, professionals and managers with safety
Semi-structured interviews and focus group interviews with older people, informal carers, professionals and managers
Interview and focus group schedules developed by SUSTAIN researchers including interview items on perception and experiences with receiving safe care, and safety consciousness
Efficiency
Number of emergency hospital admissions of older people
Care plan template (in case sites do not work with care plans, information will be retrieved from clinical notes or other documentation); template to register staff hours and costs
Template developed by SUSTAIN researchers for predetermined content analysis of care plans of older people; template developed by SUSTAIN researchers to collect data on costs and the number of staff hours from local services, organisations or registries
Length of stay per emergency admission of older people
Number of hospital readmissions of older people
Number of staff hours dedicated to initiative
Costs related to equipment and technology or initiative
Perception of older people, informal carers, professionals and managers with efficiency
Semi-structured interviews and focus group interviews with older people, informal carers, professionals and managers
Interview and focus group schedules developed by SUSTAIN researchers including interview items on perception and experiences with receiving efficient care, and finances
IMPLEMENTATION PROGRESS
Team coherence of improvement team (professionals)
Team Climate Inventory – short version (TCI-14)(Anderson and West, 1994; Kivimaki and Elovainio, 1999), administered to professionals
Survey measuring vision, participative safety, task orientation and experienced support for innovation of the improvement team
Perception and experiences of professionals
Focus group interviews with profes-sionals and minutes from steering group meetings
Focus group schedule developed by SUSTAIN researchers including interview items on experienced factors facilitating and impeding outcomes and implementation progress
Minutes cover progress, issues and contextual issues impacting on outcomes and implementation progress
Perception and experiences of managers
Semi-structured interviews with managers and minutes from steering group meetings
Interview schedule developed by SUS-TAIN researchers including interview items on experienced factors facili-tating and impeding outcomes and implementation progress
Minutes cover progress, issues and contextual issues impacting on outcomes and implementation progress

TABLE OF CONTENTS
Vienna, June 2018