
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN …
157
i “SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA’’ By DR. RAKSHITH K.R Dissertation Submitted To RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, BANGALORE, KARNATAKA In Partial Fulfillment of the Requirements for the Degree of AYURVEDA VACHASPATI (M.D. AYURVEDA) In SWASTHAVRITTA AND YOGA Under The Guidance Of Dr. SHIVAKUMAR M.D. (AYU) Associate Professor Department of Post Graduate Studies in Swasthavritta and Yoga SDM College of Ayurveda & Hospital, Hassan DEPARTMENT OF POST GRADUATE STUDIES IN SWASTHAVRITTA AND YOGA SRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF AYURVEDA & HOSPITAL, HASSAN –573 201, KARNATAKA 2017
Transcript of SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN …

i
“SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN
AMLAPITTA’’
By
DR. RAKSHITH K.R
Dissertation Submitted To
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
BANGALORE, KARNATAKA
In Partial Fulfillment of the Requirements for the Degree of
AYURVEDA VACHASPATI (M.D. AYURVEDA)
In
SWASTHAVRITTA AND YOGA
Under The Guidance Of
Dr. SHIVAKUMAR M.D. (AYU)
Associate Professor
Department of Post Graduate Studies in Swasthavritta and Yoga
SDM College of Ayurveda & Hospital, Hassan
DEPARTMENT OF POST GRADUATE STUDIES IN SWASTHAVRITTA
AND YOGA
SRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL,
HASSAN –573 201, KARNATAKA
2017

ii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
BANGALORE, KARNATAKA
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled “Survey Study On Effect Of
Ahara and Vihara In Amlapitta” is a bonafide and genuine research work carried out by
me under the guidance of Dr. Shivakumar, M.D.(AYU), Associate Professor, Department
of Post Graduate Studies in Swasthavritta and Yoga, SDM College of Ayurveda, Hassan -
573 201, Karnataka.
Date: Signature of the candidate
Place: Hassan (Dr. Rakshith K.R)

iii
DEPARTMENT OF POST-GRADUATE STUDIES IN
SWASTHAVRITTA AND YOGA
SRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL, HASSAN –573 201
(Affiliated to Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka)
Certificate
This is to certify that the dissertation entitled “Survey study on effect of
Ahara and Vihara in Amlapitta” is the bonafide record of research work
conducted by Dr. Rakshith K.R under my direct supervision and guidance as a
partial fulfillment for the award of the degree of Ayurveda Vachaspati (M.D.
Ayurveda) in Swasthavritta and Yoga.
The candidate has fulfilled all the requirements of ordinances laid down in
the prospectus of Rajiv Gandhi University of Health Sciences, Bangalore,
Karnataka, for the award of Degree of Ayurveda Vachaspati (M.D. Ayurveda) in
Swasthavritta and Yoga.
I am fully satisfied with his work and recommend this thesis to be
submitted for adjudication.
Date: Guide:
Place: Hassan Dr. Shivakumar M D (AYU)
Associate Professor,
Department of Swasthavritta and Yoga
S.D.M. College of Ayurveda, Hassan

iv
DEPARTMENT OF POST GRADUATE STUDIES IN
SWASTHAVRITTA AND YOGA
SRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF AYURVEDA
& HOSPITAL, HASSAN –573201
(Affiliated to Rajeev Gandhi University of Health Sciences, Bangalore, Karnataka)
ENDORSEMENT BY THE HOD AND HEAD OF THE INSTITUTION This is to certify that the dissertation entitled “SURVEY STUDY ON EFFECT OF
AHARA AND VIHARA IN AMLAPITTA” is the bonafide record of research work
conducted by “Dr. RAKSHITH K.R” under the guidance of Dr. SHIVAKUMAR,
Associate Professor, Department of Post Graduate Studies in Swasthavritta and Yoga,
SDM College of Ayurveda, Hassan –573 201, Karnataka.
Dr. M B Kavita MD (AYU ) Dr. Prasanna N Rao, M.S.(AYU),PhD
Associate Professor and HOD Principal
Department of P G Studies in Swasthavritta SDM College of Ayurveda, Hassan
And Yoga Karnataka
SDM College of Ayurveda, Hassan, Karnataka
Date: Date:
Place: Hassan Place: Hassan
v
COPYRIGHT
Declaration by the candidate
I hereby declare that Rajiv Gandhi University of Health Sciences, Bangalore,
Karnataka shall have the rights to preserve, use and disseminate this dissertation /
thesis in print or electronic format for academic/ research purpose.
Date: Signature of the candidate.
Place: Hassan (Dr. RAKSHITH K.R)
© Rajiv Gandhi University of Health Sciences, Karnataka

vi
ACKNOWLEDGEMENT
My gratitude, which is the mother of all virtues and most capital of all duties, has all
there order and diligence to all those who graciously involved in this venture of mine. There
is much greatness of mind in acknowledging a good turn, as in doing it.
I humbly, seek this opportunity to bow my head to the feet of The Almighty for
showering His blessings and empowering me to this eventful outcome without any
impediments.
Words are not enough to express my gratitude and indebt to the sacrifices of my
beloved and respected parents Shri. Ramaprasad and Smt. Rajalakshmi who are the cause
for me to take this noble profession and shape me into what I am today.
I pay my respectful salutations to His Holiness Rev. Sri Veerendra Heggadeji,
founder father of Sri Dharmasthala Manjunatheshwara College of Ayurveda and Hospital,
Hassan and fountainhead of educational movements, for his divine blessings in disguise and
who has been kind enough to provide me an opportunity to study and render my service in
this esteemed institution.
My vocabulary falls short of suitable words to express my recondite sense of
indebtedness to my compassionate teacher Prof. Prasanna Narasimha Rao, Principal and
Prof. Gurdeep Singh. Director, P.G. Board of Studies, they have been guiding force and
instrumental in all the proceedings of my postgraduate study and stood as an excellent
encouraging stanchion in all strides in accomplishing this meticulous effort.
It is beyond the reach of my language to inscribe the profound respect and devotion
towards my guide and guru Dr. Shivakumar for his constant support, timely guidance and
valuable suggestions to get this work done successfully.

vii
I express my sincere gratitude to my guru Dr. M. B. Kavita H.O.D., Dept. of
Swasthavritta & Yoga as without her guidance and support, this work would not have
completed.
I am extremely grateful to Dr. T.B. Tripathy, Professor Dept. of Swasthavritta &
Yoga for his constant support and guidance during my thesis work. I whole heartedly thank
Dr. Bargale Sushant Sukumar, Dr. Gurubasavaraj Yalagachin Lecturers Department of
Swasthavritta & Yoga, SDM Ayurveda College and Hospital, Hassan for their timely and
valuable advises.
Having an able team of members with distinct characters is necessary to keep the
journey flawless. It was my privilege to get such an able team in my friends, my classmates,
Dr. Dheeraj Kumar Tyagi, Dr. B Mahesh Raju, Dr. Vijeth Kumar L A, Dr. Sreeharsha N,
Dr. Asha S A, and Dr. Manjunath Kotiyal I would like to express my deepest gratitude to all
of them for they made me understand the true value of friendship. The whole work would
have been futile without their support and whole hearted cooperation.
I am very much thankful to my seniors, Dr. Abhishek Magotra, Dr. Arun K,
Dr. Sandeep, Dr. Shibu Issac , Dr. Arathi, Dr. Harish Deshpande, Dr. Saurabh Agarwal,
Dr. Arun, Dr. Jyothi Jalakoti, Dr. Haripriya, Dr. Deepuram, Dr. Rajesh Chandran without
their able guidance it would have been an impossible task to finish this work.
It was my privilege and pleasure to have such able and wonderful juniors
Dr. Venu s Achar, Dr. Harshita K J, Dr. Siddarth Yadav, Dr. Anjali Pant, Dr. Lakshmi
Varma, Dr. Pooja Hassan, Dr. Sonia, Dr. Swathi Sharma, Dr. Aparajitha , Dr. Sahana,
Dr. Swathi, Dr. Anjana, Dr. Veekshan Shetty Dr. Sushil Kumar, Dr. Sagar k kora, Dr.
Madan kumar and Dr. Vivek Aradhya for their support and encouragement throughout the
research work.
viii
Words are not enough to express my gratitude towards my dearest Brother Panith
K.R, who has always been with me in my ups and downs and has been a constant inspiration.
I express my gratitude towards grandparents Smt.Seetalakshmamma, Shri
Srinivasamurthy and Smt.Seetalakshmamma, Shri Keshavamurthy whose support has
proved to be in par with my parents.
I once again extend my heartfelt gratitude to each and every person who has
directly or indirectly helped me in this study.
Dr. Rakshith K R

ix
ABSTRACT
“SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA”
BACKGROUND
The period of 21st century is regarded as the era of modern technology and tough
competition due to which eating habits and lifestyle is totally changed. Indulgence of food
articles which are incompatible combinations, spoiled, sour or causing burning sensation and
other food and drinks which increases Pitta dosha produces Amlapitta in person, whose Pitta
dosha is already aggravated. The man of this era is becoming prey to series of life-style
disorder which are much more bothering than the infective diseases. The altered life-style
pattern like night shifts, mental stress, addictions etc. is the major risk factors for Amlapitta.
Medicine alone cannot bring the desired therapeutic effect without Pathya. On the other hand
if Pathya is observed there will be no need of medications. Hence it is necessary to educate
the people regarding dos and don'ts about diet and lifestyle as it plays a major role in
manifestation of Amlapitta.
OBJECTIVE
To study the effect of Ahara and Vihara in Amlapitta.
METHODOLOGY
Simple Random Sampling - Alternate method was used in this study. It was
questionnaire based survey study on 345 subjects from OPD and IPD of Sri Dharmasthala
Manjunatheshwara College of Ayurveda and Hospital and subjects from in and around
Hassan city who fulfils the inclusion and exclusion criteria, were selected and set of
questionnaire containing 45 questions which contains Aharaja and Viharaja Nidanas of
Amlapitta were given to them and their responses regarding the study was taken.

x
INCLUSION CRITERIA
Diagnosed subjects of Amlapitta.
Individuals of age group between 16 to 60 years.
EXCLUSION CRITERIA
Subjects who are not willing to participate.
Drug induced Amlapitta cases.
Pregnant women.
Subjects with Systemic disorders.
RESULT
Chi square and odds ratio shown risk in the manifestation for Amlapitta.
CONCLUSION
Based on result it can be concluded that there is effect of Ahara and Vihara in
manifestation of Amlapitta.
KEYWORDS
Amlapitta, ahara, vihara, hyperacidity, odds ratio, chi square.
xi
LIST OF ABBREVIATIONS
1. M N - Madhava Nidana
2. K S - Kashyapa Samhita
3. S N - Siddanta Nidana
4. B R - Bhaishajya Ratnavali
5. H S - Harita Samhita
6. Y R - Yoga rathnakara
7. S S - Susruta Samhita
8. A H - Astanga Hridaya
9. A S - Astanga Sangraha
10. B S - Bhela Samhita
11. C S - Charaka Samhita
12. Ch. Chi - Charaka Chikitsa sthana
13. B P - Bhava Prakasha
14. Vij - Vijayarakshita
15. C D - Chakradatta
16. Ckp - Chakrapani
17. S G S - Sri Gananatha Sena
18. Van - Vangasena
19. K C - Kaya Chikitsa
20. Ch Su - Charaka Sutrasthana
21. Hcl - Hydrochloric acid
22. NSAID - Non-steroid anti-inflammatory
drug
23. PGs - Prostaglandins
24. CCK - Cholecystokinin
25. GERD - Gastrooesophageal reflux
26. OD - Once daily
27. PUD - Peptic ulcer disease
28. GU - Gastric ulcer
29. DU - Duodenal ulcer
30. BAO - Basal acid output
xii
CONTENTS
No Chapters Page
1. Introduction 1-4
2. Aims and Objectives 5-6
3. Review of Literature 7-49
4. Materials and methods 50-54
5. Observation and results 55-100
6. Discussion 101-116
7. Conclusion 117-120
8. Summary 121-123
9. References 124-131
10. Annexure 132-141

xiii
LIST OF TABLES
Sl No Contents Page No.
1. Apathya according to various authors 3-4
2. General Nidanas of Amlapitta 23
3. Types of Amlapitta 26
4. Samprapti Ghataka of Amlapitta 29
5. Describe about Aggressive and Protective factors in PUD 46
6. Differentiating Chronic Gastric Ulcer from Duodenal Ulcer 47
7. How frequently you use Garlic in a week? 56
8. How frequently you use Ginger in a week? 57
9. How frequently you use Sour taste Food in a week? 58
10. How frequently you use Spoiled Food in a week? 59
11. How frequently you use Spicy Food in a week? 60
12. How frequently you use Horse gram in a week? 61
13. How frequently you use Flour items in a week? 62
14. How frequently you use Green Chili in a week? 63
15. How frequently you use Sour Curd in a week? 64
16. How frequently you use Red Chili in a week? 65
17. How frequently you use New Jaggery in a week? 66
18. How frequently you use Salty Food in a week? 67
19. How frequently you use Domestic meat with Honey in a
week?
68
20. How frequently you use Black Gram in a week? 69
21. How frequently you use Pickle in a week? 70
22. How frequently you use Fish with Curd in a week? 71
23. How frequently you use Fish with Milk in a week? 72
24. How frequently you use Horsegram with Curd in a week? 73
25. How frequently you use Milk with Raddish in a week? 74
26. How frequently you use Salt with Milk in a week? 75
27. How frequently you use Pork with Curd in a week? 76
28. How frequently you use Sour Fruits with Milk in a week? 77

xiv
LIST OF FIGURE
29. How frequently you use Leafy Vegetables with Butter in a
week?
78
30. How frequently you use Banana with Curd in a week? 79
31. How frequently you use Aerated Drinks in a week? 80
32. How frequently you use Heated Curd Preparations in a
week?
81
33. Do you have Habit of eating food irrespective of hunger? 82
34. Do you have Habit of Day sleep? 83
35. Do you have Habit of Alcohol Consumption? 84
36. Do you have Habit of Smoking? 85
37. Do you have Habit of excess intake of Tea or Coffee? 86
38. Do you have Habit of Skipping Meals? 87
39. Do you have Habit of drinking excess water soon after food? 88
40. Do you have Habit of Betal nut with tobacco? 89
41. Do you have Habit of adding extra salt or spice for food you
eat?
90
42. Do you have Habit of Hot atmosphere? 91
43. Do you have Habit of Bathing soon after having food? 92
44. Do you have Habit of Suppressing Natural urges? 93
45. Do you have Habit of Sleeping soon after having food? 94
46. Do you have Habit of Excess bath or tub bath 95
47. Do you have Habit of Drinking water between the meal? 96
48. How Often you express your Anger? 97
49. How Often you express your Stress? 98
50. How Often you express your Depression? 99
51. How Often you express your Anxiety? 100
Sl No Contents Page No.
1 Composition of Gastric juice 34

INTRODUCTION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 1
INTRODUCTION

INTRODUCTION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 2
INTRODUCTION
The people now days are living in an era of fast growing technology and tough
competition. The man of this era is becoming more susceptible to series of life style
disorders. The altered life style activities like having fried food, night shifts, mental stress
and addictions etc are the major risk factors for Amlapitta which is emerging as a
common lifestyle modification disorder. Amlapitta is one of the commonest Annavaha
Srotas Vyadhi,1 caused by vitiation of Tridosha. When any of Dosha causes Mandagni it
leads to Vidagdhajirna manifesting as Amlapitta.2 Excess intake of sour food containing
high acid levels and sedentary life style with little or no physical activity like exercise has
also been the known culprits.
Ayurveda gives a complete look into the life style of a person starting from his or
her personality to the daily food habits. The science teaches how to live in healthy way,
importance of both preventive and therapeutic aspects of medicines.
In Ayurveda the Nidanas mentioned for Amlapitta can be classified into
Aaharajanya, Vihaarajanya and Maanasika Bhavajanya all of which can be correlated to
etiologies mentioned under life style changes. The need for hour is required to find out
ways by which we can manage the condition hyper acidity through dietary and life style
modifications rather than medicines.
Need For the Study
A population-based study, using a validated questionnaire, found that 58.7% of
the population has heartburn or acid regurgitation at least once during the course of a year
and that 19.8% experience symptoms at least once weekly.3 Hence it is necessary to
INTRODUCTION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 3
educate the people about do’s and don'ts about diet and lifestyle as it plays a major role in
causing Amlapitta.
Due to work load, stress, poor eating habits, not following dinacharya,
ratricharya, ritucharya and sadvritta leads to so many diseases and as well tridosha
prakopa, which are causing so many diseases of new origin. As we know importance of
good lifestyle and healthy eating is require for a healthy and fruitful living. Amlapitta is a
disorder which is related with Ahara and Vihara factors. So here an effort was made to
study the effect of Aharaja and Viharaja Nidanas which are mentioned in classics which
cause Amlapitta.
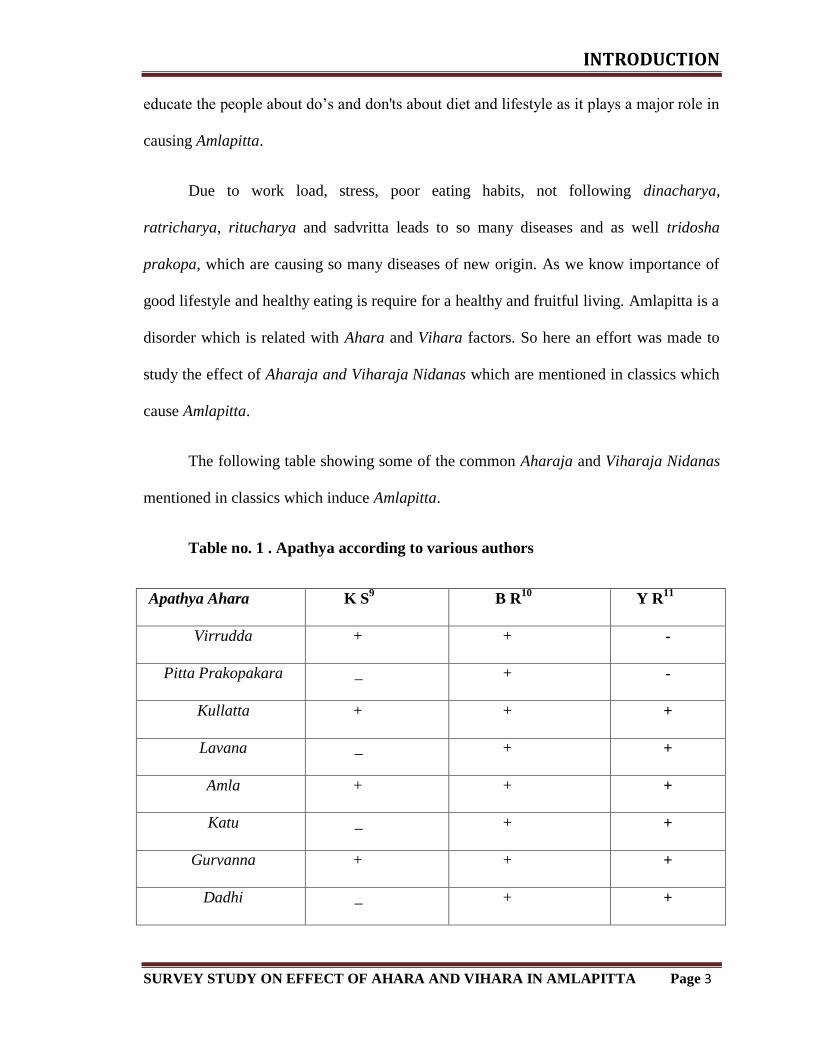
The following table showing some of the common Aharaja and Viharaja Nidanas
mentioned in classics which induce Amlapitta.
Table no. 1 . Apathya according to various authors
Apathya Ahara K S9
B R10
Y R11
Virrudda + + -
Pitta Prakopakara _ + -
Kullatta + + +
Lavana _ + +
Amla + + +
Katu _ + +
Gurvanna + + +
Dadhi _ + +

INTRODUCTION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 4
Madhya + + +
Adhyasana + _ -
Ajirna + _ -
Pistanna + _ -
Abhishyandi bhojana + _ -
Ati Ushna + _ -
Ati Ruksha + _ -
Ati Snigdha + _ +
Apathya Vihara
Vami vegadharana _ + -
Vegana dharana + _ -
Divaswapna + _ -
Atisnana + _ -
Ati avagahana + _ -
Antharodaka pana + _ -
AIMS & OBJECTIVES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 5
AIMS
&
OBJECTIVES

AIMS & OBJECTIVES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 6
AIMS AND OBJECTIVES
The present survey study entitled “Survey study on effect of Ahara and Vihara in
Amlapitta” was carried out with following aims and objectives.
1. To study the effect of Ahara and Vihara in Amlapitta.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 7
REVIEW
OF LITERATURE
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 8
REVIEW OF LITERATURE
AMLAPITTA:
For the better understanding of the subject, it is necessary to find out its historical
background, which gives a concrete understanding in the development of the concept of
the disease from time to time.
Charaka Samhita:
In Charaka Samhita, at nine different places reference regarding Amlapitta can
been found, however the disease has not been listed among the diseases in Ashtodariya
chapter.
1. While describing the indication of milk Amlapitta has been listed. 4
2. The word “Amlaka” has been included in the list of 40 Pittaja Nanatmaja
vyadhis. 5
3. Among the chief Agrya Dravyas “Kulattha” considered as the chief causative
factor for Amlapitta. 6
4. Excessive use of Lavana Rasa causes Amlapitta and due to intake of more Amla
Rasa there is burning sensation in Kanta, Uraha and Hridaya. 7
5. Intake of Viruddha Anna is responsible for diseases like sterility, blindness,
Visarpa, Amlapitta etc. 8
6. Raja Masha is the pacifying factor for Amlapitta. 9
7. Mahatikta Ghrita has been indicated in Amlapitta. 10
8. While describing the Grahani Dosha pathogenesis of Amlapitta has been clearly
mentioned. 11

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 9
9. One of the many indications of Kansa Haritaki is Amlapitta. 12
Though in Charaka Samhita there is no mention of Amlapitta as a separate
disease, from the above reference it gives a clear cut indication regarding the Nidana,
Samprapti and management during this period.
Sushruta Samhita (1000 BC):
Description of Amlapitta as a disease or word is not found, but while describing
the disease caused due to excessive use of salt he has mentioned a disease called
“Amlika” 13
which is similar to Amlapitta.
Kashyapa Samhita (1000 BC):
Kashyapa Samhita 14
is the first textbook in which Amlapitta has been explained
as a separate disease entity. It contains not only the vivid description i.e. etiological
factors, signs, symptoms, complications and treatment, but also suggests changing the
place ( Deshantargamana), for the peace of mind when the habitat itself is a triggering
factor.
Bhela Samhita (1000 BC):
There is no description about Amlapitta.
Harita Samhita (1000 BC):

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 10
Amlapitta as a separate disease and its treatment is mentioned in Harita
Samhita.15
Here it is mentioned that, Guda is the causative factor and “Amlahikka” as a
special symptom for Amlapitta.
Vagbhatta:
Amlapitta has not been described as a disease entity but description of Paittika
Hridroga seems very nearer to Amlapitta.
Madhava Nidana (7th Century):
It is the first available textbook next to Kashyapa Samhita which has description
of Amlapitta along with clinical subtypes i.e. Urdhvaga and Adhoga Amlapitta.
Chakradatta (11th century):
Mentioned only Amlapittahara Yoga.
Vangasena (12th century):
Explained details of Amlapitta and its treatment in this textbook, Avipattikara
Choorna along with some other Yoga are also mentioned.
Sharangadhara Samhita (13th century):
Amlapittahara Yoga has been described along with etiopathology of the disease.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 11
Basavarajiyam (15th Century):
Mentioned Amlapitta under 24 Nanatmaja Vyadhi of Pitta. Among the other
symptoms Swara Hinata, Jihva–vak Paridaha have been attributed to Amlapitta, which
have not been mentioned in other texts.
Bhavaprakasha (16th century):
Etiopathological factors similar as Madhava Nidana have been described. In
Bhavaprakasha, many recipes along with the Khanda Kushmanda Avaleha and Narikela
Khanda can be found.
Bhaishajya Ratnavali (18th century):
Some recipes for Amlapitta also mentioning of Soubhagya Suntimodaka and
Shunthi Khanda as an effective treatment along with Pathya - Apathya.
Yogratanakara (19th century):
Author of this textbook followed Madhava Nidana completely and also described
Avastha Vaisheshika Chikitsa along with Rasa Aushadhi.
DEFINITION AND ETYMOLOGY OF AMLAPITTA
Amlapitta is a combination of two words Amla and Pitta. Among these two words
the Amla denoted the Rasa (sour taste) and the Pitta denotes the Dosha involved in this
disease. The Pitta Dosha is bestowed with the function of digestion and metabolism.
Amla Rasa is considered as the Prakruta Rasa of Pitta 16
, where as other
authorities believe that Katu is the Prakruta Rasa of the Pitta and attains Amlata in

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 12
Vidagdhavasta.17
The disease where the natural Katu rasa of Pitta is replaced by Amlata
due to Vidagdhavastha can be called Amlapitta.
Definition:
Many definitions can be found in the textbooks of Ayurveda about Amlapitta.
According to Vijayarakshita, commentator of Madhava Nidana, Amlapitta means-the
Pitta which attains excessive Amlata because of Vidagdha Paka is called Amlapiitta.18
Other definition quotes Amlapitta as Pitta possessing excessive Amlata or the
excessive Amlaguna Udrikta Pitta.19
Srikanthdutta has defined Amlapitta as a disease
mainly due to vitiation of Pitta (Pachaka), but Kapha (Kledaka) and Vata vitiation may
be involved secondarily causing Gourava, Udgara, Klama etc.
Clinically Amlapitta can be defined as presence of Avipaka, Klama, Utklesha,
Amlodgara, Gourava, Hrit-Kantha Daha and Aruchi.[20]
So, Amlapitta is a condition
where Amlaguna of Pitta increases due to Samata causing Vidahadi condition.
Paryaya:
The paryayas (synonyms) of Amlapitta signify different aspects of it. Synonyms
of Amlapitta are as follows: 21
Prameelaka
Amlapitta
Pittavisuchika
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 13
Other synonyms of Amlapitta are Pittamla and Shuktata.22
The terms Amalaka
and Amleeka may be added as synonyms to the above for they imply the important
features of the disease.
Prameelaka:
The Pachyamana Vidagdha Annarasa immediately provokes Pittadi Dosha, there
by producing Aruchi, Mukha Vairasya, Praseka, and continuous Lavana Tiktamla
Udgara, Chardi, discolouration, emaciation, Hritshula, Sadana and restlessness. This
state is known as Prameelaka23
this term is mentioned under Kaphaja Vyadhi.
Amlapitta:
The implication of the term Amlapitta denotes the abnormal state of Pitta
especially in its Amlaguna.
Pittavisuchika:
This may pertain to both the types of Amlapitta i.e. Urdhvaga and Adhoga
Amlapitta, where their respective cardinal features are Urdhvaga Pravrutthi (Vamana)
and Adhapravrutthi (Atisara) of Pitta associated with burning sensation.
Pittamla:
This term would imply the sense of the term Amlapitta which is mentioned in
Amlapitta Chikitsa in Yogratanakara.
Shuktata:
Shuktata is mentioned as a synonym of Amlapitta in Kashyapa Samhita. 24

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 14
Amlaka:
It refers to one of the Nanatmaja Vyadhi of Pitta mentioned in the context of
Pittaja Nanatmaja Vyadhi.25
Amaleeka:
Means Amlodgara and would refer to one of the Lakshana of Samapitta.26
AGNI AND AHARA PAKA
For proper understanding of Amlapitta the knowledge of Agni and Ahara Pachana
Karma is essential and is presented below:
Agni:
Nearly all diseases included under Kayachikitsa are engendered due to impairment
of Kayagni.27
Even Amlapitta which is an Annavaha Srotodusti Vikara is caused due to
Ahiara Paka Vaigunya. Pitta, one of the trinity of Doshas is also spoken of as Agni for
the reason that this factor in the body has been stated to perform actions similar to fire.
28As stated elsewhere, Agni is generally held responsible for the conduct of Pakadi
Karma viz. Sarapaka in Amashaya and Pakwashaya, the separation of Sara from Kitta in
the Pakwashaya, 29
augmenting the action of Bhutagni, 30
thus rendering the digested
food fit for further chemo-thermal reaction described by Chakrapani as Anupaka 31
after
which follows the reactions in Dhatu Paripaka.
The two main aspects of Agni have been envisaged by all the authorities of
Ayurveda as:
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 15
[1] Koshtagni [Charaka], Pachakagni, Jataragni [Sushrutha], Pachakapitta [Vagbhata].
[2] Dhatwagni
The former is stated to be located between Amashaya and Pakwashaya.32
This
aspect of Pitta or Agni while performing all the digestive functions described in the
foregoing paragraph is also stated to lend support and augment the functions of other
Pitta elsewhere in the body including the Dhatwagni. There are four stages of Jatargni as
Sama, Vishama, Tikshna and Manda. 33
The Tridosha become involved due to the operation of different etiological factors on the
body leading to reciprocal influence between them.
Sama Agni:
In the equilibrium state of functioning of Tridosha, Jatargni is stated to function
normally. This state of its function has been described as Sama Agni. Jatargni ensures
complete digestion of food in scheduled time without any harm to the body. 34
Vishama Agni:
An erratic state of Agni arises, as a result of the influence of Vata in the condition
described as Vishama Agni. The Agni varies with periods of strong digestive power
alternating with loss / decreased digestive power. 35
Tikshna Agni:
The Agni in this state is excited by Pitta known as Tikshna Agni. In this state, Agni
digests even large quantities of food faster to the scheduled time. 36

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 16
Manda Agni:
This is a state in which Agni is considerably inhibited due to the dominance of
Kapha dosha. In this state, the Agni is unable to digest and metabolize even a less
quantity of food which is easily digestible in scheduled time. 37
Out of these, the Sama Agni is considered as the Samanya condition of the Agni
and the rest three as the Vaishamyas.
The Vaishamyata of Agni leads to improper digestion due to Vruddhi or
Kshaya of Agni in their Guna, Pramana and Karma. In Mandagni, the food will be
Apakwa. In case of Tikshna Agni, it will be Dagdhapaka and Pakwa-apakwa in case of
Vishamagni. All these lead to specific type of Ajeerna leading to formation of Ama, one
of the important causes for the further vitiation of the Annavaha Srotas and manifestation
of the disease Amlapitta.
Aharapaka:
The Aharapaka has got two phases:
1. Prathama Paka / Prapaka 38
2. Vipaka 39
Prathama Paka/Prapaka:
The preliminary phase of digestion or the first outcome of the Paka is known as
Prathama Paka. This commences from the introduction of the food into the mouth
followed by the digestion of the food in the upper part of the stomach i.e. Urdhwa
Amashaya which is comprehended by Madhurabhava.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 17
Vipaka:
Vipaka has been defined as the outcome of the action of the Jataragni on the
Ahara Dravya which is resultant of the Prathamapaka, which is to be judged from the
point of view of the taste of the end product of gastro intestinal digestion viz. Madhura
(sweet), Amla (sour) and Katu (pungent).
Vipaka occurs in 2 phases:
1. Avasthapaka (during digestion)
2. Nishtapaka (at the end of the digestion)
Avasthapaka:
Avasthapaka refers to the changes that the Ahara Dravya undergoes in the Ama -
Pakwashaya under the influence of Jatargni as follows:
Madhura Avasthapaka
Amla Avasthapaka
Katu Avasthapaka
Madhura Avasthapaka:
The presence of food in the mouth is followed by the perception of its taste under the
influence of Bodhaka Kapha 40
which is seated in the root of the tongue. The outcome of
the action of Bodhaka Kapha on food, especially that fraction of its composition which
essentially is Madhura in taste seems to be continued and complete in the upper portion
of Urdhwa Amashaya. By now, the insoluble Madhura portion of food becomes

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 18
sufficiently soluble and mixed up with the frothy Kledaka Kapha. With the help of Kleda,
Sneha and Vayu, it breaks down, becomes less complex and soft and as a result, frothy
and sweet Ahara Rasa will be produced. Since, the Ahara Rasa produced is of Madhura
Rasa and contributes to Kapha, this is called Madhura Avasthapaka. 41
Amla Avasthapaka:
At this stage, Ahara reaches the lower part of the Amashaya. The Agni i.e.
Pachaka Agni which is stimulated by Samana Vayu acts on it and results in the
Vidagdhata of the Ahara Rasa. Thus formed Ahara Rasa attains Amla Guna and hence
the name Amla Avasthapaka. 42
This synchronizes with the passing down of Ahara Rasa
which has attained Amlabhava into the lower portion of Mahasrotas where Achha Pitta is
stated to be secreted and it comes in contact with the Pittasthana.43
The outcome of
second stage of digestion is characterized a state called as Vidagdha44
, which means
Pakwa-Apakwa 45
or Kinchit Pakwa or Kinchit Apakwa. Vidagdha can be defined as
“Vidagdha Sangnyamata Amlabhavam”.46
At this stage, the food substance remains partly
digested or partly undigested.
Katu Avasthapaka:
The food is subjected to further digestive events which take place in the
Pakwashaya which attains Katubhava47
or Katu Avasthapaka. The digested food particles
passed down from Amashaya having reached the Pakwashaya being dried up by Agni 48
is
rendered into lumps. During this process, the Ahara Rasa becomes Katu in nature and
Vayu Dosha will be nourished.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 19
AHARA PARINAMAKARA BHAVA:
Six factors are responsible for proper digestion, assimilation and metabolism of
food in human body, viz. Usma, Vayu, Kleda, Sneha, Kala and Samyoga. 49
Usma:
Usma is a quality of Agni Mahabhuta. In this regard, two terms are to be
considered viz. Agni and Pitta. There is no Agni except Pitta in body. Pachaka Pitta is
situated in Amashaya and it performs the function of Agni (digestion).
They should be released at proper time and proper quantity. Usma of Pachaka
Pitta is essential for proper digestion; disturbance of it will lead to diseases of Agni.
Vayu:
Samana Vayu is seated in Amashaya, helps the Pachaka Pitta in digestion. There
is a inter connection between Prana-Apana-Samana Vata 50
, it means all these helps to
maintain Agni. The Grahana and Munchana Karma of Vayu are essential for proper
digestion. Any exacerbation or cessation in these functions will lead to improper
digestion. As certain time is required for proper digestion, delayed emptying will cause
the Shuktapaka and formation of Amavisha, which is the causative factor of Grahani
Dosha. Now it is clear that all secretary regulations can be termed as functions of Samana
Vayu. If Samana Vayu is disturbed it will lead to Ajeerna and start the pathogenesis of
Annavaha Sroto Vyadhi.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 20
Kleda:
This factor is necessary for proper digestion; it loosens and emulsifies the food.
This function is performed mainly by liquid portion of food itself i.e. saliva, mucosa and
liquid portion of various digestive juices. Kledaka and Bodhaka Kapha may be
considered in this regard. Drava has been termed as Kleda in Ahara Parinama Bhava.
The function of Kledaka Kapha can be summarized as Kledana Shithilikarana-Mrudu
karana and Sangatha bedha. The excessive klinnatha may hamper the Agni directly as
mentioned in the literature that Dravatwa ceases the Agni. Ingestion of any Ati - Ushna,
Tikshna and Katu Dravya may cause increase in Kleda, which may interfere with
digestion process and increase in Kapha causes Mandagni.
Sneha:
Usually Ahara contains Sneha. Kapha as well Pitta are having the property of
Sneha 51
, it also belongs to Apamahabhuta, Sneha is a specific quality of Ap- Dhatu.
Hence, it can be said that Sneha is also the quality of Kledaka Kapha and Pachaka Pitta.
Sneha coming from Ahara as well as Kledaka Kapha and Pachaka Pitta, perform the
function of Mardava (softness of food stuff).
Kala:
Time required for the proper secretion of all the digestive factors and for digestion
and absorption. Kala means mainly the time required for the digestion of ingested food.
But other time factors considerations are also necessary for proper digestion and
absorption of food, i.e. Kshudhakala, Trishakala, Doshakala and also Charvanakala. The
food is to be taken after the proper digestion of previous meal. The meal taken without

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 21
proper digestion of previous meals is called as Adhyasana and this is the main cause of
Agnidushti.52
Emptying of stomach requires certain time. Retention of food material in
intestine is regulated by Vayu. Any disturbance of Vata will disturb the Grahana and
Munchana period leading to improper digestion and absorption which will lead to further
provocation of Doshas. The Adhyasana and Ajeerna-bhojana, may cause the Prakopa of
the Tridosha, simultaneously Agnidushti.
Samyoga:
Equilibrium of all above factors is necessary for the proper digestion of ingested
food material. Ashtavidha Ahara Ayatana should be considered to avoid Agnidushti. Most
of the diseases have a long list of etiological factors from dietary habits and food articles
53 and hence unbalanced dietary habit is cause for vitiation of Agni.
NIDANA OF AMLAPITTA:
After a careful screening and analysis, the etiological factors of Amlapitta can be
discussed under four groups, i.e. Aharaja Hetu, Viharaja Hetu, Manasika Hetu, and
Aagantuja Hetu.54
A brief description of these factors has been presented as under.
Aharaja Hetu [Dietary Factors]:
The first and the foremost group of etiological factors of Amlapitta may be
considered as the dietary factors. Under this, the intake of food against the code of
dietetics i.e. Ahara Vidhi Vidhana and Ahara Vidhi Visheshaayatana is included. Various
types of incompatible substances, excess of Pitta aggravating factors like Katu, Amla,
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 22
Vidahi, etc. and irregular time of consumption of food are the factors against the dietetic
code and they are directly responsible for the aggravation of Pitta.
Viharaja Hetu [Behavioural Factors]:
Irregular habits of defecation, eating, sleeping time, suppression the natural call,
may disturb the equilibrium of the body; may in turn disturb Pitta as well digestion which
ultimately will lead to Amlapitta.
Manasika Hetu [Psychological Factors]:
A disturbed psyche in terms of anxiety, anger, greediness, etc. would affect the
Prana and Vyana Vata, in turn may influence Samavata. Impaired Samanavata may
vititiate Jatargni which leads to impaired physiology of the digestion.
Aagantuja Hetu [Other Related Factors]:
Under this group constant and excessive consumption of alcohol, tobacco,
beverages, smoking, or other irritant stuffs, etc are taken. These substances cause local
irritation in the stomach, which in turn vitiate the Pitta leading to increased Amla Guna of
Pitta. All these factors are as given beneath:

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 23
Table 2: Showing general Nidanas of Amlapitta
Adhyasana Bhrishta Dhanya
Abhishyandi Bhojana Dushtanna
Ajeerna Divaswapana
Akala Bhojana Ati Gorasa Sevana
Ama Guru Bhojana
Ama Pakwa Anna Sevana Ikshuvikara
Atyamla Sevana Kulattha Sevana
Antarodaka Paana Madhya
Ati Ushna Ahara Paryushitanna Sevana
Ati Ushna Ahara Pitta Prakopi Anna Pana
Ati Ruksha Ahara Pisthanna
Ati Drava Ahara Pruthuka Sevana
Ati Ashana Vidahi Anna
Ati Avagahana Viruddhaasana
These may again be simplified in a more systemic way as follows.
Ahara group:
1. According to the type of Ahara:
[a] Kulattha [b] Pruthuka [c] Pulaka (husky food)
2. According to the quality of food:

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 24
[a] Abhishyandi [b] Ati-snigdha [c] Ati-ruksha [d] Gurubhojya [e] Vidahianna
3. According Samskara done on the Ahara: -
[a] Apakwa Anna [b] Bhrishta Dhanya [c] Ikshu Vikara [d] Pishta Anna
4. According to Dushti of Ahara:
[a] Dushta Anna [b] Paryushita Anna
5. According to the Pitta provocative properties of Ahara: [a]
Adhyasana [b] Ajirniasana [c] Ama Purnata [d] Ati Ushna [e]
Ati Amla [f] Ati Drava [g] Ati Teekshna [h] Ati Panam [i]
Katvannapana [j] Viruddhashana
6. According to the capacity of weakening the digestive power by the food:
[a] Ati Snigdha Sevana [b] Ati Ruksha Sevana
Vihara group:
[a] Akala Bhojana
[b] Antrodaka Pana
[c] Bhuktwa Divaswapa
[d] Bhuktwa Ati Avagahana
[e] Kale Anashana
[f] Vegavadharana
[g] Vishamashana
[h] Bhuktwa Ati Snana

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 25
Other related factors to the disease:
[A] Annahina Madya Sevana
[B] Gorasa Sevana
[C] Madya Sevana
POORVARUPA OF AMLAPITTA:
Poorvarupa or premonitory symptoms of this disease are not narrated in any
classics. But in practice it is observed that in the patients suffering from the disease
Amlapitta, there are certain symptoms, which are present for a quite long period before
manifestation of the disease. Some of them are Ajeerna, Utklesha, feeling of reduced
digestion etc.
ROOPA OF AMLAPITTA:
Amlapitta, out of which some are short-listed here, which are having predominance in the
patients coming for treatment.
The general symptoms of Amlapitta55
are:
Avipaka (indigestion), Klama (fatigue), Hrit-Kanta Daha (retro sternal/ epigastric
burning sensation), Amlodgara (sour belching), Gaurava (heaviness), Utklesha (nausea),
Tiktodgara, Aruchi (anorexia). Other symptoms are Vidbheda (loose bowels),
Aantrakoojana (gurgling sound intestine), Udaradhmana (distension of abdomen) and
Hritsoola (pain in chest region) 56

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 26
TYPES OF AMLAPITTA:
According to Gati of Pitta Madhava Nidana has described 2 types of Amlapitta57
a) Urdhvaga Amlapitta
b) Adhoga Amlapitta
According to involvement of dosha, Kashyapa and Madhavakara both have divided.
Table 3: Showing types of Amlapitta
Kashyapa Samhita 58
Madhava Nidana 59
Vatika Sanila
Paittika Kaphanugata
Shlaishmika Vatakaphadhika
Shleshmapitta
SAMPRAPTI OF AMLAPITTA:
The word Samprapti is the process of the disease formation beginning right from
the contact of the causative factors with the body to complete manifestation of the
disease. It is a course followed by a disease in which the Dosha gets vitiated and the path
it follows for the manifestation of disease.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 27
The etiological factors, which are against Ashtavidha Ahara Vidhi Vidhana and
Asana Pravicharanas, cause the vitiation of Dosha and Agni, which results in
Agnimandya and Avipaka, and in this stage even light diet cannot be digested. It remains
as it is in Amasaya and produces Suktatva, which leads to formation of Annavisha. This
Annavisha produces Ajeerna. Once Agnidushti occurs it results in Avipaka, Ajeerna and
this further damage the Agni. Agnidushti causes Shuktapaka of Ahara, which further
disturbs the Agni. Thus, Amavisha produced disturbs the Grahani Dosha and once it
happens it further produces the Ama Dosha and vicious cycle starts. Few etiological
factors mentioned in the list directly provoke Dosha (Pitta). Few of them result in
Dooshya Daurbalya e.g. Panchakarma Vibhrama and Vyadhikarshana.
Charaka has mentioned that if Annavisha Produced by this Samprapti mixes with
Pitta, it will produce Amlapitta. Kashyapa has described the Samprapti of Amlapitta in
detail first time and it seems similar to the Samprapti of Grahani Roga described by
Charaka. Chakrapani Datta has commented on it to describe whole mechanism.
Madhavakara has mentioned the involvement of only one Dosha i.e. Pitta but Kashyapa
has given the involvement of Tridhosha by writing the word
“Vatadyavaha” with the dominance of Pitta, Shrikantha Datta has clarified that
the causative factors of Amlapitta are Kapha and Pitta. He also explained Gaurava,
Udgara and Kampa symptoms are due to involvement of Kapha and Vata respectively. 60
Hence from above discussion it is clear that Kapha and Pitta Dosha i.e. Kledaka Kapha
and Pachaka Pitta are the main Dosha but same time we know that vice versa relation of
Pachaka Pitta and Samana Vayu (As per Sushruta).

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 28
Hence, it can be concluded that there is involvement of Tridosha but with the
dominancy of Pitta and Kapha.61
In the pathogenesis of Amlapitta, the involvement of the
Dosha can be categorized as Pitta on first place and Kapha on second place and the least
involved is Vata. The conditions Pittavrita (Vata) Prana are nearer to symptomatology of
Amlapitta. Hence it seems that the Amlapitta is a disease condition produced due to Pitta-
Kaphavrita Vata mainly Prana and Samana.62
Kashyapa has described that this disease occurs mostly in individuals having
Jihvalaulya.63
Patients generally know the etiological factor of the disease but due to
greed, they continue to consume them and this disease progress to Kashtasadhya stage
and it may manifest as Upadrava like Parinama Shoola etc.
Madhavakara has given two types i.e. Adhoga and Urdhvaga, Doshaja varieties
are also mentioned by various Acharya and differentiation in this type is difficult job.
This is also supported by Madhavakara by writing Bhishaka-Mohakara Vyadhi.64
The Adhoga type is very difficult to diagnose as it coincides with Paittika,
Atisara, and Paittika Grahani. Amlapitta is a disease of Annavaha Srotas. Mithya Ahara
and Vihara are the chief causes in the origin of this disease. The etiological factors
further may be classified into two groups. The first group includes those factors, which
are responsible for the state of Agnimandya and the etiological factors under the second
group include the factors, those vitiate the liquidity of Pitta and aggravate its quantity.
Two more additional Pitta vitiating factors, Anupa Desha and the Varsha Ritu have
specifically been observed and mentioned by Kashyapa and Madhavakara respectively.
Both these factors vitiate the Pitta via Jatargni leading to Mandagni.
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 29
As a result of above stated various causes any of the Dosha is vitiated and may
cause Mandagni. In this state of Mandagni whatsoever food material are consumed by an
unwise person, become Vidagdha and are converted into Suktavastha, This Vidagdha and
the vitiated Pitta later manifests in the form of Amlapitta.65
If not treated properly in this stage, the disease leads to Bheda Avastha where the
typical characteristics and types like Urdhavagata and Adhogata are differentiated.
Further complications like Sheetapitta, Udarda, Kotha, etc. are differentiated.
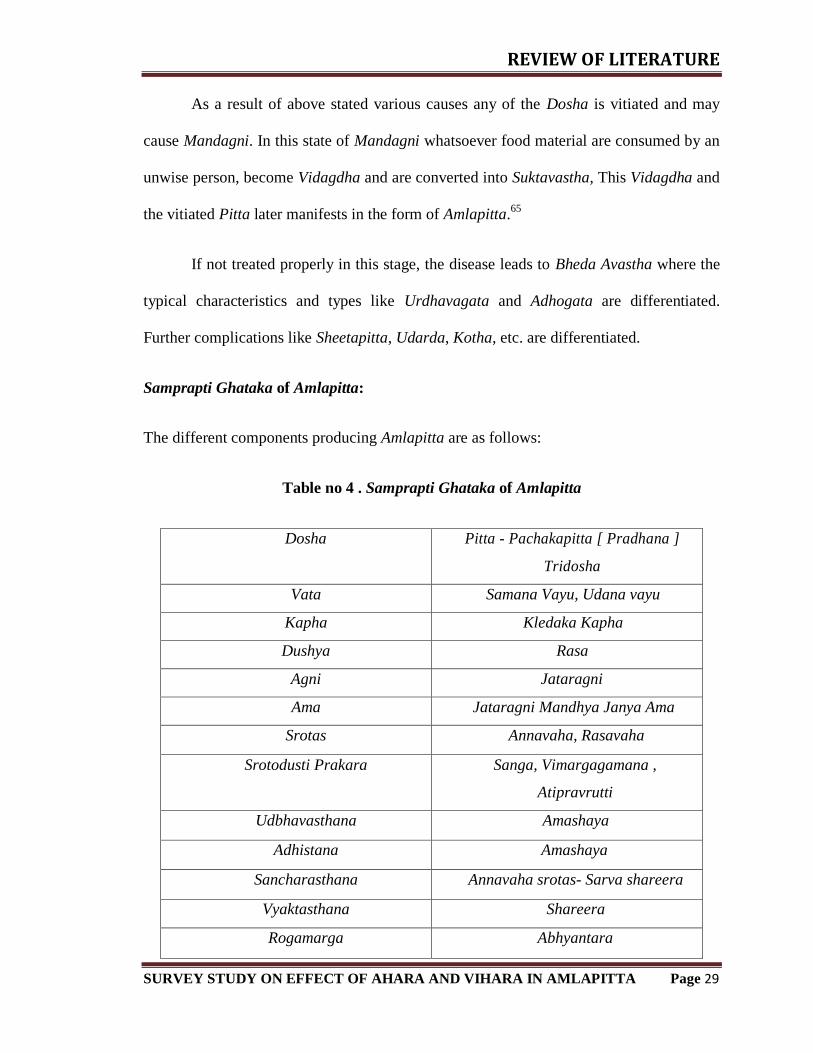
Samprapti Ghataka of Amlapitta:
The different components producing Amlapitta are as follows:
Table no 4 . Samprapti Ghataka of Amlapitta
Dosha Pitta - Pachakapitta [ Pradhana ]
Tridosha
Vata Samana Vayu, Udana vayu
Kapha Kledaka Kapha
Dushya Rasa
Agni Jataragni
Ama Jataragni Mandhya Janya Ama
Srotas Annavaha, Rasavaha
Srotodusti Prakara Sanga, Vimargagamana ,
Atipravrutti
Udbhavasthana Amashaya
Adhistana Amashaya
Sancharasthana Annavaha srotas- Sarva shareera
Vyaktasthana Shareera
Rogamarga Abhyantara

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 30
Differential Diagnosis:
Kashyapa, Madhava and Gananath Sen have mentioned specific Samprapti of
Amlapitta. The Samprapti of Grahani Roga mentioned by Charaka may be borrowed to
explain the pathogenesis of Amlapitta. There are many disease conditions which present
similar to Amlapitta e.g. Poorvarupa of Raktapitta, Gulma, Udara Poorvarupa, Arshas
symptoms, Grahani Poorvarupa, Pittaja Pandu, Udavarta, Pittavrita Vata, Pittavrita
Prana etc.
There are two main conditions from which we must differentiate the disease
Amlapitta; those are Vidagdhajirna and Samapitta. Out of which Samapitta is the stage of
Dosha. As there is no specific Dosha-Dooshya-Samurchana taken place, it cannot be
called as a disease. Vidagdhajirna is an acute state, if it occurs repeatedly it may results
into Amlapitta.
From treatment point of view we must differentiate these stages and diseases,
which may change the line of treatment. In primary stage of Vidagdhajirna, Alpa
Jalapana can relieve the symptom but in Amlapitta along with it Amla Drava Guna is
also increased.
SADHYASADHYATA
The Ayurvedic manuscripts bear the description regarding the prognostic status or
Sadhyasadhyata of the disease. Before going to the treatment, the prognosis as to the
curability [Sadhya] or incurable [Asadhya] and also whether it is easily curable [Sukha-
Sadhya] or curable with difficulty [Krichrasadhya] or maintained as long as treatment is
given [Yapya] should be estimated.
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 31
Charaka says, “A disease in its early stage is easily curable but when advanced, is
cured with quite difficulty or even becomes Asadhya”.66
Incurable diseases never become
curable while curable diseases may pass into stage of incurability on account of the short
comings in any of the four basic therapeutic factors or as the result of destiny.
Madhavakara states that, if Amlapitta is in its early stage is curable with efforts. If
it becomes chronic it becomes Yapya. In chronic cases and in persons with recent origin
indulging in Apathya Ahara Vihara, it becomes Krichrasadhya [curable with difficulty].
If Amlapitta is accompanied with the Upadrava [complications], then becomes Asadhya
[incurable].67
Kashyapa has stated that in case if the patient develops Upadrava
along with Dhatukshaya, then it becomes Asadhya [incurable].68
Hence, the early
diagnosis and prompt treatment of Nava or Taruna Amlapitta would not proceed to
become chronic and produce complications.
UPADRAVA
The occurrence of another disease in the wake of primary disease, as a
complication or sequel is termed as upadrava and is meant as Rogottarakalaja,
Rogashraya and Rogameva. The Upadrava of the disease corresponds to the intensity of
severity or chronicity of the disease.
Kashyapa in Khilasthana describes Upadrava of Amlapitta as follows:69
Jwara Shotha
Atisara Aruchi
Pandutva Bhrama
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 32
According to Gananath Sen:
Sheetapitta Vicharchika
Udarda Visphota
Kandu Pidaka
Kotha Amashaya Kshata
Mandala Grahani Kshata
MODERN REVIEW
HYPERACIDITY:
Hyperacidity word is composed of two components i.e. „hyper‟ and „acidus‟.
„Hyper‟ means over or excess and „acidus‟ means sour. So a straight meaning may be
derived as excess of sourness; i.e. any acid not particularly the HCl in stomach and a
disease, which contains this abnormal pathology, is defined as hyperacidity
The word Hyperchlorhydria indicates the condition in which there is an excessive
production of HCl in the stomach It is a characteristic observation in certain forms of
dyspepsia particularly associated with duodenal ulcer. It causes heartburn and water
brash. This term indicates about the functional abnormality i.e. hyper activity of the
secreting glands.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 33
Four processes normally take place in the stomach.
1. The conversion of starch into sugar, begun in the mouth, is carried a stage
further.
2. Proteins are changed into peptone
3. Fat globules are set free from their envelopes.
4. Milk is curdled.
Delay in digestion may be caused by
i) Deficient peristalsis of the stomach walls
ii) Deficient quality or quantity of the gastric juice
iii) Consumption of indigestible article
iv) The dilution of the gastric juice by drinking too much fluid at meal time.70
Properties of gastric juice71
Volume – 1200-1500ml/day
Reaction – highly acidic due to presence of HCl
Specific gravity – 1.002 to 1.004
PH – 0.9 to 1.2
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 34
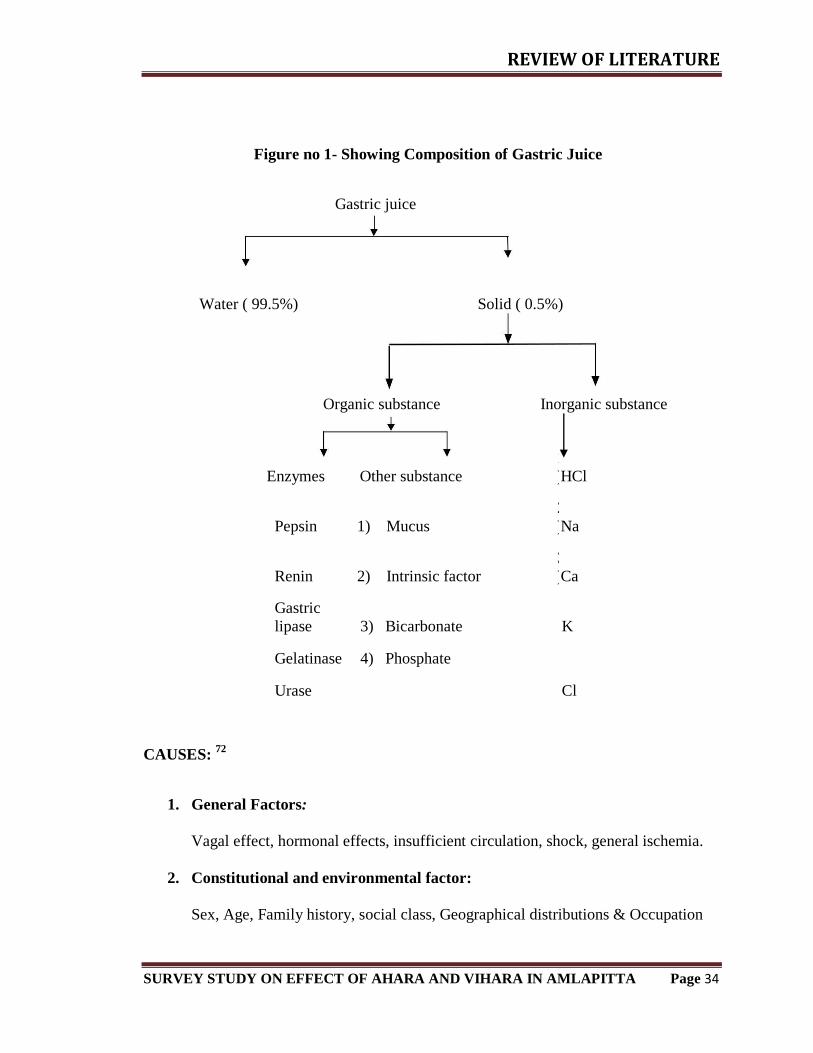
Figure no 1- Showing Composition of Gastric Juice
Gastric juice
Water ( 99.5%) Solid ( 0.5%)
Organic substance Inorganic substance
CAUSES: 72
1. General Factors:
Vagal effect, hormonal effects, insufficient circulation, shock, general ischemia.
2. Constitutional and environmental factor:
Sex, Age, Family history, social class, Geographical distributions & Occupation
Enzymes Other substance
1
) HCl
Pepsin 1) Mucus
2
) Na
Renin 2) Intrinsic factor
3
) Ca
Gastric
lipase 3) Bicarbonate K
Gelatinase 4) Phosphate
Urase Cl

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 35
3. Local factors related to Stomach:
A) Aggressive Factors: -
Hydrochloric acid, Pepsin, Refluxed bile, NSAIDs, Alcohol, Pancreatic and
Proteolytic enzymes, ingested irritants, bacterial toxins and Psychological trauma.
B) Defensive Factors: -
Mucus, bicarbonates, blood flow, restitution of epithelium. Thus defensive factors
are responsible for the enhancement of mucosal protection. Although no single element
may account for mucosal protection, all may be potentially contributing factors. Insight
into mucosal protective mechanisms was provided by studies performed by Robert. These
studies lead to the introduction of term “Cytoprotection” generally accepted to mean
protection of the gastric mucosal by prostaglandins (PGs) against damaging agents.
Defense of normal gastric mucosa against aggressive factors:
Three basic levels of defense underlined the remarkable ability of normal gastro
duodenal mucosal to resist injury from the acid and peptic activity in gastric juice.
1. Surface epithelial cells secret mucus and bicarbonates, creating a pH gradient
in the mucous layer and change the very acidic gastric lumen to the nearly
neutral surface of the mucosa.
2. Gastric mucosal cells have a specialized apical surface membrane that resists
the diffusion of acid back into the cell.
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 36
3. Mucosal cells may directly resist injury by intrinsic mechanisms; such as
extrusion a back diffused hydrogen ions by means of basolateral carriers (e.g.
Sodium - hydrogen or Sodium bicarbonate exchange).
The rapid repair of injury to the mucosa is essential to maintain the mucosal
integrity. Surface epithelial cells continually slough and adjacent cells that move to fill
them by cell replication in response to still unknown trophic signals reseal the gaps.
Blood flow in normal mucosa removes the acid that has diffused across a compromised
mucosa. Prostaglandins enhance the mucosa‟s resistance to injuries under certain
conditions, perhaps by increasing mucosal blood flow, stimulating the secretion of mucus
and bicarbonate, strengthening of the gastric mucosal barrier, decreasing the gastric
motility, increasing release of endogenous mediators of gastric Cytoprotection like
Sulfahydryls and epidermal growth factors, etc. scavenging of free radicals, decreasing
release of endogenous mediators of gastric injuries vasoactive amines and leukotrienes
and stimulation of cellular growth and repair
Role of Infection:
Lately some more information has poured in about the prevalence and changing
pattern of the disease, the influence of environmental factors and speculation on the role
of recently characterized bacterial organisms, Helicobacter pylori, which colonized the
gastric mucosa, particularly the antral region. H. Pylori are a gram-negative spiral
bacterium that is found in a patchy distribution overlaying in gastric epithelium. It was
formally named as campylobector pylori.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 37
At present 9 species of Helicobacter genus are available and all excluding
H.plyori, are of animal origin. H. Felis can be introduced into mice to produce intense
colonization and inflammation of stomach. H.plyori organisms have strong capability of
urease production. The bacteria then split urea and the ammonia thus released may
become cause of increased acidity and hence enabling organism to survive. The released
ammonia may also be cytotoxic. H.pylori has been implicated in the etiology of belching,
indigestion and chronic peptic ulceration. H.pylori induced gastritis present in about 60%
of patient with gastric ulcer. Until recently pathogenesis of gastric and duodenal ulcers
has been attributed to an imbalance between aggressive factors such as acid and pepsin
that damage the gastric mucosa and protective factors such as prostaglandins that prevent
the damage. Recent evidences relate H.pylori to the pathogenesis of chronic duodenal
ulcer as H.pylori infection and antral gastritis are found together in more than 95% of
patients with duodenal ulcers.
Pathogenesis:
Following factors are important in development of hyperacidity:
[1] Luminal acid and pepsin are requisite.
[2] Increased mucosal tissue acidosis with subsequent decrease secretion of bicarbonate.
[3] Reduced mucosal blood flow, whatever its basis (Shock, Drugs, Stress) causing
hypoxic injury & impairing the secretion of bicarbonate.
[4] Disruption of the mucosal barrier (i.e. the intake layer of surface mucosal epithelial
cells), permitting back diffusion of hydrogen ions and in turn increased shedding of
surface of cell.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 38
Species of Helicobacter genus are available and all excluding H.plyori, are of
animal origin. H. Felis can be introduced into mice to produce intense colonization and
inflammation of stomach. H.plyori organisms have strong capability of urease production.
The bacteria then split urea and the ammonia thus released may become cause of
increased acidity and hence enabling organism to survive. The released ammonia may
also be cytotoxic. H.pylori has been implicated in the etiology of belching, indigestion
and chronic peptic ulceration. H.pylori induced gastritis present in about 60% of patient
with gastric ulcer. Until recently pathogenesis of gastric and duodenal ulcers has been
attributed to an imbalance between aggressive factors such as acid and pepsin that
damage the gastric mucosa and protective factors such as prostaglandins that prevent the
damage. Recent evidences relate H.pylori to the pathogenesis of chronic duodenal ulcer
as H.pylori infection and antral gastritis are found together in more than 95% of patients
with duodenal ulcers.
Symptoms:
Disease Hyperacidity is the commonest disease of the fast, fashionable and fast
food based modern life. This is one of the commonest terms also used by the
patients to subject each gastric discomfort as Hyperacidity. Usually patients
having following signs and symptoms are coming with the chief complaint as
hyper acidity.
[1] Heart Burn
[2] Chest Pain
[3] Gastric discomfort
[4] Abdominal distention

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 39
[5] Sour Belching
[6] Refluxes of the food
[7] Nausea
[8] Loss of Appetite
TREATMENT:
Controlling gastric acidity, hyper motility and spasm and thus relieving the
associated pain. One or more of the following methods may achieve it.
Uses of antacids, or ion exchange resins.
Stimulating the release of cholecystokinin by means of a fatty meal or vegetable oil
Inhibiting gastric acid secretion by drugs.
Withdrawal of stimulants of gastric acid secretion such as alcohol and tobacco etc
Surgical removal of the acid producing gastric mucosa by gasterctomy and
Vagotomy.
All these causes, pathogenesis and symptomatology can be correlated with the
disease named Amlapitta in Ayurvedic Literature. Due to the similarity in causative
factors & signs and symptoms, one can easily correlate these two diseases as a same
disease to some extent. It is not always necessary that each sign & symptoms of the
diseases should be met with each other but the maximum possible findings are suggestive
of the similarity between both the diseases.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 40
Acid peptic disease
Etiopathogenesis – Gastrointestinal problem is one of the most common problems
for which patient seek medical help. Amlapitta can be correlated with wide range of
diseases related to lower oesophagus, stomach and duodenum which are discussed below.
1. Gastro esophageal reflux disease:
GERD is one of the most prevalent gastrointestinal disorders. Reflux occurs
because of sustained or transient decrease in lower oesophageal tone. It may be due to
muscle weakness, myopathy, smoking and smooth muscle relaxant drugs.
Regurgitation of sour material in the mouth and heartburn are the characteristic
symptoms of GERD. Heartburn is produced by the contact of refluxed material with
inflamed or sensitized esophageal mucosa. Angina like or atypical chest pain may occur
in some patients. Severe reflux may reach pharynx and mouth and result in laryngitis,
morning hoarseness and pulmonary aspiration.
Treatment: The goal of treatment is to decrease gastroesophageal reflux, improve
oesophageal clearance and oesophageal mucosa.
• Weight reduction
• Sleeping with the head of bed elevated by about 4-6 inches blocks.
• H2 receptor blockers like Ranitidine 150 mg BD or Famotidine 20 mg BD.
• In resistant cases Proton pump inhibitors like – Omeprazole 20 mg OD or
Pantoprazole 40mg OD.
REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 41
2. Oesophagitis: It is inflammatory disorder of the oesophagus. There is inflammation
of the mucosa of oesophagus and thereafter mucosal damage takes place giving rise to
dyspepsia, odynophagia, chest pain, nausea and vomiting.
3. Hiatus hernia – A Hiatus hernia is a herniation of part of stomach into thoracic cavity
through esophageal hiatus in the diaphragm.
o Sliding hiatus hernia – Here Gastroesophageal junction and fundus of
stomach slides upward.
o Para-oesophageal hernia – Here oesophagogastric junction remains fixed in
its normal location and stomach is herniated beside of gastroesophageal
junction.
Both these hernias present with nausea, vomiting, belching specially on bending
forwards. A herniated gastric pouch may cause dysphagia, develop gastritis or ulcerate
and may lead to acute chest pain and dysphagia.
4. Gastritis – The term gastritis is reserved for histologically documented inflammation
of the gastric mucosa. It is not mere mucosal erythema. The etiological factors leading
to gastritis are broad and heterogenous.
Classification of Gastritis:
a) Acute gastritis –
b) Acute H pylori infection
c) Other acute infectious gastritis-
d) Bacterial (other than H. pylori)

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 42
e) Helicobacterium helmanni
f) Phlegmonus
g) Mycobacterium
h) Syphilitic
i) Viral
j) Parasitic
k) Fungal
l) Chronic atropic gastritis –
m) Type A – Autoimmune – Body predominant
n) Type B – H. Pylori related, Antral predominant
o) Indeterminant
Uncommon forms of gastritis –
a) Lymphocytic
b) Eosinophilic
c) Crohn‟s disease
d) Sarcoidosis
e) Isolated granulomatous gastritis
Acute gastritis:
The common causes with H-pylori induced gastritis are infection e.g. acute
infection with H pylori induced gastritis. Limited mucosal histologic studies demonstrate
a marked infiltrate of neutriphils with oedema and hyperemia. Patients present with
epigastric pain, nausea and vomiting. If not treated, this picture will evolve into one of
chronic gastritis. Hypochlorhydria lasting for upto one year may follow acute H. Pylori

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 43
infection. Bacterial infection of the stomach or phlegmanous gastritis is a rare, potentially
life threatening disorder characterized by marked and diffuse acute inflammatory
infiltrates of the entire gastric wall, at times accompanied by necrosis. Elderly
individuals, alcoholics and AIDS patients may be affected. Organisms associated with
this entity include streptococci, staphylococci, E. coli, proteus and haemophilus.
Chronic gastritis:
Chronic gastritis is identified histologically by inflammatory cell infiltrates
consisting primarily of lymphocytes and plasma cells. Distribution of inflammation may
be patchy, initially involving superficial and glandular portions of the gastric mucosa.
Chronic gastritis has been classified according to histologic characteristics. These include
superficial gastritis and atrophic gastritis.
Superficial gastritis:
The inflammatory changes are limited to the lamina propria of the surface mucosa
with edema and cellular infiltrates. Additional findings may include decreased mucus in
the mucus cells and decreased mitotic fingures in the glandular cells. This is early phase
of chronic gastritis.
Atrophic gastritis:
The next stage is Atrophic gastritis. The inflammatory infiltrates extend deeper
into the mucosa with progressive distortion and destruction of the glands. The final stage
is gastric atrophy. Glandular structures are lost. Endoscopically the mucosa may be
substantially thin, permitting clear visualization of the underlying blood vessels.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 44
Type A - gastritis:
The less common of two form (type A and B) involves primarily the fundus and
body with antral sparing. Traditionally this form of gastritis is associated with pernicious
anaemia in the presence of circulating antibodies against parietal cells and intrinsic factor.
Thus it is also called autoimmune gastritis. Antiparietal cells antibodies are cytotoxic for
gastric mucus cells.
Anti-intrinsic factor antibodies are more specific than parietal cell antibodies for
type A gastritis, being present in approximately 40% of patients. The parietal cell
containing gastric gland preferentially targeted in this form of gastritis and achlorhydria
results. Gastric acid plays an important role in feedback inhibition of gastric release from
G cells. Achlorhydria, coupled with relative sparing of the antral mucosa (site G cells)
leads to hypergastrinemia. The role of gastrin in carcinoid development is well proved.
Type B gastritis:
Type B or antral predominent gastritis is the most common form of chronic
gastritis.H. Pylori infection is the cause of this entity. This form of gastritis increases with
age, being present in up to 100% of people over age 70. Multifocal atrophic gastritis,
gastric atrophy with subsequent metaplasia, has been observed in chronic H. Pylori
induced gastritis. This may ultimately lead to development of gastric adenocarcinoma. H.
Pylori infection is now considered an independent risk factor for gastric cancer.

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 45
Treatment:
All forms of gastritis require mucosal protective agents like sucralfate, misoprostil.
Acid suppressing antagonists are helpful. Proton pump inhibitors are the most potent acid
inhibitory agents available.
For diagnosed H. Pylori infection triple therapy to eradicate H. Pylori is advised.
Failure of therapy with triple therapy is usually due to infection with a resistant organism.
Quadruple therapy in these cases should be the next step.
Peptic Ulcer Disease (PUD):
An ulcer is defined as disruption of the mucosal integrity of the stomach and or
duodenum leading to a local defect or excavation due to active inflammation of > 5 mm
with depth to the submucosa. PUD encompasses both gastric and duodenal ulcers. DU
and GU share many common features in terms of pathogenesis, diagnosis and treatment.
Pathophysiology:
GU tends to occur later in life with a peak incidence reported in sixth decade. In
contrast to duodenal ulcers, gastric ulcers can represent malignancy. Benign GU is most
commonly found distal to the junction between the antrum and the acid secretary mucosa.
In general the antral mucosa extends about 2/3rd
of the distance of lesser curvature and
1/3rd
the way up the greater curvature. Benign GU associated with H. Pylori is associated
with antral gastritis. Gastric acid output (basal and stimulated) tends to normal or
decreased in GU patients when GU develop in the presence of minimal acid levels
impairment of mucosal defense factors may be present. A concomitant increase in

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 46
duodenal gastric reflux has been implicated in some patients. Delayed gastric emptying of
solids has been also been described in GU patients.
Duodenal ulcer occurs often in the first portion of duodenum (>95%) with
approximately 90% located within 3 cm of pylorus. They are usually < 1 cm in diameter.
Ulcers are sharpely demarcated – with depth at time reaching the muscularis propria. The
base of the ulcer often consists of a zone of eosinophilic necrosis with surrounding
fibrosis. Malignant DUs are extremely rare average basal and nocturnal gastric acid
secretion appears to be increased in DU patients as compared to GU. Bicarbonate
secretion is significantly decreased in the duodenal bulk of patients with an active DU, H.
pylori infection may also play a role in this process.
Table 5 - Describe about Aggressive and Protective factors in PUD:
Aggressive factors Protective factors
Increased parietal cell mass with increased Prostaglandin secretion (decreased By
HCL & pepsin. Aspirin, NSAIDs, Cigarette smoking).
Helicobacter pylori infection Bicarbonate secreted by stomach,
Duodenum, Pancreas and Biliary tree.
Tea, coffee in excess Mucus secretion
Irritant food, chillies Blood flow
Alcohol
Rapid mucosal cell
turnover

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 47
Table 6 - Differentiating Chronic Gastric Ulcer from Duodenal Ulcer
Particulars Chronic GU Chronic DU
Age Usually middle aged
Usually young or middle
aged(20-40 Years)
Sex More common in males Males dominating
Characteristics Patient is usually thin and
anemic
Patients are healthy with
steer horn Stomach.
Attacks Usually lasts for several
weeks with intervell of
freedom from 2-6 months
Attack lasts for several
weeks
Usually accuring in spring
or autumn.
Pain Pricking in nature. More severe and
spasmodic.
Investigations: 73
Routine investigations like Haemogram, ESR, urine routine for accessing
general condition of the patient are necessary. A routine stool examination for bowel
diseases, helminthes and occult blood suggesting an ulcer, neoplasm or an
inflammation.
Gastric acid secretory studies – the study consist of passing a Nasogastric tube in a
fasting subject and measuring the amount of resting gastric juice and basal and maximal
acid output (BAO/MAO) after stimulation with secretogogues such as histamine, acid

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 48
phosphate or pentagastrin. Bicarbonate concentration can also be determined. In the past,
these tests were used in diagnosis of achlorhydria, PU and Zollinger – Ellison syndrome
however, with the advent of flexible fibrotic endoscopy and availability of serum gastrin
levels, acid secretary studies are no longer routinely performed.
Manomatry: Abnormality of gastrointestinal motility is an important cause of
gastrointestinal disorder. Oesophageal manomatry is useful in patients with non cardiac
chest pain and dysphagia due to lesions such as Achalasia cardia. Ambulatory 24 hour pH
monitoring of the oesophagus is useful in patients with GERD.
Barium studies: A Barium swallow (oesophagogram) is done to evaluate oesophageal
morphology to assess motility and distensibility and for investigating gastro oesophageal
junction for hiatus hernia or reflux disease. Liquid barium is routinely used but semisolid
or solid boluses may be used. Barium meal examination is done to evaluate the stomach
and duodenum. Upper gastrointestinal series is performed for symptoms related to the
gastro oesophageal junction, stomach and duodenum.
Gastrointestinal Endoscopy:
It includes upper gastrointestinal endoscopy and lower gastro oesophageal
endoscopy. Modern endoscopes are of two types – Fiber optic and Video endoscopy. This
consists of an insertion of tube which is introduced into the patient‟s gastrointestinal tract.
A control unit for viewing as well as controlling the functions of the endoscope and an
umbilical cord which connects with the cold light source. In addition there is a channel in
the endoscope which carries air to distend the lumen and water to clean the lens during
procedures. A separate channel permits suction and allows passage of a variety of
instruments like biopsy forceps, polypectomy smear, cytology brushes and foreign body

REVIEW OF LITERATURE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 49
forceps. A majority of present endoscopes are waterproof and can therefore be fully
immersed in solutions allowing better cleaning and adequate disinfection.
Endoscopic Ultrasonography (EUS): This newer technique provides a much clear
image than conventional abdominal sonography, as imaging is performed through the
gastrointestinal wall and is hence not affected by gas in the bowel. The layers of the gut
wall can easily be identified. It is very useful in the diagnosis of submucosal tumors and
in determining the infiltration and depth of CA in the GI tract.
Treatment:
Before the discovery of H Pylori, the therapy of PUD was centered on the old dictum “No
acid – No Ulcer”. Although acid secretion is still important in the pathogenesis of PUD,
eradication of H Pylori and NSAID induced disease is the mainstay.

MATERIAL & METHODS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 50
MATERIAL
&
METHODS

MATERIAL & METHODS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 51
MATERIALS AND METHODS
The present study was planned as a Survey study and the study was approved by
Institutional Ethics Committee (IEC) prior to the starting of the work.
AIMS AND OBJECTIVES:
To study the effect of Ahara and Vihara in Amlapitta.
Research Question
Is there any effect of Ahara and Vihara in Amlapitta?
Hypothesis
Null Hypothesis: There is no effect of Ahara and Vihara in Amlapitta.
Research Hypothesis: There is effect of Ahara and Vihara in Amlapitta.
METHODOLOGY:
Study design
Cross sectional observational study.
MATERIALS & METHODS:
Source of Data
• Subjects of Amlapitta visiting different OPD and IPD of Sri Dharmasthala
Manjunatheshwara College of Ayurveda and Hospital, Hassan and subjects from
in and around Hassan city.

MATERIAL & METHODS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 52
DIAGNOISTIC CRITERIA:
The patients having Hrit, Kanta Daaha and Tikta and/or Amlodgaara along with
having at least two symptoms among the following list were diagnosed as having
Amlapitta:
• Aruchi
• Shiroruja
• Chardi
• Nausea
METHOD OF COLLECTION OF DATA:
• The subjects were be selected from OPD and IPD of Shree Dharmasthala
manjunatheshwara College of Ayurveda and Hospital and patients in and around
Hassan irrespective of Age , gender and religion .
DURATION OF THE STUDY:
Period of Study: 18 months
Settings
1. Shree Dharmasthala manjunatheshwara College of Ayurveda and Hospital
College of Ayurveda & Hospital, Hassan, Karnataka
2. Subjects from In and Around Hassan, Karnataka
Sample size
345 members out of which 155 are healthy and 196 were diseased.

MATERIAL & METHODS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 53
Recruitment of participants
During the study period, the participants were taken from SDM College of
Ayurveda, Hassan and subjects in and around Hassan satisfying the inclusion criteria. 155
subjects of control group and 196 subjects of case group were selected. An informed
consent was obtained from the participants.
Case Group: The participants in study group were diagnosed cases of Amlapitta .
Control Group: The participants of healthy group were apparently Healthy.
INCLUSION CRITERIA:
• Diagnosed subjects of Amlapitta.
• Individuals of age group between 16 to 60 years.
EXCLUSION CRITERIA:
• Subjects who are not willing to participate.
• Drug induced Amlapitta cases.
• Pregnant women.
• Subjects with Systemic disorders.
PLAN OF STUDY:
After assessing the inclusion/exclusion criteria’s, details were recorded in the
special case
proforma and questionnaires included in the study were filled.
Questionnaire

MATERIAL & METHODS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 54
Self validated questionnaire covering the lifestyle under the four domains of
Ahara and
Vihara. The reliability for the questionnaire has been analyzed via Cronbach’s alpha,
which is 0.97.
DATA ANALYSIS:
Information, lifestyle questionnaire based on Ahara and Vihara were used to
collect the data. The data was tabulated and subjected to statistical analysis with the help
of IBM Statistical Package for Social Sciences v20. Statistical test done includes Chi
Square Test and Odds test.

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 55
OBSERVATIONS
&
RESULTS

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 56
Table 7: AH. How frequently you use garlic in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to garlic who consumed and who did not consume and an association was
found between Amlapitta and Garlic , x2 (1, N=351)=295.537, P=0.000.
In this study those who consume Garlic showed a probable risk of having
Amlapitta 14.355 times (OR) than that of who did not.
Crosstab Risk Estimate
Q1: How frequently you
use garlic in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
155 0
Odds Ratio for presence
of disease (disease present
/ disease absent)
14.3
55 8.098
25.44
7
Expected
Count 75.1 79.9
For cohort How
frequently you use garlic
in a week = yes
6.25
6 4.006 9.769
Absent Count
15 181
For cohort How
frequently you use garlic in a week = no
.436 .357 .533
Expected
Count 94.9 101.1 N of Valid Cases 351
Total Count 170 181
Expected Count
170.0 181.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 295.537a 1 .000
Continuity Correctionb 291.851 1 .000
Likelihood Ratio 380.321 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 294.695 1 .000
N of Valid Cases 351
a. 0 cells (0.0%) have expected count less than 5. The minimum expected count is 75.07.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 57
Table 8: AH. How frequently you use Ginger in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Ginger who consumed and who did not consume and an association
was found between Amlapitta and Ginger , x2 (1, N=351)=282.362, P=0.000.
In this study those who consume Ginger showed a probable risk of having
Amlapitta 12.294 times than that of who did not.
Crosstab Risk Estimate
Q2:How frequently you
use Ginger in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
155 0
Odds Ratio for presence
of disease (disease
present / disease absent)
12.29
4 7.403
20.41
7
Expected
Count 76.8 78.2
For cohort How
frequently you use
ginger in a week = yes 3.477 2.646 4.570
Absent Count
19 177
For cohort How
frequently you use ginger in a week = no
.283 .208 .384
Expected Count
97.2 98.8 N of Valid Cases 351
Total Count 174 177
Expected Count
174.0 177.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 282.362a 1 .000
Continuity Correctionb 278.761 1 .000
Likelihood Ratio 361.788 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 281.558 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 76.84.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 58
Table 9: AH. How frequently you use sour taste food in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Sour taste food who consumed and who did not consume and an
association was found between Amlapitta and Sour taste food , x2 (1,
N=351)=295.465, P=0.000.
In this study those who consume Sour taste food showed a probable risk of having
Amlapitta 713.231 times or than that of who did not.
Crosstab Risk Estimate
Q3: How frequently
you use sour taste food
in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
152 3
Odds Ratio for presence of
disease (disease present /
disease absent)
713.23
1
199.56
3
2549.0
60
Expected
Count 72.9 82.1
For cohort How frequently
you use sour taste food in a week = yes
14.785 8.740 25.012
Absent Count 13 183
For cohort How frequently you use sour taste food in
a week = no
.021 .007 .064
Expected
Count 92.1 103.9 N of Valid Cases 351
Total Count 165 186
Expected
Count 165.0 186.0
Chi-Square Tests
Value Df Asymp. Sig. (2-sided)
Exact Sig. (2-sided)
Exact Sig. (1-sided)
Pearson Chi-Square 290.465a 1 .000
Continuity Correctionb 286.806 1 .000
Likelihood Ratio 360.061 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 289.637 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 72.86. b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 59
Table 10: AH. How frequently you use spoiled food in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Spoiled food who consumed and who did not consume and an
association was found between Amlapitta and Spoiled food , x2 (1,
N=351)=244.102, P=0.000.
In this study those who consume Spoiled food showed a probable risk of having
Amlapitta 129.455 times or than that of who did not.
Crosstab Risk Estimate
Q4: How frequently you
use spoiled food in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
144 11
Odds Ratio for presence
of disease (disease
present / disease absent)
129.45
5 59.248
282.85
3
Expected
Count 71.5 83.5
For cohort How
frequently you use spoiled food in a week =
yes
10.116 6.500 15.745
Absent Count
18 178
For cohort How
frequently you use
spoiled food in a week =
no
.078 .044 .138
Expected
Count 90.5 105.5 N of Valid Cases 351
Total Count 162 189
Expected
Count 162.0 189.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 244.102a 1 .000
Continuity Correctionb 240.745 1 .000
Likelihood Ratio 284.856 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 243.407 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 71.54.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 60
Table 11: AH. How frequently you use spicy food in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Spicy food who consumed and who did not consume and an
association was found between Amlapitta and Spicy food , x2 (1,
N=351)=214.398, P=0.000.
In this study those who consume Spicy food showed a probable risk of having
Amlapitta 298.350 times or than that of who did not.
Crosstab Risk Estimate
Q5: How frequently
you use spicy food
in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
153 2
Odds Ratio for presence of
disease (disease present /
disease absent)
298.3
50 70.862
1256.
141
Expected
Count 85.2 69.8
For cohort How frequently
you use spicy food in a
week = yes
4.837 3.666 6.381
Absent Count
40 156
For cohort How frequently
you use spicy food in a
week = no
.016 .004 .064
Expected
Count 107.8 88.2 N of Valid Cases 351
Total Count 193 158
Expected
Count 193.0 158.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 214.398
a 1 .000
Continuity Correctionb
211.246 1 .000
Likelihood Ratio 263.363 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 213.787 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 69.77.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 61
Table 12: AH. How frequently you use horsegram in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Horse Gram who consumed and who did not consume and an
association was found between Amlapitta and Horse Gram, x2 (1,
N=351)=291.536, P=0.000.
In this study those who consume Horse Gram showed a probable risk of having
Amlapitta 1858.267 times or than that of who did not.
Crosstab Risk Estimate
Q6: How frequently
you use horsegram in
a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
154 1
Odds Ratio for
presence of disease
(disease present /
disease absent)
1858.
267 242.690
14228
.658
Expected
Count 74.6 80.4
For cohort How
frequently you use
horsegram in a week =
yes
12.98
2 7.981
21.11
7
Absent Count
15 181
For cohort How
frequently you use
horsegram in a week =
no
.007 .001 .049
Expected
Count 94.4 101.6 N of Valid Cases 351
Total Count 169 182
Expected
Count 169.0 182.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 291.536
a 1 .000
Continuity Correctionb
287.875 1 .000
Likelihood Ratio 368.104 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 290.705 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 74.63.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 62
Table 13: AH. How frequently you use flour items in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Flour items who consumed and who did not consume and an
association was found between Amlapitta and Flour items, x2 (1,
N=351)=237.923, P=0.000.
In this study those who consume Flour items showed a probable risk of having
Amlapitta 4.828 times or than that of who did not.
Crosstab Risk Estimate
Q7: How frequently
you use flour items in
a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
155 0
Odds Ratio for presence
of disease (disease
present / disease absent)
4.828 2.996 7.780
Expected
Count 83.5 71.5
For cohort How
frequently you use flour
items in a week = yes
1.815 1.516 2.172
Absent Count
34 162
For cohort How
frequently you use flour
items in a week = no
.376 .271 .521
Expected
Count 105.5 90.5 N of Valid Cases 351
Total Count 189 162
Expected
Count 189.0 162.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 237.923
a 1 .000
Continuity Correctionb
234.609 1 .000
Likelihood Ratio 303.663 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 237.245 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 71.54.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 63
Table 14: AH. How frequently you use green chilli in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Green chili who consumed and who did not consume and an
association was found between Amlapitta and Green chili, x2 (1,
N=351)=287.579, P=0.000.
In this study those who consume Green chili showed a probable risk of having
Amlapitta 923.100 times or than that of who did not.
Crosstab Risk Estimate
Q8: How frequently
you use green chilli in
a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
153 2
Odds Ratio for presence
of disease (disease
present / disease absent)
923.1
00
207.82
8
4100.
086
Expected
Count 74.2 80.8
For cohort How
frequently you use green
chilli in a week = yes
12.89
8 7.928
20.98
3
Absent Count
15 181
For cohort How
frequently you use green
chilli in a week = no
.014 .004 .055
Expected
Count 93.8 102.2 N of Valid Cases 351
Total Count 168 183
Expected
Count 168.0 183.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 287.579
a 1 .000
Continuity Correctionb
283.942 1 .000
Likelihood Ratio 358.649 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 286.760 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 74.19.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 64
Table 15: AH. How frequently you use sour curd in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Sour curd who consumed and who did not consume and an association
was found between Amlapitta and Sour curd, x2 (1, N=351)=287.579, P=0.000.
In this study those who consume Sour curd showed a probable risk of having
Amlapitta 923.100 times or than that of who did not.
Crosstab Risk Estimate
Q9: How frequently
you use sour curd in a
week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
154 1
Odds Ratio for presence
of disease (disease
present / disease absent)
1732.
500
227.15
1
1321
3.950
Expected
Count 75.1 79.9
For cohort How
frequently you use sour
curd in a week = yes
12.17
1 7.609
19.46
8
Absent Count
16 180
For cohort How
frequently you use sour
curd in a week = no
.007 .001 .050
Expected
Count 94.9 101.1 N of Valid Cases 351
Total Count 170 181
Expected
Count 170.0 181.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 288.189
a 1 .000
Continuity Correctionb
284.549 1 .000
Likelihood Ratio 363.331 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 287.368 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 75.07.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 65
Table 16: AH. How frequently you use red chilli in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Red chili who consumed and who did not consume and an association
was found between Amlapitta and Red chili, x2 (1, N=351)=252.860, P=0.000.
In this study those who consume Red chili showed a probable risk of having
Amlapitta 500.192 times or than that of who did not.
Crosstab Risk Estimate
Q10: How frequently
you use red chilli in a
week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
153 2
Odds Ratio for presence
of disease (disease
present / disease absent)
500.1
92
116.77
9
2142.
445
Expected
Count 79.0 76.0
For cohort How
frequently you use red
chilli in a week = yes
7.441 5.200 10.64
9
Absent Count
26 170
For cohort How
frequently you use red
chilli in a week = no
.015 .004 .059
Expected
Count 100.0 96.0 N of Valid Cases 351
Total Count 179 172
Expected
Count 179.0 172.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 252.860
a 1 .000
Continuity Correctionb
249.453 1 .000
Likelihood Ratio 311.646 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 252.140 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 75.95.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 66
Table 17: AH. How frequently you use new jaggary in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to New Jaggery who consumed and who did not consume and an
association was found between Amlapitta and New Jaggery, x2 (1,
N=351)=271.250, P=0.000.
In this study those who consume New Jaggery showed a probable risk of having
Amlapitta 673.200 times or than that of who did not.
Crosstab Risk Estimate
Q11: How frequently
you use new jaggary in
a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
153 2
Odds Ratio for presence
of disease (disease
present / disease absent)
673.2
00
154.84
7
2926.
746
Expected
Count 76.4 78.6
For cohort How
frequently you use new
jaggary in a week = yes
9.674 6.383 14.65
9
Absent Count
20 176
For cohort How
frequently you use new
jaggary in a week = no
.014 .004 .057
Expected
Count 96.6 99.4 N of Valid Cases 351
Total Count 173 178
Expected
Count 173.0 178.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 271.250
a 1 .000
Continuity Correctionb
267.721 1 .000
Likelihood Ratio 335.962 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 270.478 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 76.40.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 67
Table 18: AH. How frequently you use salty food in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Salty food who consumed and who did not consume and an association
was found between Amlapitta and Salty food, x2 (1, N=351)=210.645, P=0.000.
In this study those who consume Red chili showed a probable risk of having
Amlapitta 197.600 times or than that of who did not.
Crosstab Risk Estimate
Q12: How frequently
you use salty food in
a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
152 3
Odds Ratio for presence of
disease (disease present /
disease absent)
197.6
00 59.854
652.3
45
Expected
Count 84.8 70.2
For cohort How frequently
you use salty food in a
week = yes
4.805 3.641 6.341
Absent Count
40 156
For cohort How frequently
you use salty food in a
week = no
.024 .008 .075
Expected
Count 107.2 88.8 N of Valid Cases 351
Total Count 192 159
Expected
Count 192.0 159.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 210.645
a 1 .000
Continuity Correctionb
207.522 1 .000
Likelihood Ratio 255.516 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 210.045 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 70.21.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 68
Table 19: AH. How frequently you use domestic meat with honey in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Domestic meat with honey who consumed and who did not consume
and an association was found between Amlapitta and Domestic meat with honey,
x2 (1, N=351)=243.321, P=0.000.
In this study those who consume Domestic meat with honey showed a probable
risk of having Amlapitta 121.529 times or than that of who did not.
Crosstab Risk Estimate
Q13: How
frequently you use
domestic meat with
honey in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
141 14
Odds Ratio for presence of
disease (disease present /
disease absent)
121.5
29 56.784
260.0
93
Expected
Count 68.9 86.1
For cohort How frequently
you use domestic meat
with honey in a week =
yes
11.88
6 7.290
19.38
0
Absent Count
15 181
For cohort How frequently
you use domestic meat
with honey in a week = no
.098 .059 .161
Expected
Count 87.1 108.9 N of Valid Cases 351
Total Count 156 195
Expected
Count 156.0 195.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 243.321
a 1 .000
Continuity Correctionb
239.958 1 .000
Likelihood Ratio 282.306 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 242.627 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.89.
b. Computed only for a 2x2 table
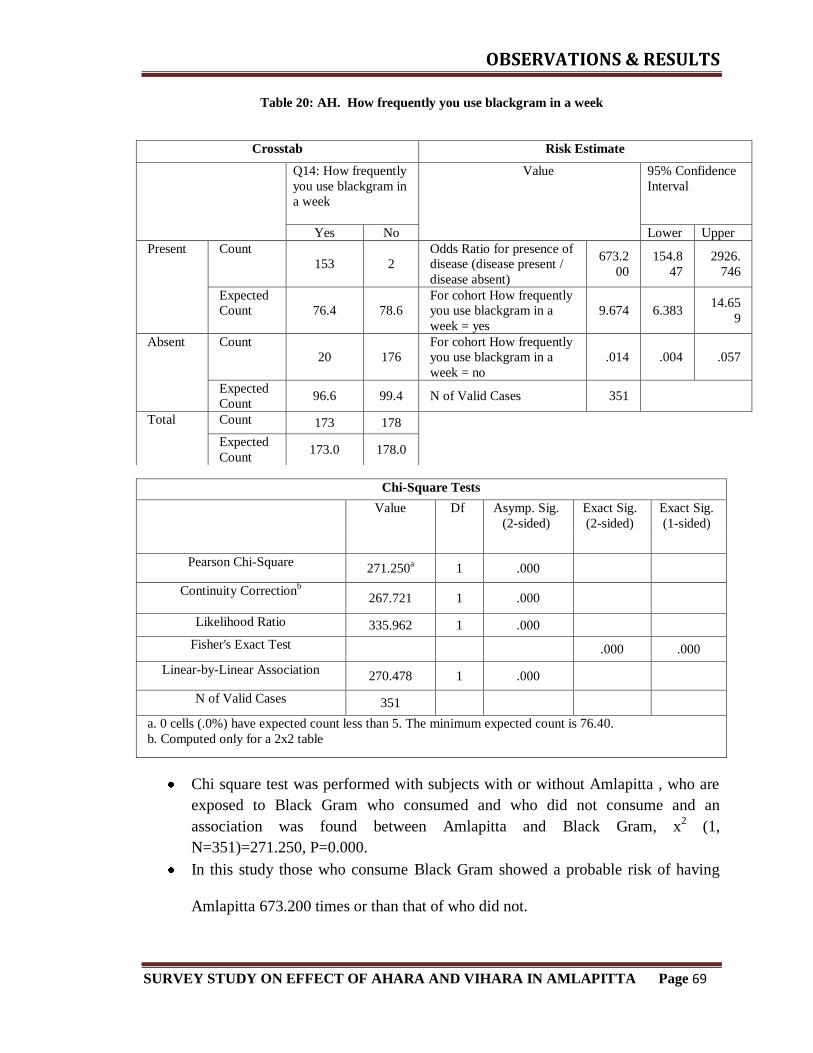
OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 69
Table 20: AH. How frequently you use blackgram in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Black Gram who consumed and who did not consume and an
association was found between Amlapitta and Black Gram, x2 (1,
N=351)=271.250, P=0.000.
In this study those who consume Black Gram showed a probable risk of having
Amlapitta 673.200 times or than that of who did not.
Crosstab Risk Estimate
Q14: How frequently
you use blackgram in
a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
153 2
Odds Ratio for presence of
disease (disease present /
disease absent)
673.2
00
154.8
47
2926.
746
Expected
Count 76.4 78.6
For cohort How frequently
you use blackgram in a
week = yes
9.674 6.383 14.65
9
Absent Count
20 176
For cohort How frequently
you use blackgram in a
week = no
.014 .004 .057
Expected
Count 96.6 99.4 N of Valid Cases 351
Total Count 173 178
Expected
Count 173.0 178.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 271.250
a 1 .000
Continuity Correctionb
267.721 1 .000
Likelihood Ratio 335.962 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 270.478 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 76.40.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 70
Table 21: AH. How frequently you use pickle in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Pickle who consumed and who did not consume and an association
was found between Amlapitta and Pickle, x2 (1, N=351)=222.061, P=0.000.
In this study those who consume Pickle showed a probable risk of having
Amlapitta 5.638 times or than that of who did not.
Crosstab Risk Estimate
Q15: How frequently
you use pickle in a
week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
155 0
Odds Ratio for presence of
disease (disease present /
disease absent)
5.638 3.554 8.943
Expected
Count 86.1 68.9
For cohort How frequently
you use pickle in a week =
yes
2.376 1.871 3.018
Absent Count
40 156
For cohort How frequently
you use pickle in a week =
no
.422 .325 .546
Expected
Count 108.9 87.1 N of Valid Cases 351
Total Count 195 156
Expected
Count 195.0 156.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 222.061
a 1 .000
Continuity Correctionb
218.849 1 .000
Likelihood Ratio 283.892 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 221.429 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.89.
b. Computed only for a 2x2 table
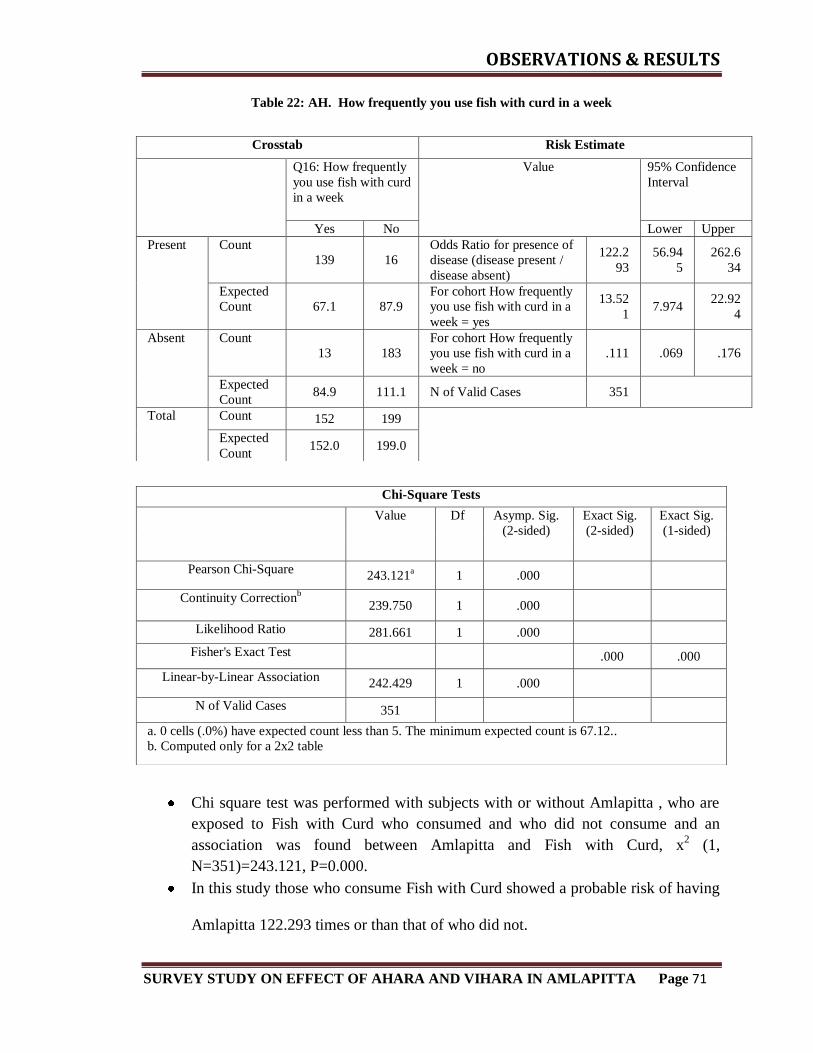
OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 71
Table 22: AH. How frequently you use fish with curd in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Fish with Curd who consumed and who did not consume and an
association was found between Amlapitta and Fish with Curd, x2 (1,
N=351)=243.121, P=0.000.
In this study those who consume Fish with Curd showed a probable risk of having
Amlapitta 122.293 times or than that of who did not.
Crosstab Risk Estimate
Q16: How frequently
you use fish with curd
in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
139 16
Odds Ratio for presence of
disease (disease present /
disease absent)
122.2
93
56.94
5
262.6
34
Expected
Count 67.1 87.9
For cohort How frequently
you use fish with curd in a
week = yes
13.52
1 7.974
22.92
4
Absent Count
13 183
For cohort How frequently
you use fish with curd in a
week = no
.111 .069 .176
Expected
Count 84.9 111.1 N of Valid Cases 351
Total Count 152 199
Expected
Count 152.0 199.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 243.121
a 1 .000
Continuity Correctionb
239.750 1 .000
Likelihood Ratio 281.661 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 242.429 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 67.12..
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 72
Table 23: AH. How frequently you use fish with milk in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Fish with Milk who consumed and who did not consume and an
association was found between Amlapitta and Fish with Milk, x2 (1,
N=351)=229.780, P=0.000.
In this study those who consume Fish with Milk showed a probable risk of having
Amlapitta 91.841 times or than that of who did not.
Crosstab Risk Estimate
Q17: How frequently
you use fish with
milk in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
137 18
Odds Ratio for presence of
disease (disease present /
disease absent)
91.84
1
44.69
2
188.7
30
Expected
Count 67.1 87.9
For cohort How frequently
you use fish with milk in a
week = yes
11.54
9 7.078
18.84
5
Absent Count
15 181
For cohort How frequently
you use fish with milk in a
week = no
.126 .081 .195
Expected
Count 84.9 111.1 N of Valid Cases 351
Total Count 152 199
Expected
Count 152.0 199.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 229.780
a 1 .000
Continuity Correctionb
226.503 1 .000
Likelihood Ratio 263.020 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 229.125 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 67.12.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 73
Table 24: AH. How frequently you use horsegram with curd in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Horse gram with Curd who consumed and who did not consume and
an association was found between Amlapitta and Horse Gram with curd, x2 (1,
N=351)=300.237, P=0.000.
In this study those who consume Horse Gram with Curd showed a probable risk of
having Amlapitta 669.524 times or than that of who did not.
Crosstab Risk Estimate
Q18:How frequently
you use horsegram
with curd in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
148 7
Odds Ratio for presence of
disease (disease present /
disease absent)
669.5
24
220.3
40
2034.
410
Expected
Count 68.0 87.0
For cohort How frequently
you use horsegram with
curd in a week = yes
31.19
1
14.17
7
68.62
8
Absent Count
6 190
For cohort How frequently
you use horsegram with
curd in a week = no
.047 .023 .096
Expected
Count 86.0 110.0 N of Valid Cases 351
Total Count 154 197
Expected
Count 154.0 197.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 300.237
a 1 .000
Continuity Correctionb
296.496 1 .000
Likelihood Ratio 370.613 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 299.382 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.01.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 74
Table 25: AH. How frequently you use milk with raddish in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Milk with Raddish who consumed and who did not consume and an
association was found between Amlapitta and Milk with Raddish, x2 (1,
N=351)=307.791, P=0.000.
In this study those who consume Milk with Raddish showed a probable risk of
having Amlapitta 948.633times or than that of who did not.
Crosstab Risk Estimate
Q19: How frequently
you use milk with
raddish in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
149 6
Odds Ratio for presence of
disease (disease present /
disease absent)
948.6
33
284.0
15
3168.
518
Expected
Count 68.0 87.0
For cohort How frequently
you use milk with raddish
in a week = yes
37.68
3
15.85
3
89.57
2
Absent Count
5 191
For cohort How frequently
you use milk with raddish
in a week = no
.040 .018 .087
Expected
Count 86.0 110.0 N of Valid Cases 351
Total Count 154 197
Expected
Count 154.0 197.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 307.791
a 1 .000
Continuity Correctionb
304.002 1 .000
Likelihood Ratio 383.965 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 306.914 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.01.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 75
Table 26: AH. How frequently you use salt with milk in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Salt with Milk who consumed and who did not consume and an
association was found between Amlapitta and Salt with milk, x2 (1,
N=351)=289.113, P=0.000.
In this study those who consume Salt with Milk showed a probable risk of having
Amlapitta 431.813 times or than that of who did not.
Crosstab Risk Estimate
Q20: How frequently
you use salt with
milk in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
147 8
Odds Ratio for presence of
disease (disease present /
disease absent)
431.8
13
158.3
06
1177.
855
Expected
Count 68.4 86.6
For cohort How frequently
you use salt with milk in
a week = yes
23.23
5
11.77
6
45.84
8
Absent Count
8 188
For cohort How frequently
you use salt with milk in
a week = no
.054 .027 .106
Expected
Count 86.6 109.4 N of Valid Cases 351
Total Count 155 196
Expected
Count 155.0 196.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 289.113
a 1 .000
Continuity Correctionb
285.445 1 .000
Likelihood Ratio 351.938 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 288.290 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.45.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 76
Table 27: AH. How frequently you use pork with curd in a week
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Pork with Curd who consumed and who did not consume and an
association was found between Amlapitta and Pork with Curd, x2 (1,
N=351)=244.943, P=0.000.
In this study those who consume Pork with Curd showed a probable risk of having
Amlapitta 142.756 times or than that of who did not.
Crosstab Risk Estimate
Q21:How frequently
you use pork with
curd in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
146 9
Odds Ratio for presence of
disease (disease present /
disease absent)
142.7
56
63.08
0
323.0
67
Expected
Count 73.3 81.7
For cohort How frequently
you use pork with curd in
a week = yes
9.231 6.083 14.00
9
Absent Count
20 176
For cohort How frequently
you use pork with curd in
a week = no
.065 .034 .122
Expected
Count 92.7 103.3 N of Valid Cases 351
Total Count 166 185
Expected
Count 166.0 185.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 244.943
a 1 .000
Continuity Correctionb
241.585 1 .000
Likelihood Ratio 287.680 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 244.245 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 73.30.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 77
Table 28: AH. How frequently you use Sour fruits with Milk in a week
Chi square test was performed with subjects with or without Amlapitta , who are exposed to Sour
fruit with Milk who consumed and who did not consume and an association was found between
Amlapitta and Sour fruit with milk, x2 (1, N=351)=274.712, P=0.000.
In this study those who consume Sour fruit with Milk showed a probable risk of having Amlapitta
272.828 times or than that of who did not.
Crosstab Risk Estimate
Q22: How frequently
you use Sour fruits
with Milk in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
146 9
Odds Ratio for presence of
disease (disease present /
disease absent)
272.8
28
110.1
21
675.9
42
Expected
Count 69.3 85.7
For cohort How
frequently you use Sour
fruits with Milk in a week
= yes
16.78
4 9.440
29.84
0
Absent Count
11 185
For cohort How
frequently you use Sour
fruits with Milk in a week
= no
.062 .033 .116
Expected
Count 87.7 108.3 N of Valid Cases 351
Total Count 157 194
Expected
Count 157.0 194.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 274.712
a 1 .000
Continuity Correctionb
271.141 1 .000
Likelihood Ratio 329.248 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 273.929 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 69.33.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 78
Table 29: AH. How frequently you use Leafy Vegetable with Butter in a week
Chi square test was performed with subjects with or without Amlapitta , who are exposed to Leafy
vegetables with butter who consumed and who did not consume and an association was found
between Amlapitta and Leafy vegetables with butter, x2 (1, N=351)=282.748, P=0.000.
In this study those who consume Leafy vegetables with butter showed a probable risk of having
Amlapitta 422.308 times or than that of who did not.
Crosstab Risk Estimate
Q23: How frequently
you use Leafy
Vegetable with Butter
in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
150 5
Odds Ratio for presence of
disease (disease present /
disease absent)
422.3
08
147.2
28
1211.
343
Expected
Count 72.0 83.0
For cohort How frequently
you use Leafy Vegetable
with Butter in a week =
yes
14.59
1 8.622
24.69
1
Absent Count
13 183
For cohort How frequently
you use Leafy Vegetable
with Butter in a week =
no
.035 .015 .082
Expected
Count 91.0 105.0 N of Valid Cases 351
Total Count 163 188
Expected
Count 163.0 188.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 282.748
a 1 .000
Continuity Correctionb
279.135 1 .000
Likelihood Ratio 344.970 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 281.942 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 71.98.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 79
Table 30: AH. How frequently you use Banana with Curd in a week
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
Banana with curd who consumed and who did not consume and an association was found between
Amlapitta and Banana with curd, x2 (1, N=351)=267.593, P=0.000.
In this study those who consume Banana with Curd showed a probable risk of having Amlapitta
222.333 times or than that of who did not.
Crosstab Risk Estimate
Q24: How frequently
you use Banana with
Curd in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
145 10
Odds Ratio for presence of
disease (disease present /
disease absent)
222.3
33
93.43
0
529.0
85
Expected
Count 69.3 85.7
For cohort How
frequently you use Banana
with Curd in a week = yes
15.28
0 8.818
26.47
7
Absent Count
12 184
For cohort How
frequently you use Banana
with Curd in a week = no
.069 .038 .125
Expected
Count 87.7 108.3 N of Valid Cases 351
Total Count 157 194
Expected
Count 157.0 194.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 267.593
a 1 .000
Continuity Correctionb
264.068 1 .000
Likelihood Ratio 318.238 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 266.830 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 69.33.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 80
Table 31: AH. How frequently you use Aerated Drinks in a week
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
Aerated drinks who consumed and who did not consume and an association was found between
Amlapitta and Aerated drinks, x2 (1, N=351)=289.113, P=0.000.
In this study those who consume Aerated drinks showed a probable risk of having Amlapitta
431.831 times or than that of who did not.
Crosstab Risk Estimate
Q25: How
frequently you
useAerated Drinks
in a week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
147 8
Odds Ratio for presence of
disease (disease present /
disease absent)
431.8
13
158.3
06
1177.
855
Expected
Count 68.4 86.6
For cohort. How
frequently you use Aerated
Drinks in a week = yes
23.23
5
11.77
6
45.84
8
Absent Count
8 188
For cohort. How
frequently you use Aerated
Drinks in a week = no
.054 .027 .106
Expected
Count 86.6 109.4 N of Valid Cases 351
Total Count 155 196
Expected
Count 155.0 196.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 289.113
a 1 .000
Continuity Correctionb
285.445 1 .000
Likelihood Ratio 351.938 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 288.290 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.45.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 81
Table 32: AH. How frequently you use heated curd preparations in a week
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
Heated curd preparations who consumed and who did not consume and an association was found
between Amlapitta and Heated curd Preparations, x2 (1, N=351)=241.834, P=0.000.
In this study those who consume heated curd preparations showed a probable risk of having
Amlapitta 135.185 times or than that of who did not.
Crosstab Risk Estimate
Q26: How
frequently you use
Heated curd
preparations in a
week
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
146 9
Odds Ratio for presence of
disease (disease present /
disease absent)
135.
185
60.06
7
304.2
44
Expected
Count 73.7 81.3
For cohort How frequently
you use Heated curd
preparations in a week = yes
8.79
1 5.858
13.19
4
Absent Count
21 175
For cohort How frequently
you use Heated curd
preparations in a week = no
.065 .034 .123
Expected
Count 93.3
102.
7 N of Valid Cases 351
Total Count 167 184
Expected
Count 167.0
184.
0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 241.834
a 1 .000
Continuity Correctionb
238.499 1 .000
Likelihood Ratio 283.591 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 241.145 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 73.75.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 82
Table 33: VH. Do you have the habit of eating food irrespective of hunger
Chi square test was performed with subjects with or without Amlapitta , who are exposed to eating
food irrespective hunger who consumed and who did not consume and an association was found
between Amlapitta and eating food irrespective hunger, x2 (1, N=351)=132.799, P=0.000.
In this study those who consume eating food irrespective hunger showed a probable risk of having
Amlapitta 23.963 times or than that of who did not.
Crosstab Risk Estimate
Q27: Do you have the
habit of eating food
irrespective of hunger
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
141 14
Odds Ratio for presence of
disease (disease present /
disease absent)
23.96
3
12.77
5
44.95
1
Expected
Count 87.9 67.1
For cohort Do you have
the habit of eating food
irrespective of hunger =
yes
3.074 2.463 3.837
Absent Count
58 138
For cohort Do you have
the habit of eating food
irrespective of hunger = no
.128 .077 .213
Expected
Count 111.1 84.9 N of Valid Cases 351
Total Count 199 152
Expected
Count 199.0 152.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 132.799
a 1 .000
Continuity Correctionb
130.311 1 .000
Likelihood Ratio 148.171 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 132.420 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 67.12.
b. Computed only for a 2x2 table
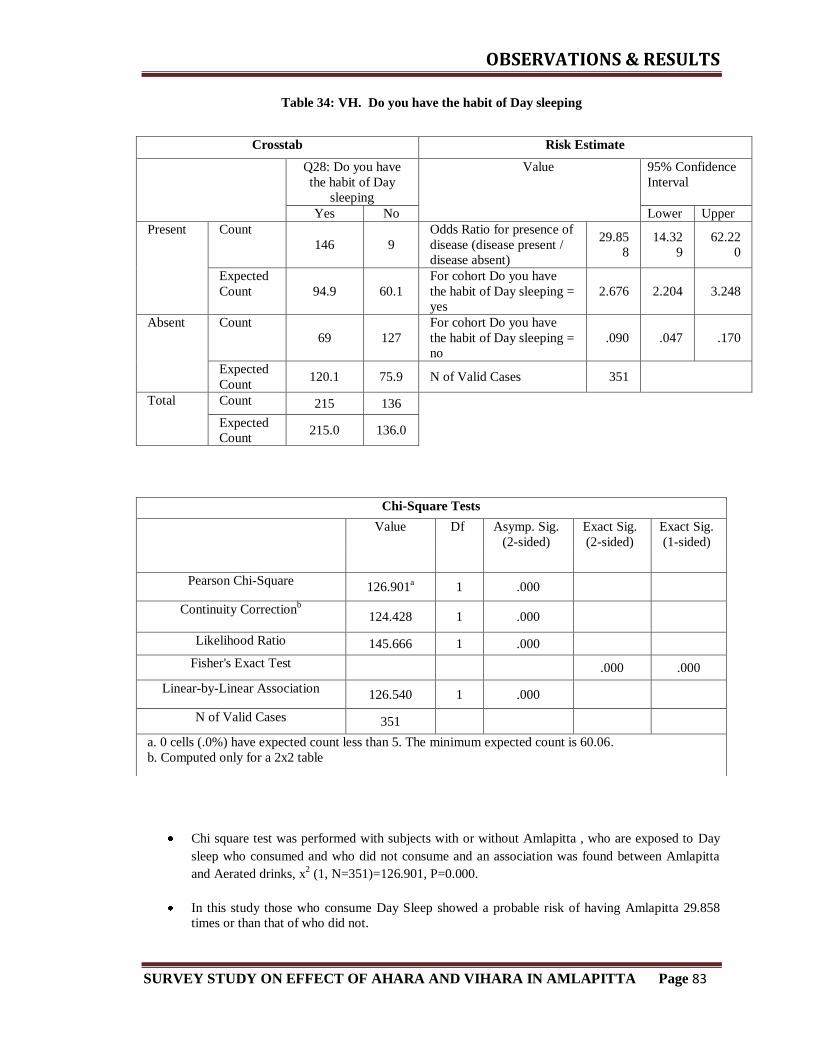
OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 83
Table 34: VH. Do you have the habit of Day sleeping
Chi square test was performed with subjects with or without Amlapitta , who are exposed to Day
sleep who consumed and who did not consume and an association was found between Amlapitta
and Aerated drinks, x2 (1, N=351)=126.901, P=0.000.
In this study those who consume Day Sleep showed a probable risk of having Amlapitta 29.858
times or than that of who did not.
Crosstab Risk Estimate
Q28: Do you have
the habit of Day
sleeping
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
146 9
Odds Ratio for presence of
disease (disease present /
disease absent)
29.85
8
14.32
9
62.22
0
Expected
Count 94.9 60.1
For cohort Do you have
the habit of Day sleeping =
yes
2.676 2.204 3.248
Absent Count
69 127
For cohort Do you have
the habit of Day sleeping =
no
.090 .047 .170
Expected
Count 120.1 75.9 N of Valid Cases 351
Total Count 215 136
Expected
Count 215.0 136.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 126.901
a 1 .000
Continuity Correctionb
124.428 1 .000
Likelihood Ratio 145.666 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 126.540 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 60.06.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 84
Table 35: VH. Do you have the habit of Alcohol Consumption
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
Alcohol who consumed and who did not consume and an association was found between
Amlapitta and Alcohol, x2 (1, N=351)=131.483, P=0.000.
In this study those who consume Alcohol showed a probable risk of having Amlapitta 18.975times
or than that of who did not.
Crosstab Risk Estimate
Q29: Do you have
the habit ofAlchohol
Consumption
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
111 44
Odds Ratio for presence of
disease (disease present /
disease absent)
18.97
5
10.86
3
33.14
6
Expected
Count 59.2 95.8
For cohort Do you have
the habit of Alcohol
Consumption = yes
6.103 4.105 9.073
Absent Count
23 173
For cohort Do you have
the habit of Alcohol
Consumption = no
.322 .249 .415
Expected
Count 74.8 121.2 N of Valid Cases 351
Total Count 134 217
Expected
Count 134.0 217.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 131.483
a 1 .000
Continuity Correctionb
128.958 1 .000
Likelihood Ratio 140.089 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 131.108 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 59.17.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 85
Table 36: VH. Do you have the habit of Smoking
Chi square test was performed with subjects with or without Amlapitta, who are exposed to
Smoking and who did not consume and an association was found between Amlapitta and
Smoking, x2 (1, N=351)=102.932, P=0.000.
In this study those who consume Smoking showed a probable risk of having Amlapitta 14.355
times or than that of who did not.
Crosstab Risk Estimate
Q30: Do you have the
habit of Smoking
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
94 61
Odds Ratio for presence of
disease (disease present /
disease absent)
14.35
5 8.098
25.44
7
Expected
Count 49.9 105.1
For cohort .Do you have
the habit of Smoking = yes 6.256 4.006 9.769
Absent Count 19 177
For cohort .Do you have
the habit of Smoking = no .436 .357 .533
Expected
Count 63.1 132.9 N of Valid Cases 351
Total Count 113 238
Expected
Count 113.0 238.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 102.932
a 1 .000
Continuity Correctionb
100.611 1 .000
Likelihood Ratio 108.510 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 102.639 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 49.90.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 86
Table 37: VH. Do you have the habit of excess intake of tea or coffee
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
Excess coffee or tea and who did not consume and an association was found between Amlapitta
and excess coffee or tea, x2 (1, N=351)=117.501, P=0.000.
In this study those who consume excess coffee or tea showed a probable risk of having Amlapitta
14.205 times or than that of who did not.
Crosstab Risk Estimate
Q31: Do you have the
habit of excess intake
of tea or coffee
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
119 36
Odds Ratio for presence of
disease (disease present /
disease absent)
14.20
5 8.473
23.81
4
Expected
Count 68.9 86.1
For cohort Do you have
the habit of excess intake
of tea or coffee = yes
4.067 3.004 5.506
Absent Count
37 159
For cohort Do you have
the habit of excess intake
of tea or coffee = no
.286 .213 .384
Expected
Count 87.1 108.9 N of Valid Cases 351
Total Count 156 195
Expected
Count 156.0 195.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 117.501
a 1 .000
Continuity Correctionb
115.168 1 .000
Likelihood Ratio 124.329 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 117.166 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.89.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 87
Table 38: VH. Do you have the habit of Skipping Meals
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
Skipping meals and who did not consume and an association was found between Amlapitta and
Aerated drinks, x2 (1, N=351)=75.060, P=0.000.
In this study those who consume Skip Meals showed a probable risk of having Amlapitta 7.502
times or than that of who did not.
Crosstab Risk Estimate
Q32:Do you have
the habit of skipping
Meals
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
114 41
Odds Ratio for presence of
disease (disease present /
disease absent)
7.502 4.660 12.07
8
Expected
Count 73.7 81.3
For cohort Do you have
the habit of Skipping
Meals = yes
2.720 2.121 3.487
Absent Count
53 143
For cohort Do you have
the habit of Skipping
Meals = no
.363 .275 .478
Expected
Count 93.3 102.7 N of Valid Cases 351
Total Count 167 184
Expected
Count 167.0 184.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 75.060
a 1 .000
Continuity Correctionb
73.207 1 .000
Likelihood Ratio 77.874 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 74.846 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 73.75.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 88
Table 39: VH. Do you have the habit of drinking excess water soon after meals
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
drinking excess water soon after food and who did not consume and an association was found
between Amlapitta and drinking excess water after food, x2 (1, N=351)=44.684, P=0.000.
In this study those who consume excess water soon after food showed a probable risk of having
Amlapitta 4.828 times or than that of who did not.
Crosstab Risk Estimate
Q33: Do you have the
habit of drinking excess
water soon after meals
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
122 33
Odds Ratio for presence
of disease (disease
present / disease absent)
4.828 2.996 7.780
Expected
Count 91.4 63.6
For cohort Do you have
the habit of drinking
excess water soon after
meals = yes
1.815 1.516 2.172
Absent Count
85 111
For cohort Do you have
the habit of drinking
excess water soon after
meals = no
.376 .271 .521
Expected
Count 115.6 80.4 N of Valid Cases 351
Total Count 207 144
Expected
Count 207.0 144.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 44.684
a 1 .000
Continuity Correctionb
43.235 1 .000
Likelihood Ratio 46.454 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 44.557 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 63.59.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 89
Table 40: VH..Do you have the habit of eating Betalnut Leaf with Tobbaco
Chi square test was performed with subjects with or without Amlapitta , who are exposed to who
consumed betel nut with tobacco and who did not consume and an association was found between
Amlapitta and eating betel nut with tobacco, x2 (1, N=351)=80.286, P=0.000.
In this study those who consume Betel nut with tobacco showed a probable risk of having
Amlapitta 8.174 times or than that of who did not.
Crosstab Risk Estimate
Q34: Do you have the
habit of eating
Betalnut Leaf with
Tobbaco
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
107 48
Odds Ratio for presence of
disease (disease present /
disease absent)
8.174 5.048 13.23
6
Expected
Count 65.8 89.2
For cohort .Do you have
the habit of eating Betalnut
Leaf with Tobbaco = yes
3.222 2.415 4.297
Absent Count
42 154
For cohort .Do you have
the habit of eating Betalnut
Leaf with Tobbaco = no
.394 .308 .504
Expected
Count 83.2 112.8 N of Valid Cases 351
Total Count 149 202
Expected
Count 149.0 202.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 80.286
a 1 .000
Continuity Correctionb
78.349 1 .000
Likelihood Ratio 83.039 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 80.057 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 65.80.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 90
Table 41: VH. Do you have the habit of Adding extra salt and spice for the food you eat
Chi square test was performed with subjects with or without Amlapitta , who are exposed to who consumed excess salt and spice above food and who did not
consume and an association was found between Amlapitta and excess extra spice
and salt above food, x2 (1, N=351)=107.471, P=0.000.
In this study those who consume excess salt and spice with food showed a
probable risk of having Amlapitta 12.294 times or than that of who did not.
Crosstab Risk Estimate
Q35: Do you have the
habit of Adding extra
salt and spice for the
food you eat
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
121 34
Odds Ratio for presence
of disease (disease
present / disease absent)
12.29
4 7.403
20.41
7
Expected
Count 72.9 82.1
For cohort .Do you have
the habit of Adding extra
salt and spice for the food
you eat = yes
3.477 2.646 4.570
Absent Count
44 152
For cohort .Do you have
the habit of Adding extra
salt and spice for the food
you eat = no
.283 .208 .384
Expected
Count 92.1 103.9 N of Valid Cases 351
Total Count 165 186
Expected
Count 165.0 186.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 107.471
a 1 .000
Continuity Correctionb
105.250 1 .000
Likelihood Ratio 113.492 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 107.165 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 72.86.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 91
Table 42: VH. Do you work in too hot atmosphere
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to hot atmosphere and who did not consume and an association was
found between Amlapitta and exposure to excess hot atmosphere, x2 (1,
N=351)=117.501, P=0.000.
In this study those who consume excess hot atmosphere showed a probable risk of
having Amlapitta 14.205 times or than that of who did not.
Crosstab Risk Estimate
Q36:Do you work in
too hot atmosphere
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
119 36
Odds Ratio for presence of
disease (disease present /
disease absent)
14.20
5 8.473
23.81
4
Expected
Count 68.9 86.1
For cohort .Do you work
in too hot atmosphere =
yes
4.067 3.004 5.506
Absent Count 37 159
For cohort .Do you work
in too hot atmosphere = no .286 .213 .384
Expected
Count 87.1 108.9 N of Valid Cases 351
Total Count 156 195
Expected
Count 156.0 195.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 117.501
a 1 .000
Continuity Correctionb
115.168 1 .000
Likelihood Ratio 124.329 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 117.166 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.89
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 92
Table 43: VH. Do you have the habit of Bathing soon after having food
Chi square test was performed with subjects with or without Amlapitta, who are exposed to Bathing soon after food and who did not consume and an association
was found between Amlapitta and Bathing soon after food, x2 (1,
N=351)=141.718, P=0.000.
In this study those who Bath soon after food showed a probable risk of having
Amlapitta 20.457 times or than that of who did not.
Crosstab Risk Estimate
Q37: Do you have the
habit of Bathing soon
after having food
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
122 33
Odds Ratio for presence of
disease (disease present /
disease absent)
20.45
7
11.83
9
35.34
6
Expected
Count 67.1 87.9
For cohort Do you have
the habit of Bathing soon
after having food = yes
5.142 3.663 7.220
Absent Count
30 166
For cohort Do you have
the habit of Bathing soon
after having food = no
.251 .185 .342
Expected
Count 84.9 111.1 N of Valid Cases 351
Total Count 152 199
Expected
Count 152.0 199.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 141.718
a 1 .000
Continuity Correctionb
139.147 1 .000
Likelihood Ratio 151.997 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 141.314 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 67.12.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 93
Table 44: VH. Do you have the habit of Suppressing Natural Urges
Chi square test was performed with subjects with or without Amlapitta , who are exposed to Suppression of natural urges and who did not and an association was
found between Amlapitta and Suppressing natural urges, x2 (1, N=351)=149.654,
P=0.000.
In this study those who suppress a natural urges showed a probable risk of having Amlapitta 23.034 times or than that of who did not.
Crosstab Risk Estimate
Q38: Do you have the
habit of Suppressing
Natural Urges
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
124 31
Odds Ratio for presence of
disease (disease present /
disease absent)
23.03
4
13.19
6
40.20
9
Expected
Count 67.6 87.4
For cohort Do you have
the habit of Suppressing
Natural Urges = yes
5.407 3.829 7.635
Absent Count
29 167
For cohort Do you have
the habit of Suppressing
Natural Urges = no
.235 .170 .323
Expected
Count 85.4 110.6 N of Valid Cases 351
Total Count 153 198
Expected
Count 153.0 198.0
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 149.654
a 1 .000
Continuity Correctionb
147.014 1 .000
Likelihood Ratio 161.372 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 149.227 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 67.56.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 94
Table 45: VH. Do you have the habit of sleeping soon after having food
Chi square test was performed with subjects with or without Amlapitta , who are exposed to
sleeping soon after food and who did not consume and an association was found between
Amlapitta and sleeping soon after food, x2 (1, N=351)=57.571, P=0.000.
In this study those who sleep soon after food showed a probable risk of having Amlapitta
5.638times or than that of who did not.
Crosstab Risk Estimate
Q39:Do you have the
habit of sleeping soon
after having food
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
109 46
Odds Ratio for presence of
disease (disease present /
disease absent)
5.638 3.554 8.943
Expected
Count 73.7 81.3
For cohort Do you have
the habit of sleeping soon
after having food = yes
2.376 1.871 3.018
Absent Count
58 138
For cohort Do you have
the habit of sleeping soon
after having food = no
.422 .325 .546
Expected
Count 93.3 102.7 N of Valid Cases 351
Total Count 167 184
Expected
Count 167.0 184.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 57.571
a 1 .000
Continuity Correctionb
55.950 1 .000
Likelihood Ratio 59.165 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 57.407 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 73.75.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 95
Table 46: VH. Do you have the habit of Excess Bath or Tub Bath
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to excess bath or tub bath and who did not and an association was found
between Amlapitta and excess bath or tub bath, x2 (1, N=351)=54.220, P=0.000.
In this study those who excess bath or tub bath showed a probable risk of having
Amlapitta 5.329 times or than that of who did not.
Crosstab Risk Estimate
Q40: Do you have the
habit of Excess Bath or
Tub Bath
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
102 53
Odds Ratio for presence of
disease (disease present /
disease absent)
5.329 3.368 8.434
Expected
Count 68.0 87.0
For cohort .Do you have
the habit of Excess Bath or
Tub Bath = yes
2.480 1.914 3.214
Absent Count
52 144
For cohort .Do you have
the habit of Excess Bath or
Tub Bath = no
.465 .368 .588
Expected
Count 86.0 110.0 N of Valid Cases 351
Total Count 154 197
Expected
Count 154.0 197.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 54.220
a 1 .000
Continuity Correctionb
52.637 1 .000
Likelihood Ratio 55.406 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 54.065 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.01.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 96
Table 47: VH. Do you have the habit of Drinking Water between the meal
Chi square test was performed with subjects with or without Amlapitta , who are exposed
to drinking water between the meal and who did not and an association was found
between Amlapitta and drinking excess water between meal, x2 (1, N=351)=88.340,
P=0.000.
In this study those who drink water between the meal showed a probable risk of having
Amlapitta 9.358 times or than that of who did not.
Crosstab Risk Estimate
Q41: Do you have the
habit of Drinking Water
between the meal
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
121 34
Odds Ratio for presence of
disease (disease present /
disease absent)
9.358 5.717 15.32
0
Expected
Count 77.3 77.7
For cohort Do you have the
habit of Drinking Water
between the meal = yes
2.833 2.225 3.609
Absent Count
54 142
For cohort Do you have the
habit of Drinking Water
between the meal = no
.303 .222 .413
Expected
Count 97.7 98.3 N of Valid Cases 351
Total Count 175 176
Expected
Count 175.0 176.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 88.340
a 1 .000
Continuity Correctionb
86.331 1 .000
Likelihood Ratio 92.743 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 88.089 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 77.28.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 97
Table 48: VH. How often you express your Anger
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to Anger and who did not and an association was found between
Amlapitta and Anger, x2 (1, N=351)=98.023, P=0.000.
In this study those who express more anger showed a probable risk of having
Amlapitta 10.795 times or than that of who did not.
Crosstab Risk Estimate
Q42: How often you
express your Anger
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
122 33
Odds Ratio for presence of
disease (disease present /
disease absent)
10.79
5 6.541
17.81
7
Expected
Count 76.0 79.0
For cohort how often you
express your Anger = yes 3.085 2.396 3.973
Absent Count 50 146
For cohort how often you
express your Anger = no .286 .209 .391
Expected
Count 96.0 100.0 N of Valid Cases 351
Total Count 172 179
Expected
Count 172.0 179.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 98.023
a 1 .000
Continuity Correctionb
95.906 1 .000
Likelihood Ratio 103.333 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 97.744 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 75.95.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 98
Table 49: VH. How often you express your stress
Chi square test was performed with subjects with or without Amlapitta , who are
exposed to stress and who did not and an association was found between
Amlapitta and stress, x2 (1, N=351)=73.702, P=0.000.
In this study those who express more stress showed a probable risk of having
Amlapitta 7.625 times or than that of who did not.
Crosstab Risk Estimate
Q43: How often you
express your stress
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
122 33
Odds Ratio for presence of
disease (disease present /
disease absent)
7.625 4.686 12.40
7
Expected
Count 82.1 72.9
For cohort how often you
express your stress = yes 2.410 1.940 2.995
Absent Count 64 132
For cohort how often you
express your stress = no .316 .230 .434
Expected
Count 103.9 92.1 N of Valid Cases 351
Total Count 186 165
Expected
Count 186.0 165.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 73.702
a 1 .000
Continuity Correctionb
71.865 1 .000
Likelihood Ratio 77.197 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 73.492 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 72.86.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 99
Table 50: VH. How often you express your depression
Chi square test was performed with subjects with or without Amlapitta, who are
exposed to Depression and who did not and an association was found between
Amlapitta and Depression, x2 (1, N=351) =183.332, P=0.000.
In this study those who express depression drinks showed a probable risk of
having Amlapitta 39.118 times or than that of who did not.
Crosstab Risk Estimate
Q44: How often you
express your
depression
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
131 24
Odds Ratio for presence of
disease (disease present /
disease absent)
39.11
8
21.26
0
71.97
5
Expected
Count 68.4 86.6
For cohort how often you
express your depression =
yes
6.902 4.716 10.10
1
Absent Count
24 172
For cohort how often you
express your depression =
no
.176 .122 .256
Expected
Count 86.6 109.4 N of Valid Cases 351
Total Count 155 196
Expected
Count 155.0 196.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 183.332
a 1 .000
Continuity Correctionb
180.413 1 .000
Likelihood Ratio 202.439 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 182.810 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.45.
b. Computed only for a 2x2 table

OBSERVATIONS & RESULTS
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 100
Table 51: VH. How often you express your Anxiety
Chi square test was performed with subjects with or without Amlapitta, who are
exposed to Anxiety and who did not and an association was found between
Amlapitta and Anxiety, x2 (1, N=351) =256.860, P=0.000.
In this study those who e showed a probable risk express more anxiety having
Amlapitta 173.600 times or than that of who did not.
Crosstab Risk Estimate
Q45: How often you
express your Anxiety
Value
95% Confidence
Interval
Yes No Lower Upper
Present Count
140 15
Odds Ratio for presence of
disease (disease present /
disease absent)
173.6
00
75.72
4
397.9
85
Expected
Count 66.2 88.8
For cohort how often you
express your Anxiety =
yes
17.70
3 9.658
32.45
1
Absent Count 10 186
For cohort how often you
express your Anxiety = no .102 .063 .165
Expected
Count 83.8 112.2 N of Valid Cases 351
Total Count 150 201
Expected
Count 150.0 201.0
Chi-Square Tests
Value Df Asymp. Sig.
(2-sided)
Exact Sig.
(2-sided)
Exact Sig.
(1-sided)
Pearson Chi-Square 256.860
a 1 .000
Continuity Correctionb
253.389 1 .000
Likelihood Ratio 301.601 1 .000
Fisher's Exact Test .000 .000
Linear-by-Linear Association 256.128 1 .000
N of Valid Cases 351
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 66.24.
b. Computed only for a 2x2 table

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 101
DISCUSSION

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 102
DISCUSSION
This study entitled “Survey study on effect of Ahara and Vihara in Amlapitta”
was aimed to find the effect of Ahara and Vihara in manifestation of Amlapitta.
Food is considered as supreme or Brahma in Upnishads. It is responsible for life
of all beings74
. Food is one among the three sub pillars supporting the life75
. Pathya is that
which will not harm the Srotas of the body, which is liked by an individual and help in
the maintenance of health. Consuming Pathya Ahara provides wholesome effect on body
and mind without causing any untoward effect. Many diseases can be cured without any
medicines by just following wholesome regimen whereas even hundreds of medicines
cannot cure a disease in absence of wholesome regimen76
. No medicine is equivalent to
food; it is possible to make a person disease free with just proper diet 77
.
The activities done by the person in a normal condition are considered under
Vihara. These may include the way he takes his food, his sleep pattern, exercise etc. The
Acharyas have given a detailed explanation of the things to be done on a daily basis under
the preview Dinacharya, Ritucharya etc. These activities have an effect on the Doshas
and thus if done in an improper manner may lead to different diseases.
In the present era different types of lifestyle disorders are dominating the list of
health problems. Amlapitta (Hyperacidity) is one among the commonest health problem
in the society which is triggered by irregular and improper food habits and lifestyle. It
may eventually lead to complications like gastric ulcers, perforation and carcinoma.
Amlapitta is potentially preventable disease. By this study it was found that altering one‟s
Ahara (diet) and Vihara (lifestyle) it can be tackled in a simple and cost effective manner.
DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 103
DISCUSSION ON QUESTIONNAIRE VALIDATION:
Based on Nidana of Amlapitta as per the classical texts of Ayurveda and different
research articles, questionnaire containing a total of 45 questions was designed. The items
were divided into two domains of Ahara (diet) and Vihara (lifestyle). Questionnaire was
distributed to 25 healthy subjects and 25 Amlapitta patients. After that data collected
from the subjects and evaluated by using SPSS version 20, with Cronbach‟s alpha. A
Cronbach‟s alpha value of 0.976 was obtained for all questions which was highly
significant. (A high value for Cronbach‟s alpha indicates good internal consistency of the
items in the scale, >0.9 = Excellent). All questions were framed in the final questionnaire
without any deletion. On further analysis by odds ratio, all questions showed odds ratio
value of more than 1 which show the risk related to Amlapitta.
After validation of questionnaire it contained 45 closed end questions, framed in 5
Likert scale having options Daily, Frequently, Occasionally, Very rarely and None. The 5
Likert scale was further collapsed into dichotomous scale (Daily, Frequently,
Occasionally as „Yes‟ and Very rarely, None as „No‟).
Questionnaire was distributed to 351 subjects (196 diseased and 155 healthy). On
their response statistical test was run to analyze the observations with odds ratio and chi
square and result was drawn.
Discussion on Odds Ratio:
An odds ratio is a measure of association between exposure and outcome of a
disease and its risk factor. The OR represents the odds that an outcome will occur given a
particular exposure, compared to the odds of the outcome occurring in the absence of that

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 104
exposure. Odds ratio are mostly used in case control study, however they can also be used
in cross sectional and cohort study design as well (with some modification and / or /
assumptions)
Odds ratio are used to compare relative odds of the occurrence of the outcome of
interest (e.g. disease or disorder), given exposure to the variable of interest (e.g. health
characteristic, aspect of medical history). The odds ratio can also be used to determine
whether a particular exposure is a risk factor for a particular outcome, and to compare the
magnitude of various risk factors for that outcome.
OR = 1, Exposure does not affect odds of outcome
OR > 1 Exposure associated with higher odds of outcome
OR < 1 Exposure associated with lower odds of outcome [67]
In the present study odds ratio value of each question was analyzed and the values
which were obtained were very high. Thus all the items were proved to be risk factors for
Amlapitta. This may be due to the fact that the items were selected based on the Nidanas
of Amlapitta. Thus substantiating the Nidanas told in our classics practically.
Discussion on Chi Square:
In medical research, there are studies which often collect data on categorical
variables that can be summarized as a series of counts. These counts are commonly
arranged in tabular format known as contingency tables. The chi square test static can be
used to evaluate whether there is association between the rows and columns in a
contingency table. More specifically this static test can be used to determine whether

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 105
there is any difference between the study groups in the proportions of the risk factor of
interest.
Chi square test is a non parametric test used for two specific purposes.
1. To test the hypothesis of no association between two or more groups, population
or criteria (i.e. to check independence between the two variables)
2. To test how likely the observed distribution of data fits with the distribution that is
expected (i.e., to test goodness of fit)
It is used to analyze categorical data (e.g. male or female patients, alcoholic and non-
alcoholic etc.)
Chi square test can be calculated by using formula and value is obtained, i.e. „P‟ value.
The conventionally accepted P value is less than 0.05. If obtained P value is greater than
accepted P value i.e. less than 0.05, null hypothesis is accepted and research hypothesis is
rejected.
DISCUSSION ON AHARA:
All the Ahara Dravyas mentioned in the questionnaire were proved to be risk
factors of Amlapitta statistically. Based on the nidanas of Amlapitta 26 questions were
framed. The probable reason behind each of them causing Amlapitta is discussed below
Garlic
It is Ushna in Veerya and Teekshna in Guna which aggravates Pitta hence it
causes Amlapitta if consumed in excess. According to modern science the main chemical
component of garlic, allicin a sulfur containing compound has been seen to cause

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 106
heartburn and increased acidity on excessive consumption. This is more common when
raw garlic is consumed. This study reveals eating garlic in excess shows risk (14.355 OR)
factor of Amlapitta.
Ginger
As a good eventhough it is Deepana Pachana its Teekshna and Lekhana Gunas
increases burning sensation if taken more frequently. In some studies conducted by the
modern researchers it was seen that a consumption of more than 4 grams of ginger
powder caused increased heartburn. This study reveals eating ginger in excess shows risk
(12.294 OR) factor of Amlapitta.
Sour food items
Amla Rasa is Laghu, Ushna and Snigdha all properties that are similar to Pitta.
Thus foods that are having Amla rasa predominant increases the Pitta thus increasing the
risk of Amlapitta. Amla food mostly contain acids, when there is addition of acidic items
into the stomach more that what is required it increases the corroding action of the gastric
acids on the mucus lining. This study reveals eating sour food items in excess shows risk
(713.231 OR) factor of Amlapitta.
Spoiled food
Food items that spoilt may have undergone fermentation process which may result
in them having Amla rasa predominance and Abhisyandhi Guna in them. These properties
not only vitiate Pitta but also are heavy for digestion thus making the stomach secrete

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 107
more juices thus becoming a causative factor for Amlapitta. This study reveals eating
spoiled food in excess shows risk (129.455 OR) factor of Amlapitta.
Spicy food
Spicy food mostly have Ushna , Teekshna guna and Lavana , Katu Rasas. Both
Lavana and Katu Rasas are having Agni Mahabhoota predominance hence increases Pitta
and burning sensation. According to modern concept the spicy food items cause irritation
to mucus membranes of esophagus, stomach etc thus resulting in thinning of the mucosa
and causing ulcers. This study reveals eating spicy food in excess shows risk (298.350
OR) factor of Amlapitta.
Horse gram
It has properties like Teekshna , Amla Vipaka , Vidahi , Ushna Veerya , Ruksha
and Raktapitta karaka. It is also told as the Agrya among those that cause amlapitta. One
among the major chemical constituents of Kulattha is ascorbic acid which may be the
reason behind its action as an Amlapitta Janaka. This study reveals eating horsegram in
excess shows risk (1858.267 OR) factor of Amlapitta.
Flour items
Food items made out of flour like bread , pizza , burger are Guru and Abhisyandhi
in nature which causes Agni Mandyata which is also causative factor of Amlapitta. They
stay in the stomach for a long time and may undergo fermentation process there. This can
also lead to increased gastric acidity. This study reveals eating flour items in excess
shows risk (4.828 OR) factor of Amlapitta.

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 108
Green Chili
The Katu rasa and Ushna Teekshna gunas of green chili causes burning sensation
in throat and chest region. It is also Pitta Vardhaka. Like other katu rasa items this also
causes mucosal erosion and gastric ulcer. This study reveals eating green chili in excess
shows risk (923.100 OR) factor of Amlapitta.
Sour curd
The sour curd is Amla Rasa Pradhana ,Ushna , Kapha Pitta Vardhaka , Vata
Rakta Kara , Pitta Prakopara and Abhishyandi. It has all the properties enlisted in the
nidanas for Amlapitta. The acidic nature of the curd due to lactic acid may increase the
acidity of stomach. The formation of curd is by the process of fermentation which is also
a factor in causing acidity. This study reveals eating sour curd in excess shows risk
(1732.500 OR) factor of Amlapitta.
Red chili
It has similar properties like the green chili. Having properties like Teekshna
Ushna Ruksha Guna , Katu Rasa , Katu Vipaka , Ushna Veerya , Vidahi Janani ,
Raktapitta Krut which makes it more efficient in causing Gastritis. This study reveals
eating red chili in excess shows risk (500.192 OR) factor of Amlapitta.
New Jaggary
Jaggary which is newly prepared is considered to be very heavy in nature and is
said to cause Agnisada. Thus when a person consumes Guda in a large quantity there is
hampering of the digestive power which may lead to Vidagdha Ajeerna and further

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 109
Amlapitta. Thus it is one of the causative factors for Amlapitta. This study reveals eating
new jaggary in excess shows risk (673.200 OR) factor of Amlapitta.
Salty food items
Lavana Rasa has the properties like Teekshna , Kaphapitta vardhaka , Vidahi ,
Ushna veerya which are favorable for causing Amlapitta. It also causes increase in the
secretions. This study reveals eating salty food in excess shows risk (197.600 OR) factor
of Amlapitta.
Black gram
Excess intake of Idly , Vada , Dosa etc which are made up of black gram and also
fermented can cause Pitta Prakopa. Masha is told to be the best among Kaphapitta
Janana Dravyas. It is Ushna and guru burning sensation in chest and sour erectations.
This study reveals eating black gram in excess shows risk (673.200 OR) factor of
Amlapitta.
Pickle
Regular intake of pickles in excess quantity increases Pitta dosha and burning
sensation leading to the manifestation of Amlapitta. The cause for this is similar to the
other Katu Dravyas. They are Laghu, Ushna and Teekshna causing the Vidahata in body.
They are also mucosal irritants. This study reveals eating pickle in excess shows risk
(5.638 OR) factor of Amlapitta.

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 110
Discussion on Viruddha Ahara:
Indulgence of food articles which are contradictory produces disease or death.In
Astanga Hrudaya Sutrasthana Acharya says that the food ,drink and medicine which does
dislodgement of Dosha from its site that is Dosha Utklesha but does not expel it out from
the body is called Viruddha.
Acharya Charaka opines that the food and drugs which dislodge the Dosha from
its normal seat but does not expel it out of the body.
These contradictory foods are unwholesome to the body like acute poison and
chronic poison and can cause death.
The reason behind the Viruddhahara causing Amlapitta may vary according to the
type of Viruddha, but it may be attributed to the tri Dosha Dooshana and Durjaratva of
such Ahara.
This study reveals eating viruddahara in excess of domestic meat with honey
(121.529 OR), fish with curd (122.293 OR), fish with milk (91.841 OR), horse gram with
curd (669.524 OR), milk with raddish (948.633 OR), salt with milk (431.813 OR), pork
with curd (142.756 OR), sour fruit with milk (272.828 OR), leaf vegetable with butter
(422.308 OR), banana with curd (222.333 OR), aerated drinks (431.813 OR), heated curd
preparation (135.185 OR) shows a risk factor in Amlapitta.
Chi Square value for above all questions on Ahara is (P = 0.000), which is highly
significant in all Aharaja nidanas.

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 111
DISCUSSION ON VIHARA:
Vihara is an important pillar in Ayurveda. It means activity. Vihara plays a very
significant role in proper functioning of the body. The principles of vihara explain clearly
how to act in different ways that are life supportive and it also includes lifestyle
guidelines for maintaining good health.
Eating Food Irrespective of Hunger
When food taken previously is completely digested only then does a person feel
hungry. So if there is no hunger it means the digestion is not complete. When a person
eats again without feeling hungry it hampers Agni and causes indigestion. The new food
mixes with the previous half digested food and may undergo fermentation. There is also
the secretion of gastric juices onto the half digested food which will increase the acidity.
This study reveals eating irrespective of hunger shows (23.963 OR) risk factor in causing
Amlapitta.
Sleeping During Day
The body has a specific timetable for its functioning called the circadian rhythm.
In this the night is the time for sleep. When a person sleeps during the day time this clock
is disrupted which will have an effect on the hormones and GIT secretions also. The sleep
slows down the process of digestion thus increasing the contact period of the gastric
juices in the stomach. Acid presence in the stomach for a long time can cause mucosal
erosion leading to ulcer. According to Ayurveda sleeping during daytime increases kapha
Pitta Dosha producing Ama which paves way for the condition of Vidagdha Ajeerna in

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 112
turn leading to Amlapitta. This study reveals sleeping during daytime shows (29.858 OR)
risk factor in causing Amlapitta.
Consumption of Alcohol
Alcohol is a very potent causative factor of Amlapitta. Its consumption in excess
quantity increases acid secretions in stomach and causes inflammation of stomach. The
properties of alcoholic beverages are all Pitta Prakopaka in nature. It has Lavana Varjita
Pancha Rasa, Amla Vipaka and Teekshna, Ushna Gunas these increase burning sensation
in chest and throat region. Taking alcohol in empty stomach also has a corrosive effect on
the gastric mucosa. Drinking alcohol relaxes the lower esophageal sphincter, making it
easier for stomach contents to escape into the esophagus thus causing Urdvaga Amlapitta.
This study reveals alcohol consumption shows (18.975 OR) risk factor in causing
Amlapitta.
Smoking
Smoking is considered to be a very potent Pitta Prakopaka Vihara Dhoomapana
is contraindicated in Pitta Kala, Pitta Prakopa, along with Madya, Matsya, Dadhi etc
thus stating its role in Pitta and Rakta Dooshana.. Smoking causes digestive stress and
lead to indigestion. It slows down production of saliva which is a natural defense of body
against stomach acid, stimulates production of stomach acid and Injures esophagus.
Smoking also results in the washing of bile salts from the intestine into the stomach,
producing acid reflux. This study reveals smoking shows (14.355 OR) risk factor in
causing Amlapitta.
DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 113
Tea or Coffee
The main constituent in tea and coffee is caffeine which is a stimulant. It causes a
rise in pulse, blood pressure and stomach acid production. Indulgence in excess of tea or
coffee also decreases pressure in lower esophageal sphincter, contributing to more gastro
esophageal reflux. Coffee is highly acidic and it can stimulate the hyper secretion of
gastric acids. Coffee tends to speed up the process of gastric emptying, which may result
in highly acidic stomach contents passing into the small intestine more rapidly than
normal leading to inflammation there. This study reveals tea or coffee shows (14.205 OR)
risk factor in causing Amlapitta.
Skipping meals
Skipping meals when hungry has a very direct and clear effect on the production
of Amlapitta symptoms. When a person is hungry it means that the previous food has
been digested and the stomach is empty awaiting the next meal. There is production of the
gastric acid during this time. So when food is not provided then, the produced acid
attacks stomach lining leading to erosion of mucosa, ulcers, inflammation and abdominal
pain every time when we consume food thereafter. This study reveals skipping meals
shows (7.502 OR) risk factor in causing Amlapitta.
Drinking excess water soon after meal
Drinking a lot of water soon after meals may cause Agni mandya causing
indigestion and produce Ama which is a cause of Amlapitta. The drop in the temperature
of stomach due to the water will cease the digestion process and will also make the

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 114
contact period of acid more. This study reveals drinking excess water soon after food
shows (4.828 OR) risk factor in causing Amlapitta.
Extra spice and salt
As told for each food item that is Katu and Lavana these food items having
Teekshna and Ushna Guna whih causes aggravation of Pitta. There is also increases level
of HCL in the stomach due to such food, which causes burning sensation and damages
stomach lining causing inflammation. This study reveals eating extra spice and salt shows
(12.294 OR) risk factor in causing Amlapitta.
Bathing soon after food
Taking bath soon after a meal will lead to Mandagni which may leads in the
condition of Tridosha Prakopa and formation of Ama takes place. This can lead to
condition Ajeerna and then Amlapitta. In the modern context, bathing will lead to a
reduced blood supply to the GIT organs leading to delayed digestion. Digestion requires a
lot of energy and a good amount of blood flow toward the stomach. When you take a bath
or shower right after eating dinner, it causes a slight decrease in body temperature thus
hampering the digestion. This study reveals bathing soon after food shows (20.457 OR)
risk factor in causing Amlapitta.
Suppressing natural urges
The suppression of the natural urges like Pureesha, Mootra Adhovata etc,leads to
vitiation of Apana vayu and causes Udavarta and subsequently vitiation of Samana Vata
which is instrumental in digestion. The Vegas are generated by action of Vata and if it is

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 115
suppressed Tridosha vitiation takes place which will also affect Agni. This study reveals
suppressing natural urges shows (23.034 OR) risk factor in causing Amlapitta.
Sleeping immediately after food
Sleeping soon after having food may feel good, but when the body is in supine
position, is difficult for the digestive system to work which may lead to abnormal HCL
leading to hyperacidity. The position can also facilitate easy refluxes of the gastric
content into the esophagus causing heartburn. The sleep also slows down the process of
digestion. Sleep according to Ayuveda causes Mandagni and Ajeerna as results. This
study reveals sleeping immediately after food shows (5.638 OR) risk factor in causing
Amlapitta.
Drinking water between meals
As per Ayurveda water is to be taken in between the meal but it is not that large
amounts of water are to be drunk. This will do more bad than good. The digestive juices
may get diluted hampering the digestion or the more liquid content may trigger acid
reflux symptoms. This study reveals drinking water between meals shows (9.358 OR) risk
factor in causing Amlapitta.
Anger, depression, stress and anxiety
The Manasika Bhavas like anger and stress vitiates Pitta Dosha. The increased
Pitta also increases the Agni and Daha in the person. Sometimes in the conditions like
depression and stress due to intense emotional feeling and lack of mood to do anything
the person may also get aversion towards everything including normal dietary intake

DISCUSSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 116
which lead to manifestation of gastritis. Stress can also deplete the production of
substances called "prostaglandins," which normally protect the stomach from the effects
of acid. When in stress body produces hormones that slow down digestion. Food stays in
your stomach longer. That means stomach acids have more time to move up into your
esophagus. This study reveals anger (10.795 OR), stress (7.625 OR), depression (39.118
OR) and anxiety (173.600 OR) shows risk factors in causing Amlapitta.
Other Vihara Factors
Eating Betalnut leaf with tobacco (8.174 OR), work in too hot atmosphere (14.205
OR), excess bath (5.329 OR) shows risk factor in Amlapitta.
Chi Square value for above all questions on Vihara is (P = 0.000), which is highly
significant in all Viharaja nidanas.

CONCLUSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 117
CONCLUSION

CONCLUSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 118
CONCLUSION
The presence study entitled “Survey study on effect of ahara and vihara in
amlapitta”, was an attempt to draw an insight on risk factors associated with ahara and
vihara in amlapitta, as amlapitta is an emerging common disease. After a detail
conceptual study critical review, observations, analysis of data and discussion, the
following conclusions were evolved. All the factors analyzed were arranged in decreasing
order of obtained odds ratio and chi square values.
This study revealed that Ahara, Vihara, Aachara, Vichar, if not following in
proper manner become a causative factor of Amlapitta.
Based on Ahara (Diet):
Horsegram (1858.267 OR), sour curd (1732.500 OR), milk with raddish
(948.633 OR), green chili (923.100 OR), sour taste food (713.231 OR), new jaggary
(673.200 OR), black gram (673.200 OR), horsegram with curd (669.524 OR), red chili
(500.192 OR), salt with milk (431.813 OR), aerated drinks (431.813 OR), leafy vegetable
with butter (422.308 OR), spicy food (298.350 OR), sour fruit with milk (272.828 OR),
banana with curd (222.333 OR), salty food (197.600 OR), pork with curd (142.756 OR),
heated curd preparation (135.185 OR), spoiled food (129.455 OR), fish with curd
(122.293 OR), domestic meat with honey (121.529 OR), fish with milk (91.841 OR),
garlic (14.355 OR), ginger (12.294 OR), pickles (5.638 OR), flour items (4.828 OR) all

CONCLUSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 119
these factors have shown risk in causing Amlapitta. Chi Square value for all questions( P
= 0.000).
Based on Vihara (Lifestyle):
Anxiety (173.600 OR), depression (39.118 OR), day sleep (29.858 OR), eating
irrespective of hunger (23.963 OR), suppressing natural urges (23.034 OR), bathing soon
after food (20.457 OR), alcohol (18.975 OR), smoking (14.355 OR), tea or coffee (14.205
OR), work in hot atmosphere (14.205 OR), adding extra salt and spice (12.294 OR),
anger (10.795 OR), drinking water between meal (9.358 OR), betalnut leaf with tobacco
(8.174 OR), stress (7.625 OR), skipping meal (7.502 OR), sleeping soon after food (5.638
OR), excess bath or tub bath (5.329 OR), drinking excess water soon after food (4.828
OR) all these factors shows risk factor in Amlapitta.
This study reveals that there is an effect of Ahara and Vihara in manifestation of
Amlapitta.

CONCLUSION
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 120
Further Scope of Study
Survey study based on measurement of food items which is consumed in routine
causes Amlapitta.
Effect of risk factors associated with Vihara in Amlapitta.

SUMMARY
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 121
SUMMARY

SUMMARY
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 122
SUMMARY
The present work entitled “Survey study on effect of Ahara and Vihara in
Amlapitta” was broadly dealt under following headings:
Introduction
Aims & Objectives
Review of Literature
Materials and Methods
Observations and Results
Discussion
Conclusion
Introduction:
It gives a brief review, why the work was selected for research.
Aims and Objectives:
The present survey study was carried out with following aims and objectives.
1. To find out the effect of Ahara and Vihara in Amlapitta.
Review of Literature:
It puts forward review on concepts of diet and lifestyle in Vedic principles,
concept of lifestyle as per Ayurveda, concept of Swastha as per Ayurveda, concept of
Agni and Ama, Arogya karanam and Roga, preventive principles in Ayurveda and
contemporary science .

SUMMARY
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 123
Materials and Methods:
Data for framing questionnaire was collected from Ayurvedic books,
contemporary books, journals and research articles. A set of 45 questions were framed on
considering possible Nidana for Amlapitta and were given to 25 healthy and 25 Amlapitta
cases. After collecting data, analysis done with SPSS 20 version, using Chronbac’s alpha
and odds ratio then questions were used to collect data from 196 cases (Amlapitta) and
155 controls (Healthy). Data analysis was done using odds ratio and chi square and
conclusion was drawn.
Discussion:
Discussion was done on framing of questionnaire, validation of questionnaire,
odds ratio, chi square. After that discussion on Ahara (diet) and Vihara (lifestyle) was
done separately. Discussion on Ahara and Viruddha Ahara was done. Discussion on
Vihara was further divided into Sharirika Vihara and Manasika vihara
Conclusion:
Conclusion was drawn on the basis of obtained odds ratio and chi square value in
decreasing order and hence proves that there is a significant role of Ahara and Vihara in
causing Amlapitta.

REFERENCE
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA
REFERENCE

REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 124
REFERENCES
1) Sri Satyapala, KashyapaSamhita with Vidyotinihindini Commentry,
Varanasi:Choukambha Sanskrit Sansthan; 2010.p.335.
2) SriSatyapala, Kashyapa Samhita, with Vidyotini hindi Commentry,
Varanasi:Choukambha Sanskrit Sansthan;2010.p.336. SriSatyapala,
3) Locke GR 3rd, Talley NJ, Fett SA, Prevalence and clinical spectrum of
gastroesophageal reflux: A population-based study in Olmsted County,
Minnesota. Gastroenterology. 1997, 112: 1448-56.
4) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.21. Acharya
5) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.114.
6) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.131.
7) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.144. Acharya
8) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia;2011.p.151. Acharya.
9) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.155. Acharya.
10) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.457. Acharya.

REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 125
11) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.517. Acharya.
12) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.487
13) Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary of
Dalhanacharya. Reprint ed. Varanasi (India): Chaukambha Sanskrit Sansthan;
2010.P 185.
14) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.336.
15) Harita,Vd.Jaymini Pandey,Harita samhita with Nirmala Hindi commentary,
Chukhamba Vishvabharti,Varanasi 2010,P.384.
16) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.16.
17) Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary
Dalhanacharya. Reprint ed. Varanasi (India): Chaukambha Sanskrit Sansthan;
2010. P 101
18) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.170.
Acharya
19) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.517.
20) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.170

REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 126
21) Sharma SP. Astanga samgraha of Vrddha Vagbata with Sasilekha Sanskrit
commentary of Indu. Varanasi (India): Chaukambha Orientalia; 2008 .p.159 .
22) Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.338
23) Sharma SP. Astanga samgraha of Vrddha Vagbata with Sasilekha Sanskrit
commentary of Indu. Varanasi (India): Chaukambha Orientalia; 2008 .p.159
24) Satyapala. Kashyapa Samhita with Vidyotini hindi commentary.
Varanasi:Choukambha Sanskrit Sansthan; 2010 .p.338
25) Sharma SP. Astanga samgraha of Vrddha Vagbata with Sasilekha Sanskrit
commentary of Indu. Varanasi (India): Chaukambha Orientalia; 2008 .p.159
26) Sharma SP. Astanga samgraha of Vrddha Vagbata with Sasilekha Sanskrit
commentary of Indu. Varanasi (India): Chaukambha Orientalia; 2008 .p.159
27) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.491.
28) Paradakara HSS, Ashtanga Hrudayam with Sarvanga Sundaram commentary of
Arunadutta and Ayurveda Rasayana of Hemadri. 9thed. Varanasi (India):
Chaukambha Sanskrit Sansthan; 2005. p.193.
29) Paradakara HSS, Ashtanga Hrudayam with Sarvanga Sundaram commentary of
Arunadutta and Ayurveda Rasayana of Hemadri. 9thed. Varanasi (India):
Chaukambha Sanskrit Sansthan; 2005. p.193.
30) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.514. Acharya
31) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.512.
REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 127
32) Paradakara HSS, Ashtanga Hrudayam with Sarvanga Sundaram commentary of
Arunadutta and Ayurveda Rasayana of Hemadri. 9thed. Varanasi (India):
Chaukambha Sanskrit Sansthan; 2005. p.193.
33) Sharma SP. Astanga samgraha of Vrddha Vagbata with Sasilekha Sanskrit
commentary of Indu. Varanasi (India): Chaukambha Orientalia; 2008 .p.401.
34) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.517.
35) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.517.
36) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.517. Acharya
37) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.517.
38) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512.
39) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512.
40) Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary of
Dalhanacharya. Reprint ed. Varanasi (India): Chaukambha Sanskrit Sansthan;
2010. p. 102.

REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 128
41) Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary of
Dalhanacharya. Reprint ed. Varanasi (India): Chaukambha Sanskrit Sansthan;
2010. p. 102.
42) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512. Acharya
43) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.512 .
44) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512
45) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512
46) Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary of
Dalhanacharya. Reprint ed. Varanasi (India): Chaukambha Sanskrit Sansthan;
2010.p. 253.
47) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512
48) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.512.

REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 129
49) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.332.
50) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.491. Acharya
51) JT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani Datta.
Reprint ed. Varanasi (India): Chaukambha Orientalia; 2011.p.52.
52) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.525.
53) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.235.
54) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.336
55) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.171
56) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.337
57) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.171
58) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.337

REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 130
59) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.171
60) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.170
61) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.336
62) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.619
63) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.336
64) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.171
65) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.336
66) Acharya JT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.66
67) Acharya YT. Madhava nidana with madhukosha commentary of Vijayarakshita
and Srikanthadatta. Reprint ed. Chaukambha orientalia; Varanasi; 2010.p.173
68) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.338
69) Sri Satyapala. Kashyapa Samhita with Vidyotini hindi commentary. Varanasi:
Choukambha Sanskrit Sansthan; 2010 .p.336.
REFFERNCES
SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 131
70) Gautham Joghad. Clinical study on the role of Virechana and Bhoonimbadi vati
in the management of Urdhwaga Amlapitta, M D Thesis. Jamnagar: Gujarat
Ayurveda University; 2004.P.88
71) K Sembulingam, Sembulingam p. Essential of Medical Physiology. # 5th
ed,
New Delhi: Jaypee Brothers Medical Publisher ( P) Ltd; 2010, p.221.
72) Vinaya T M. A Comparative study on Kushmanda rasayana and shruta sheeta
jala as Pathya in the Amlapitta( Hyperacidity). MD Thesis. Bangalore: Rajiv
Gandhi university of Health science; 2012. P.94-115
73) Vinaya T M. A Comparative study on Kushmanda rasayana and shruta sheeta
jala as Pathya in the Amlapitta( Hyperacidity). MD Thesis. Bangalore: Rajiv
Gandhi university of Health science; 2012. P.121-128
74) Vridda Jeevaka, Vatsya, sri Satyapala Bhisagcharya( editor). Kashyapa Samhita
or Vrddhajivakiya Tantra with vidyotini Hindi commentary. Reprint ed
Varanasi: Chaukhambha Sanskrit Sansthana ; 2009. Verse 4. P.249
75) Agnivesha, Charaka, Dridabala, yadavaji Trikamji. Charaka Samhita of
Agnivesa with the Ayurveda – Dipika commentary of Chakradatta and
Vidyotini hindi commentry. Reprint ed, Varanasi: Chaukhamba Sanskrit
sansthana; 2007. Verse 35. P. 160
76) .Vridda Jeevaka, Vatsya, sri Satyapala Bhisagcharya( editor). Kashyapa Samhita
or Vrddhajivakiya Tantra with vidyotini Hindi commentary. Reprint ed.
Varanasi: Chaukhambha Sanskrit Sansthana ; 2009. Verse 5. P.249
77) .Vridda Jeevaka, Vatsya, sri Satyapala Bhisagcharya( editor). Kashyapa Samhita
or Vrddhajivakiya Tantra with vidyotini Hindi commentary. Reprint ed .
Varanasi: Chaukhambha Sanskrit Sansthana ; 2009. Verse 6. P.249
ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 132
ANNEXURE

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 133
ANNEXURE
CONSENT FORM
1. TITLE OF STUDY: “SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN
AMLAPITTA”.
2. Participant enrollment ID for this trial:
3. Name of the Investigating Physician (Research Scholar): Dr Rakshith K. R
4. Name of the Guide: Dr. Shivakumar MD (Ayu)
5. I confirm that I have read / the study has been explained to me adequately and I have
understood the information sheet for the above study and had the opportunity to ask questions.
6. I hope to complete the study, but I understand that my participation is voluntary and that I am
free to withdraw at any time, without giving a reason, and without my medical care or legal rights
being affected.
7. I understand that the information will be used for medical research only and that I will not be
identified in any way in the analysis and reporting of the results. I understand that sections of any
of my medical notes may be looked at by the authorities or responsible individuals from the
members of the IEC, Regulatory authorities or Court, if necessary. I give permission for these
individuals to have access to my records.
8. I understand what is involved in this trial and agree to take part in this survey study for a
period of 1 day.
Name of the Patient: _________________________ IP NO: ____________________________
Gender: (M/F) ______________ Age: ___________ Religion:___________________________
Address: _________________________________ Signature_____________________________
Guardian(s) Signature Date: ____________________Mobile No: _________________________
Name of the witness Signature Date:_________________________________________________
Investigating physician
(Research Scholar)
Signature with Date: Dr. Rakshith K.R
Guide Signature with Date: Dr. Shivakumar MD (Ayu)

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 134
A SURVEY STUDY ON EFFECT OF AHARA AND VIHARA IN AMLAPITTA
1.How frequently you use Garlic in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಬೆಳ್ಳುಳ್ಳು G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
2. How frequently you use Ginger in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಶುಂಠಿ G¥ÀAiÉÆV¸ÀÄwÛÃj? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
3.How frequently you use sour taste foodin a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ºÀĽ¥ÀzÁxÀð
G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
4.How frequently you use spoiled food in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ºÀ¼À¹zÀ DºÁgÀ
w£ÀÄßwÛÃj?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ) (1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 135
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
5.How frequently you use spicy food in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ SÁgÀ G¥ÀAiÉÆV¸ÀÄwÛÃj? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
6.How frequently you use Horsegram in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಹುರುಳ್ಳ ತಿನ್ುುತಿತೀರಿ?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
7.How frequently you eat flour items in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ »nÖ£À¥ÀzÁxÀð
ತಿನ್ುುತಿತೀರಿ?) (Like Pizza , Burger , Sandwitch , Bread)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
8.How frequently you use Green ChillI in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ºÀ¹ªÉÄt¸ÀÄ
ತಿನ್ುುತಿತೀರಿ )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 136
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
9.How frequently you use sour Curd in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಮೊಸರು ತಿನ್ುುತಿತೀರಿ? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
10.How frequently you use Red Chilli in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ PÉ0¥ÀĪÉÄt¸ÀÄ
ತಿನ್ುುತಿತೀರಿ )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ) (4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ) (1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
11.How frequently you use new Jaggery in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಬೆಲಿ್ ತಿನ್ುುತಿತೀರಿ )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
12.How frequently you use Salty food in a week? (ನೀವುಒಂದುವರದಲಿ್ಲಎಷುುಬರಿG¦à£À DºÁgÀ
ತಿನ್ುುತಿತೀರಿ )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 137
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj
13.How frequently you use Black gram in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಉದಿ್ದನ್ಬೆೀಳ ೆತಿನ್ುುತಿತೀರಿ)?
(Idly ,Vada , Dosa)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
14.How frequently you eat Pickle in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಉಪ್ಪಿನ್ಕಯಿ ತಿನ್ುುತಿತೀರಿ)?
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
How many times in a day? (M0zÀÄ ¢£ÀzÀ°è J¸ÀÄÖ¨Áj G¥ÀAiÉÆV¸ÀÄwÛÃj?)
a) once (M0zÀĨÁj)b) twice (JgÀqÀĨÁj)c) thrice (ªÀÄÆgÀĨÁj) d) More than three times
(ªÀÄÆgÀQÌ0vÀºÉZÀÄѨÁj)
15. How frequently you useAerated Drinks in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ
vÀ0¥ÀÄ¥Á¤ÃAiÀĸÉë¸ÀÄwÛÃj? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
16.How frequently you use Domestic meat with honey in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ªÀiÁ0¸À
ªÀÄvÀÄÛ eÉãÀÄ vÀÄ¥Àà ತಿನ್ುುತಿತೀರಿ)?
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 138
17. How frequently you eat Fish with Curd in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿಮೀನ್ು, ಮೊಸರು
ಜೆೊತೆಯಗಿ ತಿನ್ುುತಿತೀರಿ )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ) (1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
18. How frequently you eat Fish with Milk in a week?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಹಲ್ು-ಮೀನ್ು
ಜೆೊತೆಯಗಿ ತಿನ್ುುತಿತೀರಿ)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ) (1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
19. How frequently you eat Horsegram with curd in a week ? (ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ
ªÉƸÀgÀನೆೊಂದ್ದಗೆ ºÀÄgÀ½PÁ¼ÀÄ ತಿನ್ುುತಿತೀರಿ? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
20. How frequently you use Milk with Raddishin a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಹಲ್ಲನೆೊಂದ್ದಗೆ
ªÀÄÆ®0V ತಿನ್ುುತಿತೀರಿ? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
21. How frequently you use salt with milk in a week? (ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ಹಲ್ಲನೆೊಂದ್ದಗೆ
ಉಪ್ಿಗಿರುವ ತಿನಸುಗಳ್ನ್ುು ತಿನ್ುುತಿತೀರಿ?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 139
22.How frequently you use pork with curd in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ªÉƸÀgÀನೆೊಂದ್ದಗೆ
ºÀ0¢ªÀiÁ0¸À ತಿನ್ುುತಿತೀರಿ?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
23. How frequently you use Sour fruits with Milk in a week? (ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ
ಹುಳ್ಳಹಣ್ುುಗಳ್ ಹಲ್ಲನ್ಸೆೀವನೆಮಡುತಿತೀರಿ )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
24. How frequently you use Leafy Vegetable with Butter in a week? (ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ
¸ÉƦà£À dvÉ ¨ÉuÉÚAiÀÄ£ÀÄß w£ÀÄßwÛÃj?)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ) (4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ) (1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
25. How frequently you use Banana with Curd in a week? (ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ ¨Á¼ÉºÀtÂÚ£À dvɪÉƸÀgÀ£ÀÄß ಸೆೀವನೆ ಮಡುತಿತೀರಿ? )
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
26. How frequently you use Heated curd preparations in a week ?(ನೀವು ಒಂದು ವರದಲಿ್ಲ ಎಷುು ಬರಿ
©¹ªÀiÁrzÀªÉƸÀgÀ£ÀÄ߸ɫ¸ÀÄwÛÃj)
a)Daily
(ನತ್ಯವೂ)
b)Frequently
(ಪದೆೀಪದೆೀ)
(4-6 days)
c) Occasionally
(ಎಂದದರೆೊಮ್ಮೆ)
(1-3 days)
d)Very Rarely
(ಅತ್ಯಂತ್ಕಡಿಮ್ಮಬರಿ)(Less
than once)
E)None
(ಇಲಿ್)
27.Do you have the habit of eating food irrespective of hunger? (¤ªÀÄUÉ ºÀ¹ªÀÅ E®èzÉ HlªÀ£ÀÄߪÀiÁqÀĪÀ
C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
28.Do you have the habit of Day sleeping? (ನಮಗೆºÀUÀ°£À°èªÀÄ®UÀĪÀ C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) /
No(ಇಲಿ್) ]

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 140
29.Do you have the habit of Alchohol Consumption? (ನಮಗೆªÀÄzsÀå¥Á£À¸Éë¸ÀĪÀ C¨sÁå¸À«zÉAiÉÄÃ?
[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
30.Do you have the habit of Smoking? (ನಮಗೆ zsÀƪÀÄ¥Á£À ¸Éë¸ÀĪÀ C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) /
No(ಇಲಿ್) ]
31.Do you have the habit of excess intake of tea or coffee? (ನಮಗೆCwºÉZÀÄÑ nÃCxÀªÀ PÁ¦üûà PÀÄrAiÀÄĪÀ
C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
32.Do you have the habit of Skipping Meals? (ನಮಗೆ Hl vÀ¦à¸ÀĪÀ C s̈Áå¸À«zÉAiÉÄÃ?
[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
33.Do you have the habit of drinking excees water soon after meals? (ನಮಗೆ Hl ªÀiÁrzÀ vÀPÀêt ¤ÃgÀÄ
PÀÄrAiÀÄĪÀ C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
34.Do you have the habit of eating Betalnut Leaf with Tobbaco? (ನಮಗೆ vÀ0ªÀiÁâQ£À dvÉ«¼ÉîÃzɯÉAiÀÄ£ÀÄß
w£ÀÄߪÀ C¨sÁå¸À«zÉAiÉÄÃ?
[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
35.Do you have the habit of Adding extra salt and spice for the food you eat? (ನಮಗೆHlzÀ°èCwºÉZÀÄÑ
SÁgÀªÀÄvÀÄÛ G¥Àà£ÀÄß w£ÀÄߪÀ C¨sÁå¸À«zÉAiÉÄÃ?
[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
36.Do you work in too hot atmosphere? (¤ÃªÀ Å Cw ºÉZÀÄÑ ©¹°£ÀªÁvÁªÀgÀtzÀ°è PÉ®¸ÀªÀiÁqÀÄwÛÃgÁ?[ Yes
(ಹೌದು) / No(ಇಲಿ್) ]
37.Do you have the habit of Bathing soon after having food? (¤ÃªÀÅ Hl ªÀiÁrzÀ vÀPÀêt ¸ÁߣÀªÀiÁqÀĪÀ
C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
38.Do you have the habit of Supressing Natural Urges? (¤ªÀÄUɤªÀÄäªÉÃUÀªÀ£ÀÄߤAiÀÄ0wæ¸ÀĪÀ C¨sÁå¸À«zÉAiÉÄÃ?[
Yes (ಹೌದು) / No(ಇಲಿ್) ]

ANNEXURE
SURVEY STUDY ON THE EFFECT OF AHARA AND VIHARA IN AMLAPITTA Page 141
39.Do you have the habit of sleeping soon after having food? (ನಮಗೆ Hl ªÀiÁrzÀ vÀPÀêt ¤zÉݪÀiÁqÀĪÀ
C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ] 40.Do you have the habit of Excess Bath or Tub Bath? (¤ªÀÄUÉ
Cw ºÉZÀÄÑ ¸ÁߣÀªÀiÁqÀĪÀ C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
41.Do you have the habit of Drinking Water between the meal? (ನಮಗೆHlzÀªÀÄzsÀåzÀ°è¤ÃgÀÄ PÀÄ¢AiÀÄĪÀ
C¨sÁå¸À«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
42.Do you often feelAngry? (¤ªÀÄUÉ«ÃUÀªÁV ¹lÄÖ§gÀÄvÀÛzÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
43.Do you often feel Stress? (ನಮಗೆCwAiÀiÁzÀªÀvÀÛqÀ«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
44.Do you often feelDepressedl? (ನಮಗೆzÀÄ:R«zÉAiÉÄÃ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]
45.Do you often feel Anxiety? (ನಮಗೆ?[ Yes (ಹೌದು) / No(ಇಲಿ್) ]













![€¦ · [ ] [ ] Anandakuti IT Group $ ! Collection No. 13 Buddhakalina Brahaman (PART III) Bhikshu Amtitananda Published by ANANDA KUTI VIHARA TRUST Ananda Kuti, Kath](https://static.fdocuments.in/doc/165x107/6029aeb97f33d2539636d058/-anandakuti-it-group-collection-no-13-buddhakalina-brahaman-part-iii.jpg)



