
Surgery tutorials for medical students
130
[email protected] Page 1 TUTORIALS COMPILED BY DR BASHIR BIN YUNUS (MBBS, ZARIA) SURGICAL RESIDENT AMINU KANO TEACHING HOSPITAL
-
Upload
bashir-bnyunus -
Category
Health & Medicine
-
view
1.357 -
download
8
Transcript of Surgery tutorials for medical students

[email protected] Page 1
TUTORIALS
COMPILED
BY
DR BASHIR BIN YUNUS (MBBS, ZARIA)
SURGICAL RESIDENT
AMINU KANO TEACHING HOSPITAL

[email protected] Page 2
Contents
PART ONE
Surgical infections………………………………………………………………………………………
Wound and wound healing…………………………………………………………………………
Sutures ……………………………………………………………………………………………………..
Cutaneous ulcers………………………………………………………………………………………..
Fluid and electrolytes therapy……………………………………………………………………..
Shock ………………………………………………………………………………………………………….
Blood transfusion………………………………………………………………………………………
Hemostasis in surgery…………………………………………………………………………………
Nutrition in surgery…………………………………………………………………………………….
Metabolic response to trauma……………………………………………………………………
Perioperative management………………………………………………………………………..
Surgical prophylaxis…………………………………………………………………………………..
SCD and surgery………………………………………………………………………………………….
Diabetics and Surgery ……………………………………………………………………………….
HIV and the surgeon …………………………………………………………………………………
Obesity and surgery…………………………………………………………………………………..
Surgery in the elderly ……………………………………………………………………………….
Surgical hypertension……………………………………………………………………………….
Asepsis in surgery…………………………………………………………………………………….

[email protected] Page 3
Multiply Injured patient …………………………………………………………………………..
Cancer chemotherapy…………………………………………………………………………………
Radiotherapy ……………………………………………………………………………………………..
Use of drains in surgery……………………………………………………………………………
Diathermy……………………………………………………………………………………………………
Lacer …………………………………………………………………………………………………………
Tourniquet…………………………………………………………………………………………………
Minimal access surgery……………………………………………………………………………..
Principles of neonatal surgery……………………………………………………………………
Biopsy ……………………………………………………………………………………………………….
Prostate biopsy
Dialysis
Informed consent………………………………………………………………………………………
Day case surgery ………………………………………………………………………………………
Medical ethics …………………………………………………………………………………………..
Surgical audit…………………………………………………………………………………………….
PART TWO (Principles in management)
Upper GI bleeding …………………………………………………………………………………….
Urinary calculi…………………………………………………………………………………………..
Calculus cholecystitis ……………………………………………………………………………….
Typhoid ileal perforation………………………………………………………………………….
Surgical management of peptic ulcer disease………………………………………….
Fournier gangrene …………………………………………………………………………………..

[email protected] Page 4
Benign prostatic hyperplasia…………………………………………………………………….
Prostate cancer………………………………………………………………………………………..
Obstructive uropathy...………………………………………………………………………………
Gastric outlet obstruction ………………………………………………………………………..
Gastrostomy …………………………………………………………………………………………………
Hernia …………………………………………………………………………………………………………..
Intestinal fistula……………………………………………………………………………………………
Malignant ascites ………………………………………………………………………………………..
Malignant bowel obstruction ……………………………………………………………………..
Malignant hyperthermia ……………………………………………………………………………..
Chest trauma……………………………………………………………………………………………….
Abdominal injury ……………………………………………………………………………………….
Mass casualty ……………………………………………………………………………………………..
Regional anaesthesia ………………………………………………………………………………….
PART THREE
Operatives…………………………………………………………………………………………………
PART FOUR
Long case ………………………………………………………………………………………………….
OSCE…………………………………………………………………………………………………………..
Surgical instruments………………………………………………………………………………….
Radiographs……………………………………………………………………………………………..
PART FIVE (pathology and management)

[email protected] Page 5
Surgical tutor …………………………………………………………………………………………..
Past questions –
Essay
Orals
SURGICAL INFECTIONS
DEFINITIONS
Infection in which there is anatomic or mechanical problem that must be resolved
by operation or another invasive procedure to cure the infection.
Antibiotic are adjunct and are not substitute for indicated surgical therapy.
BACTERAEMIA; the transient invasion of the circulation by bacteria is known as
bacteraemia.
SEPTICEMIA; this implies prolonged presence of bacteria in the blood accompanied by
severe systemic reaction.
SYSTEMIC INFLAMMATORY RESPONSE SYNDROME (SIRS): The systemic
inflammatory response to a wide variety of severe clinical insults manifests by 2 or more
of the following conditions:
• Temperature greater than 38°C or less than 36°C
• Heart rate greater than 90 beats per minute (bpm)
• Respiratory rate greater than 20 breaths per minute or PaCO2 less than 32 mm Hg
• White blood cell count greater than 12,000/mL, less than 4000/L, or 10% immature
(band) forms
SEPSIS: This is a systemic inflammatory response to a documented infection.
SEVERE SEPSIS: This is sepsis and SIRS associated with organ dysfunction,
hypoperfusion, or hypotension.
SEPTIC SHOCK: Refers to severe sepsis which is not responsive to intravenous fluid
infusion for resuscitation and requires inotropic or vasopressor agent to maintain systolic
blood pressure.

[email protected] Page 6
CHARACTERISTICS IF SURGICAL INFECTIONS
(unlike medical infections)
- Damaged host defences (especially epithelial barrier)
- Immunological defects are global – trauma, nutritional deficiency, etc
- Pathogens are polymicrobial, both aerobic and anaerobic
- Pathogens often from endogenous flora (opportunistic) as well as from exogenous.
ORGANISMS COMMONLY ENCOUNTERED IN SURGICAL INFECTIONS
The organisms commonly encountered in surgical infections are the:
Staphylococci;
o Staph. pyogenes causes boils, carbuncle, styes, septic hand, breast abscess,
osteomyelitis, wound sepsis, deep abscess, septicemia and pyaemia
o Staph albus non pathogenic though can cause low grade inflammation in
dead tissues
Streptococci; the haemolytic(α and β) and the anaerobic are surgical concern.
The toxins produce include; haemolysin, leucocidin, fibrinolysin, erythrogenic toxin,
hyaluronidase, deoxyribonuclease. Β-haemolytic strept. E.g Strep Pyogenes causes
erysipelas, cellulitis, severe wound infection, tonsillitis, otitis media, scarlet fever,
puerperal sepsis. Α-haemolytic eg Strept. Viriadans cause intra oral and dental
infections, can contaminate burns or chronic skin ulcers, seed cardiac lesions
Pneumococci; lobar pneumonia or with other organisms causing
bronchopneumonia; they may also produce otitis media, sinusitis, meningitis,
acute primary peritonitis in young girls and wound infection.
Gram negative bacteria; E.coli, Pseudomonas, Proteus, Klebsiella, Haemophilus
Influenzae. The intestinal bacteria commonly encountered are Escherichia coli,
Pseudomonas, and Proteus organisms usually described as coliforms. In general,
those bacilli which do not ferment lactose eg Pseudomonas, proteus, salmonella
B.fragilis , V.cholerae are more pathogenic for man. In surgical practice, however, it
is the lactose fermenters eg Klebsiella, E. coli, Enterobacter ,which predominate.
o They infect wounds near the lower ileum and colon, the urinary tract and
bums.

[email protected] Page 7
o They are found in mixed infections and are commonly secondary invaders in
infections by staphylococci and streptococci
o They elaborate in their capsule a powerful endotoxin which causes pyrexia,
rigors and septic shock when released into the blood stream
Other gram negatives
Klebsiella organisms are gram-negative rods usually responsible for pneumonic
lesions and hepatic abscesses but may produce wound infections especially after
transplantation procedures.
Haemophilus influenzae often found in the healthy upper respiratory tract. It
causes acute epiglottitis, meningitis and bronchitis.
INFECTIONS OF SIGNIFICANCE IN SURGICAL PATIENTS
SURGICAL SITE INFECTION (SSI)
It is defined as infection present in any location along the surgical tract after a
surgical procedure within 3odays of procedure or up to 1 year after a procedure
that has involved the implantation of a foreign material.
Classification
Incisional SSI
o Superficial- those involving only the skin and subcutaneous tissue
o Deep - those involving deep soft tissues of the incision (e.g. fascial
and muscle layers)
Organ/space SSI - involves any part of the anatomy (e.g., organs or spaces)
manipulated
Criteria for defining an SSI as superficial
1. Infection occurs within 30 days after an operation.
2. The infection involves only the skin and the subcutaneous tissue adjacent to the
incision.
3. At least one of the following is present:
a purulent discharge from the surgical site,
at least one of the signs and symptoms of infection(pain, tenderness,
localized swelling, rednessor heat),
spontaneous dehiscence of the wound or deliberate opening of the
wound by the surgeon (unless the culture results from the site are
negative),

[email protected] Page 8
an abscess or evidence of infection on direct examinationor
reoperation, or histopathologic or radiological examination,
diagnosis of infection by a surgeon or attendingphysician.
Deep incisional SSI
Criteria:
1. They occur within 30 days after surgery with no implant
(up to 1 year after surgery if an implant is left in place),
2. The infections involve deep soft tissues, fascia and muscle layers,
3. At least one of the following:
Purulent drainage/organism isolated from an aseptically obtained culture.
Fascial dehiscence or deliberate opening of the fascia by a surgeon due to
signs of inflammation.
An abscess or other evidence of infection noted below the fascia during
reoperation, radiological examination or histopathology.
A surgeon declares that a deep incisional infection is present.
Organ/space SSI
These infections involve any part of the anatomy, in organs and spaces other than the
incision, which was opened or manipulated during operation.
Criteria
1. The infection occurs within 30 days after surgery or within 1 year if an implant is
present and the infection seems related to the operation.
2. The infection involves a joint/organ/space, or anatomic structures opened or
manipulated during the operation.
3. At least one of the following:
Purulent drainage from a drain placed into the organ/space.
An organism is isolated from a culture sample obtained aseptically from joint fluid
or deep tissue.
An abscess or other evidence of infection involving a joint, organ or space during
reoperation, radiological examination or histopathology.
A diagnosis of an organ/space SSI by a surgeon
[email protected] Page 9
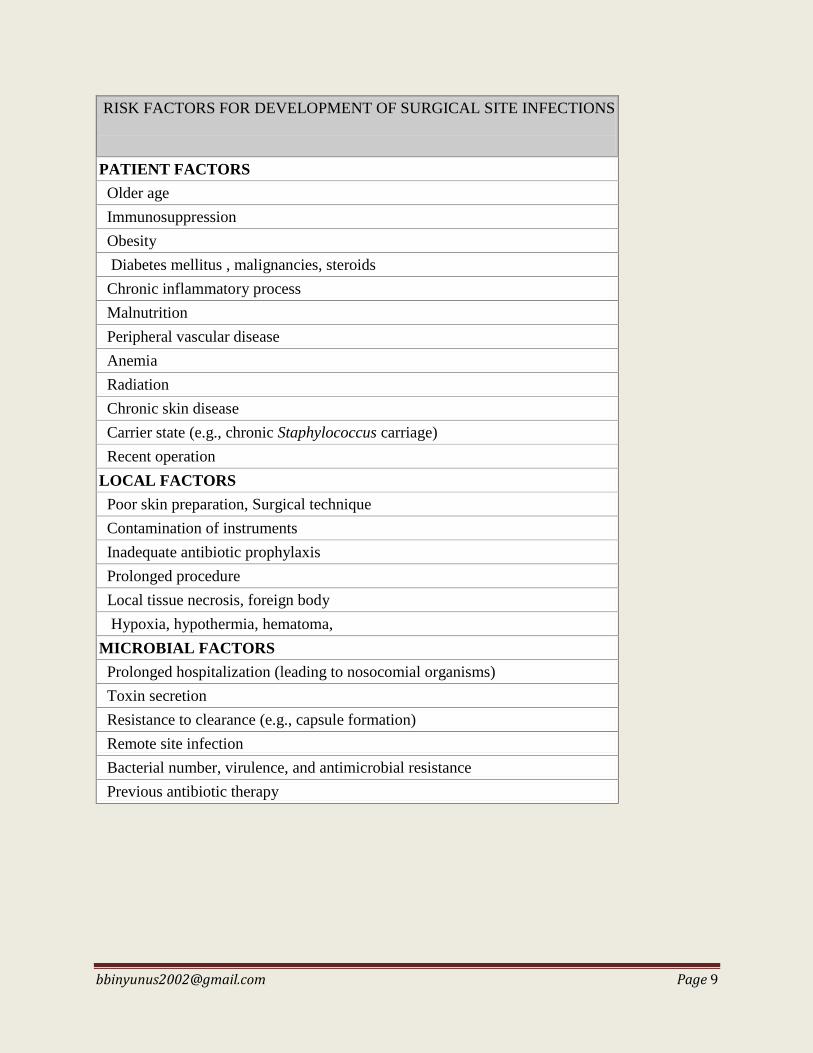
RISK FACTORS FOR DEVELOPMENT OF SURGICAL SITE INFECTIONS
PATIENT FACTORS
Older age
Immunosuppression
Obesity
Diabetes mellitus , malignancies, steroids
Chronic inflammatory process
Malnutrition
Peripheral vascular disease
Anemia
Radiation
Chronic skin disease
Carrier state (e.g., chronic Staphylococcus carriage)
Recent operation
LOCAL FACTORS
Poor skin preparation, Surgical technique
Contamination of instruments
Inadequate antibiotic prophylaxis
Prolonged procedure
Local tissue necrosis, foreign body
Hypoxia, hypothermia, hematoma,
MICROBIAL FACTORS
Prolonged hospitalization (leading to nosocomial organisms)
Toxin secretion
Resistance to clearance (e.g., capsule formation)
Remote site infection
Bacterial number, virulence, and antimicrobial resistance
Previous antibiotic therapy

[email protected] Page 10
Surgical Wound Classification According to Degree of Contamination
WOUND CLASS
DEFINITION
Clean (classI) Surgically incised, no break of asepsis.
An uninfected operative wound in which no inflammation is encountered
lumen is not entered.
Wounds are closed primarily and, if necessary, drained with closed drainage.
Surgical wounds after blunt trauma should be included in this category if they
meet the criteria
Infection rate <2%
Eg herniorrhaphy, lump excision, thyroidectomy, total joint athroplasty, lipoma
excision
Clean-
contaminated
(classII)
lumen is entered under controlled conditions and without unusual
contamination or minimal spillage
rate of infection is 5-10%
Eg Cholecystectomy, elective GI surgery (not colon), bladder surgery,
uninflamed appendectomy
Contaminated
(classIII) Open, fresh, accidental wounds. <4h
operations with major breaks in sterile technique
gross spillage from the lumen
and incisions in which acute, nonpurulent inflammation is encountered are
included in this category
Rate of infection is 15-20%
Eg appendectomy for inflamed appendix, Colorectal surgery, bowel resection
for infarcted bowel,
Dirty (class IV) Old traumatic wounds with retained devitalized tissue, perforated viscera,
abscess, fecal contamination, established infection b4 wound is made on skin.
Infection rate <40%

[email protected] Page 11
Preventive Measures for Surgical Site Infection
TIMING OF
ACTION
DETERMINANT IN WHICH THE PREVENTIVE MEASURE ACTS
Microorganism Local Patient
Preoperative
Shorten preoperative
stay
Antiseptic shower
preoperatively
Appropriate
preoperative hair
removal or no hair
removal
Avoid or treat remote
site infections
Antimicrobial
prophylaxis
Appropriate preoperative hair
removal or no hair removal Optimize
nutrition
Preoperative
warming
Tight glucose
control (insulin
drip)
Stop smoking
Intraoperative
Asepsis and
antisepsis
Avoid spillage in
gastrointestinal cases
Surgical technique:
Hematoma/seroma
Good perfusion
Complete débridement
Dead spaces
Monofilament sutures
Justified drain use
(closed)
Limit use of
sutures/foreign bodies
Delayed primary closure
when indicated
Supplemental
oxygen
Intraoperative
warming
Adequate fluid
resuscitation
Tight glucose
control (insulin
drip)
Postoperative
Protect incision for
48-72 hours
Remove drains as
soon as possible
Avoid postoperative
bacteremia
Postoperative dressing for 48-72
hours Early enteral
nutrition
Supplemental
oxygen
Tight glucose
control
(insulin drip)
Surveillance
programs
[email protected] Page 12
ACUTE INFECTIONS
Cellulitis
Phlegmon
Abscess
Pustule, furuncle and carbuncles
Hydradenitis supprativa
Infective gangrene
Tetanus
Necrotizing Fasciitis
Erysipelas
CELLULITIS
This is a diffuse inflammation of the subcutaneous tissue resulting from invasion
by pyogenic bacteria. It spreads along subcutaneous tissues and fascial planes.
Usually due to infection with ß haemolytic streptococcus- strep.pyogenes
(commonest cause) or Staph. aureus .Both produce enzymes that degrade tissue
and allow spread of infection.
Anaerobic streptococci (peptostreptococci) are part of the normal flora of the
mouth and gastrointestinal tract. In contrast to other streptococcal wound
infections, these organisms produce a thin, brown discharge, often with
crepitation in the infected tissue (anaerobic cellulitis).
Clinical features
• Cellulitis usually presents with a well demarcated area of inflammation
• Redness, heat, swelling and pain are the cardinal signs of inflammation
• Usually associated with malaise, fever and a raised white cell count
• If not rapidly treated it can progress to lymphangitis and lymphadenitis
• Localised areas of skin necrosis may occur
• Predisposing factors include
o Lymphoedema
o Venous stasis
o Diabetes mellitus
o Surgical wounds
Management
Rest and elevation of the affected limb andapplication of insulating dressings to
prevent heat loss arecomforting
Antibiotics
May initially be given orally
Intravenous administration if no rapid improvement

[email protected] Page 13
Benzylpenicillin and flucloxacillin are usually antibiotics of choice
where suppuration occurs surgical d rainage is indicated.
PHLEGMON
occurs when inflammation is relatively diffuse, i.e. like cellulitis, yet there are
small loci of necrotic tissue as well as multiple tiny pockets of pus. It is the
subsequent progression shortly to innumerable microscopic abscesses which
distinguishes a phlegmon from cellulitis. The usual causative organism is
staph. aureus, possibly in combination with virulent strains of Strep.
haemolyticus.
PUSTULE, FURUNCLE AND CARBUNCLES
These are forms of abscesses peculiar to the skin and result from infections of
hair follicles by Staph. Pyogenes. The tiny abscess thus formed is a pustule and
the inflammation may subside with egress of the bead of pus. The infection
frequently spreads to the surrounding subcutancous tissue before discharge of the
necrotic products and in this layer further extension may take place involving
several hair follicles. This is a typical boil or furuncle with a central core of
necrotic tissue which is discharged with the pus on ripening of the boil.
Carbuncles also result from infection of hair follicles but in areas such as the back
of the neck, back of the trunk, the hairy surfaces of the hand or fingers, the
lip and scalp, well-endowed with thick columns of subcutaneous fat projecting
around the follicles. Diabetics arc particularly prone to this complication. Word
meaning of carbuncle is charcoal. It is an infective ga11grane of skin and
subcutaneous tissue. Control of diabetes is essential using insulin. Antibiotics like
penicilhns, cephalosporins or depending on C/S is given. Drainage is done by a
cruciate incision and debridement or all dead tissue is done. Excision is done later.
Once wound granulates well, skin grafting may be required.
HYDRADENITIS SUPPRATIVA
It is a chronic infective and fibrous disease of the skin bearing apocrine sweat
glands. Apocrine sweat glands are coiled glands which open into the hair follicles.
Site of apocrine sweat glands:
• Axilla, Areola, Umbilicus, Groin, Perineum

[email protected] Page 14
Aetiology
• Obesity, smoking, Poor hygiene,Diabetes mellitus, Steroids.
Common bacteria involved are staphylococci, streptococci, staphylococcus
~aureus, propioni-bacterium acnes.
Clinical Features
Common in females 4 : 1.
Commonest site is axilla.
Multiple discharging sinusct., with nodules in the skin which is tender.
Induration due to fibrosis.
Investigation: Discharge study, Biopsy.
DDX: Tuberculous sinus, Malignancy (squamous cell carcinoma of skin).
Treatment
Antibiotics.
Excision of the involved area widely followed by skin grafting or flaps (radical
wound excision). Wounds in the affected area do not heal well by secondary
intention.
Antiandrogen drugs.
ABSCESS
Liquefaction of the dead tissue is produced by proteolytic enzymes contained in
the polymorphonuclear leucocytes and the mass of bacteria, leucocytes, exudate
and dying tissue residues thus formed is called pus. A pyogenic membrane of
granulation tissue soon forms separating the suppurating mass from the
contiguous normal tissues. (pyogenic abscess)
Other Types Pyaemic abscess, Metastatic abscess, Cold abscess due to chronic
infection like tuberculosis
Bacteria causing abscess
• Staph. aureus.
• Strept. pyogenes
• Gram-negative bacteria (E. coli, Pstudomonas, Klebsiella).
• Anaerobes.

[email protected] Page 15
Factors precipitating abscess formation
• General condition of the patient; nutrition, anaemia, age of the patient
• Associa1ted diseases: Diabetes, HIV, immununosuppression
• type and virulence of the organisms
• Trauma, haematoma, road traffic accidents
Clinical Features
Fever often with chills and rigors.
Localised swelling which is smooth, soft and fluctuant
Visible (pointing) pus.
Throbbing pain and pointing tenderness
Brawny induration around.
Redness and warmth with restricted movement around the joint
(Commonly cellulitis occurs first which eventually get localized to form abscess.)
Treatment
Abscess should be formed before draining. Exceptions for this rule are:Parotid abscess,
Breast abscess, Axillary abscess, Thigh abscess, Ischiorectal abscess
INFECTIVE GANGRENE
Gangrene is the death of large sections of tissue with superimposed putrefaction. It is
occasionally due to infection. It is either directly through microbial enzymes or indirectly
through thrombotic occlusion of blood vessels.
Infective gangrene is aerobic, anaerobic or synergistic. Aerobic gangrene; the causative
organisms are highly virulent strains of Strep. haemolyticus often occurring in epidemic
forms such as the classic hospital gangrene. A similar condition may result from certain
highly virulent strains of Staph. aureus - the scalded skin syndrome. P. aeruginosa
burn wound necrosis is another form of monobacterial aerobic gangrene.
Treatment: appropriate bactericidal chemotherapy and wide debridement of all necrotic
tissues.

[email protected] Page 16
Anaerobic gangrene/ Gas gangrene it is an infective gangrene caused by clostridial
organisms.
The causative organisms fall into two groups: those that breakdown starch or the
saccharolytic group (CI. Welchii or CI. Perfringens, Cl. novy, Cl. oedematiens, Cl. septicum)
and those which break down protein or the proteolytic group (Cl. Sporogenes and CI.
haemolyticus). The effects produce are as a result of exotoxins produced by organisms.
It usually takes two forms; clostridium myonecrosis (attacking muscles more serious
disease with high mortality) and clostridium welchii cellulitis (affecting subcutenous
tissue) commoner, not associated with cardiovascular disturbances.
Extensive necrosis of muscle with production of gas (hydrogen sulphide; nitrogen; carbon
dioxide) which stains the muscle brown or black. Usually muscle is involved from origin
to insertion. Often may extend into thoracic and abdominal muscles.When it affects the
liver it causes necrosis with frothy blood-foaming liver, is characteristic.
Clinical Features
Symptoms develop rapidly appearing within 10 -12 h after the injury.
Features of toxaernia, fever, tachycardia, pallor.
Wound is under tension with foul smelling discharge (sickly sweety odour).
Khaki brown colored skin due to haemolysis.
Crepitus can be felt.
Jaundice may be ominous sign and also oliguria signifies renal failure.
Prevention of gas gangrene
Proper debridement of devitalised crushed wounds.
Devitalized wou11ds should not be sutured.
Adequate cleaning of the wounds with H2O 2 and normal saline.
Penicillin as prophylactic antibiotic.
X-rays of the affected part may reveal in the soft tissues collections of gas which cannot
be demonstrated by palpation.
lnvestiga11ons
X·ray shows gas in muscle plane or under the skin.
LFT

[email protected] Page 17
Treatment
Resuscitate; correct hypotension, anaemia
Debridement
Irrigation and pack with H2O2 soaked guaze
Exhibition of antibiotics, usually penicillin in massive doses of up to 10
million units a day is essential. Clindamycin and metronidazole together
have been effective.
Administration of gas gangrene serum
Hyperbaric O2
SYNERGISTIC GANGRENE
It is the result of symbiotic infections from two or more bacterial species, and the
resultant lesion is far more fulminant than the regular lesion usually attributable to either
individual pathogen. The anaerobic partners are usually the primary pathogens
contributing the destructive enzymes. The aerobic organism extract the O2 from tissue
making it conducive for the anaerobes.
MeIeney's Gangrene or Cellulitis, a progressive recalcitrant ulcer produced by
symbiotic infections with the anaerobe Peptostreptococcus and the common
aerobe Staph. aureus.
Ulcerative gingivitis; Fusiformis bacillus and a spirochete.
Cancrum oris, or noma; Sets of gram-positive cocci and Bacteroides
melaninogenicus
Necrotizing fasciitis.; Combinations of coliforms, staphylococci, anaerobic
streptococci, peptostreptococci and Bacteroides species.
Fournier 's gangrene; Mixed aerobic-anaerobic organisms (including
Staphylococcus, micro-aerophilic Haemolytic streptococcus, E. coli, Fusobacterium
and Cl. welchi)
Treatment: antibiotics, debridement and hyperbaric O2

[email protected] Page 18
TETANUS
This is caused by a gram positive spore-forming obligate anaerobe, C. tetani, found in
the feces of humans and animals, and capable of prolonged survival in soil. Two exotoxins
are produced: tetanospasmin, a neurotoxin, and tetanolysin, a hemolysin.
PATHOGENESIS spores
Enters wound
Germinates in anaerobic media to releasing bacteria which multiply
Release of exotoxins
Tetanospasmin hemolysin
Hemolysis
Thru perineural sheath circulation
Enters the CNS, blocks toxemia (thru blood) blocks the NMJ by acting on the
cholinesterase at the anterior cholinesterase enzyme
horn cells
Causes hyperexcitability and aggravates the muscle spasm
reflex spasms of muscles
Once toxin fixed to the nerve
tissue, can no longer be neutralized
by antitoxin.

[email protected] Page 19
CLINICAL FEATURES
Symptoms
Jaw stiffness –lockjaw (usu the 1st symptom), pain and stiffness in the neck
and back muscles
Anxiousness, sweating
Headache, delirium, sleeplessness
Dysphagia
Dyspnoea
Signs
Trismus, due to spasm of masseter and pterygoids.
Risus sardonicus (smiling facies), due to spasm of the facial muscle-
zygomaticus major. Looks as if patient is smiling.
Neck rigidity.
Spasm and rigidity of all muscles.
Hyperreflexia.
Respiratory changes-due to laryngeal muscle spasm, infection,
aspiration.
Tonic-clonic convulsions.
Abdominal wall rigidity often with haematoma formation.
Severe convulsion may often lead to fractures, joint dislocations and
tendon ruptures.
Fever and tachycardia.
Retention of urine (due to spasm of urinary sphincter), constipation
(due to rectal spasm).
Rarely carditis, can cause cardiac arrest. Steroid is helpful.
Symptoms will be aggravated by stimuli like light, noise.
INCUBATION PERIOD
Time between the entry of spore and appearance of first symptom.
Usually 6-10 days.
Shorter the incubation period worser the prognosis and more severe the
course of the disease.

[email protected] Page 20
PERIOD OF ONSET
Time between appearance of first symptom and appearance of first
reflex spasm.
Shorter the period of onset worser the prognosis and vice versa.
If less than 48hrs, death is very likely
TYPES
Generalized (commonest)
Localized
Cephalic
Neonatal
DIFFERENT POSTURES IN TETANUS
Opisthotonus: Posterior muscles are acting more, so backward
bending.
Orthotonus: Straight posture. Both front and back muscles are acting
equally.
Emprosthotonus: Forward bending as front muscles are acting more.
Pleurosthotonus: lateral bending as lateral muscles act more.
STAGING OF TETANUS
Mildly ill: Rigidity, spasm, trismus and different postures.
Seriously ill: Spasm, rigidity, severe respiratory infections.
Dangerously ill: Cyanosis with respiratory failure and tonic-clonic
convulsions.
CAUSE OF DEATH IN TETANUS
Respiratory failure with aspiration pneumonia and ARDS
Severe carditis--an ominous sign
Mortality is 45-50%
PRINCIPLES FOR TETANUS PROPHYLAXIS
There are two types of immunization the active and passive. The active- toxoid- the dead
or modified organism introduce into the host body which stimulates the reticulo-
endothelial system to produce antibodies. More effective but it takes about 2-3 months to
be operational. The passive form- tetanus immune globuline- given to protect the

[email protected] Page 21
victim. It neutralizes the toxin, however it is less effective and may precipitate
anaphylaxis.
Toxoid administration; 0.5ml subcutaneously
Traditionally ; day 1, 6weeks, 6month and every 10years
Rapid method; day 1, day 4 and day 7. Using alum-precipitated toxoid.
Immunity is demonstrable in 28days.
Anti-tetanus serum: given IM, after a test dose of 0.1ml or 150 IU subcutaneously
Human ATS 250IU
Equine ATS 1500IU
TETANUS PROPHYLAXIS IN WOUND MANAGEMENT (see surgical
prophylaxis)
History of
tetanus
toxoid doses Clean, minor
wound
All other
wounds
Toxoid+ Immune
globulin
Toxoid+ Immune
globulin
Less than three
doses or
unknown
Yes No Yes Yes
Three or more
doses++
Yes if < 10 years
since last booster
No Yes if ≥ 5
years
since last
booster
No
Treatment ; aims of treatment are
Halt production of toxin
Neutralize circulating toxin
Removing source of infection
Controlling convulsion or spasms
[email protected] Page 22
General supportive measures and prevention of complications
Treatment is multidisciplinary
GENERAL MEASURES
• isolation
• Avoid noise and light
• A TG 3,000 units 1M
• ATS-50,000 IM and 50,000 IV-After test dose
• Antibiotics like inj penicillin 20 lacs 6th hourly or metronidazole
• Inj tetanus toxoid 0.5 ml 1M - to deltoid muscle
• IV fluids with TPN
• Urinary catheterization
• Nasogastric tube is passed to prevent aspiration initially, later for feeding
• Regular suction of throat
• Nasal oxygen when required
SPECIFIC MEASURES
• IV diazepam 20 mg 6th hourly
• IV phenobarbitone 30 mg 6th hourly
• IV chorpromazine 25 mg 6th hourly
• Endotracheal intubation and ventilator support or Tracheostomy if there is
severe respiratory secretions
• Steroids
• Bronchodilators like deriphylline
• Wound care- debridement, drainage, and local injection of A TG, wound is
not closed primarily.
ERYSIPELAS
This arises from cutaneous infection with strains of Strep. Pyogenes with a predilection
for the lymphatics. Rose pink rash with cutaneous lymphatic oedema develop. Vesicles
are formed which form eventually ruptures discharge. Site of predilection include face,
orbit, scrotum and umbilicus in infant. Toxemia is always a feature. Milian ear sign is
use to differentiate it from cellulitis wherein in cellulitis the ear lobe is spared. The
condition is associated with poor hygiene. Treatment is with penicillin.
[email protected] Page 23
NECROTISING FASCITIS
It is spreading inflammation of the skin, deep fascia and soft tissues with extensive
destruction, toxaemia.
Types;
Type 1-lt is due to mixed infection
Type 11- lt is due to Strep Pyogenes, usually due to minor trauma like
abrasions.
Occurs in immunocompromised patients
Often diabetic, alcoholics or intravenous drug abusers
Occurs at several characteristic sites
Limbs after cuts, abrasions or bites
Around postoperative abdominal surgical wounds
In the perineum secondary to anorectal sepsis
In the male genitalia (Fournier's gangrene)
• Polymicrobial infection involving the following:
Facultative aerobes
Streptococcal species or E. coli
Anaerobes
Exotoxins produce severe systemic toxicity
Clinical features
Often presents similar to cellulitis
Warning features include
o Severe pain - out of proportion to the clinical signs
o Severe systemic toxicity
o Cutaneous gangrene
o Hemorrhagic fluid leaking from a wound
MANAGEMENT
• Requires high clinical suspicion and early diagnosis
• Patients should be managed in high dependency unit
• Need fluid resuscitation and organ support
• Early surgical debridement is essential

[email protected] Page 24
• Requires excision well into apparently normal tissue
• Amputation or fasciotomies may be required
• Defunctioning colostomy may be required for perineal sepsis
• Antibiotic cover should include benzylpenicillin, metronidazole and
gentamycin
• Hyperbaric oxygen therapy may be of benefit.
NOSOCOMIAL INFECTION
(Hospital Acquired Infection)
It is an infection acquired because of hospital stay.
SOURCES
• Contaminated infected wounds.
• Urinary tract infection.
• Respiratory tract infection.
• Opportunistic infections.
• Abdominal wounds with severe sepsis spreading can occur from one patient
to another, through nurses or hospital staffs who fail to practice strict asepsis.
It is more common in
• Diabetics
• Immunosuppressive individuals
• Patients on steroid therapy a nd life-Supporting machines
• Instrumentations (indwelling catheter, IV cannula, tracheostomy tube)
• Patients with artificial prosthesis
ORGANISMS
Staphylococcus aureus is the commonest organism causing hospital
acquired wound infection. Others are Pseudomonas, Klebsella, E.
coli, Proteus,
Strept. pneumo, Haemophilus, Herpes,Varicella, Aspergillus,
Pneumocystis carinii are the commonest pathogens involved in hospital
acquired respiratory tract infection which spreads through droplets.
Klebsiella is the commonest pathogen involved in hospital acquired UTI
which is highly resistant to drugs.

[email protected] Page 25
MANAGEMENT
Most of the time, organisms involved are multidrug resistant, virulent and hence, cause
severe sepsis.
• Antibiotics.
• Isolation.
• Blood, urine, pus for culture and sensitivity to isolate the organisms.
• Blood transfusion, plasma or albumin therapy.
• Ventilator support.
• Maintaining optimum urine output.
• Nutritional support.
PREVENTION
• Isolation of patients with bodly infected open wounds, severe RTI/UTI.
• Following strict aseptic measures in out and in ward by hospital attendants.
• Proper cleaning and use of disinfectant lotions and sprays for bedpans,
toilets and floor.
• The precipitating causes has to be treated, along with caring for proper
nutrition and improving the anaemic status by blood transfusion.

[email protected] Page 26
WOUND AND WOUND HEALING
Wound is a break in the integrity of the skin or tissues often which may be
associated with disruption of the structure and function.
CAUSES
o Mechanical agents
o Chemical agents
o Radiation energy
o Pathogenic micro-organism
TYPES /CLASSIFICATION
Close- intact epithelial surface
o Contusion or bruise: injury to tissue subadjacent to surface
epithelium usually by blunt trauma. A subcutaneous
hematoma > 1cm is Ecchymosis
o Hematoma: is a localized collection of blood outside the blood
vessels, liquid or clotted within the tissue.
Open- break or disruption of skin or epithelium.
o Incision; a wound created with sharp instrument usually
during surgery
o Abrasion; loss of superficial layers of the epithelium
o Laceration: irregular tear-like wounds caused by some blunt
trauma or sharp instrument.
o Avulsion; injuries in which a body structure is forcibly
detached from its normal point of insertion. May be complete
(no connection between the injured and its original site) or
partial (tenuous or strands of tissue connect the tissue to site)
o Puncture: caused by pointed instrument with small entry e.g.
nail puncture
o Penetrating or perforating ; penetrating wounds enter a body
cavity such as the chest or abdomen perforating wounds
entirely pass through an organ or cavity and are characteristic
of firearms or missile injuries.
o Amputation;
o Gunshot; caused by a bullet or similar projectile driving into
or through the body. There may be two wounds, one at the
site of entry and one at the site of exit.
[email protected] Page 27
RANK AND WAKEFIELD CLASSIFICATION
o Tidy wounds
o Incised
o Clean
o Healthy tissues
o Seldom tissue loss
o Untidy wounds
o Crushed or avulsed
o Devitalised tissues
o Contaminated
o Often tissue loss
SURGICAL WOUNDS (see page 7)
o Clean
o Clean contaminated
o Contaminated
o Dirty
ACUTE AND CHRONIC WOUNDS
Acute wounds heal in a predictable manner and time frame. The process occurs with few,
if any, complications, and the end result is a well-healed wound.
A chronic wound is a wound that does not heal in an orderly set of stages and in a
predictable amount of time the way most wounds do; wounds that do not heal within
three months are often considered chronic. E.g. chronic leg ulcer
SIMPLE OR COMPLEX WOUND
In simple wounds, only skin is involved. Complex wounds, vessels, nerve, tendons, or
bones are involved.
WOUND MANAGEMENT (acute wound)
o History – timing, cause, type of injury, nature of force
o Examination – site, size, shape and depth, involvement of neighboring structures
o Initial resuscitation may be required
o Primary closure depends on the time of presentation; presentation within the
“Golden hours”- 6-8hours are primarily sutured otherwise delayed.
[email protected] Page 28
TREATMENT PROCEDURE
o Debridement
o Strict asepsis
o Wound closure
o Gentle tissue handling
o Minimize blood loss
o General measures
o Tetanus prophylaxis
o Immobilization and elevation
o Broad spectrum bactericidal antibiotics
WOUND HEALING
Wound healing is the process by which damaged tissues of the body are repaired by living
tissue. It is a natural restorative response to tissue injury.
PHASES
o HEMOSTASIS AND INFLAMMATORY
o Hemostasis precedes and initiates inflammation, with the ensuing release of
chemotactic factors from the wound site.
o Exposure of subendothelial collagen to platelets results in platelet aggregation,
degranulation, and activation of the coagulation cascade. Platelet -granules release
a number of wound-active substances, such as platelet-derived growth factor
(PDGF), transforming growth factor beta (TGF-b), platelet-activating factor
(PAF), fibronectin, and serotonin. There is also release of basic fibroblast growth
factor(b-FGF) and epidermal growth factor (EGF), VEGF, IGF-1.
o The process;
Start immediately after wounding and last 4-6days
1st vasoconstriction
2nd blood clot formation
3rd platelet aggregation
4th platelet degranulation- growth factors release, serotonin and other
chemo-attractants
5th vasodilatation- plasma,plasma proteins, C5a and C3a are poured into the
wound
6th chemotaxis

[email protected] Page 29
Granulocytes -1st 48hrs, attracted by inflammatory mediators
Monocytes –attracted by compliment, activated by fibrin, hypoxia,
acidosis, foreign body. Reach maximum at 24hrs and last for weeks.
Macrophage- 3rd day. Activated macrophage are essential for
proliferation, mediate angiogenesis,
o DESTRUCTIVE PHASE (DEMOLITION)
Immediately follows inflammatory phase
There is removal of dead and dying tissues from the wound
Neutrophils and monocytes migrate into the wound kill bacteria,
monocytes converts to macrophage.
The inflammatory and destructive phases are the LAG phases during which
wound has no tensile strength. A preparation phase, where foundation of
repair is laid down . 4-6days may be prolonged by infection.
o PROLIFERATIVE (COLLAGEN OR FIBROBLASTIC PHASE)
Tensile strength of wound increase. Rapidly from 1-6weeks and slowly upto
a year.
1st angiogenesis
2nd fibroblast formation
3rd formation of granulation tissue
4th re-epithelialization
o REMODELING (MATURATION PHASE)
Start from weeks to years
Blood vessels starts to disappear(endarteritis obliterans)
The fibroblasts starts to disappear
Type III collagen is gradually been replaced by type I
Tensile strength of scar gradually increase
TENSILE STRENGHT OF A WOUND; the capacity of the cut edge of a wound to hold
together and resist disruption. Very slight in the lag phase(4-6days) bridge only by
epithelium. It rises sharply to with peak rate at 14-15th day corresponds to fibroplasia in
the wound. After 15th day, the tensile strength but at slower rate after 6th weeks, for a year.
Attains 50% of pre-injury state at 3years. Lag phase of rectus sheeth is 7days. Increases
steeply for 3months, then more gradually for 1 year.

[email protected] Page 30
COLLAGEN; structural proteins in the extracellular space synthesis by fibroblast.
Tropocollagen is the procollagen molecule. Helical structure with glycine at every third
position, hydroxyproline(most abuntant) and hydroxylysine. Vitamin C is required in
the hydroxylation of proline and lysine. Copper is required to hydroxylate lysine. The 4
common types; I, II, III, IV seen predominantly in ‘SCAB’ (skin, connective tissues or
cartilage, arteries and basement membrane) respectively.
TYPES OF WOUND HEALING
Healing by primary intention
Healing by secondary intention
Healing by tertiary intention
Healing by primary intention
Wound edges opposed.
Normal healing.
Minimal scar
Healing In a surgically incised wound
■ By secondary intention
Wound left open.
Heals by granulation, contraction and epithelialisation
Increased inflammation and proliferation
Poor scar
Healing in a wound with much tissue loss.
■ By tertiary intention
also called delayed primary intention
Wound initially left open(4-5days)
Edges later opposed when healing conditions favourable
Heavily contaminated wound

[email protected] Page 31
FACTORS AFFECTING WOUND HEALING
Systemic
Age
Malnutrition
Trauma
Metabolic diseases
Immunosuppression
Connective tissue disorders
Smoking
Medications; Steroids, cytotoxic.
Local
Mechanical injury
Infection
Edema
Ischemia/necrotic tissue
Topical agents
Ionizing radiation
Low oxygen tension
Foreign bodies
Site of the wound; pressure, repeated movement
COMPLICATIONS OF WOUND HEALING
Wound infection, septicaemia.
Chronicity
Abnormal scars: hypertrophic scar, keloid.
Contracture
hyperpigmentation
Implantation cyst
Neoplastic change
Weak scar
Cicatrization
[email protected] Page 32
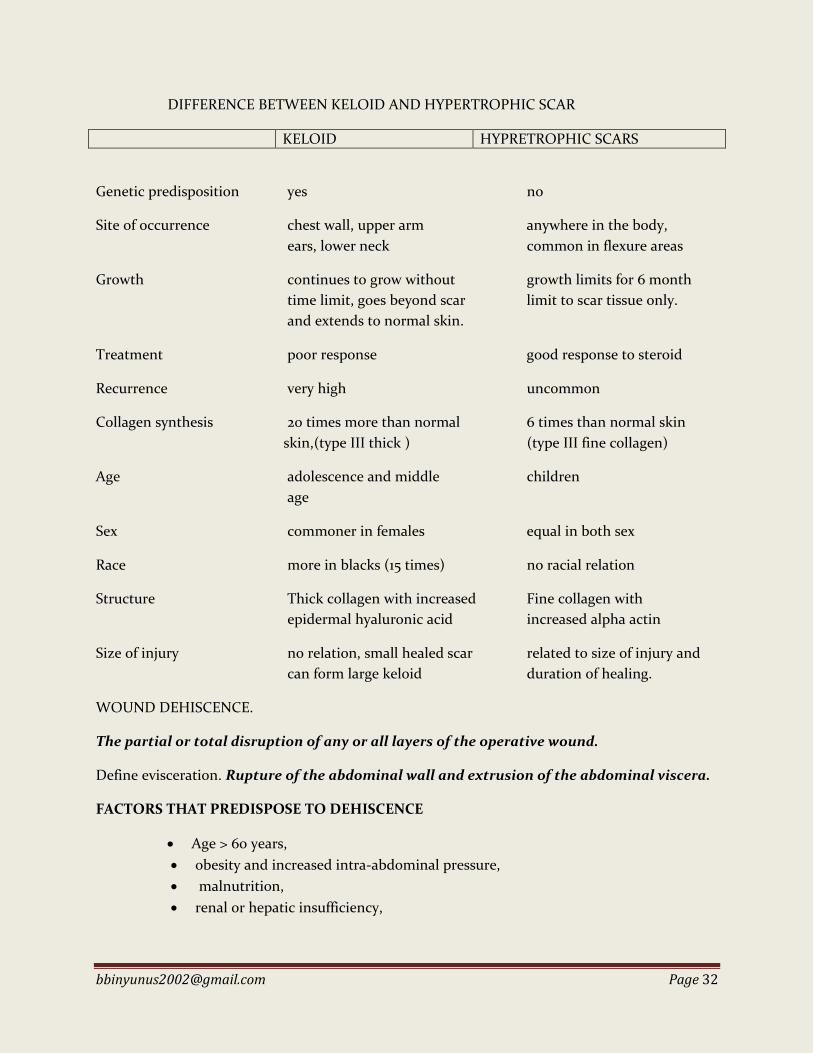
DIFFERENCE BETWEEN KELOID AND HYPERTROPHIC SCAR
KELOID HYPRETROPHIC SCARS
Genetic predisposition yes no
Site of occurrence chest wall, upper arm anywhere in the body,
ears, lower neck common in flexure areas
Growth continues to grow without growth limits for 6 month
time limit, goes beyond scar limit to scar tissue only.
and extends to normal skin.
Treatment poor response good response to steroid
Recurrence very high uncommon
Collagen synthesis 20 times more than normal 6 times than normal skin
skin,(type III thick ) (type III fine collagen)
Age adolescence and middle children
age
Sex commoner in females equal in both sex
Race more in blacks (15 times) no racial relation
Structure Thick collagen with increased Fine collagen with
epidermal hyaluronic acid increased alpha actin
Size of injury no relation, small healed scar related to size of injury and
can form large keloid duration of healing.
WOUND DEHISCENCE.
The partial or total disruption of any or all layers of the operative wound.
Define evisceration. Rupture of the abdominal wall and extrusion of the abdominal viscera.
FACTORS THAT PREDISPOSE TO DEHISCENCE
Age > 60 years,
obesity and increased intra-abdominal pressure,
malnutrition,
renal or hepatic insufficiency,

[email protected] Page 33
diabetes mellitus, use of corticosteroids or cytotoxic drugs, and radiation have
been implicated in wound dehiscence.
Infection also plays an important role; an infective agent is identified in more than
half of wounds that undergo dehiscence.
Despite these excuses, the most important factor in wound dehiscence is the
adequacy of closure. Fascial edges should not be devitalized. Ideally the linea alba
sutures should be placed neither too laterally nor too medially. Excessive lateral
placement may incorporate the variable blood supply of the rectus abdominis
muscle and compromise fascial circulation. Excessive medial placement misses
the point of maximal strength at the transition zone between the linea alba and
rectus abdominis sheath. In addition, sutures should be tied correctly without
excessive tension, and suture material of adequate tensile strength should be
chosen.
WHEN DOES WOUND DEHISCENCE OCCUR
It may occur at any time after surgery; however, it is most common between the 5th and 10th
postoperative days, when wound strength is at a minimum.
SIGNS AND SYMPTOMS OF WOUND DEHISCENCE
Normally a ridge of palpable thickening (healing ridge) extends about 0.5 cm on each side
of the incision within 1 week. Absence of this ridge may be a strong predictor of
impending wound breakdown.
More commonly, leakage of serosanguineous fluid from the wound is the first sign.
In some instances, sudden evisceration may be the first indication of abdominal wound
dehiscence.
The patient also may describe a sensation of tearing or popping associated with coughing
or retching.
MANAGEMENT OF WOUND DEHISCENCE.
If the dehiscence is not associated with infection, elective reclosure may be the
appropriate therapeutic course.
If the condition of the patient or wound makes reclosure unacceptable, however, the
wound should be allowed to heal by second intention. An unstable scar or incisional
hernia may be dealt with at a later, safer time.
Dehiscense of a laparotomy wound with evisceration is a surgical emergency with a
reported mortality of 10-20%.
[email protected] Page 34
o Initial treatment in this instance consists of appropriate resuscitation while
protecting the eviscerated organs with moist towels;
o the next step is prompt surgical closure. Exposed bowel or omentum should be
lavaged thoroughly and returned to the abdomen
o The abdominal wall should be closed; and the skin wound should be packed open.
Vacuum-assisted wound closure may be valuable in select cases.

[email protected] Page 35
SUTURES AND SUTURE MATERIALS
DEFINITION
A suture is a strand of material use in approximation of wound edges or ligation of blood
vessel.
PROPERTIES OF AN IDEAL SUTURE
• Adequate tensile strength
• Good knot holding property
• Should be least reactive (inert)
• Easy handling property
• Should have less memory
• Should be easily available and cost effective
CLASSIFICATION
Absorbable (natural or synthetic)
These are broken down in the body and eventually absorbed by digestion by lysosomal enzyme of
white blood cells or by hydrolysis (synthetic absorbable sutures).
Non-absorbable (natural or synthetic)
They effectively resists enzymatic digestion. They are used in tissues that heal more slowly, or if a
very secure tightening is required. They are either left in the body, where they become embedded
in the scar tissue, or they are removed when healing is complete.
NATURAL ABSORBABLE
o Catgut
o Plain catgut is derived from submucosa of jejunum of sheep.
o - It is yellowish white in colour.
o - It is absorbed by inflammatory reaction and phagocytosis-absorption time
is 7 days.
o - It is used for subcutaneous tissue, muscle, circumcision in children.
Chromic catgut is catgut with chromic acid salt.

[email protected] Page 36
- It is brown in colour.
- Its absorption time is 21 days.
- It is used for suturing muscle, fascia, external oblique aponeurosis, ligating
pedicles, etc.
o Collagen
This is produced from the collagen fibers from the bovine flexor tendon in
both plain and chromic form, and can be applied in the same fields as
surgical gut.
SYNTHETIC ABSORBABLE
o Polyglycolic acid
o Dexon (Polyglycolic acid) is synthetic absorbable suture material like
vicryl. It is creamy yellow in colour (braided).
o It has an excellent tensile strength (remaining unchanged for about 3
weeks) and excellent knot security. It is completely absorbed in 60-90
days.
o Polyglactin
o Vicryl (Polyglactic acid):
o - It is synthetic absorbable suture material.
o - It gets absorbed in 90 days.
o - Absorption is by hydrolysis.
o - It is violet in colour (braided).
o - It is multifilament and braided.
o - It is very good suture material for bowel anastomosis,
o suturing muscles, closure of peritoneum.
o Poly-p-dioxanone
o PDS (Poly Dioxanone Suture material) is absorbable suture material.
o It is creamy in colour with properties like vicryl.
o It is costly but better suture material than vicryl.
o The tensile strength on day 14 is 70%. Absorption is minimal up to 90 days,
but complete within 6 months.
o Maxon (Polyglyconate) monofilament.
o Monocryl (Polyglecaprone) monofilament.
o Biosyn (Glycomer) monofilament
NATURAL NON-ABSORBABLE
o Silk
o Silk is natural, multifilament, braided, non-absorbable suture material derived
from cocoon of silkwormlarva. It is black in colour. It is coated suture material
to reduce capillary action.

[email protected] Page 37
o Linen
o This is a twisted thread, which is weaker than silk; however, it is straightened
when wet. Therefore, it must be dipped into saline solution before use.
o Cotton
o This is made from twisted cotton fibers. It should also be dipped into saline
solution.
o Stainless steel
o This causes almost no tissue reaction. It is manufactured in monofilament and
twisted forms.
o It is rarely used because it is difficult to handle, it may break up and it can easily
cut tissues.
SYNTHETIC NON-ABSORBABLE
o Polyesters
o They give the strongest sutures, apart from surgical steel.
o monofilament (Miralene or Mirafil)
o braided, either uncoated (Dacron, Mersilene or Dagrofil), or coated with Teflon
(Ethiflex or Synthofil)
o Polyamide (Nylon)
o Its tensile strength for 1 year is 80%, for two 2 years is 70% and for 11 years 66% and
it causes only a minimal inflammatory response.
o Polypropylene
o Polypropylene (Prolene) is synthetic, monofilament suture material.
o It is blue in colour.
o It has got high memory. (Memory of suture material is recoiling tendency after
removal from the packet. Ideally suture material should have low memory.)
(Prolene mesh used for hernioplasty is white in colour).
o it causes only a minimal tissue reaction, it has a high tensile strength (100% for 2
years) and it holds knots better than most other synthetic materials.
o It can also be applied in infected fields.
NUMBERING OF SUTURE MATERIAL
2-Thick. For pedicle ligation.
1-
0-zero.
1-zero.
2-zero. For bowel suturing.
3-zero.
4-zero.
5-zero. For vascular anastomosis.

[email protected] Page 38
6-zero.
7-zero.
8-zero.
9-zero. For ophthalmic surgery. Requires operating microscope.
TYPES OF SUTURING
Interrupted
o Simple
o Vertical mattress
o Horizontal mattress
Continuous
o Simple
o Locked
o Subcuticular
o Purse-string
TYPES OF KNOT
Reef knot or Viennese knot
Granny knot
Surgeons knot

[email protected] Page 39
CUTENEOUS ULCERS
ULCER is a sustained breach in the continuity of the surface epithelium- skin and mucous
membrane.
PARTS
1. Margin the line of demarcation between the ulcer and the intact skin.
o Healing margin shows typical bluish line of growing epithelium which is squamous
without cornification. Margin of a healing ulcer shows 3 zones
Outer –white
Intermediate – blue
Inner – red
o Spreading ulcer margin shows irregular in malignant and inflamed in infected.
o Chronic non-healing ulcer shows fibrous thick white margin without the bluish
growing epithelium. (NB; margin commonly stated in conventional books)
2. Edge is the mode of union between the floor and the margin of the ulcer.
Slopping –healing, venous ulcers.
Punched out – trophic ulcers eg syphilitic
Undermined – tuberculous
Raised – rodent or basal cell ca.
Everted – squamous cell ca.
3. Floor the exposed surface of the ulcer. i.e the part which can be seen within the edge of
the ulcer.
Healing ulcer shows pink or red granular granulation tissue
Chronic ulcer shows pale flat and smooth granulation tissue
Infected ulcer shows unhealthy granulation tissue- contains slough.
Tuberculous ulcer has afloor with watery or apple jelly granulation tissue
A floor may also show hypertrophic granulation tissue- sprouting flesh.
4. Base the area on which the ulcer rest. The base is palpated through the floor of the ulcer
for;
Mild induration may be felt in any chronic ulcer
Marked induration is almost diagnostic of malignant ulcer
Mobility of the ulcer over the underlying structure
CLASSIFICATION
Specific
Non-specific
Malignant

[email protected] Page 40
SPECIFIC ULCERS
They are caused by specific organisms e.g. mycobacterium ulcerans bacilli, treponema pallidum or
Pertenue. The edge is characteristic for each type.
Tropical ulcers; synergistically by the anaerobic Fusobacteria (Bacteriodes
fusiformis) and the aerobic Borrelia vincenti. Commoner in males, risk factors
include malnutrition, walking bare-footed. Over 95% occur in the lower part of the
leg. Organisms are transmitted by flies.
Tuberculous; mycobacterium tb
Burili ; mycobacterium ulcerans
Syphilitic; (gummatous ulcer); Treponema pallidum
Yaws; Treponema pertenue
(NB; see text for details of specific ulcers )
NON- SPECIFIC
They have essentially the same feature of a sloping edge, but the underlying aetiologies are
varied. They are the commonest ulcers.
1. Traumatic ulcers. 2. Pyogenic ulcers. 3. Ulcers of vascular origin:
(i) Venous (gravitational) ulcers. (ii) Arterial ulcers. (iii) Decubitus ulcers. (iv) Pressure sores.
4. Neurotropic (trophic) ulcers: (i) Leprosy. (ii) Diabetic neuropathy. (iii) Cord lesions. (iv) Peripheral neuropathies. (v) Syringomyelia.
5. Ulcers associated with metabolic or systemic disease: (i) Diabetic ulcers. (ii) Haemoglobinopathic ulcers. (iii) Ulcers of spherocytosis. (iv) Ulcers of ulcerative colitis.
MALIGNANT ULCERS
Squamous cell ca
Malignant melanoma
Basal cell ca
Kaposi sarcoma
Penetrating malignant tumour

[email protected] Page 41
PHASES
A non- specific ulcer goes through the following phases
I. Acute or infective phase / extension
In this the initial phase, the ulcer is painful
The sloughing floor is covered with purulent discharge in which different types of
bacteria may be identified
Base is indurated and fixed
Surrounding skin is inflamed
II. Transition phase
The slough separates, the pus drains,
infection subsides, granulation tissue grows and the floor becomes clean and
pinkish-red.
The edge, which is sloping, has a thin bluish-white layer of young epithelium
growing inwards.
The surrounding skin is slightly hyperaemic or nonnal.
Induration diminish
III. Reparative or healing phase
The ulcer is now painless.
The healthy granulation tissue fills the floor and the epithelium grows from the
edge at the rate of 1 mm/day to cover the floor.
IV. Chronic, indolent or callous phase
Some ulcers may enter a chronic phase and remain unhealthy for a long time
because of secondary infection, defective circulation, poor general condition,
foreign body, lack of rest, malignant transformation.
Unhealthy granulation tissue
Offensive discharge, indurated base ragged edge and inflamed surrounding skin.
COMPLICATIONS OF NON-SPECIFIC ULCERS
1. Septicaemia 2. Lymphangitis 3. Lymphadenitis 4. Wasting 5. Tetanus 6. Lymphoedema:- Recurrent lymphangitis may lead to below-knee lymphoedema of varying degrees. 7. Periostitis: - When the ulcer is close to bone, periostitis occurs and if persistent may lead to new bone format ion at the base of the ulcer. 8. Malignant change:- Long-standing ulcers and unstable scars may undergo squamous carcinomatous change. 9. Deformities of the foot or ankle may occur if deep tissues are involved in the fibrosis.

[email protected] Page 42
TREATMENT OF NON-SPECIFIC ULCERS
1. ACUTE ULCERS 1. In the acute phase, the patient is admined for bed rest and the footend of the bed elevated. 2 Wound swab is done for gram staining, culture and sensitivity of any organisms cultured. 3. Broad-spectrum antibiotics are started while awaiting the results of the culture and sensitivity tests. 4. Tetanus booster dose is given to prevent tetanus infection. 5. The wound is cleansed regularly with normal saline. Acetic acid is effective for cleansing wounds suspected infected with pseudomonas. 6. Crepe bandage is applied firmly from the toes to the knee to promote lymphatic and venous drainage. 7. The affected limb is splinted in the position of function to prevent formation of contracture. 8. Physiotherapy is started early to prevent wastage of muscle and contractures. 9. Once the ulcer becomes healthy, it is grafted with split skingrart. 10. Where there is an infected slough, appropriate antibiotics are started and the slough removed either with saline soaks or by sloughectomy i.e. surgical excision of the slough. The wound is then cleansed regularly until healthy granulation tissue is formed. A wound swab is then taken for culture to rule out streptococcal infection before grafting with split skin.
2. CHRONIC ULCERS These ulcers may be excised and then grafted with split-skin graft or covered with a flap.
3. ADVICE AFTER DISCHARGE
The patient is advised on foot hygiene.
He is advised to use pressure dressing from the toes to the knee to promote lymph and venous drainage where there is excessive scarring.
Farmers are advised to wear protective clothing and boots.
The patient should seek prompt treatment for any abrasion to the affected limb.
DIFFERENTIAL DIAGNOSIS OF AN ULCER The diagnosis is arrived at after: 1. Careful history. 2. Clinical examination and 3. Investigations. HISTORY Mode of onset Duration Pain Progress of the ulcer: Painful regional lymph lIodes Symptoms or past history suggestive of; Diabetes

[email protected] Page 43
Tuberculosis DVT Varicose vein Haemoglobinopathy Neuropathy Yaws Syphilis EXAMINATION
a. The ulcer
Number
Site
Size
Shape
Edge
Floor
Base
Discharge
Surrounding skin
State of local circulation
Arterial pulsation of the limb
State of innervation
Regional lymph node b. General physical examination
INVESTIGATIONS I. Urine - for sugar and albumin. 2. Blood , (i) V.D.R.L. for syphilis. (ii) Sugar level for diabetes mellitus (iii) Haemoglobin genotype for haemoglobinopathy . (iv) Haemoglobin level to exclude anaemia. (v) Plasma protein levels (vi) Mantoux test. (vii) E.S.R. 3. Bacteriology of the ulcer - for special organisms;Mycobacteria, Fusobacteria, Borrelia 4. Radiology: (i) Plain films of ulcer to see any bony changes or calcification. (ii) Duplex Doppler scanning, arteriography or venography for vascular disorders. (iii) Plain films of the chest should be done also if tuberculosis or malignancy is suspected. 5. Biopsy of ulcer - may be the final step in definitive diagnosis. 6. Other tests may be done as indicated by the probable cause of the ulcer e.g. Lepromin test in suspected leprosy.

[email protected] Page 44
FLUID AND ELECTROLYTES Fluid and electrolyte management is paramount to the care of the surgical patient. Changes in both fluid volume and electrolyte composition occur preoperatively, intraoperatively, and postoperatively, as well as in response to trauma and sepsis.
BODY FLUIDS TOTAL BODY WATER- (TBW); Water constitutes approximately 50 to 60% of total body weight. It is primarily a reflection of body fat. Lean tissues such as muscle and solid organs have higher water content than fat and bone. TBW depends on age, sex, obesity. It is lower in the aged and obese. Male – 60% body weight Female -50% . TBW--60%
ICF40% ECF20%
Intravascular(plasma) 4%
Extravascular 16%
Transcellular 1%
Interstitial 15%
TBW in full term neonate 75%, ECF 35%. The ratio of surface area to weight in neonate is larger
with more insensible loss. In preterm, TBW is 95%. By the age of 2years, it is corrected to TBW
65%, ECF 20%.
BODY ELECTROLYTE
INTRACELLULAR;
K+ 14Ommol/l the most important cation
Na+ 8mmol/l
Mg2+ 15mmol/l
Phosphate 26mmol/l
most important anions
Protein 9mmol/l
EXTRACELLULAR
Na+ 135-145mmol/l most important cation Mg2+ 0.7-0.9mmol/l
[email protected] Page 45
K+ 3.6-5.2mmol/l Cl- 95-105mmom/l
Ca2+ 2.1-2.6mmol/l HCO3- 24-29mmol/l
24HRS FLUID AND ELECTROLYTE REQUIREMENT IN THE TROPICS
FLUID
LOSS
Insensible loss 1700ml
Urine 1500ml
Faeces 200ml
Total 3400ml
GAIN
Endogenous production
200ml
NET 3200ml
Surgical patient usually requires parenteral and not likely to pass stool, hence 24hrs requirement is
3000ml. for 10C rise in temperature, 12% of daily requirement is added to compensate for water loss in
sweating.
ELECTROLYTE
Na+ 130-140mmol/l
Urine 114mmol/l
Sweat 10-16mmol/l
Faeces 10mmol/l
K+ 60mm0l/l
Urine 50mmol/l
Faeces 10mmol/l
Sweat – negligible
As surgical patient is unlikely to pass stool, daily Na+ is 130mmol and K+ 50mmol.
Energy should be replace since patient is on NPO, and body store of glycogen (400g ≈1600kcal) is used
up in the 1st day of starvation, then 75-90% is provided from combustion of fat and protein. 100-150g of

[email protected] Page 46
exogenous glucose is given to reduce gluconeogenesis to the minimum and acidosis prevented. 2L of 5%
DW contains 100g of glucose. VitC100-200g essential for wound healing and scavenger of free radicals
Bcomplex aids protein and CHO metabolisms. Other mineral and trace element are add prolong treatment
DISTURBANCE OF FLUID BALANCE
Extracellular volume deficit is the most common fluid disorder in surgical patients and can be either
acute or chronic. Acute volume deficit is associated with cardiovascular and central nervous system signs,
whereas chronic deficits display tissue signs, such as a decrease in skin turgor and sunken eyes, in
addition to cardiovascular and central nervous system signs. The most common cause of volume deficit in
surgical patients is a loss of GI fluids from nasogastric suction, vomiting, diarrhea, or enterocutaneous
fistula. In addition, sequestration secondary to soft tissue injuries, burns, and intra-abdominal processes
such as peritonitis, obstruction, or prolonged surgery can also lead to massive volume deficits.
Dehydration is loss of water and electrolyte especially sodium. Acute dehydration is loss of ECF as in
intestinal obstruction, peritonitis, diarrhea . in chronic dehydration, there is loss of both ECF and ICF as
in GOO. There is loss of large amount of K+.
Shock ensues with ECF loss ≥ 3.5L
Signs and Symptoms of Volume Disturbances
System Volume Deficit Volume Excess
Generalized Weight loss Weight gain
Decreased skin turgor Peripheral edema
Cardiac Tachycardia Increased cardiac output
Orthostasis/hypotension Increased central venous pressure
Collapsed neck veins Distended neck veins
Murmur
Renal Oliguria —
Azotemia
GI Ileus Bowel edema
Pulmonary — Pulmonary edema
Extracellular volume excess may be iatrogenic or secondary to renal dysfunction, congestive heart failure,
or cirrhosis.
FLUID AND ELECTROLYTE THERAPY
Extracellular volume deficit leads to loss of fluid and electrolyte and the principle of correction is through
Correction of deficit

[email protected] Page 47
Correction of ongoing loss
Maintainace fluid
Monitoring of treatment
Parenteral solutions
Commonly used are;
0.9% saline
Na+ 154mmol
Cl- 154mmol
mOsmo 308
Ringer’s lactate
Na+ 130mmol
K+ 4mmol
Ca2+ 4mmol
Cl- 111mmol
HCO3- 27mmol
mOsmo 273
full strength darrows
Na+ 124mmol
K+ 36mmol
Cl- 104mmol
HCO3- 56mmol
mOsmo 320
4.3% glucose in 1/5 saline
Na 30.8mmol
Cl 30.8mmol
Glucose 43g
5% dextrose water

[email protected] Page 48
50g glucose
Correction of dehydration (deficit)
IV access secured, blood samples taken for U/ECr, PCV
Crystalloid are started ; ringers lactate, N/S IL for 30-45min
Pass urethral catheter, empty the urinary bladder, then monitor urine output
Then re-assess patient, if parameters(PR,BP, urine output ) inadequate, repeat IV fluid IL over 30-45min,
and reassess as appropriate upto 4L, then give frusemide. Otherwise if adequate, place on maintenance of
1L 8hrly.
During resuscitation, the following parameters are checked for;
Hourly urine output 30-50ml/hr (0.5-1ml/kg/min)
Half-hourly P.R and BP
Skin tugor, moistness of tongue , fill of subcutaneous veins
Frequent auscultation of the lungs and monitoring of JVP to prevent overhydration or quickly
diagnose and treat if occur.
CVP 10-15mmHg
Maintenance
With correction of deficit and patient is making adequate urine, PR,BP,CVP all within normal limit,
patient is placed on daily maintenance. 1L 8hrly, 2L of 5%DW,1L of N/S and 3g of KCL added to the
fluid. However, ongoing loss is taken into consideration and added to the total maintenance fluid.
Ongoing loss
Ongoing GI losses such as N-G tube drainage, drainage from enterocutenous fistulae, diarrhea, vomiting
are estimated and added into maintenance fluid.
Monitoring
Input –out put chart
Serum U/ECr must be checked daily and deficiency corrected,12hly for critically ill patient.
Reapeat Hb/PCV after rehydration and correct if depleted.
State of hydration assessed daily; urine output of ≥ 1000ml is indicative of good hydration
Monitoring for overload
o Frequent auscultation
o CVP

[email protected] Page 49
ELECTROLYTE DISTURBANCE
SODIUM
HYPONATREMIA-
serum sodium level of ≤130mmol/L. Manifest clinically when serum Na<125mmol/L
Symptoms; Irritability, cerebral oedema – headache, vomiting and convulsion, pulmonary
congestion, convulsion is seen in severe hyponatremia < 120mmol.
Causes; vomiting or N-G aspiration, diarrhea, internal fluid shift, enterocutenous fistulae,
excessive sweating, polyuria.
Treatment ; IV normal saline. Treat the cause. In the presence of cerebral oedema, IV diuretics is
given.
HYPERNATREMIA
Hypernatremia results from either a loss of free water or a gain of sodium in excess of water.
Like hyponatremia, it can be associated with an increased, normal, or decreased extracellular
volume.
Types of Hypernatremla
• Euvolemic (pure water loos)
• Hypovolaemic (among the loss of water and sodium, more water is lost than sodium)
• Hypervolaemic (both sodium and water gain but sodium gain is more than water gain).
Hypernatremia could either be hypervolemic(caused either by iatrogenic administration of
sodium-containing fluids, including sodium bicarbonate. Urine Na conc. > 20mEq/L),
normovolemic(result from renal causes, including diabetes insipidus, diuretic use, and renal
disease) or hypovolemic(nonrenal water loss from the GI tract or skin, although the same
conditions can result in hypovolemic hypernatremia<20mEq/L)
Management is restriction of saline and sodium. Treatment of pulmonary oedema.
Correction is slowly to prevent cerebral oedema and hyperglycemia. N/S then 1/2strength saline
and later 5% dextrose.

[email protected] Page 50
POTASSIUM
Normal value is 3.5-5.6mmol/L
Hypokalemia
Can occur suddenly in a diabetic coma patient treated with insulin and saline.
Gradual loss is seen in;
• Diarrhoea of any causes, villous tumour of the rectum, ulcerative colitis.
• After trauma or surgery.
• Pyloric stenosis with gastric outlet obstruction.
• Duodenal fistula, ileostomy.
• After uretero sigmoidostomy.
• Insulin therapy.
• Poisoning.
• Drugs like beta agonists
Clinical Features
• Slurred speech.
• Muscular hypotonia.
• Depressed reflexes.
• Paralytic ileus.
• Weakness of respiratory muscles.
• Cardiac arrhythmias.
• Inability to produce concentrated urine and so causes nocturia and polyuria.
ECG shows prlonged QT interval, depression of the ST segment and inversion of T wave,
prominent U wave, ectopic beats. Often hypokalaemia is associated with alkalosis. Serum
potassium will be decreased.
Treatment
o Deficit ×weight ×0.6
o Using KCl in 5% dextrose or N/S slowly under ECG monitoring
o Patient making adequate urine
o Not > 20mmol/hr
o Not > 40mmol/L
o Not >120mmol/day
o Not given in bolus.
HYPERKALEMIA
Serum K+ > 6mmol/L
Causes:

[email protected] Page 51
o Trauma
o Burns
o Sepsis
o Shock
o Acidosis
o Massive transfusion of old blood
o Excessive supplement
o Drugs : K sparing diuretics, ACE inhibitors, Aminoglycoside
Clinical features
o Nausea, vomiting, diarrhea, muscle weakness
ECG;
o peak T wave,
o absent P wave,
o widened QRS,
o ventricular arrhythmias,
o fibrillation, cardiac arrest.
Treatment
o Under ECG monitoring
o Sodium bicarbonate 80-100mmol over 10min to combat acidosis
o 10% calcium gluconate to prevent cardiac arrest
o Glucose under influence of insulin uses K to form glycogen;
10IU of soluble insulin in 1L of 5%dextrose is given IV or 100ml of 20% dextrose in
30min
o Ion exchange resin, calcium resonium 15-30mg 6hly or 30g rectally is given to exchange Ca for
K.
o Β-2 agonist eg neubulised or IV salbutamol increase uptake of K
o Hemodialysis or peritoneal dialysis.
HYPERMAGNESAEMIA
It is rare. Serum magnesium > 2.5 mEq/L
Causes
• Advanced renal failure treated with magnesium
containing antacids, diabetic ketoacidosis.
• Intentionally produced hypermagnesaemia while treating pre-eclampsia.

[email protected] Page 52
Clinical Features
• l.oss of tendon reflexes (commonest).
• Neuromuscular depression.
• Flaccid quadriplegia.
• Respiratoty paralysis.
• Somnolence.
• Hypotension.
HYPOMAGNESAEMIA
• Serum magnesium< 1.5 mEq/L
Causes
o Malnutrition, alcohol.
o Large GI fluid loss.
o Patients on total parenteral nutrition.
Clinical Features
o Hypereflexia.
o Muscle spasm.
o Parasthesia.
o Tetany.
It mimics hypocalcaemia. It is often associated with hypokalaemia and hypocalcaemia.
Two gram (16 mEq) of magnesium sulphate slow intravenously, in 10 minutes. Later maintenance dose
of 1 mEq/kg/ day as slow continuous infusion is given/ oral magnesium is needed.
CALCIUM
The vast majority of the body's calcium is contained within the bone matrix, with <1% found in the ECF.
Serum calcium is distributed among three forms: protein found (40%), complexed to phosphate and other
anions (10%), and ionized (50%). It is the ionized fraction that is responsible for neuromuscular stability
and can be measured directly. When total serum calcium levels are measured, the albumin concentration
must be taken into consideration:
Adjust total serum calcium by 0.8mg/dl for every 1g/dl decrease in serum albumin

[email protected] Page 53
Unlike changes in albumin, changes in pH will affect the ionized calcium concentration. Acidosis
decreases protein binding, thereby increasing the ionized fraction of calcium.
Daily calcium intake is 1 to 3 g/d. Most of this is excreted via the bowel, with urinary excretion relatively
low. Total body calcium balance is under complex hormonal control, but disturbances in metabolism are
relatively long term and less important in the acute surgical setting. However, attention to the critical role
of ionized calcium in neuromuscular function often is required
HYPERCALCEMIA
Hypercalcemia is defined as a serum calcium level above the normal range of 8.5 to 10.5 mEq/L (2.2-
2.6mmol/L)or an increase in the ionized calcium level above 4.2 to 4.8 mg/dL. Primary
hyperparathyroidism in the outpatient setting and malignancy in hospitalized patients, from either bony
metastasis or secretion of parathyroid hormone–related protein, account for most cases of symptomatic
hypercalcemia.
Anorexia, nausea/vomiting, abdominal pain, Weakness, confusion, coma, bone pain, Hypertension,
arrhythmia, polyuria, Polydipsia
ECG changes in hypercalcemia include shortened QT interval, prolonged PR and QRS intervals,
increased QRS voltage, T-wave flattening and widening, and atrioventricular block (which can progress
to complete heart block and cardiac arrest).
Treatment ; initial therapy – fluid and diuretics, bisphosphonate and calcitonin.
Treatment of the underlying cause.
HYPOCALCEMIA
Hypocalcemia is defined as a serum calcium level below 8.5 mEq/L or a decrease in the ionized calcium
level below 4.2 mg/dL. The causes of hypocalcemia include;
o pancreatitis,
o massive soft tissue infections such as necrotizing fasciitis,
o renal failure,
o pancreatic and small bowel fistulas,
o hypoparathyroidism,
o toxic shock syndrome,
o abnormalities in magnesium levels,
o tumor lysis syndrome
o malignancies associated with increased osteoclastic activity eg breast and prostate ca.
o massive blood transfusion with citrate toxicity.
Asymptomatic hypocalcemia may occur when hypoproteinemia results in a normal ionized calcium level.
Conversely, symptoms can develop with a normal serum calcium level during alkalosis, which decreases
ionized calcium. neuromuscular and cardiac symptoms do not occur until the ionized fraction falls below
2.5 mg/d.

[email protected] Page 54
paresthesias of the face and extremities, muscle cramps, carpopedal spasm, stridor, tetany, and seizures.
Patients will demonstrate hyperreflexia and may exhibit positive Chvostek's sign (spasm resulting from
tapping over the facial nerve) and Trousseau's sign (spasm resulting from pressure applied to the nerves
and vessels of the upper extremity with a blood pressure cuff).Hypocalcemia may lead to decreased
cardiac contractility and heart failure. ECG changes of hypocalcemia include prolonged QT interval, T-
wave inversion, heart block, and ventricular fibrillation.
FLUID AND ELECTROLYTE IN;
BURNS
TYPHOID PERFORATION
GASTRIC OUTLET OBSTRUCTION
PANCREATITIS
BURNS
Hyponatremia : Hyponatremia is a result of decreased sodium in the blood from the destroyed tissue
caused by burns on the body.
Hyperkalemia; Hyperkalemia happens to burn victims as a result of the destruction of cells and tissues.
TYPHOID PERFORATION
Perforation is usually preceded by diarrhoea with considerable loss of potassium (20-40mmol/L) and
limited intake of food. With perforation, paralytic ileus occurs with loss of more potassium in the
accumulating intestinal secretions. The peritoneal exudate. which may be 2-3litres, also has increased
Concentration of potassium- 10mmol/L Vomiting also causes loss of more potassium (9 mmol/L).
The potassium deficit is therefore considerable although it may be masked by dehydration. This deficit
should be corrected pre-operatively as soon as urine output has improved with vigorous fluid therapy.
Otherwise, cardiac arrhythmias and even death on the table may result.
GASTRIC OUTLET OBSTRUCTION
Both E.C F. and I.C. F. are lost. Hydrogen and chloride ions are also lost. Potassium is lost not only in the
vomitus but also in large amounts from the kidney as a result of increased aldosterone secretion to
conserve sodium. The patient therefore has hyponatraemia, severe hypokalaemia, hypochloraemia and
metabolic alkalosis in addition to water depletion. He needs dextrose saline or saline and potassium
chloride later.

[email protected] Page 55
PREOPERATIVE FLUID THERAPY
A surgical patient without deficit, preoperatively are on NPO and hence placed on daily maintenance
fluid; 3L in adult surgical patient as seen above. This is form of 2L of 5%D/W and 1L of N/S and 3g of
KCl if making adequate urine. Fluid and electrolyte deficit if present is corrected before placing on
maintenance.
Alternatively fluid maintenance is given as;
For the first 0 to 10 kg Give 100 mL/kg per day
For the next 10 to 20 kg Give an additional 50 mL/kg per day
For weight >20 kg Give an additional 20 mL/kg per day
INTRAOPERATIVE FLUID THERAPY
With the induction of anesthesia, compensatory mechanisms are lost, and hypotension will develop if
volume deficits are not appropriately corrected before the time of surgery. Hemodynamic instability
during anesthesia is best avoided by correcting known fluid losses, replacing ongoing losses, and
providing adequate maintenance fluid therapy preoperatively. Blood loss is measured , the is third space
loss. Although no accurate formula can predict intraoperative fluid needs, replacement of ECF during
surgery often requires 500 to 1000 mL/hr of a balanced salt solution to support homeostasis.
Maintaining acceptable vital signs and urine output.
Redistributive and Evaporative Surgical Fluid Losses
Degree of tissue trauma Additional fluid requirement
Minimal (herniorapphy) 2 ml/kg/hr
Moderate (cholecystectomy) 4 ml/kg/hr
Severe (bowel resection) 6 ml/kg/hr
POST OPERATIVE FLUID THERAPY
Postoperative fluid therapy should be based on the patient's current estimated volume status and projected
ongoing fluid losses. Any deficits from either preoperative or intraoperative losses should be corrected
and ongoing requirements should be included along with maintenance fluids. In the initial postoperative
period, an isotonic solution should be administered.
COMPLICATIONS OF FLUID THERAPY
Thrombophlebitis
High osmolality

[email protected] Page 56
Prolong use of same needle or cannula and vein
Infection
Leakage of fluid around the vein
Endothelial injury
Local sepsis
Septicemia
Overloading
Air embolism
Pyrogenic reaction

[email protected] Page 57
SHOCK
DEFINITION
Shock is the clinical manifestation of failure of cellular function due to inadequate tissue
perfusion and consequent cellular hypoxia resulting from a reduction in the effective circulating
blood volume.
It the most common cause of death amongst surgical patient. Hence every surgeon must
understand the pathophysiology, diagnosis as well as priority in the management.
CLASSIFICATION
• Hypovolemic
• Cardiogenic
• Septic
• Neurogenic
• Anaphylactic
Hypovolemic shock; There is reduction in the actual blood volume. It may result from
Hemorrhagic (commonest)- could be internal or external bleeding
Loss of plasma as occurs in extensive bums or peritonitis.
Loss of Extracellular Fluid as occurs in intestinal obstruction, diarrhoea, peritonitis and
vomiting
Cardiogenic shock;
Impaired function of the heart causes reduced cardiac output and so to reduced effective
circulating blood volume. It is commonly due to myocardial infarction or contusion, cardiac
tamponade, sepsis and obstruction to blood flow from the heart by massive pulmonary embolism
or tension pneumothorax
The other forms (septic, neurogenic and anaphylactic) of shock results from peripheral
vasodilatation and pooling of blood resulting in reduction in effective circulating blood volume.
Total spinal anaesthesia, spinal injury-vasovagal syndrome, are causes of neurogenic shock.
PATHOPHYSIOLOGY
The cellular changes; in shock, there is cellular hypoxia, leading to decrease ATP production
(3ATP rather than 38) resulting in decrease efficacy of Na-K pump, with subsequent leakage of K
out cells and movement of Na into the cells along with water and the cells swell. The
concentration of cyclic AMP falls and the affect the actions of hormones on cell. With further
reduced energy production, there is release of lysosomal enzymes and proteases with causes lysis
of the cell with inflammatory responses.

[email protected] Page 58
The stages of shock; the stages are illustrated using haemorrhagic shock
Early stage; The average adult person has 4-5L of blood (75-80ml/kg) and 25 per cent (1000ml)
must normally be lost before shock appears. With blood loss, there is stimulation of the
baroreceptors which in turns sends inhibitory stimulus to the cardio-inhibitory (a center that
reduces the activity of the heart, via reduced vagal activity) center and the vasomotor center
(increases sympathic out flow via adrenaline release). There is subsequent vasoconstriction,
increase venous return, increase heart rate and contraction, and bronchiolar relaxation.
Middle stage; with continued bleeding or inadequate resuscitation, there is diversion of blood
from peripheral and splanchnic to vital organs (heart and brain). Reduction of renal perfusion
leads to release of renin from the juxaglomerular cells which causes conversion of
angiotensinogen to angiotensin I, this is further converted in the epithelium of the lungs to
angiotensin II. Angiotensin II – causes vasoconstriction, release aldosterone which causes
reabsorption of sodium and water, release of ADH, stimulates thirst center, stimulates sympathetic
out flow.
Splanchnic vasoconstriction causes mucosal ischemia, with depression of the barrier and bacterial
transmigration into the systemic circulation. (link between hemorrhagic and septic shock)
Late stage; the stage of decompensation. Compensatory mechanisms break down and the
circulation fails. Further blood loss reduce coronary and cerebral perfusion. There is cardiac
failure, venous pooling of blood, capillary damage from back pressure and impaired cerebral
function resulting in confusion, restlessness, coma and death.
CLINICAL FEATURES
1. Rapid, weak and thready pulse
2. Low or unrecordable blood pressure
3. Skin and mucous membrane is cold and clammy (except in distributive shock
where skin is warm). Mucous membrane is pale, cyanotic and collapse
4. Rapid and deep respiration (air hunger)
5. Confused, restless, apathetic or comatose, blurred vision
6. Decrease Urine output or anuria
7. Severe thirst
8. Subnormal temperature
9. MODS
MANAGEMENT OF A PATIENT IN SHOCK;
Categories;
a) Those who respond to treatment
b) Those who respond and relapse
c) Those who donot respond; a and b may require surgery to control bleeding

[email protected] Page 59
Resuscitation;
1. Control bleeding
2. Elevate the foot of the bed
3. Fluid replacement; secure iv access with widebore cannula. Take samples for hemogram,
GXM, U/ECr.
Crystalloid (readily available); 1L of N/S or R/L is started over 30-45min, the re-
assess the PR, BP, urine output, CVP, if still deranged, repeat fluid up to 4L. (blood
must have been ready- in hemorrhagic shock. Otherwise septic shock in non-
hemorrhagic)
Blood; in severe blood loss, crystalloid shows only transient improvement. Blood
is cross matched and transfused. Occasionally uncrossed matched blood is given to
save life.
Blood substitute; in absent of blood, colloids; human albumin(most
physiologic), fresh frozen plasma, dextran 110 or 70, haemacel, gelofusine,
and hetastarch
4. Oxygen; oxygen supplements is given. Blood gases are monitored regularly and PO2
maintained between 80-100mmHg. If PO2 falls below 60mmHg and the PCO2 rises above
45mmHg, then ventilatory support is necessary.
5. Drugs
Morphine; if patient is in pains, may be given 10mg 1v
Vasodilators; after adequate fluid therapy, and normal CVP, but perfusion remains
inadequate;
i. Dobutamine; b-vasodilator, decreases pulmonary and systemic resistance
thereby better blood flow and O2 delivery.
ii. Isoproterenol; b-adrenergic; peripheral vasodilatation, increase force of
contraction of the heart.
iii. Dopamine; a precursor of nor-adrenaline, it acts on b1 and a-adrenergic
receptors.
Hydrocortisone
Naloxone
Mannitol
Sodium bicarbonate
MONITORING
1. CLINICAL
a. Sensorium
b. Skin; warm and vein refill
c. Pink conjunctiva
d. Capillary re-fill
2. Urine output > 30ml/h
3. PR and BP every 15min
[email protected] Page 60
4. CVP normal 10-15 cmH2O
5. Lungs and jugular vein
6. Blood gases
NON-HAEMORRHAGIC HYPOVOLEMIC SHOCK
Extracellular (extravascular) fluid loss must be at least 6% of body weight to result into shock.
That is 3600ml of ECF
IRREVERSIBLE SHOCK
Shock that does not respond to treatment.
Causes; inadequate fluid replacement, continued blood loss, undetected organ injury, metabolic
acidosis, myocardial failure, septic shock, MODS.

[email protected] Page 61
SEPTIC SHOCK
Results from moderate to severe sepsis or tissue damage. It is considered as part of a spectrum
and a progression of SIRS (systemic inflammatory response syndrome).
DEFINATION OF TERMS;
Bacteremia : transient invasion of circulation by bacteria
Septicemia: prolonged presence of bacteria in the blood accompanied by systemic reaction
SIRS (systemic inflammatory response syndrome ): it is a syndrome characterized by the presence
of two or more of the following clinical criteria:
Temperature(core) >38°C or<36°C
Heart rate >90beats/min
Respiratory rate >20b/min or PaC02 <32mmHg
WBC >12000cells/ml or <4000cells/ml or >10%immature band forms.
Sepsis: SIRS with a clearly established focus of infection
Severe sepsis: sepsis associated with organ dysfunction and hypoperfusion.
Septic shock: Refers to severe sepsis which is not responsive to intravenous fluid
infusion for resuscitation and requires inotropic or vasopressor agent to maintain
systolic blood pressure.
EPIDEMIOLOGY
4.6 cases/1000 persons in a study in US. 200,000 cases annually with 50% mortality. M>F(most
studies M=52-66%). Extreme of ages are more affected. 13th leading cause of death in US. Leading
cause of death in ICU.
AETIOLOGY
BACTERIA: gram –ve nearly 2/3, gram+ve 1/3. of the gram –ve, E.coli is the commonest.
GRAM -VE
Klebsiella,
Entrobacter,
Serratia,
Proteus,
Mirabillis/Vulgari,
Pseudomonas and
Bacteroides
GRAM +VE
Streptococci

[email protected] Page 62
Staph
Clostridia and Pneumococci
Viruses, Fungi and Parasites in a few especially the immuno-compromised.
SOURCE
Endogenous –
Skin- SSI
urinary tract- UTI
respiratory tract- LRTI
GIT- bowel surgery, perforations
Exogenous.
surgical instruments
drapes
imaging machines
staff
RISK FACTORS
Age (<10 >70years)
malnutrition,
anemia,
Primary disease: Malignancies, DM, CLD, CRF,
Immunosuppression, Immunosupresssive agents,
necrotic tissue
hematoma
poor surgical technique
Catheriration
Prolong hospitalisation
Major surgeries, trauma, extensive burns
PATHOGENESIS
Micro-organisms or products of tissue damage stimulates production of pro-inflammatory
cytokines (TNF-α, IL-1β, IL-6, IL-8) which in turn stimulate production of secondary mediators
(PGI2, PGE2, TXA2, LT, PAF,NO, KININS, IL-1,IL-6, OXYGEN FREE RADICAL, PROTEASES.) of
inflammation in order to localize infection and limit proliferation.
The production of the pro-inflammatory cytokines is regulated to limit damage.
However in poorly controlled sepsis or extensive tissue damage, there is excessive inflammatory
response which is poorly regulated.

[email protected] Page 63
Anti-inflammatory and immunosuppressive cytokines IL-10 which aided by IL-4 inhibits the
activity of the pro-inflammatory cytokines to limit damage.
In severe sepsis they become immunosuppressive to patient.

[email protected] Page 64
Effects of secondary mediators
Damage of vascular endothelium
Vasodilation of microvasculature
Activation of neutrophils(aggravates endothelial damage)
Diminished force of cardiac contraction
These ultimately lead to peripheral pooling of blood, extravasation of fluid,
hypotension, hypoxia
EFFECT OF COPLIMENT COMPONENT
vasodilatation and increase permeability
Endothelial damage
C5a causes aggregation of platelet and leucocytes thereby acting as procoagulant leading
to DICnd shock
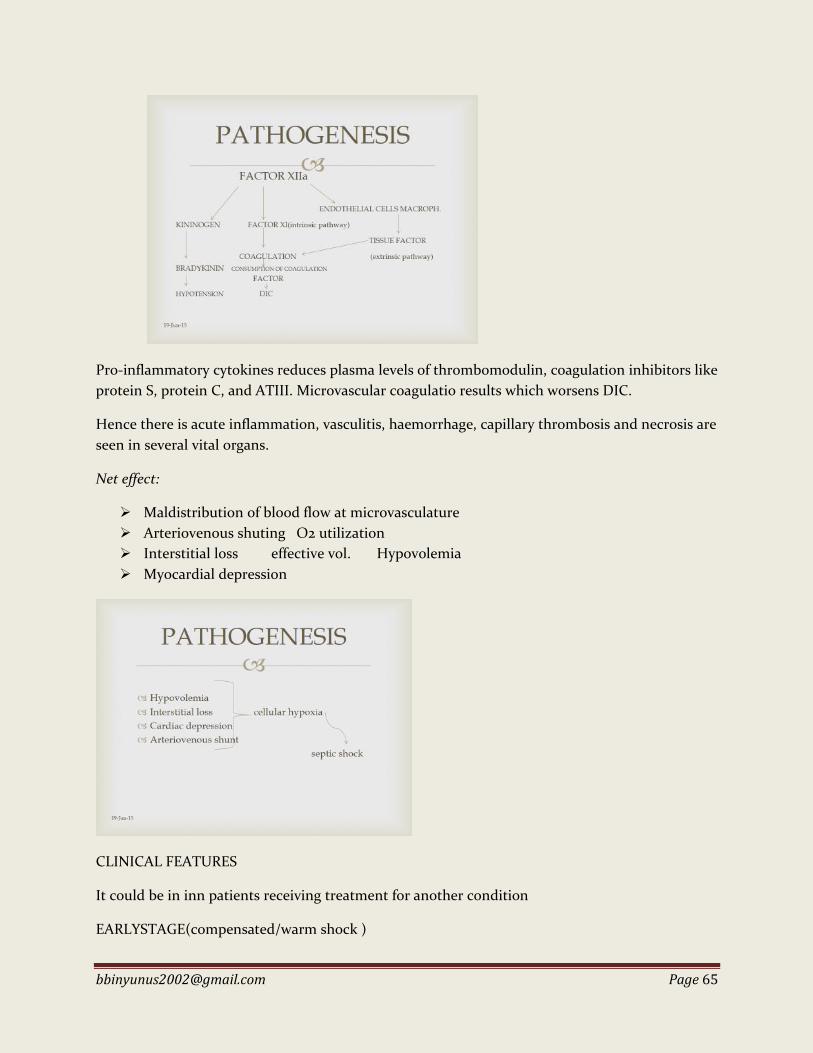
[email protected] Page 65
Pro-inflammatory cytokines reduces plasma levels of thrombomodulin, coagulation inhibitors like
protein S, protein C, and ATIII. Microvascular coagulatio results which worsens DIC.
Hence there is acute inflammation, vasculitis, haemorrhage, capillary thrombosis and necrosis are
seen in several vital organs.
Net effect:
Maldistribution of blood flow at microvasculature
Arteriovenous shuting O2 utilization
Interstitial loss effective vol. Hypovolemia
Myocardial depression
CLINICAL FEATURES
It could be in inn patients receiving treatment for another condition
EARLYSTAGE(compensated/warm shock )

[email protected] Page 66
Not associated with hypovvolemia
febrile (38.2-41°C )
Shivering and malaise
warm dry and flushed skin.
hyperventilation
rapid bounding pulse
wide pulse pressure
LATE STAGE (decompensated/ cold shock)
Hypovolemia with superimposed sepsis
altered sensorium
cold clammy skin
Feeble pulse
hypothermia, hypotension
Oliguria
Jaundice
upper GI bleeding
DIC
LOCALISING INFECTION
A good complete systemic examination is done to detect any focus of sepsis.
NOTE THAT RESUSCITATION TAKES PRECEDENCE OVER INVESTIGATIONS, WHICH
SHOULD NOT DELAY INTERVENTION
INVESTIGATION GOES HAND-IN-HAND WITH RESUSITATION
FBC: there is leucocytosis after initial leucopenia. Throbocytopenia
Septic work up; Blood culture, Sputum m/c/s, Urine m/c/s, Wound swab m/c/s,
Endocervical swab m/c/s or any exudate
Based on suspected source; CXR, Abd-X RAY, Abd-pelvic uss, CT Scan of various sites
TREATMENT
Septic shock is a medical emergency that requires prompt and efficient resuscitation
If possible patient should be admitted to ICU
AIMS:
Improve haemodynamic state
Restore tissue perfusion thereby increase O2 delivery to tissue.
Administer O2
Combat the bacteria and cytokines
[email protected] Page 67
Eliminate septic focus
RESUSCITATION
FLUID (see above)
Vasopressor ; After adequate fluid resuscitation or about 4L, with signs of fluid
overload(basal crepitation, high CVP) and persistent hypotension.
a. Norepinephrine – α & β ; 1st line for septic shock refractory to volume
replacement .Vasoconstriction & reflex bradycardia 5-20mcg/min
Dopamine – systemic vasoconstriction, inotropic, renal vasodilatation 2-20mcg/m
OXYGEN ADMISTRATION
In a cleared and patent airway, O2 is delivered via a face mask to increase O2
saturation. Increasing uptake and delivery to tissue.
ANTIBIOTIC
Give in large doses IV to combat infection. Empirical
IV Broad spectrum bactericidal & anerobe coverage (3rd generation cephalosporin)
Ceftriaxone 50-100mg/kg up to 2gm daily + Metronidazole 500mg 8hrly
Steroids
NSAID
FREE REDICALS SCAVENGERS; superoxide dismutase, allopurinol, vitamin C, a-
tocopherol
Glycemic control- soluble insulin (GKI) to maintain blood sugar – 80- 120mg/dl
has been found to ↓morbidity/mortality.
PREVENTION OF FURTHER COAGULATION
• Atiii and C₁-estrase inhibitor
• Recombinant human activated protein C
• inhibits thrombosis and inflammation, promotes fibrinolysis, and
modulates coagulation and inflammation.
SURGERY
• resuscitative & therapeutic
• If septic focus is responsible for the shock it should be dealt with as soon as
possible especially if respose to therapy is poor. E.g debridement, drainage
of abscess

[email protected] Page 68
NUTRITION IN SURGERY
Introduction
Nutritional requirements
Cause of under nutrition
Effect of malnutrition
Nutritional assessment
Nutritional support
Future trends
INTRODUCTION
The process of utilizing exogenous substances for the production of energy and synthesis of new
tissues. It entails provision of water, electrolyte, vitamins and other nutrients. Nutritional status
determines the outcome of a surgical patient. Provision of adequate nutrition requires
appreciation that injured or septic patient requires higher nutrient than healthy one. Nutrition
support is aimed in timely manner. It is given via the safest route to minimize complication.
Terms;
Resting energy expenditure (REE); the energy expended by a person at rest in a thermoneutral
environment. Basal metabolic rate (BMR); the expenditure for an individual under standard
condition of 12-18hours fasting, recumbent at mental rest in thermoneutral environment. REE and
BMR usually differs by lessthan 10% but REE is higher because it include energy expenditure at
mental activity and other expenditure. REE in newborn 55Kcal/kg/day, in adult 20-30Kcal/kg/day.
NUTRITIONAL REQUIREMENT;
Adult Neonate/infant
Energy (kcal/kg/day) 20-25 90-120
Protein (g/kg) 0.7-1.5 2.5
Fat (g/kg) 1.5-2.0 4.0
Water(/kg) 45-50ml 125-150ml
Caloric contribution; CHO 55-60%, Fat 30-35%, proteins 5-10% and 1g of CHO delivers
4kcal(17j), 1g of protein 4kcal and 1g of fat 9kcal(38j)
Vitamins; vitamin A 5000iu weekly, K 5-10mg weekly, C 60-80mg daily, B12 500mcg weekly, folic
acid 3-6mg daily. Fat soluble vitamins ADEC, water soluble B, C and folic acid. B is produced by
gut bacteria, B12(cyanocobalamin) absorbed in the terminal ileum, folic is absorbed in the
duodenum
Minerals; zinc 5mg, cu 0.5-2.0mg, Mn 70-150mcg, Cr 40mcg, Se 70-150mcg

[email protected] Page 69
The energy requirement is increased in catabolic states;
Major elective abdominal surgeries or trauma by 10-30%, generalized peritonitis 15-50%, sepsis 50-
80% and burns 80-200%. If these requirements are not met by exogenous supplement, they will
be provided from endogenous alternative ways to the deterrent of the body.
Starvation; 1st 12hrs previous meal utilized and within 24 hrs body glucose store is depleted.
After 24hrs fatty acids and amino acids are being broken down (gluconeogenesis).Obligate use of
glucose (the CNS others; rbc, wbc, fibroblast, proximal convulated tubules) is gradually being
adapted to ketones. Increased secretion of counter regulatory hormones. Exaggerated hepatic
glucose production. Pro inflammatory cytokines are produced TNF, IL6. Plasma albumin
concentration falls rapidly. There is increased catabolic state depending on the severity of
injury/infection. 12% increase in BMR/degree rise in temperature.
Trauma and sepsis; there is increased counter-regulatory hormones- adrenaline, noradrenaline
and cortisone. Energy requirement increase (upto 40kcal/kg/day). N2 requirement increase.
There is insulin resistance and glucose intolerance. There preferential oxidation of lipids. There is
increase gluconeogenesis, loss of adaptive ketogenesis, fluid retention with hypoalbuminemia.
CAUSES OF UNDERNUTRITION
DECREASE
INTAKE
INADEQUATE
ABSORBTION EXCESSIVE LOSSES EXCESSIVE
DEMAND
starvation
poverty
anorexia
nervosa
hyperemesis
cancer
sepsis
liver disease
dysphagia
alcoholism
git
obstruction
short bowel syndrome
major gastric resection
motility disorders (
irritable bowel
syndrome)
pseudo obstruction
(ogilvie syndrome)
GIT fistula
malabsorbtion states
inflammatory bowel
disease
protein loosing
enteropathy
Hypercatabolicstates
burns
sepsis
trauma
surgical stress

[email protected] Page 70
EFFECTS OF MALNUTRITION
Impaired mental function: Apathy, fatigue, poor cognition
Impaired muscle function: Respiratory failure
Impaired immune function: Increased incidence of infection
Miscellaneous: Impaired thermogenic response, Impaired wound healing
NUTRITIONAL ASSESSMENT
Aim; identify patient who are at increased risk of post-operative complication due to malnutrition
and where possible, to improve nutritional status through intervention.
Methods;
Clinical
Anthropometry
Laboratory evaluation
Clinical
detailed history and examination
HISTORY
Vomiting, difficulty in swallowing, diarrhea.
Medical history of DM, AIDS, chronic liver dx, chronic kidney dx
Surgical history of abdominal operation
Drug history; chemotherapy.
Dietery hx; 24hr dietery recall.
CLINICAL EXAMINATION
Acutely or chronically ill looking.
Wasted, sunken eyes, palor, silky hair,chelosis, pedal aodema
Cvs; displaced apex beat , haemic murmurs
Abdomen; stomas, fistula, abdominal masses, hepatomegaly.
Rectal examination; perineal fistula, pale stools
Nervous system; neuropathies

[email protected] Page 71
SUBJECTIVE GLOBAL ASSESSMENT
5 features in the history
Weight loss in the past 6months
Dietary intake
GI symptoms
Functional status or energy level
Metabolic demands
4 features in physical examination
Loss of subcutaneous fat
Oedema
Ascites
Muscle wasting
ANTHROPOMETRIC
Body mass index (BMI); 18.5-24.9kg/m2
Interpretation
Severely underweight-<16.5
Underweight-16.5-18.4
Normal weight-18.5-24.9
Overweight-25-29.9
Obesity grade 1; 30-34.9
Obesity grade 2; 35-39.9
Obesity grade 3; >40
Superobesity >50
Ideal body weight; using Devine formula
Men:50kg+ 2.3kg for every inch over 5ft
Women:45.5kg +2.3kg for every inch over 5ft.
Mid arm circumference, Triceps skin fold thickness, waist hip ratio,
LABORATORY EVALUATION
1. Serum protein concentration
a. Total protein
b. Albumin; <3.5g/dl, t ½ 21days
c. Prealbumn; for acute changes t ½ 3days

[email protected] Page 72
d. Transferrin; t ½ 10days
e. Retinol binding protein; t ½ 12-24hours
2. Total lymphocytes count < 1500/ml
3. immunological; delayed cutaneous hypersensitivity, lymphocyte blastogenesis, neutrophil
chemotaxis, compliment level
COMBINED ASSESSMENT
Nutritional risk index(NRI)
(15.19×albumin) + 41.7× (actual weight/ideal weight)
Well nourish > 100
Mild malnutrition 97.5-100
Moderate malnutrition 83.5-97.5
Severe malnutrition <83.5
INDIRECT CALORIMETRY; Using O2 consumption; respiratory quotient; 0.7-1.0 normal,
<0.7 underfeeding, >1.0 overfeeding.
NUTRITIONAL SUPPORT
GOALS
Preservation of lean body mass
Preserve or reverse nutrient deficiency
Help patient better tolerate treatment
Minimize nutrition related side-effect and complications
Maintain strength and energy
Protect immune function, decreasing risk of infection
Aid recovery and wound healing
Maximize quality of life
INDICATIONS
Recent loss of Wt. > 15%
Body Wt <80-85% of ideal B.W
Serum Album < 3g/dl
Serum Transferrin < 200mg/dl
Skin Anergy
Duration of starvation (5-7day)
Poor premorbid state
History of functional impairment.
[email protected] Page 73
Determination Of Requirement Of A Patient;
1. Harris-Bennedict equation
a. Male ; (66.47 + 13.75×weight + 5.0× height - 6.76 ×age)kcal/day
b. Female ; (66.51 + 9.56×weight + 1.85×height – 4.68×age)kcal/day
2. Total energy expenditure (TEE)= basal energy expenditure(BEE) × a stress factor
3. Resting energy expenditure (REE)= 1.44×(3.91 × vO2 + 1.10 × vCO2)–3.34×N2 excretion
4. Using stress level
a. No stress/minimal activity 20kcal/kg/day
b. Mild stress 30kcal/kg/day
c. Moderate stress 35kcal/kg/day
d. Severe stress 40kcal/kg/day
ROUTES OF ADMINISTRATION;
1. Enteral
2. Parenteral
Enteral
It entail the delivery of nutrient into gastrointestinal tract. Used in patient with
functioning GI tract.
Merit
More Physiologic
Gut barrier and immune function are better maintained
Less complications
Attenuate gut mucosal atrophy
Cheaper
The liver is not bypassed
Forms of enteral feeds;
Polymeric (blenderized diet)
Elemental diet (chemically defined)
Disease specific e.g hepatic aid.
Modular (supplemental diet).E.g Amino aid.
Techniques
Sip feeding/oral
Naso-enteral; Nasogastric tube, Nasoduodenal, Nasojejunal
[email protected] Page 74
Gastrotomy; Percutaneous endoscopic gastrostomy (PEG), Surgical
gastrostomy, Fluoroscopic gastrostomy
Jejunostomy; PEG-jejunal tube, Direct percutaneous endoscopic jejunostomy
(DPEJ), Surgical jejunostomy
Contra-indications
Intestinal obstruction
Gi bleeding
Severe diarrhea/vomitting
Enterocolitis
High output fistula
Severe pancreatitis
Complications
Tube related; Relates to feeding regimen
• Malposition
• Dislogdement/migration
• Aspiration
• Peritonitis
• Fistula formation
• Intestinal obstruction
• Tube fracture/blockage.
• Intolerance
• Hyperglycemia
• Enteric infection
• Severe diarrhea- hyperosmolar feeds
leading to dehydration and electrolyte
imbalance
PARENTERAL NUTRITION; It involves the delivery of nutrients via intravenous access.Non
physiological, has substantial complications and occasional mortality. Benefit must overweigh the
risk. Total Parenteral Nutrition(TPN): Is defined as provision of all nutritional requirements by
means of intravenous routes and without the use of GI tracts.
Hyperalimentation: Is the intravenous delivery of nutrients to a malnourished patient or patient
in hyper catabolic state in amount as high as 2.5 times his basal requirements in healthy state.
Indications;
GIT fistula ( high output)
Short bowel syndrome
Burns, severe trauma.
Renal failure
[email protected] Page 75
Hepatic failure
Mal-absorption synd
GIT anomalies in infants
Acute radiation enteritis
Prolonged ileus after major surgery
Contraindications
CVS instability
Feasibility of enteral feeding
Severe blood dyscrasia
Shock
Uncontrolled DM
Severe metabolic derangement
Techniques
Peripheral;
• Isotonic solution(around 300mosmol/L) fats
• Short period less than 2 wks
• Change site every 48hrs
Central
• Via Internal Jugular Vein or subclavian vein
• Hyperosmolar
• Prolonged nutrition
• Absence of adequate peripheral vein
Monitoring of TPN;
Daily; weighing, U/E, RBS and urinalysis
Twice weekly; Serum calcium, Phosphate , albumin and FBC
Weekly; LFT, lipid profile and serum Mg
Monthly; Serum vitB12, folate, iron, zinc and clotting profile
Complications;
1. Acute reaction to fat/A.A seen in 1-2% of pt xterised back pain shevering, fever vomiting
and headache.
2. Hyperosmolar solution causing:
- Thrombophlebitis
- Decreased myocardial contractility
- Osmotic diuresis
[email protected] Page 76
3. Sepsis – from contaminated solution or central venous catheter
4. Metabolic complications; Electrolyte imbalance e.g.Na, Hypocal>, mg,phos> refeeding
syndrome, Metabolic acidosis, Hypoglycemia – xss insulin/ ↓ glucose infusion,
Hyperglycemia – Rapid initiation of infusion/sepsis, Essential FA deficiency
5. Congestive cardiac failure
6. Technical complications
Early -
• Pneumothorax/haemothorax
• Arterial laceration
• Brachial plexus injury
• Hydrothorax
• Sympathetic effusion
• Thoracic duct injury
• Air embolism
• Catheter embolism
Late –
• Erosion of bronchus/Rt. Atrium
• Subclavian thrombosis (5 – 10%)- Remove catheter, antithrombotic
Rx.
• Septic thrombosis.
Advantages of parenteral nutrition
1. Survival rate is improved and morbidity reduced
2. Weight loss and tissue breakdown is minimized
3. Wound healing is enhanced
4. Resistance to infection and general immunity improved
5. Formation of blood element such as plasma proteins, red cells are maintained
Some clinical application of nutritional support
1. Gastrointestinal fistula
2. Bowel failure
3. Burns
4. Pancreatitis
NEW TREND
Immunomodulation; Addition of glutamine, omega 3 fatty acids, arginine and nucleosides, has
been shown to enhance immunity, wound healing, reduce infections and hospital stay.
Fistuloclysis; Reinfusion of effluents from an intestinal fistula into the distal segment.

[email protected] Page 77
FUTURE DIRECTION
Administration Of Anabolic Factors
Gut derived hormones
growth hormone
insulin like growth factor
anabolic steroids
cathecholamines
Inhibition Of Proteolysis
Pharmacolical agents
lessons from nature

[email protected] Page 78
BLOOD TRANSFUSION
Introduction
Indications for transfusion of blood and component
Types of blood transfusion
Collection and administration
Complications of blood transfusion
Massive blood transfusion
Alternative to blood transfusion
INTRODUCTION; Blood transfusion is the infusion of blood and/ or its product into the venous
system for therapeutic purposes. It should not be given without adequate reason because of its
potential hazards. Specific component deficiency should be infused to minimize hazards.
INDICATIONS FOR BLOOD TRANSFUSION
1. Whole blood;
a. Sudden blood loss of >25% blood volume
b. Exchange blood transfusion
c. Patient continue to bleed after receiving 4 units of packed cells
2. Packed cells
a. Patients with chronic anaemia
b. Elderly
c. Small children
d. Patients prone to fluid overload & cardiac failure, renal and liver failure.
e. Major operation in association with clear fluids
NB; 1unit raise Hb by 1g/dl in a 70kg adult
3. Platelet concentrate
a. Thrombocytopaenic patients undergoing operations
b. Patients undergoing chemotherapy for leukemia
c. Abnormal platelet function
d. Aplastic anemia.
e. Accelerated platelet consumption or destruction (eg, acquired immunodeficiency
syndrome, sepsis, disseminated intravascular coagulation).
f. Surgical indications (eg, cardiopulmonary bypass surgery or surgery in patients
recently treated with drugs which impair platelet function).
NB; 1unit of concentrate raise platelet count by 5-10×10⁹/L
4. Granulocytes concentrates;
a. Used in selected patients with sepsis and severe neutropaenia
5. Fresh frozen plasma
a. Deficiencies of coagulation factors or inhibitors of coagulation for which specific
concentrates are not available

[email protected] Page 79
b. Emergency treatment of warfarin overdose and vit. K deficiency when factor IX
complex concentrates is not available.
c. Treatment of TTP
d. Treatment of DIC
6. Cryoprecipitate;
a. Use in hemophilia
b. Hypofibrinoginemia
c. Von Willebrand’s disease.
NB; rich in factor VIII and XIII, fibrinogen and von Willibrand’s factor
7. Protein solutions and factor concentrates
a. Use in correcting the respective deficiency states
TYPES OF BLOOD TRANSFUSION
• Homologous (Allogenic ) Transfusion; infusion of blood collected from a donor
• Autologous Blood Transfusion; collection and subsequent re-infusion of patients own
blood. it prevents the transmition of infections and immunological complications
associated with homologous blood transfusion.
– Pre-operative autologous Blood donation (PABD)
– Acute isovolaemic Haemodilution (AIVH)
– Intra-operative Blood Salvage (IBS)
– Post-Operative Blood Salvage (PBS)
Pre-operative autologous Blood donation (PABD); Donates 1-5 units of his blood preop, to
replace blood loss intraop or postop. Donation should be 3-7 days apart, last one should not be
within 72 hours of the surgery. Initial HB > 10g/dl and PCV of >30%. Patients with bacteremia,
serious cardiac disease and sickle cell should be excluded. Elective surgeries. Ferrous sulphate,
recombinant erythropoietin are given to prevent anaemia.
Acute isovolaemic Haemodilution (AIVH); 1- 4 units of patient’s blood are removed just b4 the
operation. Replaced simultaneously with a crystalloid or colloid. 3ml of crystalloid for every 1ml of
blood. 1ml of colloid for every 1ml of blood. The blood is then re-infused during or after the
operation. Initial Hb > 12g/dl and should not fall beyond 9g/dl. PR, BP and urine output should be
monitored during the procedure. Blood collection is simultaneously replace by crystalloid or
colloid in a separate venous access.
Intra-operative Blood Salvage (IBS); Shed blood from a wound or body cavity is collected and
subsequently re-infused into the same patient. Used in ruptured ectopic pregnancy, ruptured
spleen, penetrating injuries, the shed blood is collected with a galipot into a kidney dish

[email protected] Page 80
containing anticoagulant. The blood is filtered into a bottle thru 4-6 layers of sterile gauze in a
funnel. The bottle is then sealed and the blood is re-infused.Hemolysed or infected blood should
not be used. Contra-indicated in tumour resection. Special machines are available. Blood
collected have a shelf-life of 6hours at room temp., and 24 hour at 4°C.
Post-Operative Blood Salvage (PBS); If postoperative blood loss is likely to cause
homodynamic instability and require blood transfusion. Useful in cardiac surgery, penetrating
chest injuries, some orthopedic procedures. Blood salvaged from cavities and joint spaces are re-
infused.
BLOOD DONATION & COLLECTION
Donors must be fit:
• Hb>12g/dl
• 18-65yrs & > 51kg
• No major surgery or blood donation in last 6/12
• No pregnancy or blood transfusion in last 12/12
• No clinical malaria in last 1/12
• No hypertention, splenomegaly, hepatomegaly, bleeding disorder or allergic conditions e.g
asthma
• Free of viral hepatiis, HIV, syphilis, trypanosomiasis, brucellosis
• No vaccination in last 3/12
• not in high risk group for HIV
COLLECTION; of blood should be into collapsible plastic bags containing 60ml citrate,
phosphate, dextrose, adenine. (CPDA) or CPD or saline,adenin, glucose mannitol (SAGM)
STORAGE;
• Whole blood: 2-6 ˚C
• Cryoprecipitate: -40 ˚C
• Platelet concentrate: 20-24 ˚C for maximum of 5 days.
EFFECTS OF STORAGE; WHOLE BLOOD AT 2-6 ˚C
=RBC:
• swells by 20%
• loses k+ into plasma
• ↓ATP & 2,3 DPG →↓viability.
• 1% of RBC is lost per day of storage
=WBC:
• not viable after 24 hours of storage.

[email protected] Page 81
=PLATELETS:
• no viable platelets after 24 hours.
=ELECTROLYTES:
• plasma K+ ↑ by 1 mmol/day
• plasma Na+ ↑
• No ionized ca2+
=CLOTTING FACTORS
• factos VIII & V ↓ rapidly after 24hours. No activity after 7/7
• factor X: no activity after 7/7
• factor IX: no activity after 14 days.
• factor VII: ↓ only after 14/7
• fibrinogen & factor ii: stable for 21 days
=PH: ↓from 7.2 at collection to 6.8 at 20 days
=PLASMA Hb: ↑during storage b/c of leakage from rbc
NH3:↑
ADMINISTRATION; should be based on accurate diagnosis & informed indication benefits to
outweigh risks. Informed consent is obtained from patient. ABO & Rh compatible blood should
be crossmatched with patient’s serum b/4 use. Blood to be transfused should be identified &
checked against patient’s name, group, hospital no. & ward. Secure iv access for blood transfusion
with large bore cannula under strict asepsis. Check vital signs b/4 & during the process. Exclude
air from giving set. Regulate rate according to patient & his needs observe patient regularly for
complications & treat accordingly. Untoward symptoms usually occurs during infusion of the
initial 100ml. The rate should therefore be initially 20-30drops/min i.e 2-3mls/min then increased
to 60-80drops after half an hour.
COMPLICATIONS;
Immediate complications:
• febrile non hemolytic rxn
• hemolytic rxn
• allergic or anaphylactoid rxn
• bacterial contamination
• circulation overload
• cardiac arrest
• air embolism

[email protected] Page 82
Delayed complications:
• thrombophlebitis
• delayed hemolytic rxn
• post transfusion thrombocytopenic purpura
• iron overload
• immunosuppression
• transmission of diseases:
viral hepatitis A,B,C,
malaria
syphilis
cytomegalovirus (cmv)
trypanosomiasis
brucellosis
infectious mononucleosis
HIV
parvo virus
MASSIVE BLOOD TRANSFUSION;
This is transfusion of >1/2 the patient’s blood volume in 1 hour or ≥ total blood volume (TBV) in
24hours
Most frequent indication is Hypovolaemic shock secondary to blood loss (haemorrhagic shock)
which can arise from;
trauma,
ruptured aortic aneurysm
massive GI haemorrhage,
liver transplant
exchange blood transfusion
PROBLEMS
technical & clerical errors → hemolytic rxns
circulation overload
cardiac arrhythmias & arrest due to:
• cold blood
• hyperkalemia
• hypocalcemia
• acidosis
Respiratory complications
[email protected] Page 83
Bleeding diathesis due to:
• thrombocytopenia
• deficiency of clotting factors v & viii
• hypocalcemia
Reduced O2 delivery due to ↓ 2,3 DPG
ALTERNATIVE TO BLOOD TRANSFUSION
REASONS;
Adverse reactions of blood transfusion
Costs and availability of BT
Religious reasons
TECHNIQUES;
Autologous blood transfusion
Blood substitutes
Decreasing surgical blood loss
Increasing rbcs production
BLOOD SUBSTITUTE; plasma and red cell substitute
Plasma Substitutes: fluids used to replace lost circulating blood vol.: they include
Colloids
• stable plasma protein
• albumin
• dextran 70, 110, 40
• synthetic gelatin colloids (haemacel, gelofusine)
• hydroxyethyl starch preparations (hetastarch, pentastarch)
Crystalloids
Red blood cell substitutes;
• Diaspirin cross-linked Hb solution
• Perfluorocarbons
• others: stroma free hb, encapsulated hb, recombinant dna deried hb.
CRYSTALLOIDS
Normal saline, ringer’s lactate, Hartman's solution. Readily available and cheap. Osmotic pressure
is low, diffuse thru all body compartments, only 30 % remains in the intra- vascular compartment
[email protected] Page 84
Hypertonic solns; 3% NaCl, 7.5% NaCl, hypertonic ringer’s lactate. Retained in the intravascular
compartment. They cause movement of intracellular fluid into the intravascular. May cause
dehydration, cerebral edema, hypernatremia
COLLOIDS
Contain HMW proteins as well as electrolytes. The proteins cannot diffuse through the capillaries
and remain intravascular, so they are good for volume replacement. Are not as readily available
and cheap;
Human Albumin Soln
Osmotic pressure is the same as that of plasma proteins therefore suitable as replacement fluid. It
replaces only albumin. Contains no Ig and coagulation factors. T1/2 short – 24 hours. It is
expensive
Dextran 70
Polysaccharides, MW 70,000. Osmotic pressure > that of plasma, retained in the vascular
compartment. Withdraws fluid from the extravascular compartment. Excreted by the kidney in 24
– 48 hours. May cause renal damage. Reduce platelets adhesiveness. Induces roulex formation and
so may interfere with blood GXM. Not very satisfactory for replacing blood volume.
Dextran 40
MW 40,000. More rapidly excreted, within 24 hours. It lowers blood viscosity
Hemacel; Contains degraded polypeptides. MW of 35,000. T1/2 4 – 6 hours. It does not interfere
with blood GXM. It does not impair renal function.Satisfactory for volume replacement
Gelofuscine; Modified gelatin. MW 30,000. No effect on clotting or blood GXM. Promotes
osmotic diuresis
Hetastarch; MW 200,000 – 400,000. T1/2 6 – 8 hours. 1 – 1.5L is given daily. May interfere with
coagulation.Valuable volume expander.
RBC SUBSTITUTES
Also known as artificial O2 carriers. Most are currently in clinical trial. Co-administered with
colloids and crystalloids
MODIFIED HB SOLUTIONS; Are solutions that have similar O2 carrying capacity and exchange
properties as RBC Hb. Originated from outdated human blood, genetic engineering, or of bovine

[email protected] Page 85
origin. Rapidly cleared from the circulation. Can cause renal failure.Not readily available in our
environment
PERFLUOROCARBON EMULSIONS
Compounds with high gas dissolving capacity (O2, CO2). Dissolve O2 which is released to tissues
by diffusion. After I.V administration they are taken up by the RES, slowly broken down and
released into the circulation. Finally excreted in the lungs by exhalation. Cause mild flu-like
symptoms. Decrease platelets count.
INCREASING RBCs PRODUCTION
• Hematinics; iron, folic acid, vit b12
• Erythropoitin
• IMPROVED NUTRITION; Optimize RBC mass b4 an operation
Iron ; Essential component of Hb. Necessary for erythropoiesis. Orally or parenterally
(i.v or i.m). Orally at a dose of 200mg/day. S.E gastric irritation. i.m is discouraged; pain at inj site,
staining of the skin. I.V: Iron dextran, iron sucrose. Used in Severe IDA, Intolerance of oral iron,
Ongoing blood loss, CRF, together with EPO, PABD S.E; anaphylactic rxns, headache,
hypersensitivity, urticaria, myalgia
Erythropoietin; Stimulates erythrocytes production, Usually given with iron
supplements. Administered i.v or sc. 300u/kg/day for 5 days, then on alternate days for 2 weeks.
Equivalent of 1 blood unit is produced by day 7 and 4 units by day 28. Usually started 10 – 21 days
b4 the surgery. S.E, Thrombosis, hypotension. It is Expensive and Not readily available in
developing countries
Nutrition ; Early enteral feeding Parenteral nutrition for patients who cannot be
fed. Protein supplementation
DECREASING SURGICAL BLOOD LOSS
• Pharmacological
• Non pharmacological
NON PHARMACOLOGICAL
• Meticulous surgical techniques,
• Patient positioning,
• Regional anaesthesia,
• Maintenance of normothermia,
• Microsampling,
• Quick trauma response

[email protected] Page 86
Meticulous techniques; Tourniquet, Ligation of vessels, Use of diathermy, Haemostatic agents;
trasylol, topical glues, Laparoscopic surgeries
Patient Positioning; Avoid venous engorgement from obstruction of the venous return. If
possible the surgical site should be elevated above the level of the right atrium, to improves
venous return
Regional Anaesthesia; Patients operated under R.A have been found to bleed less > G.A
The sympathetic blockade lowers the arterial BP
Maintenance Of Normothermia; Hypothermia; low ambient operating room temp, evaporation
from large body cavities, etc. Hypothermia impaired platelets function and Prolonged coagulation
enzymatic rxns leading to more bleeding. Use blankets, thermal suits, machine to warm i.v fluids
Microsampling;Minimal amount of blood required Microtubes, Microchemistry analyzers
Quick Trauma Response; Act quickly, Arrest bleeding, Apply other modalities of alternatives to
blood transfusion.
PHARMACOLOGICAL
• Aprotinin
• Tranexamic acid
• Desmopressin
• Recombinant coagulation products
• Vit K
Aprotinin; Antifibrinolytic agent. Inhibits generation of plasmin. Used in cardiac, vascular and
orthopedic surgeries.
Tranexamic Acid; Antifibrinolytic. Displace plasminogen from fibrin. Prostatectomy,
menorrhagia
Desmopressin; Improves platelet adhesion to site of vascular injury. Increases plasma level of
factor VIII and VWF
Recombinant Coagulation Products;Factor IX conc, factor VIIa conc, antihemophilic factor
concentrate. Used to manage bleeding in pts with hemorrhagic dxs; hemophilia, VW dx.
Vitamin K; For mgt of bleeding due deficiency of Vit k dependent clotting factors

[email protected] Page 87
HAEMOSTASIS
Introduction
Physiology
Abnormal hemostasis
Peri-operative control of bleeding
INTRODUCTION; Haemostasis is a complex mechanism that prevent or terminate blood loss
from a disrupted intravascular space, provides a fibrin network for tissue repair, and, ultimately
remove the fibrin when it is no longer needed.
PHYSIOLOGY; It is achieve via four interdependent processes;
Contraction of the injured vessel.
Endothelial cell secretion and interaction
Plugging of the vessel by platelets.
Coagulation of blood in the vessel
Contraction of injured vessel; Aided by Sympathetic reflex and Release of vasoconstrictors
(TXA2, serotonin and catecholamines). Platelets adhere to the walls of damaged vessels.
Endothelial cell secretion and interaction; the products of endothelial cells which promotes
Haemostasis include von Willibrand’s factor (causes platelet adhesion and aggregation),
thrombospodin (causes platelet aggregation), endothelin(vasoconstrictor), and tissue factor
(initiate extrinsic pathway)
Plugging of vessels by platelet; when a blood vessel wall is injured, platelets adhere to the
exposed collagen and von Willebrand factor in the wall via platelet receptors → Platelet
activation. Activated platelets release the contents of their granules including ADP and secrete
TXA2 →activates nearby platelets to produce further accumulation of more platelets (platelet
aggregation) and forming a platelet plug.
Coagulation of blood in the vessels; the fundamental reaction is conversion of soluble
fibrinogen by thrombin to soluble fibrin monomer which is then converted by thrombin in the
presence of calcium ions and thrombin-activated factor XIII to insoluble fibrin polymer. This is
via two pathways;
Intrinsic; The initial reaction is the conversion of inactive factor XII to active factor XIIa.
Factor XII is activated in vitro by exposing blood to foreign surface (glass test tube). Activation in
vivo occurs when blood is exposed to collagen fibers underlying the endothelium in the blood
vessels.

[email protected] Page 88
Extrinsic; Requires contact with tissue factors external to blood.This occurs when there is
trauma to the vascular wall and surrounding tissues. The extrinsic system is triggered by the
release of tissue factor (thromboplastin from damaged tissue), that activates factor VII. The tissue
thromboplastin and factor VII activate factor X.

[email protected] Page 89
PREVENTION OF FURTHER CLOTTING AND BREAKDOWN OF CLOTS; once haemostasis
have been achieved, there are processes which prevent further clot and breakdown of clot;
1. Prevention of further clotting;
a. Action of thrombin is limited by ;
i. Absorption of thrombin in the fibrin clot reduces the amout available for
further action
ii. Antithrombin III combine with thrombin to form inactive complex. It is
also potent inhibitor of factor IX, X and XI
iii. Fibrin degradation product(FDP). Inhibits thrombin.
b. Tissue factor pathway inhibitor (TFPI); product of endothelial cells, inactivates
TF/factor VIIa complex.
c. Protein C anti-coagulant pathway; inhibits factor V and VIII. Protein S act as co-
factor.
d. CI- esterase inhibitor neutralizes activated factor XIII, XI and plasma kallikrein
e. A2 macroglobin inhibits kallikrein, thrombin and activated factor X
f. Prostacyclne causes disaggregation of platelet
g. Nitric oxide is a powerful inhibitor of platelet activation and a potent vasodilator
2. Breakdown of fibrin clot(fibrinolysis); plasmin hydrolyses fibrin into fibrin degradation
product.
3. Phagocytic cells of reticulo-endothelial system also remove fibrin
ABNORMAL HAEMOSTASIS; excessive bleeding during and / or after operation
Platelet abnormality- quantitative (e.g thrombocytopenia) or qualitative(e.g Glanzman’s
disease.)
Deficiency of clotting factors
Anticoagulants
Vascular problems
CAUSES OF BLEEDIND DIATHESIS
1. PLATELET ABNORMALITIES
Platelet deficiency (thrombocytopenia); <150 × 10⁹/L. excess bleeding occurs in <50 ×
10⁹/L and spontaneous bleeding occurs in <20 × 10⁹/L
Types;
idiopathic i.e. primary seen in children and infants probably due
to immune deficience

[email protected] Page 90
secondary; causes include; d
drugs- sulphonamides,quinine, quinidine, phenacitin, cytotoxics,
cephalosporins, indomethacin, serdomid, para-aminosalysilic acid,
phenylbutazone,
infections; rubella, mumps, infectious mononeucleosis, HIV,
malaria, leishmania.
Hyperslenism
Some malignancies; acute leukemia, lymphoma, MM, bone
metastesis
Collagen disease; SLE, rheumatoid arthritis and dermatomyositis
Irradiation
Treatment;
If drug found, it is stopped and the operation delayed if not urgent
Idiopathic or hyperslenism- splenectomy
ITP- steroid oral for elective until platelet is normal. In emergency IV
immunoglobulin
Transfusion of platelet concentrate during operation in emergency or 2L of
fresh whole blood(i.e blood collected within 3hours)
Qualitative platelet dysfunction;
Congenital or acquired
Congenital; Bernard-soulier syndrome(BSS) and Glanzmann’s thrombasthemia(GT)
They are autosomal recessive
Common with consanguinity
BSS is due to defect in platelet adhesion and GT in aggregation
Present as spontaneous bruises, epistaxis, bleeding gums, petechiae, menorrhagia
BSS differs from GT by thrombocytopenia and giant platelet in the peripheral blood
Mgt; desmopressin(DDAVP) and recombinant factor activated factor VII, platelet
transfusion in severe hemorrhage.
Acquired; Aspirin ingestion and ureamia

[email protected] Page 91
Aspirin impairs aggregation, ADP release and TXA2 synthesis. If ingested within 7days of
surgery, excess bleeding may occur.
Ureamia increase levels of guanidinosuccinic acid and phenolic acid which impairs
platelet function. The defect improve after dialysis.
2. DEFICIENCY OF COAGULATION FACTORS
I. Hereditary
Haemophilia A
von Willibrand’s disease
Haemophilia B (christmas disease)
II. Acquired
Vitamin K deficiency
Ureamia
Massive blood transfusion
Disseminated intravascular coagulopathy (DIC)
HAEMOPHILIA A
Caused by deficiency of factor VIII
Symptoms occur when factor VIII activity is < 30%
Sex-linked recessive
Presents with subcut and intramuscular haematoma, haemarthrosis occasionally GI
bleeding, prolong bleeding from site of injury or surgery
• Clinical severity depends on extent clotting factor deficiency
<1% activity - severe disease with life-threatening bleeding
1-5% activity - moderate disease with post-traumatic bleeding
5-20% activity - mild disease
Laboratory findings
Factor VIII levels are; low; < 2u/dl (severe), 2-10u/dl moderate), > 10-30u/dl (mild) .
The bleeding and prothrombin times- PT are normal.
The partial thromboplastin time-PTT, a measure of intrinsic pathway is always
prolonged.
The clotting time is usually prolonged.
Treatment
• Bleeding episodes are treated with factor VIII replacement
[email protected] Page 92
• Given as either factor VIII concentrate or cryoprecipitate
• Bleeding usually well controlled if factor VIII levels raised above 20%
normal
• Desmopressin increases intrinsic factor VIII levels
• 5-10% develop antibodies to factor VIII
• Renders patients refractory to factor replacement therapy
von Willebrand’s disease; caused by deficiency of von Willibrand’s factor resulting in excessive
catabolism of factor VIII which leads to low circulatory levels. It is autosomal dominant. There is
an associated platelet dysfunction.
Laboratory findings;
Factor VIII level is low
BT and PTT are prolonged
PT is normal
Clotting time may be normal or prolonged depending on the factor VIII level
Impaired platelet aggregation with ristocetin
Reduced von Willebrand’s factor or ristocetin cofactor activity
Treatment
Desmopressin in mild cases
Severe cases are treated with factor VIII concentrate, cryoprecipitate, FFP, vWF
concentrate. In the absence of these fresh whole blood may be used
CHRISTMAS DISEASE (HAEMOPHILIA B)
Factor IX deficiency
Only PTT and clotting time are prolonged
Factor IX is low
Treatment is with double dose of factor IX
FFP or fresh whole blood can be used in the absent factor concentrate
VITAMIN K DEFICIENCY
In vitamin k deficiency there is impaired synthesis of factors- II, VII, IX, and X leading to
bleeding.
Causes of vitamin K deficiency
Obstructive jaundice and steatorrhoea
Malabsorption syndrome and high enterocuteneous fistulae
Hepatocellular disease
Prolonged broad-spectrum oral antibiotics

[email protected] Page 93
Warfarin therapy
Laboratory findings
INR is > 2
PTT is prolonged if factor X and II are severly depressed
Treatment
Vit K, 5mg IM, is administered daily for 3-5 days before operation. In an emergency, 10-
20mg Vit K given IV or IM will significantly correct the deficiency in 8-12h.
If it is not detected before operation and bleeding occurs. FFP 9-15ml/kg or fresh whole
blood 15-20ml/kg must be infused in less than I h.
UREAMIA
Coagulation screening tests are usually nonnal. The bleeding time, however, is prolonged due to
impairment of platelet function and platelet-vessel wall interaction. These abnormalities are
corrected by haemodialysis. IV. DDAVP 0.3-0.4u/kg reduces bleeding episode
MASSIVE BLOOD TRANSFUSION (see above)
DISSEMINATED INTRAVASCULAR COAGULOPATHY (DIC)
• Due to widespread intravascular activation of clotting cascade
• Causes a bleeding tendency due to consumption of clotting factors
• Presents with bruising or purpura
• Oozing from surgical wounds and venepuncture sites
Causes
• Severe (usually gram-negative or meningococcal) infection
• Widespread mucin-secreting metastatic adenocarcinoma
• Hypovolaemic shock
• Severe trauma
• Burns
• Transfusion reactions
• Eclampsia
• Amniotic fluid embolus
• Fat embolism
• Promyelocytic leukaemia
• Open heart surgery with extracorporal circulation
• Viperine venom
[email protected] Page 94
Laboratory findings
•
Thrombocytopaenia.
Prolonged bleeding time.
Prolonged partial thromboplastin time.
Clotting time is prolonged; the clot formed is small and is soon lysed.
Thrombin time is prolonged.
Hypofibrinogenaemia.
Factors V and VIII are markedly depressed.
Increased FDP and D-dimer levels.
A fibrinogen level below 10g/L and a platelet count below 100 x 10⁹/L are diagnostic.
Treatment;
The precipitating cause is treated or removed.
Fresh frozen plasma is transfused to correct hypovolaemia and provide coagulation
factors.
6 units cryoprecipitate is given if hypofibrinogenaemia is severe. It will also provide
coagulation factors.
6 units of platelet concentrate is given if the platelet count is < 100 x 10⁹/L.
Fresh whole blood may be given if FFP, cryoprecipitate and platelet concentrate are not
available.

[email protected] Page 95
ANTICOAGULANTS
Warfarin
Heparin
Aspirin
Warfarin; interferes with hepatic synthesis of vitamin K dependent clotting factors- II,VII,IX and
X, as well as protein C and S. peak plasma time 2-3days
Heparin; low dose inactivates factor Xa and inhibits conversion of prothrombin to thrombin.
High dose inactivates factors IX, X, XI, and XII and inhibits conversion of fibrinogen to fibrin.
Peak plasma time 2-4hours
Aspirin; see above
VESSEL WALL
congenital
Hereditary haemorrhagic telangiectasia
Ehlers-Danlos syndrome
Acquired
Drugs (e.g. steroids)
Sepsis
Trauma
Vasculitis
Infections; Typhoid, SBE, Meningococcal meningitis, Gram-ve septicemia
Scurvy
Purpura
PERI-OPERTIVE CONTROL OF BLEEDING TENDENCIES
PREOPERTIVE
History
Bleeding tendencies, from orifices
Prolong oozing or massive haemorrhage
Family history

[email protected] Page 96
Drug history; aspirin, warfarin, heparin
Examination
Petechiae, bruises, jaundice, lymphadenopathy, palmar erythema etc
Splenomegaly, hepatomegaly
Investigation
FBC ,bleeding time, clot reaction, PT, PTT, platelet function test, fibrinogen, FDP, D- dimer
estimation, bone marrow examination
COAGULATION TESTS
Prothrombin time (PT)
Tests extrinsic and common pathways
Thromboplastin and calcium are added to patient plasma
PT is expressed as ration (International Normalised Ratio = INR)
Prolonged in:
Warfarin treatment
Liver disease
Vitamin K deficiency
Disseminated intravascular coagulation
Activated partial thromboplastin time (APPT, KCCT)
Tests intrinsic and common pathways
Kaolin added to patient plasma
Prolonged in:
Heparin treatment
Haemophilia and factor deficiencies
Liver disease
Disseminated intravascular coagulation
Massive transfusion
[email protected] Page 97
Lupus anticoagulant
Thrombin time (TT)
Tests common pathway
Thrombin added to patient plasma
Converts fibrinogen into fibrin
Prolonged in:
Heparin treatment
Disseminated intravascular coagulation
Dysfibrinogenaemia
Bleeding time (BT)
Measures capillary bleeding
Prolonged in:
Platelet disorders
Vessel wall disorders
TREATMENT :-
Stopping anticoagulant therapy
Dialysis/renal transplant for CRF patient
EPO in CRF, Jehovah witness
Anti failure regimen in hepatic failure
Vitamin K in neonates, liver Dx
Control of HTN
Platelet, factor conc., desmopresson, FFP administration as applicable
GXM
[email protected] Page 98
INTRA-OPERATIVE
This can be achieve via:
Mechanical
Thermal
Chemical
Surgical
TYPE OF ANAESTHESIA
Type of agents to be used
GA Vs Regional Vs LA
Adequate/intensive monitoring of blood loss as well as PaO2
SKILLED SURGEON/ASSISTANT
Proper knowledge of anatomy
Proper knowledge on principles of surgery
ADEQUATE LIGHTENING: ENSURE PROPER VISUALIZATION
POSITIONING:
Trenderlenburgh
Reverse trenderlenburgh
Head tilt to 30 degrees or more in head and neck surgeries
Lateral tilt
MECHANICAL METHODS
Use of tourniquet with or without exsanguination
Direct pressure:
Finger pressure e.g nose pinching in epistaxis, direct pressure in scalp bleeding,
Pringles' maneuver
Pressure packs (wet or dry)
Use of swabs
Use of balloons eg catheter, Sensetaken-Blakemore tube, Minnesota
Elevation with evertion eg in scalp surgeries
Haemostat

[email protected] Page 99
Ligatures
THERMAL METHODS
Cold packs: causes vasospasm and endothelial adhesiveness, increases local
haematocrit; Risk of hypothermia, ventricular fibrillation and thrombocytopenia esp at
temp <35
Cold saline
Warm packs: controversial
Cautery
Diathermy
Cryosurgery : Extreme cooling of -20 to -180 is used. Causes cryogenic necrosis
through dehydration and lipid denaturation. Useful in neurosurgery and some
gynaecological procedures
Laser surgery
CHEMICAL AGENTS
They vary in their MOA. Some have vasoconstrictive effect, some anticoagulant, some
inert with hygroscopic ppties
Epinephrine : in tonsillectomy, epistaxis
Octreotide
Skeletal muscle in the past (introduced by Cushing)
Gel foam (gelatin foam): made from denatured animal skin gelatin. Improve action in
combination with thrombin
Oxycel & surgicel: both are oxidized cellulose materials. They combine with blood to form
artificial clot. Surgicel have antibacterial effect
Requires phagocytosis for removal in 1-4wks
Impairs wound healing
Microcrystalline collagen: same ppties with surgical
Fibrin glue: Have same ppties with body’s fibrin. Good for oozing blood from liver and
spleen surfaces
Bone wax: bees wax.
paraffin as softening agent
Ostene: water soluble. Made from alkylene oxide copolymer derived from ethylene &
propylene oxide
[email protected] Page 100
SURGICAL METHODS
Shunting eg portocaval, lienorenal
Resections
Splenic
Hepatic
renal
Grafting:
Venous graft
Synthetic graft
Dacron
Expanded polytetrafluoroethylene E-PTFE
POST-OP CONTROLOF BLEEDING
Dressing
Firm/gentle not to compress blood supply
Use of Vaseline gauze
Post-op monitoring of pts with bleeding tendencies by regular checking of clotting profile and
prompt treatment depending on the situation
FUTURE TREND
General aim is towards bloodless surgeries.
Microvascular surgery
Use of hemobag for modified ultrafilteration in ECMO during cardiac surgeries
Harmonic scalpels
Arterial embolisation
OPERATIONS ASSOCIATED WITH EXCESS BLEEDING
1. Prostatic surgery
2. Transplant surgery
3. Portocaval surgery
4. Extracorporeal circulation

[email protected] Page 101
METABOLIC RESPONSE TO TRAUMA
Characteristic series of local and systemic adaptive homeostatic responses by an organism
following cellular injury/trauma or sepsis aimed at restoring body’s pre-injury state.
Appropriate response maintains homeostasis and allows wound healing. Excessive response can
produce systemic inflammatory response syndrome (SIRS) and multiple organs dysfunction
syndrome (MODS).
ACTIVATION OF THE METABOLIC RESPONSE
Pain
Hypovolemia
Hypothermia
Infection
Hypoxia
CONTROL OF RESPONSE
Sympathetic nervous system
Acute phase(inflammatory) reaction
o Cytokines
o Acute phase proteins
Vascular endothelium and blood response
Endocrine response
PHASES OF RESPONSE
EBB
FLOW
EBB PHASE; The ebb phase corresponds to the period of severe shock. Immediately after
trauma and lasts 24-48 hours. Reversible by resuscitation. Priority is to maintain
life/homeostasis. There is decrease in the following;
Cardiac output
Oxygen consumption
Blood pressure
Tissue perfusion
Body temperature
Metabolic rate
FLOW PHASE; In the flow phase, the body is hypermetabolic, cardiac output and oxygen
consumption are increased, and there is increased glucose production. Lactic acid may be
normal. It is further subdivided into;

[email protected] Page 102
Catabolic phase- lasts for 3-10 days. There is fat and protein mobilization associated
with increased urinary nitrogen excretion, weight loss
Anabolic phase- lasts for 10-60 days. Restoration of fat and protein stores, weight
gain.
FACTORS INFLUENCING MAGNITUDE OF RESPONSE;
Nature and severity of injury
Nutritional status
Sepsis, underlying disease
Age- Sex
Environmental temperature
Treatment – timing, type and effectiveness
Drugs (Steroids, NSAIDS)
ATTENUATING FACTORS
Prompt correction of fluids and electrolytes
Analgesia and anaesthesia-spinal/epidural
Minimally invasive surgery
Use of prophylactic antibiotics
Wound debridement
Early enteral feeding
SUMMARY OF EVENTS
COMPLICATIONS
• SHOCK
• SIRS
[email protected] Page 103
• MOD/MODS
• DEATH
PRE AND POST-OPERATIVE CARE OF THE SURGICAL PATIENT
Introduction
Assessment of operative risk
Personal relationship
General preparation: History, PE, Investigation
Risk analysis of the patient vis-à-vis the surgery
Now patient is fit
Peri op care
Post op care
INTRODUCTION
The ultimate goal of preoperative, intraoperative and postoperative care of the surgical patient
is to reduce morbidity or mortality and to return the patient to desirable functioning
(premorbid state or better) as quickly as possible
I. Assessment of Operative Risk
A. Natural History
relative harm (risk)
relative good (benefit)
B. Stages of the disease- error in clinical staging produces the greatest number of
controversies regarding management
C. Clinical Judgment- deviations of standard treatment is associated with significant
increase in mortality and morbidity
D. Basic Factors Affecting Operative Risk
1. Age over 70 years
2. Overall physical status
3. Elective vs. emergency surgery
4. Extent of pathology
5. Associated illnesses
[email protected] Page 104
II. Personal Relationship
A. Genuine bond of communication and personal responsibilities.
B. Do not convey a sense of hurry and inadequate time for explanations.
C. Demonstrate skills to contribute to diagnosis and treatment.
D. Specific treatment.
E. Informed consent
III. General Preparation of the Patient
A. Psychological preparation
1. Pre-op steps should be enumerated, justified and explained.
2. Surgeons should not equivocate in discussing possible disfiguring operations.
HISTORY
Previous illness
Previous surgery and anaesthetic experience
Concurrent diseases
Drug therapy e.g prolonged use of steroids
Social hx: alcohol, smoking
EXAMINATION
Respiratory system: treat infections. Spirometry. BGA/PH checks
Cardiovascular system: anaesthesia reduces CO by about 20%. Note- predictors of
cardiac risk (MI, CCF, etc), pt’s functional capacity, the procedure to be carried out
Urinary system: Albumin, casts, cells, sugar, ketones, urea level
Gastrointestinal system: carious and loose tooth. Treat mouth infections. Stool exam
→deworm
Blood picture: CBC, Sickling test. Bld trx at least 3 days to time of surgery. May use parenteral
iron therapy or recombinant erythropoietin. For bleeding tendency/jaundiced pts-platelets,
prothrombin, bleeding and clotting time
Hydration and Nutrition: ↓ K → difficulties with reversal of muscle relaxants.
Malnutrition: BMI used (weight[kg]/ht2[m2])
[email protected] Page 105
Malnutrition may be evidenced by weight loss. For example, in the absence of dehydration,
loss of ≥ 10kg in the last 6 months or loss of 5% in the last month calls for closer review.
Also determine Lymphocyte count, Albumin(˂3.5gm/dl-treat), Prealbumin, total
proteins(˂5.4gm/dl-treat).
NERVOUS SYSTEM
Examine the tones. Check for conditions that may interfere with the anaesthetic agents-
myasthenia gravis, suxa in the presence of hyperkalemia may produce cardiac arrest, where
there is active demyelinating dx, a muscle spasm instead of relaxation and there may also be
malignant hyperpyrexia. It can influence the type of anaesthesia all together.
PSYCHOLOGICAL STATE
No two patients are exactly the same
May need to sedate them
MINIMUM INVESTIGATIONS
Hb, pcv, sickling, Urinalysis - albumin, sugar, casts, Stool for amoebae and worms
Hypertensives and pts ˃40yrs; Chest x ray, ECG, FBS
INVESTIONS DONE WHEN INDICATED; Fbc, Sickling electrophoresis, Blood group/ x
matching, Serum e/u, Chest x ray, ECG, Plasma proteins, PT, clotting & bleeding time, clotting
factors, G6PD, FBS, FBS
Other measures;
Obstructive Jaundice: adequate hydration, vit k, antibiotic prophylaxis.
?Bowel prep for colonic surgery
Treat infective skin lesions
Pts on steroids: Replacement dose- hydrocortisone or methylprednisolone
Assessment of risks- ASA
ASA 1- a normal fit patient
ASA 2-Mild systemic dx e.g. Hb AS, controlled bp,dm, mild asthma,
ASA 3- A pt with systemic dx that limits activity but not incapacitating. E.g renal dx pt on
dialysis
ASA 4- A pt with incapacitating systemic dx that is a constant threat e.g septic shock

[email protected] Page 106
ASA 5-Moribund.Not expected to live˃24hrs
ASA 6 – Brain dead organ donor
CHILDS-PUGH’S GROUPING OF SEVERITY OF LIVER DX
Childs-pugh’s grading: Interpretation
A. Less than 6 points: Good operative risk
B. 6-9: Moderate risk
C. Above 10: Poor risk
NOW THE PATIENT IS FIT FOR SURGERY
Consent
Bowel prep
Bladder
Empty stomach
Remove dentures
Pre anaesthetic med
Adequate labelling
Diabetics – may require special prep
PREPARING DIABETIC FOR OPERATION
I. Those on diet alone treat as normal pts
II. If on oral hypoglycaemics, stop the biguanides. Use sulphonylureas
III. Alberti regime: 500mls of 10% g + 10units of SI + 1gm of KCl to run for 4hrs. 2hrly
check of sugar and K. May use 5% d/w with 5 units of SI. Aim at 4-10mmol/l and 3.5-
4.5mmol/l for sugar and K respectively
IV. Some use sliding scale
PERIOPERATIVE CARE
Check equipments/drugs. Note that equipment may malfunction. The hands must not go to
“sleep” Adequate positioning.
Monitoring: anaesthetist, surgeon, nurses. The patient belongs to all
Blood loss estimation
Watch for and prevent; Hypothermia, Hypotension, Hypertension, Cardiac
arrhythmias, Cardiac arrest, Hypoxia, Asphyxia (combination of hypoxia and
hypercapnia and caused by respiratory obstruction)
[email protected] Page 107
POST OPERATIVE CARE
Determinants of outcome:
Basic pathology
Effect of surgery including blood loss
Duration of surgery
After effects of the anaesthesia
Complications during surgery
After surgery
Recovering room or icu. monitoring
Supervise mvt to ward on a trolley with sides
Control airway
Ward shd be prepared with relevant equipments e.g supplemental oxygen,etc
Adequate care on the ward e.g Oxygen, airway mgt, vitals, adequate pain mgt. take
care of the patient who is vomiting-position
Nutrition/Fluid
Urine
Ambulation
Use of low molecular weight heparin
Wound
Daily visits ± physiotherapy
Hb on 3rd day
Other investigations as required
Fluid; see chapter on fluid mgt
Pain mgt
Preventing circulatory stasis
Leg exercises
TED stockings (Thrombo Embolic Deterrent)
Early ambulation
Positioning
Anticoagulants
Fluid intake

[email protected] Page 108
WHAT COMPLICATIONS DO I WATCH OUT FOR?
Post-operative complications are untoward conditions occurring within 30 days of
operation, or after 30 days but directly related to the operation.
First few hours:
Respiratory insufficiency
Cardiovascular emergencies
Reactionary haemorrhage
Central nervous problems
Others e.g. hypothermia in the neonate
Complications after 24hrs;
Respiratory tract
o Atelectasis
o Pneumonia
o Hiccough
o Tracheobronchitis
o Pulmonary embolism
Cardiovascular
o secondary haemorrhage, MI, DVT, PE
Genitourinary tract
o Retention of urine, Acute renal failure, UTI
Gastrointestinal tract
o N/V, gastric dilatation, paralytic ileus, peritonitis, intra abd abscesses,
constipation, Diarrhoea, pseudomembranous colitis, Upper GI bleeding,
Jaundice
Central Nervous system
o Delirium
The wound; Haematoma, SSI, Wound dehiscence
Late complications
Incisional hernia
Mech int obst from bands and adhesions

[email protected] Page 109
CARDIAC ARREST
Sudden cessation of a demonstrable heart beat with no clinical cardiac output in a patient not
expected to die. Clinical death: pt stops breathing and the heart stops also
Brain death: when the brain undergoes irreversible damage from oxygen deprivation after
cardiac arrest. Usually 4-6 mins after an arrest
Causes of cardiac arrest;
Resp obstruction, asphyxia, hypercarbia
Severe haemorrhage leading to hypovolaemia
Shock
MI
Massive transfusion
Acidosis,
hyper or hypo K,
hypothermia
Tension pneumo, PE, cardiac tamponade
Making a diagnosis of cardiac arrest;
Absent pulsations in major peripheral arteries
Unconsciousness
Apnoea
Dilated unreactive pupil
Managing cardiac arrest
Airway opened
Breathing restored
Circulation begun
Definitive therapy(drugs, diagnosis, defibrillation, disposition)
POST-OP FEVER
- elevated temperature observed in post-op patients does not necessarily signal a serious
complication
[email protected] Page 110
- a specific cause is identified in 20% of patients with pyrexia during the initial 24 hours
- comprehensive clinical evaluation is essential
Common causes of Post op pyrexia; (also remember the 5 ‘W’s – wind, water, wound,
walk and wonder drugs)
Metabolic response to trauma
Infection or haematoma
Malaria
Lung collapse, pneumonia, bronchitis
Laryngo-tracheitis
Peritonitis/intra-abdominal abscesses
Complications at sites of IVF
Complications from blood transfusion
UTI
DVT
Injection abscess
Sickling crisis in sicklers
Pseudo membranous colitis
Non-infective causes of Post-op Fever
1. Disseminated malignancy
2. Transfusion reaction
3. Hematoma
4. Administration of irritant fluids or drugs, drug sensitivity
5. Acute pancreatitis
6. Thyroid storm
7. Pheochromocytoma
8. Dehydration

[email protected] Page 111
MGT OF POST OP FEVER
History, examination, investigation and then treatment
Factors influencing likelihood of post-op infection
1. Definite decrease in host resistance
increasing age
obesity/malnutrition
diabetic ketoacidosis
acute/chronic steroid use
immunosuppressive drugs
remote infections
2. Post op infection
3. Possible decrease in host resistance
some forms of cancer
radiation therapy
adrenocortical insufficiency
foreign body
early shaving of the operative site
4. No effect on host resistance
gender
race
controlled DM
acute nutritional deprivation
Operations benefiting from antibiotic prophylaxis
1. Head and neck surgery with open aerodigestive tract
2. Esophageal except hiatal hernia repair
3. Gastroduodenal except for complications of uncorrected hyperacidity
4. Biliary tract surgery
patients over 70 years old
acute cholecystitis.

[email protected] Page 112
choledochostomy
5. Bowel resection
6. Perforated or gangrenous appendicitis
7. Hysterectomy
8. Revascularization and prosthetic graft surgery
9. Orthopedic surgeries with implantation of prosthesis
OPERATIVE TECHNIQUE TO MINIMIZE INFECTION
Eliminate hair, if necessary, just prior to incision time
Effective skin preparation
Gentle and effective handling of tissues
Effective hemostasis
Eradicate dead space
Minimize operative time
Closed suction drain a distance from the incision
DISCHARGE
written and verbal instructions; regarding follow-up care, complications, wound care, activity,
medications and diet.
Give prescriptions and phone numbers.
Discuss actions if complications occur.
CONCLUSION
Adequate pre op, peri op and post care of the surgical patient is essential
The best surgeon is the surgeon that knows when not to operate
[email protected] Page 113
SURGICAL PROPHYLAXIS
All sciences or acts to prevent perioperative complications. Eg tetanus prophylaxis, antibiotics
and DVT prophylaxis
ANTIBIOTIC PROPHYLAXIS
Antibiotics are chemical agents, synthetic or products of microbes which damage bacteria
without harming the tissues. They are more effective in controlling established infection than
prophylaxis. Indiscriminate use results in ineffectiveness and development of resistance.
Guidelines for prophylaxis
Single preop dose is as effective as a full five days course in uncomplicated procedure
Should be administered with one hour prior to incision, preferably at induction of
anaesthesia
Should target anticipated organisms
Should not extend beyond 24hours
In prolonged procedure, should be repeated every 3hours.
Wound type;
o Clean wound – not use except in immunosuppressed, implant surgery, esp
vascular and cardiac surgeries, neurosurgical operations, excess blood loss.
o Clean contaminated and contaminated – use prophylaxis
o Dirty wound treat rather than prophylaxis.
Drug with low toxicity, long serum half-life, broad spectrum and low cost is use
DVT PROPHYLAXIS
Deep venous thrombosis is the formation of blood clot in one of the deep veins of the body
usually the lower limbs. The outcome is devastating; PE or venous gangrene. For optimal
prophylaxis, risk factors as well as risk categorization most be noted.
Risk factors
Patient factors;
Age >40years
Obesity
Varicose veins
Immobility(bed>3days)
Pregnancy

[email protected] Page 114
Pueperium
High dose oestrogen therapy
Previous DVT or PE
Thrombophilia
o Deficiency of antithrombin III, Antihospholipid antibody, lupus anticoagulant
Disease /surgical procedure
Trauma
Surgery esp. pelvic, lower limb
Malignancy
Heart failure
Recent MI
Paraplegia
Infection
IBD
Nephrotic syndrome
Polycythemia
Paraprotinemia
PN hemoglobinuria
Homocystinaemia
RISK CATEGORY (THRIFT consensus group)
High risk > 40%
• Major surgery
• Pelvic, hip fractures
• Major surgery in a patient with malignancy
• Major surgery in a patient with history of DVT or > 60years
• Lower limb paralysis or major amputation
Moderate risk 5-40%
• Major surgery in patient > 40years not in high risk group
• Major surgery or lower limb surgery in patient on oral contraceptives
• Major medical illness with prolonged immobilization
Minor risks <5%
• Minor surgery (<30min) with no risk factors
• Major surgery (>30min) in patient <40years or with no risk

[email protected] Page 115
PROPHYLAXIS
Preoperative
Weight reduction
Stoppage of OCP 1month prior to surgery
Identification of high risk – by risk categorization
Aspirin
Oral anticoagulants
Low dose subcut heparin
Dextran 70
Intraoperative prophylaxis
Epidural anaesthesia
Physical means
o Electrical calf stimulation
o External intermittent pneumatic compression of calf
o Passive leg exercise (foot pedaling machine)
Chemical means (as commenced preoperatively and continued until patient is mobile)
o Low dose subcut heparin
o Dextran 70
Post operatively
Pressure graduated elastic stockings
Early mobilization, massage and leg movt
Adequate hydration
NB; for established DVT, as confirmed by; Doppler, ascending contrast venography or
impedance plethysmography it is treated
I. Anticoagulant therapy
a. LMWH
b. Unfractionated heparin if LMWH not available
c. Warfarin (72hours before heparin is stopped )
II. Thrombolytic therapy
a. Streptokinase
b. Tissue plasminogen activator
III. Operative; venous thrombectomy, interruption of inferior vena cava- Greenfield filter.

[email protected] Page 116
TETANUS PROPHYLAXIS
Tetanus infection result from wound invasion by clostridium tetani- a gram positive spore
forming obligatory anaerobic bacillus. They produce exotoxins; most importantly the
tetanospasmin which affect the nervous system producing its characteristic clinical picture.
Clinical forms;
Generalized tetanus
Localized tetanus
Cephalic tetanus
Neonatal tetanus
Features
Trismus
Risus sardonicus
Muscle stiffness and pains- neck, back, abdomen and region of wound.
Opisthotonus in severe cases
Exhaustion and respiratory failure leads to death
There may be associated autonomic dysfunction
Prophylaxis
This is achieved by immunization. The active and passive forms. The active(toxoid) stimulate
the body to produce antibodies. More effective but takes 2-3months to be operational. The passive
uses preformed antibodies in form of human or equine tetanus immunoglobulin. It is
immediately operational but less effective and may precipitate anaphylaxis.
Immunization depends on;
Immune status of patient
Degree of wound contamination
Patients are categorized into;
Fully immunize- do not require prophylaxis
o Completed toxoid and booster within past 5years
Partially immunize
o Completed toxoid, but booster >5years <10years- give a dose of toxoid.
o Completed toxoid but booster > 10yers. For clean wound give toxoid, for dirty wound
give toxoid and immunoglobulin
Not immunize or immune status unknown

[email protected] Page 117
o Clean wound, give toxoid complete course. Dirty wound toxoid complete course
plus immunoglobulin
Active immunity
Traditional; 1ml of toxoid subcut/im start, 6weeks, 6months and every 10years
Rapid method (alum-precipitated toxoid); 1st, 4th and 7th day. Active immunity is
demonstrated in 28days.
Passive immunity
Human immune globulin. 250-500IU, Protective antibodies for at least 4-6weks.
Does not produce serum sickness
Anti tetanus serum ATS; 1500IU subcut after test dose. Use only when HIG not
available. has high risk for serum sickness. Protection 7-10days
NB; for established tetanus, treatment;
I. Neutralize toxin
Daily HTIG 500IU until 3000-6000 or start of ATS 200,000IU after a test dose.
II. Prevent further toxin production
Wound debridement
Antibiotics
III. Control spasms
IV. Management of autonomic dysfunction
V. Supportive care

[email protected] Page 118
SICKLE CELL DISEASE AND THE SURGEON
Sickle cell disease refers to a condition in which an individual has inherited two abnormal Hb
gene, at least one of which is haemoglobin S (HbS) and the resulting problem is attributed to the
sickling phenomenum. Eg HbSC, HbSD, HbSS.
Sickle cell anaemia is the most severe form of sickle cell disease characterized by inheritance of
two sickle haemoglobin(HbSS).
Surgery in a sickle cell disease is associated with higher morbidity and the management is
multidisciplinary. Improvement in outcome is seen with meticulous care and follow-up.
EPIDEMIOLOGY
Highest prevalence in tropical Africa and slave trade countries. In Nigeria, 2-3% of live birth have
SCA, 0.4%(1-4years), and 0.05%(>7years). Sickle cell trait affects 30% of northern Nigeria
population and 24% of southern population.
PATHOLOGY
Sickle cell haemoglobin gene is inherited as autosomal recessive. Normal haemoglobin has two
alpha and two beta chains. In sickle disease, single amino acid substitution occurs on beta chain.
Valine is substituted for glutamic acid at position 6. SCA is homozygous, sickle cell trait is
heterozygous. The resulting HbS is less soluble than HbA. When deoxygenated, the HbS
undergoes polymerization and forms characteristic sickle cell. There is premature distruction of
rbc, there is reduced oxygen carrying capacity and increased blood viscosity. Blockage of small
vessels results in vaso-occlussive events. Sickling may be precipitated by infection, fever,
dehydration, cold, hypotension, hypoxia, stress-trauma, exercise, sport, emotional disturbances.
Types of crisis; haemolytic, aplastic, sequestration and vaso-occlussive.
PRESENTATION TO A SURGEON
They could present as emergency or elective pathologies which could be sickle cell related or non-
sickle cell related as in other patients.
Sickle cell related problems;
Gastrointestinal tract;
Liver
Hepatomegaly with abnormal liver function.
Progressive liver damage is due to
i. Congestive hepatic crisis
ii. Cholestasis
iii. Viral hepatitis
[email protected] Page 119
iv. Intrahepatic obstructive jaundice –
Cholelithiasis :
i. pigment stones due to chronic haemolysis
ii. 6-49% in SCD
iii. 20% have stones in common bile duct
iv. Treatment : Conservative
Cholecystectomy
Spleen
I. Acute splenic sequestration - major cause of death in the first 2yrs of life.
Treatment = packed cells, Parent education. Splenectomy- (i) after
prophylaxis for pneumococcus + H.influenza.
II. Hypersplenism
-Increased spleen 4cm BLCM
-Hb <6.5g/dl
-Platelets <200 x 10⁹/L
-Reticulocytes >15%
-2 occasions 6/12 apart
Intestine
Extensive collateral circulation protects against sickling phenomenon.
Intestinal infarction - malaena, ileitis, peritonitis, adynamic intestinal obstruction
Mesenteric infarction mimicks acute abdomen
Genitourinary
PRIAPISM; painful sustained erection .
60% in pt <12yrs : sleep
Sickling in the corpora carvernosa - congestion of the penile outflow tracts.
2 types based on severity :
i. Short shuttering attacks <3hrs
ii. Major >24hrs
Conservative
Surgical -drainage by caverno-spongiosal shunt with trucut needles (via the glans)
Impotence due to penile fibrosis if >24hrs.
-Penile implants – difficult to trea - migration due to corpora cavernous fibrosis

[email protected] Page 120
Bones
Osteomyelitis
AVN
Secondary osteoarthritis
Coxa vara
Spontaneous hip fracture
Generalized osteoporosis
Soft and thin inner cortex
Skin and limbs
Commonest surgical problem
10% in W/Africa ; 2% in Hb SC
Peak incidence age group- 15-19yrs
90% in distal 1/3rd of the leg above the medial malleolus
30-50% are bilateral.
2-10cm, punched out appearance with raised edge.
Usually superficial + deep
The eye
Sluggish flow, intravascular sickling, occlusion of vessels:- necrosis-collateral
Stage 1- dilation + increased tortuosity of vessels.
Stage 2- AV nipping, micro aneurysms common btw small arterioles + venules
Stage 3- neovascularization
Stage 4-proliferative neovascularization of the vitreous
Stage 5- retinal detachment (fibrovascular detachment) - ocular changes are
common in HbSC.
Rarely require or benefit from therapy.
Scatter photocoagulation for early lesions
Pregnancy
Impaired placental bld flow
Spontaneous abortion
IUGR
Pre-eclampsia
IUFD
prevent severe anaemia, infection & VOC
Management
Elective caesarian section
[email protected] Page 121
MANAGEMENT
I. Pre-operative; aims to prevent the development of crisis by treating infection and avoiding
other precipitants, taking detail history, physical examination, investigation and adequate
optimization. NB; those presenting as emergency are resuscitated.
Investigations; genotype, FBC, septic work-up, CXR, GXM, U/ECr, others depends on the presenting
pathology
General measures;
Analgesia
Expand plasma volume: glucose, fructose.
Difficult IV access
Alkalinize blood: NaHC03, lactate
Anticoagulation -pts who are prone to embolism
Eliminate infective foci (respiratory, UTI), treat malaria
Blood transfusion - avoid increased viscosity
Anaemia
Hbss 6-10g/dl (steady state) (avg-8g/dl)
Hbsc 12g and above
HbSC thal 11g/dl
Hb Sf 10g/dl
Informed consent
First on the operation list
II. Intra-operatively
a. Anaesthesia; GA, regional (preferable). Adequate analgesia with pre-oxygenation.
b. Preoperative antibiotics
c. Position; reduced blood loss- limb elevation, reverse trendelenberg in head and neck
operation
d. Tourniquet; relatively contra-indicated(no exsanguination), adequate timing
e. Shortened operation time
f. Avoid sickling triggers ;
i. Dehydration- adequate rehydration
ii. Hypoxia : preoxygenation
iii. Hypotension : minimum drug doses
iv. Hypothermia- temperature regulation, warm fluids
v. Judicious blood replacement using fresh blood
g. Adequate monitoring – SPO2, BP, PR, TEMP., urine output.
III. Post-operatively
a. Continuous monitoring
b. Oxygen administration

[email protected] Page 122
c. Adequate analgesia
d. Adequate hydration
e. Temperature control
f. Early ambulation
IV. Follow-up
a. Effectiveness of treatment
b. Identify complications
c. Address concerns of patient
CURRENT TRENDS
Pain mgt
Infection control
Induction of fetal haemoglobin – hydroxyurea,
Haemopoetic cell transplant
Laparoscopic surgery
CONCLUSION
No surgeon is exempt. Appropriate preoperative evaluation minimizes intra- and post-operative
complications. Effective multidisciplinary management and identification of risk factors reduces
morbidity and mortality.

[email protected] Page 123
DIABETIC AND SURGERY
Introduction
Epidemiology
pathology
Presentations
Management
Conclusion
INTRODUCTION
Diabetes mellitus is metabolic disorder characterized by abnormality in insulin production and utilization
with resultant hyperglycemia and excessive fat and protein breakdown. The have glucosuria and RBS of
11.1mmol/L, FBS of >7mmol/L in two occasions or two hourly blood glucose after oral 75g glucose of
11.1mmol/L.
EPIDEMIOLOGY
Estimated about 171 million people suffer from DM worldwide. Surgical problems are more common in
diabetic than non-diabetic. 80% of diabetic are over 40years of age and surgical procedures are more
common in this age group. >50% would have one form of surgery or the other in their life time
PATHOLOGY
Diabetic complications results from interplay of vasculopathy (macroangiopathy and microangiopathy),
neuropathy and susceptibility to infection (impairment of cellular and humeral immunity).
PRESENTATION TO A SURGEON
They could present as elective or emergency with diabetic or non- diabetic related pathologies just like
other surgical patients.
Diabetic related problems;
Peripheral vascular insufficiency
o DM foot, DM hand syndrome
Retinopathies, cataracts
Infections
o cellulitis, carbuncle, abscess
o pyomyositis
o osteomyelitis
o moniliasis (vulvulitis and balanitis )
o tuberculosis
o UTI

[email protected] Page 124
PRE-OPERATIVE PREPARATION
Aims; to prevent ketosis and avoid hypoglycemia.
Details history and physical examination. Look for presence of complications e.g neuropathy,
retinopathy, hidden infections as well as autonomic neuropathy – postural hypotension, gastroparesis,
neurogenic bladder and erectile dysfuntion. As well as other co-morbidities eg hypertension
Investigation; Urinalysis, FBS, 2HPP, E/U +Cr, HbA1c, ECG, CXR, septic work-up, others depend on the
presenting pathology.
Other Perioperative considerations for elective setting include
Stopping cigarette smoking at least 2weeks before surgery
Prophylaxis against DVT
Antibiotics prophylaxis
First on list
All electrolyte derangement are corrected. Further preparation depends on;
Nature of operation- minor or major, elective or emergency
On what patient achieves control
Glycemic control of patient
Elective cases are admitted two days before operation and monitored serially for blood sugar. Elective
cases with uncontrolled sugar should be postponed until control is achieve
Minor surgery;
Patient controlled on diet on diet are only treated as normal patient but 1st on the list
Those on oral hypoglycemic drug should be taken off biguanides and sustained on short acting
sulphurnylurea. The agent may be omitted on the day of surgery
Those on long acting insulin (lante). Start an intravenous infusion of 5% DW early in the morning
of surgery and give half the usual dose of the long acting.
Major surgery
All forms of DM going for major surgery, those on oral hypoglycemic drug are stabilized on
soluble insulin for tight control. They are placed on NPO and commenced GKI on the morning of
the surgery with monitoring until post operatively when patient commences orally.
Emergency
Those going for emergency are resuscitated with IV fluids then IV soluble insulin bolus(10IU) and
in infusion(10IU/hr) until a serum glucose of ≤14mmol/L is achieved then placed on GKI or

[email protected] Page 125
sliding scale with continuous monitoring. NB; other components of resuscitation depending on
type of emergency
GKI- GLUCOSE-POTASSIUM-INSULIN infusion in a ratio of 10:10:10 or 5:5:5 that is 5% DW, 5mmol of K,
and 5IU insulin to run over 4hours with 2hourly monitoring of serum glucose and potassium.
Aims; to maintain a serum glucose of 4-10mmol/L and K of 3.5-4.5mmol/L
Two IV access is secured; one for the GKI and the other for the maintenance infusion.
If the serum glucose rise above 10mmol/L a bolus of soluble insulin is give 2IU per 2mmol/L rise.
Likewise if it falls below 4mmol/L GKI is stopped given only DW infusion.
The GKI is continue until patient is recommenced orally and placed on previous regimen.
INTRA-OPERATIVE MANAGEMENT
Anaesthesia; regional anaesthesia is preferable because it produces little metabolic disturbance. The
stress of general anaesthesia, surgery could predispose patient to hyper or hypoglycemia and
hypotension. These should be monitored throughout anaesthesia. As well as the serum potassium as
the GKI is continued.
POST-OPERATIVELY MANAGEMENT
The postoperative goal is to maintain blood glucose between 8.5-14mmol/L. insulin containing infusion
is continued with strict monitoring until commenced orally. The placed on previous controlled regimen.
CONCLUSION
The current high standard of surgical and anaesthetic technology make surgical outcome in diabetics
comparable to non-diabetic

[email protected] Page 126
PROSTATE BIOPSY
Indications;
DRE features of malignancy
Elevated PSA > 10ng/ml
o NB; 4-10ng/ml other parameters. Density 0.15ng/ml, velocity 0.75ng/ml/year, % free
PSA< 25%
Paraplegia in suspected CAP
Screening for prostate Ca in asymptomatic patient >50years(life expectancy >10years, family hx,
African-American> 45years)
Follow-up biopsy (3-6months) after diagnosis of PIN or ASAP
Contra-indications
Coagulopathy
Painful anorectal conditions
Severe immunosuppression
Acute prostatitis
Preparation of patient
Informed consent
Stop all anticoagulant
Prophylactic antibiotic
Cleansing enema
Analgesia
o Topical
o Local prostatic block
o Skin infiltration
Positioning
o left lateral decupitus position with the hips and knees flexed at 90°
o lithotomy
Technique
o transrectal prostate biopsy
TRUS guided ; sextant biopsy, extended core biopsy
o Transperineal
o Transurethral

[email protected] Page 127

[email protected] Page 128
Complications
o Post biopsy infection
o Bleeding
o Acute urine retention
o Hematuria
o Hemospermia
Histological types of prostate ca;
Adenocacenoma 85%
o Ordinary
o Mucinous
o Ductal aggressive
o Neuroendocrine
o Small cell
Transitional cell ca
Pure primary squamous cell
Sarcoma
Lymphoma
Gleasons grading ; sum of two most prominent grade
2-4 low grade
5-7 intermidiate
8-10 high grade

[email protected] Page 129
DIALYSIS; method of removing toxic substance(impurities and waste) from the blood when the kidneys
are unable to do so.
Methods;
Haemodialysis
Peritoneal
Functions;
Cleans the blood of accumulated waste product
Removes the by-products of protein metabolism(urea, Cr and uric acid)
Removes excessive fluids
Maintains or restores the buffer system of the body
Maintains or restores electrolytes levels
Indications
Clinical
o Uremic encephalopathy
o Uremic pericarditis
o Uremic nephropathy
o Pulmonary edema
o Refractory oedema
o Refractory hypertension
o Bleeding diathesis
Laboratory
o Urea ≥30mmol/L or daily raise of 5mmol/L
o Potassium ≥6.5mmol/L or daily raise of 1mmol/L
o Bicarbonate ≤10mmol/L
o Cr >600mmol/L or daily raise of 100mmol/L

[email protected] Page 130


















