Supportive Therapyfor a Patient With Toxic Epidermal...
14
L yell disease, commonly referred to as toxic epidermal necrolysis (TEN), is a rare, life- threatening condition probably related to drug hypersensitivity; the mortality rate is approximately 30%. 1 The disease is characterized by an initial pruritic, erythematous rash fol- lowed by the appearance of bullae, which subsequently lead to ulceration and sloughing of the underly- ing epidermal base similar to physiological damages caused by burns. Moreover, TEN causes crusting, desquamation, and ulceration of the mucous membranes in areas such as the oral, ocular, and genital mucosa. 2 Bleeding from internal mucous membranes, especially those in the gastrointestinal and respi- ratory tracts, can progress to hypovolemia and lead to death. TEN is often accompanied by ocular mani- festations ranging from acute conjunctivitis to corneal abrasion and, in the most severe cases, corneal ulceration. 3 These changes can lead to permanent loss of vision. Supportive Therapy for a Patient With Toxic Epidermal Necrolysis Undergoing Plasmapheresis BOZENA SECZYNSKA, RN, MSCN ILONA NOWAK, RN, MSCN AURELIA SEGA, RN, MSCN MARIA KOZKA, RN, MSCN, PhD MICHAEL WODKOWSKI, MD WIESLAW KRÓLIKOWSKI, MD, PhD WOJCIECH SZCZEKLIK, MD, PhD ©2013 American Association of Critical-Care Nurses doi: http://dx.doi.org/10.4037/ccn2013555 Feature A patient with severe toxic epidermal necrolysis underwent 2 cycles of therapeutic plasma exchange and received specialized wound care for widespread skin damage of more than 80% of his body surface area. Extensive involvement of mucous membranes, including the conjunctivas and the oropharyngeal cavity, and damage of his genitourinary organs required meticulous wound care. Daily care of injuries of tissues affected only in the most severe cases of toxic epidermal necrolysis was provided by an experienced intensive care unit nursing team. A meticulous supportive therapy regimen was a major contributing factor to this patient’s remission. (Critical Care Nurse. 2013;33[4]:26-38) 26 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org by AACN on April 19, 2018 http://ccn.aacnjournals.org/ Downloaded from
Transcript of Supportive Therapyfor a Patient With Toxic Epidermal...
Lyell disease, commonly referred to as toxic epidermal necrolysis (TEN), is a rare, life-threatening condition probably related to drug hypersensitivity; the mortality rate isapproximately 30%.1 The disease is characterized by an initial pruritic, erythematous rash fol-
lowed by the appearance of bullae, which subsequently lead to ulceration and sloughing of the underly-ing epidermal base similar to physiological damages caused by burns. Moreover, TEN causes crusting,desquamation, and ulceration of the mucous membranes in areas such as the oral, ocular, and genitalmucosa.2 Bleeding from internal mucous membranes, especially those in the gastrointestinal and respi-ratory tracts, can progress to hypovolemia and lead to death. TEN is often accompanied by ocular mani-festations ranging from acute conjunctivitis to corneal abrasion and, in the most severe cases, cornealulceration.3 These changes can lead to permanent loss of vision.
Supportive Therapy for a Patient With Toxic Epidermal NecrolysisUndergoing PlasmapheresisBOZENA SECZYNSKA, RN, MSCN
ILONA NOWAK, RN, MSCN
AURELIA SEGA, RN, MSCN
MARIA KOZKA, RN, MSCN, PhD
MICHAEL WODKOWSKI, MD
WIESŁAW KRÓLIKOWSKI, MD, PhD
WOJCIECH SZCZEKLIK, MD, PhD
©2013 American Association of Critical-Care Nurses doi: http://dx.doi.org/10.4037/ccn2013555
Feature
A patient with severe toxic epidermal necrolysis underwent 2 cycles of therapeutic plasma exchange and receivedspecialized wound care for widespread skin damage of more than 80% of his body surface area. Extensiveinvolvement of mucous membranes, including the conjunctivas and the oropharyngeal cavity, and damage ofhis genitourinary organs required meticulous wound care. Daily care of injuries of tissues affected only in themost severe cases of toxic epidermal necrolysis was provided by an experienced intensive care unit nursingteam. A meticulous supportive therapy regimen was a major contributing factor to this patient’s remission.(Critical Care Nurse. 2013;33[4]:26-38)
26 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

Pathophysiology and Clinical Manifestations
The pathophysiological changes in TEN are due toan autoimmune reaction against epithelial cells,4 usuallytriggered by the ingestion of a drug. Erythema multiforme,Stevens-Johnson syndrome (SJS), and TEN are consid-ered part of the same pathological spectrum but can bedifferentiated clinically (Table 1). So far the mechanism
behind the massive apoptosis of keratinocytes that under-lies the common basis of these 3 conditions has not beenfully elucidated. Currently Fas-mediated pathways, gran-ulysin, and reactive oxygen species are being investigatedas possible early steps in TEN.7 The clinical picture maybegin with unspecific signs and symptoms such as fever,cough, rhinorrhea, or malaise followed by the appear-ance of unevenly shaped, macular, erythematous lesionson the face and trunk that spread to the extremities andlater coalesce. Massive epidermal detachment ensuesover the next 5 to 7 days, and reepithelialization occursduring the following weeks.2 The genitourinary, gastroin-testinal, and ocular mucosal surfaces may undergo erosionand ulceration. Histological examination of a skin biopsymay greatly accelerate the diagnosis. Overall mortalityrates are about 25% to 35%.1 In a large retrospective study(47 patients, 11 deaths) of TEN by Yamada et al,8 sepsis(64%) was the most common cause of death. Other causesincluded disseminated intravascular coagulation (27%)and liver failure (11%), but the percentages may vary.Nevertheless the majority of deaths are due to sepsisand its complications.
DiagnosisThe diagnosis of TEN is based on clinical findings.
The main characteristics are erythematous macules fol-lowed by epidermal detachment and blistering, a posi-tive Nicolsky sign, and ulceration of mucosal surfaces.2
TEN can be distinguished from erythema multiforme,
All authors are affiliated with Jagiellonian University Medical Col-lege, Krakow, Poland. Bozena Seczynska is an intensive care nursein the Department of Medicine.
Ilona Nowak is an intensive care nurse in the Department of Medicine.
Aurelia Sega is an intensive care nurse in the Department of Medicine.
Maria Kozka is an assistant professor in nursing, Department ofClinical Nursing, Institute of Nursing and Midwifery, Faculty ofHealth Sciences. She is a lecturer at the Institute of Nursing.
Michael Wodkowski is an intern in intensive care in the Depart-ment of Medicine.
Wiesław Królikowski is the director of the intensive care unit in theDepartment of Medicine.
Wojciech Szczeklik is an attending physician in the intensive careunit, Department of Medicine.
Corresponding author: Wojciech Szczeklik, MD, PhD, Department of Intensive Care,Jagiellonian University Medical College, ul. Skawinska 8, 31-066 Krakow, Poland (e-mail:[email protected]).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia,Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax,(949) 362-2049; e-mail, [email protected].
Authors
Factor
Appearance of lesions1
Distribution
Confluence
Epidermal detachment, % of skin area
Causal agents
Erythema multiforme
Targetlike, erythemateous
Extremities
Isolated lesions
0
Stevens-Johnson syndrome
Dusky redFlat atypical
Face Trunk
Isolated lesions
<10
Stevens-Johnson syndrome/toxic
epidermal necrolysis
Dusky red Flat atypical
Face Trunk
Moderate confluence
10-30
Toxic epidermal necrolysis
Poorly delineated,erythematous
Flat atypical
Face Trunk Extremities
Heavy confluence
≥30
Table 1 Differentiating factors and most common causal agents of erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysisa
a Based on information from Harr and French,1 Schneck et al,5 and Huang et al.6
Nevirapine, lamotrigine, and sertraline, sulfamethoxazole/trimethoprim, sulfonamides, allop-urinol, carbamazepine, phenytoin, phenobarbital, and nonsteroidal anti-inflammatory drugsof the oxicam type
www.ccnonline.org CriticalCareNurse Vol 33, No. 4, AUGUST 2013 27
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from
SJS, or SJS-TEN on the basis of the cri-teria presented in Table 1. TEN mustbe differentiated from other autoim-mune blistering diseases such as pem-phigus vulgaris, bullous pemphigoid,acute generalized exanthema-pustulo-sis, and, albeit rare, staphylococcalscalded skin syndrome.1 Histologicalevidence of necrosis of all epidermallayers in a skin biopsy specimen andthe results of direct immunofluores-cent staining will exclude mostautoimmune conditions and confirman accurate diagnosis.
TreatmentOptimal treatment for SJS and TEN
is a topic of much debate. Because no prospective ran-domized control trials of various therapeutic optionshave been completed, no preferred method of treatmenthas been determined. Although all agree that the firststep of any treatment must be identification and discon-tinuation of the responsible agent, this interventionalone will not stop progression of the disease. Intra-venous steroids are the initial treatment of choice ofTEN. The primary alternative in resistant cases is intra-venous human immunoglobulin (IVIg).9 However, the
results of arecent meta-analysis6 sug-gest that IVIgmay not bebeneficial.The majority
of TEN patients in previous studies typically had multi-ple comorbid conditions that seemed to influence theprognosis much more than the type of treatment used.However, patients who received high doses of IVIg (>2g/kg) tended to have lower mortality than did patientswho received low doses, and infants and childrenshowed improved prognosis regardless of the dose used.6
Treatment with plasmapheresis has gained supportover the years. The filtration of plasma removes theoffending autoantibodies from circulating blood.10 Theprocedure is performed every second day for a total of 2to 5 cycles. Plasmapheresis is valued for its rapid results,rare side effects, and efficiency in treating patients with
TEN refractory to steroids or IVIg.8 The results of our ownexperience11 and the findings in other case reports,12 caseseries,13 and retrospective cohort studies8 have consistentlyindicated clinical benefits with plasmapheresis, and addi-tional research on this method has been recommended.1,7
Regardless of the therapeutic option chosen, a com-prehensive team approach that emphasizes supportivecare is essential for any patient with TEN. Detachment ofthe epidermal layer results in marked fluid and electrolytedepletion, and loss of the skin’s natural barrier propertiesincreases the risk for infection and subsequent sepsis.The possibility of infection and sepsis mandates vigilancethroughout the management of patients with TEN. Accord-ing to recommendations,14,15 patients with TEN should betransferred as soon as possible to an intensive care set-ting, typically a burn unit or a specialized intensive careunit (ICU), where they can receive the required expertwound care. In the case we describe here, the patient wassent to our specialized ICU because the unit’s medicalteam had experience treating TEN, and all necessaryresources were available onsite. Close cooperation of theprimary care team with members from dermatology,ophthalmology, otolaryngology, rehabilitation, and psy-chiatry/psychology are essential to achieve a favorablelong-term clinical outcome.
PrognosisThe SCORTEN index16,17 is a grading scheme used to
assess the severity and prognosis of SJS and TEN (Table 2).The index can also be used to evaluate the severity of
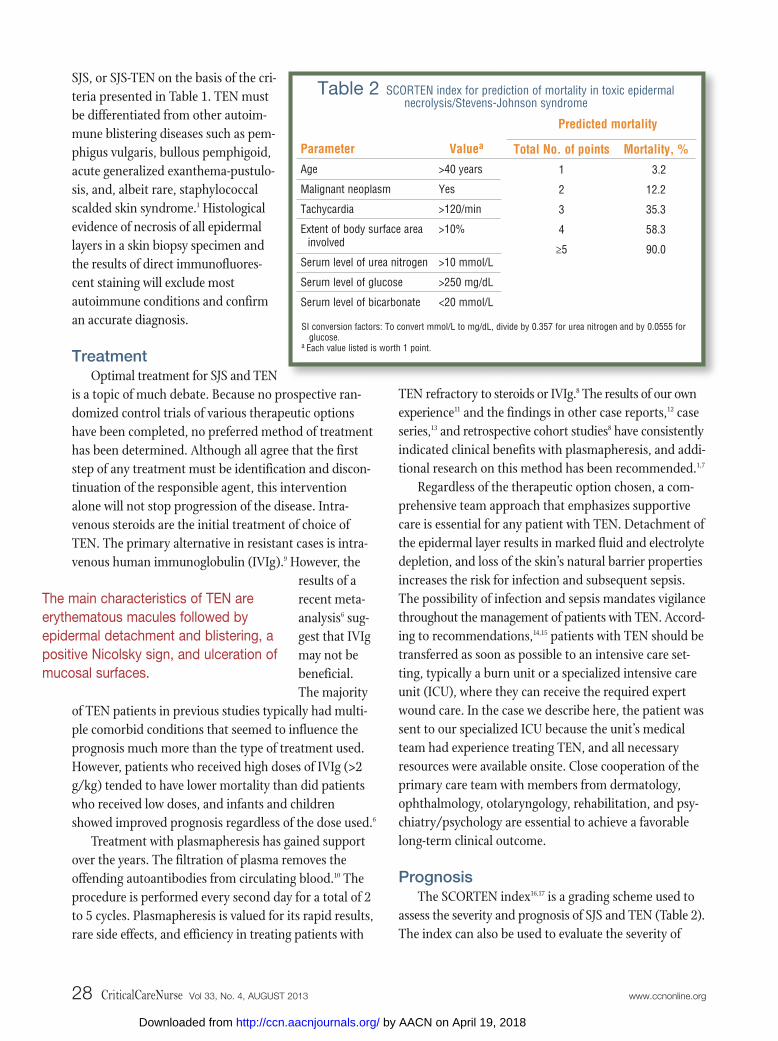
Table 2 SCORTEN index for prediction of mortality in toxic epidermalnecrolysis/Stevens-Johnson syndrome
Parameter
Age
Malignant neoplasm
Tachycardia
Extent of body surface areainvolved
Serum level of urea nitrogen
Serum level of glucose
Serum level of bicarbonate
Total No. of points
1
2
3
4
≥5
Mortality, %
3.2
12.2
35.3
58.3
90.0
Valuea
>40 years
Yes
>120/min
>10%
>10 mmol/L
>250 mg/dL
<20 mmol/L
SI conversion factors: To convert mmol/L to mg/dL, divide by 0.357 for urea nitrogen and by 0.0555 forglucose.
a Each value listed is worth 1 point.
Predicted mortality
28 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
The main characteristics of TEN are erythematous macules followed by epidermal detachment and blistering, apositive Nicolsky sign, and ulceration ofmucosal surfaces.
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

other conditions, such as burns and bullous diseases,that affect the integrity of the skin. The index has 7 cri-teria: age (>40 years), presence of malignant neoplasm,tachycardia (>120/min), percentage of affected skin sur-face (>10% total body surface area), serum concentrationof urea nitrogen (>10 mmol/L; to convert to milligramsper deciliter, divide by 0.357), serum level of glucose(>250 mg/dL; to convert to milligrams per deciliter, divideby 0.0555), and serum level of bicarbonate (<20 mmol/L).The main differentiating factor between SJS and TEN,an increase in the percentage of skin surface affected byepidermal detachment, has also been associated withincreased mortality.18
Case DescriptionThis case description is a detailed account of the sup-
portive therapy delivered during management of TEN in aspecialized ICU. We include nursing care during plasma-pheresis because the information available on this treat-ment is insufficient.
A 41-year-old man with a history of hypertension wastransferred to the ICU because he had had a rash for 72hours. A recent upper respiratory infection treated withciprofloxacin was followed by an acute onset of diffusemaculopapular rash with fluid-filled bullae over thepatient’s entire body surface. He previously had come tothe emergency department when he experienced rapidlyprogressing changes involving the conjunctivas (hemor-rhages, purulent exudates from the conjunctival sac) andoral cavity (ulcerations in mouth, throat, and larynx)within 24 hours after he had ingested 2 doses ofciprofloxacin. Results of dermatology, ophthalmology,and head and neck consultations at this time suggesteda diagnosis of TEN.
Upon admission to the ICU, the patient was conscious,verbally responsive, and anxious. Physical examinationrevealed tachycardia (heart rate 120/min), tachypnea(respirations 20/min), and a low-grade fever (body tem-perature 37.8ºC). About 80% of his skin surface was cov-ered by a maculopapular, erythematous rash with necrosis,sloughing of the epidermal skin layers, and numerousbullae with underlying ulcerations involving the oral andnasopharyngeal surfaces. The patient said he had throatpain, dysphagia, and dysarthria. He also had periorbitaledema, subconjunctival hemorrhages, and purulent exu-dates from the conjunctival sac. Although cultures ofconjunctival exudates were negative for bacterial growth,
the patient was given genta micin eye drops as recom-mended by an ophthalmologist. Ulcerative changes alsoinvolved the sclera. Additionally, painful erythematouschanges covered the genitalia.
Parenteral nutrition was begun within 24 hours ofadmission. A nasogastric tube was inserted on day 3,and enteral nutrition was provided from days 3 to 18 inaddition to parenteral nutrition. On day 18, liquid oralfeedings were begun; parenteral nutrition was used tosupplement daily requirements and was slowly taperedoff as oral intake increased. Blood glucose levels rangedfrom 8 to 10 mmol/L; insulin was administered as aninfusion. Metoclopramide was used throughout thepatient’s ICU stay to maintain motility while limitingsecretions that could lead to further damage of the mucosa.Pain was treated with an intravenous fentanyl infusion50 to 100 μg/h plus 100 μg as needed before changingof wound dressings.
An initial continuous infusion of 500 mg of intra-venous corticosteroid (methylprednisolone) in salinewas begun in the infectious diseases unit before thepatient was admitted to the ICU. The lack of improve-ment after 48 hours of treatment with corticosteroid,rapid progression of the disease, and the need for a fast-acting treat-ment promptedthe decision toimmediatelybegin therapeu-tic plasma exchange (TPE), which has been used to treatpatients with steroid-refractory TEN who required rapidimprovement.8,11 An initial 5-cycle course of TPE wasperformed (days 1, 2, 4, 5, and 6), and 30 g of IVIg wasgiven after the last cycle. Empirical broad-spectrumantibiotic therapy (ceftriaxone) was started before thepatient was admitted to the ICU, and regular electrolyteand fluid replacements were maintained throughout theICU stay. Treatment with antibiotics (meropenem, van-comycin, colistin) was started after cultures of woundspecimens were positive for Streptococcus hemolyticus andblood cultures were positive for gram-positive staphylo-cocci and to prevent infection by organisms present inthe ICU.
On day 8, the ICU team diagnosed septic shock. Thepatient had high body temperature (39°C), unstable hemo-dynamic condition (mean arterial pressure decreased from93 mm Hg to 55 mm Hg in 2 hours), and a requirement
www.ccnonline.org CriticalCareNurse Vol 33, No. 4, AUGUST 2013 29
The 2 initial treatments of choice in TENare intravenous steroids and intravenoushuman immunoglobulin.
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

for continuous vasopressor therapy (intravenousdopamine and norepinephrine). The patient also requiredsupportive oxygen therapy (fraction of inspired oxygen0.3-0.6). Packed red blood cells, fresh frozen plasma,and 20% albumin solution were administered to counter -balance the hypovolemia, anemia, and hypoalbumine-mia due to persistent blood and protein loss during skinsloughing. The purpose of these interventions was torestore intravascular oncotic pressure. The septic shockresolved gradually during the ensuing 5 days. Once thepatient’s condition was stabilized, reepithelializationbegan on day 14; the skin color in affected areas beganto become pale, and production of exudate decreased.
On day 18, a second period of profuse bleeding(mainly back and buttocks) and exacerbation of fluidlosses caused by burrowing of the ulcerations deeperinto the dermis began. The patient had a second courseof TPE (days 20, 22, 23, and 24). His clinical picture
improved after each subsequent cycle of plasmapheresis.During a period of 4 days, bleeding from the back sub-sided, the extremities regained turgor, reepithelializationbegan anew, and ulcerative changes in the oral cavityresolved, in that order. The patient was advanced to a liq-uid diet, and physical rehabilitation was begun during thefourth week of hospitalization after the skin changes hadresolved and only mild discoloration remained (Figure 1).Ophthalmological examination before discharge revealeda healed cornea and retina and normal appearance of theoptic nerve. The patient was directed to the allergy andimmunology clinic for outpatient follow-up care.
Supportive TherapyFor wound care, dressings impregnated with 0.5%
silver nitrate were applied to the entire body except thecatheter insertion sites. These sites were a challengebecause tape could not be used on them. Therefore they
Figure 1 Skin changes in a patient with toxic epidermal necrolysis before and after plasmapheresis. Changes pictured are beforetreatment (far left), during first cycle (left center), second cycle (right center), and at discharge (far right, top) or 1-year follow-up (far right, bottom).
30 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from
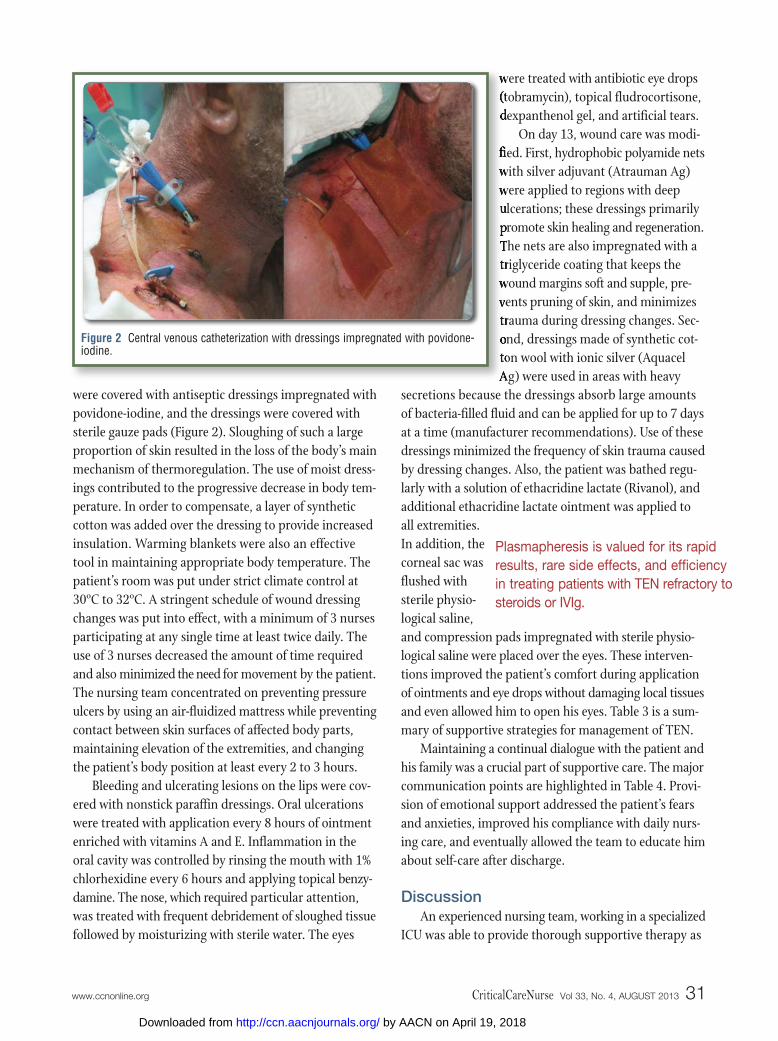
were covered with antiseptic dressings impregnated withpovidone-iodine, and the dressings were covered withsterile gauze pads (Figure 2). Sloughing of such a largeproportion of skin resulted in the loss of the body’s mainmechanism of thermoregulation. The use of moist dress-ings contributed to the progressive decrease in body tem-perature. In order to compensate, a layer of syntheticcotton was added over the dressing to provide increasedinsulation. Warming blankets were also an effectivetool in maintaining appropriate body temperature. Thepatient’s room was put under strict climate control at30ºC to 32ºC. A stringent schedule of wound dressingchanges was put into effect, with a minimum of 3 nursesparticipating at any single time at least twice daily. Theuse of 3 nurses decreased the amount of time requiredand also minimized the need for movement by the patient.The nursing team concentrated on preventing pressureulcers by using an air-fluidized mattress while preventingcontact between skin surfaces of affected body parts,maintaining elevation of the extremities, and changingthe patient’s body position at least every 2 to 3 hours.
Bleeding and ulcerating lesions on the lips were cov-ered with nonstick paraffin dressings. Oral ulcerationswere treated with application every 8 hours of ointmentenriched with vitamins A and E. Inflammation in theoral cavity was controlled by rinsing the mouth with 1%chlorhexidine every 6 hours and applying topical benzy-damine. The nose, which required particular attention,was treated with frequent debridement of sloughed tissuefollowed by moisturizing with sterile water. The eyes
were treated with antibiotic eye drops(tobramycin), topical fludrocortisone,dexpanthenol gel, and artificial tears.
On day 13, wound care was modi-fied. First, hydrophobic polyamide netswith silver adjuvant (Atrauman Ag)were applied to regions with deepulcerations; these dressings primarilypromote skin healing and regeneration.The nets are also impregnated with atriglyceride coating that keeps thewound margins soft and supple, pre-vents pruning of skin, and minimizestrauma during dressing changes. Sec-ond, dressings made of synthetic cot-ton wool with ionic silver (AquacelAg) were used in areas with heavy
secretions because the dressings absorb large amountsof bacteria-filled fluid and can be applied for up to 7 daysat a time (manufacturer recommendations). Use of thesedressings minimized the frequency of skin trauma causedby dressing changes. Also, the patient was bathed regu-larly with a solution of ethacridine lactate (Rivanol), andadditional ethacridine lactate ointment was applied toall extremities.In addition, thecorneal sac wasflushed withsterile physio-logical saline,and compression pads impregnated with sterile physio-logical saline were placed over the eyes. These interven-tions improved the patient’s comfort during applicationof ointments and eye drops without damaging local tissuesand even allowed him to open his eyes. Table 3 is a sum-mary of supportive strategies for management of TEN.
Maintaining a continual dialogue with the patient andhis family was a crucial part of supportive care. The majorcommunication points are highlighted in Table 4. Provi-sion of emotional support addressed the patient’s fearsand anxieties, improved his compliance with daily nurs-ing care, and eventually allowed the team to educate himabout self-care after discharge.
DiscussionAn experienced nursing team, working in a specialized
ICU was able to provide thorough supportive therapy as
Figure 2 Central venous catheterization with dressings impregnated with povidone-iodine.
www.ccnonline.org CriticalCareNurse Vol 33, No. 4, AUGUST 2013 31
Plasmapheresis is valued for its rapidresults, rare side effects, and efficiencyin treating patients with TEN refractory tosteroids or IVIg.
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

Nursing intervention
Regularly monitor and report skin changes Remove sloughed epidermal layer onlyApply nonadherent dressings impregnated with
0.5% silver nitrate, synthetic cotton wool dress-ings with ionic silver or nanocrystallic silver19
Stabilize dressings with cotton netting Use biosynthetic dressings (Biobrane)20
Bathe patient with ethacridine lactate (Rivanol)
Have patient gargle with 1% chlorhexidineUse paraffin dressings for vermilion zone of lipMonitor teeth for indications of infection
Flush conjunctivae with sterile physiological salineApply corticosteroid eyedropsApply antibiotic ointmentUse hydrating gelApply sterile gauze dressings soaked in distilled
water to eyelids
Monitor for indications of gastrointestinal hemorrhaging and malabsorption
Administer proton pump inhibitor prophylaxis asordered
Monitor for indications of respiratory distressUse humidified air during oxygen therapyTreat with nebulized physiological saline Institute pulmonary rehabilitation
Isolate patientFollow full-contact precautions for personnel and
visitorsBegin use of strict aseptic techniquesMonitor laboratory markers of inflammationReview results of blood and tissue culturesUse peripheral intravenous catheter (preferred)Monitor and control glycemic status
Assess patient’s pain according to verbal ornumerical rating scale
Assess pain relief according to verbal or numericalrating scale after delivery of analgesic medication
Monitor consciousness level and breathing patternInform patient in advance of all bedside nursing
activities
Replace fluids according to the amount of totalbody surface affected
Continually monitor hemodynamic parameters(heart rate, invasive blood pressure, centralvenous pressure)
Regularly measure electrolyte levels and replenishas ordered
Strictly monitor fluid intake and output
Table 3 Supportive therapy for common clinical problemsin management of toxic epidermal necrolysis
Rationale for intervention
Progression of skin change is a key indicator of the diseasecourse. Monitoring of skin is also useful for detecting earlyindications of infection. Extended release of silver ions into theaffected area enhances antiseptic activity and prevents infec-tion. Stabilization of dressings allows added comfort andincreased mobility without the danger of dressing loss
Ethacridine lactate baths reduce the risk for skin infection andsubsequent sepsis
Chlorhexidine acts as antibacterial, bacteriostatic, analgesic, andanti-inflammatory agent
This agent prevents dryness, lip cracking, and formation ofhemorrhaging scabs, improving the patient’s ability to freelyopen the mouth21
Hydration of the eyelids improves the patient’s ability to main-tain oculomotor and eyelid movements, facilitating applicationof ointments and eyedrops to conjunctivae
Early detection of increased gastrointestinal bleeding is essentialfor directing further therapy
Pharmacological prevention of stress ulcers is necessary in allpatients
Prevention of upper respiratory tract infections reduces respiratory effort
Humidification of airways prevents formation of hemorrhagingscabs
Patient is at increased risk for infection risk because of thebreakdown of the skin’s natural barrier function
Use of aseptic technique eliminates other potential sources ofinfection, including venous insertion sites, nasogastric tubes,urinary catheters
Hyperglycemia in a nondiabetic patient, also known as hyper-glycemic stress, has been linked with a higher likelihood ofinfections22
Relief of pain helps prevent stress-induced sympatheticresponses that may induce tachycardia, increased blood pres-sure, increased myocardial oxygen demand, hypercoagulabil-ity, insulin resistance, and protein metabolism
Use of opioids for analgesic purposes may result in difficultiesin respiration and disturbances in consciousness
Informing the patient helps alleviate unexpected pain caused bymovements during bedside interventions
Continuous water and serum loss occurs due to damage ofphysical skin barrier requires constant assessment
Skin changes may impede using a shoulder cuff to measureblood pressure
Continued
Problem
Epidermaldetachment
Oral cavityulceration
Conjunctivalulceration
Gastrointestinalulceration
Respiratory tractulceration
Infections andsepsis
Pain
Fluid and electrolyte loss
32 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from
comprehensive meta-analysis6 suggest that survival ratesin patients with TEN treated solely with supportive ther-apy may be similar to those of patients treated with IVIg.An odds ratio of 1.00 (95% CI, 0.57-1.75) in a comparison
part of the successful treatment of this TEN patient. Com-pared with other methods of treatment, meticulous sup-portive therapy is the sole intervention that consistentlyimproves prognosis.7 Interestingly, results from the most
Nursing intervention
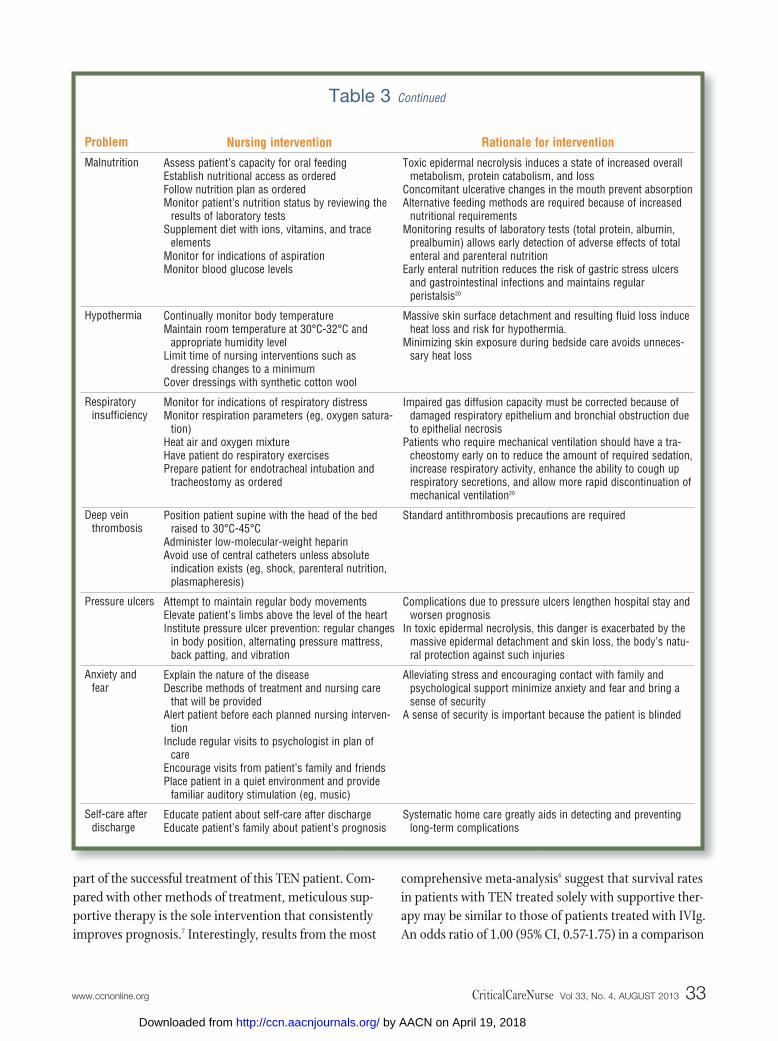
Assess patient’s capacity for oral feedingEstablish nutritional access as orderedFollow nutrition plan as ordered Monitor patient’s nutrition status by reviewing the
results of laboratory testsSupplement diet with ions, vitamins, and trace
elementsMonitor for indications of aspirationMonitor blood glucose levels
Continually monitor body temperatureMaintain room temperature at 30°C-32°C and
appropriate humidity levelLimit time of nursing interventions such as
dressing changes to a minimumCover dressings with synthetic cotton wool
Monitor for indications of respiratory distressMonitor respiration parameters (eg, oxygen satura-
tion)Heat air and oxygen mixtureHave patient do respiratory exercisesPrepare patient for endotracheal intubation and
tracheostomy as ordered
Position patient supine with the head of the bedraised to 30°C-45°C
Administer low-molecular-weight heparinAvoid use of central catheters unless absolute
indication exists (eg, shock, parenteral nutrition,plasmapheresis)
Attempt to maintain regular body movementsElevate patient’s limbs above the level of the heartInstitute pressure ulcer prevention: regular changes
in body position, alternating pressure mattress,back patting, and vibration
Explain the nature of the diseaseDescribe methods of treatment and nursing care
that will be providedAlert patient before each planned nursing interven-
tionInclude regular visits to psychologist in plan of
careEncourage visits from patient’s family and friendsPlace patient in a quiet environment and provide
familiar auditory stimulation (eg, music)
Educate patient about self-care after dischargeEducate patient’s family about patient’s prognosis
Table 3 Continued
Rationale for intervention
Toxic epidermal necrolysis induces a state of increased overallmetabolism, protein catabolism, and loss
Concomitant ulcerative changes in the mouth prevent absorptionAlternative feeding methods are required because of increased
nutritional requirementsMonitoring results of laboratory tests (total protein, albumin,
prealbumin) allows early detection of adverse effects of totalenteral and parenteral nutrition
Early enteral nutrition reduces the risk of gastric stress ulcersand gastrointestinal infections and maintains regular peristalsis20
Massive skin surface detachment and resulting fluid loss induceheat loss and risk for hypothermia.
Minimizing skin exposure during bedside care avoids unneces-sary heat loss
Impaired gas diffusion capacity must be corrected because ofdamaged respiratory epithelium and bronchial obstruction dueto epithelial necrosis
Patients who require mechanical ventilation should have a tra-cheostomy early on to reduce the amount of required sedation,increase respiratory activity, enhance the ability to cough uprespiratory secretions, and allow more rapid discontinuation ofmechanical ventilation20
Standard antithrombosis precautions are required
Complications due to pressure ulcers lengthen hospital stay andworsen prognosis
In toxic epidermal necrolysis, this danger is exacerbated by themassive epidermal detachment and skin loss, the body’s natu-ral protection against such injuries
Alleviating stress and encouraging contact with family and psychological support minimize anxiety and fear and bring asense of security
A sense of security is important because the patient is blinded
Systematic home care greatly aids in detecting and preventinglong-term complications
Problem
Malnutrition
Hypothermia
Respiratoryinsufficiency
Deep veinthrombosis
Pressure ulcers
Anxiety andfear
Self-care afterdischarge
www.ccnonline.org CriticalCareNurse Vol 33, No. 4, AUGUST 2013 33
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

of experimental treatment (IVIg) and control treatment(supportive therapy) is not conclusive but does raisequestions about the true clinical efficacy of IVIg therapy.Future trials comparing IVIg, plasmapheresis, and sup-portive therapy as first-line treatments seem justifiedand may shed some light on this observation.
The decision to use TPE in this patient was timely; theexchange halted the progression of his condition. Thepatient had a good response to treatment, with signs ofimprovement after the third cycle of the first series ofplasmapheresis and IVIg. However, the skin changesrecurred several days after the first combined plasma-pheresis cycle had been completed. A second TPE serieswas performed (without IVIg), and this time resulted inpermanent clinical improvement. These results are similarto outcomes in previous reports of therapeutic success insevere, refractory cases of TEN treated with plasmaphere-sis.10-13 The reason for the outcome is unclear. Researchersspeculate that plasmapheresis removes necrosis-inducingfactors from the bloodstream, but these factors have yet tobe identified. Only a few investigators have examined thistopic in detail. A large-scale (47 patients) study of plasma-pheresis treatment and TEN by Yamada et al8 revealed thateven a low number of cycles (mean, 3.1) had good efficacy(80.9%), and mortality (23.4%) was lower than predictedin patients with the most severe and resistant form of SJSor TEN. A major difficulty limiting further study of this
treatment method is the low incidence of TEN, a situa-tion that results in few patients who could potentially beincluded in prospective studies.
Useful articles23-25 on wound care management inTEN patients have been published. But no clear guide-lines or even case reports with practical recommendationsfor delivery of nursing care to patients undergoingplasmapheresis are available. Several important aspectsmust be addressed to provide appropriate supportivetherapy to patients being treated with TPE instead ofsteroid or IVIg therapy.26 First, surveillance of hemody-namic parameters is crucial. Either continuous monitor-ing or checking manually every 15 minutes or so is neededto detect periods of hypotension due to third spacing,which may develop suddenly during TPE procedures.Second, watching for and asking about neurologicalsymptoms such as numbness, tingling, and level of con-sciousness are important. Such symptoms often indicatethe beginning of electrolyte disturbances such as hypocal-cemia, hypokalemia, and hypomagnesemia. Third, scru-tinizing the patient for possible allergic reactions toblood products, cannulas, or extracorporeal equipmentis also important. Fourth, bleeding complications arecommon because of the use of a large-bore catheter, thelarge amounts of heparin used, depletion of coagulationfactors, and mechanical hemolysis.22 Such complicationsmust be detected early, and treatment must be altered
Timing
Meeting with patient
Meeting with family
Education for home self-care
Topics
Discussion of overnight progress and daily plan of careWarning the patient before any nursing duties are begun to reduce anxiety and increase subjective
pain thresholdFuture quality-of-life issues related to vision loss: need for vision correction, use of artificial tears,
changes to current lifestyle, living arrangements, need for home careAccess to community resources for assistance with rehabilitationAccess to social care programs that assist in employment opportunities for people with disabilities
Emotional support such as explaining nature of the disease, discussing the prognosis, and assuringthem that the patient is receiving the best of care
Discussion of long-term complications related to vision loss such as difficulty reading or driving atnight, feeling of dryness in eye
Offer of professional psychological support for concerns such as dealing with grief, anger, misunder-standing of disease impact
Regular follow-up visits with ophthalmologist, dermatologist, internistInstructions for use of artificial tears in case of dry-eye symptomsAvoidance of sunbathing because of harmful effects of ultraviolet raysAvoidance of using a sauna because of the vasodilatory effect of extreme heat on already fragile
capillariesAvoidance of sulfonamide-type drugs because of the danger of future cutaneous drug reactions
Table 4 Topics addressed during communication with the patient and his family for current and future provision of care of toxic epidermal necrolysis
34 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

to compensate. Table 5 is a summary of key aspects ofsupportive care during TPE. Finally, scrupulous recordkeeping of all signs and symptoms, laboratory results,
medications, and hemodynamic parameters is of para-mount importance, especially when electronic healthrecords are not available.
Complications
Hypovolemia
Hypervolemia
Pulmonary edema
Infections
Hypothermia
Nonhemolytic reaction afterplasma exchange
Anaphylactoid reaction oranaphylactic shock
Sepsis
Citrate poisoning after rapidreplacement with freshfrozen plasma
Transfusion-related acutelung injury
Acute hypervolemia andpulmonary edema
Purpura or ecchymoses
Transient hypercoagulablestate during procedure dueto loss of antithrombin
Potential signs and symptoms
HypotensionTachycardiaOliguriaDecreased peripheral perfusionSigns of electrolyte disturbances
HypertonicityTachycardiaHypoxemia
Acute dyspneaPeripheral edema
FeverChills
Chills
ChillsFeversHypotension
UrticariaPruritusBronchospasmRespiratory insufficiencySkin changes
FeverHypotensionTachycardiaTachypnea
Metabolic alkalosisHypokalemia
TachycardiaHypoxemiaHypotonia
DyspneaHypertonicityTachycardia
Bleeding at venous accesssites
Bleeding of mucous membranes
HemoptysisThrombosis or obstruction of
venous cannulas
Table 5 Possible complications of plasmapheresis and appropriate interventions
Interventions or prophylaxis
Monitoring of vital signs, central venous pressure,electrolyte levels
Judicious selection of fluidsReplenishment of electrolyte deficits before, during,
and after plasma exchange
Continuous monitoring and balancing of filtrate andcompensation
Monitoring of respiratory effort, oxygen saturationshown by pulse oximetry, arterial blood gases
Antibacterial precautions
Continuous monitoring of body temperatureWarming of fluidsWarming blankets
Monitoring of hemodynamic parameters
Monitoring of reaction’s progressionSupplementation with 5% albumin (preferred)Antihistamine prophylaxis before administration of
fresh frozen plasma
Use of antiseptic techniqueMonitoring of hemodynamic parameters
Regular monitoring of level of ionized calcium,blood pH, base excess, bicarbonate level
Calcium replenishment during administration offresh frozen plasma
Supplementation with 5% albuminMonitoring of vital signs, oxygen saturation, arterial
blood gasesStrict monitoring of fluid intake and outputMonitor continuously for clinical symptoms
Monitoring of respiratory effort, rate, oxygen satura-tion, arterial blood gases, central venous pressure
Individual heparin dosingMonitoring of international normalized ratio, activated
clotting time, prothrombin time, fibrinogen level,platelets, hemoglobin level, and hematocrit before,during, and after procedure
Administration of additional fresh frozen plasmaafter procedure
Continued
Causal agent
Fluid products
Blood-basedproducts
Anticoagulationtherapy anddepletion ofcoagulationfactors
www.ccnonline.org CriticalCareNurse Vol 33, No. 4, AUGUST 2013 35
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

ConclusionTEN is a severe and rare condition that occurs via a
mostly unknown pathophysiological mechanism. The highmortality rate makes management a serious challengefor both physicians and nurses. The conflicting evidenceon whether steroids or IVIg is the superior treatment accen-tuates that meticulous supportive therapy and expertwound care are still the major factors contributing toincreased survival. Supportive therapy and expert woundcare are especially needed when alternative treatments,such as plasmapheresis, are used. Reporting of effective
supportive therapy strategies is essential to ensure thatfuture cases will be successfully managed. CCN
AcknowledgmentsThe authors thank the entire ICU staff in the Department of Medicine, Jagiellon-ian University Medical College, for their help during the preparation of this article.
Financial DisclosuresNone reported.
Complications
Hematoma at site of puncture
Pneumothorax
Infection
Deep vein thrombosis
Hemolysis
Clotting of the extra-corporeal circulation
Microfilter capillary leakage
Decrease in immunoglobulinlevels
Nonspecific inflammatoryresponse to the extracor-poreal circulation filterand/or drains
Potential signs and symptoms
EdemaBruisingPain
DyspneaHypoxemia
Fever
Peripheral edemaSwellingErythemaObstruction of catheter causing
decreased blood flow
Chest painDyspneaFever and chills
TachypneaShockChange in color of plasma
filtrateIncreased transmembrane
pressure
Pressure decrease acrossinflow or outflow tubing
Increased susceptibility toinfections
Shortness of breathAbdominal painCoughPruritus
Table 5 Continued
Interventions or prophylaxis
Precision when establishing venous accessLocal anesthesia
Monitoring of breathing, oxygen saturation shownby pulse oximetry
Confirming placement via chest radiograph afteraccess established
Monitoring of changes at puncture siteUse of antiseptic technique
Use of heparin seal to secure catheter placement
Optimal blood flow through capillary microfilter(50-150 mL/min)
Custom-based plasma exchange parameters: transmembrane pressure <70 mm Hg
Monitoring of transmembrane pressure levels forinflow and outflow tubing and setup of appropriatewarning threshold
Monitoring of plasma loss and visual inspection ofplasma appearance
Maintenance of appropriate ultrafiltrate volume toblood volume proportion (should not exceed 20%)
Immunoglobulin titersMonitoring for indications of inflammatory responses
Thorough flushing of plasma microfilters and drainswith sterile saline before procedure
Causal agent
Cannulation
Technique
Now that you’ve read the article, create or contribute to an online discussionabout this topic using eLetters. Just visit www.ccnonline.org and select the articleyou want to comment on. In the full-text or PDF view of the article, click“Responses” in the middle column and then “Submit a response.”
36 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from
23. Evans J. Topical treatment protocol for Stevens-Johnson syndrome andtoxic epidermal necrolysis: a brief report. Wound Ostomy ContinenceNurs. 2009;36(5):509-511.
24. Fromowitz JS, Ramos-Caro FA, Flowers FP. Practical guidelines for themanagement of toxic epidermal necrolysis and Stevens-Johnson syn-drome. Int J Dermatol. 2007;46(10):1092-1094.
25. Worswick S, Cotliar J. Stevens-Johnson syndrome and toxic epidermalnecrolysis: a review of treatment options. Dermatol Ther. 2011;24(2):207-218.
26. Seczynska B, Sega A, Nowak I, Fajfer I, Królikowski W, Szczeklik W.Plasmapheresis—possible complications and their prevention. Przegl Lek.2011;68(9):637-640.
References1. Harr T, French LE. Toxic epidermal necrolysis and Stevens-Johnson
syndrome. Orphanet J Rare Dis. 2010;5:39.2. Rajaratnam R, Mann C, Balasubramaniam P, et al. Toxic epidermal
necrolysis: retrospective analysis of 21 consecutive cases managed at atertiary centre. Clin Exp Dermatol. 2010;35(8):853-862.
3. Chang YS, Huang FC, Tseng SH, Hsu CK, Ho CL, Sheu HM. Erythemamultiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis:acute ocular manifestations, causes, and management. Cornea. 2007;26(2):123-129.
4. Tohyama M, Hashimoto K. Immunological mechanisms of epidermaldamage in toxic epidermal necrolysis. Curr Opin Allergy Clin Immunol.2012;12(4):376-382.
5. Schneck J, Fagot JP, Sekula P, Sassolas B, Roujeau JC, Mockenhaupt M.Effects of treatments on the mortality of Stevens-Johnson syndrome andtoxic epidermal necrolysis: a retrospective study on patients included inthe prospective EuroSCAR Study. J Am Acad Dermatol. 2008;58(1):33-40.
6. Huang YC, Li YC, Chen TJ. The efficacy of intravenous immunoglobulinfor the treatment of toxic epidermal necrolysis: a systematic review andmeta-analysis. Br J Dermatol. 2012;167(2):424-432.
7. Downey A, Jackson C, Harun N, Cooper A. Toxic epidermal necrolysis:review of pathogenesis and management. J Am Acad Dermatol. 2012;66(6):995-1003.
8. Yamada H, Takamori K. Status of plasmapheresis for the treatment oftoxic epidermal necrolysis in Japan. Ther Apher Dial. 2008;12(5):355-359.
9. Mittmann N, Chan B, Knowles S, Cosentino L, Shear N. Intravenousimmunoglobulin use in patients with toxic epidermal necrolysis andStevens-Johnson syndrome. Am J Clin Dermatol. 2006;7(6):359-368.
10. Bamichas G, Natse T, Christidou F, et al. Plasma exchange in patientswith toxic epidermal necrolysis. Ther Apher. 2002;6(3):225-228.
11. Szczeklik W, Nowak I, Seczynska B, Sega A, Krolikowski W, Musial J.Beneficial therapeutic effect of plasmapheresis after unsuccessful treat-ment with corticosteroids in two patients with severe toxic epidermalnecrolysis. Ther Apher Dial. 2010;14(3):354-357.
12. Koštál M, Bláha M, Lánská M, et al. Beneficial effect of plasma exchangein the treatment of toxic epidermal necrolysis: a series of four cases. J ClinApher. 2012;27(4):215-222.
13. Narita YM, Hirahara K, Mizukawa Y, Kano Y, Shiohara T. Efficacy ofplasmapheresis for the treatment of severe toxic epidermal necrolysis:is cytokine expression analysis useful in predicting its therapeutic effi-cacy? J Dermatol. 2011;38(3):236-245.
14. Firoz BF, Henning JS, Zarzabal LA, Pollock BH. Toxic epidermal necrol-ysis: five years of treatment experience from a burn unit. J Am AcadDermatol. 2012;67(4):630-635.
15. George SM, Harrison DA, Welch CA, Nolan KM, Friedmann PS. Der-matological conditions in intensive care: a secondary analysis of theIntensive Care National Audit and Research Centre (ICNARC) Case MixProgramme database. Crit Care. 2008;12(suppl 1). doi:10.1186/cc6141.
16. Guégan S, Bastuji-Garin S, Poszepczynska-Guigné E, Roujeau JC, RevuzJ. Performance of the SCORTEN during the first five days of hospitaliza-tion to predict the prognosis of epidermal necrolysis. J Invest Dermatol.2006;126(2):272-276.
17. Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolken-stein P. SCORTEN: a severity-of-illness score for toxic epidermal necrol-ysis. J Invest Dermatol. 2000;115(2):149-153.
18. Ducic I, Shalom A, Rising W, Nagamoto K, Munster AM. Outcome ofpatients with toxic epidermal necrolysis syndrome revisited. PlastReconstr Surg. 2002;110(3):768-773.
19. Chave TA, Mortimer NJ, Sladden MJ, Hall AP, Hutchinson PE. Toxicepidermal necrolysis: current evidence, practical management andfuture directions. Br J Dermatol. 2005;153(2):241-253.
20. Boorboor P, Vogt PM, Bechara FG, et al. Toxic epidermal necrolysis:use of Biobrane or skin coverage reduces pain, improves mobilisationand decreases infection in elderly patients. Burns. 2008;34(4):487-492.
21. Struck MF, Hilbert P, Mockenhaupt M, Reichelt B, Steen M. Severecutaneous adverse reactions: emergency approach to non-burn epider-molytic syndromes. Intensive Care Med. 2010;36(1):22-32.
22. Parsons P, Watkinson P. Blood glucose control in critical carepatients—a review of the literature. Nurs Crit Care. 2007;12(4):202-210.
To learn more about caring for patients with epidermal necrolysis,read “Drug Reaction, Skin Care, Skin Loss” by Karen Cooper in CriticalCare Nurse, August 2012;32:52-59. Available at www.ccnonline.org.
www.ccnonline.org CriticalCareNurse Vol 33, No. 4, AUGUST 2013 37
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from
CCN Fast FactsSupportive Therapy for a Patient With Toxic Epidermal Necrolysis Undergoing Plasmapheresis
CriticalCareNurseThe journal for high acuity, progressive, and critical care nursing
Several important aspects must be addressed to provideappropriate supportive therapy to patients being treatedwith therapeutic plasma exchange (TPE) instead of steroidor IVIg therapy.
• First, surveillance of hemodynamic parameters is cru-cial. Either continuous monitoring or checking manu-ally every 15 minutes or so is needed to detect periodsof hypotension due to third spacing, which may developsuddenly during TPE procedures.
• Second, watching for neurological symptoms such asnumbness, tingling, and level of consciousness areimportant. Such symptoms often indicate the begin-ning of electrolyte disturbances such as hypocalcemia,hypokalemia, and hypomagnesemia.
• Third, scrutinizing the patient for possible allergicreactions to blood products, cannulas, or extracorpo-real equipment is also important.
• Fourth, bleeding complications are common becauseof the use of a large-bore catheter, the large amountsof heparin used, depletion of coagulation factors, andmechanical hemolysis.
• Finally, scrupulous record keeping of all signs andsymptoms, laboratory results, medications, andhemodynamic parameters is of paramount impor-tance, especially when electronic health records arenot available.
ConclusionsTEN is a severe and rare condition that occurs via a
mostly unknown pathophysiological mechanism. The con-flicting evidence on whether steroids or IVIg is the superiortreatment accentuates that meticulous supportive therapyand expert wound care are still the major factors contribut-ing to increased survival. Supportive therapy and expertwound care are especially needed when alternative treat-ments, such as plasmapheresis, are used. Reporting of effec-tive supportive therapy strategies is essential to ensure thatfuture cases will be successfully managed. CCN
FactsToxic epidermal necrolysis (TEN) is a rare, life-
threatening condition probably related to drug hyper-sensitivity. The disease is characterized by an initialpruritic, erythematous rash followed by the appear-ance of bullae, which lead to ulceration and sloughingof the underlying epidermal base similar to physiologi-cal damages caused by burns.
• TEN causes crusting, desquamation, and ulcera-tion of the mucous membranes in the oral, ocu-lar, and genital mucosa. Bleeding from internalmucous membranes can progress to hypovolemiaand lead to death.
• TEN is often accompanied by ocular manifesta-tions that can lead to permanent loss of vision.
• The diagnosis of TEN is based on clinical findings:erythematous macules, epidermal detachmentand blistering, a positive Nicolsky sign, andulceration of mucosal surfaces.
• Intravenous steroids are the initial treatment ofchoice of TEN. The primary alternative is intra-venous human immunoglobulin (IVIg).
• Treatment with plasmapheresis has gained sup-port. The filtration of plasma removes theoffending autoantibodies from circulating blood.Plasmapheresis is valued for its rapid results, rareside effects, and efficiency in treating patientswith TEN refractory to steroids or IVIg.
• A comprehensive team approach that emphasizessupportive care is essential. Detachment of theepidermal layer results in marked fluid and elec-trolyte depletion, and loss of the skin’s naturalbarrier properties increases the risk for infectionand subsequent sepsis.
• Meticulous supportive therapy is the sole inter-vention that consistently improves prognosis.
• Patients with TEN should be transferred as soonas possible to an intensive care setting, typicallya burn unit or a specialized intensive care unit.
Seczynska B, Nowak I, Sega A, Kozka M, Wodkowski M, Królikowski W, Szczeklik W. Supportive Therapy for a Patient With Toxic Epidermal Necrolysis UndergoingPlasmapheresis. Critical Care Nurse. 2013;33(4):26-38.
38 CriticalCareNurse Vol 33, No. 4, AUGUST 2013 www.ccnonline.org
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from

and Wojciech SzczeklikBozena Seczynska, Ilona Nowak, Aurelia Sega, Maria Kozka, Michael Wodkowski, Wieslaw KrÓlikowskiPlasmapheresisSupportive Therapy for a Patient With Toxic Epidermal Necrolysis Undergoing
http://ccn.aacnjournals.org/Published online ©2013 American Association of Critical-Care Nurses
10.4037/ccn2013555 26-38 33 2013;Crit Care Nurse
http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ccn Submit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
362-2049. Copyright ©2016 by AACN. All rights reserved. bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) Critical Care Nurse is an official peer-reviewed journal of the American Association of Critical-Care Nurses (AACN) published
by AACN on April 19, 2018http://ccn.aacnjournals.org/Downloaded from