Summer Emergencies Pacemakers Quick Trach APRIL 2015 CE CONDELL MEDICAL CENTER EMS SYSTEM SITE CODE:...
107
Summer Emergencies Pacemakers Quick Trach APRIL 2015 CE CONDELL MEDICAL CENTER EMS SYSTEM SITE CODE: 107200E-1215 Prepared by: Sharon Hopkins, RN, BSN Revised 4.16.15 1
-
Upload
philomena-joseph -
Category
Documents
-
view
213 -
download
0
Transcript of Summer Emergencies Pacemakers Quick Trach APRIL 2015 CE CONDELL MEDICAL CENTER EMS SYSTEM SITE CODE:...

Summer EmergenciesPacemakersQuick Trach
APRIL 2015 CECONDELL MEDICAL CENTER
EMS SYSTEMSITE CODE: 107200E-1215
Prepared by: Sharon Hopkins, RN, BSN
Revised 4.16.151

Objectives
Upon successful completion of this module, the EMS provider will be able to:
1. Distinguish the difference between heat cramps, heat exhaustion, and heatstroke.2. List the steps of assessment for the patient involved in water emergencies.3. Analyze signs and symptoms to determine the level of allergic reaction a patient is experiencing.4. Actively participate in review of selected Region X SOP’s as related to the topics presented.
2

Objectives cont’d
5. Review pacemaker rhythms. 6. Actively participate in case scenario discussion. 7. Actively participate at the paramedic level in return demonstration of insertion of the Quick Trach. 8. Actively participate in ventilating a manikin at
the appropriate ventilation rate for the situation. 9. Successfully complete the post quiz with a score of
80% or better.
3
Thermoregulation
The ability to maintain or regulate a steady body temperature despite changes to the environmentHypothalamus at base of brain regulates temperature
You can lose or gain heat from and within the body itself
You can lose or gain heat by contact with the external environment
The body’s core/normal temperature of deep tissues is normally 370C or 98.60F
4
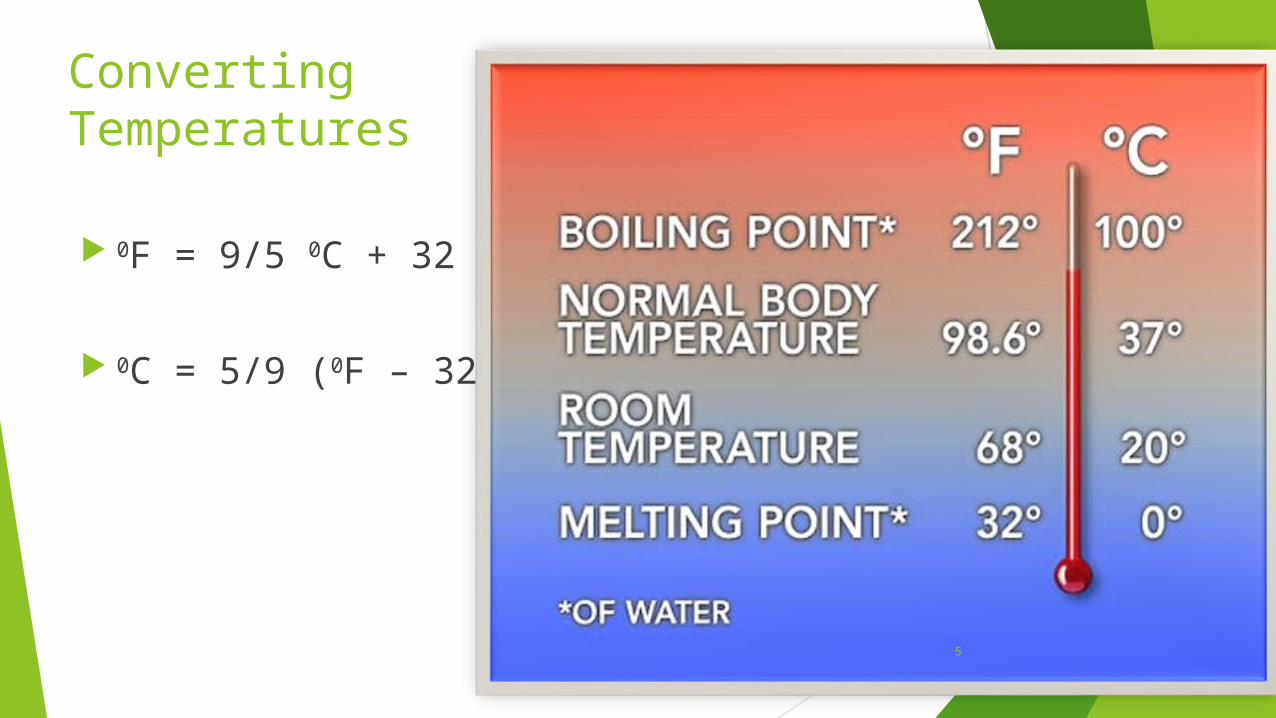
Converting Temperatures
0F = 9/5 0C + 32
0C = 5/9 (0F – 32)
5
Thermal Gradient
The difference in temperature between the environment (also called the ambient temperature) and the body
Heat flows from the warmer environment (higher temp) to the cooler environment (lower temp)
Wind and relative humidity (percent of water vapor in the air) affect heat gain and loss
6

Process of Transferring Heat
ConductionDirect contact of one surface with another
ConvectionHeat loss to air currents passing over the bodyHeat must be conducted and exposed to the air before being
carried away by convection Radiation
Heat loss via infrared raysExposed body could lose 60% of total body heat in
environment with normal room temperature
7

Transfer of Heat cont’d
EvaporationChange of a liquid to a vaporWater or sweat evaporates from skinHeat loss is great via evaporation of fluids
from the lungs Normal water loss from the skin and lungs is
approximately 600 ml per day
8
Transfer of Heat cont’d
RespirationCombines the mechanics of convection,
radiation, and evaporationAccounts for a large proportion of heat loss
Heat transfers from body to inspired air via convection and radiation
Evaporation process in lungs humidifies inspired air
During expiration, humidified air released to the environment creating on-going heat loss
9

Measuring Body Temperatures By touch – get a sense of cool, warm, hot Oral – normal 98.60F (370C) Rectal – 0.5 – 10F higher than oral Tympanic – 0.5 – 10F higher than oral Axillary – 0.5 – 10F lower than oral Core – area where most major organs are located
In the field tympanic (ear) or rectal In the hospital bladder, heart with use of
special catheters/measuring tools
10
Homeostasis
Process of maintaining constant suitable conditions Body functions within small ranges of “normal” Hypothalamus at base of brain responsible for
temperature regulation (i.e.: the “thermostat”) Body constantly compensating to maintain “normal”
Core and peripheral temperaturesOxygen levelsEnergy supplies
11

Homeostasis of Core Temperature
Body continually adjusting metabolic rateThe rate in which the body consumes energy
to maintain function required at the timeEnergy production = heat production
Temperature controlled by dilating or constricting blood vesselsDilation of blood vessels – flushed skinConstriction of blood vessels – pale skin
12

Temperature Control
To decrease the body temperature Blood vessels dilate to expose more vessel surface space
to the skin Excess heat carried from core to the periphery close to the
skin; heat dissipates from skin to environment
To increase body temperature Blood vessels constrict to shunt warm blood away from
superficial veins near skin and back into deeper veins near the core
Shivering increases the metabolic rate and generates heat
13
Risk Factors Impacting Environmental Illness Age
Especially very young and elderly
Poor general health Fatigue Predisposing medical conditions (i.e.: Diabetes – damages
autonomic nervous system & interferes with thermoregulatory input)
Certain meds – prescription and OTC Level of acclimatization – adjustment to the environment
14

Factors Influencing Impact of Environmental Challenges
Length of exposure Intensity of exposure Environmental factors
Humidity – influences evaporation rateWind – influences convection
15

Heat Emergencies - Hyperthermia
Condition involving unusually high body core temperatures
Usually involves a transfer of heat from the external environmentCould include excessive heat production within the
body Could occur with use/abuse of certain medications
Malignant hyperthermia is a severe response to use of certain anesthetics
16

Eliminating Excessive Heat
Body’s attempt to eliminate excessive heat: Diaphoresis – due to sweating mechanism
Evaporation process to reduce the temperature
Increased skin temperature to touch – due to vasodilation Moves more blood volume to the skin surface to
induce radiation, conduction, convection
Flushing due to vasodilation process
17

Heat Cramps / Muscle Cramps
Caused by overexertion and dehydration in high temperature situations
Sweating is a response to lower the body temperatureSodium (salt) is transported to the skinWater follows sodiumWater on skin surface cools body via evaporation
18

Heat Cramps cont’d
Loss of electrolytes due to sweatingCan cause intermittent skeletal muscle
crampingExtremitiesAbdominal muscles
Patient generally remains alert and complains of weakness
19

Heat Cramp Signs and Symptoms
Dizziness Syncope/near-syncope Stable vital signs Body temperature normal or slightly
elevated Skin moist and warm
20
Treatment Heat Cramps
Consider what is making the patient symptomatic
Aim your therapy at the source of the problemRemove from the offending environmentRemove clothing as necessary to facilitate coolingPatient education goals
Cooling techniquesAppropriate hydration guidelines
21
Heat Exhaustion
An acute reaction to
heat exposureThe most common heat emergencyPatient can lose 1-2 L of fluid per hour
Loses sodium and waterDehydration and electrolyte loss from sweating often account for the signs and symptoms noted
22

Heat Exhaustion – Body Responses
General vasodilationPooling of blood volume mimics a decrease in
blood volumeLeads to a decrease in cardiac output
History of exposure to a heated environment helps with the diagnosis
If treatment is not instituted, the patient may progress to heat stroke
23

Signs and Symptoms Heat Exhaustion Increased body temperature (>37.80C / 1000F) or Cool and clammy with heavy perspiration Rapid and shallow respirations Weak pulse Diarrhea Muscle cramps Weakness May have loss of consciousness
24

Forming Your General Impression
History and assessment very importantNeed clues to determine a working diagnosis to know which
treatment plan to institute In the presence of the following CNS signs &/or symptoms
consider interventions for heat stroke Headache Anxiety Paresthesia - pins and needles sensation Impaired judgment Psychosis
25

Treatment Heat Exhaustion
Move to a cooler environment Remove as much clothing as possible, as indicated Begin to fan the patient - air currents (convection) Keep patient supine IV fluid challenge
Adult: 200 ml increments; titrated with frequent reassessmentsNote: adult formula also calculated at 20 ml/kg
Peds: 20ml/kg; repeat to max of 60 ml/kg; titrated
26
Heatstroke
True environmental emergency Hypothalamic temperature regulation lost Hyperthermia leads to cell death and damage
to brain, liver, kidneys Indications of heat stroke
Central nervous system imbalanceBody temperature usually >1050F (40.60C)Absence of sweating
27
Heatstroke – Hot & Dry or Hot & Wet?
Sweating stops usually from destruction of sweat glands or due to dysfunction from sensory overload
Patient may still be covered with sweat though from earlier exertion (i.e.: marathoner, construction worker)
Classic heatstroke – hot, red, dry skinExertional heatstroke– hot, moist skin
28
Classic vs Exertional Heatstroke
Predisposing factors for classic heatstroke Age Diabetes Other medical conditions
Predisposing factors for exertional heatstroke Generally person in good health Excessive ambient temperature with excessive
exertion with prolonged exposure and poor acclimation
29

Exertional Heatstroke – Big ProblemsSevere metabolic acidosis
From excessive lactic acid accumulationLactic acid develops as by-product during
anaerobic metabolismHyperkalemia – excessive potassium
moved from the cell into the bloodstreamReleased from injured cells or created due
to renal failure (poor clearing capability) or development of metabolic acidosis
30

Signs and Symptoms Heatstroke
Hot skin that is dry or moist Very high core temperature Deep respirations (blowing off acids) that become shallow, rapid
and later slow Rapid, full pulse initially then slow Hypotension with low or absent diastolic Confusion or disorientation or unconsciousness CNS impairment – headache, anxiety, impaired judgment,
paresthesia, psychosis Possible seizures
31

Treatment Heat Stroke Move patient to cool environment Remove unnecessary clothing Fluid challenge
Adult 200 ml increments (formula 20 ml/kg)Peds 20ml/kg to a max of 60 ml/kg
Rapid cooling proceduresDouse towels or sheets with water and place over patientFan body – increases air current flow (convection)Cold packs to lateral chest wall, groin, axilla, neck, temples, behind
knees
32
Shivering
Shivering raises body core temperatureCan occur in the setting of too rapid of a cooling process
To stop shiveringAdult: Valium 5 mg IVP/IO over 2 minutes
Can repeat same dose in 2 minutes titrated to the max
Peds: Valium 0.2 mg/kg over 2 minutesCan repeat same dose in 15 minutes titrated to the max
Total maximum is 10 mg for the adultTotal max for peds is 5 mg (<5 years old) and 10mg (>5
y/o)
33

Water Emergencies
DrowningRespiratory impairment from submersion or immersion in
a liquid Outcome
Mortality – deathMorbidity – developing a medical problemNo morbidity – no problem
A leading cause of death in children Most drownings occur in freshwater – the swimming pool
34

Sequence of Events of Drowning
Submersion Struggle with attempt at breath holding Instinctive inspiratory and swallowing efforts made
Water enters mouth, posterior oropharynx, and stomach
Apnea causes rise in retained CO2 levels; decrease in O2
Hypoxia stimulates trigger to gasp Acidosis is developing Reflexive laryngospasm and bronchospasm occur
Minimizes amount of water actually measured in lungs
35
Sequence cont’d
Reflex swallowing continuesGastric distension, for vomiting and aspiration
Hypotension, bradycardia then death occur Water enters lungs (before laryngospasm or after
laryngeal relaxation) Water in airways blocks gas exchange in alveoli Even small amount of water washes away
surfactantAtelectasis develops (alveolar collapse)
36

Surfactant
A thin film substance in alveoli that keeps them open
Decreases pressure needed for subsequent inflation
Without adequate levels of surfactant, alveoli collapseBlood shunted past collapsed alveoli and is not
oxygenated before it is perfused throughout the body 37

Drowning
Outcome determined by degree of anoxia Goal of therapy directed at reversing anoxia Prehospital interventions and treatment is
the same regardless of the source of the drowning –
freshwater versus saltwater
38

Factors Affecting Survival
Cleanliness of water source Length of time submerged Age of victim General health status of victim
Positive influence on outcome – immediate recognition of the drowning and initiation of immediate CPR
39

Treatment Near Drowning
Routine medical care Spinal precautions Consider CPAP in the adult if indicated If stable (awake, alert, warm and dry, B/P
>90 in adult, then transport
40

Treatment Near Drowning cont’d
Anticipate need for ventilation support Anticipate vomitus and laryngospasms
Suction available for vomitus Positive pressure ventilations (i.e.: BVM) for
laryngospasmsMany drowning victims may have foaming present
Focus on oxygenation and ventilation more than on suctioning
Protect the patient from heat lossRemove wet clothing, cover body as much as
possible
41

Treatment Unstable Near DrowningAltered Mental Status; B/P <90
Secure airway Assess for hypothermia
If normothermic, treat dysrhythmias per protocol If hypothermic, also follow hypothermic protocol
Assist ventilations as indicated BVM – 1 breath every 5 – 6 seconds
1 breath every 3-5 seconds infant and child to 8
Advanced airway1 breath ever 6 -8 seconds
42

Immune System Responsible for fighting infection The principle system involved in allergic reactions
Goal- rid body of offending foreign material (antigen) Components found in blood, bone marrow, and lymphatic
system Additional systems affected in immune response
CardiovascularRespiratoryNervousGastrointestinal
43

Immune Response
To destroy or inactivate pathogens, abnormal cells, or foreign molecules
Activation of cascade of events triggered by exposure to foreign substance – an antigen
Immune system directs attack on foreign substance to deactivate or destroy offending agent
There is a chemical attack of antibodies on the invading agent or antigen
44

Immune Response cont’d
Primary response Initial (first time) exposure to an antigenAntibodies developed to respond at
subsequent exposures Secondary response
Release of antibodies, upon recognition of the antigen, to facilitate removal of offending antigen
45
Histamine
Potent chemical Principle chemical released in allergic reaction Goal of histamine release
Minimize body’s exposure to the antigen Bronchoconstriction - lung exposure Increased intestinal motility - move antigen thru system Vasodilation - remove antigen from circulation Increased vascular permeability - remove antigen from
circulation
46
Histamine Release – Smooth Muscle Constriction
Bronchoconstriction Minimizes amount of antigen that can enter
the respiratory tract Abdominal cramping
From increased gastric motility Diarrhea and vomiting
Attempt to move antigen quickly through the system and eliminate it from the body
47

Histamine Release – Increased Capillary Permeability
Third spacing – fluids (plasma) shift from intravascular to interstitial space Trying to move offending antigen out of circulatory system Angioedema especially of head, neck, face, upper airway
Relative hypovolemia Decreased cardiac output Decreased tissue perfusion Impaired cellular function Cellular death
48

Histamine Release – Peripheral Vasodilation
Decreased peripheral vascular resistance Less tone in blood vessels Less efficient circulation of blood Decreased preload – amount of blood returning to
the heart Decreased after-load – the pressure the heart must
pump against to move blood Blood pressure will drop Cardiac output drops
49

Allergic Reaction Exaggerated response by immune system to foreign
substance (antigen) Repeated exposure results in much stronger immune
response Hypersensitivity
Unexpected, exaggerated reaction to an antigen Range from mild skin rashes to more severe systemic
reactions throughout many more body systems
50

Anaphylaxis
Most severe allergic reaction Usually occurs when an antigen enters the circulation
Rapid and wide distribution facilitated through-out the body
Most reactions occur within seconds In a few cases there may be a delay over an hour
The more severe the reaction, the quicker the onset of signs and symptoms
51

Anaphylaxis
Life-threatening emergency requiring prompt recognition and intervention
Can develop in seconds; can cause death in minutes after exposure
Develops after exposure and sets off biochemical reactions that could lead to shock and death
Most common causative agents – injected penicillin and hymenoptera (bee and wasp) stings
52

Anaphylaxis – Presentation / Appearance
Flushing Rash – fine, red, diffusely spread over entire
body Itching Hives (urticaria) – wheal of red, raised bumps
across body Swelling – 3rd space fluid shift Pallor and/or cyanosis
53

Anaphylaxis – Respiratory System
Respiratory difficulty with tachypneaSneezing, coughing – trying to rid offending antigenWheezing, stridor – bronchoconstriction & edemaLaryngeal edema – 3rd space fluid shiftLaryngospasm – may cause difficulty in being able to
speak BronchospasmLabored breathing; use of accessory muscles
54
Anaphylaxis – Cardiovascular System
Vasodilation Increased heart rate – compensation attempt Decreased blood pressure – from capillary
leakage, peripheral vasodilation and eventual failure of compensatory mechanisms
Development of acidotic and hypoxic environment
Eventual fall in cardiac output55
Anaphylaxis – Nervous System
Dizziness Headache Change in level of consciousness Convulsions Tearing
56

Anaphylaxis – Gastrointestinal System
Nausea and vomiting – to rid offending antigen
Abdominal cramping – hypermotility Diarrhea – to rid offending antigen
57

Anaphylaxis – Ominous Signs
Decline in respiratory rate Following increasing edema of tissues and
initial dyspnea Bradycardia
After compensatory mechanisms have failed Drop in blood pressure
Significant 3rd space fluid shift has occurred along with peripheral vasodilation
58
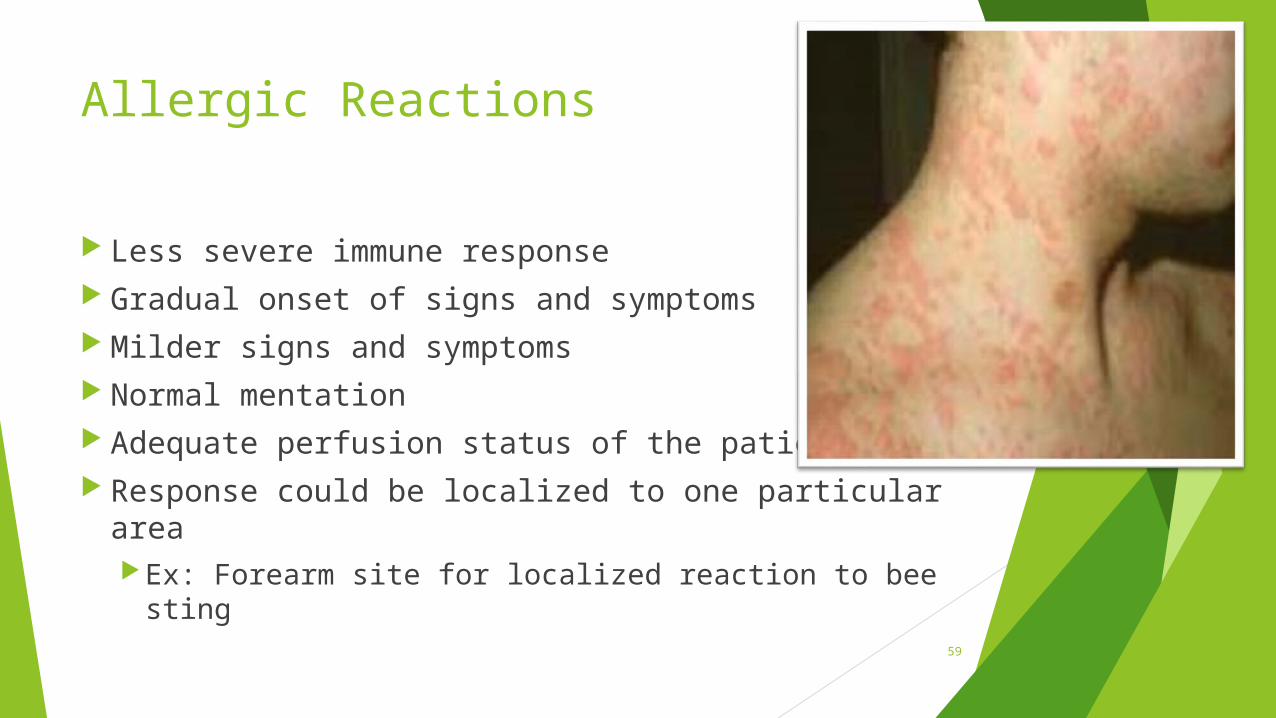
Allergic Reactions
Less severe immune response Gradual onset of signs and symptoms Milder signs and symptoms Normal mentation Adequate perfusion status of the patient Response could be localized to one particular
areaEx: Forearm site for localized reaction to bee sting
59

Allergic Reactions
May experience mild flushing, itching, and rash Urticaria (hives) may be present May experience mild bronchoconstriction
Body still trying to minimize exposure to antigen Mild abdominal cramps and diarrhea
Body still trying to rid self of offending antigen
60
Intervention of Allergic Reactions
To know the correct intervention relies on an accurate and detailed assessment
GoalsDetermine extent of immune response
Allergic reaction or anaphylaxis
61

Interventions
EpinephrineVasoconstrictorBronchodilator
BenadrylAntihistamine- stop release of
histamine response Fluids
Volume expansion62

Region X SOP - Allergic Reaction Stable
Hives, itching, red skin GI distress Alert, warm and dry; systolic B/P >90mmHg
Ice pack to site Benadryl (antihistamine) 25 mg IVP slowly over 2
minutes or IMPeds Benadryl 1 mg/kg IVP to adult max of 25 mg
63

Region X SOP – Allergic Reaction Stable with Airway Involvement
Epinephrine 1:1000 0.3mg SQMay repeat in 5 minutesPeds dose Epi 1:1000 0.01 mg/kg SQ (max 0.3 mg)
Benadryl 50 mg IVP slowly over 2 minutes or IMPeds dose Benadryl 1 mg/kg (max 50 mg)
If wheezingDuoneb treatment
Albuterol 2.5 mg with Atrovent 0.5mg
If no improvement repeat Duoneb treatment If no improvement, albuterol alone
64

Region X SOP – Anaphylactic Shock
Altered level of consciousness Systolic B/P <90 mmHg
Secure airwayMake sure patient can ventilate/breathe and is
adequately oxygenated Goals of treatment
Open airways Support vascular status
65

Adult Anaphylactic Shock Medications
Epinephrine 1:1000 0.5 mg IMCan repeat in 5 minutes
Benadryl 50 mg IVP/IO slowly over 2 minutes or IM IV/IO fluid challenge in 200 ml increments Duoneb treatment – Albuterol with Atrovent
If no improvement, administer Albuterol alone every 5 minutes
66

Pediatric Anaphylactic Shock Medications
Epinephrine 1:1000 0.01 mg/kg IMMax 0.3 mg/0.3 ml per single doseMay repeat in 5 minutes
Benadryl 1 mg/kg to max of 50 mg Fluid challenge 20 ml/kg
Titrated to desired patient responseMax 60 ml/kg
Duoneb treatment – Albuterol with Atrovent If no improvement, administer Albuterol alone every 5 minutes
67

Continued Deterioration AnaphylaxisContact Medical Control to considerEpinephrine 1:10,000
Adult 1:10,000 0.5 mg IVP/IOPeds 1:10,000 0.01 mg/kg IVP/IOAdminister slowly
This is adrenalineA strong cardiac stimulant!!!Have patient on the cardiac monitor
68

Epi Pens
Prescribed medication for use by patients Adult dose (yellow) – 0.3 mg Peds dose (green) – 0.15 mg To activate
Cap removed Gripped firmly – keeping fingers away from tip Jabbed into outer thigh and held in place 10 seconds
Caution – needle remains exposed after activation Note: If patient’s EpiPen is ready to be used by them, don’t delay. Assist patient
in using their pen; repeated doses, if necessary, of Epinephrine will be your stock
69

Pacemakers
Artificial pulse generator that delivers an electrical currentStimulates depolarization
Useful when normal pacemaker site (SA node) unreliable
How would you know a patient has one? Patient tells you See it written in the history See the bulge under the skin Medic alert tag
70
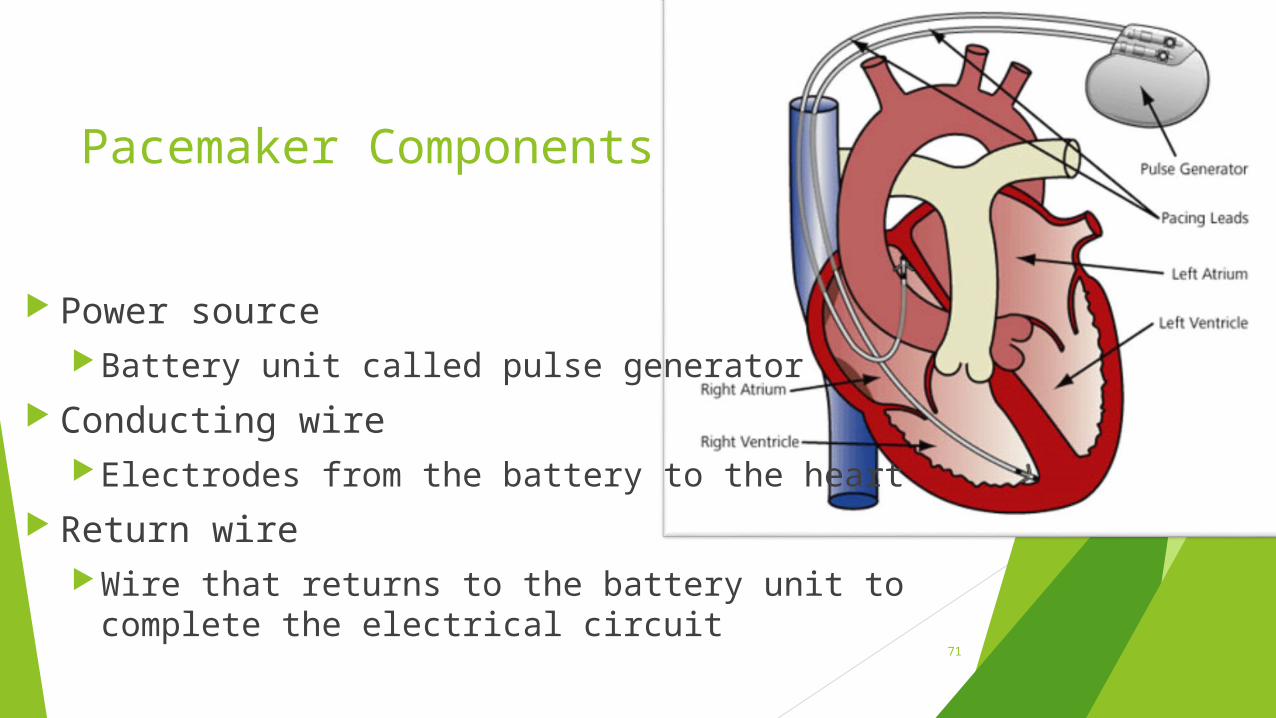
Pacemaker Components
Power sourceBattery unit called pulse generator
Conducting wireElectrodes from the battery to the heart
Return wireWire that returns to the battery unit to
complete the electrical circuit71

Pacemaker Types - Temporary
Usually used in acute setting and for relatively short periods of time (i.e.: acute MI)
Pacing unit outside the bodyTranscutaneous – stimulus across the skinTransvenous – via venous vessel access
Current measured in milliamperes (mA)
72

Pacemaker Type - Permanent
Long term support anticipated Wires inserted surgically into the right heart Battery implanted in fatty layer pocket
under the skin of the chest or abdominal wallMay be inferior to right or left clavicle
Usually opposite side to dominant hand
Could be abdominal placement – rarer nowadaysCould be combination with AICD
Current AICD’s also have capability to pace73

Pacemaker Sensing
Parameters set on pacemaker determine if pacing stimulus is necessary or is withheldDemand mode – pacemaker functions only
when patient’s own rate falls below a preset valuePacemaker functions on “demand”Most common type of pacemaker setting used
Fixed mode – pacemaker will fire regardless of what the intrinsic (normal) conduction system doesInfrequently seen nowadays
74

Pacemaker Types - Ventricular Single-chamber pacemaker Stimulates only the ventricles See spike followed by wide QRS Most common type of pacemaker implanted
Can look like slow monomorphic VT at first glanceBut, spikes are present; history supports pacemaker
75

Pacemaker Type - Atrial
Single chamber pacemaker Atria are depolarized Heart’s own conduction system used to stimulate the
ventricles See spike followed by P wave and then normal QRS
76

Pacemaker Type – AV Synchronous
Dual-chamber pacemakerBoth atria and ventricles are stimulatedAtrial kick is restored
Atria contract and therefore squeeze more blood to the ventricles prior to each contraction
See spike followed by P wave and then spike followed by wide QRS
77

Pacemaker Malfunction – Failure to Capture
Spike not followed by complex therefore no depolarization
Causes: Battery failure, displacement of lead wire, energy (mA) too low, edema/scar tissue or perforation of myocardium, electrolyte imbalance
Presentation: fatigue, bradycardia, low B/P, syncope
78

Failure to Capture EMS Intervention
EMS intervention: reposition patient in case of loss of lead wire contact – turn patient onto left sideMay “float” lead wire into myocardial wall contact
Follow symptomatic bradycardia protocolAdminister Atropine 0.5 mg IVPApply and prepare to begin operation of TCP
79

Pacemaker Malfunction – Failure to Sense / Competition
Pacemaker fires regardless of the patient’s own rhythm No sensing of spontaneous myocardial depolarization There is potential competition for control of the heart Danger – pacemaker spike may fall on vulnerable
downslope of T wave VF Causes
Battery failure, fracture of wire, displacement of electrode tip
80
Pacemaker Malfunction – Runaway Pacemaker
Pacemaker rate too fast but continues to capture
Malfunction of impulse generatorNot as common in newer models of
pacemakers Typical pacemaker rate set around 70’s
(beats per minute)
81
Pacemaker Malfunction – Battery Failure
Absence of any spikes when they would be anticipated
Can cause life-threatening situation where patient dependent on pacemaker to support a healthy heart rate
Close patient monitoring and long battery life usually avoids this problem
82

Assessment of Patient
Always check the patient first Determine perfusion status / mechanical
responseEvaluate the patient’s level of consciousnessEvaluate blood pressure to determine perfusion
Presence of radial pulse indicates B/P is present
EKG strip is printable representation of electrical activity
83

Assessment of Paced Rhythm
Does each spike capture?Each spike is followed by a complex
Is rate reasonable? Are spikes competing with the patient’s
rhythm? Is pacemaker functioning consistently and
reliably?
84

Patient Management
If pacemaker malfunctions, treat the patient and not necessarily their rhythmDon’t treat the pacemaker
Provide a copy of the rhythm strip for documentation in the patient’s hospital medical record
It is safe to touch a patient if the TCP is in useElectrical stimuli is not transferred to you 85

Transcutaneous Pacing – Potential Complications
Coughing Skin burns Interference with sensing from patient agitation
or muscle contractions Pain Failure to recognize non-capture Tissue damage 3rd degree burns
86

Documentation of TCP Use Initial and repeat EKG rhythms on patient chart Date and time pacing started
RateOutput (mA) to obtain capturePatient’s response
Intervention for comfort/pain control measuresValium 2 mg IVP/IO; repeated to max of 10mg
A benzodiazepine to take the edge off
Fentanyl 1 mcg/kg IVP/IO/IN; repeated in 5 minutes A synthetic opioid for pain control
87
QuickTrach
IndicationsEmergency assisted ventilations when all other means
have failed Contraindications
Tracheal transection; other measures are successful Adult device – size 4.0 mmID if >77# (>35 kg) Peds device – 2.0 mmID if 22-77# (10-35 kg)
<22# (10 kg) – use needle cricothyrotomy procedure88

Quick Trach Procedure
Attempt to ventilate patient Assemble equipment
Quick Trach kit – appropriate sizeBVMSkin prep material4x4’s
Position patient supine, neck hyperextended if able
89

Quick Trach Procedure cont’d
Locate Cricothyroid membrane Inferior to thyroid cartilage (Adam’s apple)Superior to cricoid cartilagePalpate from notch upward
1st bone is cricoid cartilageGo to space just above this bone
Cleanse site
90

Quick Trach Procedure cont’d
Secure larynx laterally between thumb and forefingerAnchor and stretch skin slightly
Puncture Cricothyroid membrane at 900 angle Confirm entry of needle to trachea
Aspirate air through the syringe Change angle of insertion to 600 with tip
pointed toward feet91
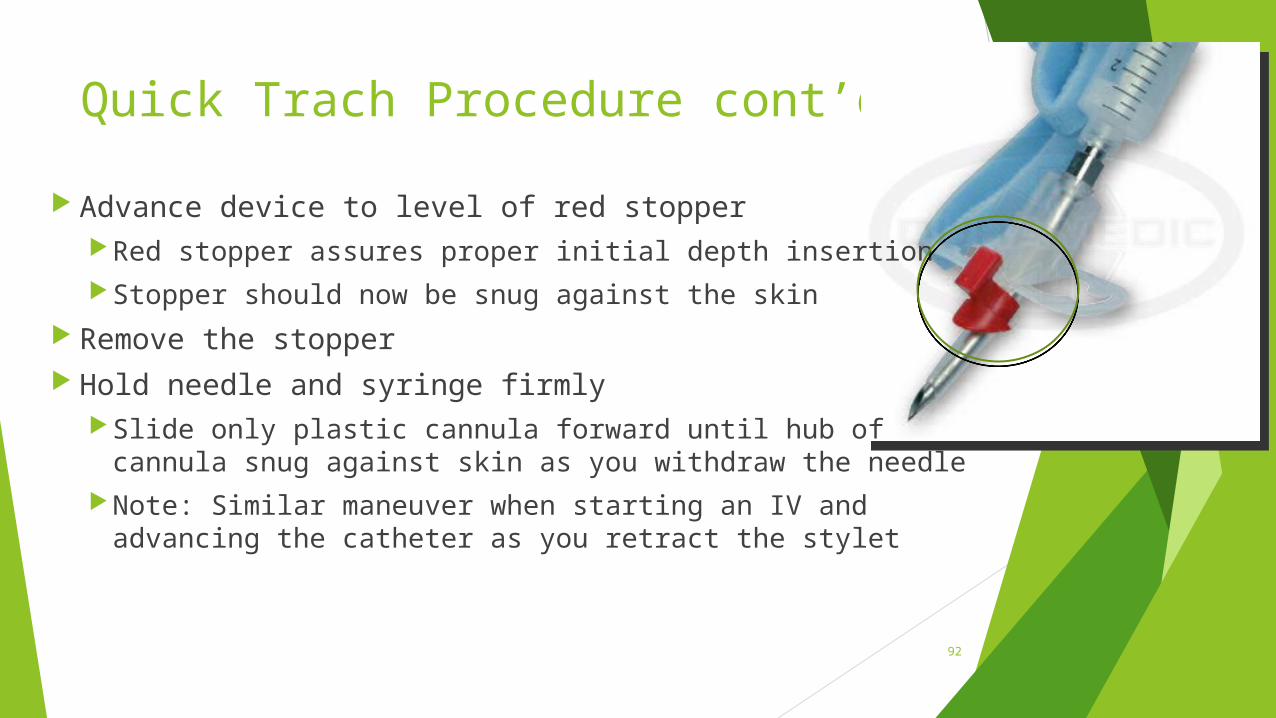
Quick Trach Procedure cont’d
Advance device to level of red stopperRed stopper assures proper initial depth insertionStopper should now be snug against the skin
Remove the stopper Hold needle and syringe firmly
Slide only plastic cannula forward until hub of cannula snug against skin as you withdraw the needle
Note: Similar maneuver when starting an IV and advancing the catheter as you retract the stylet
92

Quick Trach Procedure cont’d
Distal end of flexible tubing attached to Quick Trach hub BVM attached to proximal end of flexible tubing
Helpful to have flexible tubing already attached to BVM
Immediately begin to ventilate with 100% O2
Use pre-attached strap to secure deviceMake sure device is snug against skin
Device can easily be coughed out
Helpful to have one end of strap already attached to device prior to insertion
93

Quick Trach Use
Confirm placement by auscultation and observation of chest rise
Continuously monitor airway and lung sounds to ensure proper placement
Monitor for over expansion of chest wallMay need to detach BVM to allow for passive
exhalation to allow deflation of lungs Note general improvement in patient’s overall
condition94

Case Scenario Discussion
Review presentation of patient Determine your general impression Determine your treatment choice
Use your SOP booklets as a resource Discuss reassessment steps Discuss documentation highlights related to
the patient situation
95

Case Scenario #1
Patient works on a road crew Complains of feeling lightheaded and dizzy VS: 148/88; P – 90; R – 20; warm and sweaty History: hypertension, high cholesterol,
diabetes
General impression? Interventions?
96

Case Scenario #1 General impression
Heat emergency (exhaustion)Consider diabetic problem (blood sugar 72)Consider other medical problems
InterventionRemember to consider other causes of feeling lightheaded and
dizzyCool – remove from heat, remove extra clothingFluids – 200 ml fluid bolus increments
97

Case Scenario #2
98
Person training for a marathon found collapsed on a trail; unknown length of timeTemperature outside 940 and 85% relative humidity
Unknown medical history Patient moans when touched Hot and moist VS: 86/62; P – 110; R – 28 and labored
General impression? Interventions?

Case Scenario #2
General impressionHeat strokeAcute medical problem – acute MI, brain insultTrauma
InterventionsBegin to cool – wet towels, fanning, air conditioning
IV – O2 - monitor
IV fluids – 200 ml incremental fluid challenges
Remember to consider other causes of altered level of consciousness
99

Case Scenario #3
Your adult patient was drinking from a can of soda and was stung by a bee that was in the can
Has swollen lips Complains of itchy throat and a feeling of swelling in
the throat VS: 110/70; P – 98; R – 22; SpO2 97%
General impression? Interventions?
100

Case Scenario #3
General impressionAllergic reaction with airway involvement
InterventionsConsider IV – O2 - monitor
Epinephrine 1:1000 0.3 mg SQMay repeat every 5 minutes
Benadryl 50 mg slow IVP or IM If wheezing, Duoneb ( may repeat)
101

Case Scenario #4
Adult patient ate a dip and 15 minutes later complains of abdominal cramping, diarrhea, all over itching
You can hear audible wheezingConfirmed bilateral wheezing – breath sounds barely
audible VS: B/P 88/60; P – 116; R – 22
General impression? Interventions?
102
Case Scenario #4
General impressionAnaphylactic shock
Interventions IV – O2 – monitor
Epinephrine 1:1000 0.5 mg IM (may repeat every 5 minutes)
Benadryl 50 mg IVP/IO or IMFluid challenge – 200 ml incrementsDuo neb (may repeat Albuterol neb if needed)
103

Case Scenario #5
Your 78 year old patient complains of pounding in their chest and generally not feeling well
Pulse is irregular, skin warm and moist VS: B/P 92/50; P – 40; R – 18; SpO2 97%
Hx: Hypertension, gout, CABG, pacemaker, high cholesterol
General impression? Interventions?
104

Case Scenario #5
General impressionConsider cardiac problem
InterventionApply cardiac monitorConsider obtaining 12 lead EKG, if possible, on
cardiac calls
105

Case Scenario #5
Impression – Pacemaker with failure to capture Intervention
Turn patient onto their left sideMay “float” catheter into position
Support perfusionConsider Atropine dosePrepare for application TCPConsider need for Dopamine drip to support blood pressure
Increases strength of cardiac contractions
106

Bibliography
Bledsoe, B., Porter, R., Cherry, R. Paramedic Care Principles & Practices, 4th edition. Brady. 2013.
Region X SOP’s; IDPH Approved April 10, 2014.
Mistovich, J., Karren, K. Prehospital Emergency Care 9th Edition. Brady. 2010.
http://www.scientificamerican.com/article/why-does-lactic-acid-buil/
http://www.icufaqs.org/Pacemakers.doc http://www.cdc.gov/HAI/organisms/cdiff/Cdiff_infect.html http://www.cdc.gov/norovirus/preventing-infection.html
107