
Region X Multiple Patient Management Plan Condell Medical Center EMS System CE July 2009 Site Code...
90
Region X Multiple Patient Management Plan Condell Medical Center EMS System CE July 2009 Site Code #107200E-1209 Prepared by: Steve Holtz, FF/PM Libertyville Fire Department Reviewed/revised by: Sharon Hopkins, RN, BSN, EMT-P
-
Upload
tamsyn-douglas -
Category
Documents
-
view
215 -
download
0
Transcript of Region X Multiple Patient Management Plan Condell Medical Center EMS System CE July 2009 Site Code...

Region X Multiple Patient Management Plan
Condell Medical Center EMS System CE
July 2009Site Code #107200E-1209
Prepared by: Steve Holtz, FF/PM Libertyville Fire DepartmentReviewed/revised by: Sharon Hopkins, RN, BSN, EMT-P
ObjectivesUpon successful completion of this module, the EMS
provider will be able to:
1. Explain the purpose of the Region X Multiple Patient Management Plan.
2. Define Class 1, Class 2, and Class 3 incidents.3. Identify responsibilities of the fire department for each
class.4. Define criteria for Category I, Category II, and Category III
trauma patients.5. Define primary, secondary, and reverse triage. 6. Identify the components of the EMS Division of the
Incident Management System.7. Identify the communication process for Class 1, Class 2,
and Class 3 incidents.

Objectives cont’d
8. Describe documentation requirements for Class 2, Class 2, and Class 3 incidents.
9. Describe the purpose of the After Action Report.10. Define triage 11. Identify the principles of START and JumpStart triage.12. Identify when primary and secondary triage techniques
should be implemented.13. Identify the components of the SMART Triage Packs.14. Identify the role of critical incident stress management
(CISM) in MCI.15. Given a simulation, correctly triage patients using
START triage.16. Given a simulation, correctly perform a secondary
triage.

Purpose of the Region X Multiple Patient Management Plan
• An approach to emergency preparedness for all situations
• To provide a communication tool for quick, easy, and appropriate disbursement of patients to area-wide hospitals
• A plan to direct patients from the field to the hospital
• The plan is NOT intended to serve as guidelines for scene management
Definition – Multiple Patients
• Due to the variety of resources spread throughout the area, no number is attached to what defines the magnitude of an incident
• Multiple patients will imply any number 2 and greater
• The class to activate will be department determined
Multiple Patient Incident
• When you have more than one patient for a medical or traumatic event, you are in, at minimum, a Class 1 incident.
• The actual number of victims for a Class 1 or Class 2 can change based on resources available due to time of day, day of week, or location of department

Initial Problem
• Casualties outweigh resources• The objective is to be able to provide the
same level of care to the 1st patient equally through to the last patient
• EMS is initially overwhelmed until additional resources respond
• The hospital(s) will also be overwhelmed initially until they recruit their resources– Make hospital contact as soon as
possible

Universal Goal
• To maximize the number and quality of survivors when presented with any number of sick or injured with the resources at hand or quickly recruited resources while respecting the limitations of the “golden period”
• Golden period – the first hour after time of injury until definitive care is provided
– Starts at time of insult
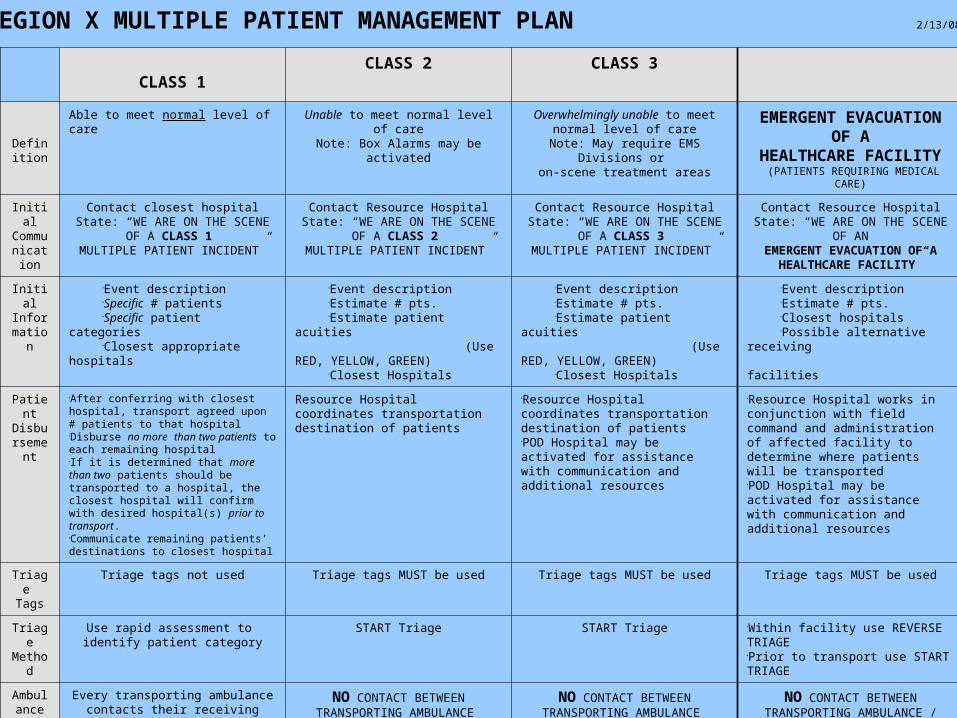
REGION X MULTIPLE PATIENT MANAGEMENT PLAN 2/13/08
CLASS 1CLASS 2 CLASS 3
Definiti
on
Able to meet normal level of care Unable to meet normal level of careNote: Box Alarms may be activated
Overwhelmingly unable to meet normal level of care
Note: May require EMS Divisions or on-scene treatment areas
EMERGENT EVACUATIONOF A
HEALTHCARE FACILITY (PATIENTS REQUIRING MEDICAL CARE)
Initial Communication
Contact closest hospitalState: “WE ARE ON THE SCENE OF A
CLASS 1 MULTIPLE PATIENT INCIDENT”
Contact Resource HospitalState: “WE ARE ON THE SCENE OF A
CLASS 2 MULTIPLE PATIENT INCIDENT”
Contact Resource HospitalState: “WE ARE ON THE SCENE OF A
CLASS 3 MULTIPLE PATIENT INCIDENT”
Contact Resource HospitalState: “WE ARE ON THE SCENE OF
ANEMERGENT EVACUATION OF A
HEALTHCARE FACILITY”
InitialInforma
tion
Event descriptionSpecific # patientsSpecific patient categoriesClosest appropriate hospitals
Event descriptionEstimate # pts.Estimate patient acuities (Use RED, YELLOW,
GREEN)Closest Hospitals
Event descriptionEstimate # pts.Estimate patient acuities (Use RED, YELLOW,
GREEN)Closest Hospitals
Event descriptionEstimate # pts.Closest hospitals Possible alternative receiving facilities
PatientDisbursement
After conferring with closest hospital, transport agreed upon # patients to that hospital Disburse no more than two patients to each remaining hospitalIf it is determined that more than two patients should be transported to a hospital, the closest hospital will confirm with desired hospital(s) prior to transport.Communicate remaining patients’ destinations to closest hospital
Resource Hospital coordinates transportation destination of patients
Resource Hospital coordinates transportation destination of patientsPOD Hospital may be activated for assistance with communication and additional resources
Resource Hospital works in conjunction with field command and administration of affected facility to determine where patients will be transportedPOD Hospital may be activated for assistance with communication and additional resources
Triage Tags
Triage tags not used Triage tags MUST be used Triage tags MUST be used Triage tags MUST be used
Triage Method
Use rapid assessment to identify patient category
START Triage START Triage Within facility use REVERSE TRIAGEPrior to transport use START TRIAGE
Ambulance to
Hospital
Communication
Every transporting ambulance contacts their receiving hospital with abbreviated
reportState:
“WE ARE TRANSPORTING FROM A MULTIPLE PATIENT INCIDENT”
NO CONTACT BETWEEN TRANSPORTING AMBULANCE
AND RECEIVING HOSPITAL
NO CONTACT BETWEEN TRANSPORTING AMBULANCE
AND RECEIVING HOSPITAL
NO CONTACT BETWEEN TRANSPORTING AMBULANCE /
PATIENT TRANSPORTATION VEHICLE AND
RECEIVING FACILITIES
Pt Care Reports
Complete patient care reports as usual Complete patient care reports as usual No patient care reports (Triage Tags serve as written report)
No patient care reports (Triage Tags serve as written report)

REGION X: CLASS 1 ACTIVATION
CLASS 1
Def
init
ion
Able to meet normal
level of care
Init
ial
Com
mun
icat
ion
Contact closest hospital
State: “WE ARE ON THE SCENE OF A
CLASS 1 MULTIPLE PATIENT
INCIDENT”
Init
ial
Info
rmat
ion Event description
Specific # patients Specific patient categories Closest appropriate hospitals
(*Closest hospital must take at least two patients.)
Pat
ient
Dis
burs
emen
t
-After conferring with closest hospital, transport agreed upon # of patients to that hospital (not less than two)
-Disburse no more than two patients to each remaining hospital.
-Communicate remaining patients’ destinations to closest hospital
Am
bula
nce
to H
ospi
tal
Com
mun
icat
ion
Transporting ambulance quickly contacts receiving hospital with an abbreviated report
State:
“WE ARE TRANSPORTING FROM A MULTIPLE
PATIENT INCIDENT”
OT
HE
R
Triage Tags not utilized Use rapid assessment to identify patient category
Complete patient care reports
TRAUMA Traumatic Arrest, Isolated Burns >20%: Transport to closest Trauma Center NO AIRWAY: Transport to CLOSEST Emergency Department
MEDICAL
↓ ↓ CATEGORY I TYPE OF HOSPITAL CATEGORY I
Unstable Vital Signs: Systolic BP ≤ 90 x 2 (Peds ≤ 80 x 2) Glasgow Coma Scale ≤ 10 or deteriorating mental status Respiratory Rate ‹ 10 or › 29 Revised Trauma Score ‹ 11 Anatomy of Injury: Penetrating injuries to head, neck, torso or groin Combination trauma with burns ≥ 20% Two or more proximal long bone fractures Unstable pelvic Flail chest Limb paralysis and / or sensory deficits above the wrist or ankle Open and depressed skull fractures Amputation proximal to wrist or ankle
Transport to
highest level
Trauma Center(s)
within 25 minutes
Transport to
closest Emergency
Department(s)
UNSTABLE
Altered mental status Systolic BP < 100
mmHg
CATEGORY II TYPE OF HOSPITAL CATEGORY II
Mechanism of Injury: Ejection from automobile Death in the same passenger compartment Motorcycle crash › 20 mph or with separation of rider from bike Rollover (unrestrained) Falls ≥ 20 feet (Peds falls ≥ 3X body length) Pedestrian thrown or run over Auto vs. pedestrian / bicyclist with › 5 mph impact Extrication › 20 minutes High speed MVC: Speed › 40 mph, intrusion ≥ 12”,
major deformity ≥ 20” Co-Morbid Factors: Age ≤ 5 without car / booster seat Bleeding disorders or on anticoagulants Pregnancy ≥ 24 weeks
Transport to
closest Trauma
Center(s)
Transport
To closest
Emergency Department(s)
STABLE
Patient alert Skin warm and dry Systolic BP >100 mmHg
CATEGORY III TYPE OF HOSPITAL CATEGORY III
Other simple trauma Transport to closest hospital(s)
Other simple medical
1/23/08
Definition – Class 1 Incident
• The department is able to provide normal level of care– “Business as usual”
• This will be department specific based on internal resources and external working relationships– If your department normally has a neighboring
department respond to certain calls, this is just “business as usual” and should not be construed as anything other than normal for your department

Definition – Class 2 Incident• The department is unable to meet the normal
level of care with their typical response pattern• Box alarms may be activated• This may be due to the severity of the complaint
or the number of patients– Think of a bleacher collapse at a football
stadium– Think of a multi-vehicle incident on the tollway
involving a large number of vehicles– Think 1 large work van rollover with 14
unrestrained ejected passengers

Definition – Class 3 Incident
• A department is overwhelmingly unable to meet normal level of care– Think of a tornado touching down in
town• The department most likely requires
activation of the Incident Management System with use of EMS Divisions with triage and on-scene treatment areas established

Definition – Category I Patient
• This is an unstable patient from traumatic or medical issues
• When possible:
–Trauma patients should be transported to the highest level Trauma Center within 25 minutes
–Medical patients are transported to the closest Emergency Department
Category I Trauma Patient
• Unstable vital signs– Adult systolic B/P < 90 on 2 readings– Pediatric (<15 years old) systolic B/P < 80 on
2 readings– Glasgow Coma Scale < 10 or deteriorating
mental status– Respiratory rate < 10 or > 29– Revised Trauma Score < 11

Category I Trauma Patient
• Anatomical injuries– Penetrating injuries to head, neck, torso, or
groin– Combination trauma with burns > 20% TBSA– 2 or more proximal long bone fractures– Unstable pelvis– Flail chest– Limb paralysis &/or sensory deficits above
wrist or ankle– Open & depressed skull fracture– Amputation proximal to wrist or ankle

Definition – Category II Trauma Patient
• This is a patient with the potential to become critical / unstable due to the mechanism of injury or nature of the complaint but is relatively stable for now
• These patients should be transported to the closest trauma center for traumatic injuries or to the closest Emergency Department for a medical insult
Category II Trauma Patient
• Mechanism of injury– Ejection from automobile– Death in the same passenger compartment– Motorcycle crash > 20 mph or with separation
of rider from bike– Unrestrained in a rollover– Falls > 20 feet for adults and x3 the height for
pediatrics– Pedestrian thrown or run over
Category II Trauma cont’d
– Auto vs pedestrian / bicyclist with > 5 mph impact
– Extrication > 20 minutes– High speed MVC: speed > 40 mph, intrusion >
12 inches; major deformity > 20 inches
• Co-morbid factors– Age < 5 without car / booster seat– Bleeding disorders or on anticoagulant– Pregnancy > 24 weeks
Definition – Category III Trauma Patient
• All other trauma that does not meet criteria for Category I or II
• Typically simple trauma– Lacerations– Simple burns– One extremity fracture– Hip fracture

Definition – Primary Triage
• Triage– The act of sorting patients based on severity
of their injuries or illness
• Object/goal– To do the most good for the most people
• Primary triage– Performed at first contact with the patient– Provides a basic categorization– Must be reproducible results from one
evaluator to another

Universal Triage Categories
• Red– Immediate care necessary
• Yellow– Treatment can be delayed
• Green– Patient requires minimal to no treatment
• Black– Patient is dead or is expected to die
Definition – Secondary Triage
• Ongoing triage • Takes place throughout the incident
– As patients are moved to the treatment area– As patients are in the treatment area– As patients are being transported– Upon arrival at the receiving facility– During their time at the receiving facility
• Patient condition may change throughout the process requiring upgrading or downgrading as determined by the reassessment

Definition – Reverse Triage• Usually used for building evacuation
• Patients that are able to exit on their own do so
• Then patients that require assistance are removed
• Then patients requiring intensive manpower are finally removed
• At the collection center, the process is reversed: most critical are transported first
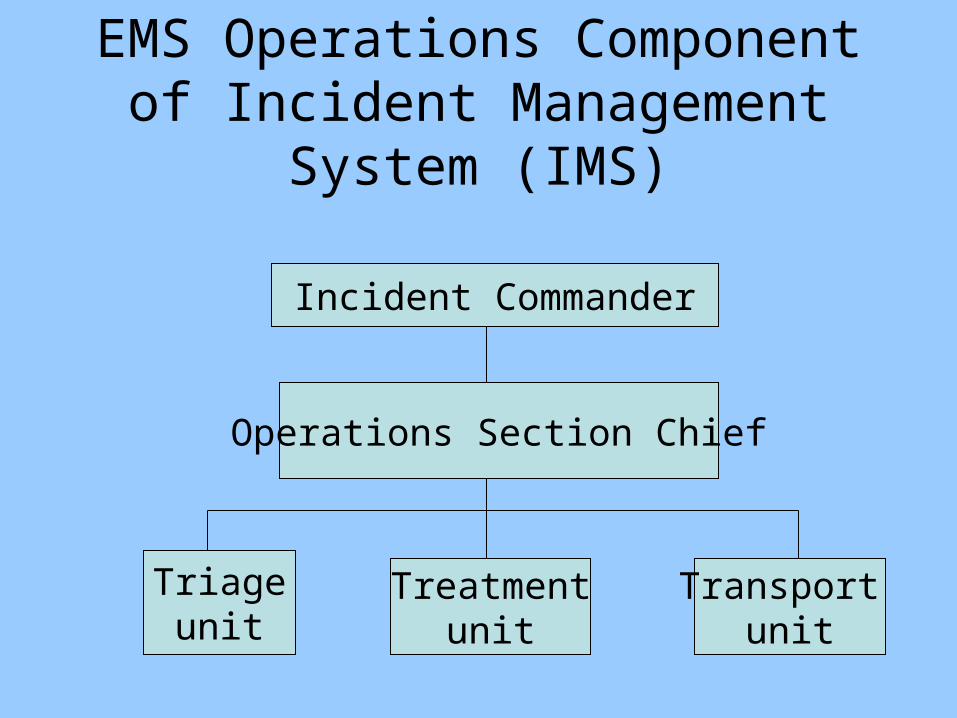
EMS Operations Component of Incident Management System
(IMS)
Incident Commander
Operations Section Chief
Triageunit
Treatmentunit
Transport unit
Communication Process – Class 1
• Contact the closest hospital– Normal facility you transport to
• Communication prompts– “This is ____FD”– “We are on the scene of a Class I multiple
patient incident”– “The incident is a ___”– “We have ____” (state number and category
of patients (ie: Category I, II, or III))

Class 1 Initial Information
• Information provided to the closest hospital:Event descriptionSpecific number of patientsSpecific patient categoriesIndicate what are the closest
appropriate hospitals you might use for transport
Field-to-Hospital Communication
• Class 1
– Every transporting ambulance calls in their individual abbreviated reports
• Respect the radio/phone time knowing multiple calls need to be made
– State:
• “We are transporting from a multiple patient incident”
Class 1 Patient Disposition
• Confer with closest hospital• Agree on number of transports taken to
the closest hospital• Disburse no more than 2 patients to each
remaining hospital– The receiving hospital may request
more than 2 patients based on what they can take
– Inform the closest hospital where patients are being transported to
Communication Process – Class 2
• Contact your Resource Hospital– Advocate Condell– Think – Class 2 is more hectic and you need more
resources than usual so consider the hospital as a resource (ie: Resource Hospital)
• Communication prompts:– “This is ____FD”– “We are on the scene of a Class 2 multiple patient
incident”– “We estimate the following types of patients ____”
(provide number and color category of patients)– “My call back number is ______”
Class 2 Initial Information
• Information provided to the Resource Hospital (CMC)Event descriptionEstimated number of patientsEstimated patient acuities
• Use red, yellow, green colorsState who your closest hospitals are
• Hospitals most likely to receive patients• List hospitals in order of their proximity
Field to Hospital Communication
• Class 2– No contact is made between transporting
ambulances and the receiving hospitals– Transportation officer will communicate with
the Resource Hospital how many reds, yellows and greens are being transported and to where
– The Resource Hospital will contact the appropriate receiving hospital with ETA

Class 2 Patient Disposition• The Resource Hospital (ie: CMC) coordinates
transportation destinations for your patients– Condell will notify the closest hospitals to
determine the bed availability in the ED– Condell will notify the contact at the scene as to
how many and what category patients the different facilities can take
– Scene to inform Condell which ambulance is taking which patient(s) to where
– Condell to contact the receiving hospital with ETA
Communication Process – Class 3
• Contact your Resource Hospital– Advocate Condell– Think – Class 3 you are overwhelmed and need lots of
resources (ie: use your Resource Hospital)– You will most likely be setting up EMS divisions to help
at the scene
• Communication prompts:– “This is ___FD”– “We are on the scene of a Class 3 multiple patient
incident”– “We estimate the following types of patients ____ “
(provide number and color category of patients)– “My call back number is ____”
Class 3 Initial Information
• Information provided to the Resource Hospital (CMC)Event descriptionEstimated number of patientsEstimated patient acuities
• Use red, yellow, green colorsState who your closest hospitals are
• Hospitals most likely to receive patients

Field to Hospital Communication
• Class 3
– No contact is made between transporting ambulances and the receiving hospitals
– Field communication will be between one designated person at the scene and the Resource Hospital
– Call back number must be provided from the scene to the hospital

Class 3 Patient Disposition
• Resource Hospital coordinates transportation destination of patients
• Resource Hospital to communicate to the one contact at the scene how many of what type of patients go to which facilities
• The Resource Hospital will contact the appropriate receiving hospital(s) with ETA after obtaining this information from the scene (ie: Transportation)

Declaring a Multiple Patient Incident
• “Business as usual” is defined differently by every department
• It must be clear to all responding personnel what level of plan is being declared so response is uniform
• Declare the Class type and follow that plan– Unless all responding personnel are aware of
the class type declared, individuals will be following what they feel is proper, not necessarily what has been declared

Field Provider Log Form
• Use this form as a voice prompt to cover all initial information important to provide to the hospital
• The form is a worksheet and NOT part of the patient record
• All departments have been provided with this form
• Form should be forwarded to the Resource Hospital along with the After Action Report– Used for critique and PI purposes
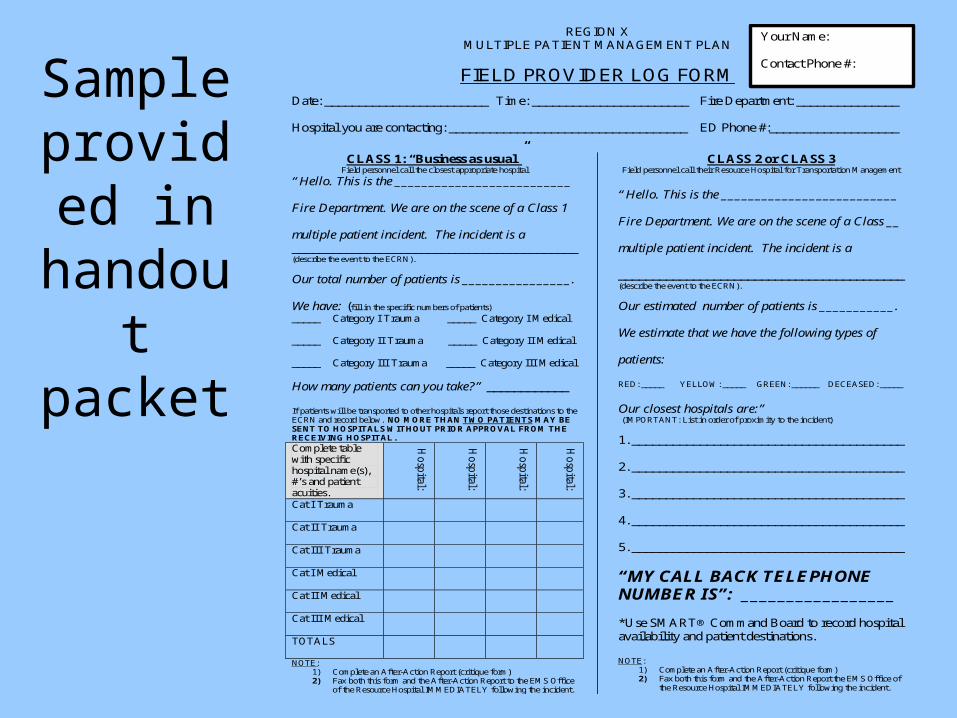
Sample provided
in handout packet
REGION X
MULTIPLE PATIENT MANAGEMENT PLAN
FIELD PROVIDER LOG FORM
Date: ________________________ Time: _______________________ Fire Department: _______________ Hospital you are contacting: ___________________________________ ED Phone #:___________________
CLASS 1: “Business as usual”
Field personnel call the closest appropriate hospital
“Hello. This is the __________________________ Fire Department. We are on the scene of a Class 1 multiple patient incident. The incident is a __________________________________________ (describe the event to the ECRN).
Our total number of patients is ________________. We have: (fill in the specific numbers of patients)
_____ Category I Trauma _____ Category I Medical _____ Category II Trauma _____ Category II Medical _____ Category III Trauma _____ Category III Medical How many patients can you take?” ____________ If patients will be transported to other hospitals report those destinations to the ECRN and record below. NO MORE THAN TWO PATIENTS MAY BE SENT TO HOSPITALS WITHOUT PRIOR APPROVAL FROM THE RECEIVING HOSPITAL.
Complete table with specific hospital name(s), #’s and patient acuities.
Ho
spital:
Ho
spital:
Ho
spital:
Ho
spital:
Cat I Trauma
Cat II Trauma
Cat III Trauma
Cat I Medical
Cat II Medical
Cat III Medical
TOTALS
NOTE: 1) Complete an After-Action Report (critique form) 2) Fax both this form and the After-Action Report to the EMS Office
of the Resource Hospital IMMEDIATELY following the incident.
CLASS 2 or CLASS 3 Field personnel call their Resource Hospital for Transportation Management
“Hello. This is the __________________________ Fire Department. We are on the scene of a Class __ multiple patient incident. The incident is a __________________________________________ (describe the event to the ECRN).
Our estimated number of patients is ___________. We estimate that we have the following types of patients: RED: _____ YELLOW: _____ GREEN: ______ DECEASED: _____
Our closest hospitals are:” (IMPORTANT: List in order of proximity to the incident)
1. ________________________________________ 2. ________________________________________ 3. ________________________________________ 4. ________________________________________ 5. ________________________________________
“MY CALL BACK TELEPHONE NUMBER IS”: _________________ *Use SMART® Command Board to record hospital availability and patient destinations. NOTE:
1) Complete an After-Action Report (critique form) 2) Fax both this form and the After-Action Report the EMS Office of
the Resource Hospital IMMEDIATELY following the incident.
Your Name: Contact Phone #:
Field Provider Log Form – Class 1 Communication Prompt
• EMS to call the closest appropriate hospital• Class 1: “Business as usual”• “Hello. This is ____FD. We are on the scene of a
Class 1 multiple patient incident. The incident is a __(describe the event to the ECRN)___. Our total number of patients is ___. We have (fill in the number of Category I, II, III trauma or medical patients).
• “How many patients can you take?”

Field Provider Log Form
• Space is provided in a table format for the field provider to record which hospital will take what number of patients
• Table information will assist in patient distribution
• Return this form with the After Action Report to the EMS office at CMC
Field Provider Log Form – Class 2 or 3 Incident
• EMS to call their Resource Hospital
• Class 2 – unable to meet normal level of care
• Class 3 – overwhelmingly unable to meet normal level of care
• “Hello.” This is ____FD. We are on the scene of a Class __ multiple patient incident. The incident is a _(describe event to the ECRN)_

Field Provider Log Form cont’d– Class 2 or 3 Incident
• “We estimate we have the following types of patients (number of red, yellow, green, deceased patients is given)”
• “Our closest hospitals are ____”• Provide the ECRN with a call back number• Use SMART command board to record hospital
availability and patient destinations• Return this form with the After Action Report to
the EMS office

Documentation – Class 1 Plan
• Triage tags NOT used
• Complete patient care reports as usual
• Class 1 is business as usual after-all
• The anticipation is that you will make only one transport run to the hospital

Documentation – Class 2 Plan
• Use triage tags– Fold appropriate color to show– Use tags to make “notes”
• Complete patient care reports as usual
• The anticipation is to transport only once from the scene
• If you are needed to return to the scene, do so as soon as possible and then write reports

Documentation – Class 3 Plan
• Use triage tags• NO patient care reports are
completed• Triage tags serve as the written report
• The anticipation is that you will be making several runs back and forth between the scene and receiving hospitals

After Action Report
• Form used to critique the process
• Submit the After Action Report with the Field Provider Log Form to your Resource Hospital EMS office
• The form requires a description of the incident and asks for a check-off of the type of incident with the total number of patients involved
After Action Report Questions
• Which hospital was contacted?• Mode of communication used?• Difficulties with communication?• Difficulties in declaring which incident to
declare?• Difficulties with triage?• Difficulties with patient disbursement?• What references or forms were used?• How effective was the plan in patient
disbursement?
START Triage
• Simple Triage and Rapid Transport• A color coding system used in triage to
communicate priorities• Smart tag used to communicate by sight
the triage color• Red – immediate priority• Yellow – urgent priority• Green – delayed priority• Black – deceased or soon to be
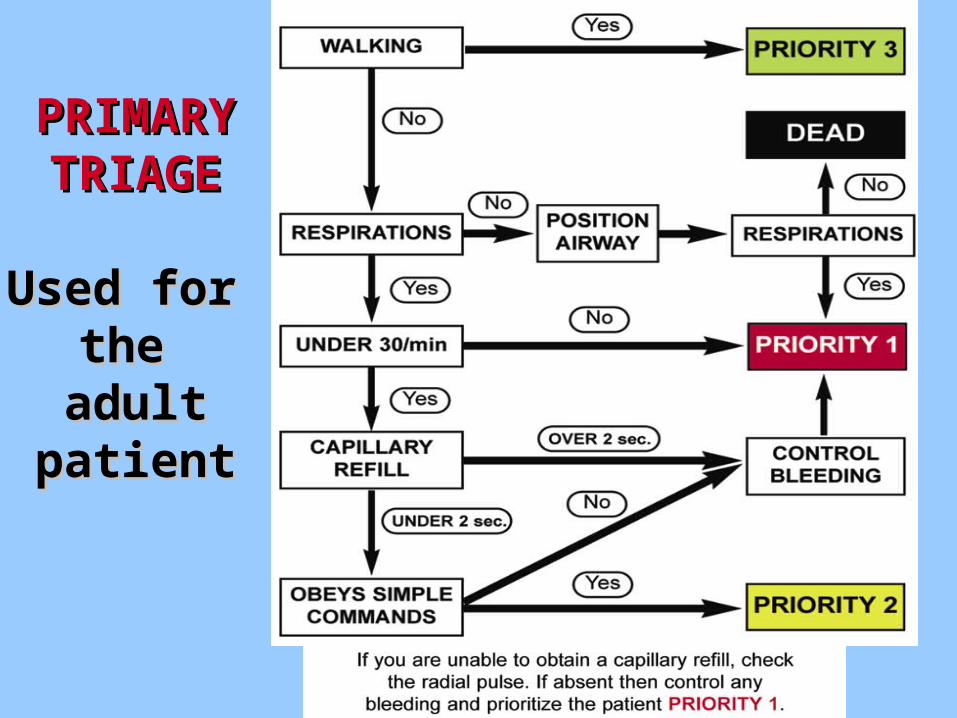
Primary Triage - Adults
• Primary triage must be:– Dynamic providing the ability to reassess
• Some patients get better, some worse– Safe– Fast– Reproducible
• Every person who assesses the same patient needs to be making a decision based on identical criteria
• Need the ability to upgrade and downgrade injured people throughout the process
Primary Triage - Walking• There is NO time for head-to-toe assessments in
this first evaluation• First step
– “Can you walk?”• People who are walking have an airway and
adequate respiratory and circulatory systems to be upright and walking
• These patients have a wide range of injuries and some could be potentially life-threatening
• If the patient can walk to another area, consider them as Priority 3 – GREEN for now
– All patients deserve constant reassessment and may need to be moved to another triage level
Primary Triage - Respirations
• If the patient cannot walk to another area, then move on to evaluation of respirations
• If the airway needs to be opened, provide chin lift with jaw thrust.
• If the patient does not breathe with this maneuver, they are BLACK / dead
• If the airway needs to be maintained with the maneuver, try to recruit a bystander / other less injured person
• If respirations can be maintained, patient tagged Priority 1 - RED
Primary Triage - Respirations
• For patients who can breath, assess for the rate of respirations– Respiratory rate >30 tagged Priority 1 –
RED– Respiratory rate < 30 move on to
circulation assessment• Once the patient is determined to be any
priority / color, the triage process is done for now and move onto the next patient
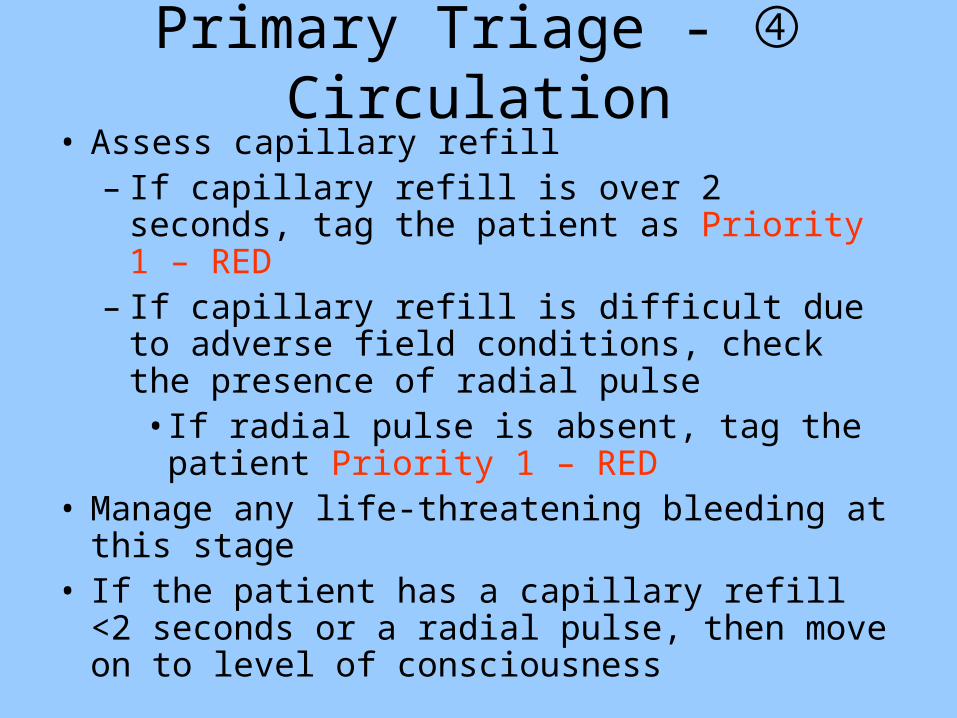
Primary Triage - Circulation• Assess capillary refill
– If capillary refill is over 2 seconds, tag the patient as Priority 1 – RED
– If capillary refill is difficult due to adverse field conditions, check the presence of radial pulse• If radial pulse is absent, tag the patient
Priority 1 – RED• Manage any life-threatening bleeding at this
stage• If the patient has a capillary refill <2 seconds or
a radial pulse, then move on to level of consciousness

Primary Triage – Level of Consciousness
• If the patient cannot obey simple commands, they are tagged as Priority 1 – Red– Simple command could be response to “what
is your name” or “raise your arm”
• If the patient can obey simple commands, they are tagged Priority 2 – Yellow– Patients will/should be retriaged with the
secondary triage to again determine the category they will be in
PRIMARY PRIMARY TRIAGETRIAGE
Used for Used for the the
adultadultpatientpatient
JumpSTART Pediatric Triage
• Children are not small adults
• An adult system will not be accurate for children
• A child’s length is proportional to their physiology– A child at 8 years-old becomes physiologically
similar to the adult
• Pediatric triage has to satisfy the same criteria as the adult: dynamic, fast, safe, and reproducible

PEDIATRIC PEDIATRIC TRIAGETRIAGE
JumpSTARTJumpSTART
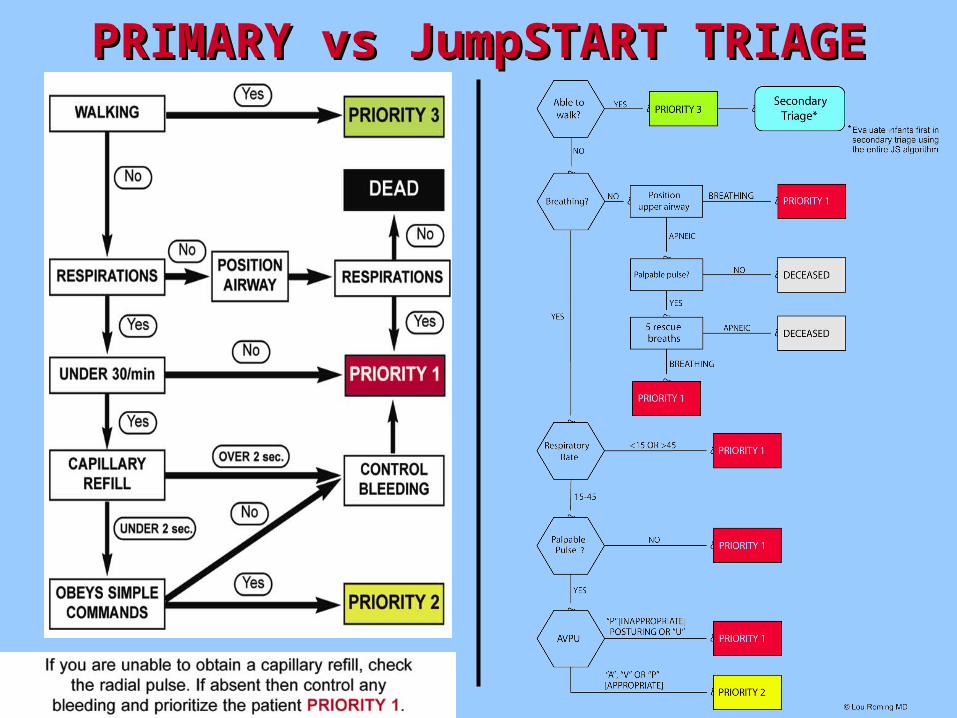
PRIMARY vs JumpSTART TRIAGEPRIMARY vs JumpSTART TRIAGE
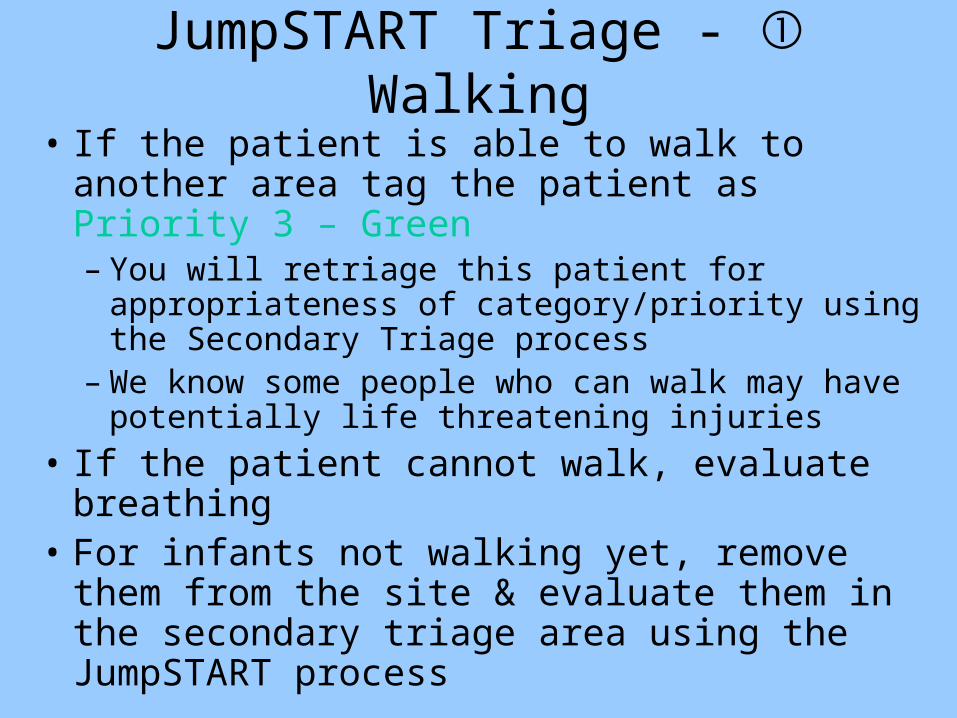
JumpSTART Triage - Walking
• If the patient is able to walk to another area tag the patient as Priority 3 – Green– You will retriage this patient for appropriateness
of category/priority using the Secondary Triage process
– We know some people who can walk may have potentially life threatening injuries
• If the patient cannot walk, evaluate breathing• For infants not walking yet, remove them
from the site & evaluate them in the secondary triage area using the JumpSTART process

• If the patient is NOT breathing, open the airway– If the patient begins to breath, tag them
Priority 1 – RED– If the patient is apneic, check for a palpable
pulse• If no pulse, tag them BLACK – dead• If they have a palpable pulse, give 5 rescue
breaths–If the patient begins to breath, tag them
Priority 1 – RED–If no breathing, tag the patient BLACK
JumpSTART Triage - Breathing

JumpSTART Triage – Respiratory Rate
• If the patient is breathing, check the rate
– If the rate is < 15 or > 45, tag them Priority 1 – RED
– If the rate is between 15 and 45, check for a palpable pulse

JumpSTART Triage - Pulses
• If there is no palpable pulse with the breathing patient, tag them Priority 1 – RED
• If there is a palpable pulse with the breathing patient, evaluate their level of consciousness (ie: AVPU)
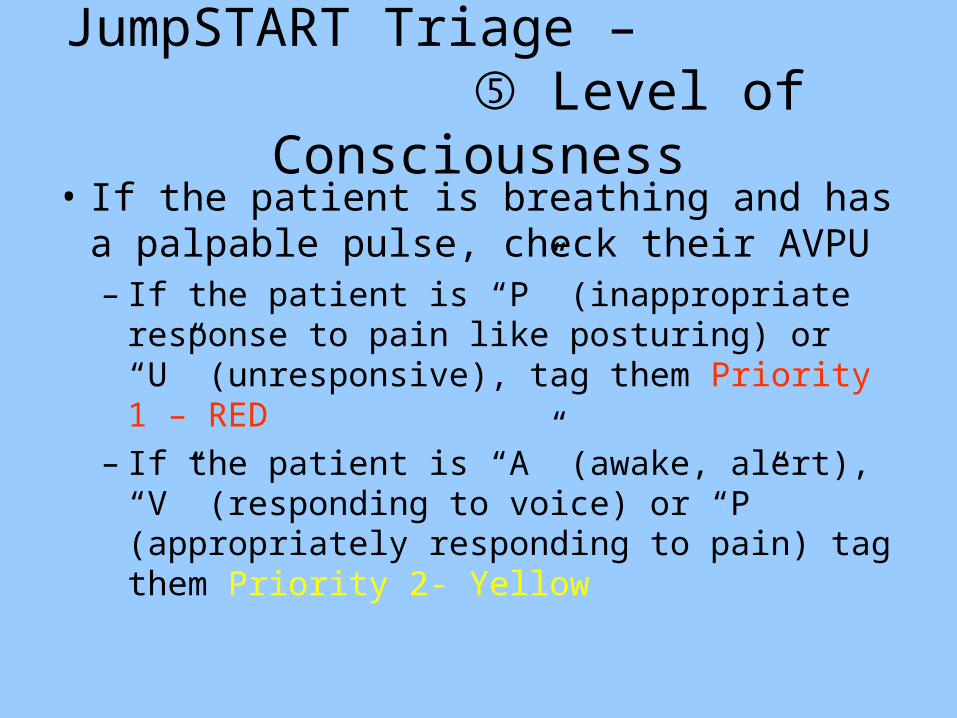
JumpSTART Triage – Level of Consciousness
• If the patient is breathing and has a palpable pulse, check their AVPU– If the patient is “P” (inappropriate response to
pain like posturing) or “U” (unresponsive), tag them Priority 1 – RED
– If the patient is “A” (awake, alert), “V” (responding to voice) or “P” (appropriately responding to pain) tag them Priority 2- Yellow

Secondary Triage• Used to assist in getting the patient to the right
place in the right time• Secondary triage refines the initial clinical picture
of patient sorting• Primary triage just started segregating patients
into groups– Getting those that can to walk to another area
lessens that amount of patients your staff has to walk through while looking for the most serious injuries
• Performed to place patient in correct treatment zone (ie: RED, YELLOW, GREEN, BLACK)

Secondary Triage
• Uses a refined physiological scoring system and anatomical examination– Glasgow coma scale
• Best eye opening• Best verbal response• Best motor response
– Vital signs• Respiratory rate• Systolic blood pressure

SECONDARSECONDARY TRIAGEY TRIAGE
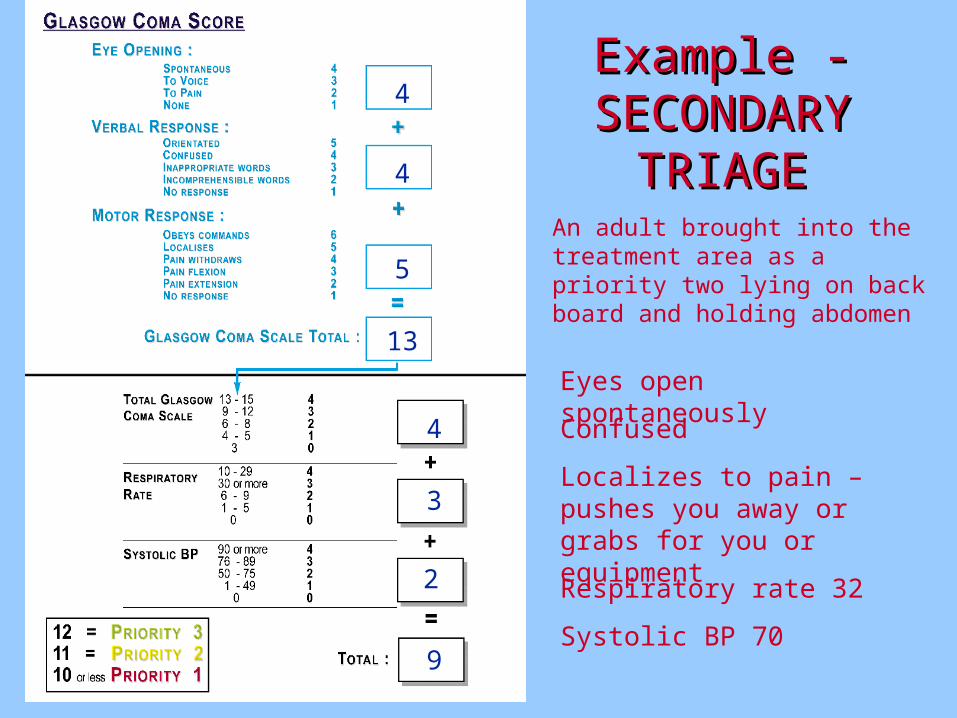
Example - Example - SECONDARY SECONDARY
TRIAGETRIAGEAn adult brought into the treatment area as a priority two lying on back board and holding abdomen
Eyes open spontaneously
Confused
Localizes to pain – pushes you away or grabs for you or equipment
4
4
5
13
4
Respiratory rate 32
3
2
Systolic BP 709
Secondary Triage Practice
• Review the following cases and using your handout, score these patients.
• First step is to calculate the Glasgow coma scale
• Then convert the 3-15 score to 0-4 points• Score the respiratory rate• Score the systolic blood pressure• Add the converted GCS, RR, and systolic
B/P to get the secondary triage score

Secondary Triage Practice
• Pt #1 - adult looking around, confused, grabbing at equipment. RR 26; B/P 108/60
• Pt #2 - adult; eyes open when their name is called; yells out occasional words but not appropriate to the situation, withdraws/pulls back extremities when touched. RR 18; B/P 114/72
• Pt #3 - adult; eyelids flicker when earlobe is pinched; mumbles incomprehensibly; withdraws to pain. RR 6; B/P 84/54
Secondary Triage cont’d
• Pt #4 – child; looking around; answers all questions, moves all extremities and assists with care provided. RR 24; B/P 92/68.
• Pt #5 – infant; watching those around them, crying for their mother, moves all extremities and tries to pull away when you provide care (normal response). RR 28, B/P 88/50
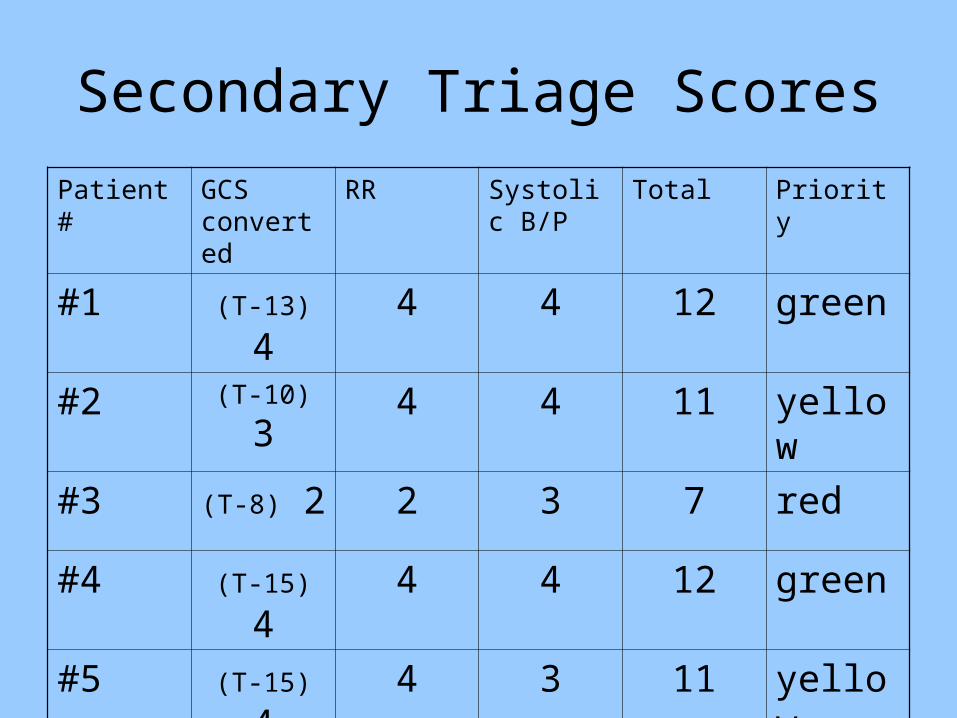
Secondary Triage Scores
Patient # GCS converted
RR Systolic B/P
Total Priority
#1 (T-13) 4 4 4 12 green
#2 (T-10) 3 4 4 11 yellow
#3 (T-8) 2 2 3 7 red
#4 (T-15) 4 4 4 12 green
#5 (T-15) 4 4 3 11 yellow

SMART MCI BAG™SMART MCI BAG™
• Purpose– To assist the operational management
personnel on the scene– Compact and mobile– Provides a command
board for fluid documentation
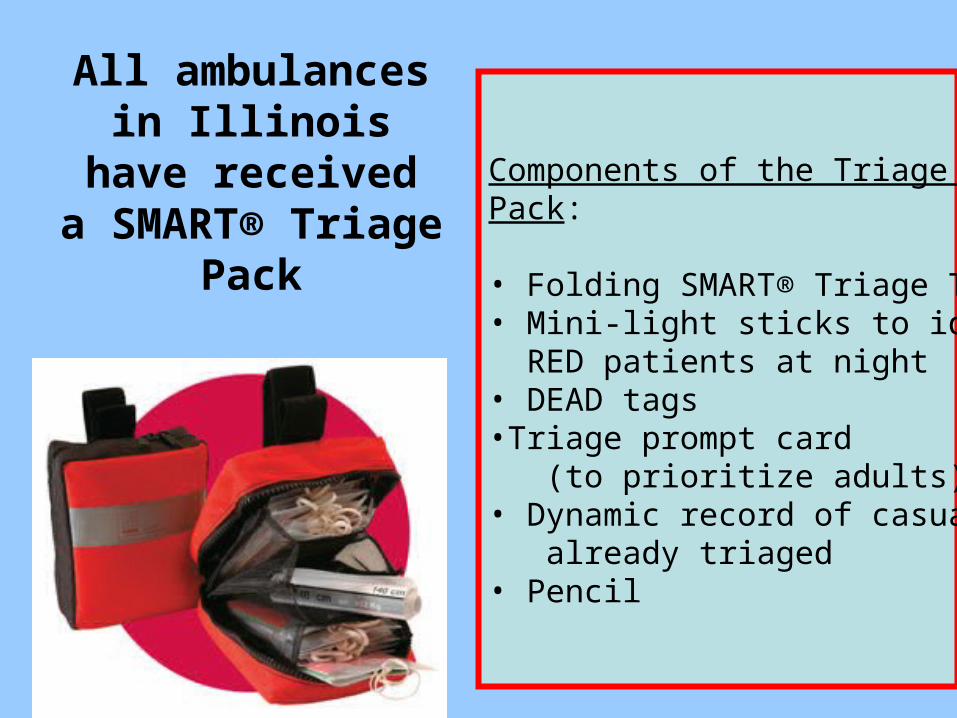
All ambulances in Illinois have
receiveda SMART® Triage
Pack
Components of the Triage Pack:
• Folding SMART® Triage Tags• Mini-light sticks to identify RED patients at night• DEAD tags•Triage prompt card (to prioritize adults)• Dynamic record of casualties already triaged• Pencil

The State of Illinois has adopted the START triage method in partnership with the SMART® Incident
Command System as a state-wide standard
SMART® Tags to be used when
doing START Triage
Use SMART tags forClass 2 and Class 3
Incidents
Refold tags as needed if the
patient conditionchanges
Forms
• During the incident use the “Field Provider Log Form”– Provides prompts for hospital communication
• After the incident, individually or as a group, complete the “After Action Report”– Provides a critique opportunity
• Return both forms to the EMS Resource Hospital as soon as possible

CISM
• We all need to monitor our peers for evidence of traumatic stress– One event stressful for one person may not be
stressful for another responder
• Purpose of CISM– To provide psychological first aid and management of
traumatic stress for those affected by the event – Signs and symptoms of traumatic stress may not
develop for up to 2 months after the event
• Staff may need to be rotated through rehabilitation periodically throughout a long term response

Components of Psychological First Aid
• Listening• Conveying compassion• Assessing needs• Making sure basic needs are met• Not forcing persons to talk• Providing support to family/significant
others• Encouraging, not forcing, social support• Protecting from additional harm

CISD Activation
• Any member of the Condell Medical Center EMS System is authorized to contact CISM resources
For CISD, contact
1-800-225-2473
Scenario Practice
• For the following scenarios, run the call as you would normally respond from your station
• All members of the department should be involved– The 2-3 responding personnel will need to
initiate a plan of action– When others respond from the station to take
over command, everyone needs to function with the same guidelines and definitions
Two autos have been involved in a head-on crash. Each autowas traveling in excess of 60 mph. Three people have been thrown from the wreckage and are unconscious.
Four others are trapped inside with various types of severe injuries.
What Class?What Category trauma?
Which hospital do you contact?What do you say?
How does this affect the transporting ambulances?
The administrator at a private school calls 911 to reportthat a strange odor in the building has caused several
students to collapse. Someone has pulled the firealarm to evacuate the building.
As you arrive, students are running towards you.
What Class?What Category medical?
Which hospital do you contact?What do you say?
How does this affect the transporting ambulances?
What Class?What Category trauma?
Which hospital do you contact?What do you say?
How does this affect the transporting ambulances?
Two patients were in this car.
One patient is in traumatic arrest.
One patient is unresponsive but
breathing.
What Class?What Category trauma?
Which hospital do you contact?What do you say?
How does this affect the transporting ambulances?
Four teenagers have stolen this vehicle and hit the building
at a moderate rate of speed.
Upon your arrival, all victims are sitting
on the curb with minor injuries and in police custody.

What Class?What Category medical?
Which hospital do you contact?What do you say?
How does this affect the transporting ambulances?
Five members of a familywere rescued from this home.
All five are exhibiting signs of severe smoke inhalation.
What Class?Which hospital do you contact?
What do you say?How does this affect the transporting
ambulances?
This accident involvesa total of five patients:
2 Category I Trauma Patients3 Category II Trauma Patients

What Class?Which hospital do you contact?
What do you say?How does this affect the transporting
ambulances?
This crash involves four vehicles.
Category I = 3 patientsCategory II = 1Category III = 2
What Class?Which hospital do you contact?
What do you say?How does this affect the transporting
ambulances?
A car traveling at 60 mphhas hit a group of seven
bicycle riders. The bikes weretraveling at a high rate of speed.
The victims include:6 Category One Trauma Patients1 Category Two Trauma Patient

Bibliography
• Bledsoe, B. Porter, R., Cherry, R. Paramedic Care Principles and Practices.
• Region X Multiple Patient Management Plan, 2009.
• Region X SOP’s. March 2007, Amended January 1, 2008
• Smartmci.com (TSG Associates Ltd 2004 -2008.)


















