Successes & challenges of multi sectoral - CNM.gov.kh
36
SUCCESSES AND CHALLENGES OF MULTI SECTORAL AND INTERNATIONAL COLLABORATION FOR MALARIA CONTROL AND ELIMINATION EXAMPLES IN CAMBODIA Dr Char Meng Chuor, Director, National Center for Malaria Control Parasitology and Entomology (CNM), Cambodia 1 Presentation for the Sub-TWGH for CNM, 8 Oct 2013, Phnom Penh
Transcript of Successes & challenges of multi sectoral - CNM.gov.kh
SUCCESSES AND CHALLENGES OF MULTI SECTORAL AND INTERNATIONAL COLLABORATION FOR
MALARIA CONTROL AND ELIMINATION EXAMPLES IN CAMBODIADr Char Meng Chuor,
Director, National Center for Malaria Control Parasitology and Entomology (CNM), Cambodia
1
Presentation for the Sub-TWGH for CNM, 8 Oct 2013, Phnom Penh

Outline
I. Background information
II. Collaboration with inter-ministerial
III. Collaboration with Development Partners (DPs)
IV. Selected Examples of Successful stories
V. Lessons Learnt
VI. On-going Constraint s and Challenges
2

I-Background: Endemic Areas• Population: 14.3 million• Permanent resident of malaria endemic areas: 3.3 million• Cambodia Forest Map almost coincides with Malaria Map
3
• Malaria specific incidence rate among male adult is around 5 times higher than that of
women/children
• Mobile migrant workers are mainly exposed
• 50% of malaria patient treated in Thai provinces bordered with Cambodia are Cambodian
migrant workers
FORESTRY Map Malaria Endemic Map

4
I. Background: Plasmodium species (Blood Slides by Public Facilities)
2005: The worst drought to hit Cambodia in 50 years (Ref.: www.orientexpat.com/forum/1813)

I. Background: Change malaria morbidity/mortality(Progress toward MDG 2015)
5

6
TF/DHP: 2008(6.4%); 2009(8.1%) 2010(21.4%)
TF/A+M2002 (13.8%) 2004(9.9%) 2011(0%) 2012(0%)
TF/DHP: 2012(19% -31%)
DHP: Dihydroartemisinin 40mg + piperaquine 320 m. A+M: Artesunate 50 mg + mefloquine 250 mData for 2013 are not completely verified except Ouddar Meanchey
TF/DHP: 2009(2.5%) 2013(40% confirmed by PCR)
2013DHP(14.7%)
TF/DHP: 2010(0%)
TF/DHP: 2013: 0%
???
???
???
???
???
TF/DHP: 2012(0%)
???
TF/DHP: 2012(0%)
???
TF/DHP: 2008(0%); 2010(0%)2011(9.5%) 2012(8.7%)2013(31.9%)
???
Pf Resistance:
Are we punished
by our success?
Atovaquone + Proguanil: 2013(Emerging of pfcybbut uncertain about proguanil)
TF for Atovaquone+ Proguanil: 2008(0%.)
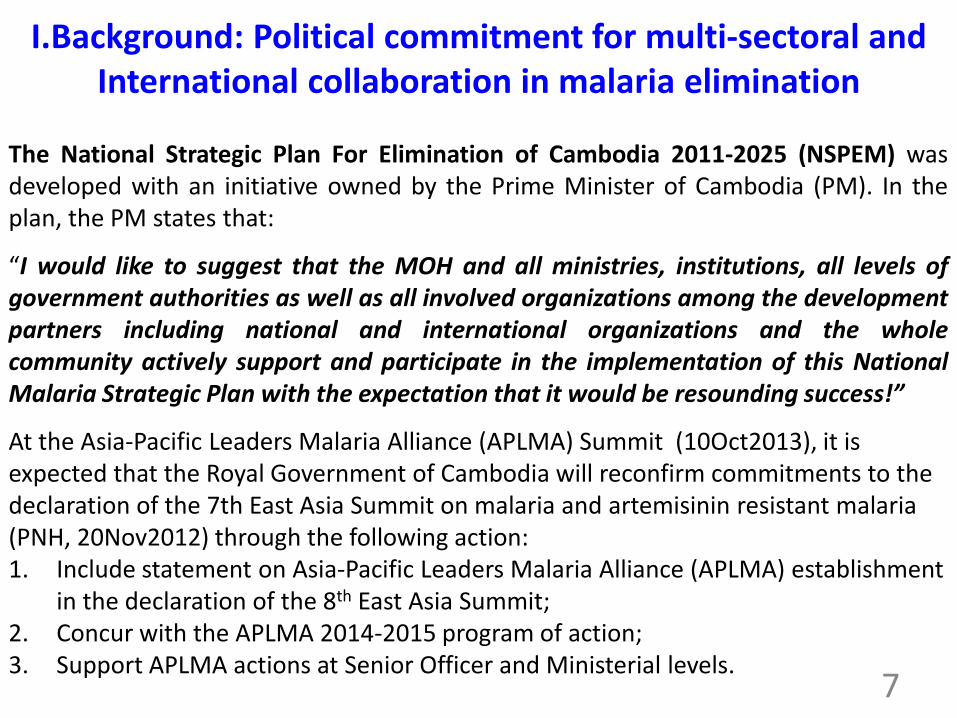
I.Background: Political commitment for multi-sectoral and International collaboration in malaria elimination
The National Strategic Plan For Elimination of Cambodia 2011-2025 (NSPEM) wasdeveloped with an initiative owned by the Prime Minister of Cambodia (PM). In theplan, the PM states that:
“I would like to suggest that the MOH and all ministries, institutions, all levels ofgovernment authorities as well as all involved organizations among the developmentpartners including national and international organizations and the wholecommunity actively support and participate in the implementation of this NationalMalaria Strategic Plan with the expectation that it would be resounding success!”
At the Asia-Pacific Leaders Malaria Alliance (APLMA) Summit (10Oct2013), it is expected that the Royal Government of Cambodia will reconfirm commitments to the declaration of the 7th East Asia Summit on malaria and artemisinin resistant malaria (PNH, 20Nov2012) through the following action:1. Include statement on Asia-Pacific Leaders Malaria Alliance (APLMA) establishment
in the declaration of the 8th East Asia Summit;2. Concur with the APLMA 2014-2015 program of action;3. Support APLMA actions at Senior Officer and Ministerial levels.
7

• Government established Technical Working Group (TWG) for each sector as Monthly
Forum for coordination with relevant development partners. The TWG in health (TWGH)
is co-chaired by MOH and WHO
• The TWGH established its Sub-TWG for CNM and for PPP with CNM as a
representative: most recently, the outstanding subjects in its meeting agenda are
mainly malaria initiatives.
• The NSPEM indicates that all activities will be attained through collaborative inter-sectoral efforts to benefit from each entity’s strengths.
• The Provincial Task Force for Malaria Elimination (PTME) for each province was
established in according with NSPEM and within the context of decentralization & de-
concentration of power from central ministries to local governor and commune
council). PTME is leaded by a representative from the Provincial Governor and
supported by a secretariat based at the provincial health department. Other members
come from relevant entities including government agencies and civil societies.
I. Background: Framework and institutional arrangement for multi-sectoral Collaboration
8

II-Examples in Collaboration Inter-Ministerial
• Ministry of Defence: Malaria Prevention and Treatment to military at malaria
risk area as specially at the border
• Ministry of Interior:
– Malaria Prevention and Treatment to police at malaria risk area as
specially at the border(Department of health)
– Collaboration between anti economic crime Police & Drug Inspector
to Control Counterfeit & Artemisinin Monotherapies Drugs
• Ministry of Women Affair: Malaria education to women in target risk malaria
• Ministry of Education, Youth and sport(MoYS): School Health Education, …
• Ministry of Economic and Finance (MoEF): Payment for taxes/duties,
Member Cambodia Malaria Containment task force,
• Ministry of Commerce: Member Cambodia Malaria Containment task force
• MOP/NIS: Dissemination data determinant of health 9
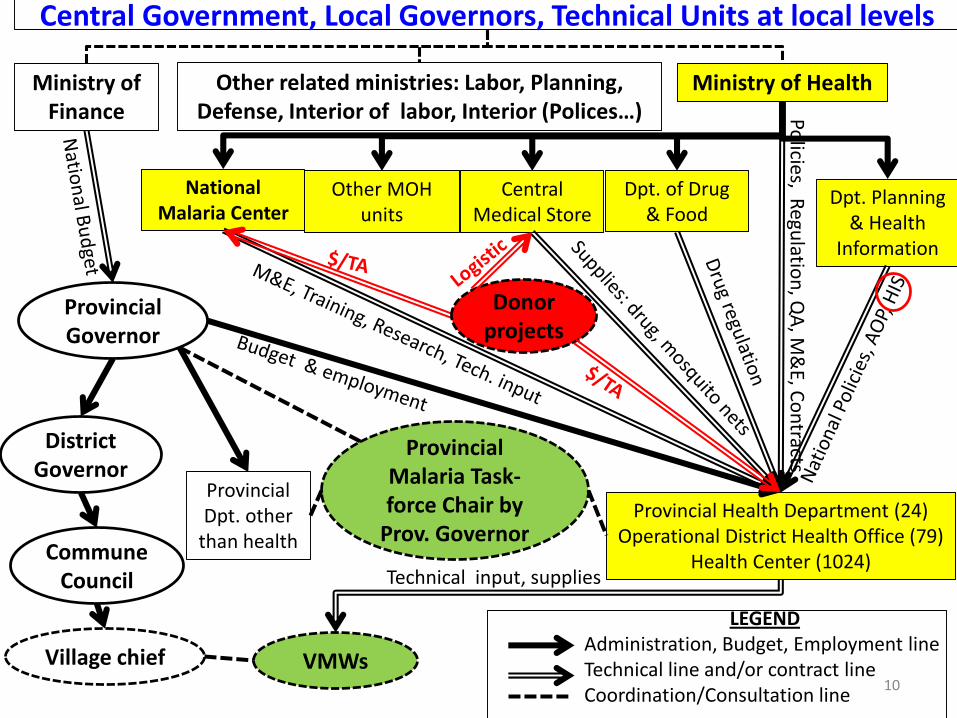
Central Government, Local Governors, Technical Units at local levels
Ministry of Health
National Malaria Center
Central Medical Store
Dpt. of Drug & Food
Dpt. Planning & Health
Information
Ministry of Finance
Other related ministries: Labor, Planning, Defense, Interior of labor, Interior (Polices…)
Provincial Health Department (24)Operational District Health Office (79)
Health Center (1024)
Provincial Governor
Policies, R
egulatio
n, Q
A, M
&E, C
on
tracts
District Governor
Commune Council
Provincial Dpt. other
than health
Provincial Malaria Task-force Chair by
Prov. Governor
Village chief VMWs
Technical input, supplies
Other MOH units
LEGENDAdministration, Budget, Employment lineTechnical line and/or contract lineCoordination/Consultation line
10
Donor projects

III-Government and Development Partners (Donors, NGOs…)An Example: Relation between CNM and
the Department of Planning and Health Information (DPHI)
11
• User of DPHI Website (Data uploaded by ODs, selected NGOs & Private Providers
• Strategic advocacy to PHD/OD during AOP process
DPHIEstablish AOP
& HIS
Other National Centers
PHD
ODs & Health Centers
CNM in charge of 3 National Programs:
Dengue, Malaria, NTDs)
Consensus on Designing AOP/HIS processes
(Training, Supervision and mentoring in AOP/HIS and Equity Fund)
(Training, Supervision and mentoring in AOP/HIS and Equity Fund)
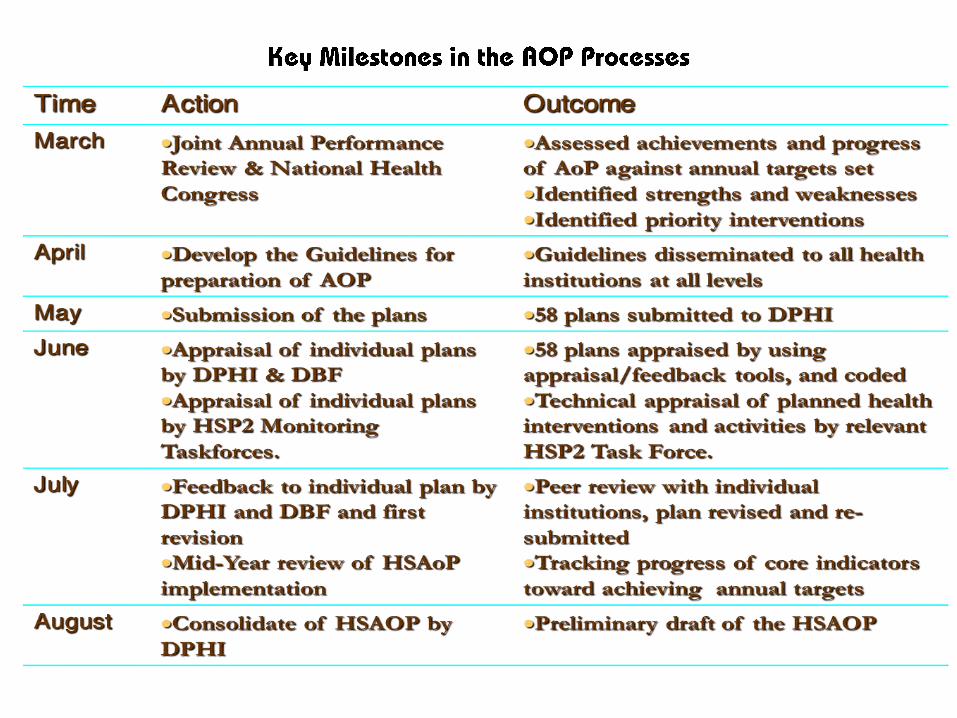

A FORMAT FOR Annual Operational Plan

III-Government and Development Partners (Donors, NGOs…)EVOLVING CNM FUNCTIONS DECENTRALIZATION/DE-CONCENTRATION
14
• Endorsed by MOH 23 Oct 2012 (www.cnm.gov.kh/userfiles/file/CNM%20Structure%20and%20Fuction.pdf)
• Several functions being progressively decentralized to sub-national levels.
• CNM has no direct authority for planning/financing of its national programmes at sub-national levels.
• The DPHI leads the sector Planning & M&E process for land guides sub-national health units during the
entire process including formulation of Annual Operational Plans (AOPs).
• The PHC functions including treatment and prevention for malaria, dengue and helminthiasis involving
activites such as bednet/abate distributions, antihelminthic drug distribution, diagnosis and treatment by
VMWs, etc.), are in the process of being decentralised to sub-national units…
• Eg.: Under ADB/CDC2 and HSSP2 CNM has had no authority in PHD/OD financial management
• Direct transfer of authorities in human, financial, logistic and other appropriate resources (except
procurement of health products and pharmaceuticals which will be undertaken through the MOH
national budget) to the district and commune councils with decision making and implementation resting
with these entities.
• CNM inputs will be limited to setting the direction for priority interventions to be delivered at each level of
the health system, but it will have no mandate in actual resource allocation to the implementing
agencies.
• Bottom-up planning including formulation of AOPs at every level of implementation will be encouraged
and nurtured over the next several years during which CNM will provide guidance for prioritisation and
actual implementation.

Our explicit open door policies
• Funding arrangements in the health sector “open” for both partners who wish
to join pool funding and those not wishing to join pool funding (MOH Official Letter
to DPs, 23 Mar 2007)
• MOH/CNM ownership in term of policies, strategies, technical protocols,
coordination
Building and maintaining trust in Partnership
• Having confidence in one another, that each partner will do what they say they will do, and
mean what they say.
• Each partners (Donors, Government…) has their own agendas, cultural values and ethics,
but they should find agreed code of conduct and specific partnership Rules
• To sustain and maintain trust and goodwill, it is essential to put in place agreed mechanisms
to support accountability, transparency of decision making, information and reporting, audit
evaluation and so on
III-Government and Development Partners (Donors, NGOs…)
15
• GFATM & B&MGF: Main source of funding since 2003
• WHO : Back-bone in Technical Expertise and Coordination Mediator
• Press/Media: Sensitization of support, mass media campaign
• Malaria Consortium (MC): General BCC, M&E, consultancies
• URC/USAID: CAP Malaria 2011-2016
• FHI360: Community Participation
• CHAI, PATH, USP-US/USAID: Public Private Partnerships
• PSI has worked on social marketing of nets, diagnostics and ACTs since 2002.Currently in process of targeting specifically mobile migrant workers
• AMDA, HPA, PFD: Community Participation
• WMC , BBC Trust: Mass Media for increase awareness about malaria
• AFRIMS, IPC, MORU, NAMRU, NIH, LSHTM : Malaria research
III-Government and Development Partners (Donors, NGOs…)
16
IV. SELECTED SUCCESSFUL STORIES
1.Containment Artemisinine Resistance (B&MGF/WHO)
2.Carrot and Sticks synergy in PPP: Ban of Oral ArtemisininMono-Therapie & Subsidizing of supplies for malaria activities
5.Participation in regional collaboration
3.Community participation: Villages Malaria Workers
6.The outcome: Progress towards the MDG2015
4.Working with media agencies, TV/Radio, Journalist
17

Locations of Artemisinin Resistance Containment Zones
28
17
6 4 10
5
10
15
20
25
30
2008 2009 2010 2011 2012
Nu
mb
er o
f ca
se
Year
Malaria mortality in Containment Z1(2008 to 2012)
Source : HIS
1.Containment Artemisinine Resistance
18

4.4%
2.6%
0.9%
0.5%
1.3%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
CMS 2004 CMS 2007 CMS 2010
Pre
vale
nce
of
po
siti
ve b
loo
d s
lides
Cambodia Malaria Surveys 2004-2010: Prevalence of Malaria-positive Slides
Total
Domain 1 (10 containment provinces)
Domain 2 (10 other at-risk provinces)
19

MOH Official letter on Ban of Arthemisinin Mono-Therapies.
MOH justice police force with uniform dress & basictraining. Visits by these have been made duringwhich AMTs were confiscated and destroyed (200justice police in zone 1).
GFATM support t hrough AMFm has providedsupport to the Anti-Economic-Crime Police.
418 Police have been trained to identify andinvestigate counterfeit anti-malarials and enforceban on oral AMT.
2.Carrot and Sticks synergy in PPPThe stick: Ban of oral Arteminisin Mono-Therapie (AMT)
20

Ministry of Interior and CNM staff conducted field visits tokey provinces and border check points to discuss proposedaction plans and encourage collaboration with localauthorities.
INTERPOL, which played a major role in tracking downproducers of fake antimalarials, still collaborates with thepolice
CNM still finds Artemisinine Monotherapie occasionally bymystery clients, a method worth continuing.
The regulatory agency for drugs and foods, DDF, has thepower to revoke licenses; it undertakes extensive inspections,not only for antimalarials
Registration cannot be proceeded without CNM advice; andrecently, MOH accepted request for registration of Anti-malaria drug by CNM only
The Stick: Artemisinin Mono-Therapy (AMT) ban in private sector
21

The carrot: PSI Subsidizes ACT/RDT for Private Sector to deliver Public Health
Fever diagnosis and malaria case management
page 22

1. Can Test for
malaria
2. Can Treat simple malaria
3. Should Refer ChildU5, PW
& severe
malaria cases
With ACT/RDT at subsidized price, Private Providers:
23

Constant ACT & RDT Supplies Vital !
9 mo.stock out
0
50,000
100,000
150,000
200,000
250,000
300,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
0
100,000
200,000
300,000
400,000
500,000
600,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
6 mo.stockou
t + panic
buying
7 mo.stock out
Dry year
24

Case management is a package of services not simply a commodity
Accessible quality drugs & testsResponsible providersInformed patients
10 yearsNational
25

Annual Early Diagnosis & TreatmentTraining for Private Providers
2012: 1,854 providers + 1,550 graduate nursing students
page 26

Market Share of Drugs in the Public and Private SectorsCambodia, 2009 and 2011
Source: PSI ACTwatch Outlet Survey 2011 27

Public & Private Approaches working together (PSI)
Free Net Campaigns
Net Markets
39% people said they bought their net from the market38% said they received their net from the Government/NGO [1]
&
[1] n= 22,528 Households: 2009 Household Survey
PSI bundled 70% of 1 Million Nets imported into Cambodia annually for 3 years with free net retreatment kits.
28
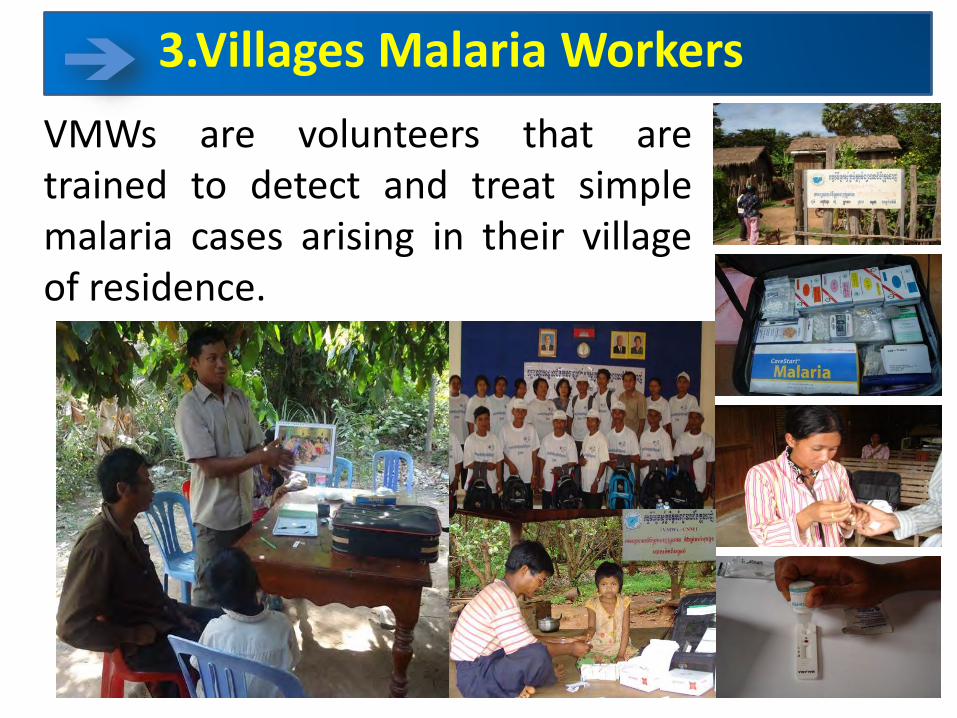
VMWs are volunteers that aretrained to detect and treat simplemalaria cases arising in their villageof residence.
3.Villages Malaria Workers
29

VILLAGE MALARIA WORKERS ACTIVITIES• Directly
Observed Treatment (DOT)
• DOTs expansion nationwide needs increase number of VMW from 3000 in 2012 to 8000 in 2015.
30

• Year 2012,VMWs conducted 106,032 RDT tests and 29,039 were positive. Malaria deaths in target VMW villages Zero
• Year 2011,VMW conducted 138070 RDT test and 48,750 were positive. Malaria deaths in target VMW villages: 2 .
• Positive cases decreased by 40% and deaths decreased by 100%
Trend of malaria mortality rate per 100,000 populationin VMW target vs Health Facilities data (HIS) ,2004-2012
Source: HIS and VMW
31

4. Examples: Working with TV/Radio, Journal reporters.
During the past three years i.e. after the Prime Minister launched the National Elimination Strategy 2011-2025, malaria became one of the outstanding news/stories told by TV/Radio and journal
Freedom of disclosed of information on malaria intervention also attracted participation of media agencies.
It was observed that CNM Website is not necessary a best source of news for media agencies as they always want hotline direct interface with program managers
Regular updating of malaria to selected journal/TV reporters prior to hotline direct interviews.
Key messages oftently broadcasted free of charge by TV/Radio and journal are about how many victim? When? When? What MOH did to addressed to problem? And how to prevent innfection/death?
A 24mn TV spot on malaria is being produced by CNC. Production and broadcast are free of charge 32

5. Cambodia participation to regional Collaborations
Cambodia adopted the Declaration of the 7th East Asia Summit on Regional Responses to malaria Control and Addressing Resistance to Antimalarial Medicines (PNH, 20 Nov 2012)
As part of regional approaches, PMI/USAID/CAP-M project strengthens cross-border collaborations through “Twin-City” along the border areas with the outstanding achievements: regular cross border meeting, joint world malaria day, shared update malaria information, exchange field visits, deploy bi-lingual IEC/BCC materials, and use bi-lingual patient card to reinforce treatment compliance.
Map health facilities and VMWs/MMWs both sides of the border to ensure/facilitate accessibility of migrant workers.
Cambodia is regional hub in the WHO’s Framework for the "Emergency Response to Arteminisin Resistance in the GMS”
It is expect that Cambodia get benefit from the GFATM’s RAI
33

V-Lessons learned• Foundation for success in multi-sectoral intervention Strong Political
commitment with government lead processes.
• Mechanism for regular updating of malaria event/situation attractedparticipation of media sector (TV/Radio, Journal) in broadcast ofcorrect information on prevention, treatment and multi-sectoral efforts.
• Rationalized district health system: The health coverage plan withintegration of basic services at frontline of public health services.
• Empowering Community can help expand service coverage at anacceptable quality (VMWs)
• Motivation of health workers in public and community
• Concrete synergy of the combined “carrot and sticks” approaches inPublic Private Partnerships
• Building and maintaining “trust” may minimize procedures that may “killproject objectives”
• Constant ACT & RDT Supplies is Vital but simply commodity alone is notenough to support a package of services in case management 34

Technical issues on identification and tracking movement of migrants and mobile workers seeking employment in endemic areas in or outside Cambodia are difficult
Cambodia Pf ability in adaptation to any new anti-malaria drug
since 1950s: Chloroquine, Sulfadoxine-Pyrimethamine, Arteminsinine. Recently TF rate in “40%” Oddar Meanchey
Proportion of Pv in being increased while prevalence of G6PD in Cambodia has been maintaining at around 22% since 1960s including severe deficiency prevalence recently estimated at around 8.2%.
Difficulty in maintaining the quality of health services to be delivered by VMWs when there is less and less malaria patient in each villages.
Limited ability in interface with media (TV/Radio, Journal…)
VI-We are exploring approaches to overcome the following Constraint/Challenge:
35

Next Step?
36