
Subtle overlapping deletions in the terminal region of chromosome 6q24.2-q26: Three cases studied...
6
Subtle Overlapping Deletions in the Terminal Region of Chromosome 6q24.2-q26: Three Cases Studied Using FISH S. Sukumar, 1 S. Wang, 1 K. Hoang, 1 C.M. Vanchiere, 2 K. England, 3 R. Fick, 4 B. Pagon , 5 and K.S. Reddy 1 * 1 Cytogenetics Department, Quest Diagnostics Inc., San Juan Capistrano, California 2 Childrens Clinic of Southwest Louisiana, Lake Charles, Louisiana 3 Casa Blanca Clinic, Mesa, Arizona 4 Mary Bridge Children’s Health Center, Tacoma, Washington 5 Children’s Hospital and Regional Medical Center, Seattle, Washington Interstitial deletions in the terminal region of chromosome 6 are rare. We describe three new cases with subtle interstitial deletions in the q24-q26 region of the long arm of chromosome 6. The karyotypes were ana- lyzed at a 550 band level. Patient1 is a 9-month-old boy with an interstitial dele- tion, del(6)(q24.2q25.1), developmental de- lay, low birth weight, hypotonia, heart mur- mur, respiratory distress, craniofacial and genital anomalies. This is the first report of a case with deletion del(6)(q24.2q25.1). Pa- tient 2 is a 17-year-old young man with an interstitial deletion del(6)(q25.1q25.3), de- velopmental delay, short stature, mental re- tardation, autism, head, face, chest, hand and feet anomalies and a history of seizures. For the first time autism was described as a manifestation in 6q deletions. Patient 3 is baby boy with a de novo interstitial dele- tion, del(6)(q25.1q26), anomalies of the brain, genital organs, limbs and feet. This is the first report of a case with deletion, del(6)(q25.1q26). In all three patients, fluo- rescence in situ hybridization (FISH) using chromosome 6 painting probe ruled out an insertion. The ESR (6q25.1) and TBP (6q27) probes were used to confirm the break- points. Since TBP signal is present in all cases, it confirmed an interstitial deletion proximal to this probe. Patient 1 has a dele- tion of the ESR locus; Patient 2 and 3 have signals for the ESR locus on both chromo- somes 6. Therefore the deletion in Patients 2 and 3 are between ESR and TBP loci distal to that of Patient 1. FISH validated the de- letion breakpoints assessed by conventional cytogenetics. Am. J. Med. Genet. 87:17–22, 1999. © 1999 Wiley-Liss, Inc. KEY WORDS: d e l e t i o n 6q24.2q25.1, 6q25.1q25.3 and 6q25.1q26; FISH painting; clinical find- ings INTRODUCTION Deletions of chromosome 6q have been known since 1975 [Milosevic and Kalicanin, 1975]. At least 60 cases with deletions of the long arm of chromosome 6 are reported [Matkins et al., 1987; McLeod et al., 1990; Narahara et al., 1991; Valtat et al., 1992; Meng et al., 1992; Hopkin et al., 1997]. Valtat et al. [1992] pointed out that interstitial deletion breakpoints are largely located in the segment of 6q between q14 through q23. The breakpoints appear to be evenly distributed within that segment. They also pointed out that 6q25 is a pref- erential location for breakpoints in the 6q terminal de- letions. This was confirmed later by another study [Hecht and Hecht, 1992] which showed that 11 of 19 breakpoints in the terminal deletions were clustered in band 6q25. Interstitial deletions in the terminal region of chromosome 6 are rare [Matkins et al., 1987; McLeod et al., 1990; Narahara et al., 1991; Rubtsov et al., 1996]. To correlate phenotype with genotype, Hopkin et al. [1997] divided 6q deletions into three groups. Four- teen patients were categorized as Group A [del(6)(q11q16)]. They had a high incidence of hernias, up-slanting palpebral fissures, and thin lips with lower frequency of microcephaly, micrognathia, and heart malformations. Nineteen patients were classified un- der Group B [del(6)(q15q25)]. Their condition com- prised intrauterine growth retardation, respiratory problems, hypertelorism, and upper limb malforma- tions. Twenty-six patients were categorized as Group C *Correspondence to: Dr. Kavita S. Reddy, Cytogenetics Depart- ment, Quest Diagnostics Inc., 33608 Ortega Highway, San Juan Capistrano CA 92690. E-mail: [email protected] Received 19 January 1999; Accepted 12 July 1999 American Journal of Medical Genetics 87:17–22 (1999) © 1999 Wiley-Liss, Inc.
Transcript of Subtle overlapping deletions in the terminal region of chromosome 6q24.2-q26: Three cases studied...

Subtle Overlapping Deletions in the TerminalRegion of Chromosome 6q24.2-q26: Three CasesStudied Using FISH
S. Sukumar,1 S. Wang,1 K. Hoang,1 C.M. Vanchiere,2 K. England,3 R. Fick,4 B. Pagon ,5 andK.S. Reddy1*1Cytogenetics Department, Quest Diagnostics Inc., San Juan Capistrano, California2Childrens Clinic of Southwest Louisiana, Lake Charles, Louisiana3Casa Blanca Clinic, Mesa, Arizona4Mary Bridge Children’s Health Center, Tacoma, Washington5Children’s Hospital and Regional Medical Center, Seattle, Washington
Interstitial deletions in the terminal regionof chromosome 6 are rare. We describe threenew cases with subtle interstitial deletionsin the q24-q26 region of the long arm ofchromosome 6. The karyotypes were ana-lyzed at a 550 band level. Patient1 is a9-month-old boy with an interstitial dele-tion, del(6)(q24.2q25.1), developmental de-lay, low birth weight, hypotonia, heart mur-mur, respiratory distress, craniofacial andgenital anomalies. This is the first report ofa case with deletion del(6)(q24.2q25.1). Pa-tient 2 is a 17-year-old young man with aninterstitial deletion del(6)(q25.1q25.3), de-velopmental delay, short stature, mental re-tardation, autism, head, face, chest, handand feet anomalies and a history of seizures.For the first time autism was described as amanifestation in 6q deletions. Patient 3 isbaby boy with a de novo interstitial dele-tion, del(6)(q25.1q26), anomalies of thebrain, genital organs, limbs and feet. This isthe first report of a case with deletion,del(6)(q25.1q26). In all three patients, fluo-rescence in situ hybridization (FISH) usingchromosome 6 painting probe ruled out aninsertion. The ESR (6q25.1) and TBP (6q27)probes were used to confirm the break-points. Since TBP signal is present in allcases, it confirmed an interstitial deletionproximal to this probe. Patient 1 has a dele-tion of the ESR locus; Patient 2 and 3 havesignals for the ESR locus on both chromo-somes 6. Therefore the deletion in Patients 2and 3 are between ESR and TBP loci distal
to that of Patient 1. FISH validated the de-letion breakpoints assessed by conventionalcytogenetics. Am. J. Med. Genet. 87:17–22,1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: d e l e t i o n 6 q 2 4 . 2 q 2 5 . 1 ,6q25.1q25.3 and 6q25.1q26;FISH painting; clinical find-ings
INTRODUCTION
Deletions of chromosome 6q have been known since1975 [Milosevic and Kalicanin, 1975]. At least 60 caseswith deletions of the long arm of chromosome 6 arereported [Matkins et al., 1987; McLeod et al., 1990;Narahara et al., 1991; Valtat et al., 1992; Meng et al.,1992; Hopkin et al., 1997]. Valtat et al. [1992] pointedout that interstitial deletion breakpoints are largelylocated in the segment of 6q between q14 through q23.The breakpoints appear to be evenly distributed withinthat segment. They also pointed out that 6q25 is a pref-erential location for breakpoints in the 6q terminal de-letions. This was confirmed later by another study[Hecht and Hecht, 1992] which showed that 11 of 19breakpoints in the terminal deletions were clustered inband 6q25. Interstitial deletions in the terminal regionof chromosome 6 are rare [Matkins et al., 1987; McLeodet al., 1990; Narahara et al., 1991; Rubtsov et al.,1996]. To correlate phenotype with genotype, Hopkin etal. [1997] divided 6q deletions into three groups. Four-teen patients were categorized as Group A[del(6)(q11q16)]. They had a high incidence of hernias,up-slanting palpebral fissures, and thin lips with lowerfrequency of microcephaly, micrognathia, and heartmalformations. Nineteen patients were classified un-der Group B [del(6)(q15q25)]. Their condition com-prised intrauterine growth retardation, respiratoryproblems, hypertelorism, and upper limb malforma-tions. Twenty-six patients were categorized as Group C
*Correspondence to: Dr. Kavita S. Reddy, Cytogenetics Depart-ment, Quest Diagnostics Inc., 33608 Ortega Highway, San JuanCapistrano CA 92690. E-mail: [email protected]
Received 19 January 1999; Accepted 12 July 1999
American Journal of Medical Genetics 87:17–22 (1999)
© 1999 Wiley-Liss, Inc.

[del(6)(q25qter)]. These patients had retinal abnor-malities, cleft palate, and genital hypoplasia. The onlyuniversal finding reported among all the patients with6q deletions was mental retardation. Other findingscommon to all three groups included ear anomalies(90%), hypotonia (82%), and postnatal growth retarda-tion (68%). Three new cases with interstitial deletionsof 6q, del(6)(q24.2q25.1), del(6)(q25.1q25.3) anddel(6)(q25.1q26) are described in this report. An at-tempt is made to refine the phenotype to genotype cor-relation within the terminal region of chromosome 6q.
CLINICAL FINDINGSPatient 1
A 9-month-old boy was referred for chromosomestudy. He was born two weeks prematurely by vaginaldelivery. Birth weight was low, 2.7 kg. Family historywas unremarkable. He was thought to have had meco-nium aspiration syndrome and required hospitaliza-tion for ventilation therapy. There was a heart mur-mur, which was suspected to be due to tricuspid regur-gitation. He was hypotonic. However, at age 4 months,he started to show better tone and movement. Whenexamined at age 9 months, his length was 71.12 cm.(15th centile) and he weighed approximately 7 kg (<5thcentile). The head circumference (OFC) was 43.4 cm(2nd centile, microcephaly) and the infant had a promi-nent forehead, epicanthic folds, prominent nasal bridgeand thin lips. Anterior fontanelle was flat and soft. Re-sults of Bruchner test were symmetrical. Skin wasclear with good turgor. Testes were undescended. Atage 1 he weighed approximately 7.36 kg. His lengthwas 75.6 cm. The OFC was 44.5 cm. (< 50th centile).Testes were still undescended. He was able to interactverbally with three or four words. He was attemptingto crawl and appeared to be able to see and hear.
Patient 2
A 17-year-old Caucasian boy was referred for fragileX chromosome study (Fig.1A). His brother and a sisterare normal. He was delivered two weeks late by cesar-ean section to a non-consanguineous couple. Birthweight was 3.18 kg, length 50.8 cm and OFC 34.29 cm.Immediately after birth he was noted to have micro-gnathia with glossoptosis, although this apparentlycaused no breathing difficulties. At age 11 he developedhigh fever for which he was hospitalized. Work-up didnot show any bacterial infection. The fever was attrib-uted to a viral infection. Father’s family history wasnegative. During the mother’s pregnancy, there was noexposure to alcohol, smoking or chemicals. Bendectinwas taken, as needed, for nausea throughout the preg-nancy.
In the first year of life, the baby boy showed markeddelay in development. He sat at age 9 months, crawledby one year, walked at age 2 years and did not speakany words. When tested at age18 months, his hearingwas normal. Heart was normal. He had a history ofseizures of cyanotic breath holding spells. His anteriorfontanelle was open about one half fingertip. He wasnoted to have epicanthic folds. Teeth were small. Atage 28 months his skin was observed to be very dry and
was loose over his fingers. He had a prominent fore-head.
When examined at age 3 years, his height was 92cm.(25–50th centile), weight 11.42 kg (3rd centile) andOFC 45.8 cm. (<5th centile). He had marked blondstreaks in the front scalp hair, protruding ears (5 cmlong), inner canthal distance of 2 cm, downward slant-ing palpebral fissures, broad alveolar ridges, small peg-shaped teeth with gaps. His fingers were square with atotal hand length of 9 cm and mid-finger length of 4 cm,hyperextensible thumbs, rocker-bottom feet andmarked hypo/hyperpigmented areas over the chest,trunk, front and back. Extraocular movements werefull. Pupillary reactions were normal. Optic fundi couldnot be examined due to the agitation of the patient. Anormal 46,XY karyotype was reported (at another lab).Repeat study for fragile X syndrome showed no evi-dence of expression of the fragile site on the X chromo-some.
At age 16 1/2 years, his height was 162 cm, weight 60kg, and OFC 53 cm. Head shape was normal. Testiclesseemed slightly large. He needed glasses for closework. The skin on his palms and soles was thick andinsensitive. He appeared to have a skin rash/infection.
Fig. 1. A: Patient 2, a 17-year-old with developmental delay and be-havioral problems has del(6)(q25.1q25.3). B: Patient 3, a new born withmultiple congenital abnormalities has del(6)(q25.1q26).
18 Sukumar et al.

He was described as a short, non-verbal (could expressonly few words), autistic individual with a troubledsleep cycle, mental retardation and behavior problemsincluding temper tantrums, hostility towards othersand slapping himself. He had a normal CT scan and anelectroencephalogram (EEG).
Patient 3
A newborn boy with multiple congenital abnormali-ties was referred for chromosome study (Fig. 1B). Hewas born at 38 weeks of gestation to a G2 P2, 23-year-old mother and unrelated 25-year-old father both ofCaucasian origin. Mother had an abnormal Pap smearprior to pregnancy. Multiple ultrasound examinationswere performed during the pregnancy to look for evi-dence of incompetent cervix. She did not smoke, drinkalcohol or abuse drugs during the pregnancy. She hadoccasional colds and took amoxicillin in a low dose atthe end of the pregnancy due to respiratory infection.She has a 2-year-old daughter from a previous relation-ship who appears to be normal. A maternal uncle, whois in his 50’s, is said to be a slow learner and to havecryptorchidism. Father’s history was unremarkable.
Ultrasound examination several days prior to deliv-ery showed brain anomalies. C-section was performedbecause of breech presentation. Birth weight was 2.9kg, length 45 cm, and OFC 32.5 cm. There was sometransient respiratory distress for three days. MRIshowed agenesis of the corpus callosum and temporaland occipital horn enlargement (colpocephaly). Echo-cardiogram showed patent foramen ovale, patent duc-tus arteriosus, and possible pulmonary hypertension.However, no cardiac symptoms were found and therewas no concern regarding the cardiac findings. He hadundescended testes palpable in the inguinal area, clubfeet, and mild abnormalities of the retinal vessels inboth eyes. The normal arcing temporal vascular ar-cades were replaced by a curious anomaly of the retinalvessels. In the right eye there were two major retinalveins. One lead superiorly at 12 o’clock and the otherinferiorly at 6 o’clock. In the left eye, there were threemajor retinal vessels at 8, 11, and 2 o’clock. There wasno inferotemporal major vein. Despite these vascularpattern anomalies, macular development was intact,and the general retinal architecture appeared to be sat-isfactory. Hearing in the left ear was abnormal.
At age 2 weeks, the baby showed growth delay:weight was 3.06 kg (10th centile), length was about 47cm. (<5th centile), OFC 33.2 cm. (< 5th centile). Headwas symmetrically small with a sloping forehead. Theanterior fontanel was fingertip palpable. His eyebrowswere slightly broad. The right ear was somewhat ir-regularly shaped with a slightly triangular appearanceto the superior helix. He had a preauricular pit on theright ear but it was absent on the left ear. The alveolarridges were slightly broad. There was some redundantskin posteriorly on his neck. His scrotum was flat andrugated and testes were palpable in the inguinal area,the right higher than the left. The phallus was some-what deep-set into the pubic fat pad. There was de-creased extension at both knees, a flexible equinovarusdeformity of both feet and reduced muscle mass in bothcalves. His back was mildly hirsute.
MATERIALS AND METHOD
Peripheral blood cultures were synchronized withmethotrexate (amethopterin 0.05 mg/ml; SIGMA#M6770) for 17 hours and released with thymidine (2.5ug/ml; SIGMA #T5018) for 5.5 hours. The cultureswere harvested following the addition of colcemid.Chromosomes were GTG-banded. FISH studies wereperformed using coatasome 6, TBP probe that maps to6q27 and estrogen receptor (ESR) probe that maps to6q25.1(Oncor Inc.). The slides were denatured in 70%formamide/2X SSC at 70°C for 2 minutes, followed bydehydration in 70%, 80%, 90% and absolute alcohol.Ten microliters of the probe was applied to the slide. Itwas coverslipped and sealed. Following incubation
Fig. 2. Partial karyotypes of del(6)(q24.2q25.1) in Patient 1,del(6)(q25.1q25.3) in Patient 2 and del(6)(q25.1q26) in Patient 3. The nor-mal chromosome 6 is on the left and the deleted chromosome 6 is on theright. The bracket on the left chromosome in the ideogram shows the de-leted region and the arrow on the right chromosome shows the location ofthe deletion.
Deletions in the Terminal Region of Chromosome 6q24.2-q26 19
overnight in a humid chamber at 37°C, the slides werewashed in 1X SSC (coatasome 6) or 2X SSC (TBP andESR) at 72°C for 5 min. Detection was carried out usingrhodamine labeled anti-digoxigenin and counterstain4,6-diamidino-2-phenylindole (DAPI).
Cytogenetic Studies
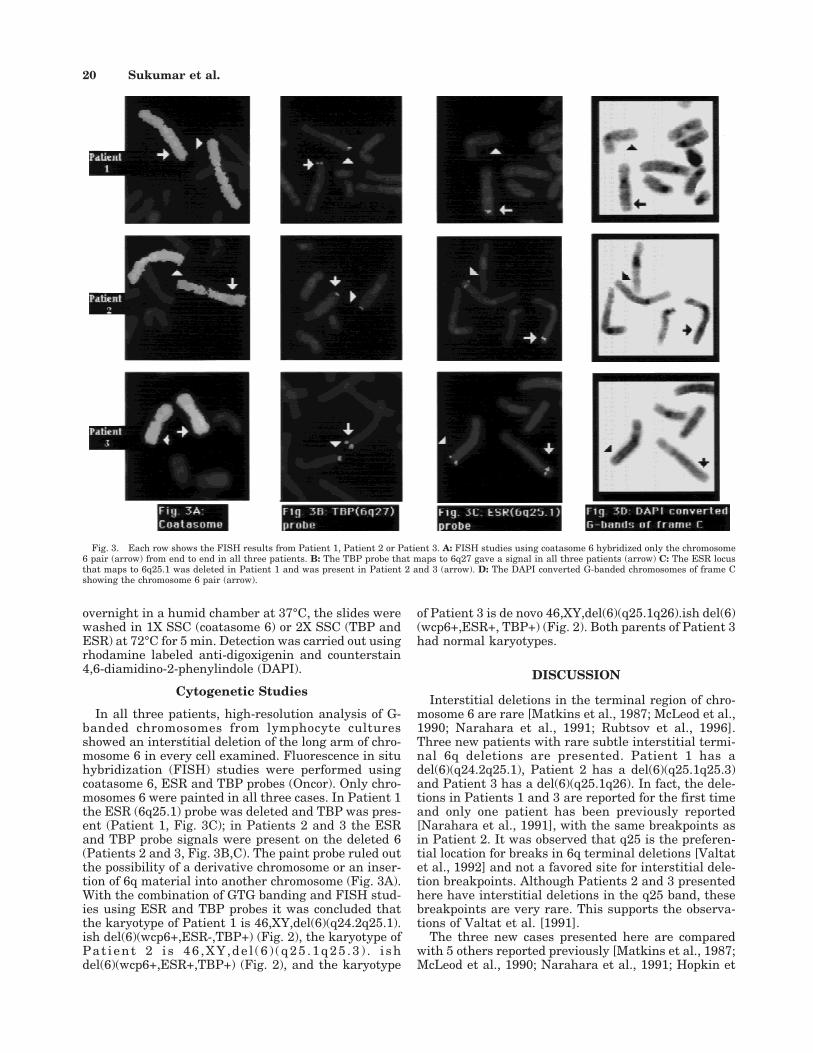
In all three patients, high-resolution analysis of G-banded chromosomes from lymphocyte culturesshowed an interstitial deletion of the long arm of chro-mosome 6 in every cell examined. Fluorescence in situhybridization (FISH) studies were performed usingcoatasome 6, ESR and TBP probes (Oncor). Only chro-mosomes 6 were painted in all three cases. In Patient 1the ESR (6q25.1) probe was deleted and TBP was pres-ent (Patient 1, Fig. 3C); in Patients 2 and 3 the ESRand TBP probe signals were present on the deleted 6(Patients 2 and 3, Fig. 3B,C). The paint probe ruled outthe possibility of a derivative chromosome or an inser-tion of 6q material into another chromosome (Fig. 3A).With the combination of GTG banding and FISH stud-ies using ESR and TBP probes it was concluded thatthe karyotype of Patient 1 is 46,XY,del(6)(q24.2q25.1).ish del(6)(wcp6+,ESR-,TBP+) (Fig. 2), the karyotype ofPat ient 2 i s 46 ,XY,de l (6 ) (q25 .1q25 .3 ) . i shdel(6)(wcp6+,ESR+,TBP+) (Fig. 2), and the karyotype
of Patient 3 is de novo 46,XY,del(6)(q25.1q26).ish del(6)(wcp6+,ESR+, TBP+) (Fig. 2). Both parents of Patient 3had normal karyotypes.
DISCUSSION
Interstitial deletions in the terminal region of chro-mosome 6 are rare [Matkins et al., 1987; McLeod et al.,1990; Narahara et al., 1991; Rubtsov et al., 1996].Three new patients with rare subtle interstitial termi-nal 6q deletions are presented. Patient 1 has adel(6)(q24.2q25.1), Patient 2 has a del(6)(q25.1q25.3)and Patient 3 has a del(6)(q25.1q26). In fact, the dele-tions in Patients 1 and 3 are reported for the first timeand only one patient has been previously reported[Narahara et al., 1991], with the same breakpoints asin Patient 2. It was observed that q25 is the preferen-tial location for breaks in 6q terminal deletions [Valtatet al., 1992] and not a favored site for interstitial dele-tion breakpoints. Although Patients 2 and 3 presentedhere have interstitial deletions in the q25 band, thesebreakpoints are very rare. This supports the observa-tions of Valtat et al. [1991].
The three new cases presented here are comparedwith 5 others reported previously [Matkins et al., 1987;McLeod et al., 1990; Narahara et al., 1991; Hopkin et
Fig. 3. Each row shows the FISH results from Patient 1, Patient 2 or Patient 3. A: FISH studies using coatasome 6 hybridized only the chromosome6 pair (arrow) from end to end in all three patients. B: The TBP probe that maps to 6q27 gave a signal in all three patients (arrow) C: The ESR locusthat maps to 6q25.1 was deleted in Patient 1 and was present in Patient 2 and 3 (arrow). D: The DAPI converted G-banded chromosomes of frame Cshowing the chromosome 6 pair (arrow).
20 Sukumar et al.

al., 1997; Meng et al., 1992] with deletions in the 6qterminal region. The clinical findings of all these casesare listed in Table I. Hopkin et al. [1997] divided 6qdeletions into three groups A, B, and C i.e. proximal(6q11q16), middle (6q15q25) and distal (6q25qter). Thepatients in Table I fall in the category of Group B,Group B and C or Group C based on their breakpoints.The common clinical findings of Group B are an excessof males (68%), intrauterine growth retardation,prominent forehead, microcephaly, micro/retrognathia,short palpebral fissures, hypertelorism, prominentnose, thin lips, a high arched palate. Chronic respira-tory illness and apnea or other respiratory problemsare described in 42% of this group. Infant mortality inthis group is very high. Common anomalies in Group Cincluded cleft palate, clubfoot, retinal abnormalities,seizures, hydrocephalus, brain abnormalities, abnor-mal hair pattern, and cryptorchidism associated withgenital hypoplasia. Minor anomalies include micro-cephaly, broad nasal tip, prominent nasal bridge, epi-canthic folds and short palpebral fissures that mayslant up or down. Mental retardation was a universalfinding among all patients with 6q deletions. Low birthweight, developmental delay, hypotonia, congenitalheart defects and cryptorchidism are common toGroups A, B and C.
The clinical findings in Patient 1, with deletion6q24.2q25.1, are compared with two reported caseswith deletions 6q23q25 [McLeod et al., 1990] and6q23.1q24.2 [Matkins et al., 1987]. The common clini-cal findings in these three patients are low birthweight, growth retardation and microcephaly. Epican-thic folds and congenital heart defect are observed inboth cases with deletions 6q24.2q25.1 (Patient1) and6q23q25 [McLeod et al., 1990]. A prominent nasalbridge, thin lips and respiratory distress are observedin 6q24.2q25.1 (Patient 1) and 6q23.1q24.2 [Matkins etal., 1987] deletion cases. Patient 1 also has a prominentforehead, cryptorchidism and hypotonia not observedin the two reported cases. Some of the more commonclinical findings of Group C [del(6)(q25qter)] such ascleft palate, retinal abnormalities, seizures, hydroceph-alus, foot and hair pattern abnormalities are not ob-served in these three patients. The phenotype of thesepatients seems to be more of Group B [del(6)(q15q25)]described by Hopkin et al.[1997]. Therefore, the distalsubband q24.2q24.3 deletion appears to be critical forthe clinical findings in Group B.
Narahara et al. [1991] reported on a patient with thesame deletion, del(6)(q25.1q25.3), as in Patient 2. Pa-tient 2 has a prominent forehead, down-sloping palpe-bral fissures, large protruding ears, feeding problems,
TABLE I. Clinical Findings In Selected Cases With 6q Deletions†
Clinical findingsPatient 1*
(B & C)Matkins et al.
1987 (B)McLeod et al.
1990 (B)Patient 2*
(C)Narahara et al.
1991 (C)Patient 3*
(C)Hopkin et al.
1997 (C)Meng et al.
1992 (C)
Deletion 6q breakpoints q24.2q25.1 q23.1q24.2 q23q25 q25.1q25.3 q25.1q25.3 q25.1q26 q25.2 q25.3Sex M F M M M M M FAge, months (M), Years (Y) 1Y 2Y <1M 17Y 17M <1M 2Y 2YLow birth weight + + + − + − + +Growth retardation + + + + + + + +Hydrocephalus − − − − − − + −Microcephaly + + + + + + − −Prominent forehead + − − + − − − +Hypertelorism − + − − − − − −Epicanthic folds + − + + + − − +Downslanting palpebral fissures − − − + − − − −Upslanting palpebral fissures − − − − + − − −Retinal, macular abnormality** − − − − − + + +Large ears − − − + − − − +Low set ears − + − − − − + +Posteriorly rotated − − − − − − + −Malformed ears − − + − + + −Broad, prominent nasal bridge + + − − + − + +Micrognathia − − + + + − − +High arched palate − − − − − − − +Abnormal philtrum − − − − − − + −Thin lips + + − − − − − −Cleft palate − − − − − − − +Congenital heart defect + − + − − − + +Respiratory distress + + − − + + + −Feeding problems − − − + − − + −Cryptorchidism + NA − − − + − NAShort neck − + + − + − − −Chest and trunk asymmetry − − − + − − − +Spine abnormality − − + − − − − +Foot abnormality − − − + − + − −Abnormal hand, fingers − − + + + − − −Joint laxity − − − − − − − −Hypotonia + − − − − − + +Hair − − − + − + − −Abnormal dermatoglyphics − − + − + − − −Skin abnormality − − + − − − + −Seizures, cyanotic spells − − − + − − − −Developmental delay + + ND + + ND + +
†+, Characteristic present; −, Characteristic absent or not reported; NA, Not applicable; ND, not documented; *, Patient in the present study; B, B & C,C, Hopkin’s classification; **, Retinal abnormalities include abnormalities of the blood vessels in the retina.
Deletions in the Terminal Region of Chromosome 6q24.2-q26 21

foot and hand abnormalities, hyperextensible thumbs,seizures, hair and skin abnormalities, autism andother behavioral problems. The clinical findings in thecase reported by Narahara et al.[1991] were up-slanting palpebral fissures, broad nasal root, respira-tory distress, and short neck. But both these patientshave in common the following clinical findings: growthretardation, microcephaly, epicanthic folds, microgna-thia, abnormalities of fingers and developmental delay.Patient 2, presents some of the frequently seen abnor-malities in terminal 6q25qter deletions of Group C[Hopkin et al., 1997]. They include foot anomaly, sei-zures and abnormality of the hair that were not ob-served in the patient reported by Narahara et al.[1991]. So far no author has recorded autism, a uniquefinding in Patient 2, with 6q deletions.
Patient 3 has growth retardation and microcephalylike Patient 2 and the case described by Narahara et al.[1991]. In addition Patient 3 also has abnormalities ofthe brain, clubfeet, cryptorchidism and vascularanomalies of the retina, anomalies frequently seen inthe 6q25qter deletions of Group C. The q26 band ap-pears to be critical for retinal abnormalities found inGroup C. In the two patients, with the more terminaldeletions q25.2 and q25.3 [Hopkin et al., 1997; Meng etal., 1992] the common clinical findings were low birthweight, growth retardation, retinal abnormalities, lowset ears, broad or prominent nasal bridge, congenitalheart defect, developmental delay and hypotonia. Hy-drocephalus was reported in one patient [Hopkins etal., 1997]. Retinal and macular abnormality is ob-served in distal terminal deletion q25.2qter and
q25.3qter cases [Hopkin et al., 1997; Meng et al., 1992].A gene for retinal cone dystrophy is thought to be lo-cated in the 6q25-26 region [Warburg, 1991].
REFERENCES
Hecht F, Hecht BK. 1992. Nonrandom chromosome breakpoints in 6q de-letion. Clin Genet 41:167–168.
Hopkin RJ, Schorry E, Bofinger M, Milatovich A, Stern HJ, Jayne C, SaalHM. 1997. New insights into the phenotypes of 6q deletions. Am J MedGenet 70: 377–386.
Matkins SV, Meyer JE, Berry AC. 1987. A child with partial monosomy 6qsecondary to a maternal direct insertional event. J Med Genet 24:227–229.
McLeod DR, Fowlow SB, Robertson A, Samcoe D, Burgess I, Hoo JJ. 1990.Chromosome 6q deletions: a report of two additional cases and a reviewof the literature. Am J Med Genet 35:79–84.
Meng J, Fujita H, Nagahara N, Kashiwai A, Yoshioka Y, Funato M. 1992.Two patients with chromosome 6q terminal deletions with breakpointsat q24.3 and q25.3. Am J Med Genet 43:747–750.
Milosevic J, Kalicanin P. 1975. Long arm deletion of chromosome no.6 in amentally retarded boy with multiple physical malformations. J MentDefic Red 19:139–144.
Narahara K, Tsuji K, Yokoyama Y, Namba H, Murakami M. Matsubara T,Kasai R, Fukushima Y, Seki T, Wakui K, Seino Y. 1991. Specificationof small distal 6q deletions in two patients by gene dosage and in situhybridization study of plasminogen and alpha-L-fucosidase 2. Am JMed Genet 40:348–353.
Rubtsov N, Senger G, Kuzcera H, Neumann A, Kelbova C, Junker K,Beensen V Claussen U. 1996. Interstitial deletion of chromosome 6q:precise definition of the breakpoints by microdissection, DNA amplifi-cation, and reverse painting. Hum Genet 97:705–709.
Valtat C, Galliano D, Mettey R, Toutain A, Moraine C. 1992. Monosomy 6q:report on four new cases. Clin Genet 41:159–166.
Warburg M, Sjo O, Tranebjaerg L. 1991. Chromosome 6q deletion andretinal cone dystrophy. Am J Med Genet 38:134.
22 Sukumar et al.


















