
Strokes in Pregnant and Post- Partum Populationswcm/@swa/documents/... · Strokes in Pregnant and...
72
Strokes in Pregnant and Post- Partum Populations Mark Alberts MD Robin Novakovic MD Shivani Patel MD G. Lee Pride Jr. MD Departments of Radiology, Neurosurgery, Neurology and OB/GYN- Maternal Fetal Medicine 1
Transcript of Strokes in Pregnant and Post- Partum Populationswcm/@swa/documents/... · Strokes in Pregnant and...

Strokes in Pregnant and Post-Partum Populations
Mark Alberts MD
Robin Novakovic MD
Shivani Patel MD
G. Lee Pride Jr. MD
Departments of Radiology, Neurosurgery, Neurology and OB/GYN-
Maternal Fetal Medicine
1

Faculty
2
Mark Alberts MD, FAHAProfessor and Vice ChairDepartment of Neurology& NeurotherapeuticsStroke Neurologist
Shivani Patel MDAssistant ProfessorDepartment of Obstetricsand GynecologyMaternal-Fetal Medicine
Robin Novakovic MDAssociate ProfessorDepartments of Radiology,Neurology & NeurotherapeuticsNeurointerventionalistNeurointensive Care
G. Lee Pride, Jr. MDProfessorDepartments of Radiologyand NeurosurgeryNeurointerventionalistNeuroradiologist

Stroke in Pregnancy Case
…Presentation and Initial Management

Monday 5/18/15…
• 27 YORHF 8 weeks pregnant• No significant PMHx, hyperemesis gravid.• Last normal 1030am• 1039am found abnormal by 3YO son• EMS called… PSC arrival 1124am• NIHSS 10, BP 114/67, HR 78, Glucose 96• CT 1130am ASPECTS 9-10, dense R MCA 0hr 54min

Stroke Neurologist’s Perspective
…Medical Treatment Decisions, Stroke in the Young
Mark Alberts MD FAHA
Professor and Vice Chair of Neurology
5

Epidemiology of Strokes During Pregnancy
6James et al., Ob-Gyn, Sept 2005

Types of Stroke by Trimester
7 Scott et al., Ob and Gyn, Aug 2012

Risk Factor Odds Ratio Comment
Migraine 16.9 Most common condition
Thrombophilia 16.0 Variety of conditions
Lupus 15.2 Diverse mechanisms
Heart disease 13.2 Various diseases
Sickle cell disease 9.1 Easy to detect
Hypertension 6.1 Very common
Thrombocytopenia 6.0 Possibly related to lupus
Diabetes 2.5 Common risk factor
Substance/ETOH abuse 2.3 Variety of drugs
Smoking 1.9 Common risk factor
Obesity 1.4 Common
Risk Factors for Stroke in Pregnancy
8James et al., Ob-Gyn, Sept 2005

Stroke Type RR during Pregnancy RR Post-Partum( 6 weeks)
Cerebral Infarction 0.7 8.7
CerebralHemorrhage
2.5 28.5
Stroke Type and Pregnancy
9
Feske, Seminars in Neurology, V 27, 2007

Major Types of Stroke in Pregnancy
Scott et al., Ob and Gyn, Aug 2012

Post-partum cardiomyopathy
Peri-partum CNS vasculitis
Amniotic fluid embolization
PFO with paradoxical embolization
–Must have source of clot
–Right to left shunt
Arterial dissection during labor
Arterial dissection due to hyper-emesis
Overlooked or Under-Appreciated Cause of
Stroke in Pregnancy
11

Cardiac etiologies
–SBE with negative Cx, papillary fibroelastoma, atrial myxoma, PFO
Subtle arterial dissections
–May be history of minor trauma
CNS vasculitis (often isolated)
Hypercoagulable state: in setting of cancer, pregnancy
Metabolic disorders: Hyper-homocysteine, Fabry’s disease
Infectoins: HIV, CNS infection, syphilis
Migraines: especially if older, + smoking, + OCPs
Pregnancy: numerous etiologies
Drug abuse: (often not tested for)
Genetic etiologies: (CADASIL, CARASIL, MELAS, etc.)
Causes of Stroke in Young People
12

National Inpatient Sample; 2005-2010
18,392 pregnant patients with a stroke
–27% due to cerebral venous thrombosis
–23% ICH or SAH
70 patients Rx with IV TPA
–79% discharged home
–14% to nursing home
–7% dead
Studies of Stroke in Pregnancy
13
Song et al., Neurology 2014; vol 82, supp 10; P 3.100

Case series; 8 patients
Most due to cardio-embolic or hypercoagulable state
Pregnancy duration:
–4 at 4-6 weeks; 2 at 8-10 weeks; 1 at 12 and 1 at 37 weeks
Outcomes
–Pregnancy termination, fetal death, miscarriage in 6/8 cases
–Patient outcomes: 3/8 with some type of cerebral hemorrhage
IV TPA Use in Pregnancy for Stroke
14
Murrugappan et al., Neurology 2006

Endovascular Therapy for Stroke in Pregnancy
Advantages
Focal therapy, clot specific
New devices appear to be
safe, effective
Avoid systemic effects
Disadvantages
Invasive procedure
Radiation exposure
Sedation often required
Bleeding risks
15
Endovascular Therapy for Stroke in PregnancySupported by Small Cases Series, Reports

Strokes related to pregnancy are often due to unique
etiologies that differ from typical populations
The evaluation of patients with strokes during
pregnancy requires special testing
The use of IV TPA in this population is likely associated
with an increased risk of bleeding and fetal loss
EVT is an option in centers that offer this therapy
A multidisciplinary team approach is needed to ensure
optimal outcomes
Conclusions
16

DISCUSSION
Stroke in Pregnancy Case
…Large Vessel Occlusion Management Decisions

Monday 5/18/15…
• IV t-PA given 1223pm at PSC• No vascular imaging• No immediate improvement
1hr 53min

Monday 5/18/15…
• Transferred to CSC, arrival 1326pm• Clinical deterioration en route despite IV t-PA• NIHSS 19, L HP, right gaze, L visual field cut, L Neglect• No vascular imaging• ? Imaging ?Intervention
2hr 56min

Neurointerventionalist’s Perspective
…Imaging and Endovascular Treatment Decisions
Robin Novakovic MD
Associate Professor of Radiology, Neurology and
Neurotherapeutics
21

Radiation Exposure in Endovascular Procedures
• Past 10 years, the use of radiologic examinations in pregnant women has increased by 107%.
• Radiation is an invisible threat in endovascular interventions.
• The interventionalist has the role of overseeing the radiation protection for staff, patient and fetus; as well as determining the appropriateness of performing the endovascular procedure to treat the stroke.
• Currently, the dose to the embryo/fetus is not subject to legal dose limits, but we are guided by recommendations and current evidence.
Walsh SR, et al. Ionizing radiation in endovascular interventions. J Endovasc Ther2008;15:680-7.

Effects of Radiation on the Embryo
• In this topic we have to differentiate between:
• ionizing radiation (x-rays, gamma rays, internal and external radionuclides, neutrons)
• nonionizing radiation (ie, electromagnetic fields of various frequencies, microwave radiation, communication band radiation, diathermy, lasers, and ultrasound).
• We are focusing on ionizing radiation during pregnancy.
• It is estimated that a fetus will be exposed to 1 mGy of background ionizing radiation during pregnancy.

Damage Effects of Ionizing Radiation
Deterministic (threshold effect): result from damage to a number of cells, with a dose threshold before damage occurs. (malformations, mental retardation and death).
– No effect expected below a dose of 100 mGy.
Stochastic: result from damage to a single cell and can lead to carcinogenesis. There is no absolute dose threshold, but the risk of damage increases with radiation dose, however, the severity of the effect remains the same (risk of cancer and genetic effects).

Measuring Radiation
• There are several measurement for radiation dose.
• The absorbed dose is measured in the rad and the effective dose is measured in the rem.
• In the international system of units, the rad is measures as the Gray (Gy) and the rem is measured as the Sievert (SV).
• 1 rad = 10 mGy and 1 rem = 10 mSV

Teratogenesis Induced by Ionizing Radiation
• The most vulnerable stage of the embryo to teratogenesis is between the 2nd and 20th weeks of gestation, particularly the period between the 8th and 15th weeks (fetal organogenesis).
• In its 2007 recommendations, the International Committee on Radiological Protection concluded that no deterministic effects of practical significance would be expected to occur below a dose of 100 mGy.
• At a radiation exposure dose of <50 mGy, the fetus at all stages of gestation generally suffers no major developmental abnormalities.
Brent RL. What are the reproductive and developmental risks of ionizing radiation? In: Hales B, Scialli A, Tassinari M, eds. Teratology primer. 2nd ed. Philadelphia, Pa: Thomas Jefferson University, 2010; 56–58. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP 2007;37:2–4. Wrixon AD. New ICRP recommendations. J Radiol Prot 2008;28(2):161–168.

• The risk to a fetus from ionizing radiation is dependent on the gestational age at the time of exposure and the dose of radiation.
• If extremely high-dose exposure (>1 Gy) occurs during early embryogenesis, it most likely will be lethal to the embryo.
American College of Radiology. ACR-SPR practice parameter for imaging pregnant or potentially pregnant adolescents and women with ionizing radiation. Resolution 39. Reston (VA): ACR;2014.Tremblay E et al. Quality initiatives: guidelines for use of medical imaging during pregnancy and lactation. Radiographic 2012:32:897-911.

Radiation Exposure to the Fetus
• In humans, growth restriction, microcephaly, and intellectual disability are the most common adverse effects from high-dose radiation exposure.
• Based on data from atomic bomb survivors, it appears that the risk of CNS effects is greatest with exposure at 8-15 weeks of gestation.
• It has been suggested that a minimal threshold for this adverse effect may be in the range of 60-310 mGy.
• However, the lowest clinically documented dose to produce severe intellectual disability is 610 mGy.
Blot WJ et al. Mental retardation following in utero exposure to the atomic bombs of Hiroshima and Nagasaki. Radiology 1973;106:617-9.Miller RW. Discussion: severe mental retardation and cancer among atomic bomb survivors exposed in utero. Teratology 1999;59:234-5.

Teratogenesis Induced by Ionizing Radiation
• Fetal risk of anomalies, growth restriction or spontaneous abortion have not been reported with radiation exposure of less than 50 mGy, a level above the range of exposure for diagnostic procedures.
Gjelsteen AC et al. CT, MRI, PET, PET/CT, and ultrasound in the evaluation of obstetric and gynecologic patients. SurgClin North Am 2008;88:361-90.ACOG Committee on Obstetric Practice. ACOG Committee Opinion, February 2016 (replaces no. 299, September 2004): guidelines for diagnostic imaging during pregnancy and lactation. Obstet Gynecol February 2016;656:1-6.

Risk of Carcinogenesis from Ionizing Radiation Exposure
• Risk of carcinogenesis as a result of in-utero exposure to ionizing radiation is unclear but is probably very small.
• A 10-20 mGy fetal exposure may increase the risk of leukemia by a factor of 1.5-2.0 over a background rate of approximately 1 in 3000.
• With larger doses (eg, a fetal dose of 20–50 mGy received during pelvic CT), the risk of carcinogenesis increases approximately by a factor of 2.
• Keep in mind the overall risk still remains low.
Leyendecker JR et al. MR imaging of maternal diseases of the abdomen and pelvis during pregnancy and the immediate postpartum period. Radiographics 2004;24:1301-16.Gjelsteen AC et al. CT, MRI, PET, PET/CT, and ultrasound in the evaluation of obstetric and gynecologic patients. SurgClin North Am 2008;88:361-90.

Risk of Carcinogenesis from Ionizing Radiation Exposure
• Should a pregnant woman need to undergo multiple imaging studies using ionizing radiation, it is prudent to consult with a radiation physicist to calculate the total dose expected and received by the fetus.
• The Health Physics Society maintains a web site with an ask-the-expert feature: www.hps.org/publicinformation/ate/cat4.html.
Leyendecker JR et al. MR imaging of maternal diseases of the abdomen and pelvis during pregnancy and the immediate postpartum period. Radiographics 2004;24:1301-16.Gjelsteen AC et al. CT, MRI, PET, PET/CT, and ultrasound in the evaluation of obstetric and gynecologic patients. SurgClin North Am 2008;88:361-90.

Radiation Exposure in Endovascular Procedures
• When counseling pregnant patients regarding the risks of radiation exposure to their fetus, these risks should be balanced with the potential benefits.
• When it is necessary to use radiation during pregnancy, a risk assessment should be conducted referencing:
• the gestational age at the time of exposure
• the extent to which the fetus in included in the radiation field
• the radiation level received
Walsh SR, et al. Ionizing radiation in endovascular interventions. J Endovasc Ther2008;15:680-7.

How Much Dose are We Predicting?....
• As an example, pulmonary embolism is a common condition in pregnant women –If the pregnant woman were to undergo chest radiography, lung scintigraphy, CT pulmonary angiography, and traditional pulmonary angiography, the fetus would be exposed to only about 1.5 mGy of radiation.
ACOG Guideline Statement: The radiation dose to the embryo or fetus that is likely to result from any diagnostic procedure in current use should present no risk of fetal death, malformation, growth retardation, or impairment of mental development.




Dose to Patient During Endovascular Revascularization
• At our institution, recent endovascular stroke treatments had a mean radiation dose exposure to the patient of 1148 mGy (650 – 1951 mGy range).


Use of IV Contrast During Pregnancy
• ACR concluded in the 2015 Manual of Contrast Media there is no evidence of either mutagenic or teratogenic effects secondary to IV or IA iodinated contrast exposure during pregnancy.
• Supported by the FDA classification of most iodinated contrast agents as category B medications.
• Although iodinated contrast media can cross the placenta and either enter the fetal circulation or pass directly into the amniotic fluid, animal studies have reported no teratogenic or mutagenic effects from its use.
Atwell TD et al. Neonatal thyroid function after administration of IV iodinated contrast agent to 21 pregnant patients. AFR Am J Roentgenol 2008;191:269-71.Webb JA et al. The use of iodinated and gadolinium contrast media during pregnancy and lactation. Member of Contrast Media Safety Committee of European Society of Urogenital Radiology (ESUR). Eur Radiol 2005;15:1234-40.American College of Radiology. ACR committee on drugs and contrast media. ACR Manual on Contrast Media. Version 10.1. American College of Radiology, 2015.

Use of IV Contrast During Pregnancy
• The fetal thyroid plays an important role in the development of the CNS.
• IV administration of iodinated contrast media does not affect short-term neonatal thyroid stimulating hormone (TSH), likely because the overall amount of excess iodide in the fetal circulation is small and transient.
• To date, there has been no documented case of neonatal hypothyroidism from the maternal IV injection of water-soluble iodinated contrast agents.
American College of Radiology. ACR committee on drugs and contrast media. ACR Manual on Contrast Media. Version 10.1. American College of Radiology, 2015. Quality Initiatives Guidelines for use of medical imaging during pregnancy and lactation. RadioGraphics 2012;32:897-911.
•ACR Guideline statement: Given the current available data and routine evaluation of all newborns for congenital hypothyroidism at the time of their birth, no extra attention is felt to be necessary.

Breast Feeding and IV Contrast
• Because contrast is water soluble, less the 1% of iodinated contrast administered to a lactating woman is excreted into the breast milk and less than 1% of this amount of contrast will be absorbed through the infant's gastrointestinal tract.
ACOG Committee on Obstetric Practice. ACOG Committee Opinion, no. 299, September 2004 (replaces no. 158, September 1995): guidelines for diagnostic imaging during pregnancy and lactation. Obstet Gynecol February 2016;656:1-6. American College of Radiology. ACR committee on drugs and contrast media. ACR Manual on Contrast Media. Version 10.1. American College of Radiology, 2015.
•ACOG and ACR Guideline statement: Breastfeeding can be continued without interruption after the use of iodinated contrast.
Summary
• No deterministic effects of practical significance would be expected to occur below a dose of 100 mGy.
• At a radiation exposure dose of <50 mGy, the fetus at all stages of gestation generally suffers no major developmental abnormalities.
• The radiation dose to the embryo or fetus that is likely to result from any diagnostic procedure in current use should present no risk of fetal death, malformation, growth retardation, or impairment of mental development.
• Breastfeeding can be continued without interruption after the use of iodinated contrast.
Summary
• Should a pregnant woman need to undergo multiple imaging studies using ionizing radiation, it is prudent to consult with a radiation physicist to calculate the total dose expected and received by the fetus.
• The Health Physics Society maintains a web site with an ask-the-expert feature: www.hps.org/publicinformation/ate/cat4.html.

DISCUSSION
Stroke in Pregnancy Case
…Large Vessel Occlusion Management

Monday 5/18/15…
• Repeat Head CT 1340pm (3hr 10min)• CT ASPECTS 9• No CTA or non-invasive vascular imaging• Taken directly to angio suite• NIHSS 19, L HP, right gaze, L visual field cut, L neglect
3hr 10min

Monday 5/18/15…
47
Groin access 1400, Angios 1402, 1410Right carotid occlusion
3hr 40min

Monday 5/18/15…
48
Clot definition, 1421pm Clot in ICA/MCA 3hr 51min

Monday 5/18/15…
49
Solitaire/Aspiration 1430pmClot in ICA/MCA
4hr 0min

Monday 5/18/15…
50
Vessel open 1437pmTICI 3 flow
Radiation output : 1133 mGyContrast 125cc Isovue
4hr 7min

Monday 5/18/15…
51
Some spasm in vessel from deviceGood flow to brain
Door to groin: 36minDoor to reperfusion: 71minOnset to reperfusion: 247min…..NIHSS 19 to NIHSS 4 at 1610pm
5hr 40min

Tuesday…Follow-up MRA 23hrs
52
NIHSS improved to 2 1000amSpasm in MCA resolved
23hr 30min

Tuesday… MRI 23 hours
53
Relatively small stroke/ischemiaNIHSS improved to 0 1400pmTransferred from ICU to floorNeurologically NORMALDischarged home Thursday 5/21/15 NIHSS 0, MRS 0
27hr 30min

Stroke in Pregnancy Case
…Work-up, Recovery and Care after Stroke

Work-up and treatment
55
• Aspirin therapy 81mg daily 24hrs after t-PA
• SQ Heparin DVT prophylaxis• TTE: EF 66%, no thrombus. Bubble
study not done in pregnancy, interatrial septal color flow abnormality on apical view suggests possible SMALL PFO.
• NSR, normal EKG.• Initial labs CBC, BMP, LFTs WNL• Chol 152, triglycerides 159• LE/pelvic ultrasound neg. for clot• Normal fetal US 5/28/15

Work-up and treatment
56
• Aspirin therapy 81mg continued during pregnancy/delivery
• Hypercoagulable evaluation 6/29/15• ESR 27• ANA, ENA, Complement, HIV,
cryoglobulin, hypercoag labs, ACE, factor V leiden, prothrombin mutations all neg.
• No hypercoagulable or thrombophilic abnormalities
• Holter monitoring 9/8/15: NSR with sinus arrhythmia. No A-fib
• Pelvic/LE U/S x 2 and MRI neg• Vaginal delivery on ASA 12/17/15

OB/GYN Perspective
…Evaluation and Care of the Pregnant Stroke Patient
Shivani Patel MD
Assistant Professor of Obstetrics and Gynecology
57

Incidence: 1.5-71 per 100,000 pregnancies
• Maternal mortality from stroke is about 15%
• 10% are discharged to a facility other than home
Antepartum: 10%
Intrapartum: 40%
Postpartum: 50%
What are the chances?
58
James A et al. Incidence and risk factors for stroke in pregnancy and the puerperium. Obstetrics & Gynecology, Sept. 2005
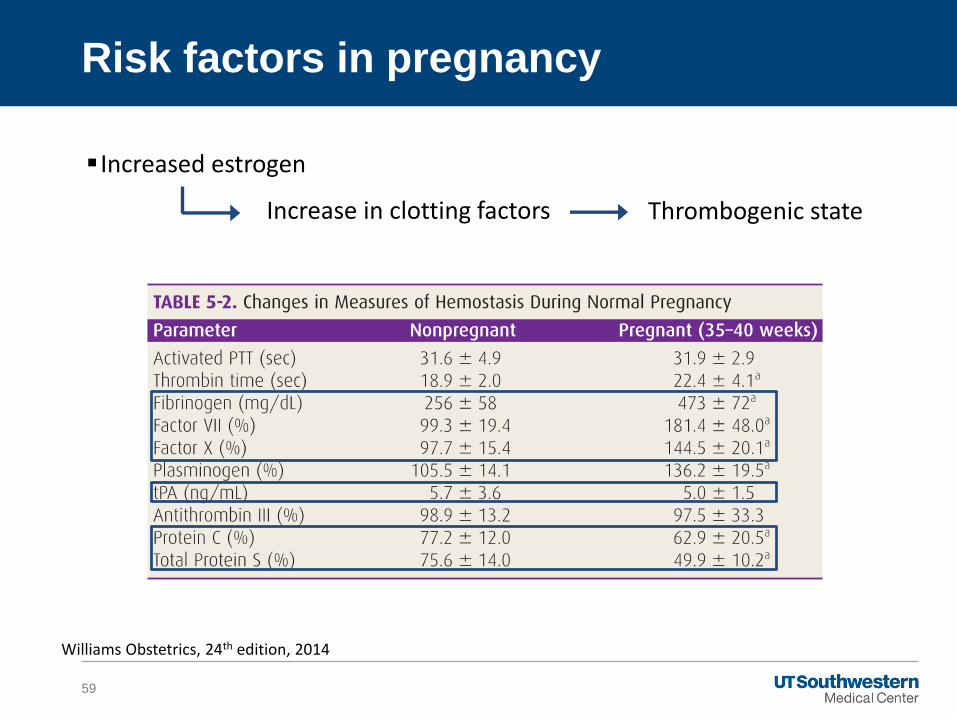
Increased estrogen
Risk factors in pregnancy
59
Increase in clotting factors Thrombogenic state
Williams Obstetrics, 24th edition, 2014

Increased estrogen
Large gravid uterus
Risk factors in pregnancy
60
Compression of pelvic veins Venous stasis

Increased estrogen
Large gravid uterus
Hypertension disorders of pregnancy
• Complicate 5-10% of pregnancies
Hemorrhage
Cesarean section
• 30% nationwide
Risk factors in pregnancy
61
Williams Obstetrics, 24th edition, 2014CDC Fastats 2014

Other risk factors
62
Risk Factor Odds Ratio Comment
Gestational HTNPre-eclampsia
4.4 Very common
Estrogen 2.0
Cesarean section 1.7 30% of deliveries
Postpartum hemorrhage
1.8 Affects 4-8%
Blood transfusion 10.3 2-3% of patients
Postpartum infection 25.0
James A et al. Incidence and risk factors for stroke in pregnancy and the puerperium. Obstetrics & Gynecology, Sept. 2005

Types of Stroke by Trimester
63
Time of Stroke Hemorrhagic Stroke
IschemicStroke
Cerebral Vein Thrombosis
Antepartum 13% 29% 40%
Intrapartum 27% 31% 20%
Postpartum 60% 45% 40%
James A et al. Incidence and risk factors for stroke in pregnancy and the puerperium. Obstetrics & Gynecology, Sept. 2005

Do not withhold workup or treatment because of pregnancy
Imaging in Pregnancy
64
ACOG Committee Opinion Number 656, February 2016
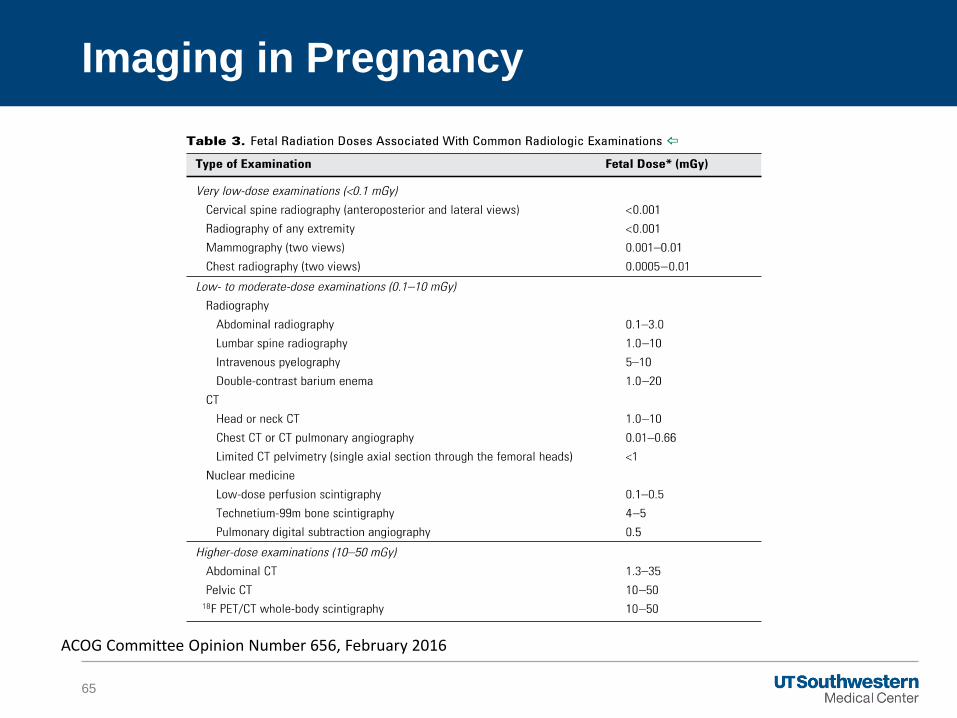
Imaging in Pregnancy
65
ACOG Committee Opinion Number 656, February 2016

Acute:
• IV t-PA
• Gestational age
• Bleeding?
• Endovascular therapy
• Gestational age
• Sedation
• Fetal monitoring
Treatment
66
Long-term:
• Low dose aspirin
• Anti-platelet agents
• Lovenox/Heparin
• Warfarin

Logistics of labor and delivery
Long-term disability
• Self care
• Infant care
Death
Maternal Considerations
67

Fetal monitoring during the procedure
Fetal affects of maternal hypoxia
• Fetal heart rate tracing
• Fetal MRI in the later 3rd trimester
Delivery timing
• Gestational age
• Maternal treatment
Fetal Considerations
68

All imaging studies are acceptable in women who are breastfeeding
–Including all contrast agents except radioactive iodine
Aspirin and anti-platelet agents are safe
All anticoagulation agents are safe
Breastfeeding
69

Pregnant women are at increased risk for stroke secondary to physiologic
changes of pregnancy and pregnancy related complications.
The workup for stroke is the same in pregnant population, as the non-
pregnant population, including all imaging studies.
The same treatment modalities may be considered paying special attention
to gestational age of the fetus and risk of bleeding.
All medications are safe to use during breastfeeding.
Conclusions
70

DISCUSSION
http://www.utsouthwestern.edu/education/medical-school/departments/obstetrics-gynecology/index.html

Contacts
Dr. Alberts: [email protected]
Dr. Novakovic: [email protected]
Dr. Patel: [email protected]
Dr. Pride: [email protected]


















