Streptococci Lecture 5
27
Streptococci Lecture 5 Medical Microbiology SBM 2044
description
Streptococci Lecture 5. Medical Microbiology SBM 2044. a -haemolytic. non-haemolytic. b -haemolytic. Streptococcus. Gram-positive. Grow in chains. Non-motile. Facultative anaerobes. 3 types of streptococci classification:. - PowerPoint PPT Presentation
Transcript of Streptococci Lecture 5

StreptococciLecture 5
Medical MicrobiologySBM 2044

Streptococcus Gram-positive Grow in chains Non-motile Facultative anaerobes
• Early studies distinguished 3 broad groups on blood agar• non-haemolytic • -haemolytic • -haemolytic
• Group-specific antigens (Lancefield classification) – by serological reactivity of extracted cell wall antigens (A U)• Species – biochemical tests
3 types of streptococci classification:


• > 100 distinct M types of GAS distinguished since then - called M1, M2, M3, M4,……..etc.
• M-type specific antigen was sensitive to proteases M proteins
Streptococcus pyogenes
Natural habitat: Humans Strains distinguished by M serotyping
• Devised by Lancefield in 1920s, using panels of absorbed sera to hot-HCl extracted antigen, she called “M antigen”
Highly versatile pathogen
• Toxinogenic diseases
• Suppurative infections
• Immunologically-mediated diseases

GAS diseases – changing patterns• Changes in virulence of prevailing GAS strains ?
• Changes in social conditions – less crowding?
Reemergence of severe invasive infections • Sporadic cases since mid-1980s – new virulent strains?• Streptococcal toxic shock
o Some cases associated with obviously severe tissue infectionso Many others – shock following mild or unapparent infections
• Sporadic – implies predisposing factors

Group A Streptococci
Principle sitesof infection:
Pharyngitis, tonsillitis,otitis media, sinusitis.
Local spread (e.g.) Invasive infections
Bacteraemia or septicaemia
Deep-seated tissues
Skin pyroderma, erysipelas
Pharynx
StreptococcalToxic Shock
Occasionally Extensive necrosis(necrotizing fasciitis)
Other tissues
• Puerperal fever (childbirth fever) in women – major killer in past

Follicular tonsillitisTonsillitis
Streptococcus pyogenes

Cellulitis Erysipleas
Streptococcus pyogenes
Impetigo

(< 24 hours post surgery)
Streptococcus pyogenes
Necrotizing fasciitis

Scarlet fever
Streptococcus pyogenes

Group A Streptococci
• Encounter– Carriers appear asymptomatic– Person-to-person spread is mediated by
respiratory droplets or by direct contact to skin• Entry
– For pyodermal infections, streptococci need to gain entry into deeper layers of skin
– In pharyngeal infections, to prevent from being swept away, GAS must adhere to lipoteichoic acid (LTA), protein F and/or M protein

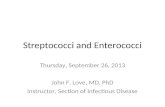
M protein
• Important for cell adherence to keratinocytes
• Prevent opsonization by complement– bind to fibrinogen and interferes with
the alternative pathway– bind with host complement control
proteins and inhibit opsonins formation• Hypervariable regions of M protein
are antigenic, but there are > 100 M protein serotypes

EM showing the M Proteins (hair-like surface structures) of S. pyogenes

Group A Streptococci
• Spread and multiplication– Most GAS remain localised to the site of initial
infection– In pharynx and tonsils, may result in erythema and
exudate associated with strep throat– Peritonsillar abscess (quinsy) or spread to adjacent
structures (mastoid and middle ear)– Impetigo in skin – Erysipelas and cellulitis in deeper layers of skin– GAS may spread laterally in deep tissues, by
secreting enzymes• necrotizing fasciitis and myositis

GAS virulence factors – Excreted products
Cytolytic toxins• Streptolyxin O (SLO)• Streptolysin S (SLS) Produced by all strains
• Both lyse wide range of cells, including PMNs suppuration and/or necrosis
• Various subtle effects at sub-lytic concentrations
-haemolysis• SLO – ‘sensitive’ to O2 • SLS – stable in O2
“Thiol-activated” toxin

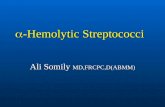
+ 0.5
0.0
- 0.5
- 1.0
- 1.5
- 2.0
- 2.5
WT sloΔ1 sagBΔ1 sloΔ1-sagBΔ1
PBS
Wei
ght g
ain
(gra
ms)
~3 x 109 cfu~3 x 108 cfu~3 x 107 cfu ~3 x 105 cfu
~3 x 106 cfuSterile
SLO- and SLS-defective mutants
murine s.c. model - weight loss at 24h post infection

Hyaluronic acid capsule
• Antiphagocytic structure on bacterial surface
• Hyaluronic acid is abundant in human connective tissue - hence GAS can camouflaged themselves
• But capsule may interfere with the adherence of GAS to epithelial cells– so GAS shed the capsule during the early
stages of infection using hyaluronidase

Secreted protein FunctionProteases
Hyaluronidase spreading factor
Streptolysins S and O form pores in the host membranes
Deoxyribonucleases (DNase)
Streptokinase – bind to human protein plasminogen, and convert this to plasmin
plasmin degrades fibrin

Damage • GAS can evoke an intense inflammatory
responses in tissues• Streptococcal pyrogenic exotoxins (SPE)
– SPE A, B and C cause rash, a characteristic of scarlet fever
– SPE A and C are bacterial superantigens that activate a large subset of T cells
• Immunologically mediated disease (nonsuppurative sequelae) – acute rheumatic fever (ARF)– acute post-streptococcal glomerulonephritis

Toxic Shock
In past – probably linked to scarlet fever
Since mid-1980s – associated with ‘new’ highly virulent strains - rapidly fulminating
• some cases in previously healthy young adults, no obvious predisposing factors
Associated with production of superantigenic toxins, but other factors also involved

• rheumatic heart disease (RHD) (ca 50% cases) - damage to heart valves, permanent scaring in survivors
• antibodies and/or T cells X-react with host antigens? (later)
Acute rheumatic fever (ARF)
autoimmune disease - triggered only by GAS pharyngitis
associated with strong immune response to GAS.
Symptoms arise > 10days + after GAS infection• responsible GAS strain already ‘cleared’
Symptoms may include:• inflammation multiple sites, starting with major joints (arthritis)• neurological disorders (Sydenhams chorea)

Acute rheumatic fever (ARF)
Initial attack rates low (3% in untreated pharyngitis)
Widespread prescription of penicillin for ‘sore throats’
Remarkably, GAS have not (yet ?) developed resistance to penicillins
High recurrence (up to 50%) - increasing in severity

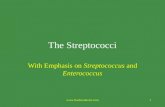
Post-streptococcal acute glomerulonephritis (PSGN):
GAS infections - complications
Common, but rarely life-treating - some GAS infections of either pharynx or skin.
Symptoms arise some 10 days after infection
• Most probably entrapment of GAS antigen-host antibody complexes at basement membranes of glomeruli
• reflect kidney dysfunction, probably involving inflammation of glomeruli
Pathogenesis:
• might also involve an ‘autoimmune’ response

Mesangial cell Mesangial cellintrusionEndothelial
cell, has
Basement membrane
Small complexes diffuse thro’basement membrane into urine, but the occasional larger complexcan’t & is normally removed bymesangial cell
Normal glomerulus Glomerulonephritis
Inflammation
PMN
100 nmpores
Too much large immunecomplex entrapment ?
S. pyogenes infectionsExample: Sequel of some

Treatment and Prevention
• Penicillin – 10 day oral therapy• Erythromycin or other macrolide antibiotics
for individuals allergic to penicillin

Group B streptococci
• Streptococcus agalactiae are aerobic G+ diplococci that are β-haemolytic on blood agar plates– found in lower GIT and female genital tracts– GBS is a leading cause of neonatal sepsis
and meningitis– prevent opsonization and phagocytosis with a
polysaccharide capsule

Enterococci
• Enterococcus faecalis cause UTI, wound infections, endocarditis, intraabdominal abscesses and bacteremia.– Normal flora of GIT and GUT– resistant to bile and high salt concentrations– nosocomial infections– resistance to many antibiotics, often bacteriostatic– bacterial killing must use a combination treatment of
a β-lactam and an aminoglycoside