STRATEGIES OF MUCOADHESIVE DRUG … OF MUCOADHESIVE DRUG DELIVERY SYSTEM- AN UPDATE ON NASAL DRUG...
12
REVIEW ARTICLE Department of Pharmaceutics Amitava et.al / UJPSR / 1 (2), 2015, 23-34 e ISSN: 2454-3764 Print ISSN: 2454-3756 STRATEGIES OF MUCOADHESIVE DRUG DELIVERY SYSTEM- AN UPDATE ON NASAL DRUG DELIVERY Abstract Key words This article gives an idea of bioadhesive delivery systems based on hydrogels to biological surfaces that are covered by mucus. Techniques that are frequently used to evaluate the mucoadhesive drug delivery systems are discussed. Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces. Mucoadhesion is a complex phenomenon which involves wetting, adsorption and interpenetration of polymer chains. The concept of mucoadhesion in drug delivery was introduced in the early 1980s. Thereafter, several researchers have focused on the investigations of the interfacial phenomena of mucoadhesion with the mucus. Nasal mucoadhesive drug delivery systems is one of the most important novel drug delivery systems with its various advantages and it has a lot of potential in formulating dosage forms for various chronic diseases. Nasal delivery is a promising drug delivery option where common drug interactions such as intravenous, intramuscular or oral are inapplicable. Recently it has been shown that many drugs have better bioavailability by nasal route than the oral route. This has been attributed to rich vasculature and highly permeable structure of the nasal mucosa coupled with avoidance of hepatic first-pass elimination, gut wall metabolism and/or destruction in the G.I. tract. Bioadhesive, evaluation techniques, mechanism, nasal mucoadhesives. ARTICLE INFO: Article history: Received: 06 September 2015 Received in revised form: 15 September 2015 Accepted: 1 November 2015 Available online: 10 November 2015 The term bioadhesion refers to any bond formed between two biological surfaces or a bond between a biological and a synthetic surface. In case of bioadhesive drug delivery, the term bioadhesion is used to describe the adhesion between polymers, either synthetic or natural or soft tissues or the gastrointestinal mucosa. In cases where the bond is formed with the mucus the term mucoadhesion may be used synonymously with bioadhesion. INTRODUCTION Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces. Generally speaking, bioadhesion is a term which broadly includes adhesive interactions with any biological or biologically derived substance, and mucoadhesion is used when the bond is formed with a mucosal surface [1-4]. 1 * 1 2 Amitava Roy , Arka Roy, Pallab Kanti Haldar 1 Department of Pharmaceutics, Himalayan Pharmacy Institute, Majhitar, Rangpo, E. Sikkim - 737136, INDIA 2 Department of Pharmaceutical Technology, Jadavpur University, Jadavpur, West Bengal, INDIA Amitava Roy Department of Pharmaceutics Himalayan Pharmacy Institute Majhitar, E-Sikkim-737136, INDIA E-mail: [email protected] Phone: +919733304853 Corresponding Author: www.ujpsr.com 23 nd 2 Issue
Transcript of STRATEGIES OF MUCOADHESIVE DRUG … OF MUCOADHESIVE DRUG DELIVERY SYSTEM- AN UPDATE ON NASAL DRUG...

REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015, 23-34
e ISSN: 2454-3764Print ISSN: 2454-3756
STRATEGIES OF MUCOADHESIVE DRUG DELIVERY
SYSTEM- AN UPDATE ON NASAL DRUG DELIVERY
Abstract
Key words
This article gives an idea of bioadhesive delivery systems based on hydrogels to biological surfaces that are covered by mucus. Techniques that are frequently used to evaluate the mucoadhesive drug delivery systems are discussed. Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces. Mucoadhesion is a complex phenomenon which involves wetting, adsorption and interpenetration of polymer chains. The concept of mucoadhesion in drug delivery was introduced in the early 1980s. Thereafter, several researchers have focused on the investigations of the interfacial phenomena of mucoadhesion with the mucus. Nasal mucoadhesive drug delivery systems is one of the most important novel drug delivery systems with its various advantages and it has a lot of potential in formulating dosage forms for various chronic diseases. Nasal delivery is a promising drug delivery option where common drug interactions such as intravenous, intramuscular or oral are inapplicable. Recently it has been shown that many drugs have better bioavailability by nasal route than the oral route. This has been attributed to rich vasculature and highly permeable structure of the nasal mucosa coupled with avoidance of hepatic first-pass elimination, gut wall metabolism and/or destruction in the G.I. tract.
Bioadhesive, evaluation techniques, mechanism, nasal mucoadhesives.
ARTICLE INFO:
Article history:
Received: 06 September 2015
Received in revised form:
15 September 2015
Accepted: 1 November 2015
Available online: 10 November 2015
The term bioadhesion refers to any bond formed between two biological surfaces or a bond between a biological and a synthetic surface. In case of bioadhesive drug delivery, the term bioadhesion is used to describe the adhesion between polymers, either synthetic or natural or soft tissues or the gastrointestinal mucosa. In cases where the bond is formed with the mucus the term mucoadhesion may be used synonymously with bioadhesion.
INTRODUCTION
Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces. Generally speaking, bioadhesion is a term which broadly includes adhesive interactions with any biological or biologically derived substance, and mucoadhesion is used when the bond is formed with a mucosal surface [1-4].
1 * 1 2Amitava Roy , Arka Roy, Pallab Kanti Haldar
1Department of Pharmaceutics, Himalayan Pharmacy Institute, Majhitar, Rangpo, E. Sikkim - 737136, INDIA
2 Department of Pharmaceutical Technology, Jadavpur University,Jadavpur, West Bengal, INDIA
Amitava Roy
Department of Pharmaceutics
Himalayan Pharmacy Institute
Majhitar, E-Sikkim-737136, INDIA
E-mail: [email protected]
Phone: +919733304853
Corresponding Author:
www.ujpsr.com 23nd2 Issue

Mucoadhesive drug delivery systems includes the following
?Buccal delivery system
?Oral delivery system
?Vaginal delivery system
?Rectal delivery system
?Nasal delivery system
?Ocular delivery system
g g + g cos Qtg = bt bg
g g gtb > bt + bg
The spreading coefficient, S can be given by,b/t
S = g -g -gb/t tg bt bg
MECHANISM OF MUCOADHESION
Mucoadhesion means the attachment of the drug along with a suitable carrier to the mucous membrane. Mucoadhesion is a complex phenomenon which involves wetting followed by adsorption and interpenetration of polymer chains. Mucoadhesion has the following mechanism,
a. Close contact between a bioadhesive and a membrane (wetting or swelling phenomenon),
b. Interpenetration of the bioadhesive into the tissue or into the surface of the mucous membrane.
THEORIES OF MUCOADHESION [4,5]
WETTIBILITY THEORY:
Ability of bioadhesive and mucus to spread and develop intimate contact with its corresponding substrate is an important factor in bond formation. The wetting theory was developed predominantly in regard to liquid adhesives, uses interfacial tensions to predict spreading and in turn adhesion. The study of surface energy of polymers and tissues to predict mucoadhesive performance has been given considerable attention. The contact angle (Q) which should ideally be zero for adequate spreading is related to interfacial tensions (g) as per the Young's equation,
Where the subscripts "tg" and "b" represent tissue, gastrointestinal contents and bioadhesive polymer respectively, for spontaneous wetting to occur,
For the bioadhesion to take place the spreading coefficient must be positive, hence it is advantageous to maximize the interfacial tension at the tissue-GI contents interface and minimizing the surface tension at the other two interfaces. The interfacial tension can be measured by methods like the Wilhelmy plate method. It has been shown that the BG-tissue interfacial tension can be calculated as,
Where the values of F (interaction parameter) can be found in published papers. thus by the wetting theory it is possible to calculate spreading coefficients for various adhesives over biological tissues and predict the intensity of the bioadhesive bond.
ELECTRONIC THEORY[6,9]:
The electronic theory depends on the assumption that the bioadhesive material and the target biological material have different electronic surface characteristics. Based on this, when two surfaces comes in contact with each other, electron transfer occurs in an attempt to balance their Fermi levels, resulting in the formation of a double layer of electrical charge at the interface of the bioadhesive and the biologic surface. The bioadhesive force is believed to be present due to the attractive forces across this double layer.
FRACTURE THEORY:
This is by-far the most accepted theory on bioadhesion. It explains the forces required to separate the two surfaces after adhesion has taken place. It measures the maximum Tensile stress(S ) m
produced during detachment as follows,
Where F and A represents the maximum force of m o
detachment and the total surface area respectively. In a uniform single-component system, fracture strength (s ),which is equal to the maximum stress f
of detachment (s ),is proportional to the fracture m
energy (g ),Youngs modulus of elasticity (E) and c
the critical crack length (c) of the fracture site as follows,
1/2s (g E/c)f c
Fracture energy can be obtained by sum of the reversible work of adhesion, W (work done to r
produce new fracture surfaces) and the irreversible
1/2 g =g +g -2F( )bt b t gbgt
S =F /Am m o
www.ujpsr.com 24nd2 Issue
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756

work of adhesion, W (work of plastic deformation). j
g =W +W c r j
ADSORPTION THEORY [7,9]
This theory state that the bioadhesive bond formed between an adhesive substrate and the tissue is due to the weak Van Der Waals forces and hydrogen bond formation. It is one of the most widely accepted theories of bioadhesion.
DIFFUSION THEORY
The concept of the interpenetration and entanglement of the bioadhesive polymer chains and mucous polymer chains is supported by the diffusion theory. The bond strength increases with the increase in the degree of penetration. This penetration is dependent on the concentration gradients and the diffusion coefficients. It is believed that interpenetration in the range of 0.2-0.5Bm is required to produce effective bond strength. The penetration depth (I) can be estimated
1/2by, I = (tDb)
Where t is the time of contact and D is the diffusion b
coefficient of the bioadhesive material in the mucus
FACTORS AFFECTING MUCOADHESION:
The mucoadhesion of a drug carrier system to the mucous membrane depends on the below mentioned factors [9-12].
?Polymer based factors-Molecular weight of the polymer,
?Concentration of polymer used,
?Flexibility of polymer chains,
?Swelling factor,
?Stereochemistry of polymer,
?Physical factors-
?ph at polymer substrate interface,
?Applied strength contact time
?Physiological factors-
?Mucin turn over rate,
?Diseased state.
?Prolongs the residence time of the dosage
ADVANTAGES OF ORAL MUCOADHESIVE DRUG DELIVERY SYSTEMS [10,13-14]
form at the site of absorption, hence increases the bioavailability.
?Excellent accessibility, rapid onset of action.
?Rapid absorption because of enormous blood supply and good blood flow rates
?Drug is protected from degradation in the acidic environment in the git
?Improved patient compliance
DISADVANTAGES OF MUCOADHESIVE DRUG DELIVERY SYSTEMS
?Occurrence of local ulcerous effects due to prolonged contact of the drug possessing ulcerogenic property
?One of the major limitations in the development of oral mucosal delivery is the lack of a good model for in vitro screening to iden t i fy drugs su i tab le for such administration.
?Patient acceptability in terms to taste, irritancy and mouth feel is to be checked.
POLYMERS USED FOR MUCOADHESIVE DRUG DELIVERY [11, 13-16]
These polymers are classified as,
Hydrophillic polymers: Contains carboxylic group and possess excellent mucoadhesive properties. These are -
?PVP (Poly vinyl pyrrolidine)
?MC (Methyl cellulose)
?SCMC (Sodium carboxy methyl cellulose)
?HPC (Hydroxyl propyl cellulose)
Hydrogels: These swell when in contact with water and adhere to the mucus membrane, these are further classified according to their charge
?Anionic polymers- Carbopol, polyacrylates,
?Cationic polymers- Chitosan
?Neural/non ionic polymers- Eudragit analogues
METHODS OF EVALUATION [11,14,17-19]
Mucoadhesive polymers and drug delivery systems can be evaluated by testing their adhesion strength by both in vitro and in vivo tests.
www.ujpsr.com 25nd2 Issue
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756

In vitro tests [11]
?Methods determining tensile strength
?Methods determining shear stress
?Adhesion weight method
?Fluorescent probe method
?Flow channel method
?Mechanical spectroscopic method
?Falling liquid film method
?Colloidal gold staining method
?Viscometer method
?Thumb method
?Adhesion number
?Electrical conductance
?Swelling properties
?In vitro drug release studies
?Mucoretentability studies
In vivo methods
?Use of radioisotopes
?Use of gamma scintigraphy
?Use of pharmacoscintigraphy
?Use of electron paramagnetic resonance (EPR)oximetry
?X-ray studies
?Isolated loop techniques
These techniques are less common due to high cost, time consuming and ethical factors. But these are important to assess the true mucoadhesive potential especially in the case of oral mucoadhesive drug delivery.
The GI transit time can be measured by using one of the many radio opaque markers like barium sulphate which is coated to the bioadhesive dosage form so as to assess the GI transit by means of X-ray inspection. By means of gamma scintigraphy both the distribution and retention can be studied.
In 1985 Chang et.al. studied the transit of various radio labelled polyacrylic acid beads through the rat GI tract. The beads were fed to the rats and at various time intervals the rats were sacrificed. The rat's intestine was then systemically dissected into
20 equal parts and the amount of radiation in each part measured thus allowing, the transit overtime to be realized. The development of a non invasive technique to determine the transit time of mucoadhesive polymers was done by Davis. The transit time could be imaged via labelling of the polymer with a gamma emitting nucleotide which was determined with the help of gamma scintigraphy [11].
A recent technique by Albrecht et.al. was to use magnetic resonance imaging to localize the point of release of thiolated polymers from dosage forms via the use of gadolinium. In vivo mucoadhesion was determined by ascertaining the residence time of the fluorescently tagged thiomer on intestinal mucosa of rats after 3 hours.
Shear stress method: The measurement of the shear stress gives a direct correlation to the adhesion strength. In a simple shear stress measurement based method two smooth, polished plexi glass boxes were selected; one block was fixed with adhesive araldite on a glass plate, which was fixed on levelled table. The level was adjusted with the spirit level. To the upper block, a thread was tied and the thread was passed down through a pulley, the length of the thread from the pulley to the pan was 12cms. At the end of the thread a pan of weight 17 gms was attached into which the weights can be added. A recent method involves the measurement of mucoadhesion by use of a stainless steel rotating cylinder which was coated with freshly excised porcine intestinal mucosa to which polymer discs were attached. The cylinder was placed in a dissolution apparatus and rotated at 125rpm. It was analysed every 30 minutes for the attachment of the polymer discs [9,14].
Detachment force measurment: The Wilhelmy plate method is one of the traditional methods for the measurement of the force of adhesion of bioadhesive dosage forms. The method involves the measurement of the dynamic contact angle and utilizes a microtensiometer and a microbalance. The CAHN dynamic contact angle analyzer is used for this purpose. Wilhelmy plate method measures the bioadhesive force between the mucosal tissue and the polymer/dosage form attached to a metal wire and suspended into the microtensiometer. The mucosal tissue (usually rat jejunum) is used which placed in the tissue chamber, this chamber is raised so as to make contact between the tissue and the test material. After a certain period (7 mins for
www.ujpsr.com 26nd2 Issue
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756

microspheres) the stage is lowered and the force of adhesion is measured. This apparatus measures the following parameters [11,12].
Fracture strength: Its defined as the force per unit area required to break the adhesive bond.
Deformation to failure: It is the distance required to move the stage before complete separation occurs [12,14].
Two new methods used for the measurement of the force of attachement are the modified Wilhelmy plate method and the modified dual tensiometer method .
The modified Wilhelmy plate method consists of a glass plate which is coated with the polymer layer, suspended from a microbalance into a beaker containing mucus. The work done to detach the polymer from the mucus is found. This system has the demerit of not involving any living tissue. The modified dual tensiometer method was developed by Leung and Robinson. The texture analyzers have also been used like the TA-XT2 analyzer.
Swelling studies: Buccal adhesive dosage forms were weighed individually (w1) and separately in petridishes containing 4 ml of phosphate buffer ph 6.6. at regular intervals (.5,1,2,3,4,5,6 hours) the dosage forms were removed from the petridishes and excess surface water was removed using filter paper. The dosage form wee reweighed and swelling index (SI) was calculated as follows,
SI = (W2-W1)/W1
In vitro drug release [20]: These are performed in phosphate buffer ph 6.6, 150 ml at 37c in a modified dissolution apparatus which consist of a 250 ml beaker and a glass rod attached with a grounded glass disk (2 cm diameter) as a donor tube. The back surface of the NBAS was attached to the glass disk with an adhesive cynoacrylate adhesive. The donor tube was dipped into the medium and stirred at constant rpm 5ml aliquots were withdrawn at preset times (.08,.16.1,2,3,4,5,6 hours),filtered through a 0.2 micron filter and absorbance measured at 290 nm.
Rheological measurement of mucoadhesion[19-20] Madsen and colleagues determined the interactions between four mucoadhesive and a homogenized mucus gel. Using a dynamic rheological method it was seen that the incorporation of a mucoadhesive polymer into mucus produced rheological behavior that was indicative of a weakly cross linked gel.
Novel electromagnetic force transducer technique: It is remote sensing instrument that utilizes a calibrated electromagnet to detach a magnetic loaded polymer from a tissue. It measures the adhesive force by monitoring the magnetic force required to exactly oppose bioadhesive force.
Tests for mucoadhesive microspheres [18-20]
Adhesion number- It is the ratio of number of particles attached to the substrate to the total number of applied particles. It is expressed as percentage.
Falling liquid film method: It is a quantitative, in-situ technique. In this method the percentage of particles which get retained on a mucosal tissue, spread on a plastic slide in an inclined position, when a suspension of the microspheres is allowed to flow down the tissue. The quantification can be done by the aid of coulter-current method.
Other in vitro tests: Park and Robinson determined the effect of various polymer and mucin interactions via the use of fluorescent probes. This technique involved the labelling of the lipid bilayer of cultured human conjunctiva cells with the fluorescent probes pyrene. The adhesion caused a change in the degree of fluorescent which was proportional to the polymer binding [17].
Batchelor and co workers designed a technique in which fluorescently labelled alginate solutions of known rheological profile were delivered onto porcine oesophageal tissue. A washing solution to mimic flow was selected and it was seen that the 20% of the dose remained in contact with the tissue for upto 30 mins.
Another imaging technique that did not involve fluorescence was developed by Kockisch and colleagues. Here investigators developed a semi quantitative image analysis based on the technique for the in vitro and in vivo detections of polymers with an affinity for the mucosal surfaces of the oral cavity.
Takeuchi and co workers measured the mucoadhesion of different polymers via the BIACORE instrumentation. This system was based on the optical phenomenon of surface plasmon resonance (SPR).
Strategies of drug delivery through the nasal mucosa:
A midline septum divides the human nasal cavity into two non-connected chambers. Each chamber
www.ujpsr.com 27nd2 Issue
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756

consists of three regions: Firstly, the vestibule consisting of the region just inside the nostrils with
2an area of about 6 cm . Secondly, the olfactory region, which in man is situated in the roof of the nasal cavity covers about 10% of the total nasal area
2of 150 cm and thirdly the respiratory region which constitutes the remaining region. The respiratory region contains three nasal turbinates, the superior, the middle and the inferior which project from the lateral wall of each half of the nasal cavity. The presence of these turbinates creates a turbulent airflow through the nasal passages which ensures a better contact between the inhaled air and the mucosal surface. Similar, more or less complex turbinate structures are present in all animal models normally used for nasal delivery studies.
The nasal vestibule is covered with stratified squamous epithelium which gradually changes
posteriorly into a pseudostratified columnar epithelium that covers the respiratory epithelium. The respiratory epithelial cells are covered by microvilli and the major part of these cells is also covered with cilia. These cilia, which are long (4-6 mm) thin projections, are mobile and beat with a frequency of 1000 strokes per min. The beat of each cilium consists of a rapid forward movement, where the cilium is stretched and the tip of the cilium reaches into the nasal mucus layer and carries this forward followed by a mucosa has a metabolic capacity that will help slow return beat, where the cilium is bent and moves in the sol layer that lies beneath the mucus layer. In this way the mucus layer is propelled in a direction from the anterior towards the posterior part of the nasal cavity. The mucus flow rate is in the order of 5 mm per min and hence the mucus layer is renewed every 15 - 20 min.
www.ujpsr.com 28nd2 Issue
Figure 1. Structure of the nasal cavity
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756

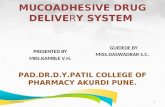
Figure 2. Human Nasal mucosa: Cell types of the nasal epithelium showing ciliated cell (A), nonciliated cell (B), goblet cell (C), gel mucus layer (D), sol layer (E), basal cell (F) and basement membrane (G) (16)
Nasal sectionsEpithelial Characteristics
Cells / FunctionsSurface area Vascularization Permeability
Poor Low20.6 cm
Stratified squamous and keratinized epithelial cells with nasal hairs/ Supportand protection
Vestibule
Atrium Low Reduced-
Stratified squamous cells / Support Pseudostratified cells / Support
Columnar non ciliated cells / Support Columnar ciliated cells / Support andmuciliary clearanceGoblet cells / Mucus secretionBasal cells / Progenitors of other cell types
Good Very high 2130 cmRespiratory
region
Table 1. Human nasal epithelium characteristics
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756
www.ujpsr.com 29nd2 Issue
Olfactory
region
Sustentacular cells / Support Olfactory receptor cells / Olfaction perceptionBasal cells / Progenitors of other cell Types
215 cm High Direct access to CNS

Mechanisms of transport of drugs via nasal
mucosa
Transport across the nasal mucosa is effected either
by olfactory pathway or trigeminal pathway[21-24]
Olfactory pathway
The olfactory epithelium is a gateway for
substances entering the CNS and the peripheral
circulation. It can broadly classify the pathways
into two possible routes from the olfactory mucosa
in the nasal cavity into the CNS along the olfactory
neurons: the intraneuronal pathway or olfactory
nerve pathway (axonal transport) and extraneuronal
pathway, i.e. the olfactory epithelial pathway.
Agents that are able to enter the olfactory receptor
cells, by endocytotic or pinocytotic mechanisms,
could utilize the olfactory nerve pathway and thus
be transported by intracellular axonal transport to
the olfactory bulb. The axonal transport requires a
long time for drugs to reach different brain regions.
Mouse hepatitis, vesicular stomatitis, viruses and
agglutinin-conjugated horseradish peroxidase have
been shown to enter the brain by axonal transport.
Axonal transport of endogenous substances, in
either the anterograde or retrograde direction, is a
well-known phenomenon. Anterograde transport
may be either fast (20-400 mm/day) or slow (0.1 - 4
mm/day), depending on the substance that is being
transported. Further, the transport rate also varies in
different animal models. Retrograde transport,
which involves pinocytotic vesicles, lysosomal
organelles and mitochondria, occurs at a rate similar
to that of the fast anterograde transport. The
extraneuronal pathway probably relies on bulk flow
transport through perineural channels, which
deliver drug directly to the brain parenchymal
tissue, or to the cerebrospinal fluid, or to both. This
extraneuronal pathway allows therapeutic agents to
reach the CNS within minutes. In this pathway, the
substance must first cross the olfactory epithelium.
The general transport mechanisms across the
olfactory epithelium are similar to those across
other types of epithelium. The substance could be
absorbed by passive diffusion through the
supporting cells or Bowman's glands or could be
transported by a paracellular route through the tight
junctions between the supporting. After entering the
lamina propria, adjacent to the olfactory neurons,
the substance could then enter the perineural space
and reach the CNS. This extracellular pathway relies
on the anatomical connection between the nasal
submucosa and the subarachnoid space. The
perineural space around the olfactory neurons is an
extension of the subarachnoid space and the fluid in
the perineural space is in direct contact with the CSF.
Transport of substances into the CNS via the
epithelial pathway could thus be more rapid than
that via axonal transport. It is likely that smaller
compounds that appear rapidly in the CSF after
nasal administration have been transported through
this pathway.
Trigeminal pathway
Trigeminal neural pathway also may be involved in
rapidly delivering protein therapeutic agents, such
as insulin-like growth factor-I to the brain and spinal
cord following intranasal administration. The
trigeminal nerves innervating areas of the nasal
cavity are responsible for most chemo perception
other than olfaction and sense diverse stimuli,
including hot spices, formaldehyde and other
chemicals.
Factors influencing nasal drug absorption[23,26]
A) Factors Related to Drug
a) Lipophilicity
Increasing lipophilicity, increases the permeation of
the compound through nasal mucosa. Although the
nasal mucosa was found to have some hydrophilic
character, it appears that these mucosae are
primarily lipophilic in nature and the lipid domain
plays an important role in the barrier function of
these membranes [19]. A number of lipophilic drugs
such as naloxone, buprenorphine, testosterone [20]
and 17a-ethinyloestradiol [21], have been reported
to be completely or almost completely absorbed
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756
www.ujpsr.com 30nd2 Issue

nasally in animal models. A correlation between lipophilicity and nasal drug absorption has been
demonstrated using several compounds[22].
b) Chemical Form
The chemical form of a drug can play an important role in determining absorption. For example, conversion of the drug into a salt or ester form can alter its absorption. Huang et al. [23] studied the effect of structural modification of drug on absorption. It was observed that in situ nasal absorption of carboxylic acid esters of L-Tyrosine was significantly greater than that of L-Tyrosine.
c) Polymorphism
Polymorphism affects the dissolution rate and solubility of drugs and thus their absorption through biological membranes. It is therefore advisable to study the polymorphic stability and purity of drugs for nasal powders and/or suspensions [24].
d) Molecular Weight
In the case of lipophilic compounds, a direct relationship exists between the molecular weight and drug permeation whereas water soluble compounds bear an inverse relationship. Based on the reports of Fisher et al and Yamamoto et al. it can be concluded that the permeation of drugs less than 300 Dalton is not significantly influenced by the physicochemical properties of the drug, which will mostly permeate through aqueous channels of the membrane. On the contrary, the rate of permeation is highly sensitive to molecular size for compounds with molecular weight = >300 Da.
e) Partition Coefficient and pKa
According to the pH partition theory, unionized species are absorbed better compared with ionized species and the same holds true in the case of nasal absorption. Jiang et al. conducted a study to determine the quantitative relationship between the physicochemical properties of drugs and their nasal absorption, using diltiazem hydrochloride and paracetamol as model drugs. The results showed that a quantitative relationship existed between the partition coefficient and the nasal absorption constant.
f) Solubility & Dissolution Rate
Drug solubility and dissolution rates are important
factors in determining nasal absorption from powders and suspensions. The particles deposited in the nasal cavity need to be dissolved prior to absorption. If a drug remains as particles or is cleared, no absorption takes place.
B) Factors Related to Formulation [26-29]
Physicochemical Properties of the Formulation
a) pH and mucosal irritancy
The pH of the formulation, as well as that of nasal surface, can affect a drug's permeation. To avoid nasal irritation, the pH of the nasal formulation should be adjusted to 4.5-6.5. In addition to avoiding irritation, it causes efficient drug permeation and prevents the growth of bacteria.
b) Osmolarity
Ohwaki et al. studied the effect of osmolarity on the absorption of secretin in rats and found that absorption reached a maximum at a sodium chloride concentration of 0.462 M, because shrinkage of the nasal epithelial mucosa was observed at this salt concentration. This leads to increased permeation of the compound resulting from structural changes and was further confirmed when sorbitol was used as an osmoregulatory agent. The authors found that permeation of secretin subsequently decreased and, therefore, isotonic solutions are usually preferred for administration.
c) Viscosity
A higher viscosity of the formulation increases contact time between the drug and the nasal mucosa thereby increasing the time for permeation. At the same time, highly viscous formulations interfere with the normal functions like ciliary beating or mucociliary clearance and thus alter the permeability of drugs.
Nasal permeation enhancers
Permeation enhancers are generally a class of chemical compounds which help to increase the permeation of the drug from the dosage form into the systemic circulation via the nasal mucosa. They are classified as physical and chemical enhancers. Chemical enhancers act by destroying the nasal mucosa, very often irreversibly, whereas physical enhancers affect nasal clearance reversibly by forming a gel. The enhancing effect continues until
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756
www.ujpsr.com 31nd2 Issue

the gel is swallowed.
These enhancer systems work by a variety of mechanisms but generally change the permeability of the epithelial cell layer by modifying the phospholipid bilayer, leaching out protein from the membrane or even stripping off the outer layer of the mucosa. Some of these enhancers also have an effect on the tight junctions and/or work as enzymatic inhibitors [29]. Some of the nasal enhancers are discussed below:
Cyclodextrins
Cyclodextrins have been investigated for their nasal absorption enhancement potential. The most studied types are: á-cyclodextrin, â-cyclodextrin, ã-c y c l o d e x t r i n , m e t h y l c y c l o d e x t r i n a n d hydoxypropyl â-cyclodextrin. Only â-cyclodextrin is reported to be a compendial substance and is being considered for a GRAS (generally recognised as safe) status for nasal delivery. The effects of a dimethyl-â-cyclodextrin powder formulation on intranasal insulin absorption were studied in healthy subjects and patients with insulin-dependent diabetes mellitus (IDDM). Mean absolute bioavailabilities of 3.1% and 5.1% were achieved in healthy subjects and diabetics, respectively. Actually cyclodextrin increased nasal bioavailability of insulin by acting on tight junctions of nasal mucosa and facilitating paracellular transport of insulin.
Fusidic acid derivatives
Sodium tauro-24, 25-dihydrofusidate (STDHF) is the most extensively studied among the derivatives of fusidic acid. On the basis of its characteristics, STDHF was considered a good candidate for the transnasal delivery of drugs such as insulin, growth hormone and octreotide. Lee and colleagues determined the radioimmunoactive bioavailability of intranasal salmon calcitonin in 10 healthy human volunteers. The improved nasal absorption of calcitonin in the presence of STDHF showed a limited transient irritation of the nasal mucosa in some subjects. Intranasal administration of human growth hormone (hGH) in combination with STDHF at 1% concentration was studied in patients with hGH deficiency. It was found that in combination with STDHF, the plasma peak of hGH was similar to the endogenous peak. Laursen and co workers prepared various formulations for determining the absorption of growth hormone in
h u m a n s u b j e c t s u s i n g d i d e c a n o y l - L -phosphotidylcholine (DDPC) as an enhancer with different concentrations: 0, 4, 8, and 16%. It was observed that increasing the relative concentration of DDPC increases the absorption of nasally administered hGH. Drejer et al studied the intranasal administration of insulin with DDPC in healthy human volunteers. They found that intranasal insulin was absorbed in a dose dependent manner with slight or no nasal irritation [29].
Phosphatidylcholines (PC)
Phosphat idylchol ines are surface-act ive amphiphilic compounds produced in biological membranes and liposomes. It has been reported that these phospholipids can be used as enhancers for systemic nasal drug delivery. Newman et al investigated the distribution of a nasal insulin formulation containing DDPC labelled with 99mTc-human serum albumin (99mTc-HSA) in human volunteers. From the scintigraphic data, the entire dose from the spray was shown to be deposited in the nasal cavity with no deposition in the lungs even after 4 h. The Novo Nordisk study group reported encouraging results following the nasal administration of an insulin/ DDPC microemulsion formulation in human volunteers. The study demonstrated good absorption of insulin whilst preventing or minimizing nasal irritation.
Bile salts and surfactants
Commonly used bile salts are sodium cholate, sodium deoxycholate (SDC), sodium glycocholate (SGC), sodium taurocholate (STC), sodium taurodeoxycholate and sodium glycodeoxycholate. Yokosuka et al reported a study in which healthy volunteers were administered nasal solutions of insulin and 1% SGC. Significant decreases in serum glucose concentrations were observed and there was a positive correlation between the peak serum insulin levels and the dose of insulin applied. Hirata et al investigated the efficacy of a nasal insulin formulation containing 1% SGC in healthy volunteers and diabetic patients. The nasal formulation resulted in rapid increases in serum insulin levels and decreases in blood glucose levels in healthy volunteers and diabetics. A nasal solution formulation of insulin and 1% SGC, administered as a spray, resulted in a monophasic increase in serum insulin levels. Salzman and colleagues investigated the efficacy of 1% laureth-9 in enhancing the nasal
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756
www.ujpsr.com 32nd2 Issue

absorption of insulin in patients with IDDM and non-diabetic controls. Insulin was shown to be rapidly absorbed via the nasal route lowering plasma glucose levels to 50% of basal values after 45 min in normal subjects compared to 50% in 120 min in diabetics [27-30].
CONCLUSION
The phenomenon of mucoadhesion is a novel controlled drug delivery approaches. The various advantages of the oral mucoadhesive drug delivery systems like prolongation of the residence time of the drug which in turn increases the absorption of the drug are important factors in the oral bioavailability of many drugs. A number of both in vitro and in vivo techniques have been developed for the evaluation of the mucoadhesive drug delivery systems. Mucoadhesive dosage forms extend from the simple oral mucosal delivery to the nasal, vaginal, ocular and rectal drug delivery systems. The most widely studied and accepted polymers for mucoadhesion have been the
hydrophilic, high molecular weight, anionic molecules like carbomers. Recently the focus has been on the novel second generation polymers like the thiolated polymers, lectins and lecithins. Nasal mucosa has been considered as a potential administration route to achieve faster and higher levels of drug absorption. This is because the nasal mucosa is permeable to more compounds than the gastrointestinal tract due to lack of pancreatic and gastric enzymatic activity, neutral pH of the nasal mucus and less dilution by gastrointestinal contents. It is easily accessible and suitable for self-medication. During the past several decades, the feasibility of drug delivery via the nasal route has received increasing attention from pharmaceutical scientists and clinicians. Many review articles describing the anatomy and physiology of human nose are available. Our endeavour in this article was to highlight the anatomy and physiology along with the technical aspects involved in nasal mucoadhesion.
1. 1. S. Ganga, Mucosal drug delivery- a review, vol.5, issue 6, 2007. http // www.pharmainfo.net. Accesed on 08/07/2010.
2. Andrews G.P., Laverty T.P., Jones D.S. Mucoadhesive polymeric platforms for controlled d r u g d e l i v e r y , E u r . J . P h a r mBiopharm.,71: 505-518, 2009.
3. Chowdhary K.P.R., Srinivas L., Mucoadhesive drug delivery systems: A review of current status. Indian drugs.,37 (9):400-406, 2000.
4. Gandhi R.B., Robinson J.R., Bioadhesion in drug delivery. Ind. J. Pharm. Sci., 50(3):145-152, 1988.
5. N.A. Peppas., P.A. Buri., Surface, interfacial and molecular aspects of polymer bioadhesion on soft tissue. J Controlled Release, 2 :257-275, 1985.
6. A.G. Mikos, N.A. Peppas, Measurement of the surface tension of mucin solutions. Int. J. Pharm, 53: 1-5, 1989.
7. A. Baszk in , J .E . P rous t , P.Monsengo , M.M.Boissonnade, Wettability of polymers by mucin aqueous solutions. Biorheology, 27:503-514, 1990.
8. C.M. Lehr, H.E. Bodde, J.A. Bowstra, H.E. Junginger, A surface energy analysis of mucoadhesion. II. Prediction of mucoadhesive performance by spreading coefficients. Eur. J. Pharm. Sci, 1:19-30, 1993.
9. C.M. Lehr, H.E. Bodde, J.A. Bowstra, H.E. Junginger, A surface energy analysis of mucoadhesion: Contact angle measurements on polycarbophil and pig intestinal mucosa in physiology relevant fluids, Pharm Res, 9:70-75, 1992.
10. R.T. Spychal, J.M Marrero, S.H. Saverymuttu, T.C. Northfield. Measurement of the surface hydrophobicity of human gastro-intestinal mucosa. Gastroenterology, 97:104-111, 1989.
11. D.H. Kaelble, J. Moacanin. A surface energy analysis of bioadhesion. Polymer, 18:475-482, 1977.
12. K.V. Ranga Rao, P. Buri. Bioadhesion and factors affecting the bioadhesion of microparticles. In: High Performance Biomaterials, M. Szycher, Lancaster PA, (eds.), Technomic Publishing Company, New York, 1988, pp. 259-268.
13. C.T. Reinhart, N.A. Peppas. Solute diffusion in swollen membranes. Part II. Influence of crosslinking on diffusive properties. J. Mat. Sci. 18: 227-239, 1984.
14. B.O. Baetup. Surface Chemistry and adhesion. Int. J. Adhesive, July: 233-239, 1989.
15. S. Wu. Surface and interfacial tensions of polymer melts. II. Poly (methyl methacrylate), poly (n- butyl methacrylate) and polystryrene. J. Phys. Chem., 74:632-638, 1989.
REFERENCES
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756
www.ujpsr.com 33nd2 Issue

16. R. J. Good. Spreading pressure and contact angle. J Colloid Interface Sci., 52: 308-313, 1975.
17. J.W. Lee, J.H. Park, J.R. Robinson, Bioadhesive based dosage forms: the next generation, J. Pharm. Sci, 89:850-866, 2000.
18. B.V. Derjaguin, Y.P. Toporov, V.M. Muller, I.N. Aleinkova. On the relationship between the molecular component of the adhesion of elastic particles to a solid surface. J. Colloid Interface Sci., 58:528-533, 1966.
19. Mathiowitz E, Chickering D.E., Definitions, Mechanisms and theories of bioadhesion, In: Bioadhesive Drug Delivery Systems, Fundamentals, Novel Approaches and Development, Mathiowitz E, Chickering III D.E., Lehr C.M., (eds.), Marcel Dekker Inc. New York, 2010, PP. 4-8.
20. H.W. Kammer. Adhesion between polymers. Acta Polym, 34: 112, 1983.
21. Zhang L, Parsons DL, Navarre C, Kompella UB. Development and in-vitro evaluation of sustained release Poloxamer 407 (P407) gel formulations of ceftiofur. J Control Release 2002; 85: 73-81.
22. Choi HK, Jung JH, Ryu JM, Yoon SJ, Oh YK, Kim CK. Development of in-situ gelling and mucoadhesive acetaminophen liquid suppository. Int J Pharm 1998; 165: 33-44.
23. Ozbilgin ND, Saka OM, Bozkir A. Preparation and in vitro/ in vivo evaluation of mucosal adjuvant in situ forming gels with diphtheria toxoid. Drug Deliv 2014; 21: 140-7.
24. Schmolka IR. Artificial skin. I. Preparation and properties of Pluronic F-127 gels for the treatment of burns. J Biomed Mater Res 1972; 6: 571-82.
25. Xu X, Shen Y, Wang W, Sun C, Li C, Xiong Y, Tu J. Preparation and in-vitro characterization of thermosensitive and mucoadhesive hydrogels for nasal delivery of phenylephrine hydrochloride. Eur J Pharm Biopharm 2014; 88: 998-1004.
26. Lin H, Gebhardt M, Bian S. Enhancing effect of surfactants on fexofenadine HCl transport across the human nasal epithelial cell monolayer. Int J Pharm 2007; 330: 23-31.
27. Majithiya RJ, Ghosh, PK, Umrethia ML, Murthy RS. Thermoreversible-mucoadhesive gel for nasal delivery of sumatriptan. AAPS Pharm Sci Tech 2006; 7: 67.
28. Miyazaki S, Nakamura T, Yokouchi C, Takada M. Effect of Pluronic gels on the rectal absorption of indomethacin in rabbits. Chem Pharm Bull 1987; 35: 1243-8.
29. Türker S, Onur E, Özer Y. Nasal route and drug delivery systems. Pharm World Sci 2004; 26: 137-42.
30. Mahdi MH, Conway BR, Smith AM. Development of mucoadhesive sprayable gellam gum fluid gels. Int J Pharm 2015; 488: 12-9.
REVIEW ARTICLE
Department of Pharmaceutics
Amitava et.al / UJPSR / 1 (2), 2015,
23-34e ISSN: 2454-3764
Print ISSN: 2454-3756
www.ujpsr.com 34nd2 Issue