
STRATEGIES FOR PREVENTION AND CONTROL OF DIABETES · STRATEGIES FOR PREVENTION AND CONTROL OF...
28
S TRATEGIES FOR PREVENTION AND CONTROL OF DIABETES Marti Macchi, MEd, MPH Senior Consultant National Association of Chronic Disease Directors
Transcript of STRATEGIES FOR PREVENTION AND CONTROL OF DIABETES · STRATEGIES FOR PREVENTION AND CONTROL OF...

STRATEGIES FOR PREVENTION AND
CONTROL OF DIABETES
Marti Macchi, MEd, MPH
Senior Consultant
National Association of Chronic Disease Directors

National Association of Chronic Disease
Directors
• National public health association
• Provides a national forum for chronic disease prevention and control efforts
• Founded in 1988
• Headquartered in Atlanta, GA
– 11 professional staff
– 25 national content experts
• 1,500 members

Mission Statement
The National Association of Chronic
Disease Directors provides state-
based leadership and expertise for
chronic disease prevention and
control at the state and national
level.
and US

Integrative Values
�Collaborative
�Partnerships
�Member Driven
Crosses ALL programs,
projects, and strategies

Today’s Presentation
• The Diabetes Problem
• National Diabetes Program Framework
• State Diabetes Systems (DPCPs)
• Diabetes Policy Implications and
Opportunities
• Call to Action and Next Steps to address the
Diabetes Problem

Diabetes: Recognizing the
Problem

Diabetes in the United States
Centers for Disease Control and Prevention. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011.

Number and Percentage of U.S. Population with Diagnosed Diabetes, 1958-2009
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics

Cost of Diabetes
• $174 billion: Total costs of diagnosed diabetes
in the United States in 2007
• $116 billion for direct medical costs
• $58 billion for indirect costs (disability, work
loss, premature mortality)
After adjusting for population age and sex differences,
average medical expenditures among people with
diagnosed diabetes were 2.3 times higher than what
expenditures would be in the absence of diabetes

Estimated lifetime risk of developing diabetes for
individuals born in the United States in 2000
0
10
20
30
40
50
60
Men Women
Perc
en
t
Total Non-Hispanic WhiteNon-Hispanic Black Hispanic
Narayan et al, JAMA, 2003
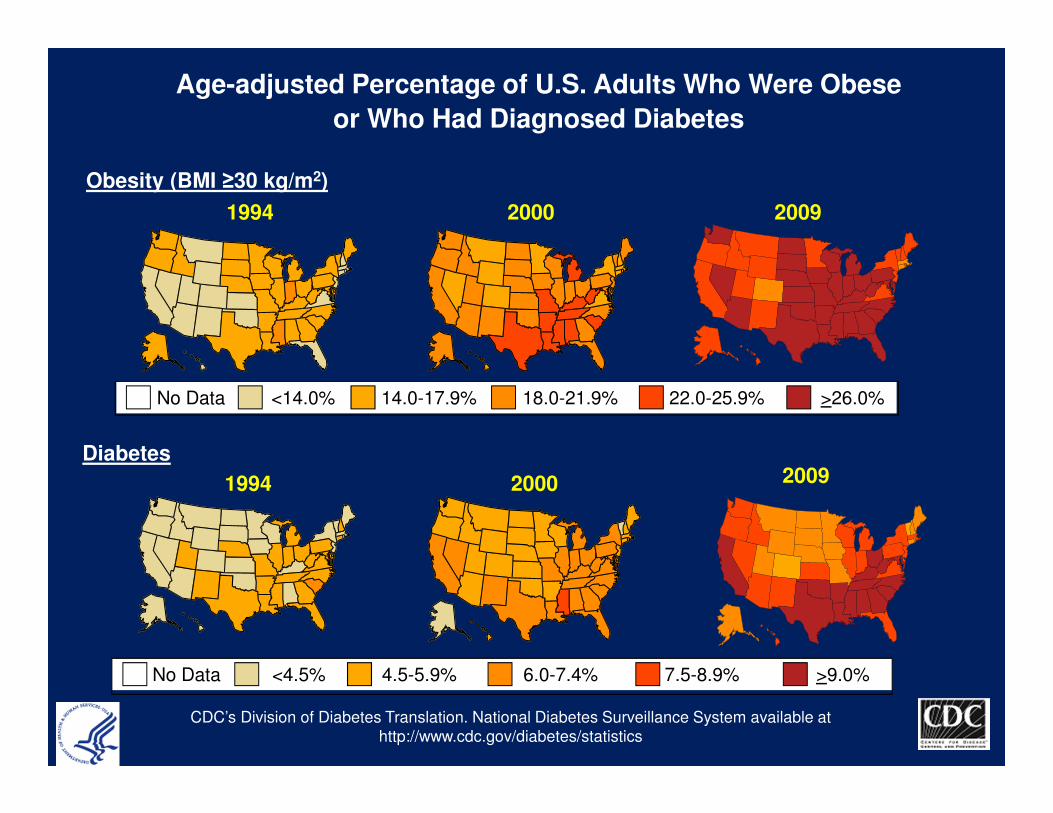
Age-adjusted Percentage of U.S. Adults Who Were Obese
or Who Had Diagnosed Diabetes
Obesity (BMI ≥30 kg/m2)
Diabetes
1994
1994
2000
2000
No Data <14.0% 14.0-17.9% 18.0-21.9% 22.0-25.9% >26.0%
No Data <4.5% 4.5-5.9% 6.0-7.4% 7.5-8.9% >9.0%
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at
http://www.cdc.gov/diabetes/statistics
2009
2009

At Risk and Pre-Diabetes
• Obesity
• Pre-diabetes
– About 35% of adults
– Generally, less than 10% are aware

26 millionwith Diabetes
79 millionwith Prediabetes

Management and Complications
Management
• Dilated Eye Exam
• Foot Exam
• Immunizations
– Influenza
– Pneumococcal
– Hepatitis B
• Self-glucose monitoring
Complications
• Blindness
• Amputations
• End Stage Renal Disease
• Cardiovascular Disease

We’re only touching the surface!
• People with diabetes complications
• People with diagnosed diabetes
• People with undiagnosed diabetes
• People with Prediabetes
• People at risk for diabetes

National Diabetes Program
Framework
• Prevent Diabetes
• Prevent the complications, disabilities
and burden associated with diabetes
• Eliminate diabetes-related health
disparities
• Maximize organizational capacity to
achieve the National Diabetes Program
goals

State Diabetes Prevention and Control
Programs (DPCP)
Three Intervention Areas • Policy and Environmental Change
– Creating supportive community environments to help people take
responsibility for their health
• Health Systems Change
– Improving use and delivery of quality clinical preventive services to
promote health and improve disease detection and management
• Community and Clinical Linkages
– Building a stronger connection between clinical and community
settings; implementing community programs like the National
Diabetes Prevention Program to improve quality of life and reduce
health care costs
Improve A1C, Blood Pressure, Cholesterol and Smoking (ABCS)

Identifying Solutions

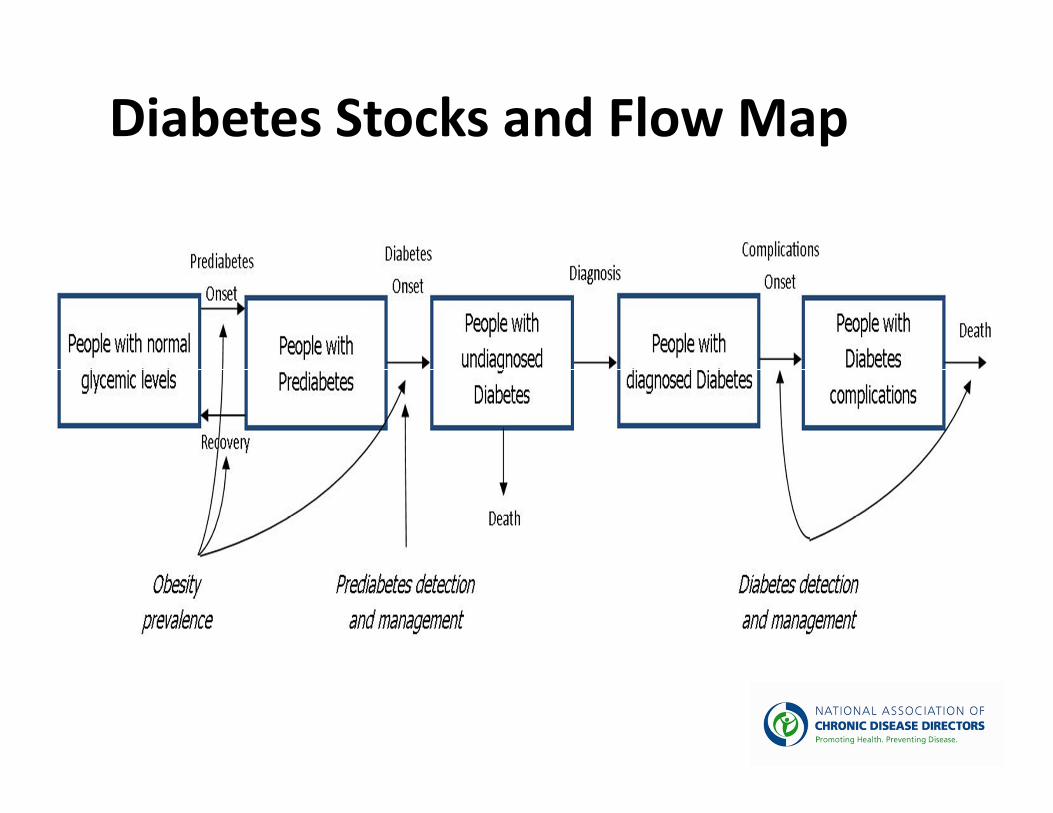
Diabetes Stocks and Flow Map

Strategy #1: Improve quality of clinical care for people
with and at risk for diabetes to improve control of
ABCSPolicy-related Strategies:
� Support implementation of policies within health care organizations that contribute to
and help sustain quality care improvements for people with diabetes/pre-diabetes.
� Support implementation or maintenance of evidence-based reimbursement strategies
and policies (e.g., reduced patient insurance copayments; public insurance
reimbursement of medications and testing supplies; physician reimbursement
incentives and performance-based payment; value-based insurance designs; assistance
for un- or underinsured patients with diabetes.)
Clinical/Health Systems-related Strategies:� Promote the adoption of models to improve delivery and quality of care in clinical
settings (e.g., Patient Centered Medical Home, Planned Care Model).
Communication/Media-related Strategies:� Support health communication efforts that reinforce the interventions listed above to
improve quality of clinical care for people with and at risk for diabetes.

Strategy #2: Increase access to sustainable self-management education and support services for people with diabetes to improve control of ABCS
Policy-related Strategies:
� Support implementation of policies that promote financial
sustainability/reimbursement for DSME/CDSM programs.
� Support implementation of policies that promote financial
sustainability/reimbursement for CHWs involved in providing self-
management education and support services for people with diabetes.
Clinical/Health Systems-related Strategies:
� Expand the role of allied health professionals (e.g., pharmacists,
nurses, community health workers [CHWs]) in providing diabetes self-
management education (e.g., Asheville Model).
Communication/Media-related Strategies:
� Support health communication efforts that reinforce the interventions
listed above to increase access to sustainable self-management
education and support services for people with diabetes.

Strategy #2 (cont.): Increase access to sustainable self-management education and support services for
people with diabetes to improve control of ABCS
Community-related Strategies:
� Expand reach/spread of diabetes self-management education (DSME)
and chronic disease self-management support (CDSM) programs in
community settings to reach vulnerable populations with greatest
diabetes burden/risk.
� Support implementation of policies/environmental supports within
worksites that contribute to improved control of A1C, blood pressure,
and cholesterol, and promote tobacco cessation among people with
diabetes.
� Increase access to tobacco cessation services for people with diabetes
who smoke (e.g., quitlines, etc.).

Strategy #3: Increase access to sustainable, evidence-based
lifestyle interventions to prevent/delay onset of type 2
diabetes among people at high risk
Community-related Strategies:
� Increase access/availability and use of the 16-session core and 6-
session post-core lifestyle program as an intervention targeting
populations with multiple diabetes risk factors including but not
limited to women with previously diagnosed gestational diabetes.
� Facilitate access to safe, attractive, and affordable places for people
with prediabetes or multiple diabetes risk factors to engage in physical
activity, including but not limited to promotion of workplace policies
and programs that increase physical activity.
Policy-related Strategies:
� Partner with employers and health plans to offer the 16 session core
and 6 session post-core lifestyle program as a covered benefit to
prevent or delay onset of diabetes.

Strategy #3 (cont.): Increase access to sustainable, evidence-based lifestyle interventions to
prevent/delay onset of type 2 diabetes among people at high risk
Clinical/Health Systems-related Strategies:
� Implement systems to increase provider referrals of people with pre-
diabetes or multiple diabetes risk factors to sites providing the 16
session core and 6 session post-core lifestyle intervention program.

NACDD Support to State Programs• 3 Full Time Consultants
– Link to the states
– Technical assistance and support
• Policy State Technical Assistance Team (PSTAT)
– Policy training to address emerging policy issues
• Diabetes Policy Workshops
– Integrated educational forum focused on the foundational knowledge
of policy change to
– Goal is to enhance state-based programming and regional
collaboration among state Diabetes Prevention and Control Programs
and their partners.
• Diabetes Council
– Influencing decisions
– Making Connections
– Building Capacity

QUESTIONS?

For Additional Information
���� 2872 Woodcock Blvd. Suite 220 Atlanta, Georgia 30341
�(770) 458-7400
���� www.chronicdisease.org
���� [email protected]


















