Strategic Clinical Networks Improving Management of · PDF fileStrategic Clinical Networks ....
51
NHS England “High quality care for all, now and for future generations.” Strategic Clinical Networks Improving Management of Seizure Paper prepared by Claire Braid Northern England Strategic Clinical Networks Dr Paul Goldsmith Consultant Neurologist / Neurological Conditions Network Clinical Lead Purpose This paper provides information on current work within the Northern SCN area for patients with seizure. It is intended to be read alongside the national seizure paper. Version Control: Version Purpose / Change Author Date V0.2 Draft Claire Braid Paul Goldsmith 7 Oct 14 V0.3 Insert Cumbria Guidelines Claire Braid
Transcript of Strategic Clinical Networks Improving Management of · PDF fileStrategic Clinical Networks ....

NHS England “High quality care for all, now and for future generations.”
Strategic Clinical Networks Improving Management of Seizure Paper prepared by
Claire Braid Northern England Strategic Clinical Networks Dr Paul Goldsmith Consultant Neurologist / Neurological Conditions Network Clinical Lead
Purpose This paper provides information on current work within the Northern SCN area for patients with seizure. It is intended to be read alongside the national seizure paper.
Version Control: Version Purpose / Change Author Date V0.2 Draft Claire Braid
Paul Goldsmith 7 Oct 14
V0.3 Insert Cumbria Guidelines Claire Braid
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
17 Feb 15
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text

Contents Introduction and background ....................................................................... 3
Local Data – Highlights ............................................................................... 3
Known Local Guidelines / Protocol .............................................................. 4
Proposals for local implementation ............................................................. 5
References ................................................................................................. 7
Appendices ................................................................................................. 8

3 of 8
Introduction and background
In April 2013, twelve Strategic Clinical Networks (SCNs) were introduced to the new
NHS structures for England. Working within the Mental Health, Dementia and
Neurological Conditions Network, each area has been tasked with improving
services for people with neurological conditions. During the first year of operation,
there has been time invested in reviewing evidence and speaking to local
stakeholders about areas of health and social care which warrant large scale
change. Seizure was identified as an area that places significant demand on acute
neurology services and there is scope to improve the management of this condition.
In April 2014, it was agreed that management of seizure would form one of the
national priorities for the Neurological Conditions Strategic Clinical Networks. A
national working group was subsequently set up to identify any existing pathways,
share good practice and develop a common integrated care pathway for local
adaptation and use. A national document was produced (1), with comprehensive
information on the rationale, background and evidence base to this project and a
compendium of known pathways, protocol and guidance. This document is intended
to be read in conjunction with the national paper.
Local Data – Highlights
The Strategic Clinical Network Business Support Team identified local data on
seizure, in terms of epilepsy prevalence rates, prescribing, admission rates (primary
and mentions), proportion of patients managed by a Consultant Neurologist
emergency bed days, Choose and Book referrals for neurology, and diagnostics
(Appendix 1).
Most CCGs in the Northern SCN area have epilepsy prevalence rates higher than
the national average, with only two CCGs being in line with the national average
(charts 3 and 4). In terms of prescribing, per capita spend is generally above the
national average in a number of CCGs, although spend is significantly lower than
the national average for Levetiracetam across the SCN area (charts 5-12).

4 of 8
For patients who are admitted with a primary diagnosis of epilepsy, there is variation
around the national average, although this is not significant (chart 13). The
proportion of these patients whose care was managed by a Consultant Neurologist
varies across the SCN area, but generally numbers are low, ranging from 4% to
15% (chart 15). There is wide variation across the SCN area for bed days following
emergency admission for epilepsy (chart 16). Rates per 100,000 population for
emergency admissions with a primary diagnosis of epilepsy are generally high
across the SCN area, although two CCG areas are significantly below the national
average (chart 20).
The proportion of all neurology Choose and Book referrals attributed to epilepsy
range from 4% to almost 9% across the CCG areas. This is compared to a national
average of 5.7% (chart 22).
A number of hospitals also participated in the second National Audit of Seizure
Management in Hospitals (NASH2). This provided site-specific audit information
regarding how patients with seizures were managed in emergency departments. An
overall report has been produced which details the outcome of the audit for all
participating sites across the Northern SCN area (2). This is available on the
Northern England SCN website.
Known Local Guidelines / Protocol
An exercise was carried out to understand what is currently in place across the
Northern England SCN area, in terms of existing pathways, guidelines and protocol
to support the management of seizure.
A number of emergency departments have locally developed seizure pathways in
place (County Durham and Darlington NHS Foundation Trust, South Tyneside NHS
Foundation Trust and North Tyneside General Hospital). Other departments use
documents such as the Guideline for the Management of First Seizure in the
Emergency Department, published by the College of Emergency Medicine (3).
The main issues identified across the Northern SCN area are:
• Lack of neurology specialty in district general hospitals

5 of 8
• Lack of capacity in neurology to meet NICE guidance target of people being
seen by a specialist within 2 weeks of a first fit
• Limited communication between neurology to emergency departments on the
quality of referrals
• Increased numbers of patients with alcohol-provoked seizures in emergency
departments
• Lack of access to neurology notes in district general hospital emergency
departments
• Inadequate community-based long term care
• Lack of access to EEG in district general hospitals, affecting ability to make
an accurate diagnosis
• Lack of an agreed management protocol that spans primary and secondary
care.
• Lack of support for patients with non-epileptic attack disorder (NEAD)
Nationally, the main areas identified for improvement are:
• Supporting rapid access to accurate diagnosis
• Decreasing avoidable admissions for people with established epilepsy
• Providing on-going support via annual reviews and information provision for
people with a diagnosis of epilepsy
• Improving access to epilepsy specialist nurses
• Improving transition for young people into adult service.
• Links to improvement work for people with non-epileptic attack disorder.
Proposals for local implementation
A number of proposals have been developed to be considered by the Network
stakeholder group. These include:
• Implementation of a standardised pathway across the SCN area to facilitate
rapid access to accurate diagnosis, using learning from local and national
good practice examples
• Education for rotating emergency department staff, linking with neurologists
from local specialist centres

6 of 8
• Linking with another work stream incorporating non-epileptic attack disorder,
aiming to provide education for staff on this condition
• Exploring the potential for the role of epilepsy specialist nurses in emergency
departments
It is also proposed to link with a broader project led by the Maternity and Child
Health SCN on transition.

7 of 8
References
1. Strategic Clinical Networks: Epilepsy Pathway Development. Draft v2 (July
2014). NHS England.
2. National Audit for Seizure Management in Hospitals (NASH2) (July 2014)
North East SCN Regional Report. University of Liverpool.
3. Turner, S and Benger, J (2009) Guideline for the Management of First
Seizure in the Emergency Department. College of Emergency Medicine.

8 of 8
Appendices
Appendix 1 Data
Appendix 2 County Durham and Darlington Seizure Guideline
Appendix 3 South Tyneside Seizure Guideline
Appendix 4 Northumbria Healthcare and Newcastle Hospital Seizure Management
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Appendix 5
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Cumbria Guidelines
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text

Appendices
Appendix 1 – Data
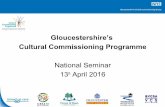
Northern England Strategic Clinical Networks Neurological Conditions Network Neurology Baselines Overview Across England there were over 15million hospital admission episodes in 2012/13, with just over 1 million in CCGs in the network area (no adjustment for Cumbria) across all specialties. This number equates to 7.3% of the national total which is slightly higher than the proportion of the national population in this area which is 6.1%. Of those admission episodes, over 1.3m (8.2%) are attributed to Neurology (either primary diagnosis or mentions); across network CCGs Neurology episodes account for 8.5% of all admissions. Generally admission rates (per 100,000 population) are higher in network CCGs than in England and this is mirrored for neurology admissions. See Chart 1 below Chart 1
Nationally 35.2% of all admissions are emergencies; across network CCGs there is some variation with a range from 32.6% in South Tyneside to 39.7% in South Tees. For Neurology
32,209
35,302 34,738
29,202 31,376
33,388 32,512 34,454 35,116
39,521 37,163
31,733
26,661
37,370
33,772
2,390 2,950 2,918 2,503 2,810 2,595 2,469 3,239 2,996 3,198 3,029 2,712 2,345 3,531 2,857 -
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
NHS
DAR
LIN
GTO
N C
CG
NHS
DU
RHAM
DAL
ES,E
ASIN
GTO
N A
ND
SED
GEF
IELD
CCG
NHS
GAT
ESHE
AD C
CG
NHS
NEW
CAST
LE N
ORT
H A
ND
EAS
TCC
G
NHS
NEW
CAST
LE W
EST
CCG
NHS
NO
RTH
DU
RHAM
CCG
NHS
HAR
TLEP
OO
L AN
D S
TOCK
TON
-ON
-TE
ES C
CG
NHS
NO
RTH
UM
BERL
AND
CCG
NHS
SO
UTH
TEE
S CC
G
NHS
SO
UTH
TYN
ESID
E CC
G
NHS
SU
ND
ERLA
ND
CCG
NHS
CU
MBR
IA C
CG
NHS
HAM
BLET
ON
, RIC
HM
ON
DSH
IRE
AND
WH
ITBY
CCG
NHS
NO
RTH
TYN
ESID
E CC
G
Tota
l NEC
N
FAEs - rate per 100,000 - all Specialties and NeurologyAll FAEs FAEs - Neurology
All FAEs - England FAEs - Neurology - England

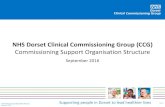
patients 58.7% of admissions are emergencies nationally - generally rates for network CCGs are slightly below this, ranging from 52.8% in North Durham to 61.8% in Darlington. Chart 2
Epilepsy Prevalence Chart 3 – Number in Cohort
61.8%
55.6%57.7%
52.9% 53.2% 52.8%
58.6%
54.4%
60.5%
55.8%57.9%
55.0%52.7% 52.9%
55.8%
37.6% 36.7% 37.5% 36.4% 37.0% 34.6% 35.0% 33.8% 39.7% 32.6% 34.8% 33.2% 33.2% 36.2% 35.4%0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
NH
S DA
RLIN
GTO
NCC
G
NH
S DU
RHAM
DALE
S,EA
SIN
GTO
N A
ND
SEDG
EFIE
LD C
CG
NH
S G
ATES
HEAD
CCG
NH
S N
EWCA
STLE
NO
RTH
AN
D EA
STCC
G
NH
S N
EWCA
STLE
WES
T CC
G
NH
S N
ORT
HDU
RHAM
CCG
NH
S H
ARTL
EPO
OL
AND
STO
CKTO
N-
ON
-TEE
S CC
G
NH
SN
ORT
HU
MBE
RLA
ND
CCG
NH
S SO
UTH
TEE
SCC
G
NH
S SO
UTH
TYN
ESID
E CC
G
NH
SSU
NDE
RLAN
DCC
G
NH
S CU
MBR
IACC
G
NH
SHA
MBL
ETO
N,
RICH
MO
NDS
HIRE
AND
WHI
TBY
CCG
NH
S N
ORT
HTY
NES
IDE
CCG
Tota
l NEC
N
FAEs - % Emergency
FAEs - Neurology FAEs -All Specialties All - England Neurology - England
3,66
9
832
2,34
0
1,48
2
952
2,15
9
973
1,02
1
1,61
8
1,65
6
2,36
5
2,43
2
1,13
7
2,25
2
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
0.00
500.00
1000.00
1500.00
2000.00
2500.00
3000.00
3500.00
4000.00 NESCN - Number and %Number in Cohort % Prevalence National Prevalence

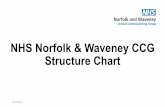
There are 24,888 patients with epilepsy on GP registers in network CCGs and this represents .9% of the CCG populations. Nationally just under 0.8% of the total registered populations are estimated to have epilepsy. For network CCGs most are above this with 0.9 -1%. Only Hambleton and Newcastle North and East are in line with the national average and have the lowest % prevalence (0.8%) in the network. South Tees has the highest rate in the network and is ranked 3 across all CCGs nationally. Prevalence rates (crude per 100,000) are generally significantly higher than the national average. The Chart below shows only HRW and NNE have rates which are not significantly different to the national average. Chart 4 - % Prevalence
0.00
200.00
400.00
600.00
800.00
1000.00
1200.00
NHS
Cum
bria
CCG
NHS
Dar
lingt
onCC
G
NHS
Dur
ham
Dale
s,Ea
singt
on…
NHS
Gat
eshe
adCC
G
NHS
Ham
blet
on,
Rich
mon
dshi
r…
NHS
Har
tlepo
olAn
d St
ockt
on-
On-
Tees
CCG
NHS
New
cast
leN
orth
And
Eas
tCC
G
NHS
New
cast
leW
est C
CG
NHS
Nor
thDu
rham
CCG
NHS
Nor
thTy
nesid
e CC
G
NHS
Nor
thum
berla
nd
CCG
NHS
Sou
thTe
es C
CG
NHS
Sou
thTy
nesid
e CC
G
NHS
Sund
erla
ndCC
G
Prevalence - Epilepsy by CCG

Prescribing Spend per 1,000 on individual drugs shows variation across network CCGs and this may reflect preferred drugs use. However, per capita spend is generally above the national average (often significantly so) for all listed drugs in a number of CCGs – so high spend on one product is not offset by low spend on another – although spend is significantly lower across the board for Lavetiracetam than the national average. Chart 5 - Phenytoin Sodium
Chart 6 - Sodium Valporate
7952
6.19
7117
7.92
6477
9.98
9080
4.75
5564
8.08
6172
4.07
7664
0.51
8367
1.66
8432
6.90
7066
6.37
8208
6.25
5488
0.57
9128
8.89
7528
2.20
0.00
10000.00
20000.00
30000.00
40000.00
50000.00
60000.00
70000.00
80000.00
90000.00
100000.00 Per Capita Spend - Phenytoin Sodium
4457
9.83
5397
7.09
5493
8.67
5642
8.45
3670
5.24
3574
5.88
5076
8.92
4906
5.47
5215
1.87
4280
6.68
4915
8.81
4065
8.66
5949
9.80
4791
6.74
0.00
10000.00
20000.00
30000.00
40000.00
50000.00
60000.00
70000.00 Per Capita Spend - Sodium Valporate

Chart 7 - Lavetiracetam
Chart 8 - Carbamazepine
4378
8.96
1703
2.09
3501
6.38
1554
4.16
2621
7.43
2888
9.07
2702
3.06
2511
5.72
2226
1.01
2490
3.67
2011
0.41
2969
4.48
2160
5.93
2356
1.37
0.00
5000.00
10000.00
15000.00
20000.00
25000.00
30000.00
35000.00
40000.00
45000.00
50000.00 Per Capita Spend - Lavetiracetam34
805.
96
3620
2.34
4097
0.56
4579
3.28
3338
8.47
3915
0.36
3921
0.74
4340
0.14
4100
4.28
4354
4.21
4254
5.59
3934
2.35
4105
7.39
4283
4.85
0.00
5000.00
10000.00
15000.00
20000.00
25000.00
30000.00
35000.00
40000.00
45000.00
50000.00 Per Capita Spend - Carbamazepine

Chart 9 - Others (Excl Pregbalin)
From the Neuro Compendium data for prescribing and daily dosages are generally higher than the national average – which will impact on spend – consideration should be given to whether increased levels are to be expected as a result of higher prevalence in the network area. Chart 10 – Total Prescribed
1088
68.6
6
9349
1.65
1345
87.3
7
1141
22.3
3
1243
84.4
7
1274
77.0
7
1101
08.5
1
1377
55.0
1
1609
73.0
8
1272
02.5
6
1470
24.0
1
1358
94.4
8
1220
36.4
3
1010
20.9
6
0.00
20000.00
40000.00
60000.00
80000.00
100000.00
120000.00
140000.00
160000.00
180000.00 Per Capita Spend - Other Drugs excl Pregabalin19
08.0
6
2928
.52
2660
.95
3327
.79
2819
.63
2905
.18
1558
.23
2708
.73
2137
.46
2728
.53
3028
.47
2698
.12
2877
.49
2990
.98
0.00
500.00
1000.00
1500.00
2000.00
2500.00
3000.00
3500.00
01H
- NHS
Cum
bria
CCG
00P
- NHS
Sun
derla
nd C
CG
00L
- NHS
Nor
thum
berla
nd C
CG
00D
- NHS
Dur
ham
Dal
es,
Easin
gton
and
Sed
gefie
ld C
CG
00M
- N
HS S
outh
Tee
s CCG
99C
- NHS
Nor
th T
ynes
ide
CCG
03D
- NHS
Ham
blet
on,
Rich
mon
dshi
re a
nd W
hitb
y CC
G
00J -
NHS
Nor
th D
urha
m C
CG
00K
- NHS
Har
tlepo
ol a
ndSt
ockt
on-o
n-Te
es C
CG
00N
- N
HS S
outh
Tyn
esid
e CC
G
00F
- NHS
Gat
eshe
ad C
CG
00G
- NHS
New
cast
le N
orth
and
East
CCG
00H
- NHS
New
cast
le W
est C
CG
00C
- NHS
Dar
lingt
on C
CG
NESCN - Epilepsy - Prescribing Total Prescribed per 10,000 population

Chart 11 – Daily Usage
Chart 12 – Net Ingredient Cost
3338
2.32
4185
9.02
4236
7.97
5079
8.98
4895
4.26
4390
1.23
3094
7.19
4094
2.25
4019
0.45
4276
8.39
4693
0.36
3670
7.50
4172
9.15
4151
6.25
0.00
10000.00
20000.00
30000.00
40000.00
50000.00
60000.0001
H - N
HS C
umbr
ia C
CG
00P
- NHS
Sun
derla
nd C
CG
00L
- NHS
Nor
thum
berla
nd C
CG
00D
- NHS
Dur
ham
Dal
es,
Easin
gton
and
Sed
gefie
ld C
CG
00M
- N
HS S
outh
Tee
s CCG
99C
- NHS
Nor
th T
ynes
ide
CCG
03D
- NHS
Ham
blet
on,
Rich
mon
dshi
re a
nd W
hitb
y CC
G
00J -
NHS
Nor
th D
urha
m C
CG
00K
- NHS
Har
tlepo
ol a
ndSt
ockt
on-o
n-Te
es C
CG
00N
- N
HS S
outh
Tyn
esid
e CC
G
00F
- NHS
Gat
eshe
ad C
CG
00G
- NHS
New
cast
le N
orth
and
East
CCG
00H
- NHS
New
cast
le W
est C
CG
00C
- NHS
Dar
lingt
on C
CG
NESCN - Epilepsy - Prescribing Total DDD Usage per 10,000 population43
404.
06
4851
4.07
4688
9.87
5897
9.84
5706
9.06
4843
2.56
3954
3.91
4781
1.01
4496
4.06
4680
8.92
5177
6.72
4095
7.73
4661
7.70
4724
4.83
0.00
10000.00
20000.00
30000.00
40000.00
50000.00
60000.00
70000.00
01H
- NHS
Cum
bria
CCG
00P
- NHS
Sun
derla
nd C
CG
00L
- NHS
Nor
thum
berla
nd C
CG
00D
- NHS
Dur
ham
Dal
es,
Easin
gton
and
Sed
gefie
ld C
CG
00M
- N
HS S
outh
Tee
s CCG
99C
- NHS
Nor
th T
ynes
ide
CCG
03D
- NHS
Ham
blet
on,
Rich
mon
dshi
re a
nd W
hitb
y CC
G
00J -
NHS
Nor
th D
urha
m C
CG
00K
- NHS
Har
tlepo
ol a
ndSt
ockt
on-o
n-Te
es C
CG
00N
- N
HS S
outh
Tyn
esid
e CC
G
00F
- NHS
Gat
eshe
ad C
CG
00G
- NHS
New
cast
le N
orth
and
East
CCG
00H
- NHS
New
cast
le W
est C
CG
00C
- NHS
Dar
lingt
on C
CG
NESCN - Epilepsy - Prescribing Total Nic per 10,000 population

Hospital Activity Chart 13 – Admitted - Primary
This chart shows the rate of admission per 100,000 (CCG population aged 18+) with a primary diagnosis of Epilepsy. While there is variation around the national average; wide confidence intervals mean that many differences are not significant. The next chart shows the same for admissions with a mention of epilepsy in diagnostic codes – the admission may or may not be a result of the epilepsy. For this cohort, all CCGs have rates above the national average – however this could be a reflection of more efficient coding of admissions. Chart 14 – Admitted - Mention
53.5
6
48.6
9
68.2
4
74.5
0
41.3
9
67.4
5
53.6
9
70.1
9
50.7
7
54.8
9
68.1
6
75.3
5
67.3
2
53.1
3
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00 Proportion Admitted - Primary Diagnosis of Epilepsy30
2.44
342.
04
375.
99
352.
69
296.
66
376.
65
332.
55
441.
60
310.
10
347.
83
356.
14
493.
29
387.
09
355.
66
0.00
100.00
200.00
300.00
400.00
500.00
600.00 Proportion Admitted - Diagnosis Mention of Epilepsy

Chart 15 - Inpatient Management
This chart shows the % of admission episodes with a Primary Diagnosis of Epilepsy where the care was managed by a neurologist (spec 400). There is no national comparator; but levels are varied across the network – and all CCGs demonstrate very low numbers with a range from less than 4% to just over 15%. These cases have a primary diagnosis of epilepsy, so it would be reasonable to assume that admissions are related to the condition and therefore the question is whether care received is appropriate and effective for the patient. Chart 16 - Emergency Bed Days
This chart shows rate per 100,000 for bed days following emergency admission for epilepsy. There is wide variation across the network with a range from 94 in HRW to almost 700 in Newcastle North
3.77
3.77
4.02
10.1
3
8.06
10.1
5
13.1
0
15.1
5
10.7
4
8.59
7.98
16.3
9
5.17
12.7
5
0.00
5.00
10.00
15.00
20.00
25.00 Proportion Admitted - Epilepsy managed by Consultant Neurologist
388.
51
257.
72
248.
63
383.
33
94.0
0
206.
72
350.
98
672.
63
160.
77
249.
61
313.
63
353.
10
355.
83
296.
38
0.00
100.00
200.00
300.00
400.00
500.00
600.00
700.00
800.00 Use of Emergency Bed Days following admission for Epilepsy

and East. Rates for most CCGs are above the national average – a number significantly so; 3 CCGs have rates significantly below the national average. Chart 17 - Disease Management
For most CCGs the proportion of patients on the QOF register who have been seizure free for 12 months is broadly in line with the national average – this measure has been dropped from QOF so data after this issue for 12/13 will not be available. Chart 18 - Admission Episodes – Primary
62.7
1
59.9
8
58.3
8
58.5
0
66.9
1
56.8
3
53.7
5
56.2
2
62.1
1
60.2
1
64.8
6
53.0
8
58.5
8
53.4
2
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00 12 Months Seizure Free
5.2%
4.8%
5.5%
5.9%
8.0%
4.4%
4.5%
4.4%
7.4%
7.4%
6.7%
6.6%
7.4%
5.6%
9.7%
11.0
%
10.8
%
12.1
%
15.6
%
9.0%
7.4%
9.3%
13.7
%
16.9
%
14.2
%
14.8
%
15.8
%
9.6%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
01H
- NH
S Cu
mbr
ia C
CG
00P
- NHS
Sun
derla
nd C
CG
00L
- NHS
Nor
thum
berla
ndCC
G
00D
- NH
S Du
rham
Dal
es,
Easi
ngto
n an
d Se
dgef
ield
CCG
00M
- N
HS
Sout
h Te
es C
CG
99C
- NHS
Nor
th T
ynes
ide
CCG
03D
- NH
S Ha
mbl
eton
,Ri
chm
onds
hire
and
Whi
tby
CCG
00J -
NH
S N
orth
Dur
ham
CCG
00K
- NH
S H
artle
pool
and
Stoc
kton
-on-
Tees
CCG
00N
- N
HS
Sout
h Ty
nesi
deCC
G
00F
- NHS
Gat
eshe
ad C
CG
00G
- N
HS N
ewca
stle
Nor
than
d Ea
st C
CG
00H
- NH
S N
ewca
stle
Wes
tCC
G
00C
- NHS
Dar
lingt
on C
CG
% Neurological FAEs - Epilepsy - Primary Diagnosis
All FAEs Emergency

Finished admission episodes with a primary diagnosis of epilepsy nationally account for just under 7% of neurology admissions; for CCGs in the network area epilepsy admissions rate from 4.4% in North Tyneside and North Durham to 8% in South Tees. Emergency Admissions with a primary diagnosis of Epilepsy nationally account for almost 13% of all neurological emergency admissions; across the network epilepsy accounts for between 7.4% in Hambleton, Richmondshire & Whitby and 16.9% in South Tyneside. Chart 19 – Admission Episodes - Mentions
Nationally Epilepsy is mentioned in 15.4% of admission episodes; across the network values range from 14.6% in Northumberland to 24.3% in South Tees. Emergency neurological episodes with a mention of Epilepsy account for 16% of the total; again network CCG rates are generally broadly in line with this, ranging from 13.4% in HRW to 24% in South Tees. Nationally there are more than 1.3m neurological admission episodes each year of which 60.2% are Emergencies.
15.9
%
14.8
%
14.6
%
16.5
%
24.3
%
15.1
%
15.6
%
16.0
%
18.2
%
17.3
%
16.0
%
19.6
%
18.6
%
17.1
%
15.4
%
16.6
%
15.2
%
17.7
%
24.0
%
14.7
%
13.4
%
15.8
%
18.1
%
18.0
%
16.6
%
20.2
%
18.8
%
17.1
%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
01H
- NH
S Cu
mbr
ia C
CG
00P
- NHS
Sun
derla
nd C
CG
00L
- NHS
Nor
thum
berla
ndCC
G
00D
- NH
S Du
rham
Dal
es,
Easi
ngto
n an
d Se
dgef
ield
CCG
00M
- N
HS
Sout
h Te
es C
CG
99C
- NHS
Nor
th T
ynes
ide
CCG
03D
- NH
S Ha
mbl
eton
,Ri
chm
onds
hire
and
Whi
tby
CCG
00J -
NH
S N
orth
Dur
ham
CCG
00K
- NH
S H
artle
pool
and
Stoc
kton
-on-
Tees
CCG
00N
- N
HS
Sout
h Ty
nesi
deCC
G
00F
- NHS
Gat
eshe
ad C
CG
00G
- N
HS N
ewca
stle
Nor
than
d Ea
st C
CG
00H
- NH
S N
ewca
stle
Wes
tCC
G
00C
- NHS
Dar
lingt
on C
CG
% Neurological FAEs - Epilepsy - Mentions
All FAEs Emergency

Emergency Admissions Chart 20 – Emergency Admission Rates – Primary
Rates per 100,000 population for emergency admissions with a primary diagnosis of Epilepsy are generally high across network CCGS, though in some cases differences are not significant. HRW and North Durham are both significantly below the national average. For admissions where epilepsy is mentioned rates are similarly above the national average, with the exception of the same 2 CCGs Chart 21 – Emergency Admission Rates – Mentions
66.4
3
62.9
4
83.8
9
84.1
2
44.8
4
80.5
8
64.1
1
86.7
6
52.7
6
71.0
7
87.3
1
95.5
0
91.3
6
62.7
9
0.00
20.00
40.00
60.00
80.00
100.00
120.00 Epilepsy Emergency Admissions - Primary Diagnosis31
1.09
339.
66
391.
20
380.
93
243.
19
364.
38
317.
32
422.
10
287.
20
364.
01
362.
65
572.
14
426.
36
390.
79
0.00
100.00
200.00
300.00
400.00
500.00
600.00
700.00 Epilepsy Emergency Admissions - Mentions

Chart 22 – Choose & Book Referrals
The above chart shows the proportion of Choose and Book Referrals attributed to Epilepsy out of all neurology choose and book referrals. CCG rates range from 4% to almost 9% compared to the national average of 5.7%. Diagnostics Chart 23 – Diagnostic Tests
This chart shows numbers for diagnostic imaging tests for all neurological conditions and the number of those attributed to epilepsy. The % of epilepsy tests is also shown. Typically
4.4% 7.0% 4.7% 4.9% 8.9% 4.0% 5.0% 5.8% 8.8% 5.1% 7.1% 6.4% 8.7% 8.3%0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
01H
- NH
S Cu
mbr
ia C
CG
00P
- NHS
Sun
derla
ndCC
G
00L
- NHS
Nor
thum
berla
nd C
CG
00D
- NH
S Du
rham
Dal
es, E
asin
gton
and
Sedg
efie
ld C
CG
00M
- N
HS
Sout
h Te
esCC
G
99C
- NHS
Nor
thTy
nesi
de C
CG
03D
- NH
S Ha
mbl
eton
,Ri
chm
onds
hire
and
Whi
tby
CCG
00J -
NH
S N
orth
Dur
ham
CCG
00K
- NH
S H
artle
pool
and
Stoc
kton
-on-
Tees
CCG
00N
- N
HS
Sout
hTy
nesi
de C
CG
00F
- NHS
Gat
eshe
adCC
G
00G
- N
HS N
ewca
stle
Nor
th a
nd E
ast C
CG
00H
- NH
S N
ewca
stle
Wes
t CCG
00C
- NHS
Dar
lingt
onCC
G
% Choose & Book Referrals for Neurology which are Epilepsy
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
0.00
1000.00
2000.00
3000.00
4000.00
5000.00
6000.00
7000.00
8000.00
9000.00
10000.00
01H
- NHS
Cum
bria
CCG
00P
- NHS
Sun
derla
nd C
CG
00L
- NHS
Nor
thum
berla
ndCC
G
00D
- NHS
Dur
ham
Dal
es,
Easi
ngto
n an
d Se
dgef
ield
CCG
00M
- N
HS S
outh
Tee
s CCG
99C
- NHS
Nor
th T
ynes
ide
CCG
03D
- NHS
Ham
blet
on,
Rich
mon
dshi
re a
nd W
hitb
yCC
G
00J -
NHS
Nor
th D
urha
mCC
G
00K
- NHS
Har
tlepo
ol a
ndSt
ockt
on-o
n-Te
es C
CG
00N
- N
HS S
outh
Tyn
esid
eCC
G
00F
- NHS
Gat
eshe
ad C
CG
00G
- NHS
New
cast
le N
orth
and
East
CCG
00H
- NHS
New
cast
le W
est
CCG
00C
- NHS
Dar
lingt
on C
CG
Total Diagnostic Tests (DIDS)
Total - All Neurology Total - Epilepsy % Epilepsy

between 10% and up to 20% of imaging is attributed to epilepsy. Data should be checked as that for the 2 Newcastle CCGs is much lower than for other CCGs – this may be a coding issue. From the Diagnostic Imaging Dataset the next 2 charts show median waiting times for each test by CCG. There is some variation in the data – but this is worthy of further scrutiny as some of the numbers are very small and data completeness issues continue. Chart 24 – Median Wait Times Diagnostics
Chart 25 – Median Wait Times
10.50
1.00 1.00 1.001.00 1.00 2.00 1.00
12.00
3.00 4.501.00
5.001.00
3.00 17.00
1.00 1.00
12.00
2.50
6.00
3.503.00
11.00
16.5027.00
14.50 22.006.00 18.00
33.0016.00
10.5013.50
15.00
28.00
14.00
4.00
12.00
3.00
10.00
2.00
8.00
23.50
7.00
8.00
5.00
6.00
9.00
14.0025.00
15.00
7.5017.00
17.00
14.00
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
01H
- NHS
Cum
bria
CCG
00P
- NHS
Sun
derla
ndCC
G
00L
- NHS
Nor
thum
berla
nd C
CG
00D
- NHS
Dur
ham
Dale
s, E
asin
gton
and
…
00M
- N
HS S
outh
Tee
sCC
G
99C
- NHS
Nor
thTy
nesi
de C
CG
03D
- NHS
Ham
blet
on,
Rich
mon
dshi
re a
nd…
00J -
NHS
Nor
thDu
rham
CCG
00K
- NHS
Har
tlepo
olan
d St
ockt
on-o
n-Te
es…
00N
- N
HS S
outh
Tyne
side
CCG
00F
- NHS
Gat
eshe
adCC
G
00G
- N
HS N
ewca
stle
Nor
th a
nd E
ast C
CG
00H
- NHS
New
cast
leW
est C
CG
00C
- NHS
Dar
lingt
onCC
G
Median Diagnostic Waitng Times - Epilepsy
Unknown
SPECT
PET
XRay
Nuclear
Medical Photography
MRI
Fluoroscopy
Endoscopy
US
CT
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.0001H - NHS Cumbria CCG
00P - NHS Sunderland CCG
00L - NHS Northumberland CCG
00D - NHS Durham Dales,Easington and Sedgefield CCG
00M - NHS South Tees CCG
99C - NHS North Tyneside CCG
03D - NHS Hambleton,Richmondshire and Whitby CCG
00J - NHS North Durham CCG
00K - NHS Hartlepool andStockton-on-Tees CCG
00N - NHS South Tyneside CCG
00F - NHS Gateshead CCG
00G - NHS Newcastle North andEast CCG
00H - NHS Newcastle West CCG
00C - NHS Darlington CCG
Median Wait Times - Diagnostic Tests - Epilepsy
CT
US
Endo
Fluoroscopy
MRI
Med Photography
Nuclear Med
X Ray
PET
SPECT
Unknown

Appendix 2 – County Durham and Darlington Seizure Guideline
Guideline on the management of First Seizure in the Emergency Department Introduction Seizures are a common occurrence. Prospective, population based studies show up to a 2-4% lifetime risk of one seizure, and a 2% chance of epilepsy. People with epilepsy have a premature death that is 2-3 times higher than the general population. Seizures are a frequent reason for attendance to the ED, accounting for around 1.2% of attendances. Around a quarter of these are due to first seizure. Scope This guideline is based on that developed by the College of Emergency Medicine. It is for adult patients (≥16yrs of age) presenting to the ED with a suspected first convulsive seizure (not including status epilepticus). Is it a seizure or not? If at all possible get as much details as you can from any witnesses (see appendix 1) and invite them to attend the neurology outpatient appointment if possible. Below is a basic guide to help differentiate seizures from syncope. Think about:
Seizure: Syncope:
Context - From sleep or awake?
Relevant triggers / precipitants?
Before - Aura? Lightheadedness / sweating Pallor Chest pain / palpitation
During - Convulsion Head turning Automatism / posturing Tongue biting
Brief myoclonus
Afterwards - Confusion Rapid recovery and orientation ED management Baseline observations Temperature, Pulse, Blood Pressure,
Sats, GCS & pupils, EWS, BM
Investigations (Ix) Bloods (FBC, U&Es, Glucose, Calcium, ethanol) ECG (to be faxed with the referral) Urine pregnancy test (if woman of child-bearing age) Other Ix to consider CXR, LP, toxicology

Neuroimaging The following patients should be considered for immediate CT head:
• New focal neurological deficit or persistent altered mental state • Fever • Persistent headache • Focal or partial onset before generalised • History of acute head trauma • Malignancy (CT with contrast) • Immunocompromised, HIV infection (CT with contrast) • Alcoholism • Anticoagulation or bleeding diathesis
Requesting of Urgent out-patient MRI Patients that present with a good history of first seizure (including an eye-witness account of tonic-clonic seizure activity with post-ictal phase) should have an Urgent out-patient MRI requested. This imaging will then be reviewed and actioned by the neurologist in out-patients. The scan itself does not need to be performed prior to ED discharge. MR brain imaging should only be requested for those patients in whom a first seizure is considered likely. The named consultant should be the ED consultant on-call at the time of the ED attendance. Need for admission Patients who have fully recovered, have no neurological deficit, and have normal initial investigations can be discharged from the ED. Admission should be considered in all patients with:
• Alcoholism • Poor social circumstances • No responsible adult to stay with
Advice Patients should be given verbal and written advice about driving and lifestyle changes prior to being discharged from the ED e.g. bathing/ swimming and working at heights/ with machinery Advice given to patients should be documented in the medical notes. Referral Please ensure that a copy of the ED notes, ECG, witness statement (if possible) and the attached checklist filled out and all faxed to 64405 for the attention of Dr Williams/ Dorman (Consultant Neurologists) to the Central Appointments Bureau.

First Fit referral checklist Suitability for protocol driven investigation (all Yes)
Yes No 16 years old or over
Suspected first seizure, convulsive
Not status epilepticus
Seizure not related to head injury or ecclampsia
ED Management (all Yes)
Performed and results in notes Yes No Baseline observations
FBC, U&Es, serum ethanol, Calcium, Glucose
ECG (copy to be faxed with referral)
Complete witness statement form- if possible (copy to be faxed with referral)
Pregnancy test (if appropriate)
Urgent out-patient MRI requested (if high likelihood of convulsive tonic-clonic seizure with post-ictal phase confirmed by eye-witness)
Yes No Advice given & documented in notes(all Yes)
Yes No Written First Seizure card given
Verbal explanation- swimming/ bathing and working at heights/ with machinery
Driving advice (if appropriate)
Please ensure checklist faxed to Central Appointments Bureau on 64405 with a copy of the
ED summary, ECG and witness statement (if available)

DETAILS OF EVENT / SEIZURE FROM A WITNESS- PLEASE BRING THIS INFORMATION TO YOUR CLINIC APPOINTMENT
Witness Name: Your name:
1. What was the person doing just before the seizure event?
2. What alerted you to the seizure/ event?
3. What time of day did the seizure event happen?
4. Describe what you saw during the seizure / event What parts of the body were affected ? Was one side affected more than the other?
Did the person go stiff? What types of movements did the person make if any? (eg twitching, jerking, thrashing) Were there any facial movements?
Was the person unconscious or was there a change in awareness( could the person speak to you, did the speech make sense?
Were their eyes open or shut?
Did their colour change (eg flushed, clammy pale)? Did their breathing change ? If so, in what way?
How long did the seizure last? Did the person injure himself or herself?
Anything else you noticed that you feel would be helpful to tell us (use the back of the sheet if necessary) How did the person behave after the seizure?
Were they sleepy, confused or alert?
How long did the person take to recover?
Did they want to sleep afterwards?

Appendix 3 – South Tyneside Seizure Guideline
Management of First Seizure in the Emergency Department Protocol
Background The National Institute for Health and Care Excellence (NICE) have produced guidance for the management of Epilepsy (CG137-Epilepsy 2012) which is a common long-term condition. Within this protocol there is guidance on the management of a first seizure. Furthermore, the National Confidential Enquiry into Patient Outcome and Death Audit -National Audit into Seizure management in Hospitals, 2011, (NASH) has identified areas for improvement nationally and locally. This protocol has been developed to improve the management of first seizure presentations by risk stratification allowing identification of patients requiring in-patient management and those that can be managed in an ambulatory out-patient pathway in an efficient manner.

MANAGEMENT OF FIRST SEIZURE IN THE EMERGENCY DEPARTMENT
FLOWCHART SUITABILITY FOR PROTOCOL BASED INVESTIGATIONS CRITERIA FOR NEUROIMAGING DISCHARGE RISK ASSESSMENT GUIDANCE NOTES PATHWAY CHECK LIST MRI CHECKLIST REFERRAL FOR ACUTE ACCESS CLINIC

Patient with suspected first seizure
See Notes
Check Suitability
Needs Emergency Department Neuroimaging
(Check imaging criteria) Yes Arrange
neuroimaging (see notes)
No
Discharge Risk Assessment
(See Risk Assessment Criteria)
High
Moderate
Low
Admit
1. Laboratory Investigations & Bedside Tests
2. Choice of neuroimaging modality
3. Treatment
4. Discharge
5. Advice
• Discharge advice • Driving advice • Occupational and
Hazardous activities advice
• Document all of above advice given in Patient Medical Notes
• MRI Checklist • Fax copy of AAC
referral form and MRI checklist to Dr Wahid’s Secretary on ext 2910

SUITABILTY FOR PROTOCOL BASED INVESTIGATION (ALL YES) 1.
16 years old or over Suspected first seizure Not status epilepticus Seizure not related to head injury or eclampsia
Observations: TEMPERATURE, HEART RATE, RESPIRATORY RATE, OXYGEN SATURATIONS, BM Laboratory: FBC, UREA ELECTROLYTE, COAGULATION, SERUM GLUCOSE, CALCIUM, MAGNESIUM, PHOSPHATE, LIVER FUNCTION TEST. ECG, PREGNANCY TEST, CXR, Other investigations such as TOXICOLOGY AND ALCOHOL LEVELS if clinically indicated. CRITERIA FOR NEUROIMAGING (ANY YES): 2.
New focal neurological deficit Persistent altered mental status Fever or persistent headache or vomiting Focal or partial onset seizure History of Cancer, HIV, Head Injury, Anticoagulation, Bleeding disorder, Alcoholism
Follow up cannot be ensured Needs Lumbar Puncture
DISCHARGE RISK ASSESSMENT 3.
YES
NO
1 Simple fit with full recovery
(HIGH)
2 No neurological deficit
(HIGH)
3 Normal initial investigations
(HIGH)
4 No history of/suspected alcoholism (MOD)
5 No poor social circumstances
(MOD)
6 Responsible adult to look after (MOD)
7 Likely to return (MOD)
Risk High if answer NO to Q 1, 2 or 3. Low if no high and no moderate All otherwise classed as moderate risk.

NOTES: 1. Laboratory Investigations & Bedside Tests:
Laboratory investigations other than those outlined in protocol based investigations, should only be done if clinically indicated.
2. Choice of neuroimaging modality: MRI preferable to CT, if readily available within an acceptable time period, in a patient who has fully recovered. (See page 8) CT should be used if MRI is not readily available or in an individual who has not fully recovered. CT is the modality of choice if the patient is critically ill, requires monitoring or MRI is not available /contraindicated.
3. Treatment: Antiepileptic should not routinely be prescribed in the ED. If antiepileptic is to be prescribed, this should only be after consultation with an epilepsy specialist/ neurologist.
4. Discharge: Patients with a normal neurological examination and normal baseline investigations can be safely discharged from the ED with outpatient follow-up. Consider admitting those patients without a responsible adult to stay with, or patients who are unlikely to attend out-patient investigations and follow-up.
5. Advice: Give discharge advice including first aid, driving, occupation and hazardous activities; document advice in patient’s medical record.
6. Follow-up: Arrange follow-up in the next available slot in Acute Access Clinic. Arrange outpatient neuroimaging if not already scanned, or do the MRI head request or checklist.

Management of First Seizure in Emergency Department:
Check List: DESCRIPTION COMPLETED Emergency Department notes
First seizure Pathway
MRI head request/checklist
DVLA instructions- see website
Occupational and Hazardous activities advice
Patient contact details
Responsible Adult to Stay
Fax Referral Form & MRI checklist to Dr S. Wahid (Fax No 2910)
Place Emergency Department notes & First Seizure Pathway in docket in the Ambulatory Care Unit (AMB Care)

Neuroimaging Due to the strong magnetic field there are instances where MRI is contraindicated. See STFT intranet, Radiology Department page – MRI Request form and Safety Checklist. SOUTH TYNESIDE NHS FOUNDATION TRUST MRI Department CHECK LIST Due to the strong magnetic field there are instances where MRI is contraindicated. If the answer to any of the following safety questions is yes, please contact the MRI Department (ext. 3156) for advice. Failure to provide accurate information will be regarded as a potential clinical incident. Does the patient have or has ever had: Pacemaker? Implanted defibrillator? Retained pacing wire? Metallic heart valve? If yes, please give details
(make, model): Brain surgery? If yes, please give details: History of foreign body metal in eye?
If yes, please give details
Implanted electronic / magnetically / mechanically controlled devices?
If yes, please give details:
Has the patient undergone surgery involving metal in the past 8 weeks?
If yes, please give details:
History of stent insertion for an aortic aneurysm (thoracic / abdominal)?
If yes, please give details (make, model)
Is patient arriving by ambulance? TABLE WEIGHT LIMIT 140kg/22stone What is the patient’s weight? Can patient attend at short notice?
If yes, please give details:
Is patient barrier nursed? If yes, please give reason: Is pregnancy known or suspected?
If yes, please give details:
Does patient have any known communication difficulties?
If yes, please give details:
Is patient in renal failure? If yes , please state GFR: Does patient have any allergies including latex?
If yes, please give details:

REFERRAL TO (DR WAHID) ACUTE ACCESS CLINIC (AAC) FOR FIRST SEIZURE
Patient Name:
Date:
Address: DOB: A&E or Ward: PAS/NHS No: Referring Consultant: CRITERIA YES (tick) No (tick) 16 years and older Suspected first seizure Status Epilepticus Seizure not related to head injury or eclampsia Simple fit with full recovery Neurological deficit Normal initial investigations History of/suspected alcoholism Poor social circumstances Responsible adult to look after for 24-hrs? Likely to return? Patient has been seen by or discussed with senior doctor (Middle Grade or Consultant)
IF ANSWERS ARE ALL YES PATIENT IS SUITABLE FOR REVIEW IN AAC. UNDERTAKE THE FOLLOWING:
1. Sign this form 2. Complete MRI check list 3. FAX THIS REFERRAL FORM AND MRI CHECKLIST TO: Ext. 2910 4. Place the completed first seizure pathway, A&E Casualty Card and ECG in the docket found in the Ambulatory Care Unit reception area
Name and Grade of doctor completing form (print): Date__ __ /__ __ /20__ __

Relevant to: (Northumbria Healthcare Foundation Trust NHS Trust, primarily Emergency Care Staff but others may find this of use)
1. MANAGEMENT OF STATUS EPILEPTICUS
See Page 2 for detailed Anti-Epileptic drug (AED) therapy & Doses. Generalised tonic clonic status epilepticus should be managed immediately;
- Secure airway. - Give oxygen. - Assess cardiac and respiratory function. - Secure intravenous access in a large vein. - Check BM at an early stage – if low give 10% Glucose iv 100 - 500ml according to
response - Check FBC, U&E, LFT, glucose, calcium, drug levels and consider urine for toxicology. - Give two pairs of Pabrinex®* ampoules (vials I & II) by IV infusion initially in A&E if any
suggestion of alcohol dependency - ECG when able More detailed recommendations about baseline assessment and management are available in appendix C of the NICE guideline: www.nice.org.uk/nicemedia/pdf/CG020fullguideline_appendixC_corrected.pdf
.
Seizure Management in the Emergency Department (Adult)
Document Type: Clinical Guideline Clinical Lead: Phil Stamp Author: Phil Stamp Directorate: Emergency Care Approved by Sub Committee/Group: ECSUB
Date Approved by Sub Committee/Group: TBCDate Approved by Clinical Guidelines Group:25/10/12Date of Issue: 3rd December 2012Review Date: December 2015 Version: 1
Important Notes: This Guideline is primarily aimed at Emergency Department Staff. It has been adapted from the “Newcastle, North Tyneside and Northumberland Guidelines for the diagnosis and Management of epilepsy in Primary and Secondary Care” Criteria for Use: this guideline covers
1. Status Epilepticus 2. First Fit (including referral form and patient information)
Prescribers should review patients for any contra-indications before initiating drugs. The drugs are recommended assuming there are no contra-indications to treatment, and no contra-indications develop.
http://nww.northoftyne.nhs.uk/documents/copy_of_policies/not-05-diagnosis-and-management-of-epilepsy
Alewis
Typewritten Text
Appendix 4 North Tyneside General Hospital Seizure Guidelines
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text

2
Emergency Anti-epileptic Drug (AED) therapy for convulsive status epilepticus
Premonitory stage Diazepam 10−20 mg given rectally, repeated once 15 minutes later if status continues to threaten, or midazolam 10 mg given buccally If seizures continue, treat as below
Early status Usually a 4mg bolus, repeated once after 10-15 minutes. However, in low−weight patients consider smaller initial bolus. Diazapam may be used if rate not critical.Give usual AED medication if already on treatment For sustained control or if seizures continue, treat as below.
Established status Phenytoin infusion and/orPhenobarbitone bolus of 10-15 mg/kg at a rate of 100 mg/minute
Refractory status* General anaesthesia, with one of:
- Propofol (1-2mg/kg bolus, then 2-10mg/kg/hour) titrated to effect.
- Midazolam (0.1-0.2mg/kg bolus, then 0.05-
0.5mg/kg/hour) titrated to effect.
- Thiopentone (3-5mg/kg bolus, then 3-5mg/kg/hour) titrated to effect; after 2-3 days infusion rate needs reduction as fat stores are saturated.
Anaesthetic continued for 12−24 hours after the last clinical or electrographic seizure, then dose tapered
*In the above scheme, the refractory stage (general anaesthesia) is reached 60/90 minutes after the initial therapy. If status epilepticus remains refractory: anaesthetics/critical care should be called, and propofol and thiopental used to control seizures. Critical life support is required. Transfer of intravenous agents to oral agents In patients with known epilepsy oral AEDs should continued throughout, via an NG tube if needed. If used, intravenous phenytoin should continue until the patient has been seizure free for 24 hours, then weaned down aiming to discontinue after 48 hours. In those without known epilepsy, intravenous phenytoin should be continued and further management discussed with a neurologist. Phenytoin is not normally recommended as a long term AED.

In all cases the reason for status epilepticus should be investigated. This may include poor concordance, infection, other drugs interacting with AEDs. Blood should be taken at baseline for assessment of drug levels to aid in the diagnosis of poor concordance. Pseudo seizures presenting as possible status epilepticus This can be difficult to diagnose. Patient safety is most important, but where this is a possible diagnosis, this should be discussed with a neurologist urgently. An EEG may be required to aid in diagnosis.
2. First Fit – See ‘Pathway for First Fits’ (Appendix 1)
- A patient may only be discharged following a first fit, if they have fully recovered. - Diagnosis Clear: -refer directly to the first seizure clinic & copy of the referral
should be sent to the GP. Results of any investigations (eg bloods) should be included with the referral, including a copy of the ECG. Transfer CT images (if done) to Newcastle Hospital PACS system.
- Diagnosis less certain: -refer to the GP for review - referral can be made by the GP. ADVICE to patient/carer: All patients referred with a suspected seizure, and their carers as appropriate, should be provided with preliminary advice at the time of referral, including; • To stop driving pending confirmation of the diagnosis • First aid if a further seizure occurs • Advice regarding work / leisure if dangerous • Reasons for referral to hospital • To take a witness of the seizure to the first hospital appointment An information leaflet is included in this guideline (Appendix 3)
Guidance relating to alcohol and first fit: See guidelines on Intranet (hyperlink) If a First Seizure has occurred more than a month after acute withdrawal, referral would generally be made.
Reference: NICE and North of Tyne Guidance

Pathway for First Fits
Was this a first seizure? No Consider causes of non-epileptic attacks eg. Arrhythmia, vaso-vagal etc.
Manage ABC Yes
Has hypoglycaemia been excluded? No
Yes
Treat hypoglycaemia & address the underlying cause then reassess.
Does the patient require an urgent CT?
Indications for CT scan prior to disposal
•Persistent new focal neurological deficit
•Persistent altered mental status
•Fever or persistent headache
•Recent head trauma
•History of cancer or HIV infection
•Patients with focal or partial onset seizure
•Anticoagulation or bleeding diathesis
•Past history of stroke / TIA
•Patients whose FU cannot be ensured (DW senior)
Yes Emergency CT head
Is it normal?
Yes No
Refer case to appropriate specialityNo
Are the ECG and blood results all normal? (U&Es, glucose & bone profile)
(Consider uraemia, hyponatraemia, hypoglycaemia, hypercalcaemia & prolonged QT)
Is the CXR normal? (all patients with signs or symptoms)
> 16 years of age
No Refer for admission
Yes
Consider discharge with appropriate advice and followup (see referral form)
*ADMIT ALCOHOL RELATED FITS DUE TO HIGH MORTALITY*

Referral form from A&E for adults with uncomplicated first generalised seizure (copy to GP) (Advice on completion of form: see pathway for information regarding this form) Inclusion Criteria
Patients > 16 yrs Clear history of first generalised epileptic seizure
Exclusion Criteria
• Patients with non-epileptic attacks • Those with symptomatic seizures e.g.
hypoglycaemia, acute trauma, eclampsia • People more suited to elderly care review
Name DOB Address Tel no Attach address label
Temp:
Pulse:
BP:
History: (continue onto second page if needed)
BM:
Investigations table (enter results or attach results sheet) ECG (send photocopy with form)
Urea Alk Ph Creat ALT Na Bil K Alb CO2 Hb Ca MCV GGT WCC Gluc Plat CXR
CT
Indications for CT scan prior to disposition • Persistent new focal neurological deficits • Persistent altered mental status • Fever or persistent headache • Recent head trauma • History of cancer or HIV infection • Patients with focal onset seizure • Anticoagulation or bleeding diathesis • Past history of stroke /TIA • Patients whose follow-up cannot be ensured (discuss
with senior) PLEASE ENSURE ALL FILMS ARE TRANSFERRED TO THE NEWCASTLE HOSPITALS SYSTEM
Discharge table – instructions in all sections must be fulfilled before referral is made Patient has fully recovered with no persistent neurological symptoms or signs (incl. headache)
Normal observations and investigations (incl. temperature)
Consider social circumstances prior to discharge (will the patient be safe?)
Patient has been given departmental written advice sheet - including driving and lifestyle changes
Patient suitable for First Seizure Clinic follow up - copies of form and all notes forwarded FAO Neurology - First Seizure Clinic - NB if you do not do this you may delay your patients follow up - fax number 0191 2825027
Copy referral form to GP
Retain original form in A&E notes
Hospital/department referring patient……………………………………………………………………………… Signature/Name (in capitals)………………………………………………………………………………………….. contact phone number of person faxing referral…………………………………………………………………..

Directorate of Neurosciences
Have you had a seizure?
First aid advice and Information
First Aid for Seizures If you have had one seizure, you and your relatives may be worried about what to do if you have another. Take the time to read this leaflet and show it to your friends and relatives so they can help you if you do have another seizure. If someone has a seizure don't panic. During the Seizure • If possible, move anything from around them that they may injure themselves on. • If you can, note the time. • Don't move the person unless they are in danger. • Don't put anything in their mouth. • Protect their head but don't restrict their movements. After the Seizure • Turn them on to their side (see diagram). • If they seem to be having difficulty breathing, check there is nothing blocking their
airway e.g. food, false teeth etc. • Don't leave them until they are fully recovered. Call an ambulance if ; • The seizure lasts more than 5 minutes. • If the person has injured themselves. • Or if the person has a series of seizures without regaining consciousness.

Seizures can be allowed to run their natural course following these guidelines. Recovery time varies from person to person. Some people need to rest for a few minutes; others may need to sleep for some time. Remember • If you have a driving licence you must inform the Driver Vehicle Licensing
Authority (DVLA) and you must not drive until they say you can. • Many people have only one seizure but it is wise to take some precautions for a
while. Consider what the risks may be to you in any situation and minimise them as far as possible. For example: consider using a shower rather than a bath, avoid climbing ladders or scaffolding and if you go swimming, go with a friend and inform the attendants.
• You may be referred to a specialist for further tests. When you attend your appointment make sure you take someone with you who has seen your attack.
Further information If you have any questions or require further information please contact: Epilepsy Society Tel: 01494 601 400 Website: http://www.epilepsysociety.org.uk Epilepsy Action Tel: 0808 800 5050 Website: http://www.epilepsy.org.uk Epilepsy Specialist: Nurse Penny Burt : Tel; 0191 282 3995 (Mon-Fri, 9am-5pm) Every effort has been made to ensure that the information in this leaflet is correct. It is, however, only intended as a guide and each individual's care may be different. Your doctor will advise you on your own personal treatment. Information produced by Epilepsy Specialist Nurse. July 2003 Reviewed; Jan 2006. Jan 2008, April 2011 Next review; April 2014

Further information/contacts…………………………………………………………….. Clinical Lead Signature ………………….Print Name…P Stamp……….Date……………… Authors Signature…………………………Print Name…P Stamp………Date……………… Trust Approved Signature………………..Print Name…P Stamp………Date……………… Add to Intranet –Emergency Care and Medicine

Referral form from A&E for adults with uncomplicated first generalised seizure (copy to GP) (Advice on completion of form: see pathway for information regarding this form) Keywords - Epilepsy; First fit For further information, see Seizure Management in Emergency Care (Adult) Guideline Inclusion Criteria
Patients > 16 yrs Clear history of first generalised epileptic seizure
Name DOB Address Tel no Attach address label
Exclusion Criteria
• Patients with non-epileptic attacks • Those with symptomatic seizures e.g.
hypoglycaemia, acute trauma, eclampsia • People more suited to elderly care review
History: (continue onto second page if needed)
Temp:
Pulse:
BP:
BM:
Investigations table (enter results or attach results sheet) ECG (send photocopy with form)
Indications for CT scan prior to disposition • Persistent new focal neurological deficits • Persistent altered mental status • Fever or persistent headache • Recent head trauma • History of cancer or HIV infection • Patients with focal onset seizure • Anticoagulation or bleeding diathesis • Past history of stroke /TIA • Patients whose follow-up cannot be ensured (discuss
with senior) PLEASE ENSURE ALL FILMS ARE TRANSFERRED TO THE NEWCASTLE HOSPITALS SYSTEM
Urea Alk Ph Creat ALT Na Bil K Alb CO2 Hb Ca MCV GGT WCC Gluc Plat CXR
CT
Discharge table – instructions in all sections must be fulfilled before referral is made Patient has fully recovered with no persistent neurological symptoms or signs (incl. headache)
Normal observations and investigations (incl. temperature)
Consider social circumstances prior to discharge (will the patient be safe?)
Patient has been given departmental written advice sheet - including driving and lifestyle changes
Patient suitable for First Seizure Clinic follow up - copies of form and all notes forwarded FAO Neurology - First Seizure Clinic - NB if you do not do this you may delay your patients follow up
fax number 0191 282 4085
Copy referral form to GP
Retain original form in A&E notes
Hospital/department referring patient……………………………………………………………………………… Signature/Name (in capitals)………………………………………………………………………………………….. contact phone number of person faxing referral…………………………………………………………………..
Alewis
Typewritten Text
Alewis
Typewritten Text
Alewis
Typewritten Text

1
Relevant to: (Northumbria Healthcare Foundation Trust NHS Trust; North Tyneside General Hospital etc)
Febrile seizure is a benign seizure that occurs between the age of 6 months and 5 years, peak incidence at 18 months. It is usually associated with fever or rising temperature with no intracranial infection or defined cause for their seizure. It occurs in a neurodevelopmentally normal child, with no previous non-febrile fits. . 1 3 4
Criteria for diagnosis: 1 3 4
Simple febrile seizure – all of the following;
Complex febrile seizure - any of the following;
Fit is generalised tonic-clonic Any focal symptoms Duration < 15 minutes, Duration >15 minutes No more than one seizure in 24 hours Recurrence within 24 hours Followed by full recovery within 1 hour Not followed by full consciousness within
one hour Investigations including lumbar puncture and neuro-imaging (CT brain if focal seizure) are often warranted for complex febrile seizures. Initial management: see THE FITTING CHILD - Convulsions - Paediatrics
Febrile Convulsions - Paediatrics
Document Type: Clinical Guideline Clinical Lead: Dr Stephen Bruce Author/s: Dr Anjali Chaudhari Directorate: Child Health Approved by Sub Committee/Group: Child Health Clinical Policy Group
Date Approved by Sub Committee/Group:TBCDate Approved by Clinical Guidelines Group:14/12/2011 Date of Issue: October 2011 Review Date: October 2014 Version: 1
Febrile seizures
Simple Complex
Important Notes/Exclusions Criteria for Use: For use in paediatric services

2
Evaluation of a child with a febrile seizure: • Detailed history including family history of febrile seizure, and epilepsy. 3
• Examine carefully for focus for the temperature, evidence of meningitis, underlying neurological
deficit, asymmetry, and stigmata of neurocutaneous markers and measuring the head circumference. 3
• Routine blood tests are not recommended unless where clinically indicated,3
and urine infection needs to be ruled out.
• In younger children signs of meningitis can be subtle. So consider a lumbar puncture in children less than 12 months unless a site of infection is clearly identified.
The decision not to perform an LP should be made by a middle grade or more senior doctor
• A short period of close observation is reassuring. Control fever: • Paracetamol is the most useful drug. • Ibuprofen is also useful (use with caution if clinically dehydrated). (Recent NICE guidelines for fever advice against use of paracetamol for just reduction of fever. Also, alternating paracetamol and Ibuprofen is not recommended by NICE)
• Remove most of clothing, but do not allow child to become cold peripherally
• Use fan to move air in room if necessary, but do not direct onto child
• Tepid sponging is of no value as it often causes cutaneous vasoconstriction Admission: Offer admission to all children with their first febrile convulsion. Counsel parents: • Increasingly, a genetic predisposition is recognised, with febrile seizures occurring in
families but the exact mode of inheritance varies between families. • The risk of another child having febrile seizure is one in five if one sibling is affected, and
one in three if both parents and a previous child had febrile seizure. 1 • Other risk factors associated with an increased rate of febrile seizure recurrence include
young age at onset (less than 12 months), history of simple or complex febrile seizures, and body temperature at onset of less than 40 °C.
• Age at onset seems the most constant predictive factor, with 50% of children aged less than 12 months, and 30% of children aged more than 12 months, presenting with a recurrent febrile seizure
• Simple febrile seizures may slightly increase the risk of developing epilepsy but have no adverse effects on behaviour, scholastic performance, or neurocognition.
• Prevent by controlling fever - as above • Regular prophylactic anticonvulsants are not indicated for treatment of simple febrile
seizure as there is no evidence to reduce the risk of epilepsy developing and considerable potential side effects exist. 3 4

3
• Issue Advice/Information leaflet
REFERENCES
(1) Leena D Mewasingh. Febrile seizures. BMJ clinical evidence 2008; 05:324.
(2) Feverish illness in children .Assessment and initial management in children younger than five years. NICE clinical guidelines 47.
(3) C Waruiru,R Appleton. Febrile seizures: an update. Arch Dis Child 2004; 89:751-56.
(4) Lynette G Sadleir, Ingrid E Scheffer. Febrile seizures. BMJ 2007; 334:307-11.
AUDITABLE OUTCOMES
Further information/contacts……………………………………………………………..
Clinical Lead Signature …………Print Name Dr Stephen Bruce Date October 2011 Authors Signature…………………Print Name Dr Anjali Chaudhari Date October 2011 Trust Approved Signature………………..Print Name……………………Date……………… Add to Intranet – Please Indicate appropriate Specialties: Paediatrics & Emergency Care

Status Epilepticus – Adults Issued: 23/07/2014 Review: May 2015
Status Epilepticus in Adults
If seizure persists after 10 minutes
If seizure persists after 10 minutes
If seizure persists after 20 minutes
Notes: In refractory status epilepticus consider the diagnosis of pseudostatus and the use of other drugs (eg Phenobarbitone 10mg/kg) References: Lockey A S., 2002. Emergency Department Drug Therapy for status epilepticus in adults, Emergency Medicine Journal;19(2), pp 96-100. National Institute for Health and Care Excellence (NICE), 2012. The epilepsies: the diagnosis and management in adults and children in primary and secondary care, CG137 – issued January 2012.
Manage ABC High flow oxygen
IV access Check glucose and treat
Lorazepam 2-4mg IV over 2 minutes If alcohol misuse suspected give Pabrinex
High Potency 1&2 (2 pairs)
Lorazepam 2-4mg IV over 2 minutes
Phenytoin 20mg/kg IVI at a rate not to exceed 50mg/min with BP/ECG
monitoring
General anaesthesia
Alewis
Typewritten Text
Appendix 5 - Cumbria Guidelines
Alewis
Typewritten Text

Status Epilepticus – Adults Issued: 23/07/2014 Review: May 2015
Status Epilepticus in Adults
Document Type: Clinical Guideline Author/s & Clinical Lead: James Hayton Approved by Business Unit/ Committee: Emergency Department Date approved by Business Unit/Sub Committee: 22/04/2014
Date ratified by Clinical Guidelines Group: 19/06/2014 Date of Issue: 23/07/2014 Review Date: May 2015 Version: 1.2
Relevant to: North Cumbria University Hospitals NHS Trust Please complete additional information required for implementation and publication on the Intranet
Changes made: None Brief Description: To provide information and advice on management of adults patients (16 years and over) with generalized convulsive status epilepticus Specialities: Emergency Care, General Medicine Keywords: Status Epilepticus, Epilepsy, Convulsion, Seizures, GCSE, Further information / local contact(s): James Hayton, EM Consultant, WCH Staff training: Incorporated in EM and general medicine training Dissemination: Available on trust website Auditable Outcomes: TBC

Status epilepticus 2012-14
Status Epilepticus – Paediatrics Issued:23/07/2014 Review: December 2014
Status Epilepticus - Paediatrics Call for senior paediatric help at an early stage Follow each step until fits resolve, but do not treat post-ictal posturing as seizure Prepare next step in algorithm immediately after previous one administered Do not give more than 2 doses of benzodiazepine, including any pre-hospital doses
Diazepam (IV)
If lorazepam not available Diazepam (rectal) Midazolam (buccal) Paraldehyde (rectal)
volume of 50:50 diluted Aged 1month – 12 years: 300-400microgram/kg (max 10mg)
Aged 1 month–2 yr: 5 mg
Aged <6 months: 300 microgram/kg (max 2.5 mg)
Neonate 0.8m/kgL
Aged >12 yr: 10 mg Aged 2–12 yr: 5–10 mg
Aged 6 months–1 yr: 2.5 mg
1 month – 18 yr 0.8ml/kg
Aged >12 yr: 10 mg Aged 1–5 yr: 5 mg Aged 5–10 yr: 7.5 mg Aged >10 yr: 10 mg Age 5–18 yr: 5–10 mL
Airway High flow oxygen
Glucose measurement
Vascular access?
Lorazepam* 0.1 mg/kg IV/IO (max 4 mg) over 6 min (dilute 1:1 with sodium chloride 0.9%)
Midazolam buccal$
(see Table below for dose)
Lorazepam* 0.1 mg/kg IV/IO#
Phenytoin** 20 mg/kg IV/IO over 20 min with cardiac monitoring
Call anaesthetist/PICU RSI with thiopental
CT scan not routine: only if history of head injury or new focal seizure
Yes No
If seizure continuing 10 min after start of step 1
Step1
Step 2
Step 3
Pre-prepare phenytoin. Call for senior help
If seizure continuing 10 min after start of step 2
Reconfirm it is an epileptic seizure
If seizure continuing 10 min after start of step 3
* If lorazepam not available give IV diazepam. $ If buccal midazolam not available give rectal diazepam # If vascular access and intraosseous still not obtained give paraldehyde PR: 0.8 mL/kg ready
mixed solution or 0.4 mL/kg diluted with equal volume of olive oil **If already taking phenytoin, give phenobarbital 20 mg/kg IV/IO over 20 min diluted 1:1 with water
for injection(available from SCBU at WCH and CIC)

Status epilepticus 2012-14
Status Epilepticus – Paediatrics Issued:23/07/2014 Review: December 2014
Status Epilepticus - Paediatrics Document Type: Clinical Guideline Clinical Lead: James Hayton Author/s: North Staffordshire Guideline Group Approved by Business Unit/ Committee: Emergency Department Date approved by Business Unit/Sub Committee: 22/04/2014
Date ratified by Clinical Guidelines Group: 19/06/2014 Date of Issue: 23/07/2014 Review Date: December 2014 Version: 1.0
Relevant to: North Cumbria University Hospitals NHS Trust
Please complete additional information required for implementation and publication on the Intranet
Changes made: Note regarding emergency supply of phenobarbitone from SCBU at CIC/WCH. Brief Description: To provide information and advice on management of paediatric patients (under 16 years old) with status epilepticus Specialities: Emergency Care, Paediatrics Keywords: Status Epilepticus, Epilepsy, Convulsion, Seizures Further information / local contact(s): James Hayton, EM Consultant, WCH Staff training: Incorporated in EM and Paediatric training Dissemination: Available on trust website Auditable Outcomes: Compliance with flowchart