Straight tubules of proliferative endometrium Early secretory endometrium with subnuclear vacuoles.
75
-
Upload
joella-bryant -
Category
Documents
-
view
241 -
download
0
Transcript of Straight tubules of proliferative endometrium Early secretory endometrium with subnuclear vacuoles.


Straight tubules of proliferative endometrium

Early secretory endometrium with subnuclear vacuoles

Basal vacuoles (arrow) appear 36 to 48 hours after ovulation

Tortuous glands of late secretory endometrium with luminal secretions

Menses - endometrium is fragmented and mixed with blood

Accumulation of plasma cells in chronic endometritis

UTERUS: INFLAMMATIONUTERUS: INFLAMMATION
Acute bacterialAcute bacterial only in puerperium (strep, staph, clostridium, mixed)only in puerperium (strep, staph, clostridium, mixed) NOTNOT gonococcal, chlamydia gonococcal, chlamydia
Chronic bacterialChronic bacterial chronic PID (pelvic inflammatory disease)chronic PID (pelvic inflammatory disease) tuberculosistuberculosis IUDIUD retained placental productsretained placental products

Multiple granulomas within endometrium from TB
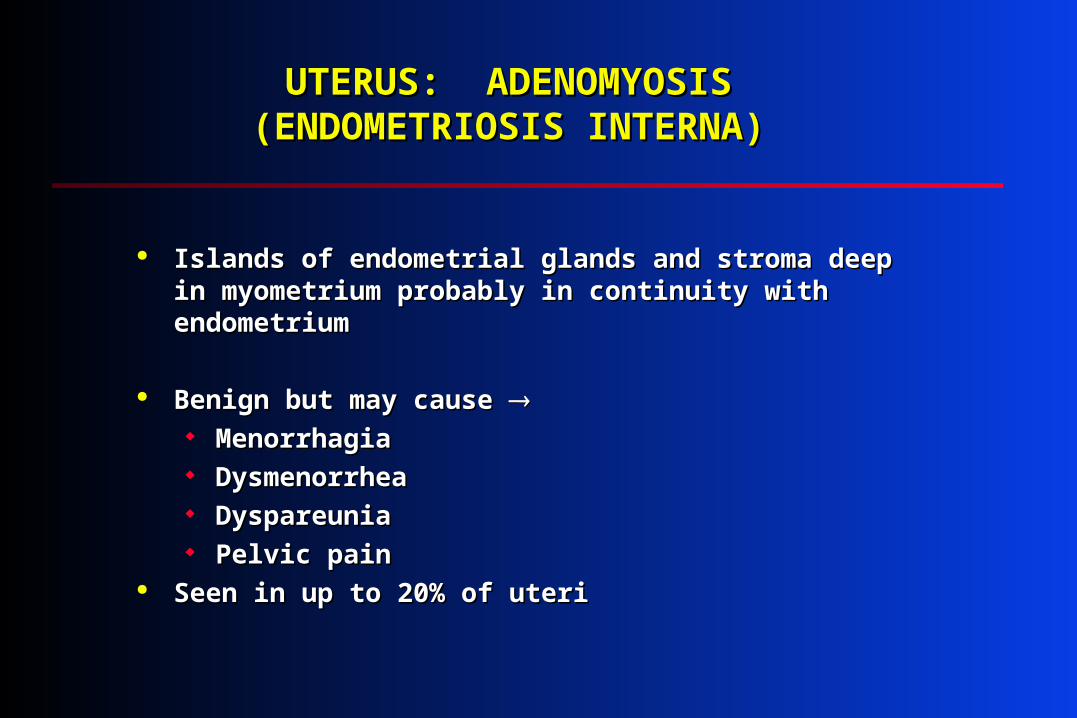
UTERUS: ADENOMYOSIS UTERUS: ADENOMYOSIS (ENDOMETRIOSIS INTERNA)(ENDOMETRIOSIS INTERNA)
Islands of endometrial glands and stroma deep in Islands of endometrial glands and stroma deep in myometrium probably in continuity with endometriummyometrium probably in continuity with endometrium
Benign but may cause Benign but may cause MenorrhagiaMenorrhagia Dysmenorrhea Dysmenorrhea Dyspareunia Dyspareunia Pelvic pain Pelvic pain
Seen in up to 20% of uteriSeen in up to 20% of uteri
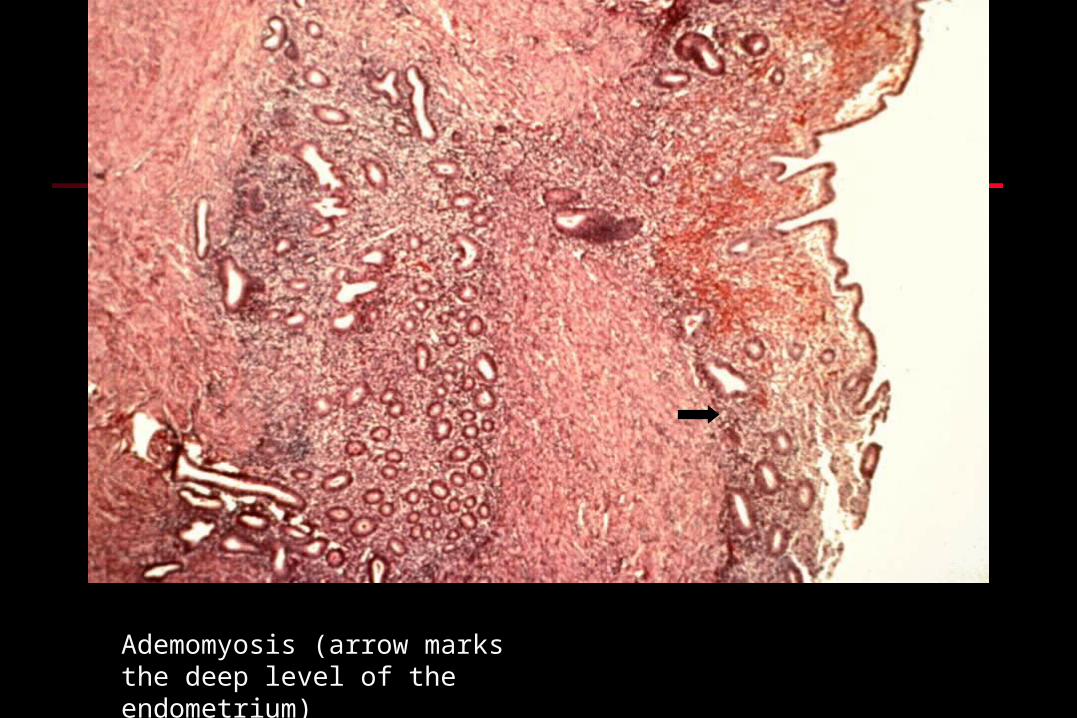
Ademomyosis (arrow marks the deep level of the endometrium)

Adenomyosis with circumscribed area of glands within myometrium
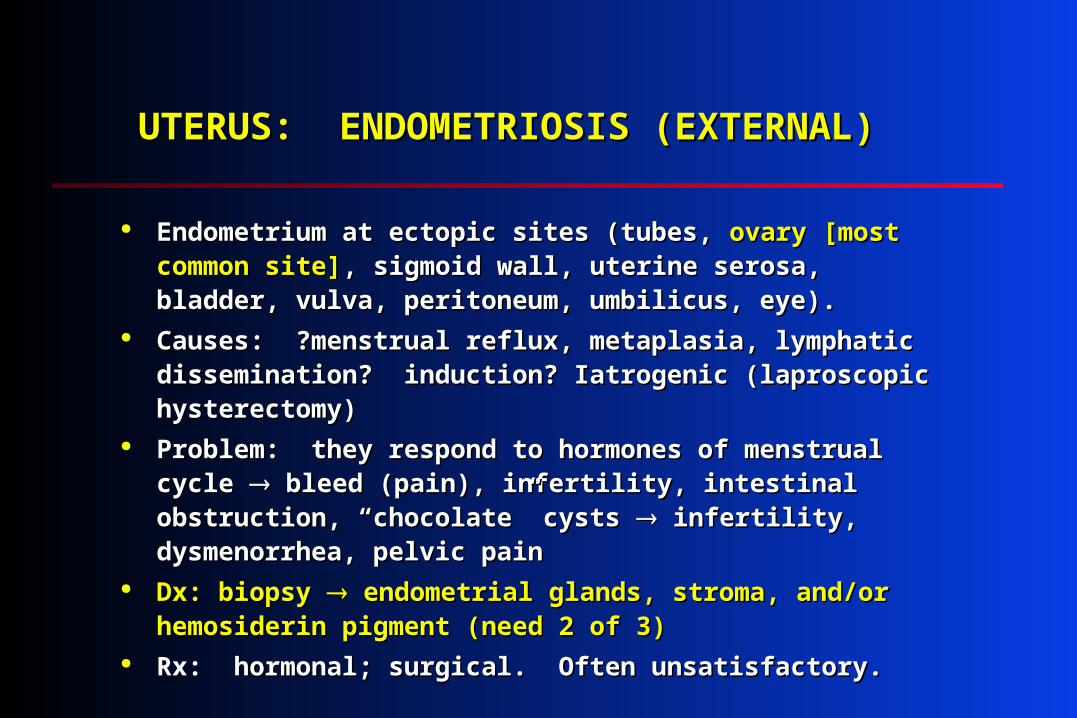
UTERUS: ENDOMETRIOSIS (EXTERNAL)UTERUS: ENDOMETRIOSIS (EXTERNAL)
Endometrium at ectopic sites (tubes, Endometrium at ectopic sites (tubes, ovaryovary [most common [most common site]site], sigmoid wall, uterine serosa, bladder, vulva, peritoneum, , sigmoid wall, uterine serosa, bladder, vulva, peritoneum, umbilicus, eye).umbilicus, eye).
Causes: ?menstrual reflux, metaplasia, lymphatic Causes: ?menstrual reflux, metaplasia, lymphatic dissemination? induction? Iatrogenic (laproscopic dissemination? induction? Iatrogenic (laproscopic hysterectomy)hysterectomy)
Problem: they respond to hormones of menstrual cycle Problem: they respond to hormones of menstrual cycle bleed (pain), infertility, intestinal obstruction, “chocolate” bleed (pain), infertility, intestinal obstruction, “chocolate” cysts cysts infertility, dysmenorrhea, pelvic pain infertility, dysmenorrhea, pelvic pain
Dx: biopsy Dx: biopsy endometrial glands, stroma, and/or hemosiderin endometrial glands, stroma, and/or hemosiderin pigment (need 2 of 3)pigment (need 2 of 3)
Rx: hormonal; surgical. Often unsatisfactory.Rx: hormonal; surgical. Often unsatisfactory.

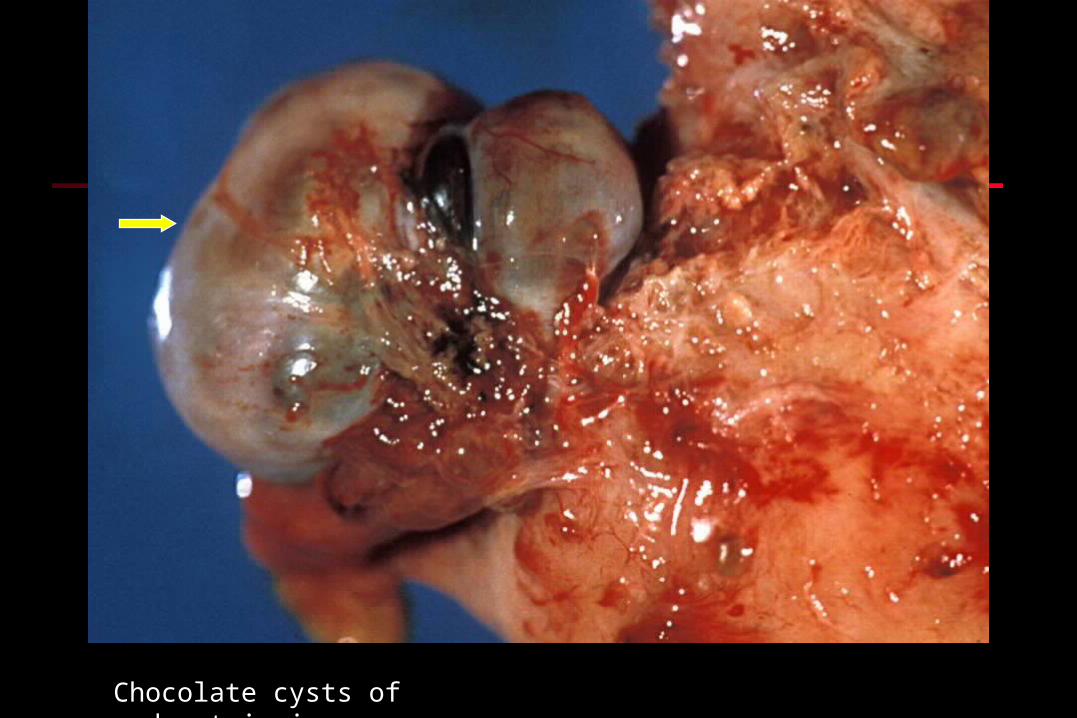
Chocolate cysts of endometriosis

Bilateral chocolate cysts flank opened uterus

Opened cyst of endometriosis

Wall of endometrial cyst
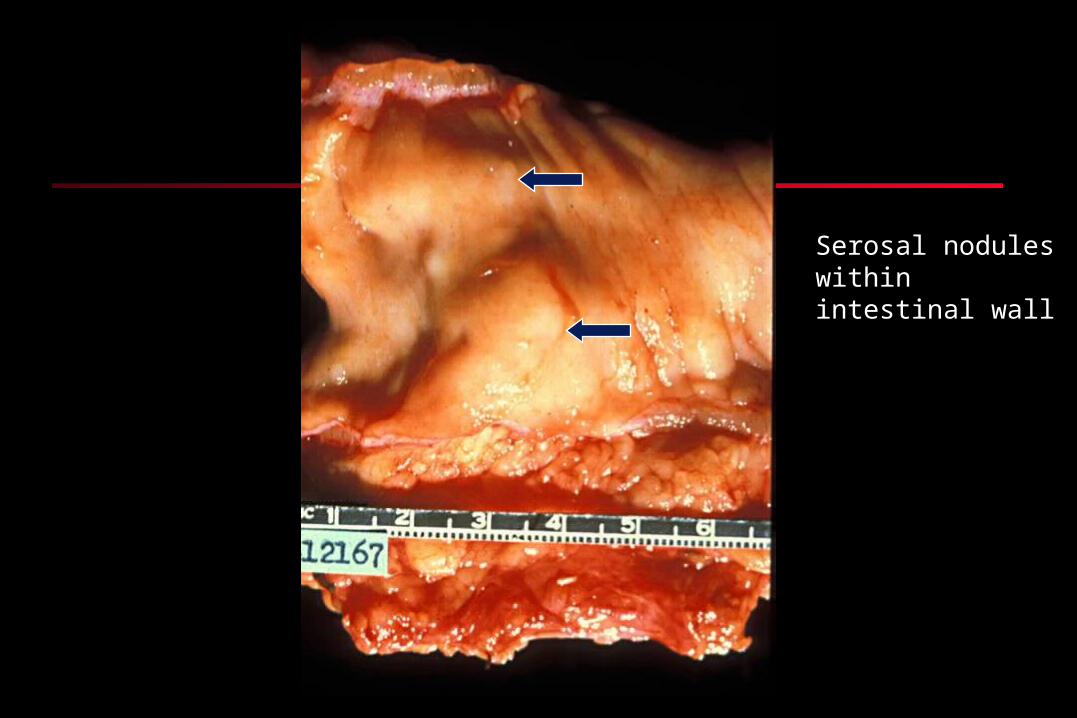
Serosal nodules within intestinal wall

Endometriosis within intestinal wall
Mucosa
Fat

Wall of cyst of endometriosis containing numerous hemosiderin-laden macrophages
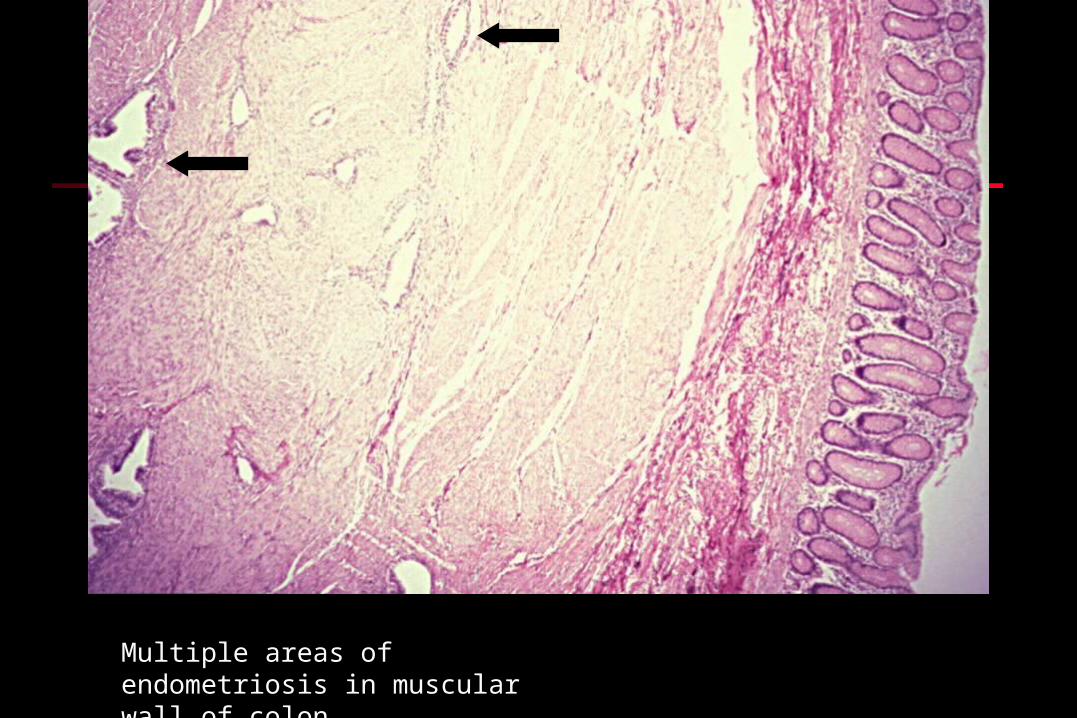
Multiple areas of endometriosis in muscular wall of colon
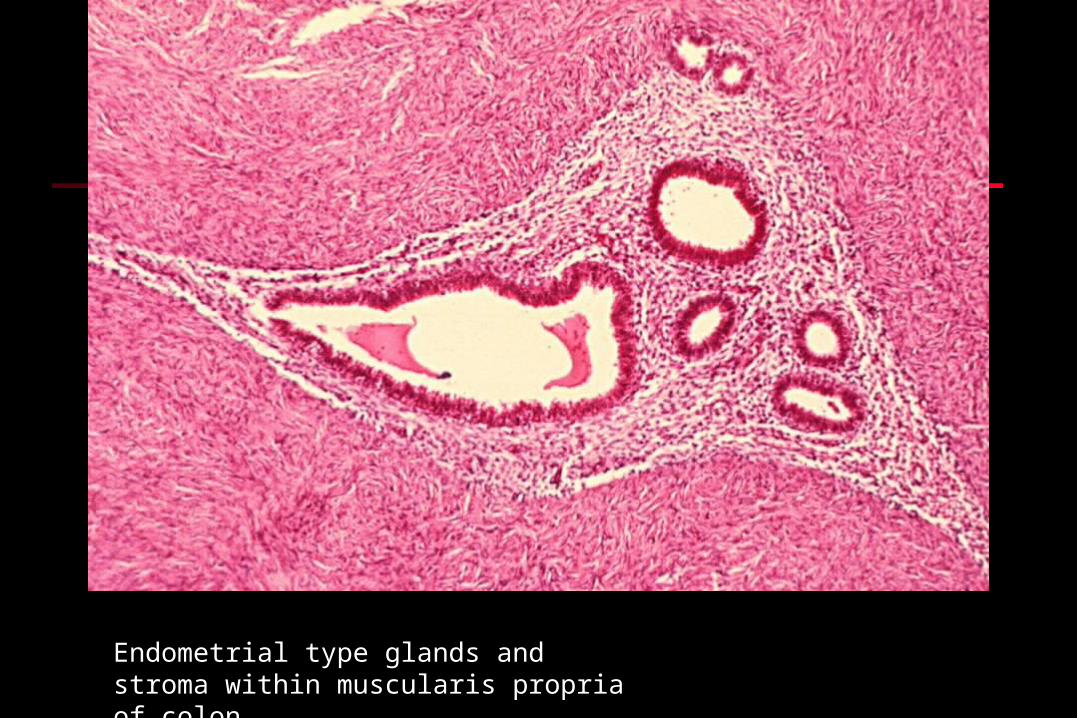
Endometrial type glands and stroma within muscularis propria of colon

Early secretory endometrium in focus of endometriosis

Umbilical cyst of endometriosis
Dysfunctional Uterine BleedingDysfunctional Uterine Bleeding
Excessive bleeding during or between Excessive bleeding during or between menstrual periods menstrual periods
DDx includes polyps, endometrial hyperplasia, DDx includes polyps, endometrial hyperplasia, trophoblastic disease, adenomyosis, & trophoblastic disease, adenomyosis, & carcinoma carcinoma
Bx endometrium to rule out malignancy Bx endometrium to rule out malignancy Most often due to anovulatory cycle which Most often due to anovulatory cycle which
leads to prolonged estrogenic stimulation.leads to prolonged estrogenic stimulation. See Robbins PathologySee Robbins Pathology

Other Endometrial ChangesOther Endometrial Changes
Oral contraceptives: Oral contraceptives: Inactive glands Inactive glands Predecidualized stroma (abundant Predecidualized stroma (abundant
cytoplasm as in pregnancy)cytoplasm as in pregnancy) Postmenopausal:Postmenopausal:
Senile cystic atrophy Senile cystic atrophy Atrophic endometrium with cystic dilatation Atrophic endometrium with cystic dilatation
of glandsof glands

Widely spaced glands and stromal cells with abundant cytoplasm 2 to oral contraceptives (predecidual)

Senile cystic atrophy

UTERUS: ENDOMETRIAL HYPERPLASIAUTERUS: ENDOMETRIAL HYPERPLASIA
Clinical presentation: abnormal uterine bleedingClinical presentation: abnormal uterine bleeding Mechanism: prolonged estrogenic stimulation Mechanism: prolonged estrogenic stimulation
(polycystic ovary, estrogen-producing tumors, (polycystic ovary, estrogen-producing tumors, estrogen Rx, etc.)estrogen Rx, etc.)
Histo: simple or complex cystic hyperplasia, Histo: simple or complex cystic hyperplasia, adenomatous or atypical hyperplasia (25% of latter adenomatous or atypical hyperplasia (25% of latter ca)ca)
Dx and Rx: D&C; hormonal , surgeryDx and Rx: D&C; hormonal , surgery
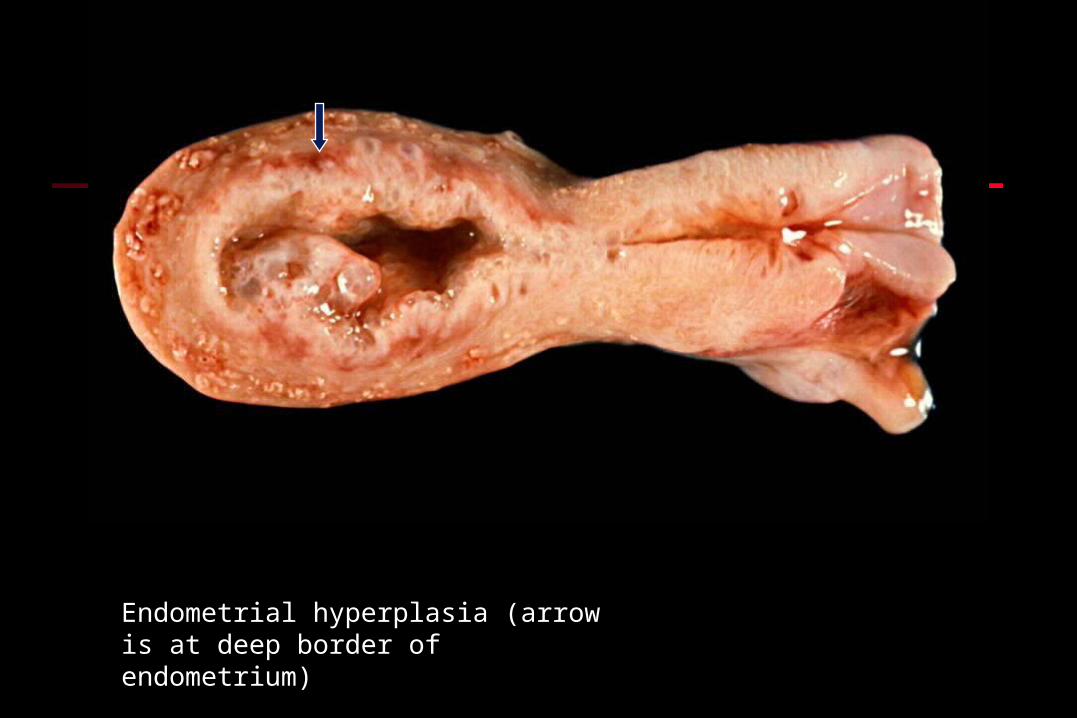
Endometrial hyperplasia (arrow is at deep border of endometrium)

Benign simple cystic hyperplasia
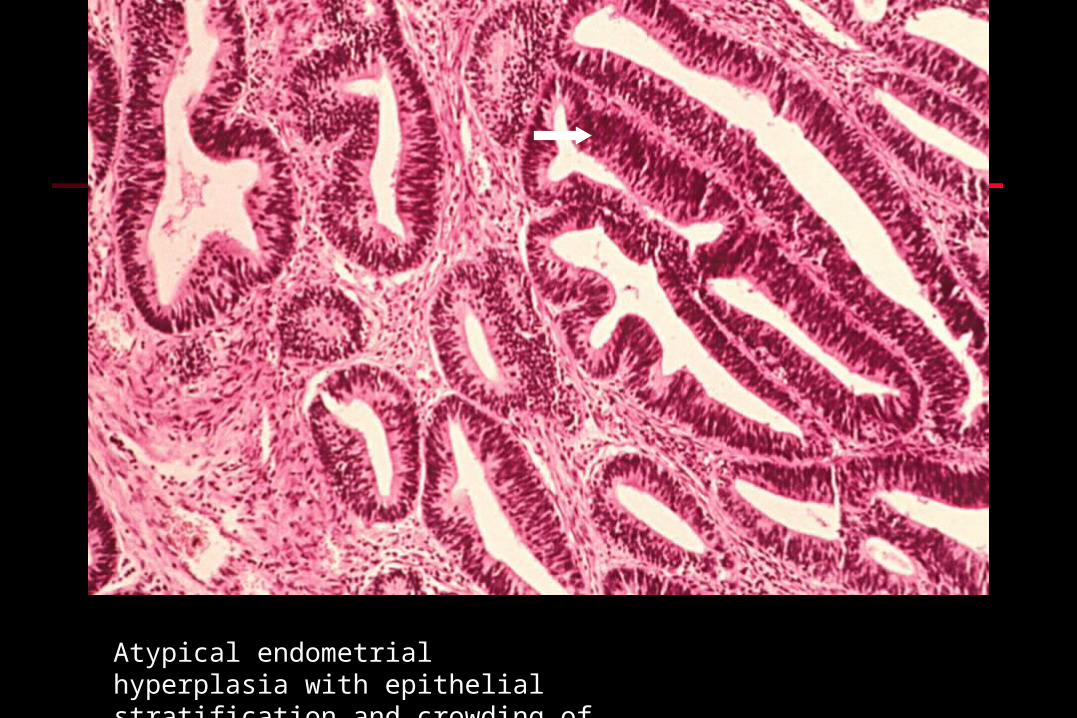
Atypical endometrial hyperplasia with epithelial stratification and crowding of glands

UTERUS: POLYPSUTERUS: POLYPS
Pathology: cystic endometrial glands with Pathology: cystic endometrial glands with
stroma; benign (rarely cancer may arise within stroma; benign (rarely cancer may arise within
polyp)polyp)
Age: any but especially perimenopausalAge: any but especially perimenopausal
Sx: ulceration Sx: ulceration bleeding bleeding
Rx: D&CRx: D&C

Opened uterus with endometrial polyp filling lumen

Infarcted endometrial polyp

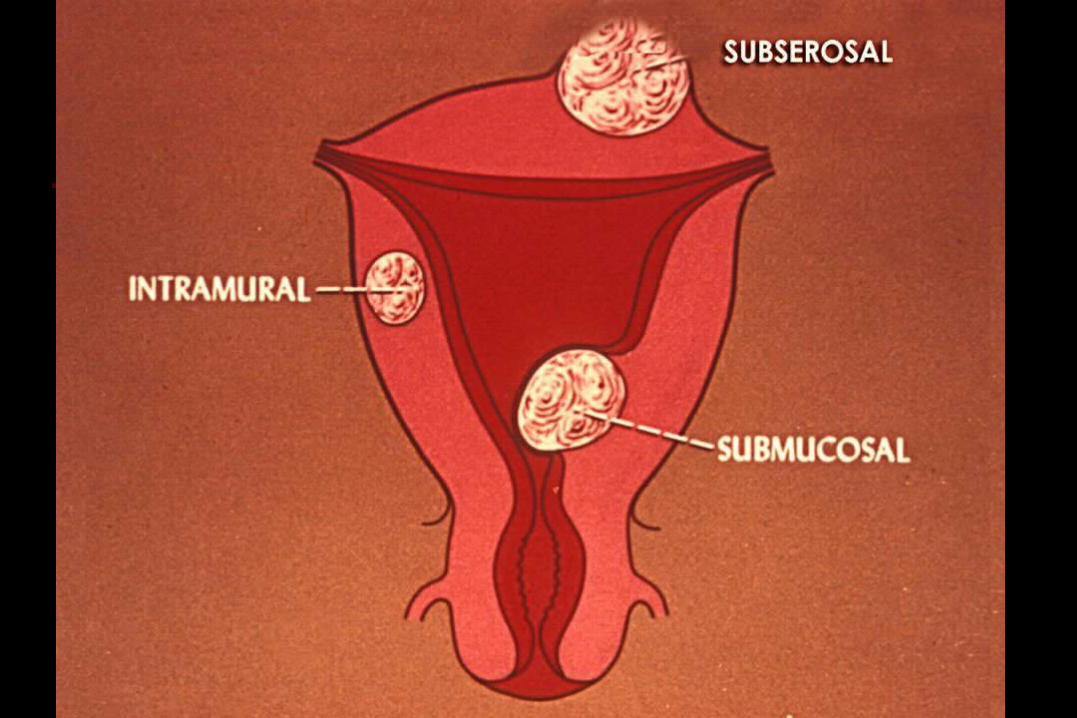
UTERUS: LEIOMYOMA (“FIBROID”)UTERUS: LEIOMYOMA (“FIBROID”)
Location: submucosal, intramural, subserosal, Location: submucosal, intramural, subserosal, broad ligament, cervixbroad ligament, cervix
Common; benign; estrogen-responsive.Common; benign; estrogen-responsive. CSx: bleeding; large obstruct birth (dystocia); CSx: bleeding; large obstruct birth (dystocia);
spontaneous abortionspontaneous abortion Histo: whorled fascicles of smooth muscle cells; Histo: whorled fascicles of smooth muscle cells;
clear cell and pleomorphic variations; also clear cell and pleomorphic variations; also “intravenous leiomyomyosis”“intravenous leiomyomyosis”
Leiomyosarcoma: arise de novo; sarcomatous Leiomyosarcoma: arise de novo; sarcomatous histo; usually fatalhisto; usually fatal

Uterine architecture distorted by large leiomyoma

Previous specimen opened to demonstrate leiomyoma

Cut surface of leiomyoma. Tumor is firm, white, and usually has a whorled appearance

Submucosal leiomyoma
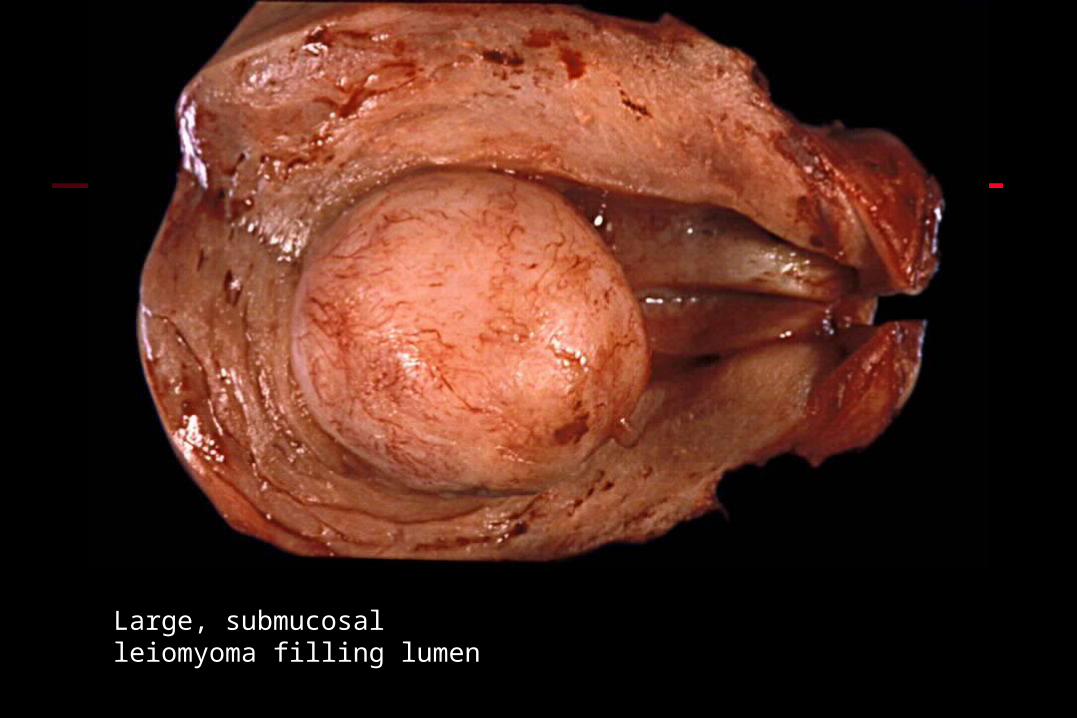
Large, submucosal leiomyoma filling lumen

Cut surface of submucosal “fibroid”

Infarcted submucosal leiomyoma extending through cervical os

Multiple leiomyomata


Pedunculated subserosal leiomyoma

Distorted uterus from multiple leiomyomata

Fascicles of smooth muscle cells of leiomyoma

Fascicles of smooth muscles: individual nuclei are cigar-shaped and there are no mitoses. When bundle is cut in cross-section you get a halo around the nucleus

Cellular leiomyoma
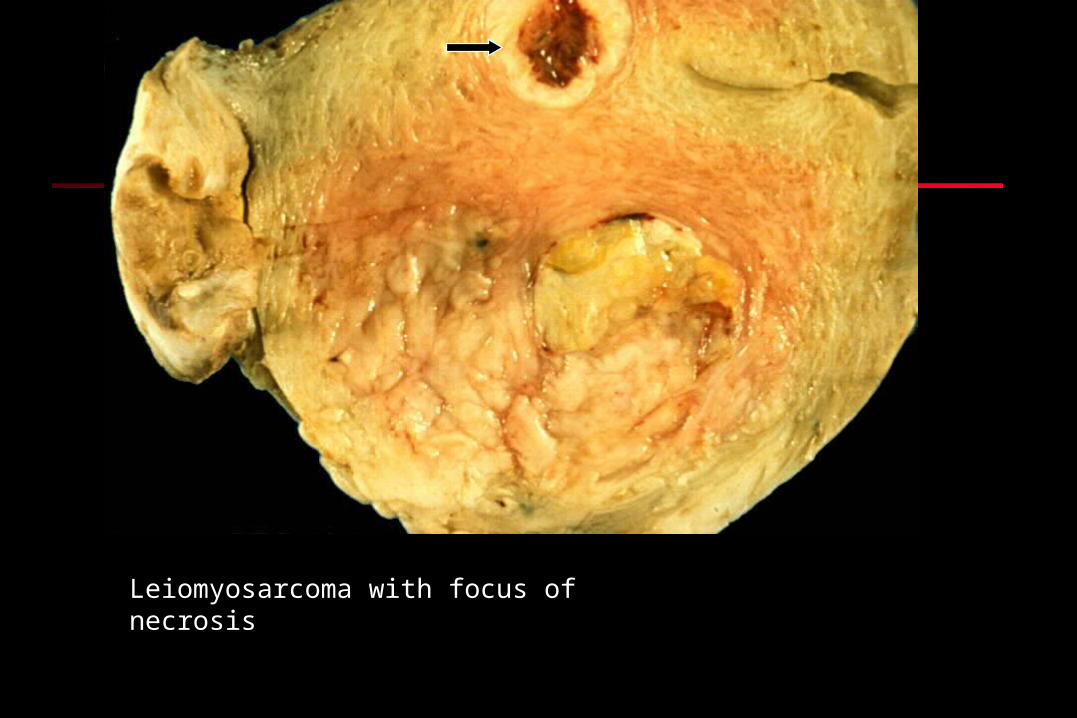
Leiomyosarcoma with focus of necrosis
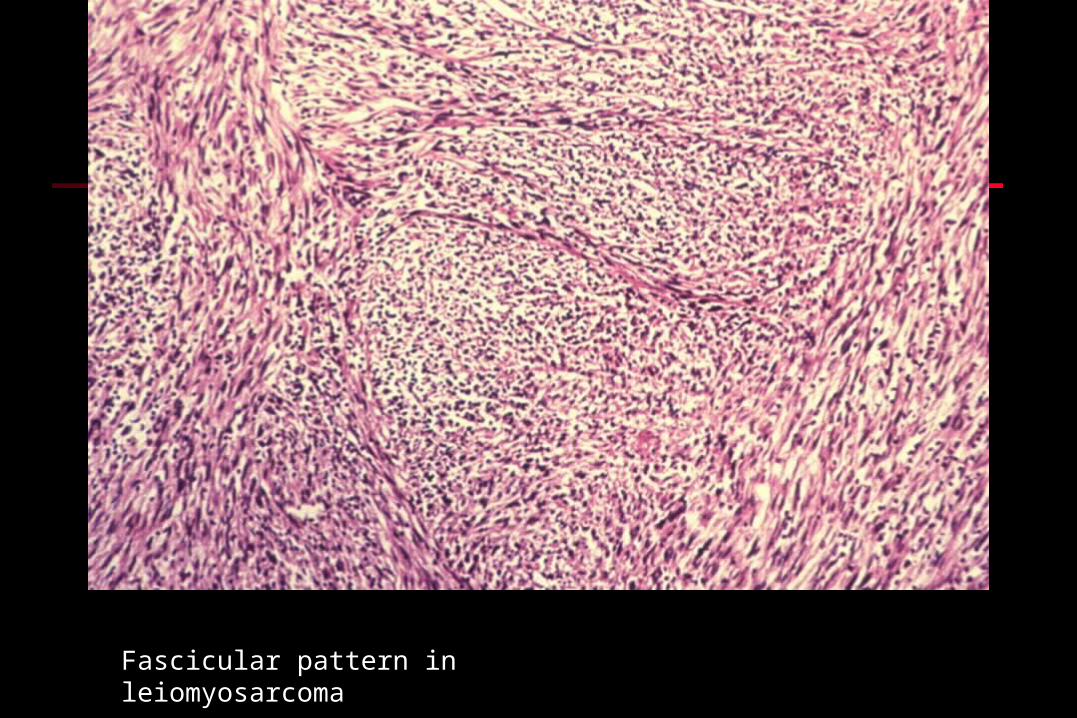
Fascicular pattern in leiomyosarcoma
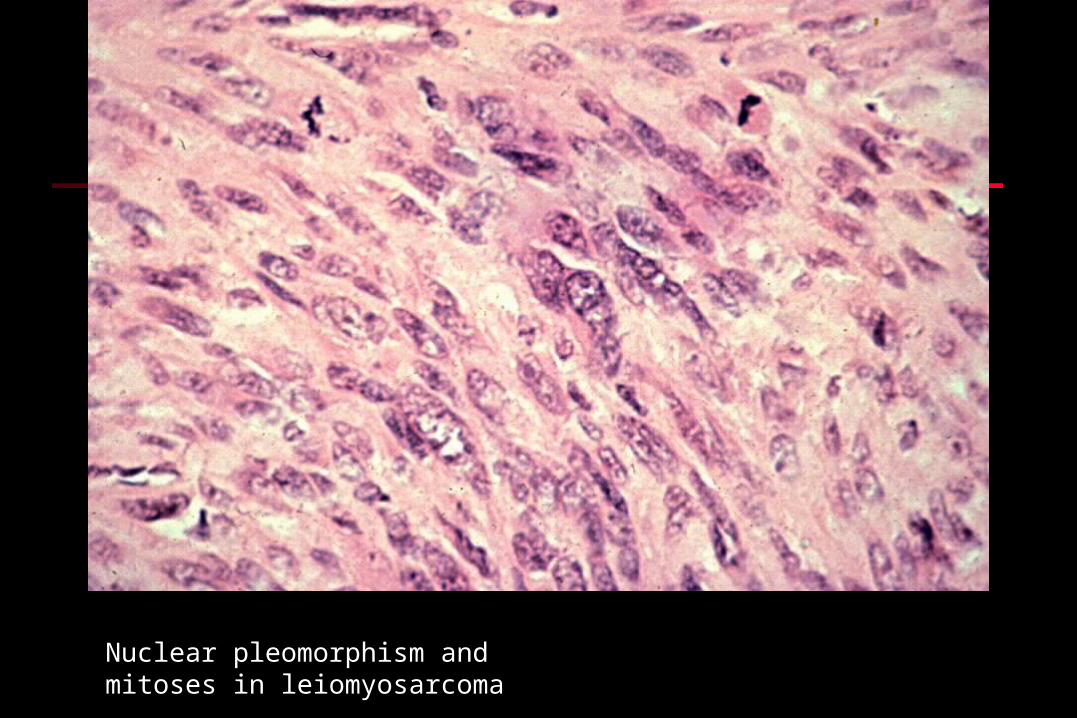
Nuclear pleomorphism and mitoses in leiomyosarcoma
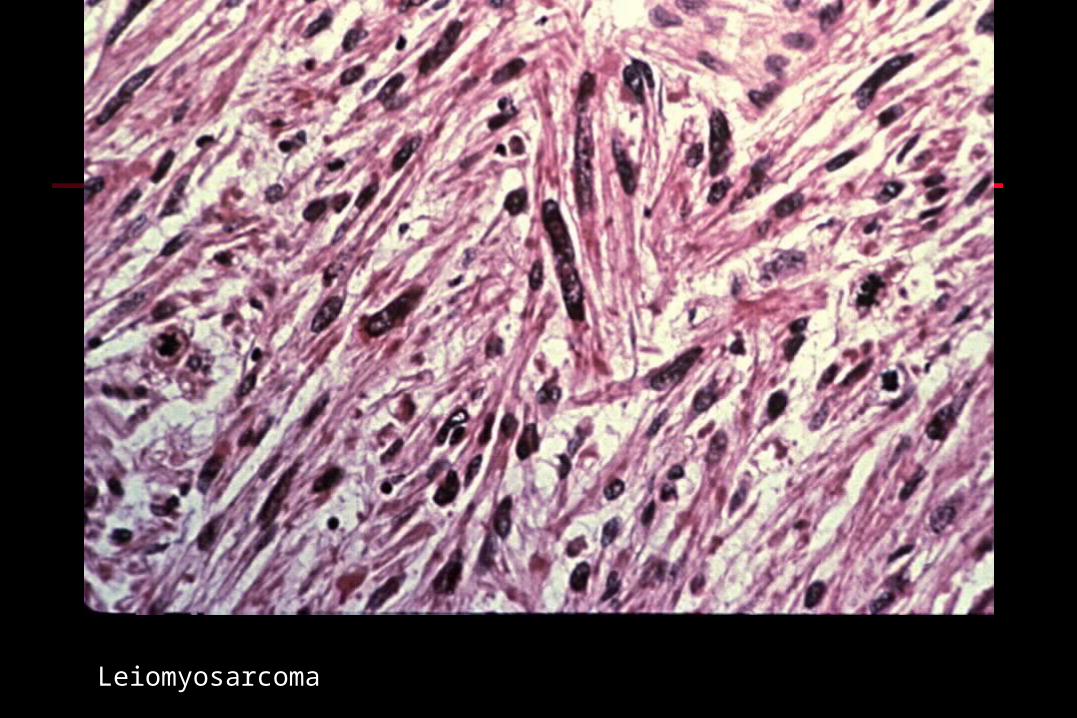
Leiomyosarcoma

UTERUS: ENDOMETRIAL ADENOCARCINOMA (1)UTERUS: ENDOMETRIAL ADENOCARCINOMA (1)
Epidemiology: risk factorsEpidemiology: risk factors postmenopausalpostmenopausal Obesity – common risk factor, likely has to do with estrogenObesity – common risk factor, likely has to do with estrogen diabetesdiabetes hypertensionhypertension infertility infertility hyperestrinismhyperestrinism
nulliparousnulliparous anovulatory cyclesanovulatory cycles estrogenic estrogenic tumorstumors RxRx

UTERUS: ENDOMETRIAL ADENOCARCINOMA (2)UTERUS: ENDOMETRIAL ADENOCARCINOMA (2)
Histology:Histology:
most endometrioid (adenocarcinomas with villoglandular most endometrioid (adenocarcinomas with villoglandular
histology)histology)
some adenoca with foci of squamous metaplasia some adenoca with foci of squamous metaplasia
(adenoacanthoma)(adenoacanthoma)
some adenoca with malignant squamous foci (10% then some adenoca with malignant squamous foci (10% then
truly called adenosquamous ca)truly called adenosquamous ca)
variations: variations:
clear cell caclear cell ca
papillary serous capapillary serous ca Very aggressive

UTERUS: ENDOMETRIAL ADENOCARCINOMA (3)UTERUS: ENDOMETRIAL ADENOCARCINOMA (3)
Staging: similar to cervixStaging: similar to cervix
Grading: FIGO system, I < 5% solid, II = 5-50% Grading: FIGO system, I < 5% solid, II = 5-50%
solid, III > 50% solid (serous papillary & clear solid, III > 50% solid (serous papillary & clear
cell are grade III tumors)cell are grade III tumors)
Sx: postmenopausal bleedingSx: postmenopausal bleeding
Dx and Rx: D&C; hysterectomy; radiationDx and Rx: D&C; hysterectomy; radiation
Prognosis: stage 1 = 90%; III = 20% 5 yr Prognosis: stage 1 = 90%; III = 20% 5 yr

Stage I endometrial adenocarcinoma. Endometrium is thickened and irregular.

Endometrial carcinoma: tumor is friable and focally ulcerated.
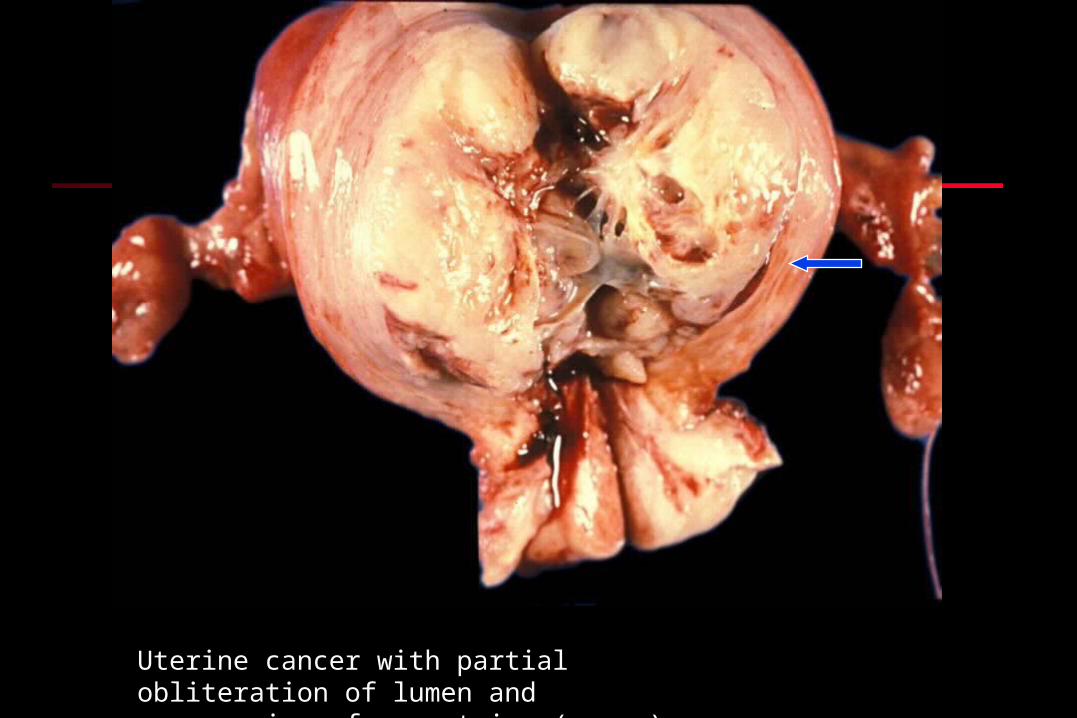
Uterine cancer with partial obliteration of lumen and compression of myometrium (arrow)
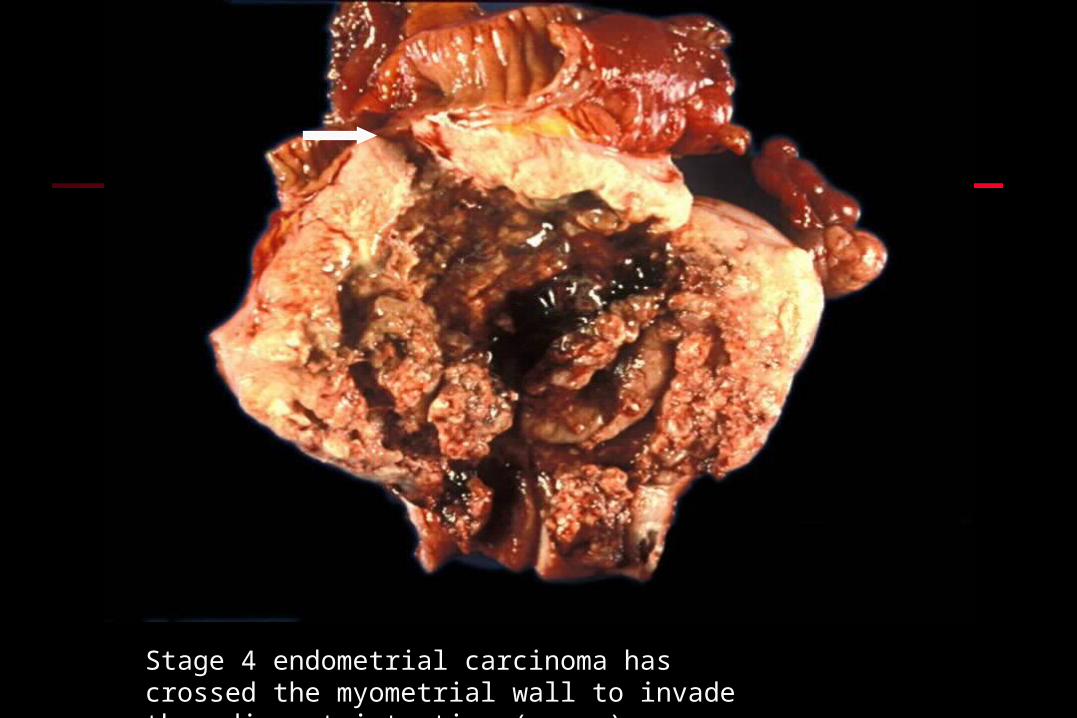
Stage 4 endometrial carcinoma has crossed the myometrial wall to invade the adjacent intestine (arrow)
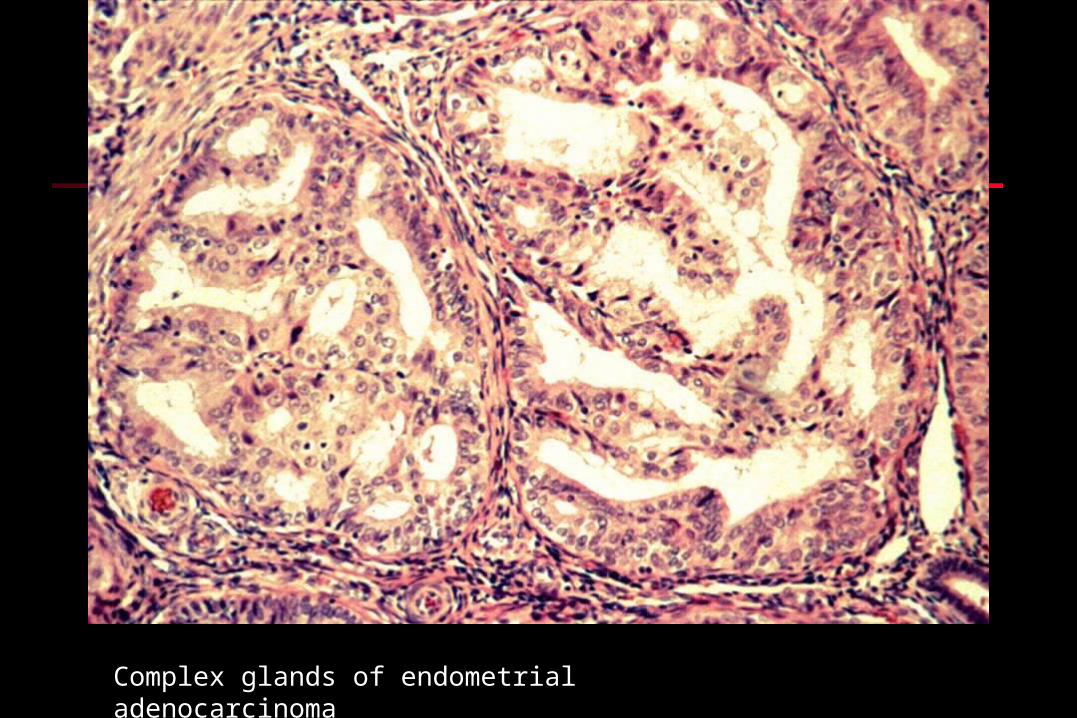
Complex glands of endometrial adenocarcinoma

Back to back glands of endometrial adenocarcinoma

Solid area within endometrial adenocarcinoma

Adenoacanthoma: squamous metaplasia is present (arrow)
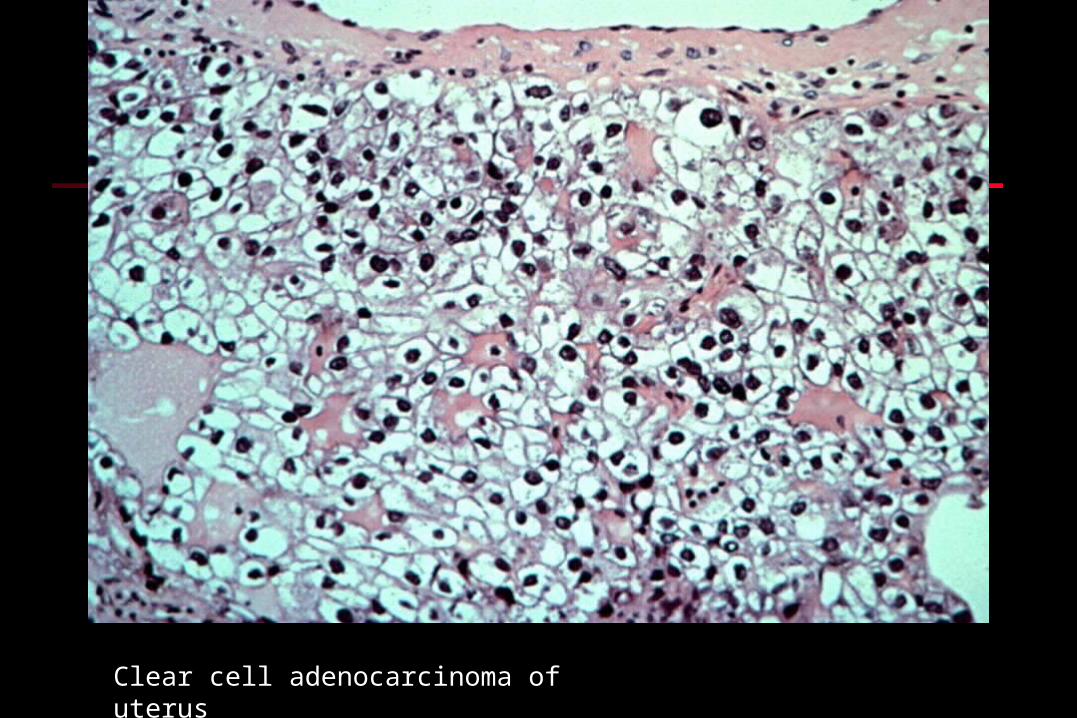
Clear cell adenocarcinoma of uterus

Serous papillary carcinoma of uterus: tumor usually has high-grade histology and is very aggressive

UTERUS: Carcinosarcoma (Malignant Mixed UTERUS: Carcinosarcoma (Malignant Mixed Mullerian Tumor)Mullerian Tumor)
Histo: endometrial adenocarcinoma with malignant Histo: endometrial adenocarcinoma with malignant
stromal differentiation (sarcomatous differentiation)stromal differentiation (sarcomatous differentiation)
Muscle, cartilage, osteoidMuscle, cartilage, osteoid
Some things never seen in uterus (cartilage, bone), Some things never seen in uterus (cartilage, bone),
others are (smooth muscle)others are (smooth muscle)
Otherwise similar to poorly differentiated Otherwise similar to poorly differentiated
endometrial adenocarcinomaendometrial adenocarcinoma
Prognosis: overall = 25% 5 yr survivalPrognosis: overall = 25% 5 yr survival

Malignant cartilage within endometrial adenocarcinoma
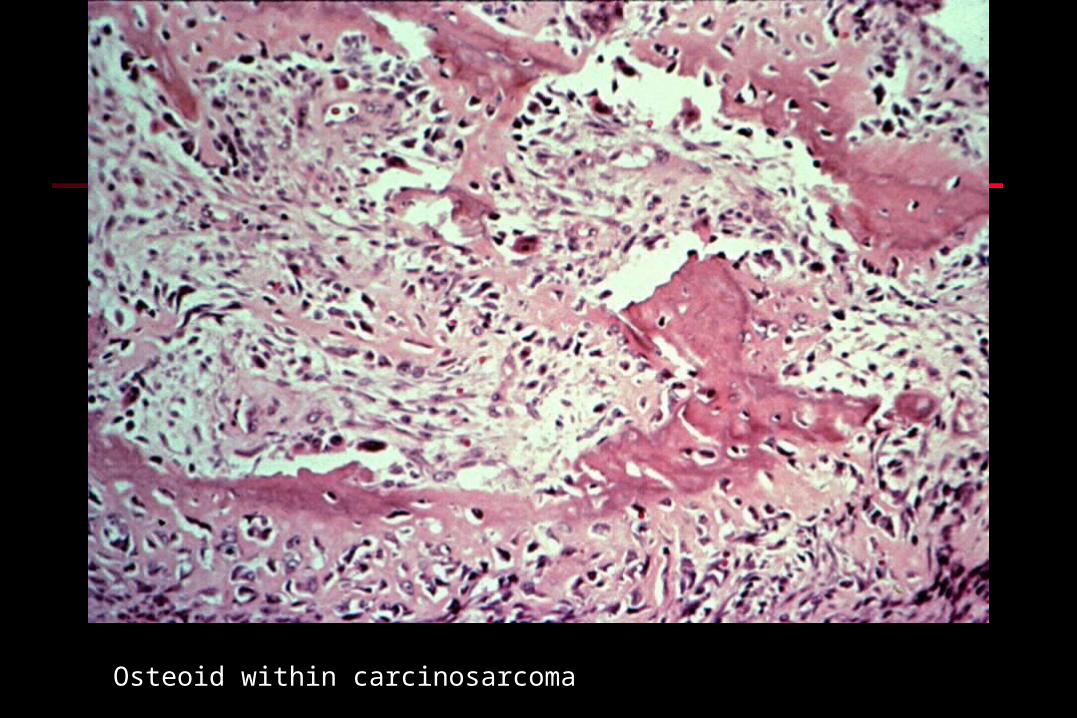
Osteoid within carcinosarcoma

Endometrial Stromal TumorsEndometrial Stromal Tumors
Two classes:Two classes: Benign stromal nodules Benign stromal nodules well- well-
circumscribed aggregate of stromal cells circumscribed aggregate of stromal cells within myometriumwithin myometrium
Stromal sarcoma Stromal sarcoma neoplastic endometrial neoplastic endometrial stroma invading myometrium: stroma invading myometrium:
Diffuse between muscle bundles, orDiffuse between muscle bundles, or Intralymphatic Intralymphatic
High recurrence rate (80% for stage III/IV)High recurrence rate (80% for stage III/IV) 5 yr survival~ 50%5 yr survival~ 50%

Multiple nests of stromal cells have invaded myometrium

Stromal sarcoma has invaded lymphatic channel within the myometrium