Stockholms läns läkemedelskommitté - Janusinfo · The clinical pharmacologist provided support...
148
Stockholms läns läkemedelskommitté
Transcript of Stockholms läns läkemedelskommitté - Janusinfo · The clinical pharmacologist provided support...

Stockholms läns läkemedelskommitté









Day 2, Wednesday September 12 Study visits
Hold on to this

International organizing group
Lars L Gustafsson, Stockholm
Dr Richard Laing, WHO Geneva,
Eva Andersén Karlsson, Stockholm
Dr Brian Godman, Stockholm/Liverpool
Dr Öyvind Melien, Oslo
Dr Sabine Vogler, Vienna

Organizing group, Stockholm Eva Andersén Karlsson, Chairperson DTC, Stockholm, associate
professor
Johan Bratt, associate professor
Carl-Gustaf Elinder, professor
Lars L Gustafsson, professor
Rickard Malmström, associate professor
Malena Jirlow, communication officer
Kristina Johansson, pharmacist
Paula Nordahl, executive secretary
Anna-Lena Forssén, executive secretary
Magnus Edlund, graphic designer

Welcome to Stockholm!

The Stockholm Model Including the ”Wise List”
Associate professor Eva Andersén Karlsson
Chairperson, Drug and Therapeutics Committee
(DTC), Stockholm County Council

Objectives
Efficient and safe treatment for patients
Making sure every patient receives the drug/s
that she/he needs – neither too much, nor too
little

Prescribers
Internal
Patients
External
County Council Board SLL administration/Support for Evidence-Based Medicine Stockholm DTC Information physicians/pharmacists Politicians Health care information officers Pharmacy stakeholders
Primary care Hospitals Private practitioners Students/KI Heads of Departments
Nat´l Board of Health and Welfare Ministry of Health Medical Products Agency Dental and Pharmaceutical Benefits Agency Sw Council on Health Technology Assessment Sw Assn of Local Authorities and Regions Sw Assn of the Pharmaceutical Industry Pharmaceutical companies Pharmacy stakeholders Patient organisations Sw. Med.Assn./sections Other county councils
Population Patient organisations
Stakeholders in the pharmaceutical field
Mass media
It all happens here!

Drug and Therapeutics Committee in Stockholm County Council
Rumiana Zlatewa Specialistläkare CityHeart Hjärtspecialistmottagning

Produktion
21 Expert Panels
Spesam
KUST Val- beredn
Evidence-based Medicine
QRC
Karolinska Institutet
HSF
Med fort- bildning
Metodrådet
Försäkringsmed kommitté
Pat.säkerhets- kommittén
Central strål- skyddskommitté
Central gaskommitté Vårdhygien
Stockholms län
Smittskydd Stockholm
Strama Stockholm
Sakkunnig- kansli
Med program- arbete
Dept. Support
Omv- råd
28 Specialist Boards
Produktion
SLK- kansli
Stockholm Drug and Therapeutics
Committe DTC
Stockholm Medical Board
SMR

Drug and Therapeutics Committee
Qualified analysis of
medicines –
recommendations
Wise List
New Medicines
Prescribing data
feedback to
prescribers and head
physicians
Identify poor
prescribing
– Medical Education
– Follow-up

The Key Role of Experts and Opinion Leaders Expert Panels:
21 Expert Panels covering all major diseases
Leaders in academic medicine and clinical drug research
(Karolinska Institutet)
Representatives from major specialist clinics, Primary Health
Care Centres, together with clinical pharmacologists and
pharmacists
In some cases, nurses are also members of the Expert Panel
The clinical pharmacologist provided support in drug evaluation
principles
2010-04-13
8
Stockholm DTC – 21 Expert Advisory Panels General medicine
Analgetics/rheumatological diseases
Anaesthetics, fluid therapy/nutrition
Endocrinological /metabolic diseases
Gastroenterological diseases
Geriatric diseases
Cardio-vascular diseases
Skin diseases
Infectious diseases
Pulmonary and allergic diseases
Medical kidney diseases
Neurological diseases
Obstetrics and gynaechology
Oncological and hematological
diseases
Plasma products and certain
antithrombotic drugs
Psychiatric diseases
Radiological drugs
Orphan drugs
Urology
Vaccinations
Eye diseases

Expert Advisory Panels Play Very Important Role
Some 180 medical experts have reviewed over
800 drugs – evaluating the scientific literature,
the clinical experience and pharmaceutical
appropriateness of various preparations, as
basis for decisions
Continuous real-world intelligence gathered
within specialised areas, following EMA,
pharma industry

2012-09-13
Medicinskt Kunskapscentrum
10
South/South-West 32 units
Anna Zucco Christer Norman
South-East 41 units
Sten Ronge Per Hedman
City 26 units
Kristina Aggefors
North-West 38 units
Laila Bucht Sjöström Sara Hallander
North-East 32 units
Teresa Alton Borgelin Eva Wikström
Johnsson
Division areas of responsibility Information pharmacists and physicians
West 26 units
Marie Bergfeldt
Södertälje 12 units
Johan Eklund
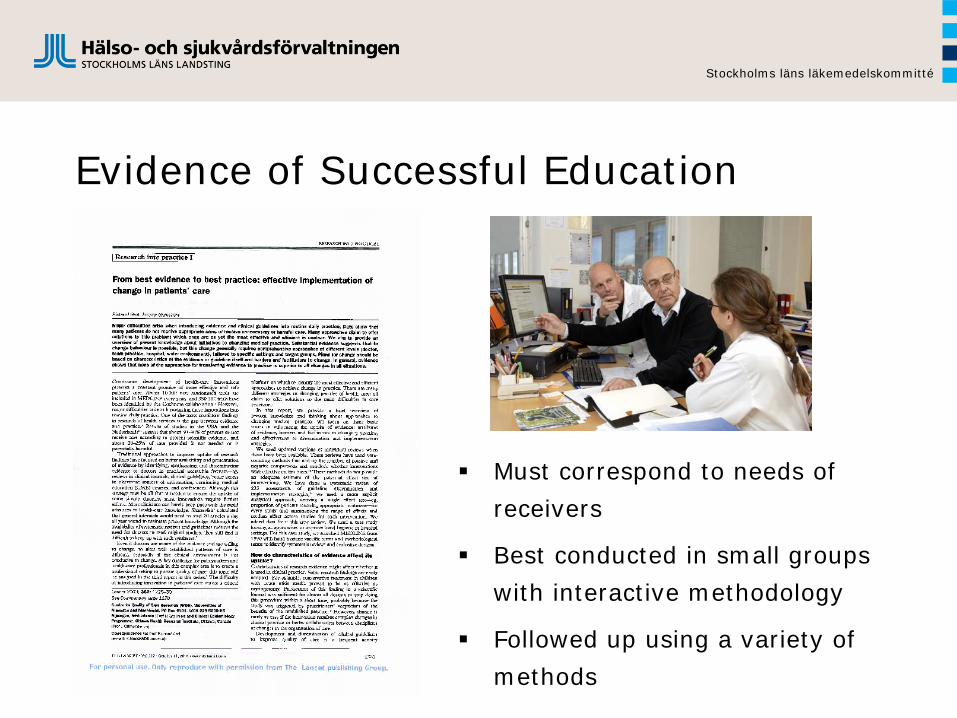
Evidence of Successful Education
Must correspond to needs of
receivers
Best conducted in small groups
with interactive methodology
Followed up using a variety of
methods
Stockholms läns läkemedelskommitté

Continued Medical Education
Drug information as part of the treatment
panorama for a certain disease
Information cannot stand by itself
Knowledge about diseases is a prerequisite for
high-quality treatment
Knowledge about diseases is a prerequisite for
selecting the right drug

Continued Medical Education and Communication Between Peers
Update medicine and
drugs at
Södersjukhuset
Hospital
Stockholms läns läkemedelskommitté

Kloka Listan Forum 2012

Academic detailing in a PHC

Continuing Medical Education 2012 – some examples

Implementing the Wise List – Summary
Kloka Listan Forum
Evening seminars
Update about medicines at hospitals
Academic detailing at Primary Health
Care Centres and workplaces
– Information physicians and pharmacists
– Interactive continuous medical education and follow-up of drug use

The Drug Bulletin ”Evidens”

www.janusinfo.se – independent, up-to-date guidelines, drug news and more

New drugs – flow chart within the County Council through February 2013
Horizon scanning – unbiased, expert evaluation – supported by groups of experts and passed in DTC (a recurrent item at DTC meetings)
Communication plan
Continuing Medical Education according to scientific, well-tried methods
Target group-approproate communication (e.g. cardiologists, pediatricians, oncologists, family doctors)
Tools, e.g. Take Care
Follow-up, evaluation

Ongoing challenges High cost of incorrect/irrational drug utilization
Regional and socio-economic differences
Changed premises for selling drugs
Lack of knowledge regarding environmental impact of drugs
Drugs poorly integrated with/evaluated against other forms
of therapy
Increasing number of drugs approved for sale are biological
drugs – effects of generic reform will decrease
There is a potential to develop the price-setting model
further
Too-slow uptake of new drugs?

Success Factors Drug Therapeutic Committee, DTC Expert advisory groups Wise List Knowledge-based support enabling wise,
evidence-based presribing Drug statistics stimulating physicians to
follow-up their own prescribing Credible, independent continuing medical
education, CME Operative support via Division Support for
Evidence-Based Medicine

Stockholm Drug Therapeutics Committee
The way in which the DTC by way of
expert-driven, efficient tendering and
attractive knowledge-based management
enables evidence-based and cost-
effective drug utilization in Stockholm
County Council
Stockholms läns läkemedelskommitté

2007-12-17
Läkemedelscentrum
24
Thank You!

New Instruction for DTC in Stockholm County Council – HSN decision 20.12.2011
Stockholms läns läkemedelskommitté

Kloka Listan - the Wise Drug list
Issued by the regional
Drug and Therapeutics Committee
Focus on the rational choice of drugs
for common diseases in outpatient care
Drugs selected by 21 expert panels
with GPs, specialists, pharmacists
& clinical pharmacologists
Information campaigns towards
prescribers (and patients/the public)
Website www.janusinfo.se

Wise Drug Use and Prescribing
Pedagogical recommendations – Wise List/Wise Advice/Wise guidelines
Communication strategy – well-considered – adapted to target groups
Computerised decision support –Take care…
Networking – the whole of Stockholm Interactive pedagocial model Follow-up
Stockholms läns läkemedelskommitté
Wise Drug Utilization
Requires long-term strategies with a patient focus, committed collaborators, experts and management in every county council/region and national concordance
Requires evidence-based recommendations for old and new drugs valid regardless of type of management according to national/international recommendations from independent DTCs with a central, independent role in knowledge-based management in every region/county council

Wise Drug Utilization
Becomes problematic without national and successively international collaboration and standardization between health care regions, particularly expert evaluations, management of e-health services, introduction of new, expensive drugs and financing
Requires systematic introduction and follow-up of new drugs and consistency/integrity in contacts with pharma industry and other stakeholders
Requires economic management and incentives based on medical usefulness/safety, professional involvement and responsibilty, expert recommendations and follow-up

Introduction of new drugs
Discussion: Need of horizontal prioritization A holistic apprach
DTC is planning a seminar on drugs and priorities with some concrete examples September 2012 Target groups: politicians, civil servations,
experts, DTC reference group, physicians with interest in pharmaceuticals
Stockholms läns läkemedelskommitté

Introduction of new expensive therapies! Strict guidelines and follow-up protocols for
expensive drugs (per patient) or in total – new principles and biological drugs
For patient groups that have been studied Need for CME and quality follow-up Need for complementary natural studies
including randomized dito Health economic evaluations
Stockholms läns läkemedelskommitté

Stockholms läns läkemedelskommitté
Independent drug expert organization with network • Regional DTC with expert panels with shared values and policy for declaring and managing potential conflicts of interest – in particular with the pharmaceutical industry. The policy is known, communicated and followed. This policy is fundamental for the DTC system and for trust in its experts [28]. • General practitioners, hospital-based specialists, clinical pharmacologists and pharmacists from major health care providers in the region are members of the regional DTC. They participate in selection of drugs in the ‘Wise List’. • Training of members of the DTC in the principles of critical drug evaluation by clinical pharmacologists. This helps to maintain high quality of drug selection principles across expert groups.

Law Governing DTCs
33
Stockholms läns läkemedelskommitté

The Wise Drug List
KLOKA LISTAN
LÄKSAKStockholmsläns landsting
2010
KLOKA LISTAN
Stockholms läns läkemedelskommittéStockholms läns landsting
2012

Rational use of medicines: The challenge of interface collaboration between ambulatory and hospital
care an International perspective
Richard Laing, WHO Geneva
Stockholm Interface Course 2012 1
Where in the world is the interface between hospitals and primary care good?
• Not many places! Often in some areas in a country but often not systematic and often dependent on committed leaders
• Some country examples – Zimbabwe – Scotland – Netherlands – Stockholm
Stockholm Interface Course 2012 2

Country Examples Zimbabwe
• Since 1986 Zimbabwe has had an integrated Essential Drug List (EDLIZ) and Treatment Guidelines for hospitals and primary care with tiered levels of medicines.
LEVEL OF AVAILABILITY C drugs are those required at primary health care level and should be available at all levels of care. B drugs are found at district hospital level or secondary and higher levels of care. Some B drugs may be held at primary health care facilities on a named patient basis – for example in the management and follow up of chronic illnesses. A drugs are prescribed at provincial or central hospital levels. S drugs (specialist only) have been brought back into this edition. These are drugs that require special expertise and /or diagnostic tests before being prescribed.
Stockholm Interface Course 2012 3

MAJOR HIGHLIGHTS IN THE LATEST EDLIZ
Need for Hospital formularies and Hospital Therapeutics Ideally each hospital should create its own local drug formulary which shows which drugs are considered very useful in that setting so that you do not have to order drugs that your nurse or doctors will not prescribe or use. For instance you should not keep specialist drugs if there is no specialist to prescribe them. Hospital Drug and Therapeutics Committees should select drugs for use in their hospital using the EDLIZ.
Stockholm Interface Course 2012 4
Country Examples Scotland
Next presentation by Prof K Paterson Key elements • Formularies which apply equally in primary and
secondary care • Guidelines jointly written • Managed Clinical Networks which are cross-
specialty (physicians, surgeons, pharmacists …) • Health Technology Assessment through SMC with
primary & secondary care at the table
Stockholm Interface Course 2012 5
From http://whocc.goeg.at/Downloads/Conference2011/PraesentationenPPRIKonferenz/Day1_afternoon_Sitzungssaal_1300_Paterson.pdf

Country Examples Scotland Key elements
• 20 years working together • Clinical benefits first then financial • Culture of openness and transparency • Primary and Secondary NOT Primary vs secondary • Joined up thinking • Accepted part of medicine use by clinicians,
patients and pharma
Stockholm Interface Course 2012 6
From http://whocc.goeg.at/Downloads/Conference2011/PraesentationenPPRIKonferenz/Day1_afternoon_Sitzungssaal_1300_Paterson.pdf

Country Examples Netherlands
• Two recent PhD Theses – Ruther Stuffken Medication
changes in patients transitioning between health care settings (http://igitur- archive.library.uu.nl/dissertations/2011-1027-200508/UUindex.html
– Fatma Karapinar Transitional Pharmaceutical Care for Patients Discharged from the Hospital (http://igitur-archive.library.uu.nl/dissertations/2012-0412-200334/UUindex.html
Stockholm Interface Course 2012 7

Country Examples Stockholm
Wise List Approach
• Annual Issue of List • Focus on primary care with recent addition of
hospital wise list • 20 Expert groups involving specialists, clinical
pharmacologists, GPs and pharmacists • Information Campaigns • Monitoring using DU 90%
Stockholm Interface Course 2012 8 http://whocc.goeg.at/Downloads/Conference2011/PraesentationenPPRIKonferenz/Day1_afternoon_Sitzungssaal_1300_Malmström.pdf
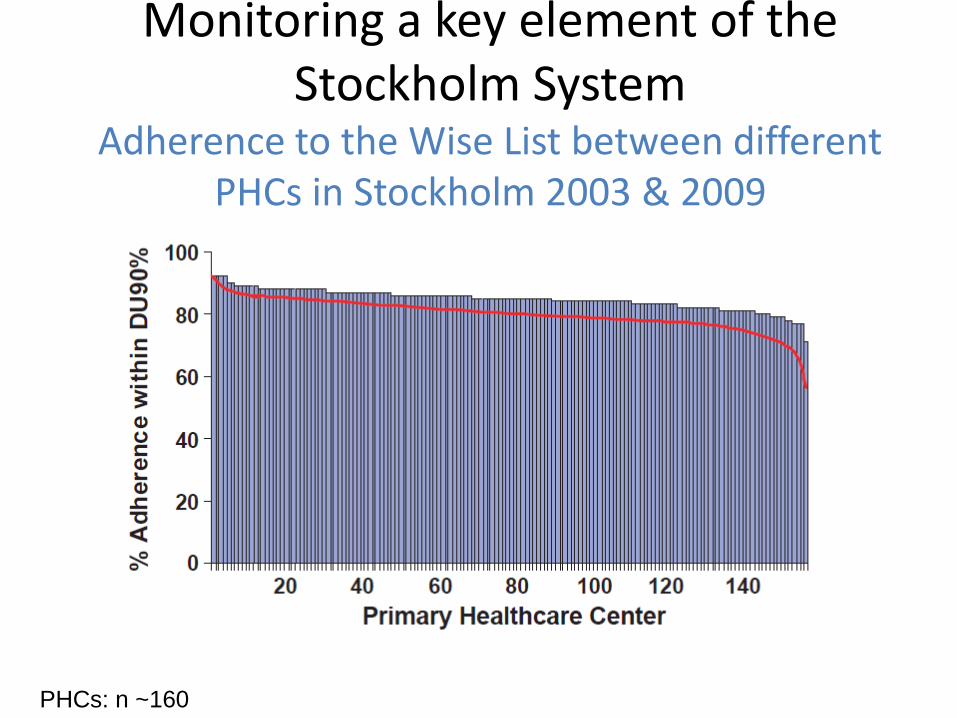
Monitoring a key element of the Stockholm System
Adherence to the Wise List between different PHCs in Stockholm 2003 & 2009
PHCs: n ~160

Database on medicines use
• Database of all medicines use surveys using standard indicators in primary care in developing and transitional countries
• Studies identified from INRUD bibliography, PUBMED, WHO archives
• Data on study setting, interventions, methods and drug use extracted & entered
• All data extraction and entry checked by 2 persons
• Now > 900 studies entered • Systematic quantitative review • Evidence from analysis used for
WHA60.16 in 2007

% compliance with guidelines by WB region
0102030405060
1982-1994 1995-2000 2001-2006
Sub-Saharan Africa (n=29-48) Lat. America & Carrib (n=5-13)Middle East & C. Asia (n=4-8) East Asia & Pacific (n=7-11)South Asia (n=6-12)

12
What are countries doing to promote rational use of medicines ?
0 20 40 60 80 100
EML updated in last 5 years
STGs updated in last 5 years
EML for insurance reimbursement
Information centre for prescribers
DTCs in most referral hospitals
Independent CME for prescribers
Public education in last 2 years
National strategy to contain AMR
Drug use audit in last 2 years
% countries implementing policies to promote rational use
Source: TCM pharmaceutical database 2003

Conclusion
• Much more to be done • Much to learn • Will need research • Can learn from others' experiences both
positive and negative
Stockholm Interface Course 2012 13

Scottish Countrywide Collaboration to Integrate
Medicine Therapy between Primary and Hospital Care
Ken Paterson Stockholm
11 September 2012

NHS Scotland Virtually monopoly payer and provider Universal coverage from general taxation Free at point of care No co-payment - all medicines provided free Secondary care provided by state-run hospitals Primary care provided by independent doctors
…but contracted to work within system ‘rules’ Long history of ‘controlled prescribing’
Initially on good clinical grounds Now also includes cost considerations

Managing the Interface - 1
Early (1990) recognition of the problems Primary care prescribing influenced by
secondary care recommendation Differential pricing of medicines in primary
and secondary care (‘loss leaders’ in hospitals)
Clinical risks in use of too many medicines …and in switching between medicines
Huge range of medicines stocked by pharmacies in community and hospitals

Managing the Interface - 2
Early introduction of joint working Drug & Therapeutics (D & T) Committees
involving primary and secondary care Safe, quality prescribing the initial driver Cost containment soon also a factor
…equally in primary and secondary care! Single budget for healthcare (1ary and 2ary)
Joint working then established as the norm …and transferred to other areas of activity

Managing the Interface - 3
Formularies Communications Guidelines Managed clinical networks Horizon Scanning Health technology assessment
Impact on pricing/reimbursement

Drug & Therapeutics Committees
Multidisciplinary Joint primary and secondary care May include patient/public input Evidence-based approach
Full declarations of interest Limited role for ‘key opinion leaders’ Part of the clinical community

Formularies
All 14 Health Boards have a Formulary Some individual, others shared
All are developed jointly between primary and secondary care
All apply equally in primary and secondary care …no ‘carte blanche’ for specialists
All prescribing is monitored and Formulary adherence assessed
Some medicines limited to use on specialist advice (or even specialist prescription)

Non-Formulary Prescribing
Obviously permitted if it can be justified Individual patient treatment request possible
Would be questioned if high in primary care Prescriber would be individually targetted
Might be questioned in ‘real time’ in hospital Therapeutic substitution in some settings Case-by-case justification before medicine used Routine pharmacist monitoring of non-Formulary
medicines, especially high-cost

Communication
Formulary in paper/electronic version DTC minutes on website Regular Formulary updates
Good prescribing advice ‘Drug of choice’ initiatives
Communications are local Maintain involvement and ownership Content must follow national policy

Guidelines
Almost all guidelines are jointly written Full declarations of interest Evidence-based rather than opinion-based Interface issues usually specifically addressed
eg guidance on referral to secondary care
Guideline advice informs Formulary content …and vice versa - if the guideline
recommends a class of medicine, the Formulary will name an individual medicine

Managed Clinical Networks
Disease-specific networks Cross-specialty (physician/surgeon/pharmacist..) Across the interface - primary + secondary care
Aim to cover all aspects of management Diagnosis, investigation, monitoring …also medicines use Facilitates managed introduction of new drugs
Adherence to all aspects of MCN monitored

Horizon Scanning
Identify pipeline medicines 12-24 months before launch
Focus on key medicines High cost (to allow financial planning) Service implications (to allow redesign) Interface issues (to allow guidance/protocols)
“no surprises” the aim!

Health Technology Assessment
New medicines assessment a challenge Vital to keep Formulary up-to-date Often significant cost implications
New medicines a cost pressure in all systems
Pre-2001 - local assessments 15 assessments in Scotland - wasteful Sometimes different decisions - divisive Variable quality of decisions - open to challenge
Since 2001 - Scottish Medicines Consortium

Scottish Medicines Consortium
Consortium of existing (joint) DTCs 30-member committee
Doctors, pharmacists, patients, industry Primary and secondary care at the table
Advises on ALL new medicines Primary, secondary and tertiary care
Rapid process - 18 weeks “shape practice, not change practice”
Assesses value - not reference pricing!

SMC - 2002-2011
729 submissions considered 2002 – 29 2003 – 62 2004 – 74 2005 – 87 2006 – 130 (111) 2007 – 110 (95) 2008 – 105 (87) 2009 – 81 (73) 2010 – 102 2011 – 91

Outcome of Assessments
Accepted for Use – 35% Accepted for Restricted Use – 36% Not Recommended – 29% Perhaps more ‘No’ in recent years
0
10
20
30
40
50
60
2002 2004 2006 2008 2010
AcceptRestrictNo
%

SMC Influences
Advice informs local Formulary decisions SMC says ‘no’, cannot be in local Formulary SMC says ‘yes’, can be in local Formulary
Advice informs Guideline content Guideline cannot recommend non-approved
medicine Advice informs MCN protocols
Protocol cannot recommend non-approved medicine

Case Study - Clopidogrel
Expensive compared to aspirin Time-limited therapy appropriate 3/6 month course provided by secondary care Medicine never on primary care prescription
Savings re-invested in implantable defibs Generic clopidogrel launched - different salt
SMC facilitated pan-Scotland decision Generic clopidogrel the formulation of choice

Locus of Control/Action
Define where control/action best sited National
Horizon scanning Health technology assessment Guidelines
Local Formularies/protocols Communications Prescribing monitoring

Impact on Pricing/Reimbursement
Medicines pricing reserved to UK Local policies affect local pricing/expenditure
85% of prescribing is ‘generic’ (by rINN) 70% of dispensed medicines are generics
No ‘loss leaders’ in secondary care No point in ‘influencing’ KOLs in secondary care Value assessment promotes ‘patient access schemes’
Often simple discounts (exact amount may be secret!)
Even a small (non-)country can negotiate better value-for-money

The Scottish Experience
Built over 20 years of joint working Clinical benefits prime, then financial Needs culture of openness and transparency
…no conflicts of interest - see the big picture! 1ary + 2ary, not 1ary v 2ary!
Needs careful ‘joined-up’ thinking Mixed messages unhelpful to everyone
Now an accepted part of medicines use …by clinicians and patients (and pharma!)

Scottish Medicines Consortium
www.scottishmedicines.org.uk

Catalonian country-wide collaboration to integrate
medicine therapy between primary and hospital care
Interface Management of Pharmacotherapy Promoting Hospital-Primary Care Collaboration for
Rational Use of Medicines
Eduard Diogène
Stockholm, September 11th, 2012

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Overview Financial incentives and indicators @prescribing Drug and Therapeutics Committees
2

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Catalonia: 7.500.000 inhabitants
Catalan Institute of Health ● 8 hospitals
• 3.247 physicians • DTC
● 288 Primary Health Care Centres • 6.399 physicians
3

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Drug Policies
PHC and hospitals
Efficiency Clnical management of new drugs Conservative prescribing: safety and quality Participation and responsibility of physicians
4

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Drug and Therapeutics Committee
35 members: ● Physicians (PHC and H) ● Pharmacists (PHC and H) ● Clinical Pharmacologists (PHC and H)
3 Stable Working Groups
● Formulary ● Information and communication ● Pharmacovigilance
5

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Drug and Therapeutics Committee
Formulary New drugs evaluation Information Continuous medical education Pharmacovigilance Drug and Quality Prescription Indicators monitoring
6

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Drug expenditure 2011
Primary Health Care: ● 1.211,78 M € (-7,6%)
Hospitals:
● 218,46 M € (-6,9%)
7

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
PHC drug expenditure 2011
8
ATC 2010 (M €)
2011 (M€)
Difference (M €)(%)
N06. PSYCHOANALEPTICS 124,2 116,1
-8,1 (-6,54 %)
R03 . DRUGS FOR OBSTRUCTIVE AIRWAY DISEASES 105,5 108,6
3,1 (3,01%)
C09. AGENTS ACTING ON THE RENIN-ANGIOTENSIN SYSTEM 108,1 95,9
-12,1 (-11,22%)
A10. DRUGS USED IN DIABETES 79,9 87.7
7,6 (9,54%)
N05. PSYCHOLEPTICS 69,3 65,7
-3,7 (-5,29%)
C10. LIPID MODIFYING AGENTS 87,6 63,6
-23,9 (-27,38%)
N03 ANTIEPILEPTICS 51,8 53,9
2,1 (4,10%)
A02. DRUGS FOR ACID RELATED DISORDERS 52,8 46,0
-6,8 (-12,94%)
N02. ANALGESICS 44,3 43,6
-0,7 (-1,62%)
G04. UROLOGICALS 42,3 41,8
-0,5 (-1,27%)

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
PHC drug expenditure: january-june 2012
9

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Indicator Score Indicator Score
1. Non recommended new drugs / total 15 7. Asthma drugs 8
2. Generics / Total 5 % BETA 2+ CORTICOIDS/ TOTAL
%RECOMMENDED/TOTAL ANTIASMÀTICS 3 - 1 5 3
3. Antihipertensive drugs (AHT) 10 8. Antidepressants 8
%DIURETICS/ TOTAL AHT %ARB/ (ACE + ARB)
%RECOMMENDED / TOTAL AHT
2 - 1 4 ´ 3 - 2
4 - 3
%RECOMMENDED/ TOTAL
ANTIDEPRESSANTS 8 - 4
4. Antiulcer drugs (AU) 8 9. Anxiolytics and hypnotics (ANX) 8
%RECOMMENDED/ TOTAL AU
8 - 4
%RECOMMENDED/TOTAL ANX
8 - 4
5. NSAID 8 10. Non insulin antidiabetic drugs (NIAD) 8
%RECOMMENDED/TOTAL NSAID
8 - 4
% RECOMMENDED/TOTAL NIAD 8 - 5 - 3
6. Antibiotics 8 11. Lipid lowering drugs (LL) 12
DDD ANTIBIOTICS* %PENICILINS/ANTIBIOTICS
%AMOXI/ AMOXI+AMOXI-CLAVULANATE %RECOMMENDED/ANTIBIOTICS
4 - 2 1 1
2 - 1
% RECOMMENDED/TOTAL LL 12 - 8 - 4
PHC: Incentives and prescribing indicators

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Hospitals: incentives and prescribing indicators
11
Indicators (DTC) Score
Outpatient/discharged/emergency adherence to CIH Formulary: Non-recommended new medicines ARB / (ARB + ACEI) Recommended Antiulcer drugs Recommended NSAID Recommended Lipid Lowering drugs Recommended Non- insulin Antidiabetic drugs
2 -1 1 - 0,5
0,5 0,5
1 - 0,5 1 - 0,5
Safe use of drugs 1,5
@prescribing for outpatient/discharged/emergency 1,5
TOTAL 9

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 12

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 13

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 14

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 15

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 16

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 17

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
DTC recommendation
19
Unadequate INR control: 60%
Alergy or intollerance

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Atrial fibrillation patients and dabigatran follow-up
May 2012 70.135 patients on acenocumarol
1.066 patients on dabigatran Sex: 525 women (49,25%) + 546 men (51,22%) Age: 75 ± 9,9 (range: 25-100). 628 patients (58,91%) ≥ 75
20
Dabigatran (Catalonia)
Dabigatran 110mg (RE-LY)
Dabigatran 150mg (RE-LY)
Age (years)
75 ± 9,9 71,4 ± 8,6 71,5 ± 8,8
Men 546 (51,22%) 3865/6015 (64,3%) 3840/6076 (63,2%)
Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
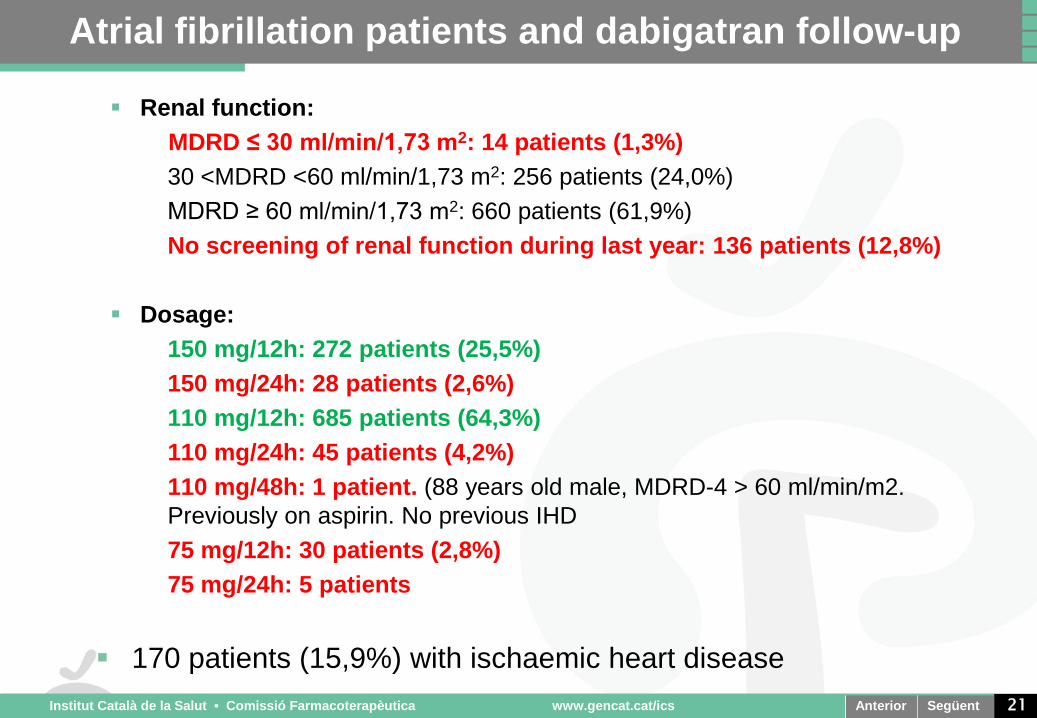
Atrial fibrillation patients and dabigatran follow-up
Renal function: MDRD ≤ 30 ml/min/1,73 m2: 14 patients (1,3%)
• 30 <MDRD <60 ml/min/1,73 m2: 256 patients (24,0%) • MDRD ≥ 60 ml/min/1,73 m2: 660 patients (61,9%) • No screening of renal function during last year: 136 patients (12,8%)
Dosage:
• 150 mg/12h: 272 patients (25,5%) • 150 mg/24h: 28 patients (2,6%) • 110 mg/12h: 685 patients (64,3%) • 110 mg/24h: 45 patients (4,2%) • 110 mg/48h: 1 patient. (88 years old male, MDRD-4 > 60 ml/min/m2.
Previously on aspirin. No previous IHD • 75 mg/12h: 30 patients (2,8%) • 75 mg/24h: 5 patients
170 patients (15,9%) with ischaemic heart disease
21

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Previous Treatment
OAC: 380 patients (35,6%) OAC + aspirin: 54 patients (5,1%)
Clopidogrel: 54 patients (5,1%) Clopidogrel + aspirin: 18 patients (1,7%) Aspirin: 235 patients (22,0%)
Naïve: 325 pacients (30,5%)
22

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 23
Dabigatran prescriptions
0 20 40 60 80
100 120 140 160 180 200
0
200
400
600
800
1000
1200
Nº p
atie
nts
Nº p
atie
nts
2011 2011 2012 2012
New dabigatran prescriptions Acumulated dabigatran prescriptions

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 24

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 25
Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Participation and responsibility of physicians
Drug and Therapeutics Committees H ● Follow-up of patients and recommendations ● Analysis of drug expenditure ● Outpatients, discharged patients and emergency ward ● Safe use of drugs ● @prescribing ● Ad-hoc small groups
● Debate
● At least 1 PHC professional (Pharmacist, clinical
pharmacologist or family doctor) 26

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Population 189.091
PHC physicians 151
PHC centres 22
Hospital 1
PHC Drug and Therapeutics Committee
Terres de l’Ebre

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
PHC DTC Terres de l’Ebre
Coordinator: PHC physician
11 PHC physicians 1 clinical pharmacologist 1 pharmacist General manager

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Education ● Electronic Drug Bulletins ● Clinical Guidelines ● Follow-up feed-back
Engineering ● Indicators of adherence to formulary
Economics ● Financial incentives
Enforcement ● DTC recommendations
29

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 30
Thank you for your attention

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
PHC drug expenditure 2011
31
Drug 2010 (M €)
2011 (M €)
Difference (%)
Salmeterol 37,7 37,1 -1,5%
Atorvastatin 45,9 24,2 -47,2%
Pregabalin 19,4 22,6 14,4%
Formoterol 19,9 21,3 6,7%
Tiotropium 17,8 19,4 8,9%
Glargine Insulin 15,3 17,7 15,8%
Omeprazol 18,6 16,7 -9,7%
Clopidogrel 27,6 14,2 -48,5%
Olanzapine 17,5 14,1 -19,1%
Risperidone 13,7 12,7 -6,8%

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 32
Results UH Germans Trias i Pujol (January - April 2012)
Indicator Result Goal Score
Non-recommended new medicines
2,73% ≤2,08% (2) ≤2,14% (1)
0
ARB / (ARB + ACEI) 52% ≤48% (1) ≤49% (0,5)
0
Recommended Antiulcer drugs 80% ≥80% (0,5) 0,5
Recommended NSAID 60% ≥56% (0,5) 0,5
Recommended Non- insulin Antidiabetic drugs 41% ≥44% (1) ≥43% (0,5)
0
Recommended Lipid Lowering drugs 34% ≥40% (1) ≥39% (0,5)
0
Safe use of drugs
3,01 / 1.000 > 2,55 ADR /1.000 inpatients (1,5)
1,5
@prescribing for outpatient/discharged/emergency*
No data ≥30% (1,5) ----
* 4th trimestre 2012

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 33
Eficiència i sostenibilitat Gestió clínica de la introducció dels nous
medicaments Prescripció prudent: segura i de qualitat Participació i corresponsabilització dels clínics

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Dades de la fitxa tècnica
34
Posologia recomanada: 150 mg/12h
Ajust de dosi en situacions especials:
· Pacients entre 75-80 anys: A criteri del metge, es pot considerar una dosi de 110 mg/12h quan el risc
tromboembòlic és baix i el risc d'hemorràgia és alt.
· Pacients ≥ 80 anys: 110 mg/12h
· Pacients amb un major risc d'hemorràgia: 110 mg/12h
· Insuficiència renal greu: contraindicat
· Insuficiència renal moderada i alt risc de sagnat: 110 mg/12h
· Administració concomitant amb verapamil: 110 mg/12h
· Pacients amb elevació enzims hepàtics> 2 vegades el límit superior de la normalitat: no es recomana
Pacients amb ≥ 80 anys: 406 pacients (38,2%)
Dosi de dabigatran en pacients ≥
80 anys en l’ICS:
• 110 mg/12h: 335 pacients (82,5%) • 150 mg/12h: 25 pacients (6,2%) • 75 mg/12h: 20 pacients (4,9%) • 110 mg/24h: 20 pacients (4,9%) • 150 mg/24h: 3 pacients (0,7%) • 75 mg/24h: 3 pacients (0,7%)

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Seguiment prescripció dabigatran
Gràfica 1. Distribució per àmbits dels pacients a tractament amb dabigatran
0
50
100
150
200
250
300
350
Nº p
atie
nts
Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
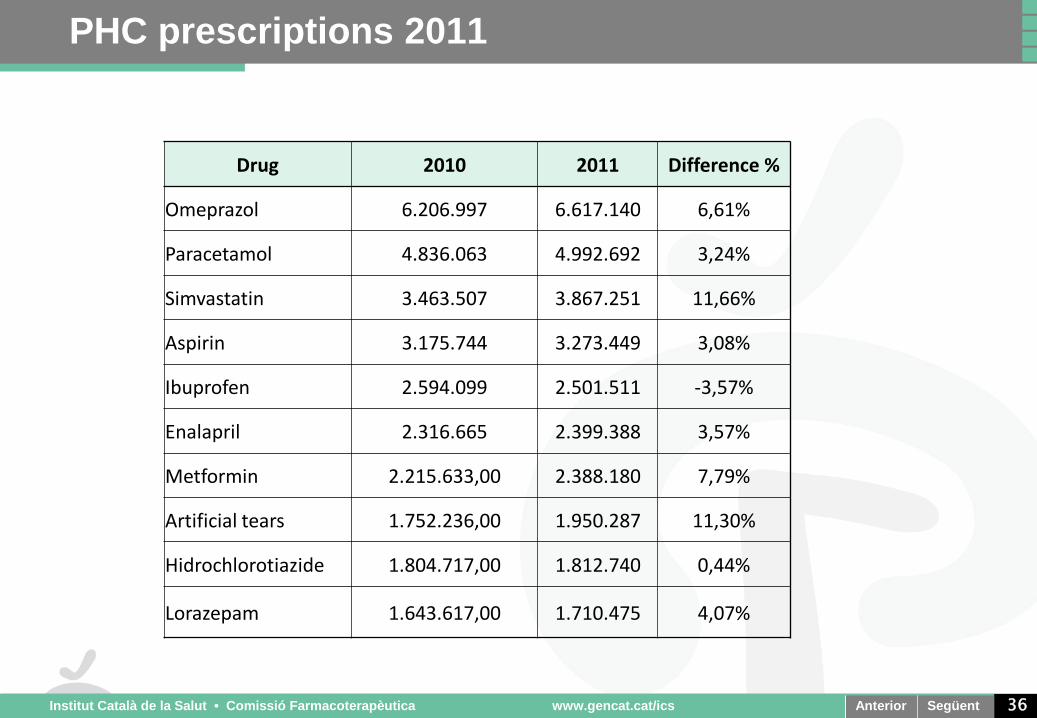
PHC prescriptions 2011
36
Drug 2010 2011 Difference %
Omeprazol 6.206.997 6.617.140 6,61%
Paracetamol 4.836.063 4.992.692 3,24%
Simvastatin 3.463.507 3.867.251 11,66%
Aspirin 3.175.744 3.273.449 3,08%
Ibuprofen 2.594.099 2.501.511 -3,57%
Enalapril 2.316.665 2.399.388 3,57%
Metformin 2.215.633,00 2.388.180 7,79%
Artificial tears 1.752.236,00 1.950.287 11,30%
Hidrochlorotiazide 1.804.717,00 1.812.740 0,44%
Lorazepam 1.643.617,00 1.710.475 4,07%

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Participació i corresponsabilització dels clínics
Comissions Farmacoterapèutiques H ● Seguiment d’acords i pacients: adeqüació, pacients ● MHDA ● Consultes externes, altes i urgències ● Seguretat en l’ús dels medicaments ● Prescripció electrònica ● Debat
37

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
Acord de Gestió EAP
38
Sostenibilitat Tancament pressupostari 15%
Compliment DMA 10%
Activitat i qualitat assistencial
Estàndard Qualitat Assistencial de l’EAP (EQA) 25%
Estàndard Qualitat Prescripció Farmacèutica de l’EAP (EQPF) 15%
Seguretat ús del medicament 10%
Gestió IT 5%
Millora organitzativa
Gestió compartida demanda
Implementació e-consentiment 5%
demanda aguda lleu 5%
Pla Qualitat i Seguretat del pacient 10%
Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
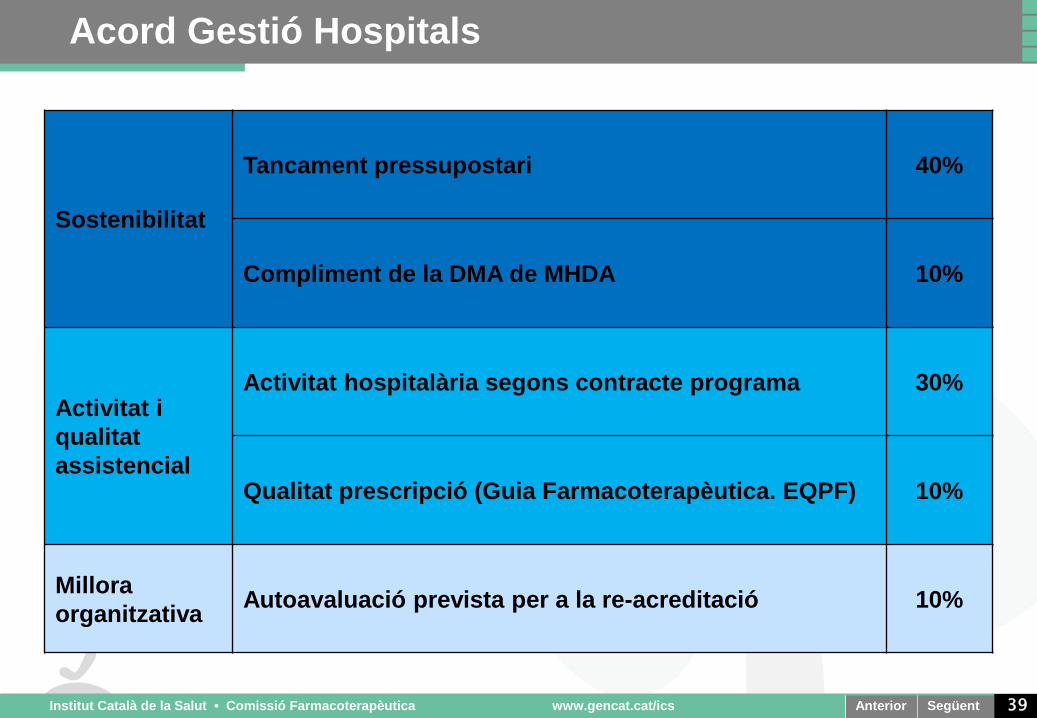
Acord Gestió Hospitals
39
Sostenibilitat
Tancament pressupostari
40%
Compliment de la DMA de MHDA 10%
Activitat i qualitat assistencial
Activitat hospitalària segons contracte programa 30%
Qualitat prescripció (Guia Farmacoterapèutica. EQPF) 10%
Millora organitzativa Autoavaluació prevista per a la re-acreditació 10%

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics
PHC DTC Terres de l’Ebre
May 2007 Monthly meetings Analysis and debate Information Continuous education CIH Drug Policy

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 41
2010 2011 Var 2011/2010
Pacients (N) 39.294 38.805 - 0,6 %
Facturació (Milions d’€) 234,6 218,5 - 6,9 %
Facturació / pacient (€/ pacient) 6.007 5.630 - 6,3 %

Anterior Següent Institut Català de la Salut • Comissió Farmacoterapèutica www.gencat.cat/ics 42
Agrupació Import 2011 % Import % Import Acumulat
Antiretrovirals actius contra VIH 54,1 Milions d’€ 24,8% 24,8%
Resta de medicaments d’ús hospitalari
34,1 Milions d’€ 15,6% 40,4%
Immunosupressors selectius 27,9 Milions d’€ 12,8% 53,2%
Citostàtics 25,3 Milions d’€ 11,6% 64,8%
Esclerosi múltiple 22,6 Milions d’€ 10,3% 75,1%
Total MHDA 218,5 Milions d’€ 100% 100%

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Interface management in Norway - status and initiatives at national and regional levels
Øyvind Melien MD PhD Norwegian Directorate of Health Dept. of Medical Devices and Medicinal Products

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Interface management in Norway
Issues • The present situation • Improvement of interface management • Implementation of new initiatives
| Interface Management of Pharmacotherapy Stockholm September 11 2012
The present situation
Health care organization and responsibilities Status at the interface
• The Patients • The Health Care System • Funding of medicines use

| Interface Management of Pharmacotherapy Stockholm September 11 2012
The present situation
Responsibility levels in Health Care
• National level - Health Ministry with agencies
• Regional level - Regional Health Enterprises – Specialist Health
Care
• Local level - Primary Health Care

| Interface Management of Pharmacotherapy Stockholm September 11 2012
National level
Ministry of Health with agencies Norwegian Directorate of Health National therapeutic guidelines
Norwegian Knowledge Centre for Health Services Evaluations, knowledge reports and HTA body
The Norwegian Medicines Agency Regulatory authority, drug information etc.
| Interface Management of Pharmacotherapy Stockholm September 11 2012
Regional level
Specialist Health Service System • Organized in four Health Regions as Public Health
Enterprises • Formularies for medicines use
Within each hospital, not at regional level

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Local level
Primary Health Care • National guidelines, ex. use of Antibiotics in Primary
Health Care • National recommendations for preferred prescription • Drug and Therapeutic Committees not organized
• Local formularies within certain institutions

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Status at the interface
The Patients - gaps in medicines treatment National Working Group established by Health Ministry
indicated a risk for gaps in patient treatment, in particular related to transfer of patients between levels in the health care system
Reference: Report from National Working Group on Rational Medicines Use, May 2009

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Status at the interface
The Health Care System National guidelines in certain fields covering all levels Implementation and follow-up systems – a major
challenge No common Common Drug and Therapeutic
Committees or common formularies developed, covering both Specialist and Primary Health Care

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Status at the interface
Different funding systems for medicines use - Specialist health care covers medicines expenses in
the hospital sector based on funding from the government
- Local governments are responsible for medicines
expenses in local institutions
- National insurance is responsible for reimbursement of medicines expenses outside institutions

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Improvement of interface management
Project for ”Summary Care Records” A project under the Directorate of Health is established
to develop Summary Care Records, intended to be accessible at all levels in the health care system, containing key information concerning the individual patients, including their medicines use.
The Summary Care Records may offer a major tool for
interface management in future patient treatment

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Improvement of interface management
Lists for medicines use for the patients As part of the National Patient Safety Campaign a
project has been initiated to promote the use of medicines lists for the individual patients in order to ensure correct information at any level in Specialist or Primary Health Care.
| Interface Management of Pharmacotherapy Stockholm September 11 2012
Novel initiatives in implementation
The Coordination Reform A national reform for coordination between all levels in
the Health Care System from 2012 Based on various policy instruments using
• Legislation To facilitate cooperation between levels • Professional efforts Develop patient pathways • Organisation E.g. local medical centers • Financial incentives Co-payment for hospitalization

| Interface Management of Pharmacotherapy Stockholm September 11 2012
Systematic introduction of methods in health care Implementation from 2012 In Specialist Health Care A comprehensive system For introduction of new methods in all fields of specialist
health care combining existing functions with new
| Interface Management of Pharmacotherapy Stockholm September 11 2012
The new system will include
• Horizon scanning
• Health Technology Assessment (HTA) • Single Technology Assessment (STA)
• New medicines: The Norwegian Medicines Agency • Other methods: The Norwegian Knowledge Centre
• Full HTA • All methods: The Norwegian Knowledge Centre
• Mini HTA
• Performed within the specialist health care

| Interface Management of Pharmacotherapy Stockholm September 11 2012
The new system will include
• Processes for decision making • According to regulation for prioritization based on principles
for severity of disease, benefit from treatment and cost-effectiveness
• Implementation strategies
• National guidelines: The Norwegian Directorate of Health • Implementation in specialist health care
• Coordination, monitoring and follow-up systems
South-Eastern Norway Drug Therapy Forum Working Group
Recommendations (cont.): • Well-functioning electronic
communication systems is a must for the daily use and the updating of drug lists and guidelines.
• The work should be done in close cooperation with the national initiatives in the primary health care.

Common drug and therapy guidelines
Recommendations from a
regional working group in South-Eastern Norway
Jan Henrik Lund MD South-Eastern-Norway Regional Health Authority

Responsibility levels Norwegian Health Care
• National level
–Health Ministry with agencies
• Regional level –Regional Health Enterprises – Specialist
Health Care
• Local level –Primary Health Care

Regional level
Specialist Health Care • Four regional health authorities as public health
enterprises
• South-Eastern-Norway Regional Health Authority: – 15 hospital trusts – Population: 2,7 mill
• South-Eastern Regional Drug and Therapeutic
Committee established 2008

Coverage of medicine costs on different levels
- Hospital trusts cover medicine costs in the hospitals based on funding from the government
- Local communities cover medicine costs in local
institutions
- National insurance is responsible for reimbursement of medicine expenses outside institutions

Initiatives in the hospital sector
Drug and Therapy Committees at regional level • Common drug and therapy recommendations? • Could Norway get its ”Wise List”?
• A working group in the South-Eastern Region
formed to consider common drug list and therapy recomnmendations at regional level, including interaction with primary health care

South-Eastern Norway Drug Therapy Forum Working Group
Aim: • To describe the actual situation in the region
regarding drug and therapy recommendations • To indentify obstacles hindering the forming of a
common regional drug and therapy list • To give recommendations on how to achieve a
common regional drug and therapy list • To look on how to integrate with drug lists used
in the primary health care

South-Eastern Norway Drug Therapy Forum Working Group
Recommendations: • The work for regional, or even national,
common drug and therapy guidelines should be intensified.
• Common drug and therapy guidelines must be based on national consensus and supported by the leading medical authorities.