Stereotactic Targeting of the Globus Pallidus Internus … · in Parkinson’s Disease: Imaging...
12
TECHNIQUE APPLICATIONS Stereotactic Targeting of the Globus Pallidus Internus in Parkinson’s Disease: Imaging versus Electrophysiological Mapping Jorge Guridi, M.D., Ph.D., Arancha Gorospe, M.D., Eduardo Ramos, M.D., Gurutz Linazasoro, M.D., Maria C. Rodriguez, M.D., Jose Angel Obeso, M.D., Ph.D. Centro de Neurologia y Neurocirugia Funcional (JG, AG, ER, GL, MCR, JAO), Clinica Quiron, San Sebastian, and Neurosurgical Department (JG), Hospital de Navarra, Pamplona, Spain OBJECTIVE: The reintroduction of pallidotomy for the treatment of Parkinson’s disease (PD) has generated various opinions regarding the ideal anatomic or physiological location of the target within the globus pallidus. The role of microelectrode recording guidance in pallidotomy for the treatment of advanced PD is presently under debate. The purpose of this study was twofold. The first goal was to determine the degree of accuracy in the targeting of the globus pallidus internus (GPi) with magnetic resonance imaging (MRI), by comparing these results with the final placement of the thermolytic lesions (as defined by electrophysiological assessment). The second goal was to ascertain the somatotopic arrangement of the GPi in PD. METHODS: The analysis involved 50 patients with PD who underwent microrecording-guided pallidotomy. The theo- retical coordinates for lesioning were calculated after definition of the intercommissural line by MRI. The actual placement of the lesions was determined after mapping of the GPi by microrecording, using stimulation to identify the sensorimotor region and its somatotopic organization. RESULTS: In most cases, the lesions were placed posterior and lateral to the targets chosen by MRI. Mapping by microrecording revealed differences of 2.3 6 1.55 mm and 3 6 1.9 mm in the mediolateral and anteroposterior coordinates, respectively. The actual lesion overlapped the theoretical target for only 45% of the patients. The somatotopic organization of the GPi was analyzed. Most of the units with sensorimotor activity or tremor-related activity were in the lateral portion of the nucleus. Upper limb and axial units were in the most lateral region and mainly in the ventral one-third of the nucleus. Lower limb responses were recorded mainly in the dorsal one-third of the nucleus. Tremor-related cells were found throughout the sensorimotor region of the nucleus. CONCLUSION: These results indicate that lesion targeting based on MRI alone is not sufficiently accurate to guarantee placement of the lesion in the sensorimotor region of the GPi. (Neurosurgery 45:278–289, 1999) Key words: Microrecording, Pallidal somatotopy, Pallidotomy, Parkinson’s disease P allidotomy has been revived as a surgical procedure for the treatment of advanced Parkinson’s disease (PD). Pallidal lesions alleviate mainly bradykinesia, rigidity, and tremor during the “off” period and abolish dyskinesia induced by chronic treatment with levodopa (3, 10, 23, 25, 28, 42). Improvements after the stereotactic procedure are mainly on the side contralateral to the operation, with less alleviation on the ipsilateral side. Pallidotomy as a neuroablative surgical procedure is the subject of a continuing debate regarding target localization. Some teams consider anatomic localization by imaging and macroelectrical stimulation to be sufficient, and others think that physiological localization is necessary to yield the best possible results. The first aim of this study was to investigate the discrep- ancies between the final, electrophysiologically determined lesions in the globus pallidus internus (GPi) and the targets that had been previously chosen by magnetic resonance imaging (MRI). In addition, we define the somatotopic 278 Neurosurgery, Vol. 45, No. 2, August 1999
Transcript of Stereotactic Targeting of the Globus Pallidus Internus … · in Parkinson’s Disease: Imaging...

TECHNIQUE APPLICATIONS
Stereotactic Targeting of the Globus Pallidus Internusin Parkinson’s Disease: Imaging versus
Electrophysiological Mapping
Jorge Guridi, M.D., Ph.D., Arancha Gorospe, M.D.,Eduardo Ramos, M.D., Gurutz Linazasoro, M.D.,
Maria C. Rodriguez, M.D.,Jose Angel Obeso, M.D., Ph.D.
Centro de Neurologia y Neurocirugia Funcional (JG, AG, ER, GL, MCR, JAO),Clinica Quiron, San Sebastian, and Neurosurgical Department (JG),
Hospital de Navarra, Pamplona, Spain
OBJECTIVE: The reintroduction of pallidotomy for the treatment of Parkinson’s disease (PD) has generated variousopinions regarding the ideal anatomic or physiological location of the target within the globus pallidus. The roleof microelectrode recording guidance in pallidotomy for the treatment of advanced PD is presently under debate.The purpose of this study was twofold. The first goal was to determine the degree of accuracy in the targeting ofthe globus pallidus internus (GPi) with magnetic resonance imaging (MRI), by comparing these results with thefinal placement of the thermolytic lesions (as defined by electrophysiological assessment). The second goal wasto ascertain the somatotopic arrangement of the GPi in PD.
METHODS: The analysis involved 50 patients with PD who underwent microrecording-guided pallidotomy. The theo-retical coordinates for lesioning were calculated after definition of the intercommissural line by MRI. The actualplacement of the lesions was determined after mapping of the GPi by microrecording, using stimulation to identify thesensorimotor region and its somatotopic organization.
RESULTS: In most cases, the lesions were placed posterior and lateral to the targets chosen by MRI. Mapping bymicrorecording revealed differences of 2.3 6 1.55 mm and 3 6 1.9 mm in the mediolateral and anteroposteriorcoordinates, respectively. The actual lesion overlapped the theoretical target for only 45% of the patients. Thesomatotopic organization of the GPi was analyzed. Most of the units with sensorimotor activity or tremor-relatedactivity were in the lateral portion of the nucleus. Upper limb and axial units were in the most lateral region andmainly in the ventral one-third of the nucleus. Lower limb responses were recorded mainly in the dorsal one-thirdof the nucleus. Tremor-related cells were found throughout the sensorimotor region of the nucleus.
CONCLUSION: These results indicate that lesion targeting based on MRI alone is not sufficiently accurate toguarantee placement of the lesion in the sensorimotor region of the GPi. (Neurosurgery 45:278–289, 1999)
Key words: Microrecording, Pallidal somatotopy, Pallidotomy, Parkinson’s disease
Pallidotomy has been revived as a surgical procedure forthe treatment of advanced Parkinson’s disease (PD).Pallidal lesions alleviate mainly bradykinesia, rigidity,
and tremor during the “off” period and abolish dyskinesiainduced by chronic treatment with levodopa (3, 10, 23, 25, 28,42). Improvements after the stereotactic procedure are mainlyon the side contralateral to the operation, with less alleviationon the ipsilateral side. Pallidotomy as a neuroablative surgicalprocedure is the subject of a continuing debate regarding
target localization. Some teams consider anatomic localizationby imaging and macroelectrical stimulation to be sufficient,and others think that physiological localization is necessary toyield the best possible results.
The first aim of this study was to investigate the discrep-ancies between the final, electrophysiologically determinedlesions in the globus pallidus internus (GPi) and the targetsthat had been previously chosen by magnetic resonanceimaging (MRI). In addition, we define the somatotopic
278 Neurosurgery, Vol. 45, No. 2, August 1999

organization of the GPi and discuss its importance forpallidotomy.
PATIENTS AND METHODS
Fifty patients (29 men and 21 women; mean age, 52.28 yr;age range, 42–74 yr) with advanced PD (average duration ofdisease, 19.2 yr) were subjected to microelectrode-guided pal-lidotomy. Seventeen operations were performed in the righthemisphere and 33 in the left. All surgical procedures wereunilateral, on the side opposite that on which the signs weremore severe.
Patients selected for surgery were identified as having id-iopathic PD according to the Brain Bank Criteria (13), withinitially positive responses to levodopa. All patients exhibitedmajor complications, such as motor fluctuations and dyskine-sia, related to chronic treatment.
Patients were excluded from surgery if they exhibited car-diac or pulmonary disease, uncontrolled arterial hyperten-sion, evidence of atypical parkinsonism (with signs of uppermotor neuron disease and cerebellar involvement), unrespon-siveness to levodopa treatment, or dementia. The age of thepatients was a relative criterion for exclusion, with an upperlimit of 75 years being established.
Image acquisition
A Leksell Model G stereotactic frame was positioned afteradministration of local anesthesia, and MRI was performed(0.5 T; General Electric Medical Systems, Milwaukee, WI).Images were acquired using a T1-weighted inversion recov-ery sequence (3-mm-thick axial and sagittal slices; repetitiontime, 1500 ms; inversion time, 650 ms; field of view, 22–25 cm)and T2-weighted (3-mm-thick slices) and T1-weighted (1.8-mm-thick slices, with no interslice gap) spin echo sequences tolocalize the anterior and posterior commissures (192 3 192matrix). The software of the MRI instrument measured thedistance between the anterior and posterior commissureswith respect to the center of the frame. These data weretranscribed to a digitized sagittal stereotactic map of theSchaltenbrand-Bailey atlas (34). The atlas image was thenadjusted to fit the intercommissural distance for the patient.The initial target chosen was a point 20 to 22 mm lateral to themidline (when the third ventricle was wider, the target wasmore lateral), 2 to 3 mm in front of the center of the intercom-missural line, and 5 to 6 mm below the line described byLaitinen (26) and Laitinen et al. (27).
Surgical procedure
With the patient in a semi-sitting position, after local anes-thesia had been administered, a 14-mm burr hole (20 mmlateral to the midline and anterior to the coronal suture) wasmade. After coagulation of the dura and cortex, a guide tubewas introduced for recording. A special instrumental config-uration had been developed for neuronal recording; a mi-
crostereotactic head-stage with x-y coordinates had beenadapted to fit the stereotactic head-frame. The initial targetcoordinates were centered at 100 and 100 on the head-stage,and subsequent adjustments in the mediolateral (x) or antero-posterior (y) planes were made by withdrawing the guidecarrier and adjusting the coordinates of the x-y stage, withoutchanging the angles of the stereotactic arc. This procedureallows a rapid and precise change in coordinates; all tracks ortrajectories under study are parallel to the sagittal plane atlasand exhibit similar recording characteristics. Microrecordingwas performed by using platinum/iridium-coated microelec-trodes, with tip diameters of 2 to 4 mm (impedance, 0.2–1.0MV at 1000 Hz). The electrode was placed in a stainless steelcarrier tube (26 gauge) attached to a hydraulic microdrive(25-mm total length; David Kopf Instruments, Precision De-signs for Research, Tujunga, CA), which was connected to thehead-stage. This allowed the microelectrode to be moved, bymicrometers or more (when not recording), by a course drive.The electrode carrier and the inner guide tip were set at 45mm from the target.
A high-impedance preamplifier for recording was attachedto the microdrive assembly. The preamplifier was connectedto standard electrophysiological equipment for amplification,filtering, and discrimination of the electrophysiological sig-nals (Neurosystem-2; Atlantic Research System, Atlanta, GA).The electrode could also be used for microstimulation. Therecorded signals from single cells or units were displayed andanalyzed on an oscilloscope screen, transmitted to a signalaudio-amplifier for neuronal electromyographic recording,and stored on tape for subsequent off-line analysis.
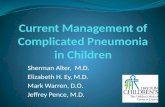
Recording tracks were made in the parasagittal plane at anangle of 45 to 60 degrees with respect to the horizontal planeof the frame. To record neuronal activity throughout thestriatum, the globus pallidus externus and GPi were moni-tored. After passing through the most ventral portion of theGPi, the microelectrode traversed the ansa lenticularis andthen entered the optic tract or internal capsule. The optic tractwas identified by a high-frequency audio signal coincidingwith a light stimulus and by the reporting of phosphene bythe patient (Fig. 1).
During the recording phase, the globus pallidus externuswas identified by two different patterns of discharge. A ma-jority of units (70–80%) exhibited periods of high-frequencydischarge separated by pauses. A few units discharged at lowfrequency, with brief high-frequency bursts. In the GPi, themajority of neurons were identified by a high-frequency andtonic discharge pattern.
To determine the somatotopic arrangement of the sensori-motor area of the GPi, neuronal activity was first recorded for30 to 60 seconds with the patient at rest; responses to passivemanipulation and active movements of the limbs (wrist, el-bow, shoulder, ankle, knee, and hip on the contralateral andipsilateral sides, with respect to the surgical procedure), neck,and orofacial region were then assessed. The neck, paraver-
Targeting the Internal Pallidum in Parkinson’s Disease
279Neurosurgery, Vol. 45, No. 2, August 1999

tebral, and abdominal musculature was passively tested withpressure (no active movements could be undertaken), andorofacial movements were assessed as jaw opening and clos-ing, tongue protrusion, and ocular movements. The units thatshowed conspicuous changes in their firing rates (judgedon-line by the investigator) in response to passive and activemovements of the contralateral joints were labeled as kines-thetic cells. After a unit was well isolated and clearly recog-nized as kinesthetic for a given body part, the investigatorcompleted testing of the remaining body regions. For practicalreasons, it was not possible to test all studied units for bothpassive and active movements. For patients who exhibitedresting tremors during the procedure, neurons discharging insynchrony with the tremors, which were identified by visualinspection of the limbs and simultaneous surface electromyo-graphic recording in the contralateral limbs, were classified astremor-related cells. The precise locations of only clearly iso-lated and stable units in each recording track were noted;these locations were subsequently compared with the atlas, todefine the topographic features of the sensorimotor regionand its somatotopic arrangement. High-quality recording for
these analyses was performed for 18 patients. Recording datafrom the remaining 32 patients were used for topographicdefinition of the GPi during surgery but not for off-line anal-ysis. Generally, recording tracks were maintained in the samesagittal plane until the internal capsule was detected. A finaltrack was then obtained in a more lateral plane (usually 2–3mm), with maintenance of the same rostrocaudal coordinate.With this template, the GPi is shorter than in previous tracks,indicating the outer limit of the GPi. Microstimulation (10–100mA, 300 Hz, 0.2–0.5 ms) was also used to establish the bound-aries of the GPi (especially the optic tract and internal cap-sule). Three to five recording tracks were generally sufficientfor mapping of the GPi sensorimotor area (Fig. 1).
Lesioning procedure
The lesioning electrode probe (tip of probe, 2 mm; diame-ter, 1.1 mm; Radionics, Burlington, MA) was advanced as faras the dorsal border of the GPi, and macrostimulation wasperformed at selected intervals (2 mm) until the optic tractwas reached. The stimulation frequency was 300 Hz (pulsewidth, 0.2 ms), and the safety stimulation thresholds were 0.7to 1 mA for the optic tract and 0.3 to 0.5 mA for the internalcapsule (Grass S48 stimulator; Medical Instruments, Quincy,MA). These parameters allowed the pallidotomy to be per-formed approximately 1 mm above the optic tract and 2 mmanterior to the internal capsule, without producing any per-manent deficits. The temperature of the lesioning probe was60°C, 70°C, and then 80°C, each for 60 seconds (radiofrequen-cy generator RFG-C; Radionics). This procedure producedcylindrical lesions of approximately 3 mm in diameter, withvariable lengths of 4 to 7 mm (43). The volumes of the lesions,as calculated in the operating room and later confirmed byMRI, were approximately 100 to 150 mm3 (volume 5 4/3p 3r1 3 r2 3 r3, where r1 is the anteroposterior radius, r2 is theventrodorsal radius, and r3 is the mediolateral radius). Whenthe most caudally placed lesion was thought to miss the entiresensorimotor region, as defined above, a second or thirdlesion was made in a more rostral location. The average timefor the procedure was 3.5 hours.
Fifty patients underwent surgery, and 50 GPi analyses, witha total of 285 recording trajectories or tracks, were performed.The mean number of recording tracks for mapping duringguided pallidotomy was 4.92 (range, 3–11). The mean numberof lesions was 2.3 (range, 1–3) for each patient. A few days(3–5 d) after surgery, control MRI was performed. The imageswere used to reconstruct the coordinates of the lesion, takinginto consideration the data recorded during the mappingprocedure. In MRI analysis, the lesions were measured in T1-and T2-weighted scans (2-mm-thick slices, with no interslicegaps) in the axial plane only. The high-intensity signal wasmeasured. Therefore, the coordinates of the initial lesion cor-responded (by definition, on the basis of the method used) tothe most lateral and posterior region of the GPi explored ineach operation. Taking this as a reference, we extrapolated thelaterality of the recording tracks for each patient, dividingthe GPi into three sagittal templates (L-17, L-20, and L-22 orgreater) according to the Schaltenbrand-Wharen atlas (35).
FIGURE 1. Methodological details of pallidotomy guided bymicrorecording. The first track was generally located in amediolateral plane of approximately 20 to 22 mm. In 70% ofthe cases, the optic tract was recorded and microstimulatedin this trajectory. In the same sagittal plane, the later tracksanalyzed the GPi length, somatotopic organization, and dis-tance between the optic tract and the ventral border of thenucleus. When the internal capsule was stimulated, the nextand final track was placed in a more lateral plane. After indi-vidual mapping of the nucleus, which revealed boundaries,optic tract position, and internal capsule location, the lesionwas planned. The first track was generally in ParasagittalTemplate 20 of the Schaltenbrand-Wharen atlas (35) and isanterior in this report. The optic tract and GPi ventral borderindicated laterality and helped establish the rostrocaudallocation. AC, anterior commissure; GPe, globus pallidusexternus; IC, internal capsule; OT, optic tract.
280 Guridi et al.
Neurosurgery, Vol. 45, No. 2, August 1999

The L-22 plane was the lesion template, the L-20 plane gen-erally coincided with the first track recorded, and the L-17plane was more medial than the initial recording track. Thisprocedure was used for all patients, regardless of the actualdistance between the lesion and the midline or the mediolat-eral extent of the sensorimotor pallidum. It must be noted thatthese three planes may not correspond exactly to the actuallaterality values for every patient and should be used asrelative references. The dorsoventral distribution of the GPiwas determined by subdividing the GPi into three equal axialplanes, taking the level of the optic tract (as established byrecording and microstimulation) as the initial reference.
The coordinates chosen after MRI and digitized sagittalstereotactic mapping corresponded to the first recording trackand are defined as the “theoretical coordinates.” The coordi-nates of the most ventrolateral and posterior lesions, whichwere chosen according to the microrecording and stimulationfindings, are regarded as the “final coordinates.” Deviationsfrom the target coordinates were calculated using absolutevalues for the three coordinates of the space, regardless oftheir relative positions. We compared the degree of matchingbetween the two coordinate sets, to assess the accuracy oftargeting by imaging alone. This calculation does not take intoaccount the locations of other lesions (usually more anteriorlyplaced) that were subsequently made. Our strategy was tolesion the sensorimotor portion of the GPi as extensively aspossible.
RESULTS
Clinical results
The effects of pallidotomy in this group of patients after 1year of follow-up monitoring (for 35 patients) have beenpresented at different meetings and reported in detail else-where (15, 29, 30). In summary, the most significant improve-ment was in contralateral dyskinesia (90%, P , 0.01). Con-tralateral pallidal lesions decreased the mean “off” motor
Unified PD Rating Scale score by 33.7% (P , 0.01) 1 year aftersurgery. Significant improvements were also observed in con-tralateral tremors (72%) and rigidity (67%) (P , 0.01). Brady-kinesia scores were improved by 46% (P , 0.01). Axial signswere improved, but these results were less predictable. Twocases involved major complications (hemorrhage) that weredirectly related to surgery. One patient died 2 months aftersurgery, and the other experienced a good recovery. Neitherof these patients belonged to the group of 18 patients whowere studied in detail intraoperatively and are described be-low. Antiparkinsonian drug administration was decreased by5% after surgery (not significant). The results of the pallidallesions after 1 year of follow-up monitoring are shown inTable 1.
Accuracy of targeting by MRI
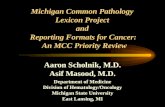
The distributions of the lesion coordinates in the threestereotactic planes are shown in Figures 2 and 3. The differ-ence between the theoretical target and the final target in thex coordinate (mediolateral plane) was between 6 mm lateraland 3 mm medial, with a mean of 2.3 6 1.55 mm (Fig. 2A). Thedeviation in the y coordinate (anteroposterior plane) showeda range of 3 mm anterior to 8 mm posterior, with a mean of3 6 1.9 mm (Figs. 2B and 3). The mean deviation in the zcoordinate (dorsoventral plane) was 1.6 6 1.11 mm, rangingfrom 4.0 mm dorsal to 5.0 mm ventral (Fig. 3).
In most cases, the coordinates of the final target were lo-cated posteriorly and laterally, with respect to the initial tar-get established by imaging (Fig. 3). The estimated extension ofthe final lesion included the theoretical target in only 45%of the procedures (Fig. 4).
Somatotopic organization of the GPi
Data for 18 patients for whom neuronal activity was suffi-cient for assessment were analyzed. A total of 403 units wereisolated from the GPi. One hundred forty-five (38.2%) neu-
TABLE 1. Results of Pallidotomy (35 Patients) after 1 Year of Follow-up Monitoringa
Scoreb
PRange Basal 1-yr Follow-up
UPDRS score 0–108 49 (15.5) 32.46 (11.6) ,0.01Tremor, contralateral 0–4 1.37 (1.2) 0.7 (0.16) ,0.01Rigidity, contralateral 0–4 2.27 (0.7) 0.84 (0.45) ,0.01Bradykinesia, contralateral 0–4 2.74 (0.7) 1.33 (0.7) ,0.01Axial signs 0–4 2.18 (0.9) 1.36 (0.7) ,0.01Dyskinesia, contralateral 0–4 2.5 (1.1) 0.07 (0.3) ,0.01Tremor, rigidity, and bradykinesia, ipsilateral 0–36 13.1 (6.2) 14.18 (5.5) NSTremor, rigidity, and bradykinesia, contralateral 0–36 19.0 (5.1) 7.68 (3.6) ,0.01
a The results of our study showed that, 1 year after surgery, the most significant improvement was the reduction of dyskinesia; this wasmaintained for 1 year of follow-up monitoring. Pallidotomy significantly improved “off” contralateral Unified Parkinson’s Disease Rating Scale(UPDRS) motor performance, by 33.7% (P < 0.01). The alleviation of contralateral tremor and rigidity was more significant than that ofbradykinesia (P < 0.01). The improvement in axial signs was less predictable but was significant. The calculated median preoperative andpostoperative group scores were compared using the Wilcoxon rank test. NS, not significant.
b Numbers in parentheses are standard deviations.
Targeting the Internal Pallidum in Parkinson’s Disease 281
Neurosurgery, Vol. 45, No. 2, August 1999

rons of 368 assessed units showed changes in their firing rateswith contralateral movements (kinesthetic cells), and 35 unitswere tremor-related cells. The somatotopic distribution of thekinesthetic neurons is shown in Table 2. Distal joints (wrist,fingers, and ankle) of the contralateral limbs showed a greaterpercentage of responses than did proximal joints (elbow,shoulder, and hip), with 57% in the lower limb and 55% in theupper limb. Some neurons showed changes in their firingrates in response to stimulation of several segments or jointsand were labeled as “multiunits.” There were 5 multiunits forthe lower limb and 10 for the upper limb.
The dorsoventral distribution of the neurons with sensori-motor responsiveness, according to the body part activated toelicit neuronal discharges, is summarized in Table 2 and Figure5. The leg representation was found dorsally in the nucleus, so
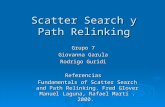
that 50% of leg-related units were in the most dorsal one-thirdof the GPi (Fig. 6). Units correlated with facial, jaw, and axialmovements were ventral in the GPi, with 68.7% being in theventral one-third of the nucleus (Fig. 7). For the upper limb, 66%of neurons were in the ventral two-thirds of the GPi (Fig. 8).
With respect to the mediolateral organization, 81 units(62%) were located in the most lateral plane (L-22) and 52units (37%) were isolated in the L-20 plane (Fig. 5), whichoften coincided with the first recording track (the theoreticaltarget). Nine neurons with “driving” were found in the L-17plane, a template that was usually medial to the initial record-ing track. Neurons corresponding to the upper limb weredistributed between the L-20 and L-22 planes, predominatingin the most lateral template (60% of the neurons were re-corded in the L-22 plane) (Fig. 8). Face and jaw units and the
FIGURE 2. Distribution of the pallidallesions after microrecording and theirdistances from the targets chosen byMRI, for the x coordinate (A) and the ycoordinate (B ). The target chosen byimaging was the first recording trajec-tory. There were mismatches of 2.3 mmin the mediolateral plane and 3.0 mmin the anteroposterior plane.
282 Guridi et al.
Neurosurgery, Vol. 45, No. 2, August 1999

few neurons corresponding to the neck and trunk were foundprimarily in the L-22 plane (Fig. 7). The lower limb wasequally represented in the three lateral planes, but it is note-worthy that all neurons in the L-17 plane belonged to the leg(Fig. 6).
In summary, the majority of cells with sensorimotor re-sponses in the GPi were found in the L-20 plane or beyond.The face representation was mainly lateral and ventral. Theleg was dorsal and present in the three sagittal templates.Neurons related to the arm were mainly lateral and werefound in the ventral two-thirds of the GPi.
Thirty-five tremor-related cells were recorded and identi-fied in these patients. Oscillatory or rhythmic neuronal activ-ity was not detected in patients in whom tremor was notpresent at the time of surgery. The somatotopic distribution oftremor-related cells is summarized in Figures 5 and 6. Thesecells were evenly distributed in the three sagittal planes andshowed the same somatotopic pattern as kinesthetic units.Tremor-related units were recorded throughout the dorso-ventral extent of the GPi.
Optic tract and absent GPi recording
Microstimulation with the recording electrode elicited anoptic tract response with the first trajectory in eight patients(16%) for whom recording had shown typical striatal andglobus pallidus externus neuronal activity but no GPi units.The initial recording trajectory in these cases was anterior tothe GPi.
DISCUSSION
There is now renewed interest in the therapeutic possibil-ities of pallidotomy and deep-brain stimulation of the palli-
FIGURE 3. Final placement of the pallidal lesions aftermicrorecording and their correlation (in millimeters) with thetargets chosen by imaging, in the y direction (anteroposteriorcoordinate) and the z direction (ventrodorsal coordinate).Black square, target chosen by imaging.
FIGURE 4. Mean distancebetween the theoreticaltarget determined by imaging(20–22 mm lateral to themidline, 3 mm anterior to themidpoint of theintercommissural line, and5–6 mm below theintercommissural line) (blackpoint) and the finalplacement of the lesion after
guided GPi pallidotomy (gray circle). Dashed lines, laminapallida, medial and lateral. The first lesion (diameter,approximately 3 mm) overlapped the target chosen byimaging for only 45% of the patients. The diagramrepresents 4.5 mm below the intercommissural line (Plate 55in the Schaltenbrand-Wharen atlas [35]).
TABLE 2. Somatotopy in the Globus Pallidus Internusa
No. of Units
Lower limb (45 units, 34.%)b
Dorsal 25 (50%)Medial 15 (30%)Ventral 5 (10%)
Upper limb (54 units, 44.%)c
Dorsal 13 (19%)Medial 16 (26%)Ventral 25 (40%)
Axial and facial (32 units, 22%)d
Dorsal 3 (9.3%)Medial 7 (22.5%)Ventral 22 (68.7%)
Multiunits (15)e
aTotal isolated units in the globus pallidus internus, 368; total unitswith driving, 145 (38.3%).
b Hip, 10 units; knee, 6 units; ankle, 29 units.c Shoulder, 10 units; elbow, 8 units; wrist, 29 units; fingers, 7 units.d Neck, 4 units; jaw, 26 units; lumbar, 2 units.e Lower limb multiunits, 5; upper limb multiunits, 10.
FIGURE 5. Somatotopic representation of units correlatedwith passive and active contralateral movements of the limbsand facial units in patients who underwent pallidotomy. Thediagram represents units analyzed in Templates L-20 andL-22 of the Schaltenbrand-Wharen atlas (35). GPe, globuspallidus externus; IC, internal capsule; OT, optic tract.
Targeting the Internal Pallidum in Parkinson’s Disease 283
Neurosurgery, Vol. 45, No. 2, August 1999

dum and subthalamic nucleus in PD. This enthusiasm couldrapidly fade if the surgical technique used fell below requiredstandards. In this regard, our findings are directly relevant tothe issue of ensuring the outcome of surgery in PD.
Targeting
We observed a relative discrepancy between the coordi-nates of the lesion defined by imaging (theoretical target) andthose finally chosen for the lesion (final target). Such a differ-ence has several practical consequences with respect to thegoal of obtaining the best possible results and minimal sideeffects with pallidotomy.
The preferred method for subcortical target localization isthe subject of an ongoing debate in the field of functionalneurosurgery (9, 21). For PD in particular, the classic ap-proach has consisted of defining the coordinates by usingventriculography and, more recently, computed tomographyor MRI of the brain as imaging methods plus macrostimula-tion with the lesioning probe as a means of functional assess-ment. The reintroduction of pallidotomy for the treatment ofPD has evolved with the physiological definition of the sen-sorimotor region of the GPi, mainly using the microrecording-guided technique (3, 28, 31, 38, 42). Pallidotomy is now widelyused throughout the world, but there is no agreement regard-ing the necessity of using microrecording (9, 21, 42). Essentialto this argument is the question of whether definition of thetarget is only anatomic (imaging) or requires physiologicalconfirmation. Our findings support the latter view.
It might be argued that our results are explainable becausethe MRI resolution achieved in this study was inadequate forthe purpose of defining the GPi. According to this view, theapplication of MRI with higher magnetic fields might reducethe degree of variability (14). However, Lozano et al. (31),using 1.5-T MRI, observed a similar degree of error, suggest-ing that imaging quality is not the only or crucial factorinvolved in the inaccuracy discussed here. Hiner et al. (18)reported that microrecording led to a change in the finalplacement of the lesion in 70% of patients, and Azizi et al. (2)showed that, in 25% of the cases, the theoretical coordinateswere more than 5 mm away from the final site of the lesion.Tsao et al. (40) recently reported that, in 13 of 25 patients,hypothetical lesion positions were located in such a way thatthe lesion center would not have remained in the globuspallidus without microelectrodes. Vitek et al. (43) indicatedthat, in their most recent experience, there were overall dif-ferences of 2.2 and 1.3 mm in the rostrocaudal and mediolat-eral planes, respectively, between the target location determinedby MRI and the final coordinates of the lesion determined bymicrorecording. It seems, therefore, that a certain degree of
FIGURE 6. Somatotopic representation of units correlatedwith contralateral movements of the lower limb and tremor-related units detected during surgery. There is a preponder-ance of units representing the lower limb in the dorsalregion. Tremor-related cells for any body part are distributedevenly throughout Nucleus Templates L-20 and L-22 of theSchaltenbrand-Wharen atlas (35). GPe, globus pallidus exter-nus; IC, internal capsule; OT, optic tract.
FIGURE 7. Somatotopic representation of units correlatedwith facial, jaw, and axial neurons. A striking predominanceof neurons in the posteroventral and lateral regions isobserved. GPe, globus pallidus externus; IC, internal capsule;OT, optic tract.
FIGURE 8. Somatotopic representation of units correlatedwith the upper limb. Units predominate in the lateral andventral zones of the GPi. GPe, globus pallidus externus;IC, internal capsule; OT, optic tract.
284 Guridi et al.
Neurosurgery, Vol. 45, No. 2, August 1999

variability between imaging-derived and physiologically speci-fied targets is the rule in basal ganglia surgery.
Sources of errors
Stereotactic frames have provided extreme levels of me-chanical precision for surgical localization, but the procedureis not completely accurate because the errors of localizationare additive (32). Errors arise from two main sources, namelyimaging and individual variations. Imaging errors introducedistortion during the image-acquisition phase and exist withany method used for targeting identification. Positive-contrastventriculography is associated with imaging distortion be-cause of anterior shifting of the third ventricle; in addition,ventriculography prolongs hospital stays and may be accom-panied by unpleasant side effects (16). Computed tomogra-phy and MRI are noninvasive techniques and provide directobservation of brain structures, but both introduce distortionduring the imaging procedure. The accuracy of the computedtomography-guided stereotactic system is dependent on thecomputed tomographic scan slice thickness, the interslicespacing, and the size of the target itself (5). MRI has beenwidely reported to introduce distortion resulting from inho-mogeneities in the magnetic field and nonlinear magneticfield gradients (24, 37). The stereotactic frame itself, with itsmetal components, may introduce errors or distortion duringimage acquisition (44).
The second source of error lies in individual anatomic vari-ations. Hawrylyshyn et al. (17) reported that the thalamocap-sular border shifts in accordance with the width of the thirdventricle. The thalamic border is more lateral when the ven-tricle is wider. Kelly et al. (22) reported that the theoreticaltarget did not coincide with the final target, as established byphysiological findings, for 75% of patients subjected to thalam-otomy. Variability is greater in the pallidum than in the thala-mus, because the pallidum is farther away from the midline andhas a more complex shape. Another factor to be considered is thepossibility of brain shifting after opening of the dura and duringsurgery. There may be variations between the brain positionwhen the patient is in the supine position during imageacquisition and that when the patient is in a semi-sittingposition during surgery. This effect may be particularly im-portant in older patients, who have wider subarachnoidspaces and cisterns.
Although the accuracy of targeting without microelectrodeguidance may be quite good for a high proportion of patientswho undergo pallidotomy, the findings reported in this andother studies suggest that there is a high incidence of changesin the final lesion locations, indicating that macrostimulationalone does not provide sufficient information for lesioning.Macrostimulation allows determination of the boundaries ofthe nucleus with tonic or clonic movements and phosphenes,indicating that the tip of the electrode is close to the capsuleand optic tract, respectively. However, macrostimulation doesnot indicate whether the electrode is within the GPi, as in theeight cases showing false-positive stimulation among our pa-tients. We suggest that precise mapping with a microelectrodeguide is the best way to create a lesion with sufficient prob-
ability of improving the long-term outcome. Although thisreport suggests improved accuracy with these recording tech-niques, there is no consensus demonstrating their clinicalbenefits.
Importance of defining the sensorimotor region ofthe GPi
The current use of pallidotomy for the treatment of PD aimsto define the sensorimotor region of the GPi while sparing theassociated regions (1, 7). This is based on experimental evi-dence indicating that the basal ganglia are somatotopicallyorganized in monkeys (7, 12) and that only inactivation of thesensorimotor region of the GPi led to alleviation of parkinsonisminduced by 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridinein monkeys (45). Finally, there is current clinical evidenceindicating that only lesions of the posteroventral and lateralGPi are associated with clear-cut motor benefits; dorsomediallesions produced no improvement or only transient improve-ment (43) (JL Vitek, personal communication). The GPi inpatients with PD has a somatotopic organization that is sim-ilar to that described in monkeys (38, 43).
Microrecording is the only effective method for investigatingthe somatotopic organization of the GPi. In monkeys madeparkinsonian with 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine,the number of cells responding to active and passive movementsof the limbs is significantly increased, regardless of whether thesomatotopic arrangement is preserved, as has been analyzed indetail (4, 7, 11, 12). Filion et al. (12) showed that, in monkeys, theparkinsonian state is correlated with a larger number of unitsresponding to movement of several body parts. This character-istic may account for the variability encountered in human stud-ies. In patients with PD, the proportion of cells with responses topassive and active limb movements varies from 19 to 46% (36, 38,43). This large range may be attributable to bias in the selection ofthe cells. Our own results (38% of cells with sensorimotor re-sponses) agree with those reported for monkeys and are probablynear the actual values. The somatotopic organization of the GPiin patients with PD has been analyzed by a few groups, withvarying findings. Vitek et al. (43) reported an organization sim-ilar to that described for monkeys. The majority of neurons withsensorimotor responses were found in the posterolateral regionof the GPi (L-18 or L-19 of the Schaltenbrand-Bailey atlas [34]).The leg was preferentially represented dorsomedially, with re-spect to the arm and face. The jaw representation was foundmore ventrally. On the other hand, Taha et al. (38) described armneurons in two cluster groups distributed rostrocaudally (i.e., arostral segment 5 mm above the pallidal base and a caudalsegment 1.5 to 3 mm above the pallidal base), whereas legkinesthetic units were located more centrally (3–4.5 mm abovethe pallidal base). In this study, we found that arm-related neu-rons were located mainly in the ventromedial region and cau-dolaterally of the nucleus. The leg-related cells were mainlydorsal and extended mediolaterally throughout the nucleus,reaching as medially as 17 mm from the midline in the atlas ofSchaltenbrand and Wharen (35). A large majority of axial andface-related units were found ventrally and laterally (more than20 mm from the midline). Our results, therefore, are in keeping
Targeting the Internal Pallidum in Parkinson’s Disease 285
Neurosurgery, Vol. 45, No. 2, August 1999

with the findings for monkeys (6, 8) and the observations byVitek et al. (43) for patients with PD. The somatotopic arrange-ment confirmed here in the parkinsonian state is valid, we think,for practical intraoperative purposes and as a general referenceregarding the organization of the GPi in human subjects. We didnot use any test designed to detect possible internal segregationof motor neurons according to their cortical projection areas, asindicated by Hoover and Strick (19) in normal monkeys. There-fore, we suggest that in PD the somatotopic arrangement of theGPi can be summarized as follows: the majority of cells arelocated posterolaterally in the nucleus and, within this region,the leg is more dorsal than the arm and the face, which (with thejaw) is mainly ventral.
Tremor-related cells
Cells with tremor-related activity were present only in thesensorimotor region of the GPi and showed a somatotopicdistribution similar to that of the kinesthetic cells discussedabove. The existence of tremor-related cells in the GPi wasfirst described by Umbach and Ehrhardt (41) and was morerecently analyzed by Hutchinson et al. (20), who found thesecells approximately 3 to 6 mm above the optic tract butprovided no additional details regarding their somatotopicarrangement. We found tremor-related cells within the sen-sorimotor region of the GPi, with no specific clustering fortheir distribution (Figs. 5 and 6).
Recognition of GPi somatotopy and the distribution oftremor-related cells may have practical implications for pro-ducing optimal results with pallidotomy. Not all patients whoundergo surgery have the same clinical characteristics. In arelatively large proportion of patients, the clinical motor signsand dyskinesia predominate in one body segment (for exam-ple, the leg). In such instances, our experience indicates thatfailure to determine the location of neurons related to thatbody part may yield suboptimal benefits. In keeping with thissuggestion, Taha et al. (39) reported that the efficacy of pal-lidotomy in the treatment of tremors was significantly greaterfor patients in whom tremor-related cells were recorded at thetime of surgery.
CONCLUSION
The only approach to definitively establish whether micro-recording is critical for the achievement of optimal resultsafter pallidotomy involves a prospective randomized study.Such a trial is unlikely to be performed with this methodol-ogy. The clinical benefits obtained for our patients and thoseof other groups using similar methods are not substantiallydifferent, at first glance, from those reported by teams notusing microrecording. This is clearly true for the antidyski-netic effects of pallidotomy, but a closer analysis of the pub-lished data suggests that patients with lesions in the sensori-motor pallidum retained their benefits, including alleviationof axial symptoms, whereas patients with lesions outside thesensorimotor GPi region lost their benefits (43).
In accordance with the aforementioned technical limitationsof stereotactic procedures and the experimental and clinicaldata indicating the functional organization of the basal gan-
glia, we think that pallidotomy should be performed withprecise delineation of the sensorimotor region. This approachrequires functional definition of the GPi motor territory,which is not possible with either imaging alone or imagingand macrostimulation together. Placement of the lesion on thebasis of MRI and macrostimulation findings without micro-electrode recording is considered, according to the resultspresented here, to be insufficient for adequate lesioning of theGPi in patients with PD.
We confirmed that the somatotopic arrangement of the GPiin patients with PD is similar to that found in monkeys; theleg representation is located in the most dorsal and medialplanes with respect to the arm, face, and jaw, which are foundmore ventrally and laterally in the sensorimotor region of thenucleus. A similar distribution was found for cells withtremor-related activity. We think that verifying this organiza-tion in each patient by microrecording is the best way toachieve optimal clinical results with pallidotomy.
ACKNOWLEDGMENTS
We thank Carol Elsden for assistance in the preparation ofthis manuscript.
This work was supported in part by the National ParkinsonFoundation (Miami, FL).
Received, November 10, 1998.Accepted, March 30, 1999.Reprint requests: Jorge Guridi, M.D., Ph.D., Centro de Neurologia yNeurocirugia Funcional, Clinica Quiron, 20012 San Sebastian, Spain.
REFERENCES
1. Alexander GE, DeLong MR, Strick PL: Parallel organization offunctionally segregated circuits linking basal ganglia and cortex.Annu Rev Neurosci 9:357–381, 1986.
2. Azizi A, Goldman WH, Moreledge D: Posteroventral pal-lidotomy: Comparison of the accuracy of anatomical targets de-fined by MR and CT imaging with physiological targets definedby microelectrode recording. Neurology 46[Suppl]:A199, 1996(abstr).
3. Baron MS, Vitek JL, Bakay RAE, Green J, Kaneoke Y, HashimotoT, Turner RS, Woodward JL, Cole SA, McDonald WM, DeLongMR: Treatment of advanced Parkinson’s disease by posterior GPipallidotomy: 1-year results of a pilot study. Ann Neurol 40:355–366, 1996.
4. Bergman H, Wichmann T, Karmon B, DeLong MR: The primatesubthalamic nucleus: Part II—Neuronal activity in the MPTPmodel of parkinsonism. J Neurophysiol 72:507–520, 1994.
5. Bucholz RD, Ho HW, Rubin JP: Variables affecting the accuracy ofstereotactic localization using computerized tomography. J Neuro-surg 79:667–673, 1993.
6. DeLong MR: Activity of pallidal neurons during movement.J Neurophysiol 34:414–427, 1971.
7. DeLong MR: Primate models of movement disorders of basalganglia origin. Trends Neurosci 13:281–285, 1990.
8. DeLong MR, Crutcher MD, Georgopoulos AP: Primate globuspallidus and subthalamic nucleus: Functional organization.J Neurophysiol 53:530–543, 1985.
286 Guridi et al.
Neurosurgery, Vol. 45, No. 2, August 1999

9. Favre J, Taha JM, Nguyen TT, Gildenberg PL, Burchiel KJ: Pal-lidotomy: A survey of current practice in North America. Neuro-surgery 39:883–892, 1996.
10. Fazzini E, Dogali M, Sterio D, Eidelberg D, Beric A: Stereotacticpallidotomy for Parkinson’s disease: A long-term follow-up ofunilateral pallidotomy. Neurology 48:1273–1277, 1997.
11. Filion M, Tremblay L: Abnormal spontaneous activity of globuspallidus neurons in monkeys with MPTP-induced parkinsonism.Brain Res 547:142–151, 1991.
12. Filion M, Tremblay L, Bedard PJ: Abnormal influences of passivelimb movement on the activity of globus pallidus neurons inparkinsonian monkeys. Brain Res 444:165–176, 1988.
13. Gibb WRG, Lees AJ: The relevance of the Lewy body to thepathogenesis of idiopathic Parkinson’s disease. J Neurol Neuro-surg Psychiatry 51:745–752, 1988.
14. Giller CA, Dewey RB, Ginsburg MI, Mendelsohn DB, Berk AM:Stereotactic pallidotomy and thalamotomy using individual vari-ations of anatomical landmarks for localization. Neurosurgery42:56–65, 1998.
15. Guridi J, Gorospe A, Linazasoro G, Ramos E, Mozo A, Obeso JA:Two years follow-up of pallidotomy for advanced Parkinson’sdisease. Acta Neurochir (Wien) 140:846, 1998 (abstract).
16. Hariz MI, Bergenheim AT: A comparative study on ventriculographicand computerized tomography-guided determinations of brain targetsin functional stereotaxis. J Neurosurg 73:565–571, 1990.
17. Hawrylyshyn PA, Tasker RR, Organ LW: Third ventricular widthand the thalamocapsular border. Appl Neurophysiol 39:34–42,1976–1977.
18. Hiner B, Madden K, Neal J: Effect of microelectrode recording onfinal lesion placement in pallidotomy. Neurology 48[Suppl]:A251, 1992 (abstr).
19. Hoover JE, Strick PL: Multiple output channels in the basal gan-glia. Science 259:819–821, 1993.
20. Hutchinson WD, Lozano AM, Tasker RR, Lang AE, DostrovskyJO: Identification and characterization of neurons with tremor-frequency activity in human globus pallidus. Exp Brain Res 113:557–563, 1997.
21. Kelly PJ: Pallidotomy in Parkinson’s disease. Neurosurgery 36:1154–1157, 1995.
22. Kelly PJ, Derome P, Guiot G: Thalamic spatial variability and thesurgical results of lesions placed with neurophysiologic control.Surg Neurol 9:307–315, 1978.
23. Kishore A, Turnbull IM, Snow BJ, de la Fuente-Fernandez R,Schulzer M, Mak E, Yardley S, Calne DB: Efficacy, stability andpredictors of outcome of pallidotomy for Parkinson’s disease:Six-month follow-up with additional 1-year observations. Brain120:729–737, 1997.
24. Kondziolka D, Dempsey PK, Lunsford LD, Kestle JRW, Dolan EJ,Kanal E, Tasker RR: A comparison between magnetic resonanceimaging and computed tomography for stereotactic coordinatedetermination. Neurosurgery 30:402–407, 1992.
25. Kopyov O, Jacques D, Duma C, Buckwalter G, Kopyov A, Lieber-man A, Copcutt B: Microelectrode-guided posteroventral medialradiofrequency pallidotomy for Parkinson’s disease. J Neurosurg87:52–59, 1997.
26. Laitinen LV: Pallidotomy for Parkinson’s disease. NeurosurgClin North Am 6:105–112, 1995.
27. Laitinen LV, Bergenheim AT, Hariz MI: Leksell’s posteroventralpallidotomy in the treatment of Parkinson’s disease. J Neurosurg76:53–61, 1992.
28. Lang AE, Lozano AM, Montgomery E, Duff J, Tasker RR,Hutchinson W: Posteroventral medial pallidotomy in advancedParkinson’s disease. N Engl J Med 337:1036–1042, 1997.
29. Linazasoro G, Gorospe A, Rodriguez MC, Guridi J, Ramos E,Mozo A, Obeso JA: Assessment of prognostic factors of long termclinical outcome after pallidotomy. Mov Disord 13[Suppl 2]:304,1998.
30. Linazasoro G, Gorospe A, Rodriguez MC, Guridi J, Ramos E, MozoA, Obeso JA: Pallidotomy in the treatment of complicatedParkinson’s disease: Clinical results at two years and analysis ofprognostic factors [in Spanish]. Neurologıa 14:53–61, 1999.
31. Lozano A, Hutchinson W, Kiss Z, Tasker R, Davis K, DostrovskyJ: Methods for microelectrode-guided posteroventral pal-lidotomy. J Neurosurg 84:194–202, 1996.
32. Maciunas RJ, Fitzpatrick JM, Galloway RL, Allen GS: Beyondstereotaxy: Extreme levels of application accuracy are providedby implantable fiducial markers for interactive image-guidedneurosurgery, in Maciunas RJ (ed): Interactive Image-Guided Neuro-surgery. Park Ridge, AANS, 1993, pp 259–270.
33. Obeso JA, Guridi J, DeLong MR: Surgery for Parkinson’s disease.J Neurol Neurosurg Psychiatry 62:2–8, 1997 (editorial).
34. Schaltenbrand G, Bailey P: Introduction to Stereotaxis with an Atlasof the Human Brain. Stuttgart, Thieme, 1959.
35. Schaltenbrand G, Wharen W: Atlas for Stereotaxy of the HumanBrain. Stuttgart, Thieme, 1977.
36. Sterio D, Beric A, Dogali M, Fazzini E, Alfaro G, Devinsky O:Neurophysiological properties of pallidal neurons in Parkinson’sdisease. Ann Neurol 35:586–591, 1994.
37. Sumanaweera TS, Adler JR Jr, Napel S, Glover GH: Characteriza-tion of spatial distortion in magnetic resonance imaging and itsimplications for stereotactic surgery. Neurosurgery 35:696–704, 1994.
38. Taha JM, Favre J, Baumann TK, Burchiel KJ: Characteristics andsomatotopic organization of kinesthetic cells in the globus pal-lidus of patients with Parkinson’s disease. J Neurosurg 85:1005–1012, 1996.
39. Taha JM, Favre J, Baumann TK, Burchiel KJ: Tremor control afterpallidotomy in patients with Parkinson’s disease: Correlationwith microrecording findings. J Neurosurg 86:642–647, 1997.
40. Tsao K, Wilkinson S, Overman J, Koller WC, Batnitzky S, GordonMA: Pallidotomy lesion locations: Significance of microelectroderefinement. Neurosurgery 43:506–513, 1998.
41. Umbach W, Ehrhardt KJ: Microelectrode leads in the basal gan-glia in man [in German]. Arch Psychiatr Nervenkr 207:106–113,1965.
42. Vitek JL, Bakay RAE: The role of pallidotomy in Parkinson’sdisease and dystonia. Curr Opin Neurol 10:332–339, 1997.
43. Vitek JL, Bakay RAE, Hashimoto T, Kaneoke Y, Mewes K, ZhangJY, Rye D, Starr P, Baron M, Turner R, DeLong MR: Microelectrode-guided pallidotomy: Technical approach and application for medi-cally intractable Parkinson’s disease. J Neurosurg 88:1027–1043,1998.
44. Walton L, Hampshire A, Forster DMC, Kemeny AA: A phantomstudy to assess the accuracy of stereotactic localization, usingT1-weighted magnetic resonance imaging with the Leksell stereo-tactic system. Neurosurgery 38:170–178, 1996.
45. Wichmann T, Baron MS, DeLong MR: Local inactivation of thesensorimotor territories of the internal segment of the globuspallidus and the subthalamic nucleus alleviates parkinsonian mo-tor signs in MPTP-treated monkeys, in Percheron G, McKenzie JS,Feger J (eds): The Basal Ganglia IV: New Ideas and Data on Structureand Function. New York, Plenum Press, 1994, pp 357–363.
COMMENTS
This is another article demonstrating the advisability ofelectrophysiological recording during deep-brain stereotactic
Targeting the Internal Pallidum in Parkinson’s Disease 287
Neurosurgery, Vol. 45, No. 2, August 1999

surgery, especially for far-midline targeting. Whether imag-ing distortion, individual anatomic variability, or individualfunctional variability among patients with Parkinson’s dis-ease (PD) prompts the use of physiological mapping is amatter of discussion. Perhaps all three play a role in thevariations observed, in almost every case, between the prede-termined target and the final target of posteroventral pal-lidotomy, but the last, i.e., the functional variability of theglobus pallidus internus (GPi) among individual patientswith PD, is probably the most important. Unfortunately, thereis no way to demonstrate changes in the somatotopic arrange-ment of the sensorimotor area of the GPi in normal subjectsversus patients with PD, as implied in the Discussion. There-fore, we must consider imaging distortion and individualanatomic variations. Although I am primarily in agreementwith the authors, I am not sure that positive-contrast or evenair ventriculography should be completely disregarded asadequate imaging techniques for stereotactic functional neu-rosurgery; together with microelectrode recording, these tech-niques were adequate in the era before computed tomogra-phy and magnetic resonance imaging (MRI). However, forcorrection of individual anatomic variations, microelectroderecordings are unsurpassed.
Jose Gerardo Martın RodrıguezMadrid, Spain
Guridi et al. describe their stereotactic targeting of the GPi.Their anatomic versus electrophysiological mapping and theirdescription of the somatotopic organization of the GPi andtremor-related cells are very similar to our work (2–4). Al-though it is most rewarding to see one’s own work corrobo-rated by others in a well-performed study, I have a fewadditional points to discuss.
The somatotopic arrangement described here is identical tothat which we have observed (3, 4). This arrangement is notlike that seen in the thalamus or sensorimotor cortex. It iscrude at best and in PD one cell may respond to multiplejoints, which is probably not true in the normal state. AsHoover and Strick (1) have observed in monkeys, there maybe several somatotopic maps with different cortical projec-tions. We find that mapping of somatotopic features is quitehelpful for determining laterality. It is also useful for evalu-ating the effectiveness of lesioning. If we do not observe muchimprovement in the leg, we perform more medial lesioning. Thistype of information should be helpful to stereotactic neurosur-geons regardless of whether they use microelectrodes.
Anatomic versus electrophysiological localization techniquescontinues to be controversial. Regardless of published reportsdescribing anatomic versus electrophysiological variants, thevalue of microelectrodes remains unproven. Whether the sametype of corrections can be made with macrostimulation remainsvery difficult to ascertain. I think that microelectrodes are ex-tremely useful, but I have no proof. When performed by expe-rienced neurosurgeons, I think that macrostimulation alone maybe sufficient in the thalamus, where there are good electrophys-iological end points. For other targets, such as the pallidum,macrostimulation is much less useful and the importance of
microelectrodes emerges. The findings obtained using micro-electrode recording clearly help define the target and can yieldmore precise initial anatomic targeting (2).
I think that most investigators would agree that electro-physiological confirmation is useful. The ultimate anatomi-cally based lesioning method is radiosurgery, for whichthalamotomy and pallidotomy results have been mediocre.There has been one exception (5), but those results were onlyshort term (unbiased data were obtained for only 6 months)and were not as good as the best results obtained usingelectrophysiologically monitored lesioning, whether with mi-croelectrodes or macroelectrodes alone.
In summary, I think that the information obtained in thisstudy should be quite useful for all stereotactic neurosur-geons. Finally, I strongly agree with the authors that, in ad-dition to a randomized trial, long-term comprehensive eval-uation of patients is essential for assessment of the relativemerits of these techniques.
Roy A.E. BakayAtlanta, Georgia
1. Hoover JE, Strick PL: Multiple output channels in the basal gan-glia. Science 259:819–821, 1993.
2. Starr PA, Vitek JL, DeLong M, Bakay RAE: Magnetic resonanceimaging-based stereotactic localization of the globus pallidus andsubthalamic nucleus. Neurosurgery 44:303–314, 1999.
3. Vitek JL, Bakay RAE, DeLong MR: Microelectrode-guided pal-lidotomy for medically intractable Parkinson’s disease. AdvNeurol 74:183–198, 1997.
4. Vitek JL, Bakay RAE, Hashimoto T, Kaneoke Y, Mewes K, ZhangJY, Rye D, Starr PA, Baron MS, Turner RS, DeLong MR:Microelectrode-guided pallidotomy: Technical approach and itsapplication in medically intractable Parkinson’s disease. J Neuro-surg 88:1027–1043, 1998.
5. Young RE, Shumway-Cook A, Vermeulen SS, Grimm P, BlaskoJB, Posewitz A, Burkhart WA, Goiney RC: Gamma knife radio-surgery as a lesioning technique in movement disorder surgery.J Neurosurg 89:183–193, 1998.
The article summarizes a single-center experience involv-ing the treatment of 50 patients with advanced PD who un-derwent unilateral stereotactic pallidotomy. The target foreach lesion was chosen using stereotactic MRI and was thenrefined using intraoperative microrecording. The authorsshowed that the difference between the initial MRI target andthe final lesion location varied between 4 and 8 mm in eachdirection. Only 45% of all patients experienced overlap be-tween the MRI target and the actual lesion, which is very closeto the recently published results of Tsao et al. (4), in which52% of hypothetical lesions were found to be outside theglobus pallidus.
These results are similar to the findings of our group andseveral other groups (1–4). They confirm the usefulness andimportance of intraoperative microrecording in the delinea-tion of major surrounding structures and the selection of thefinal target location. The authors also present a review of theirfindings on the somatotopic representation of the GPi. Unfor-tunately, the GPi is not divided into separate sections that are
288 Guridi et al.
Neurosurgery, Vol. 45, No. 2, August 1999

responsible for various parts of the body; instead, these areasare overlapping and interwoven. However, surgeons may aimmore laterally and ventrally for arm targeting and more me-dially and dorsally for leg targeting. Whether improved res-olution of MRI scanners and/or the use of intraoperativeimaging for target confirmation will eventually decrease oreliminate the need for microrecording is not clear. The issue ofindividual variability cannot be ignored.
Kim J. BurchielKonstantin SlavinPortland, Oregon
1. Iacono RP, Shima F, Lonser RR, Kuniyoshi S, Maeda G, YamadaS: The results, indications, and physiology of posteroventral pal-lidotomy for patients with Parkinson’s disease. Neurosurgery36:1118–1127, 1995.
2. Sutton JP, Couldwell W, Lew MF, Mallory L, Grafton S,DeGiorgio C, Welsh M, Apuzzo MLJ, Ahmadi J, Waters CH:Ventroposterior medial pallidotomy in patients with advancedParkinson’s disease. Neurosurgery 36:1112–1117, 1995.
3. Taha JM, Favre J, Baumann TK, Burchiel KJ: Tremor control afterpallidotomy in patients with Parkinson’s disease: Correlationwith microrecording findings. J Neurosurg 86:642–647, 1997.
4. Tsao K, Wilkinson S, Overman WC, Batnitzky S, Gordon MA:Pallidotomy lesion locations: Significance of microelectrode re-finement. Neurosurgery 43:506–513, 1998.
Guridi et al. present a study of 50 patients who underwentmicroelectrode recording-guided pallidotomy. The value ofthe study is twofold; it relates the imaging-derived target tothe final electrophysiologically determined target and it ad-dresses the issue of somatotopy in the globus pallidus. Both ofthese issues are directly relevant to the performance of pal-lidotomy and, ultimately, to the outcome of this procedure.
The results the authors present emphasize that the use ofimaging alone for localization is insufficient. On the basis oftheir recordings, the authors needed to adjust their pal-lidotomy targets to optimize the lesioning and to avoid inap-propriate lesion placement. Their analysis of the somatotopyof kinesthetic representation in the GPi is quite interesting.Although there are data regarding the somatotopic represen-tation in the GPi of normal primates, analysis of somatotopyin the GPi in the parkinsonian state (for example, in the1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine model) has notbeen performed. As described by Filion et al. (1), the issue ofGPi somatotopy in the dopamine-deficient state is quite com-plex. Pallidal neurons in PD respond to multiple joints ratherthan single joints, the responses are exaggerated, and severalneurons adopt reciprocal responses, i.e., they become excitedin one direction and inhibited in the opposite direction. Ad-ditional neurons may respond to both ipsilateral and con-tralateral limb movements, as reported for patients with PDby Lozano et al. (4). This is perhaps the underlying basis for
the bilateral improvements seen after pallidotomy or pallidalstimulation.
Another important finding concerning GPi organization isthat the GPi is parceled along functional territories, and eventhe motor circuit is further subdivided in subcircuits. Thework of Hoover and Strick (3) has shown that there aremultiple motor representations in the pallidum, correspond-ing to pallidal outflow to various motor areas, including thesupplementary motor area, the premotor area, the motor cor-tex, and the dorsolateral prefrontal cortex. There is somato-topic representation within each of these subcircuits. Thissuggests that there are multiple clusters of somatotopy thatare concatenated within the GPi, rather than general areas forthe arm, leg, and face, as Guridi et al. suggest. In addition,because in the parkinsonian state (at least in primates) defo-cusing of receptive fields and exaggerated responses are ob-served, it is unlikely that the GPi of patients with PD has suchdiscrete arm, leg, and face areas as the authors suggest. Nev-ertheless, the somatotopic model in PD and the multiplerepresentation of motor subcircuits lead us to several testablehypotheses. It could be predicted that, if somatotopy is indeedfunctionally relevant, then discrete lesions within the palli-dum might provide benefit to one limb or one body part andnot others. Additional lesions in a motor subcircuit mightimprove some aspects of parkinsonian disability and not oth-ers. Indeed, recent work by Gross et al. (2) suggests thatcertain parkinsonian features respond differentially as a func-tion of the location of the pallidotomy lesion within the GPi.Not all pallidotomies are equal.
The main points of this work are that there is still much tolearn regarding the functions and organization of the globuspallidus and that imaging is an important component of lo-calization but is currently insufficient for determining theultimate target. It is only when the imaging results are con-gruent with physiological features and functional findingsthat functional neurosurgeons can be confident that localiza-tion is optimal.
Andres M. LozanoToronto, Ontario, Canada
1. Filion M, Tremblay L, Bedard PJ: Abnormal influences of passivelimb movement on the activity of globus pallidus neurons inparkinsonian monkeys. Brain Res 444:165–176, 1988.
2. Gross RE, Lombardi WJ, Lang AE, Duff J, Hutchison WD, Saint-Cyr JA, Tasker RR, Lozano AM: Relationship of lesion location toclinical outcome following microelectrode-guided pallidotomyfor Parkinson’s disease. Brain 122:405–416, 1999.
3. Hoover JE, Strick PL: Multiple output channels in the basal gan-glia. Science 259:819–821, 1993.
4. Lozano AM, Hutchison WD, Kiss ZHT, Tasker RR, Davis KD,Dostrovsky JO: Methods for microelectrode-guided posteroventralpallidotomy. J Neurosurg 84:194–202, 1996.
Targeting the Internal Pallidum in Parkinson’s Disease 289
Neurosurgery, Vol. 45, No. 2, August 1999