
STATEMENT 5
38
APAGE Working Party on Diagnosis, Genetic, Epidemiology Management and Surgical Perspective of Crohn's Disease in Asia Pacific
-
Upload
benjamin-stewart -
Category
Documents
-
view
28 -
download
0
description
APAGE Working Party on Diagnosis, Genetic, Epidemiology Management and Surgical Perspective of Crohn's Disease in Asia Pacific. STATEMENT 5. - PowerPoint PPT Presentation
Transcript of STATEMENT 5

APAGE Working Party on Diagnosis,
Genetic, Epidemiology Management and Surgical
Perspective of Crohn's Disease in Asia Pacific
STATEMENT 5
• There is considerable variation in the distribution of disease location for Crohn's disease although within East Asia, combined small and large bowel predominates
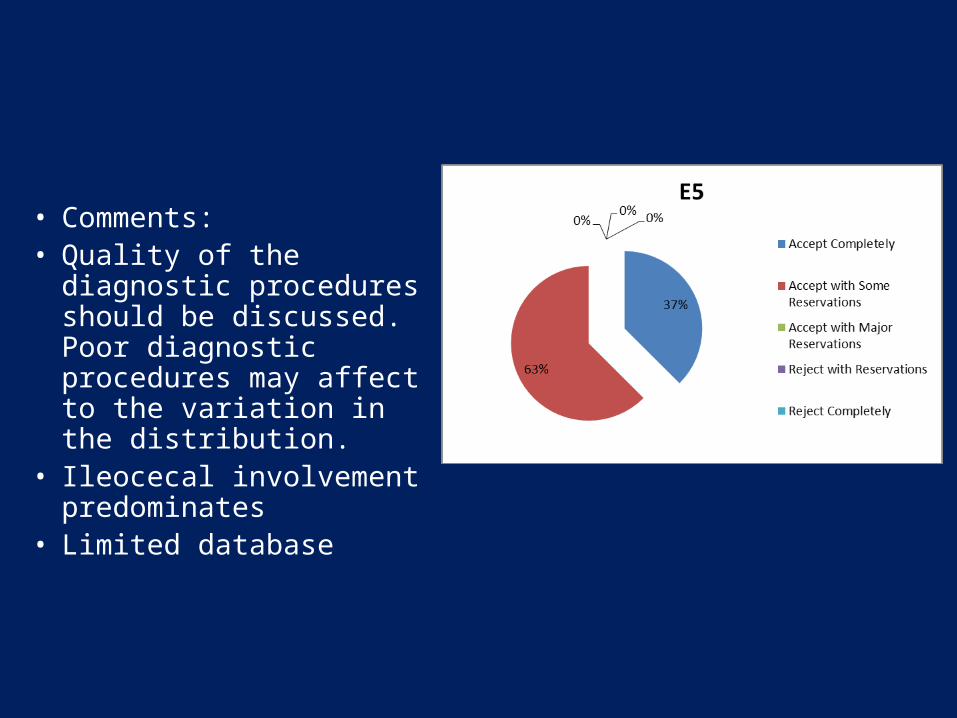
• Comments:• Quality of the diagnostic
procedures should be discussed. Poor diagnostic procedures may affect to the variation in the distribution.
• Ileocecal involvement predominates
• Limited database
Problems in identifying disease location in CD
• Different classifications used (none/Vienna/ Montreal)
• Objective upper GI and small bowel assessment not carried in all patients
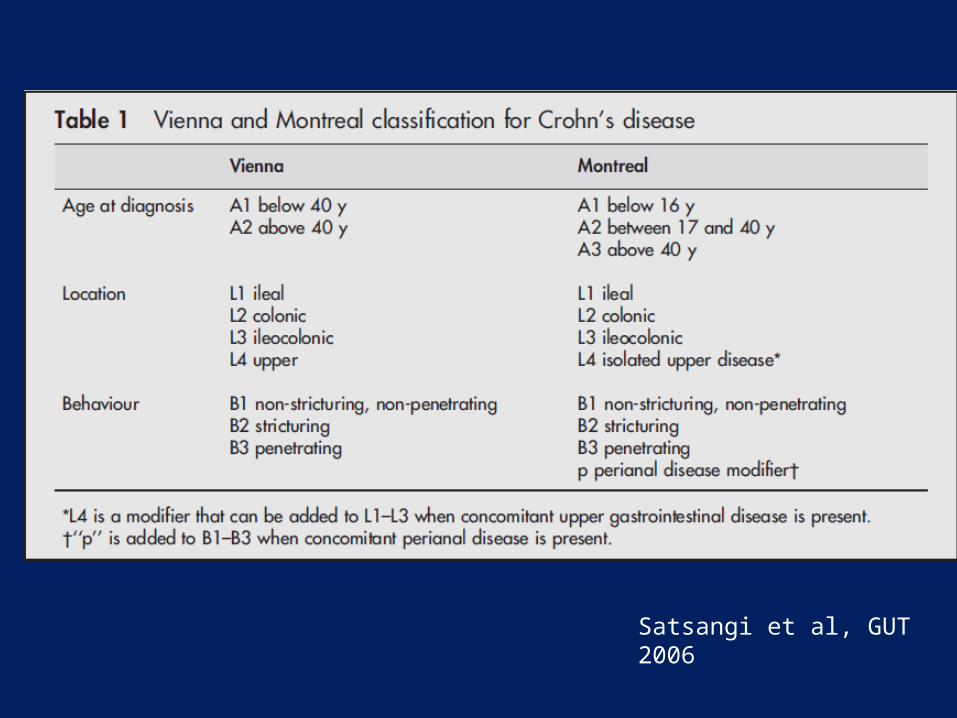
Satsangi et al, GUT 2006
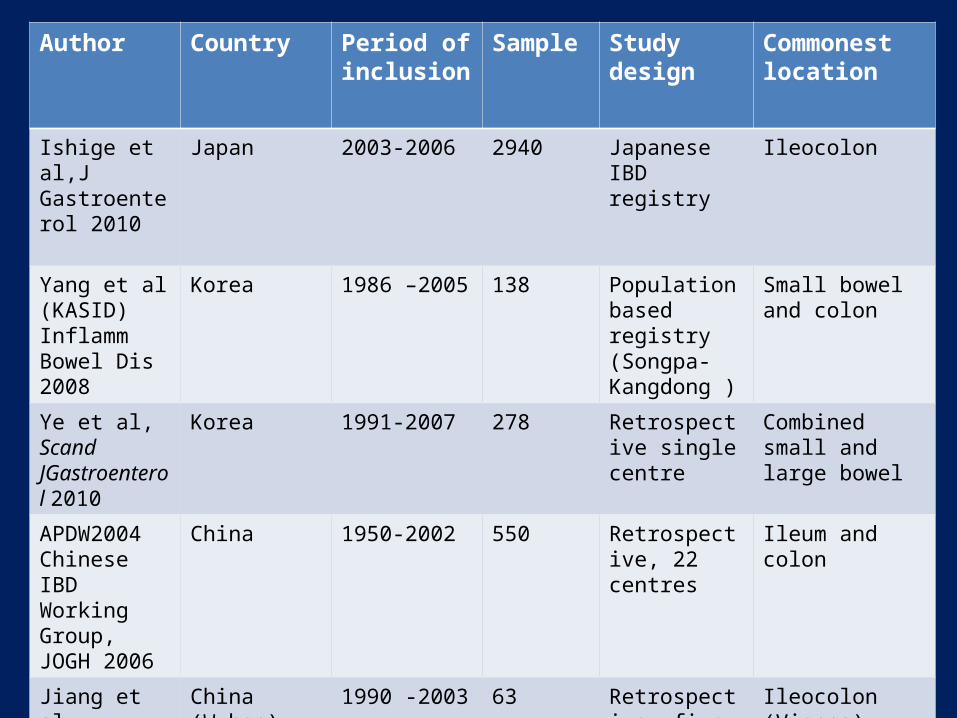
Author Country Period of inclusion
Sample Study design Commonest location
Ishige et al,J Gastroenterol 2010
Japan 2003-2006 2940 Japanese IBD registry
Ileocolon
Yang et al (KASID) Inflamm Bowel Dis 2008
Korea 1986 –2005 138 Population based registry (Songpa-Kangdong )
Small bowel and colon
Ye et al, Scand JGastroenterol 2010
Korea 1991-2007 278 Retrospective single centre
Combined small and large bowel
APDW2004 Chinese IBD Working Group, JOGH 2006
China 1950-2002 550 Retrospective, 22 centres
Ileum and colon
Jiang et al, Inflamm Bowel Dis 2006
China (Wuhan) 1990 -2003 63 Retrospective, five centres
Ileocolon (Vienna)
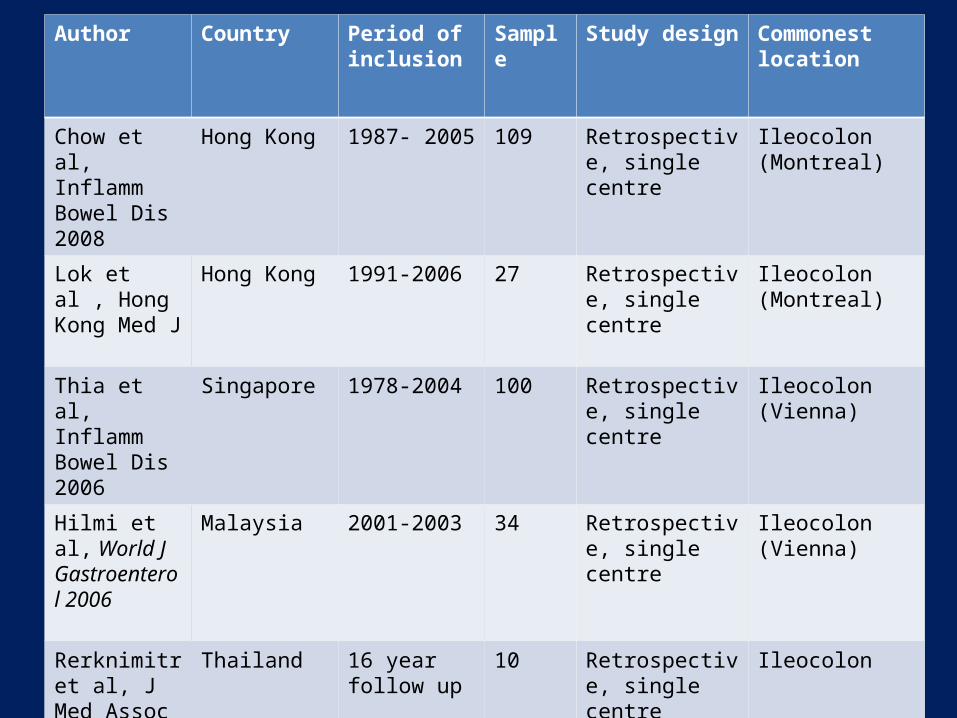
Author Country Period of inclusion
Sample Study design Commonest location
Chow et al, Inflamm Bowel Dis 2008
Hong Kong 1987- 2005 109 Retrospective, single centre
Ileocolon (Montreal)
Lok et al , Hong Kong Med J
Hong Kong 1991-2006 27 Retrospective, single centre
Ileocolon(Montreal)
Thia et al,Inflamm Bowel Dis 2006
Singapore 1978-2004 100 Retrospective, single centre
Ileocolon (Vienna)
Hilmi et al, World J Gastroenterol 2006
Malaysia 2001-2003 34 Retrospective, single centre
Ileocolon (Vienna)
Rerknimitr et al, J Med Assoc Thai 2005
Thailand 16 year follow up
10 Retrospective, single centre
Ileocolon

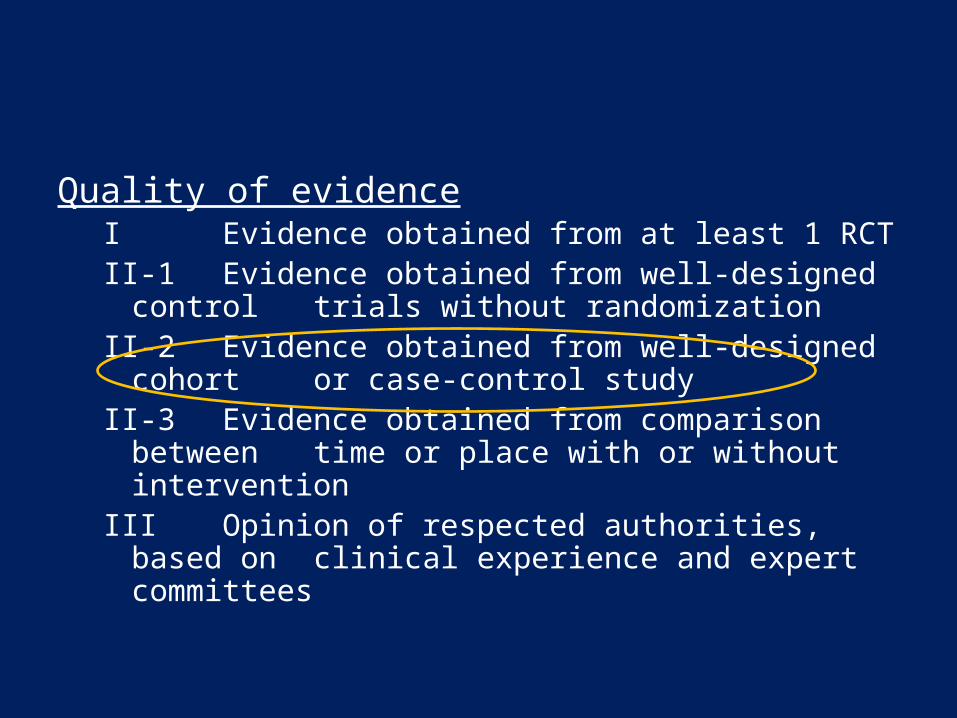
Quality of evidenceI Evidence obtained from at least 1 RCTII-1 Evidence obtained from well-designed control
trials without randomizationII-2 Evidence obtained from well-designed cohort
or case-control studyII-3 Evidence obtained from comparison between
time or place with or without interventionIII Opinion of respected authorities, based on
clinical experience and expert committees

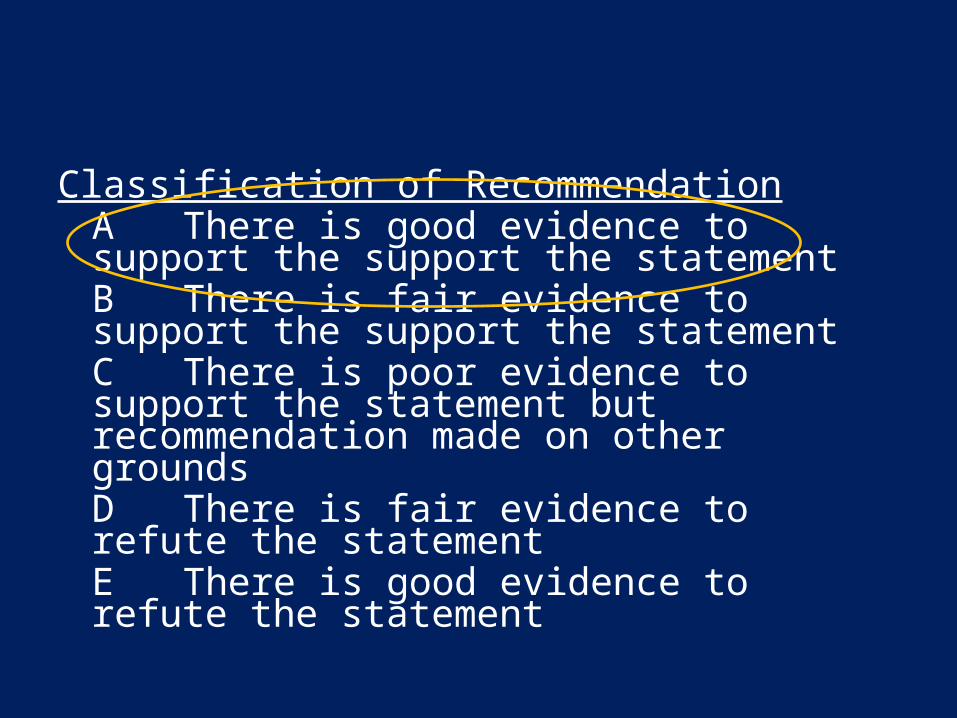
Classification of RecommendationA There is good evidence to support the support the statementB There is fair evidence to support the support the statementC There is poor evidence to support the statement but recommendation made on other groundsD There is fair evidence to refute the statement E There is good evidence to refute the statement

Suggested modification• Although there is considerable variation in the
distribution of disease location for Crohn's disease within Asia, the commonest disease location is ileocolonic.
Statement 6
• Similar to Western population, Crohn 's patients in the Asia-Pacific have a tendency towards progression of intestinal complications such as strictures and fistulas with time.
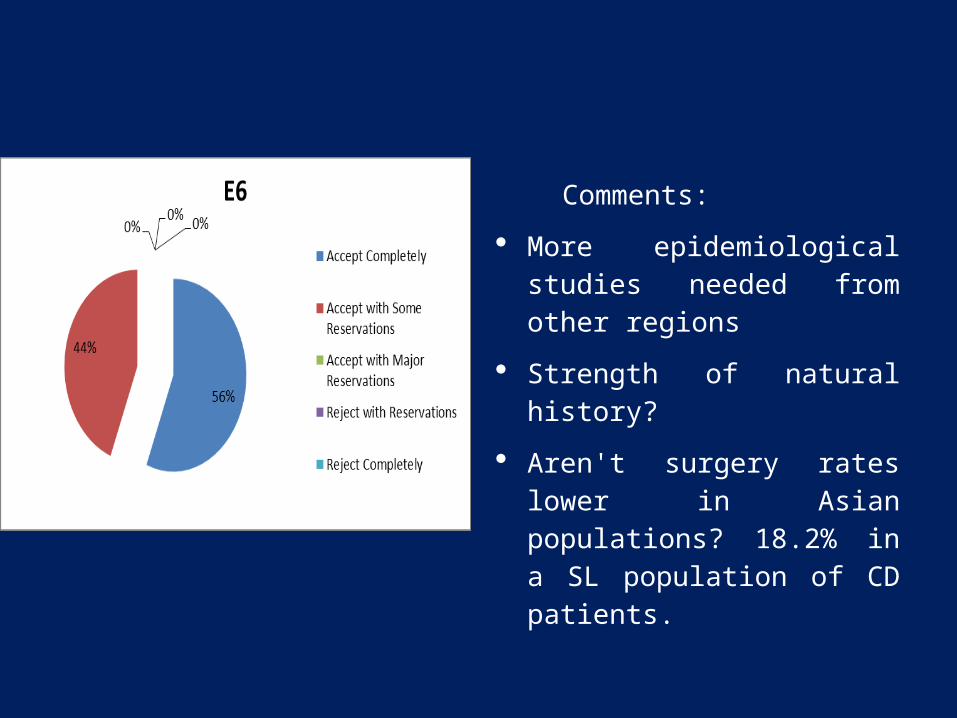
Comments:
More epidemiological studies needed from other regions
Strength of natural history?
Aren't surgery rates lower in Asian populations? 18.2% in a SL population of CD patients.

Disease behaviour
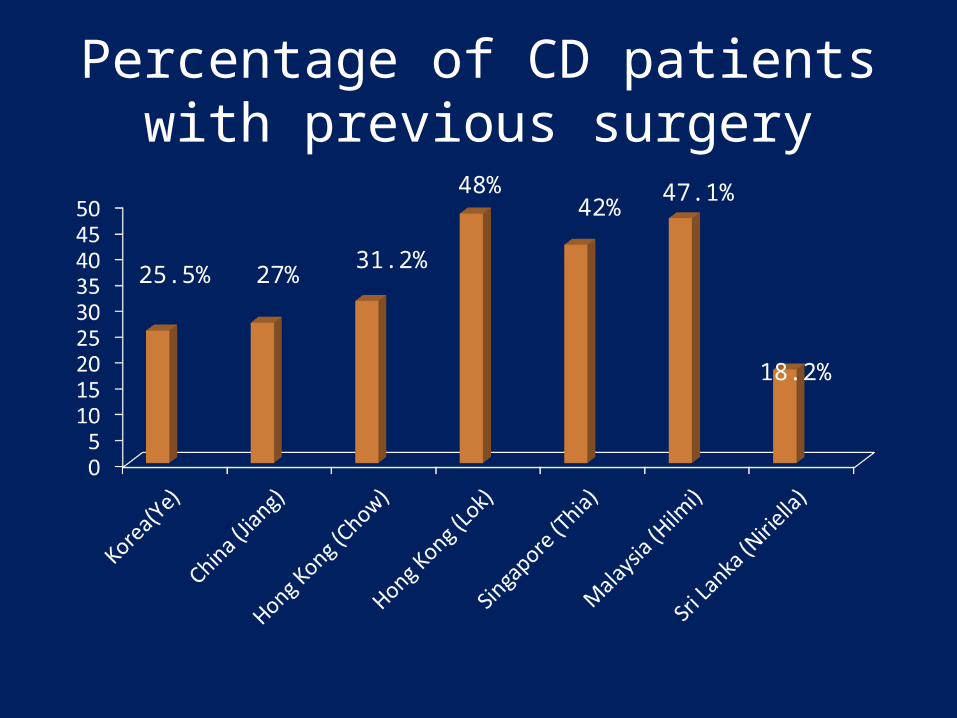
Percentage of CD patients with previous surgery
25.5% 27%31.2%
48%42%
47.1%
18.2%

31.3% 50.7%
Ye et al, Scand J Gastroenterol. 2010
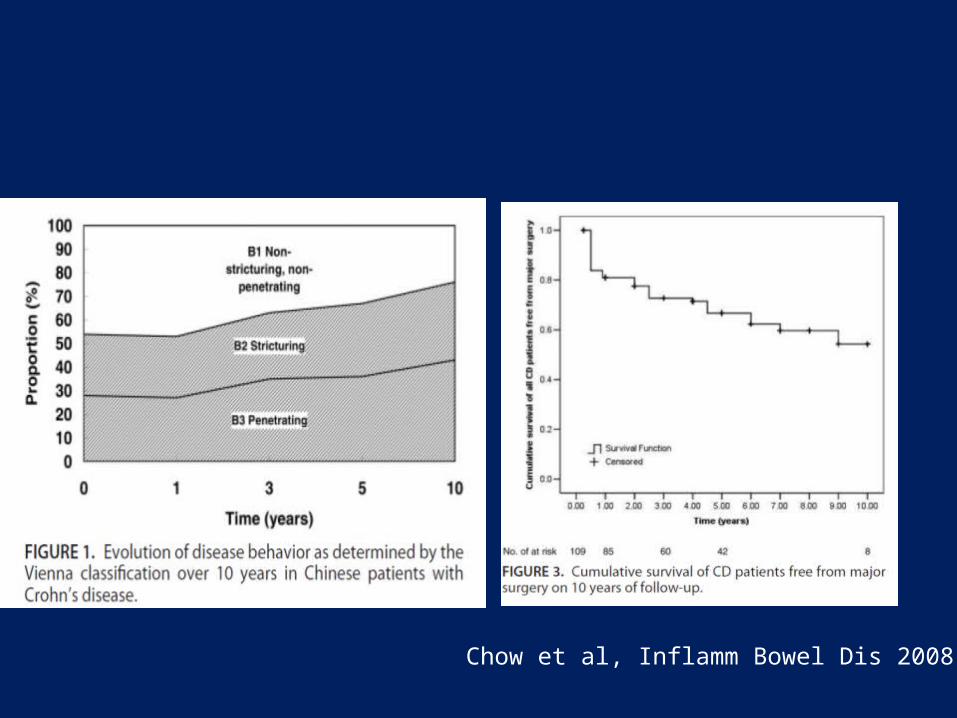
Chow et al, Inflamm Bowel Dis 2008
Quality of evidenceI Evidence obtained from at least 1 RCTII-1 Evidence obtained from well-designed control
trials without randomizationII-2 Evidence obtained from well-designed cohort
or case-control studyII-3 Evidence obtained from comparison between
time or place with or without interventionIII Opinion of respected authorities, based on
clinical experience and expert committees
Classification of RecommendationA There is good evidence to support the support the statementB There is fair evidence to support the support the statementC There is poor evidence to support the statement but recommendation made on other groundsD There is fair evidence to refute the statement E There is good evidence to refute the statement
Statement 7
• A positive family history of IBD is uncommon among Crohn's disease patients and is likely to be related to a low prevalence of IBD in the region
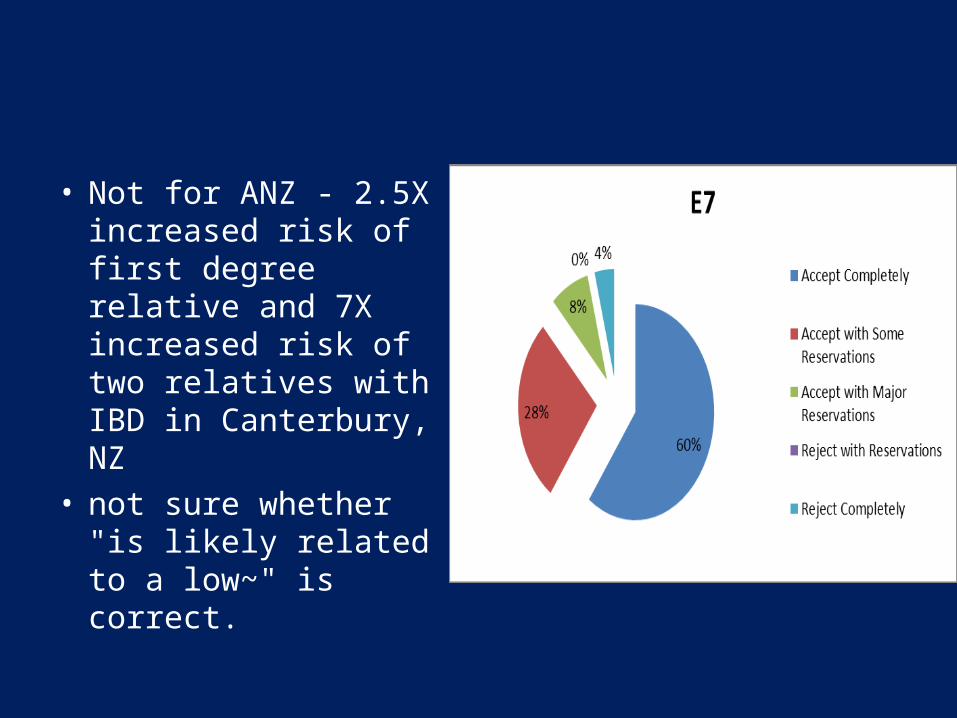
• Not for ANZ - 2.5X increased risk of first degree relative and 7X increased risk of two relatives with IBD in Canterbury, NZ
• not sure whether "is likely related to a low~" is correct.
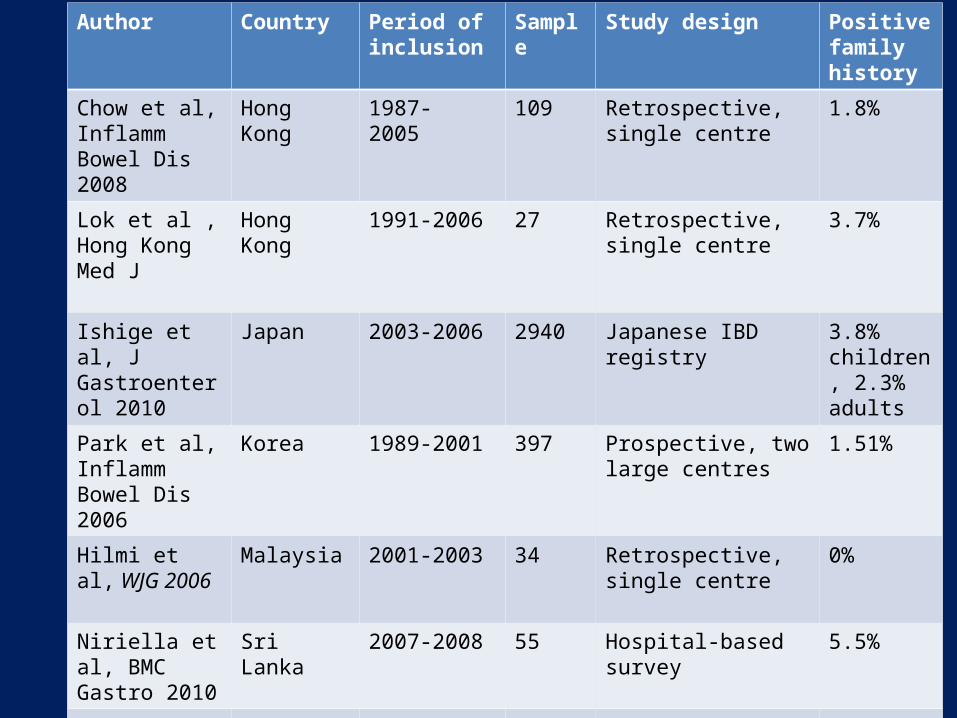
Author Country Period of inclusion
Sample Study design Positive family history
Chow et al, Inflamm Bowel Dis 2008
Hong Kong 1987- 2005 109 Retrospective, single centre
1.8%
Lok et al , Hong Kong Med J
Hong Kong 1991-2006 27 Retrospective, single centre
3.7%
Ishige et al, J Gastroenterol 2010
Japan 2003-2006 2940 Japanese IBD registry 3.8% children, 2.3% adults
Park et al, Inflamm Bowel Dis 2006
Korea 1989-2001 397 Prospective, two large centres
1.51%
Hilmi et al, WJG 2006
Malaysia 2001-2003 34 Retrospective, single centre
0%
Niriella et al, BMC Gastro 2010
Sri Lanka 2007-2008 55 Hospital-based survey 5.5%
Gearry et al,JOGH 2010
New Zealand
2003-2005 638 Prospective population based study case control study
34.8%
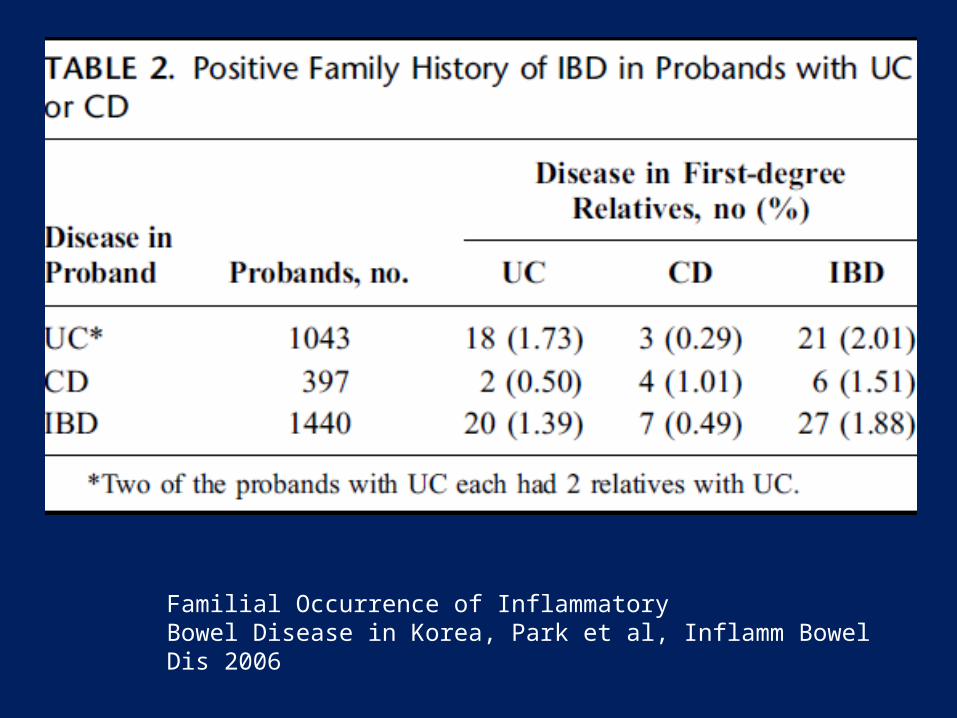
Familial Occurrence of InflammatoryBowel Disease in Korea, Park et al, Inflamm Bowel Dis 2006

Familial Occurrence of InflammatoryBowel Disease in Korea, Park et al, Inflamm Bowel Dis 2006
Quality of evidenceI Evidence obtained from at least 1 RCTII-1 Evidence obtained from well-designed control
trials without randomizationII-2 Evidence obtained from well-designed cohort
or case-control studyII-3 Evidence obtained from comparison between
time or place with or without interventionIII Opinion of respected authorities, based on
clinical experience and expert committees
Classification of RecommendationA There is good evidence to support the support the statementB There is fair evidence to support the support the statementC There is poor evidence to support the statement but recommendation made on other groundsD There is fair evidence to refute the statement the statementE There is good evidence to refute the statement
Modified Statement 7
• A positive family history of IBD is uncommon among Crohn's disease patients in areas of low prevalence.

Proposed additional statements
Statement 8
• The cause for the increasing incidence and prevalence of CD in the Asia Pacific Region remains unknown. Environmental changes are likely to play a role.

• Minimal data available• A Japanese review suggested that prevalence
of CD and UC began to increase > 20 years after an increased daily consumption of dietary animal meat and fats, milk and dairy products, and after a decreased consumption of rice.
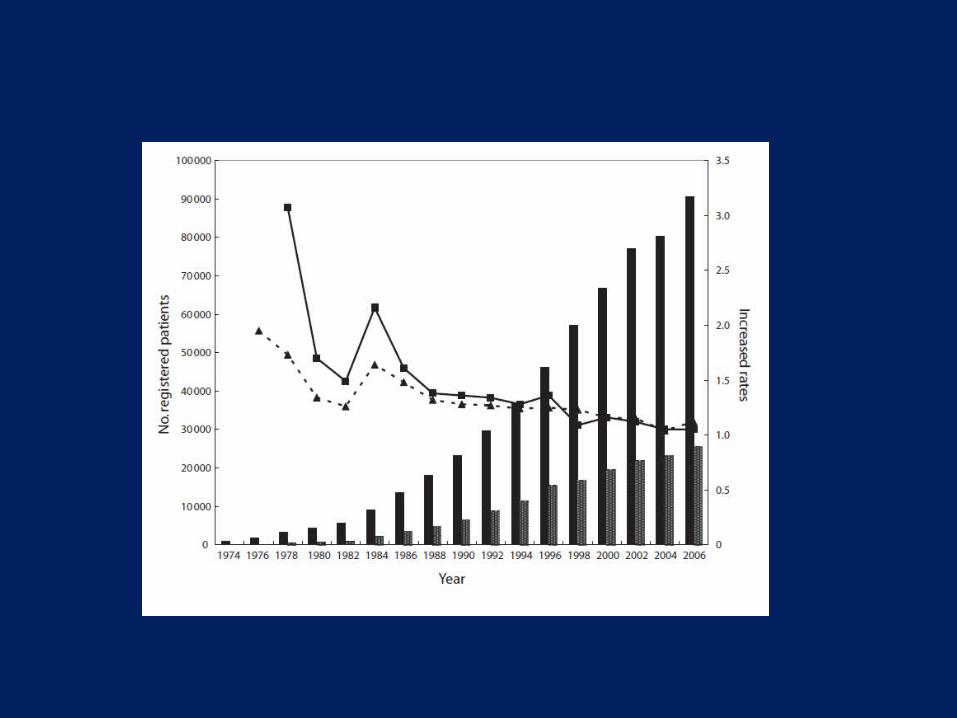

Asakura JOGH 2008
CD and the environment
• The New Zealand population study found• Positive association with– High social class at birth– City living
• Negative association with – History of being breastfed– Having a childhood vegetable garden

Quality of evidenceI Evidence obtained from at least 1 RCTII-1 Evidence obtained from well-designed control
trials without randomizationII-2 Evidence obtained from well-designed cohort
or case-control studyII-3 Evidence obtained from comparison between
time or place with or without interventionIII Opinion of respected authorities, based on
clinical experience and expert committees
Classification of RecommendationA There is good evidence to support the support the statementB There is fair evidence to support the support the statementC There is poor evidence to support the statement but recommendation made on other groundsD There is fair evidence to refute the statement E There is good evidence to refute the statement
Statement 9
• Smoking has been shown to be positively associated with CD in New Zealand but in other parts of the Asia Pacific region, the role of smoking has not been determined

• Very little data on smoking and CD available in the Asia Pacific region
• Population study in Canterbury, New Zealand (Gearry et al) found cigarette smoking at diagnosis was positively associated with CD OR 1.99; 95% CI:1.48–2.68
• Leong et al found that among Chinese patients, ex-smokers, but not current smokers or previous and current smokers combined were at greater risk of developing CD
• Another study by Leong et al found that current or previous smoking protected against the development of granulomas (OR: 0.16; 95% CI: 0.04-0.59)
Quality of evidenceI Evidence obtained from at least 1 RCTII-1 Evidence obtained from well-designed control
trials without randomizationII-2 Evidence obtained from well-designed cohort
or case-control studyII-3 Evidence obtained from comparison between
time or place with or without interventionIII Opinion of respected authorities, based on
clinical experience and expert committees
Classification of RecommendationA There is good evidence to support the support the statementB There is fair evidence to support the support the statementC There is poor evidence to support the statement but recommendation made on other groundsD There is fair evidence to refute the statement E There is good evidence to refute the statement


















