STATE SURVEILLANCE UNIT, INTEGRATED DISEASE SURVEILLANCE ... · PDF fileINTEGRATED DISEASE...
59
STATE SURVEILLANCE UNIT, INTEGRATED DISEASE SURVEILLANCE PROGRAMME, PUBLIC HEALTH & COMMUNICABLE DISEASES BRANCH, DIRECTORATE OF HEALTH SERVICES, GOVT. OF WEST BENGAL.
Transcript of STATE SURVEILLANCE UNIT, INTEGRATED DISEASE SURVEILLANCE ... · PDF fileINTEGRATED DISEASE...
STATE SURVEILLANCE UNIT,
INTEGRATED DISEASE SURVEILLANCE PROGRAMME,
PUBLIC HEALTH & COMMUNICABLE DISEASES BRANCH,
DIRECTORATE OF HEALTH SERVICES,
GOVT. OF WEST BENGAL.
This set of slides is a guideline on surveillance, prevention & control ofanthrax, that is issued from the State Surveillance Unit of I.D.S.P., WestBengal. The slides, on one hand, briefly describe the epidemiology and themodes of transmission and outbreak control measures, that may interest apublic health manager.
On the other hand, these slides deal with the basics of diagnosis & casemanagement (including prophylaxis), that would be quite relevant for theMedical Officers.
1. Causative Agent of Anthrax
2. Epidemiology of Anthrax
3. Transmission and Pathogenesis
4. Clinical Signs of Anthrax
5. Case Management
6. Case Definition
7. Specimen to Collect
8. Prevention and Control/Action to be taken during Anthrax outbreak
9. Anthrax Surveillance System
CONTENT
CAUSATIVE AGENT OF ANTHRAX
Anthrax is also known as Malignant pustule, Malignant oedema, Wool sorter's
disease.
In West Bengal known as ‘TARKA’ in animal.
One of the oldest recorded disease of animals.
Primarily a disease of herbivorous animals (cattle, sheep, goats horses and wild
herbivores).
Occasionally affects human (incidental).
First disease of humans and other animals in which the causative agent was
definitely demonstrated as a specific microorganism by the French biologist
Casimir-Joseph Davaine in 1863 and by the German bacteriologist Robert Koch
in 1876 who isolated the organism in pure culture.
WHAT IS ANTHRAX
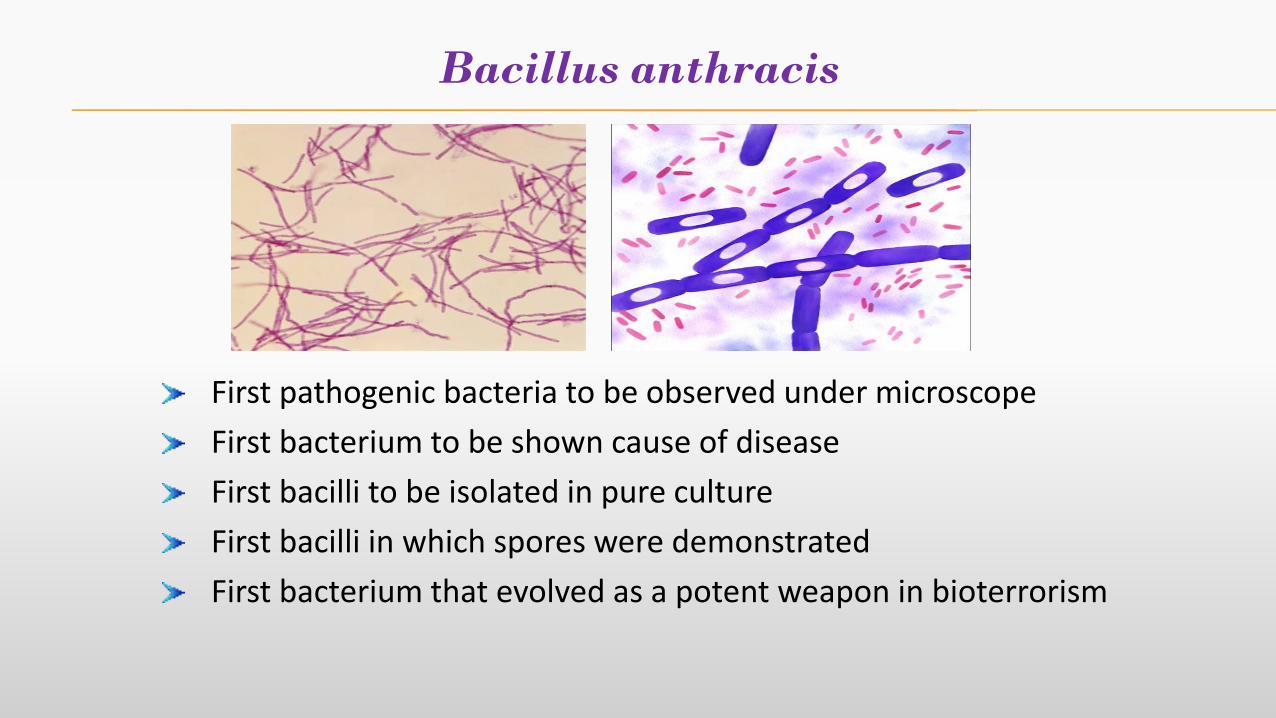
Bacillus anthracis
First pathogenic bacteria to be observed under microscope
First bacterium to be shown cause of disease
First bacilli to be isolated in pure culture
First bacilli in which spores were demonstrated
First bacterium that evolved as a potent weapon in bioterrorism
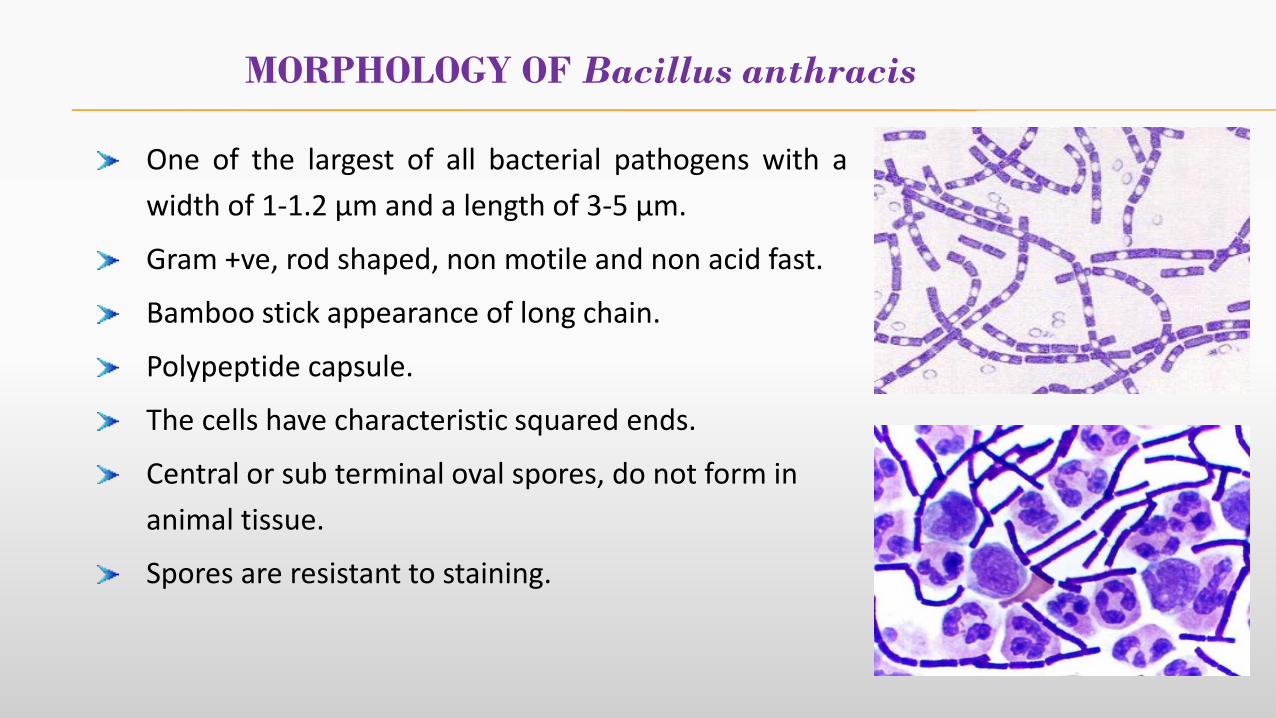
MORPHOLOGY OF Bacillus anthracis
One of the largest of all bacterial pathogens with a
width of 1-1.2 μm and a length of 3-5 μm.
Gram +ve, rod shaped, non motile and non acid fast.
Bamboo stick appearance of long chain.
Polypeptide capsule.
The cells have characteristic squared ends.
Central or sub terminal oval spores, do not form in
animal tissue.
Spores are resistant to staining.
Moist heat kills – Vegetative cells at 60 0 C X 30 minutes
Spores at 100 0 C X 10 minutes
Spores are also killed by - 5% Formaldehyde
- 4% KMnO4
- Hypochlorite ( 0.5%)
PHYSICAL PROPERTIES OF B. anthracis
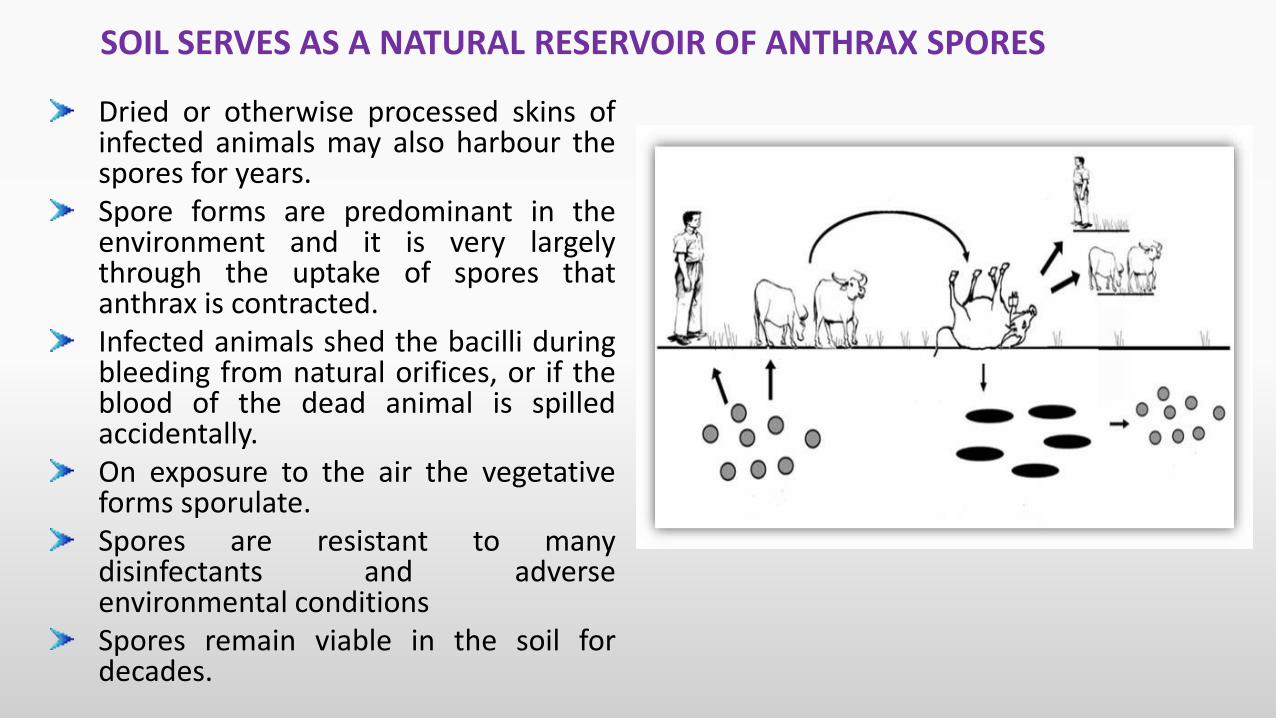
Dried or otherwise processed skins ofinfected animals may also harbour thespores for years.Spore forms are predominant in theenvironment and it is very largelythrough the uptake of spores thatanthrax is contracted.Infected animals shed the bacilli duringbleeding from natural orifices, or if theblood of the dead animal is spilledaccidentally.On exposure to the air the vegetativeforms sporulate.Spores are resistant to manydisinfectants and adverseenvironmental conditionsSpores remain viable in the soil fordecades.
SOIL SERVES AS A NATURAL RESERVOIR OF ANTHRAX SPORES
EPIDEMIOLOGY OF ANTHRAX
Distribution worldwide.
Most common in agricultural regions where it occurs in animals.
These include South and Central Americas, Southern and Eastern Europe, Africa,
the Caribbean, Middle East & Asia (China, Pakistan, India).
Human to human or animal to animal transmission is rare.
Grazing animals become infected through ingestion of spores in soil (carcasses are
usually the source).
Epidemic : A. Spread to contiguous geographic areas - by infected animalB. Spread to non-contiguous geographic areas by
- Biting flies- Vultures- Contaminated surface water pool
EPIDEMIOLOGY
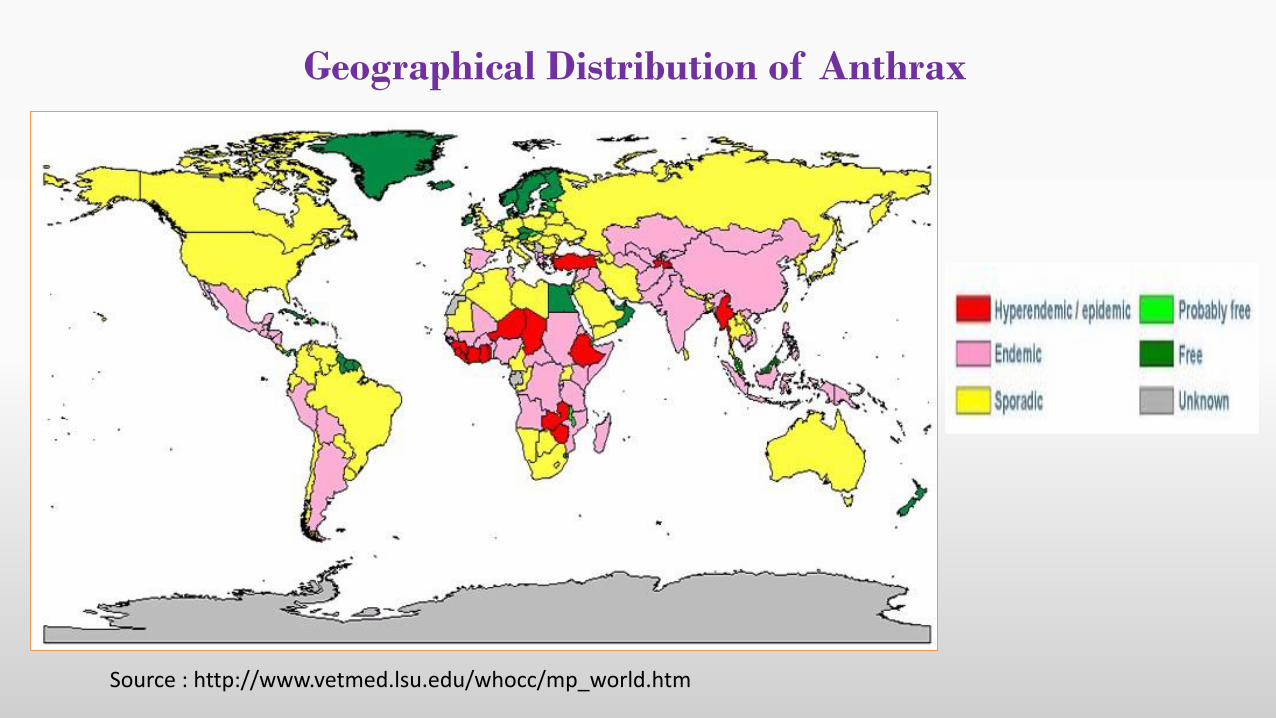
Geographical Distribution of Anthrax
Source : http://www.vetmed.lsu.edu/whocc/mp_world.htm
Year District
No. of
outbreak
No. of cases
in outbreaks
No. of deaths
in outbreaks C.F.R. (%)
2015
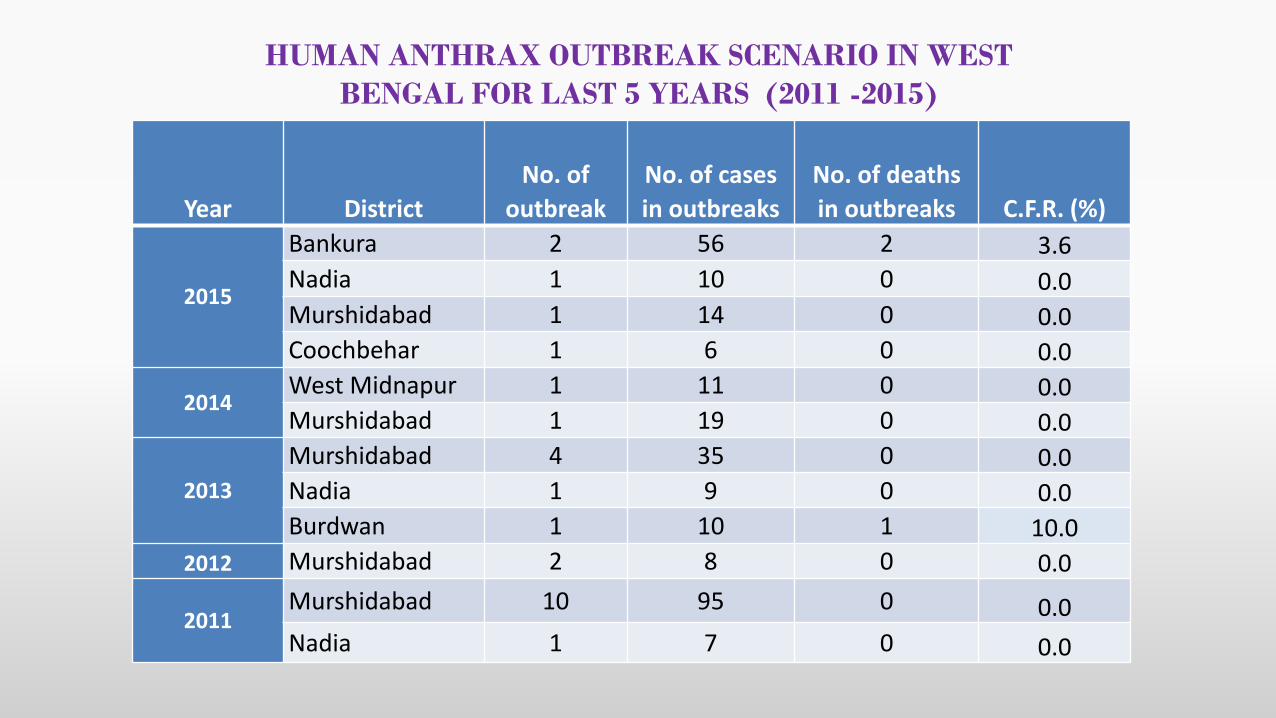
Bankura 2 56 2 3.6
Nadia 1 10 0 0.0Murshidabad 1 14 0 0.0Coochbehar 1 6 0 0.0
2014West Midnapur 1 11 0 0.0Murshidabad 1 19 0 0.0
2013
Murshidabad 4 35 0 0.0Nadia 1 9 0 0.0Burdwan 1 10 1 10.0
2012 Murshidabad 2 8 0 0.0
2011Murshidabad 10 95 0 0.0
Nadia 1 7 0 0.0
HUMAN ANTHRAX OUTBREAK SCENARIO IN WEST
BENGAL FOR LAST 5 YEARS (2011 -2015)
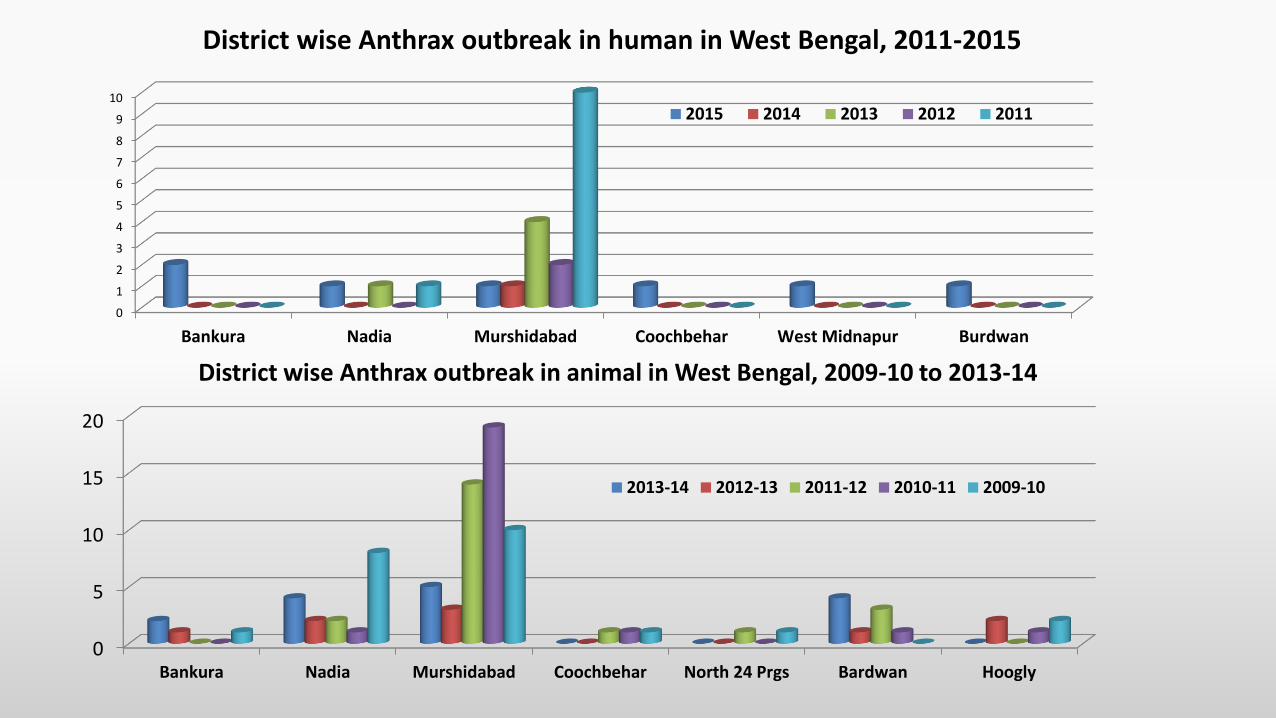
District wise Anthrax outbreak in human in West Bengal, 2011-2015
0
5
10
15
20
Bankura Nadia Murshidabad Coochbehar North 24 Prgs Bardwan Hoogly
2013-14 2012-13 2011-12 2010-11 2009-10
0
1
2
3
4
5
6
7
8
9
10
Bankura Nadia Murshidabad Coochbehar West Midnapur Burdwan
2015 2014 2013 2012 2011
District wise Anthrax outbreak in animal in West Bengal, 2009-10 to 2013-14
TRANSMISSION AND PATHOGENESIS
Animal1. Ingestion – Most common
Contaminated soil or feeds.
Heavy rain, drought.
Omnivores and carnivores through contaminatedmeat, bone meal and other feeds
Among wild life from feeding on anthraxcarcasses.
TRANSMISSION
2. Inhalation : Least common3. Cutaneous :
Mechanical (insect bite)Vultures have been reported to spread the organism from one area to another.
Incubation period in the susceptible herbivore ranges from 1 to 14 days.
1. Cutaneous anthrax :
After exposure to infected animals and contaminated animalproducts such as hair, hides, wool, bones, or skin.
Biting fly from infected animal.
2. Inhalation anthrax :
Inhalation of spores. Aerosols of such particles may be createdby the agitation of the hair or wool in the industry settings.
3. Intestinal anthrax :
Results from ingestion of contaminated meat.
Incubation period - few hours to 7 days.
Most cutaneous anthrax (by biting flies) occur within 48 hours of exposure
TRANSMISSION…(Cont’d)
Human
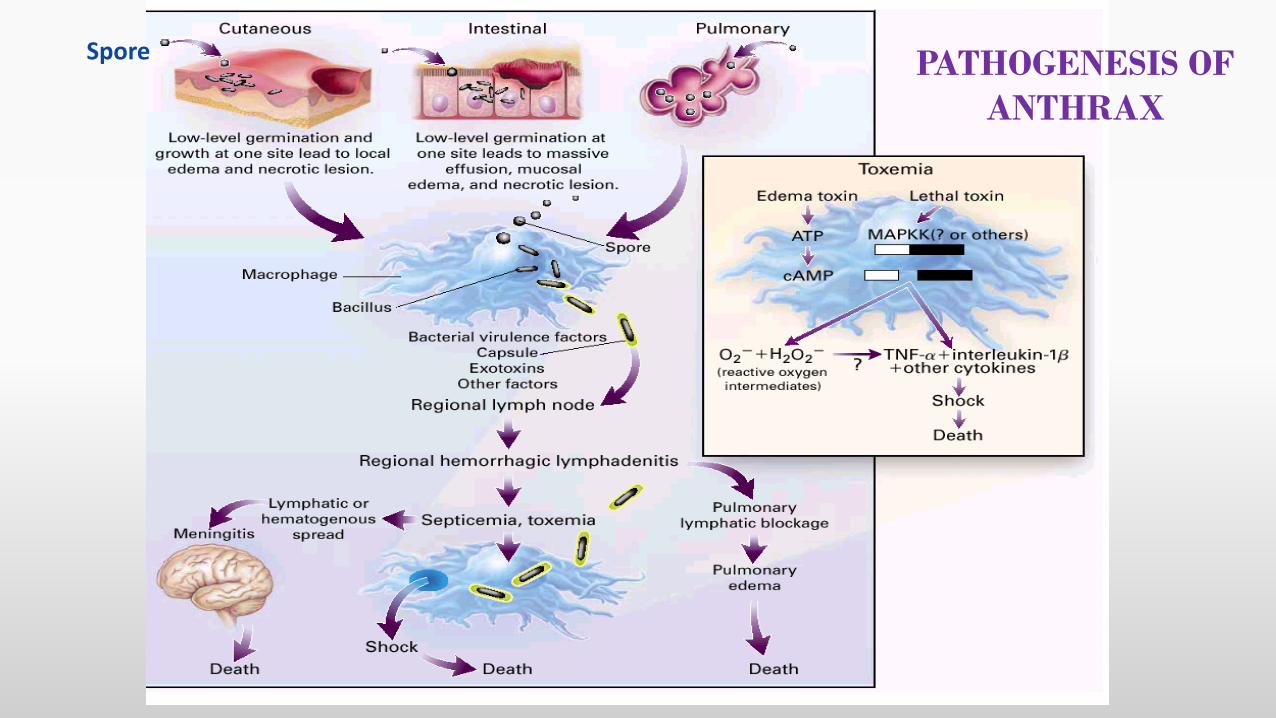
Spore PATHOGENESIS OF
ANTHRAX
CLINICAL SIGNS OF ANTHRAX
Many species of animal affected
Ruminants at greatest risk
Three forms in animal
1) Per acute
Cattle, sheep, goat, antelope
2) Acute
Ruminants & equine
3) Subacute-chronic
Swine, dogs, cats.
CLINICAL SIGNS OF ANTHRAX IN ANIMAL
CLINICAL SIGNS OF ANTHRAX IN ANIMAL…(Cont’d)
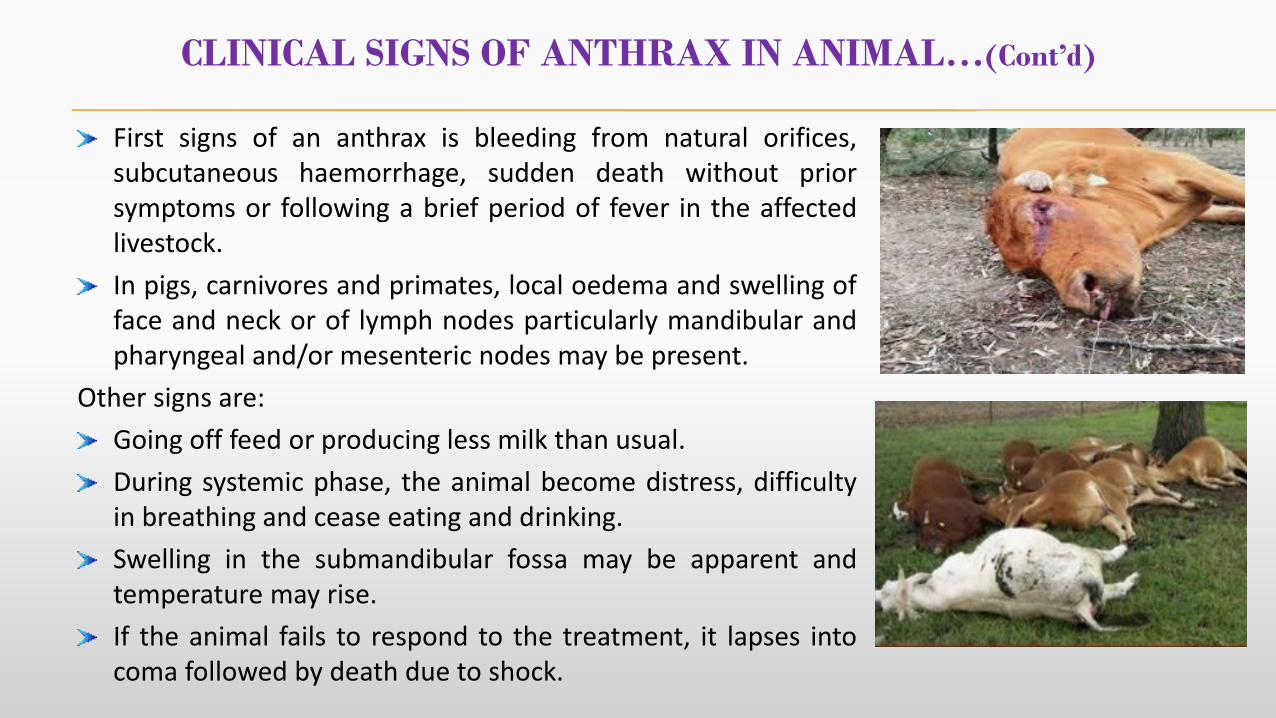
First signs of an anthrax is bleeding from natural orifices,subcutaneous haemorrhage, sudden death without priorsymptoms or following a brief period of fever in the affectedlivestock.
In pigs, carnivores and primates, local oedema and swelling offace and neck or of lymph nodes particularly mandibular andpharyngeal and/or mesenteric nodes may be present.
Other signs are:
Going off feed or producing less milk than usual.
During systemic phase, the animal become distress, difficultyin breathing and cease eating and drinking.
Swelling in the submandibular fossa may be apparent andtemperature may rise.
If the animal fails to respond to the treatment, it lapses intocoma followed by death due to shock.
Clinically three forms of Human anthrax occurA. Cutaneous anthraxB. Inhalation anthraxC. Ingestion anthrax
Broadly can be classified into:
Non Industrial/Agricultural (through infected animals)Cutaneous anthrax intestinal anthrax
Industrial Anthrax (through animal products)Mostly through animal products (wool, hair, hides, bones) Likely to develop cutaneous and inhalation anthrax
CLINICAL SIGNS OF ANTHRAX IN HUMAN
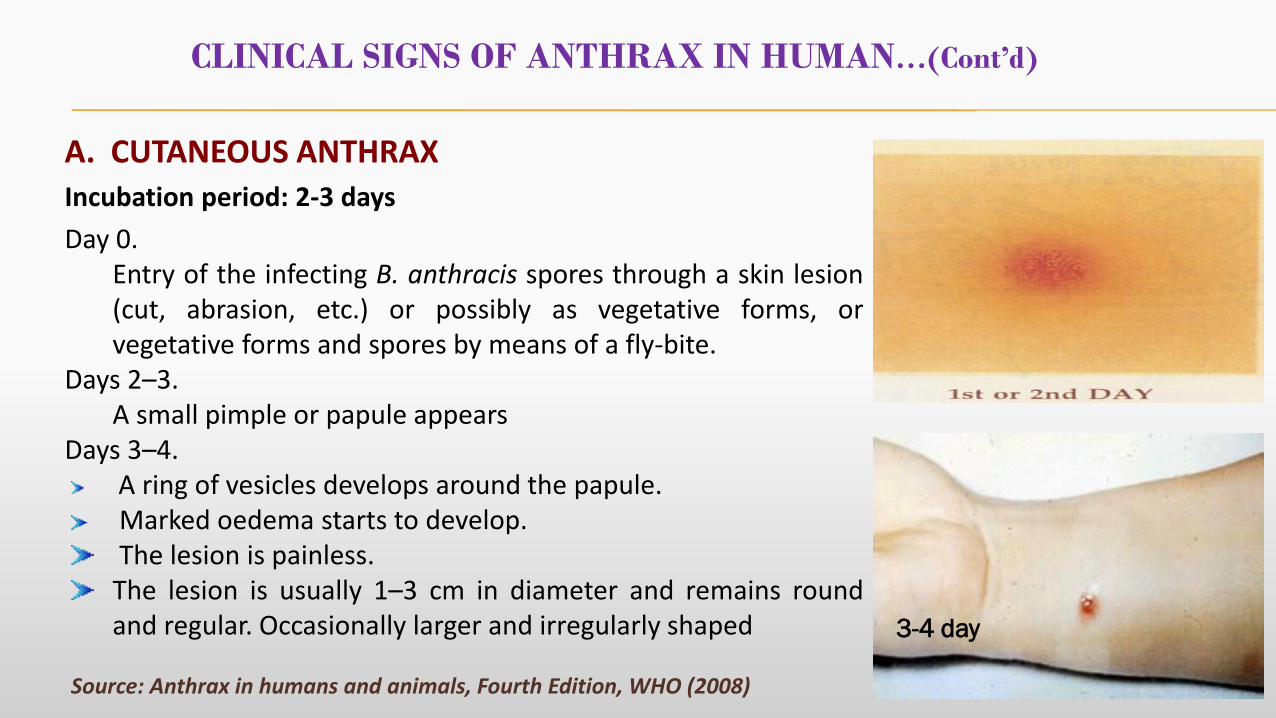
A. CUTANEOUS ANTHRAX
Incubation period: 2-3 days
Day 0.Entry of the infecting B. anthracis spores through a skin lesion(cut, abrasion, etc.) or possibly as vegetative forms, orvegetative forms and spores by means of a fly-bite.
Days 2–3.A small pimple or papule appears
Days 3–4.A ring of vesicles develops around the papule.Marked oedema starts to develop.The lesion is painless.
The lesion is usually 1–3 cm in diameter and remains roundand regular. Occasionally larger and irregularly shaped
Source: Anthrax in humans and animals, Fourth Edition, WHO (2008)
CLINICAL SIGNS OF ANTHRAX IN HUMAN…(Cont’d)
3-4 day
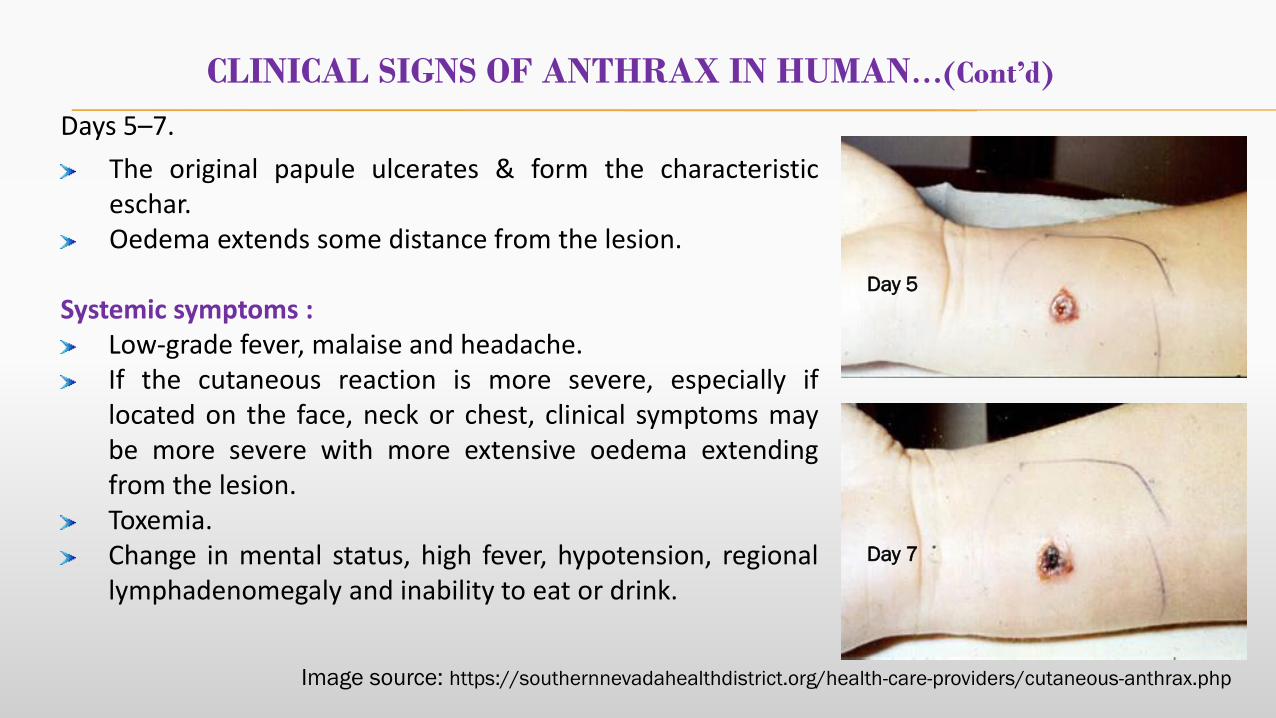
Days 5–7.
The original papule ulcerates & form the characteristiceschar.Oedema extends some distance from the lesion.
Systemic symptoms :Low-grade fever, malaise and headache.If the cutaneous reaction is more severe, especially iflocated on the face, neck or chest, clinical symptoms maybe more severe with more extensive oedema extendingfrom the lesion.Toxemia.Change in mental status, high fever, hypotension, regionallymphadenomegaly and inability to eat or drink.
Day 5
Day 7
CLINICAL SIGNS OF ANTHRAX IN HUMAN…(Cont’d)
Image source: https://southernnevadahealthdistrict.org/health-care-providers/cutaneous-anthrax.php
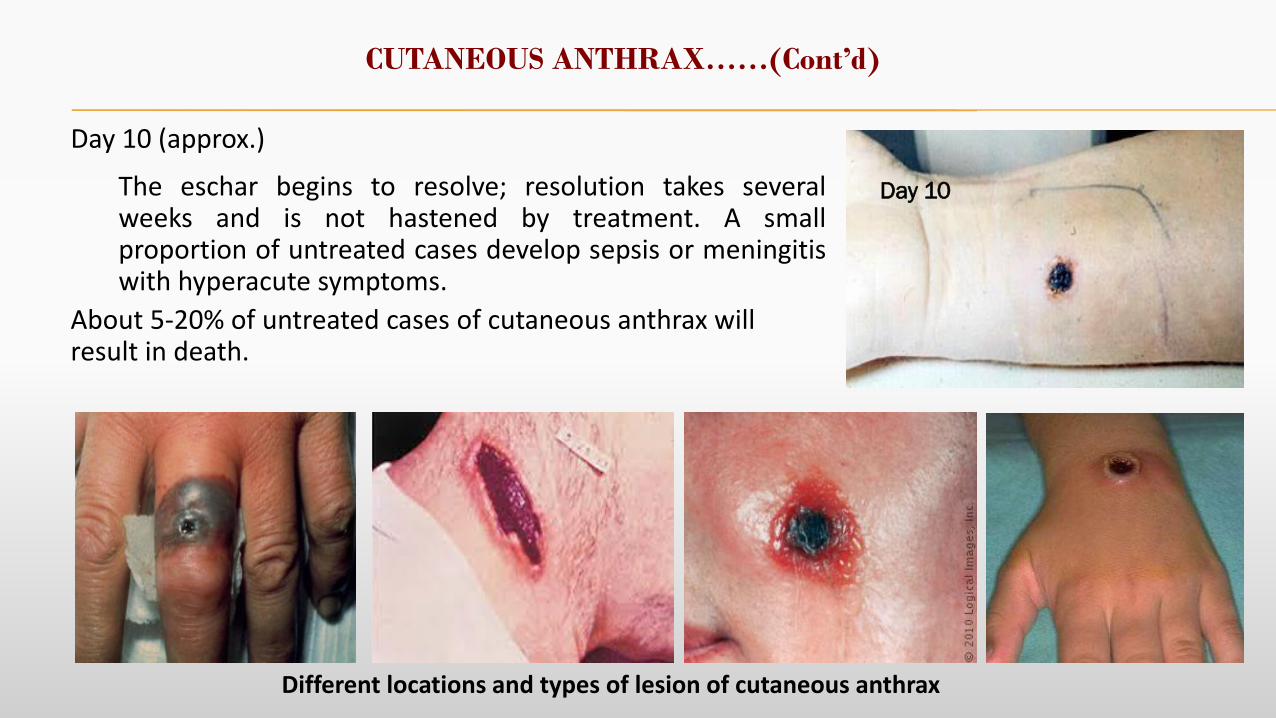
Day 10 (approx.)
The eschar begins to resolve; resolution takes severalweeks and is not hastened by treatment. A smallproportion of untreated cases develop sepsis or meningitiswith hyperacute symptoms.
About 5-20% of untreated cases of cutaneous anthrax will result in death.
CUTANEOUS ANTHRAX……(Cont’d)
Day 10
Different locations and types of lesion of cutaneous anthrax
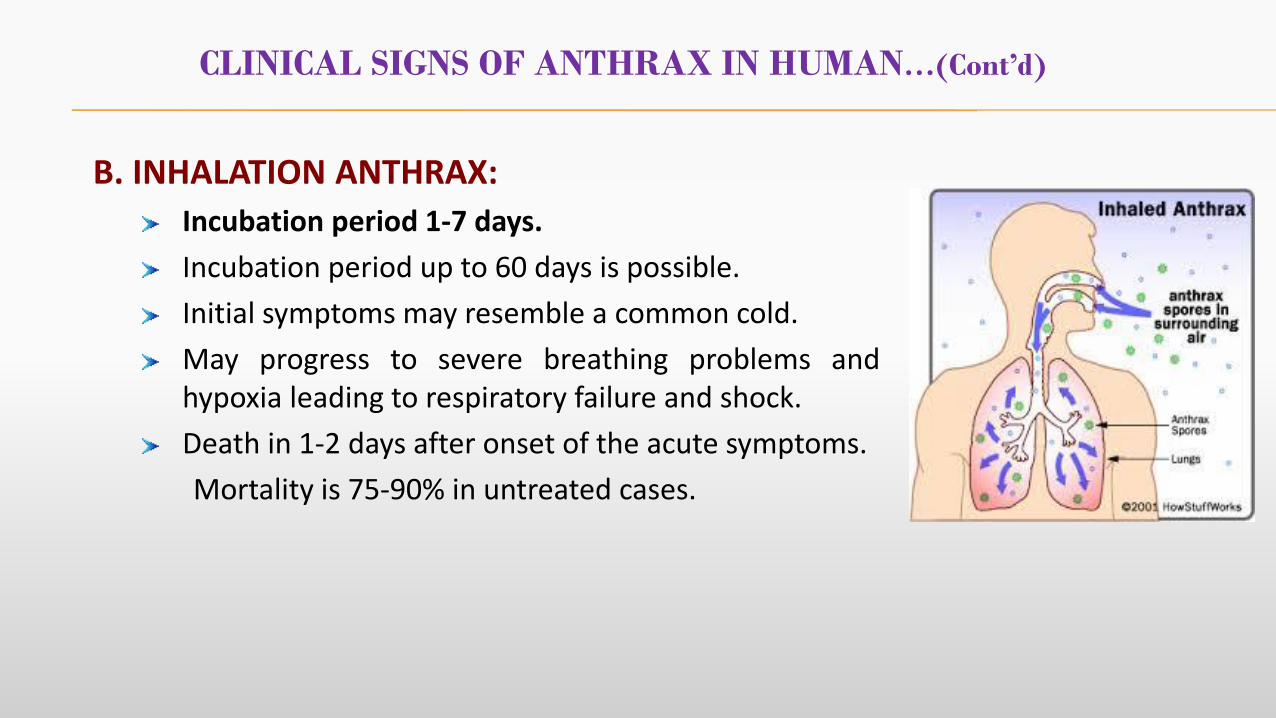
B. INHALATION ANTHRAX:
Incubation period 1-7 days.
Incubation period up to 60 days is possible.
Initial symptoms may resemble a common cold.
May progress to severe breathing problems andhypoxia leading to respiratory failure and shock.
Death in 1-2 days after onset of the acute symptoms.
Mortality is 75-90% in untreated cases.
CLINICAL SIGNS OF ANTHRAX IN HUMAN…(Cont’d)
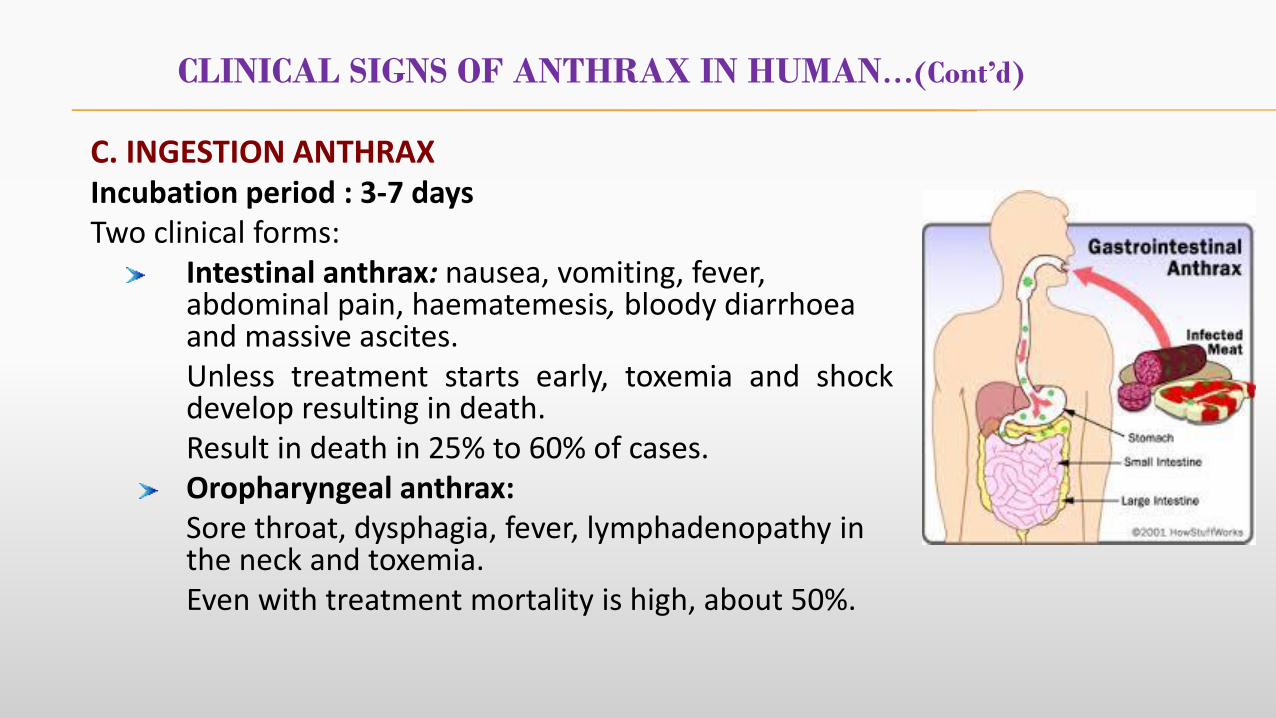
C. INGESTION ANTHRAXIncubation period : 3-7 daysTwo clinical forms:
Intestinal anthrax: nausea, vomiting, fever, abdominal pain, haematemesis, bloody diarrhoea and massive ascites. Unless treatment starts early, toxemia and shockdevelop resulting in death.Result in death in 25% to 60% of cases.Oropharyngeal anthrax: Sore throat, dysphagia, fever, lymphadenopathy in the neck and toxemia. Even with treatment mortality is high, about 50%.
CLINICAL SIGNS OF ANTHRAX IN HUMAN…(Cont’d)
OTHER FORMS
Anthrax Meningitis :Meningitis due to anthrax is a serious clinical developmentIt may follow any of the other three forms of anthrax Intense inflammation of the meninges with accompanying oedema.Anthrax meningitis is a haemorrhagic leptomeningitis with symptoms of
neck pain with or without flexionheadache changes in mental statevomiting and high-grade fever neurological signs include cranial nerve palsies, myoclonus, fasciculation, decerebrate posturing and papilloedema
The prognosis is extremely poorMay develop in 30‐40% cases100% mortality
CASE DEFINITION
RECOMMENDED CASE DEFINITION FOR HUMAN
Suspect: A case that is compatible with the clinical description and has anepidemiological link to confirmed or suspected animal cases or contaminated animalproducts.
Presumptive: A suspected case where
The clinical specimen in culture shows typical characteristic; or
In smear short chain of capsulated bacilli are seen when stained withpolychrome methylene blue.
Confirmed: A suspected case that is laboratory confirmed by one or more of thefollowing:
Where it shows encapsulated, non-motile, non-haemolytic gram positive bacillisusceptible to penicillin and the isolate is susceptible to gamma phage lysis.
PCR confirming presence of toxin and capsule genes.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
SPECIMEN TO COLLECT
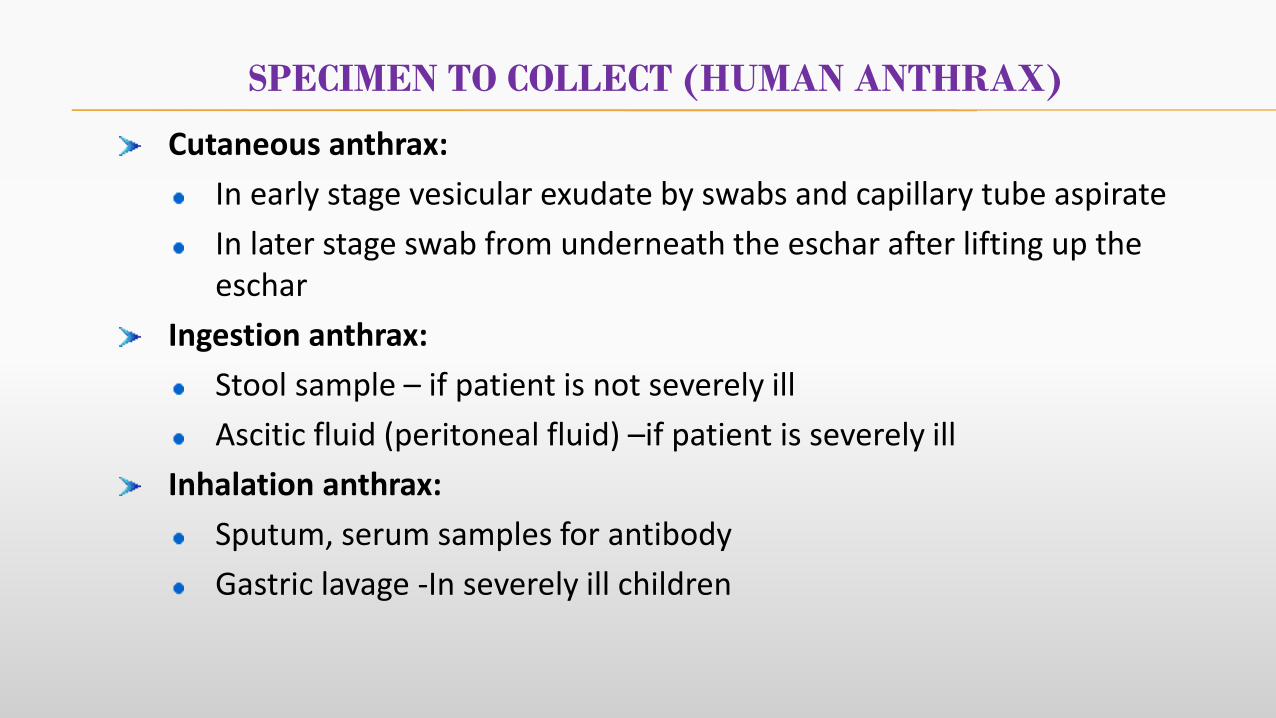
SPECIMEN TO COLLECT (HUMAN ANTHRAX)
Cutaneous anthrax:
In early stage vesicular exudate by swabs and capillary tube aspirate
In later stage swab from underneath the eschar after lifting up the eschar
Ingestion anthrax:
Stool sample – if patient is not severely ill
Ascitic fluid (peritoneal fluid) –if patient is severely ill
Inhalation anthrax:
Sputum, serum samples for antibody
Gastric lavage -In severely ill children
CASE MANAGEMENT
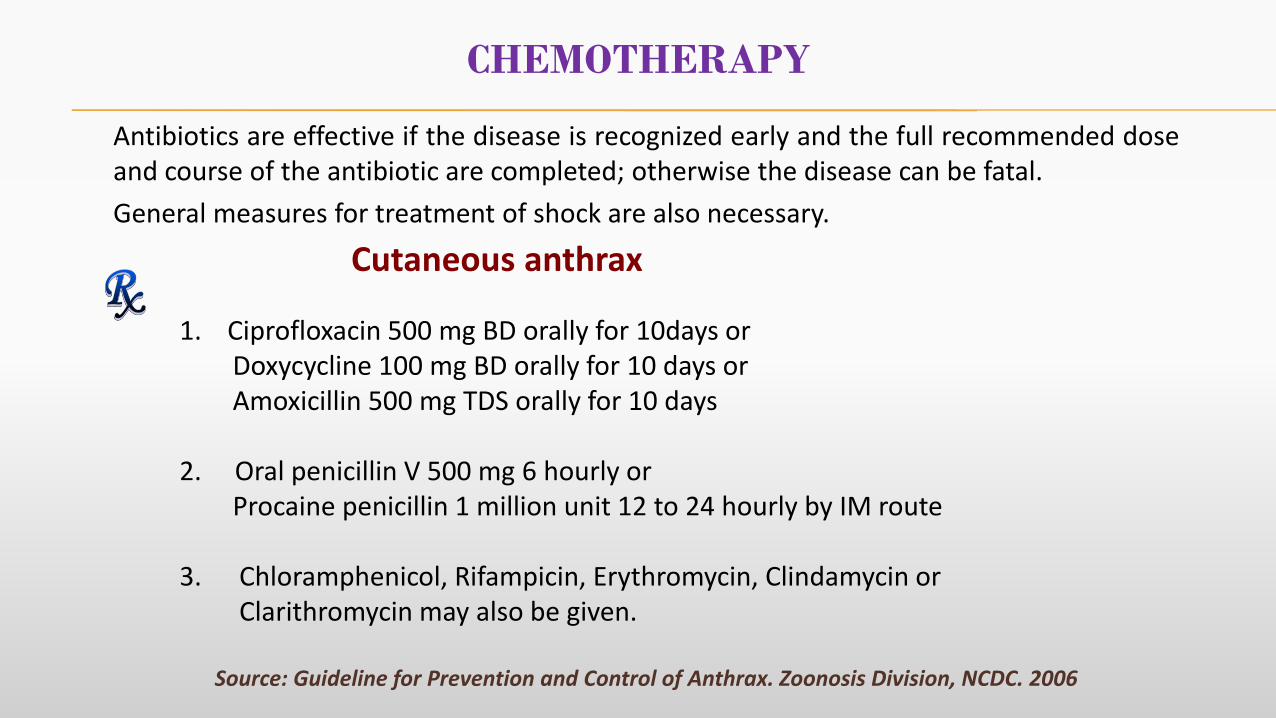
CHEMOTHERAPY
Antibiotics are effective if the disease is recognized early and the full recommended doseand course of the antibiotic are completed; otherwise the disease can be fatal.
General measures for treatment of shock are also necessary.
1. Ciprofloxacin 500 mg BD orally for 10days orDoxycycline 100 mg BD orally for 10 days orAmoxicillin 500 mg TDS orally for 10 days
2. Oral penicillin V 500 mg 6 hourly orProcaine penicillin 1 million unit 12 to 24 hourly by IM route
3. Chloramphenicol, Rifampicin, Erythromycin, Clindamycin or Clarithromycin may also be given.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
Cutaneous anthrax
Ciprofloxacin 400 mg IV BD till 2 weeks after the clinical response orPenicillin G- 2million units/day by infusion or by slow IV injection should beadministered until the temperature returns to normal.Thereafter treatment should be continued with Procaine penicillin 1 million units every12- 24 hrs by IM route.
Streptomycin 1-2 gms/day IM, may act synergistically with penicillin.Supportive care:
Oxygen inhalationRespiratory supportTreatment of shock if present
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
Inhalation and Ingestion anthrax
CHEMOTHERAPY…(Cont’d)
VACCINE AGAINST ANTHRAX
VACCINE FOR HUMANS (Source: National Health Portal)
Anthrax vaccine is recommended for people of 18 to 65 years of age. These people should get 5 doses of vaccine (IM):
Dose : A. First dose when risk of a potential exposure is identified
B. Remaining doses at 4 weeks and 6, 12 and 18 months after the first dose
C. Annual booster doses are recommended for ongoing protection
Who are to be vaccinated (not widely available)
Professionals (Veterinarians, butcher, person working in hide, wool and bone meal industry, Zookeeper, Wild life workers, Forest guards) should be vaccinated if their exposure is frequent and ifthe human vaccine is available.
VACCINE FOR ANIMALS: Anthrax spore vaccine (for livestock 1 ml SC). (Source: IAH &VB, West Bengal)
Dose : A. 1st dose at 3rd to 5th month of age - then annual booster dose
B. Before rainy season
PREVENTION AND CONTROL /
ACTION TO BE TAKEN DURING ANTHRAX
OUTBREAK
PREVENTION AND CONTROL OF ANTHRAX
The problem of anthrax continues because of
Consumption of meat from sudden death animals and utilizing their hair, hides,bones etc.
Lack of cooperation over reporting sudden deaths in animals.
Long delays in diagnosis due to poor communication and inadequate locallaboratory facilities.
Failure to implement policies on disposal of carcasses and subsequentdisinfection and decontamination.
Control of disease in animals is key to prevent the disease in human.
Control measures aim at
Breaking the cycle of infection
If a potential infectious source is known to exist, it should be eliminated withoutdelay.
In the event of a case of anthrax outbreak occurring in livestock, controlmeasures consists of:
1. Proper disposal of carcasses
2. Disinfection, decontamination and disposal of contaminated materials
3. Initiation of treatment and/or vaccination of other animals asappropriate
4. Intersectoral coordination
CONTROL MEASURES TO BE ADOPTED DURING
ANTHRAX OUTBREAK
1. PROPER DISPOSAL OF CARCASS
AVOID performing an autopsy when anthrax is being considered.
Prevent escape of bloody exudates from the carcass
Ensure that all body openings (e.g. anus, mouth, nose, etc.) are plugged withan absorbent material (e.g. non-perforated paper towel, cloths, etc.) toprevent leakage of exudates.
Ensure that the entire head is covered with a heavy plastic bag that issecured at the neck, behind the ears, and across the poll with duct tape ortied with rope.
The methods of disposal of an anthrax carcass are incineration, rendering or deep
burial.
CONTROL MEASURES TO BE ADOPTED DURING ANTHRAX OUTBREAK…(Cont’d)
PROPER DISPOSAL OF CARCASS…(Cont’d)
General Consideration
Incinerate or burn by either pit or raised carcass method (pyre), which is the preferredmethod of disposal.
Be aware that ventilation and adequate airflow within a pyre or pit are essential.
Understand that, if the fire burns too quickly, a complete burn will not be achieved,necessitating a secondary burn.
Avoid using materials that may be environmentally harmful (e.g. rubber tires).
Ensure that an adequate amount of fuel is available to completely reduce the carcass toash.
Burn contaminated materials with the carcass.
A. Incineration : The goal is to destroy as many spores as possible,thereby decreasing environmental anthrax contamination.Must be done with appropriate care to ensure completeburning so that the carcass should be completely reducedto ash.
PROPER DISPOSAL OF CARCASS…(Cont’d)
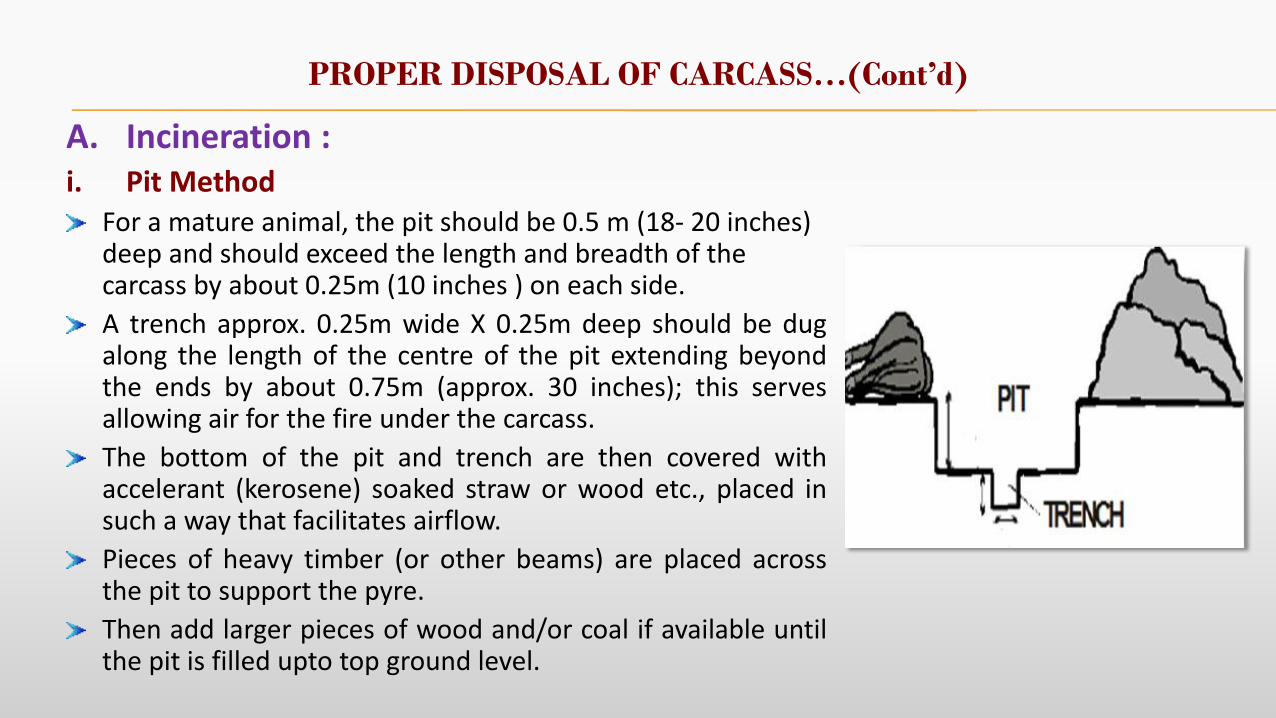
A. Incineration :i. Pit Method
For a mature animal, the pit should be 0.5 m (18- 20 inches) deep and should exceed the length and breadth of the carcass by about 0.25m (10 inches ) on each side.
A trench approx. 0.25m wide X 0.25m deep should be dugalong the length of the centre of the pit extending beyondthe ends by about 0.75m (approx. 30 inches); this servesallowing air for the fire under the carcass.
The bottom of the pit and trench are then covered withaccelerant (kerosene) soaked straw or wood etc., placed insuch a way that facilitates airflow.
Pieces of heavy timber (or other beams) are placed acrossthe pit to support the pyre.
Then add larger pieces of wood and/or coal if available untilthe pit is filled upto top ground level.
PROPER DISPOSAL OF CARCASS…(Cont’d)
Pit Method…(Cont’d)
Saturate all the fuel with kerosene.
The carcass can be drawn onto the pyre, propping up the carcass to lay it on its back.
Pour kerosene over the carcass. Set the fire at either end of the longitudinal trench.
After about first hour, the pyre should be covered with corrugated iron or other metalsheet in such a way as to reduce the heat loss without cutting off the ventilation.
Approx. quantities of fuel needed for a large domestic animal are
Straw 20kg, kerosene 10 liters and either 2 tonnes of wood or 0.5 tonnes of wood and0.5 tonnes of coal.
Note: Decontaminate the ground where the carcass lay and from where it was removed tothe pit and also the ground, equipment etc. contaminated during this moving process.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
PROPER DISPOSAL OF CARCASS…(Cont’d)
A. Incineration…(cont’d)
ii. Raised Carcass Method (Pyre)
Appropriate when labour is scarce or the ground is unsuitable for construction of a pit.
Place straw over a 2 x 1.5 metre area.
Place 2 wooden beams (approx. 2m length) over the straw parallel to each other andabout 1.2m apart.
Soak the straw with kerosene and cover with thin and thick pieces of wood and coal ifavailable.
Place further cross- pieces of wood or other material across the two main beams tosupport the carcass.
Prop up the carcass to lay it on its back.
The fuel (wood or coal) is banked up on either side of the carcass.
Fuel and carcass further soaked with kerosene.
The fire can then be started and when well underway, it should be covered, as in pitmethod, with metal sheet to retain heat but without inhibiting ventilation.
PROPER DISPOSAL OF CARCASS…(Cont’d)
Raised carcass method…(cont’d)
More fuel may be required than with pit method.
For a large domestic animal, an estimate is 0.75 tonnes coal + 0.5 tonnes wood or,
If coal is unavailable, approximately 3 tonnes of wood, plus 20 kg straw and 20 liters of kerosene.
Note: Decontaminate the ground where the carcass lay and from where itwas removed to the pyre and also the ground, equipment etc.contaminated during this movement.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
PROPER DISPOSAL OF CARCASS…(Cont’d)
B. Rendering
Essentially a cooking process which results in sterilization of raw materials ofanimal origin such that parts of carcass may be utilized safely for subsequentcommercial purposes.
In general, the raw materials are finely chopped and then passed into a steamheated chamber.
Temperatures ranging from 100°C to 150°C for 10-60 minutes.
Disadvantage:
There is risk of spreading disease during movement of anthrax infected carcassesto rendering facilities.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
PROPER DISPOSAL OF CARCASS…(Cont’d)
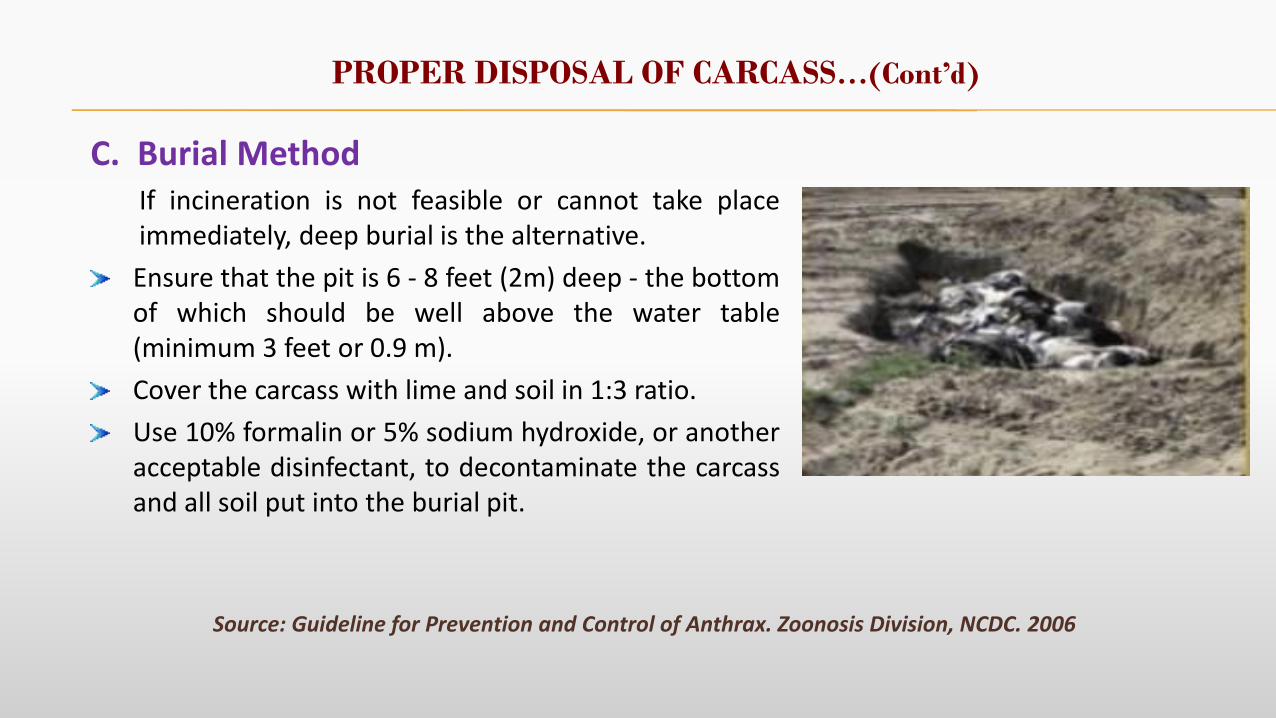
C. Burial Method If incineration is not feasible or cannot take placeimmediately, deep burial is the alternative.
Ensure that the pit is 6 - 8 feet (2m) deep - the bottomof which should be well above the water table(minimum 3 feet or 0.9 m).
Cover the carcass with lime and soil in 1:3 ratio.
Use 10% formalin or 5% sodium hydroxide, or anotheracceptable disinfectant, to decontaminate the carcassand all soil put into the burial pit.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
General consideration:
Consider the water table level and soil composition - clay soil is preferable, whereas sand orgravel should be avoided.
Do not locate burial pit in areas prone to water logging or at risk of flooding.
Ensure that there is no drinking water supply, river, well or any field drain near the burialsite.
Do not bury carcass in polythene bags or other impervious materials.
Burial should be discouraged in favour of incineration or rendering wherever possible.
Disadvantages
Disturbance of burial site brings the spores to the soil surface.
PROPER DISPOSAL OF CARCASS…(Cont’d)
Burial Method…(cont’d)
PROPER DISPOSAL OF CARCASS…(Cont’d)
D. The last resort Situations where incineration, rendering or burial may not be feasible. This is the leastpreferred option.
Leave the carcass unmoved and adequately closed off from other animals particularlyscavengers or people.
The carcass should be fenced off and covered using branches of trees, corrugated ironsheet or any other available materials, and hazard signs should be posted around thesite.
Cover the carcass and the surrounding area with disinfectants such as 10% formalin or5% solution of sodium hydroxide, and repeated as needed.
B. anthracis within the animal carcass does not sporulate and is inactivated by theputrefactive process in a few days.
Environmental contamination due to bloody exudates escaping from natural orifices ofthe dead animals could be minimized by scorching the site with fire after the carcass haseffectively putrefied, though this may be many months later.
Source: Guideline for Prevention and Control of Anthrax. Zoonosis Division, NCDC. 2006
2. Disinfection and DecontaminationDisinfectants should be available in reasonable quantities.Site where the animal died is to be disinfected with 5% formaldehyde after disposalof the carcass.Spores resistant to heat, sunlight, drying and many disinfectants.Disinfectants
- Formaldehyde (5%)- Glutaraldehyde (2%)- Sodium hydroxide (10%)- Bleach
Gas or heat sterilizationGamma radiation
Any milk collected from a cow, buffalo or goat showing signs of anthrax within 8 hours ofmilking is to be destroyed, along with any other milk that may have been mixed with thesuspected milk.
CONTROL MEASURES TO BE ADOPTED DURING ANTHRAX OUTBREAK…(Cont’d)
Disinfection and Decontamination…(Cont’d)
Preliminary disinfection
10% formaldehyde
4% glutaraldehyde (pH 8.0-8.5)
Cleaning
Hot water, scrubbing, protective clothing
Final disinfection (one of the following)
10% formaldehyde
4% glutaraldehyde (pH 8.0-8.5)
3% hydrogen peroxide
1% peracetic acid
CONTROL MEASURES TO BE ADOPTED DURING ANTHRAX OUTBREAK…(Cont’d)
3. Vaccination
All symptomatic animals are to be treated.
All other animals in the affected herd are to be vaccinated.
All cattle of neighboring premises should be vaccinated.
4. Quarantine
Affected premises are to be quarantined for at least 3 weeks after the last case.
A buffer zone, 20-30 Km wide, is to be established around the infected areawithin which all cattle are to be vaccinated and quarantined.
CONTROL MESURES TO BE ADOPTED DURING ANTHRAX OUTBREAK…(Cont’d)
CONTROL MEASURES TO BE ADOPTED DURING ANTHRAX OUTBREAK…(Cont’d)
Personal Protection For Human
People entering infected premises are required to wear protective clothing andfootwear, which are disinfected before leaving the premises.
Such persons should avoid any contact with other persons or animals withoutfirst changing clothing, washing hands and taking appropriate disinfectionmeasures.
Where there is a risk of aerosolization of spores, further precautions should beconsidered such as damping down the material, possibly with 5% formalin,wearing face masks etc.
Chemoprophylaxis for exposed person:
Asymptomatic exposed individuals are to be put on a four week course ofdoxycycline 100 mg twice daily or ciprofloxacin 500 mg twice daily.
ANTHRAX SURVEILLANCE SYSTEM
The primary objectives of any anthrax surveillance system are:(1) to prevent or reduce livestock losses and (2) to prevent human disease.
Monitoring the incidence of the disease in both animal and human populations.
All unexplained livestock deaths or suspected human and animals cases mustbe investigated with laboratory support.
In animals, biological samples should be collected with the help of veterinarian.
Prompt Reporting
Mandatory reporting of sudden deaths among livestock.
Mandatory reporting of all human cases.
Early and correct diagnosis and prompt treatment (both for human and
animal)
ANTHRAX SURVEILLANCE SYSTEM
Intersectoral Coordination
Control of anthrax among humans depends on theintegration of veterinary and human health surveillanceand control programmes.
Routine cross-notification between the veterinaryand human health surveillance systems is needed.
Close collaboration between the two health sectorsis particularly important during epidemiological andoutbreak investigations.
Intersectoral cooperation is important in areas wherewildlife areas abut with livestock areas, or wherewildlife and livestock intermingle.
ANTHRAX SURVEILLANCE SYSTEM…(Cont’d)
Implementation Of Control Measures
ANTHRAX SURVEILLANCE SYSTEM…(Cont’d)
Education /Awareness Campaign Education of both those who will be involved in the surveillance systemand those who own or handle livestock, meat, hides and other animalproducts – about modes of anthrax transmission, care of skin abrasionsand personal cleanliness. Control dust and properly ventilate all hazardous industries
particularly which handle raw animal materials. Handle of animals properly in slaughter houses, tanning industry etc. Treat properly the effluents from hazardous industries handling
animals etc.Not to kill sick animals for consumption. Proper cooking of meatproducts.Do not use/sell hide of animals exposed to anthrax nor use theircarcasses to make feed supplement.