Spring semester 2017 Seminar 3 - Nursing - UOW · Spring semester 2017 Seminar 3 - Nursing ......
20
Spring semester 2017 Seminar 3 - Nursing Dr Jeannette Stirling, Senior Lecturer, Learning Development; Additions by Dr Carol Priestley, Lecturer, Learning Development
Transcript of Spring semester 2017 Seminar 3 - Nursing - UOW · Spring semester 2017 Seminar 3 - Nursing ......

Spring semester 2017 Seminar 3 - Nursing
Dr Jeannette Stirling, Senior Lecturer, Learning Development; Additions by Dr Carol Priestley, Lecturer, Learning Development

Spring semester,
2017
Using
Evidence
Effectively

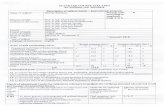
Subject
Assessment
1
Assessment
2
Assessment
3
Assessment
4
NMIH105 Week 4
Formative in-class quiz
Week 6
Essay
2000 words
40%
Weeks 8 & 9 Group presentation
20%
Exam Period Final exam
100 MCQ
40%
NMIH106 Week 4
Formative Basic Life
Support (BLS)
laboratory
Week 9 In-class quiz
MCQ
20%
Week 10 Case Study
2500 words
40%
Exam Period Final exam
100 MCQ
40%
NMIH107 Week 4 Case study
1500 wds
40%
Week 5
Formative on-line Moodle
quiz
Week 13 Case study
2,500 wds
60%
Week 13
WPE/NCAS
NMIH108 Week 4
Formative in-class quiz
Week 7 Essay
1500 wds
60%
Exam Period Final exam
40%

But first: how are you tracking with the NMIH105 essay?
What are the key terms in this question?
QUESTION:
According to the World Health Organisation (WHO) more than 900
million international journeys are undertaken every year. Global travel on
this scale exposes many people to a range of health risks. Many of these
risks can be minimized by precautions taken before, during and after
travel (WHO 2012).
Recently, the West African Ebola outbreak has been the largest, most
severe and most complex in human history. For more than a year,
people from all over the world have answered the call to work with WHO
to overcome this outbreak.

REMEMBER THE GOALS ARE TO:
conduct library research in order to acquire
knowledge and understanding about the Ebola
virus and safety precautions when travelling.
As a consequence of this research and critical
thinking, develop an appreciation of health
precautions and preventions surrounding the
virus.
What are the instruction words in this question?

Analyse the question & plot your navigational points
…
Analyse the task
• WHAT are the key words / concepts relevant to the task? Do you
understand their meaning?
• WHAT do the instruction words tell you to do?
Brainstorm
• WHAT will be the organising focus for your discussion? • WHAT main points do you need to include?
Consider logical flow
• HOW do you need to order your response?
• PLAN each stage of your task so that when you begin writing, you can be fairly sure that you’re going to address all aspects of the topic.

Do I understand the history and pathophysiology of Ebola and its mode of transmission?
Can I discuss the incidence and prevalence of reported cases of Ebola internationally including the
current estimated morbidity and mortality rates?
Can I clearly identify the incubation period of Ebola along with the current treatment methods of persons
affected by Ebola including vaccination options?
What are the current prevention and control methods deployed by health workers to reduce the
transmission of the virus?
Do I understand the World health organisation’s role In preventing Ebola outbreaks ?
Planning your structure …

The function of paragraphs in academic writing is to
…
Identify the main
idea/point (topic
sentence).
Provide some evidence to support your
point.
Synthesis:
connect this point to your
wider discussion /
the topic
(analysis)

Hudson (2009) claims that life expectancy is one of the key measures
of a population’s health. Australian Bureau of Statistics’ (ABS 2010)
data indicate that the life expectancy gap between Indigenous
Australians and other Australians registered as 11.5 years for males
and 9.7 years for females during the period 2005-07. However,
Hudson (2009, p. 4) argues that Indigenous life expectancy figures
‘fail to show how low the life expectancy rate is in some communities’.
The major factor in the life expectancy gap for Indigenous Australians
is chronic disease (Zhao 2004, p. 498). In 2004-05 reported rates of
chronic disease in Indigenous communities included cardiovascular
disease (12%), diabetes (6%), and kidney disease (2%) (ABS 2007). According to Solar and Irwin (2010) there are multiple factors which
underpin the poorer health outcomes experienced by Indigenous
population groups. The sociocultural burden of chronic disease on
these communities further complicates health outcomes for Aboriginal
and Torres Strait Islander peoples over and above life expectancy.
Topic
sentence:
main point.
Evidence &
extrapolation
Synthesis
Used with permission

P3: Eighty nine percent of townships in the Northern Territory,
Western Australia and Queensland are defined as remote
because of their lack of medical services and distances
from medical facilities.
P4: Archell, Hill and Jackson-Pulver (2007) identify the issues
around retention and attraction of medical officers to
remote and regional areas of the Aboriginal and Torres Strait
Islander health services.
P5: The negative affect that being removed from community
and loved ones in a time preceding birth has detrimental
effects on the emotional state of the mother and family.
P6: Watson, Hodson and Johnson (2002) point out the
communication issues confronting many of the women sent
from remote communities, some of who have English as a
second or third language. This communication problem can
only be more complicated when these women are confronted
with medical jargon which they do not understand.
P1. Three issues impacting
on quality family-centred
care for Indigenous
women during
pregnancy and birthing
are: the lack of readily
accessible health care
professionals and
facilities; the extensive
travel and expense of
travelling to larger
medical facilities when
complications occur; and
language barriers.
Create clear links / connections between paragraphs with topic sentences.
Used with permission

Remember, too, that the Conclusion……
Will draw together the key strands of the
preceding discussion and indicate how these
key ideas support or prove your stated thesis
claim.
Χ Will not introduce new evidence.

In conclusion, it is apparent that for decades health policies for
Indigenous women at the time of birthing have been inadequate.
Paternalistic approaches to obstetric and neonatal care have
resulted in a lack of awareness about cultural safety. The statistics
examined in the preceding discussion also strongly indicate the
need for more Indigenous doctors and health workers to promote
better outcomes for Indigenous mothers and their babies in remote
communities throughout Australia. As I have argued, sending
pregnant women away from their support networks and into the
unfamiliar surroundings of a health care system unaware of
Indigenous culture, birthing rituals and language can have
significantly negative effects for these women and their families.
The Canadian midwifery services for Indigenous women in northern
remote communities have been a success for low risk pregnancies
and allow Canadian Indigenous women to remain in their townships
and give birth, assisted by locally trained registered midwives.
Finally, the financial costs to the individual for travel, food,
accommodation, phone calls, and so forth, are effectively
addressed by the Canadian model. Because of all
these factors the model presents a valuable
solution for those health care issues confronting
Australian Indigenous women living in remote
communities.
Three issues impacting on quality family-centred care
for Indigenous women during pregnancy and birthing
are: the lack of readily accessible health care
professionals and facilities; the extensive travel and
expense of travelling to larger medical facilities when
complications occur; and language barriers. Strategies
to improve health outcomes for Indigenous families will
involve attracting and retaining health care
professionals who are aware of the need for Aboriginal
cultural safety at the fore front of treatment. In
examining possible solutions for the problems facing
Australian Aboriginal mothers and babies, Canadian
midwifery services in remote Inuit communities will be
discussed. Many of these communities have developed
successful birthing programmes for their Indigenous
populations. These programmes incorporate the family
care model which, in Australia, has been largely
overlooked as an option for remote Aboriginal
communities.
Introduction Conclusion

What is referencing?
Ever happen to you?
Comic Strip: Used with permission

Three aspects of referencing ….
The ‘mechanics’: ensuring your citation
information conforms to recommended style
conventions. Putting things in the right place and
format!
The ‘courtesy’: the ‘thanks mate’ component where
you respectfully acknowledge the intellectual
contributions of others to your own thinking & writing.
The ‘art’: strategically weaving research evidence into
your discussion for maximum effect.

The ‘mechanics’ of Harvard: referencing web sites

In text …
According to the Australian Bureau of Statistics (ABS 2009), the occurrence of
diabetes is three times higher for Indigenous Australians than non-Indigenous
Australians (Australian Aboriginal and Torres Strait Islander Health Survey 2012-13).
However, health disparities between Indigenous and non-Indigenous Australians are
not limited to diabetes, with higher statistical occurrence of other chronic diseases
including cardiovascular, renal, retinopathy and mental health, accounting for the
majority of the Indigenous health gap (ABS 2009; Browne et al. 2009). These diseases
are all largely preventable and have similar risk factors, therefore efforts to ‘close the
gap’ in the social determinants of health for Australian Indigenous populations should
be addressed holistically and not isolated to a particular disease type (Vos et al. 2009).
This analysis examines the correlatives between being an Indigenous Australian and
the risk factors associated with developing Type 2 diabetes. The World Health
Organisation (WHO 2013) indicates that Type 2 diabetes comprises approximately
90% of all diabetes diagnoses and is strongly linked to lifestyle factors and hence
considered preventable in most cases. The following discussion will therefore focus on
Type 2 diabetes because this disease is where the greatest discrepancy between
Indigenous and non-Indigenous health is notable. It should be noted, however, that
according to the Australian Institute of Health and Welfare (AIHW 2012) not all studies
differentiate diabetes types despite the marked difference in aetiology.

Basic Principles for referencing government publications
Author, i.e. the government or non-government body
Year of publication is the year of release (not the date in the title)
Title of document or report in Italics
Publisher: it’s common to have the same group as author and publisher
Place of publication: in Australia it’s Canberra (unless it’s a state
government department)
Viewed: give the date you viewed it
URL: for online reports
Australian Bureau of Statistics 2013, Australian Aboriginal and Torres Strait
Islander Health Survey 2012-13, Australian Bureau of Statistics, Canberra,
viewed 16 August 2017,
http://www.abs.gov.au/ausstats/[email protected]/mf/4727.0.55.001

Many Australian Bureau of Statistics documents have a Catalogue
number. Include this at the end of the title preceded by cat. no. :
Australian Bureau of Statistics 2013, Australian Aboriginal and
Torres Strait Islander Health Survey 2012-13, cat. no.
4727.0.55.001, Australian Bureau of Statistics, Canberra, viewed 16
August 2017,
http://www.abs.gov.au/ausstats/[email protected]/mf/4727.0.55.001
Australian Bureau of Statistics 2015, National Health Survey: First
Results, 2014-15, cat. no. 4364.0.55.001, Australian Bureau of
Statistics, Canberra, viewed 16 August 2017,
http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/43
64.0.55.001~2014-15~Main%20Features~Diabetes%20mellitus~12
Australian Institute of Health and Welfare 2015, The health and welfare of Australia’s Aboriginal and Torres Strait Islander peoples 2015, Australian Institute of Health and Welfare, Canberra, viewed 16 August 2017 http://www.aihw.gov.au/indigenous-observatory/reports/health-and-welfare-2015/ World Health Organisation 2013, Diabetes mellitis, Fact sheet No.
138. World Health Organisation, Geneva, viewed 16 August 2017,
http://www.who.int/mediacentre/factsheets/fs138/en/

Closer Title