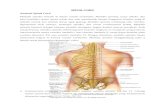
Spinal Cord,Vertebrae,Csf,Somatic Sensory and Motoric Pathway
Upload
kaden-beachCategory
view
72download
2description

Spine (Vertebrae) Fracture And Spinal Cord
Injury
Dr. Hermansyah, SpOTBag. Bedah/ SMF Orthopedi
FK-Unand/ RSUP Dr. M. Djamil PadangRSUD Lubuk Basung

Normal Spinal AnatomyNormal Spinal Anatomy

Spinal ligamentSpinal ligament
• Intrasegmental• Ligamentum flavum• Intertransverse ligament• Interspinous ligament• Intersegmental• ALL• PLL• Supraspinous ligament

EpidemiologyEpidemiology
Incidence: 10,000 new cases/yearIncidence: 10,000 new cases/yearPrevalence: 191,000 cases and risingPrevalence: 191,000 cases and risingPrime occurrence: males, peak of their Prime occurrence: males, peak of their
productive livesproductive livesCost: $ 5.6 billion/year in the USCost: $ 5.6 billion/year in the USCost per person: directly related to the Cost per person: directly related to the
level level
of SCI and patient’s ageof SCI and patient’s age

Common MechanismsCommon Mechanisms
CompressionCompression FlexionFlexionExtensionExtensionRotationRotationLateral bendingLateral bendingDistractionDistractionPenetrationPenetration

Whiplash injuryWhiplash injury

Suspect spinal injury with...Suspect spinal injury with...
Sudden decelerations (MVCs, falls)Sudden decelerations (MVCs, falls) Compression injuries (diving, falls onto feet/buttocks)Compression injuries (diving, falls onto feet/buttocks) Significant blunt trauma (football, hockey snowboarding, Significant blunt trauma (football, hockey snowboarding,
jet skis)jet skis) Very violent mechanisms (explosions, cave-ins, lightning Very violent mechanisms (explosions, cave-ins, lightning
strike) strike) Unconscious patient Unconscious patient Neurological deficit Neurological deficit Spinal tendernessSpinal tenderness

NeurologicalNeurologicalassessment: Sensoryassessment: Sensory

Goal of spine trauma careGoal of spine trauma care
Protect further injury Protect further injury during evaluation during evaluation and managementand management
Identify spine injury Identify spine injury or document absence or document absence of spine injuryof spine injury
Optimize conditions for maximal Optimize conditions for maximal neurologic recoveryneurologic recovery

Goal of spine trauma careGoal of spine trauma care
Maintain or restore spinal alignmentMaintain or restore spinal alignment
Minimize loss of spinal mobilityMinimize loss of spinal mobility
Obtain healed & stable spineObtain healed & stable spine
Facilitate rehabilitationFacilitate rehabilitation

Pre-hospital managementPre-hospital management
Protect spine at all times during the Protect spine at all times during the management of patients with multiple management of patients with multiple injuriesinjuries
Up to 15% of spinal injuries have a Up to 15% of spinal injuries have a second (possibly non adjacent) fracture second (possibly non adjacent) fracture elsewhere in the spineelsewhere in the spine
Ideally, whole spine should be Ideally, whole spine should be immobilized in neutral position on a firm immobilized in neutral position on a firm surfacesurface

PROTECTION PROTECTION PRIORITY PRIORITYDetection Detection Secondary Secondary
““Log-rolling”Log-rolling”

Pre-hospital management Pre-hospital management
Cervical spine immobilizationCervical spine immobilization
Transportation of spinal cord-injured Transportation of spinal cord-injured patients patients

Cervical spine immobilizationCervical spine immobilization
““Safe assumptions”Safe assumptions”Head injury and unconsciousHead injury and unconsciousMultiple traumaMultiple traumaFall Fall Severely injured workerSeverely injured workerUnstable spinal columnUnstable spinal column
Hard backboard, rigid cervical collar and lateral support (sand bag)Hard backboard, rigid cervical collar and lateral support (sand bag)
Neutral positionNeutral position

Philadelphia hard collarPhiladelphia hard collar

Transportation of spinal cord-injured Transportation of spinal cord-injured patientspatients
Emergency Medical Systems (EMS)Emergency Medical Systems (EMS)Paramedical staffParamedical staffPrimary trauma centerPrimary trauma centerSpinal injury centerSpinal injury center

Clinical assessmentClinical assessment
Advance Trauma Life Support (ATLS) Advance Trauma Life Support (ATLS) guidelinesguidelines
Primary and secondary surveys Primary and secondary surveys Adequate airway and ventilation are the Adequate airway and ventilation are the
most important factorsmost important factorsSupplemental oxygenationSupplemental oxygenationEarly intubation is critical to limit Early intubation is critical to limit
secondary injury from hypoxiasecondary injury from hypoxia

Physical examinationPhysical examination Inspection and palpation Inspection and palpation
Occiput to CoccyxOcciput to CoccyxSoft tissue swelling and bruisingSoft tissue swelling and bruisingPoint of spinal tendernessPoint of spinal tendernessGap or Step-offGap or Step-offSpasm of associated musclesSpasm of associated muscles
Neurological assessmentNeurological assessmentMotor, sensation and reflexesMotor, sensation and reflexesPRPR
Do not forget the cranial nerve (C0-C1 injury)Do not forget the cranial nerve (C0-C1 injury)

Neurogenic ShockNeurogenic ShockTemporary loss of autonomic function of the Temporary loss of autonomic function of the
cord at the level of injurycord at the level of injury results from cervical or high thoracic injuryresults from cervical or high thoracic injury
PresentationPresentationFlaccid paralysis distal to injury siteFlaccid paralysis distal to injury siteLoss of autonomic functionLoss of autonomic function
• hypotensionhypotension
• vasodilatationvasodilatation
• loss of bladder and bowel controlloss of bladder and bowel control
• loss of thermoregulationloss of thermoregulation
• warm, pink, dry below injury sitewarm, pink, dry below injury site
• bradycardiabradycardia

20
Neurogenic Hypovolemic
Etiology Loss of sympathetic outflow
Loss of blood volume
Blood pressure
Hypotension Hypotension
Heart rate Bradycardia Tachycardia
Skin temperature
Warm Cold
Urine output
Normal Low
Comparison of neurogenic and hypovolemic shock

Neurologic assessmentNeurologic assessment
Spinal shockSpinal shockBulbocavernosus reflexBulbocavernosus reflex
Complete VS incomplete cord injuryComplete VS incomplete cord injury ต้�องพ้�นภาวะ ต้�องพ้�นภาวะ spinal shock spinal shock ไปก่�อนไปก่�อนSacral sparingSacral sparing
• Voluntary anal sphincter controlVoluntary anal sphincter control• Toe flexorToe flexor• Perianal sensationPerianal sensation• Anal wink reflexAnal wink reflex


Neurologic assessmentNeurologic assessment
American Spinal Injury Association gradeAmerican Spinal Injury Association gradeGrade A – EGrade A – E
American Spinal Injury Association scoreAmerican Spinal Injury Association scoreMotor score (total = 100 points)Motor score (total = 100 points)
• Key muscles : 10 musclesKey muscles : 10 musclesSensory score (total = 112 points)Sensory score (total = 112 points)
• Key sensory points : 28 dermatomesKey sensory points : 28 dermatomes


Incomplete cord injuryIncomplete cord injury
Anterior cord syndromeAnterior cord syndromeBrown-Sequard syndromeBrown-Sequard syndromeCentral cord syndromeCentral cord syndrome

Anterior cord syndromeAnterior cord syndrome
Loss of motor, pain Loss of motor, pain and temperatureand temperature
Preserved Preserved propioception and propioception and deep touch deep touch

Brown-Sequard syndromeBrown-Sequard syndrome
Loss of ipsilateral Loss of ipsilateral motor and motor and propioceptionpropioception
Loss of contralateral Loss of contralateral pain and pain and temperaturetemperature

Central cord syndromeCentral cord syndrome
Weakness : Weakness : upper > lower upper > lower
Variable sensory Variable sensory lossloss
Sacral sparingSacral sparing

IMAGINGIMAGING
Numerous large prospective studies haveNumerous large prospective studies have
described the large cost and low yield ofdescribed the large cost and low yield of
the indiscriminate use of c-spine radiologythe indiscriminate use of c-spine radiology
in trauma patients.in trauma patients.
WHO NEEDS AN X-RAY???WHO NEEDS AN X-RAY???

NEXUSNEXUSCriteria were as follows…..Criteria were as follows…..
1.1. Absence of tenderness in the posterior Absence of tenderness in the posterior midlinemidline
2.2. Absence of a neurological deficitAbsence of a neurological deficit
3.3. Normal level of alertness (GCS15)Normal level of alertness (GCS15)
4.4. No evidence of intoxicationNo evidence of intoxication
5.5. No distracting pain elsewhereNo distracting pain elsewhere

NEXUSNEXUS
1.1. Any patient who fulfilled all 5 of the Any patient who fulfilled all 5 of the aforementioned criteria were considered aforementioned criteria were considered low risk for C-spine injury and as such low risk for C-spine injury and as such did not receive C-spine radiographydid not receive C-spine radiography
2.2. For patients who had any of the 5 For patients who had any of the 5 criteria,radiographic imaging was criteria,radiographic imaging was indicated in the form of AP, lateral, and indicated in the form of AP, lateral, and odontoid C-spine viewsodontoid C-spine views

Canadian C-Spine RulesCanadian C-Spine Rules

Plain Film RadiologyPlain Film Radiology
The standard 3 view plain film series is the lateral, The standard 3 view plain film series is the lateral, antero-posterior, and open-mouth view antero-posterior, and open-mouth view
The lateral cervical spine film must include the base of The lateral cervical spine film must include the base of the occiput and the top of the first thoracic vertebrathe occiput and the top of the first thoracic vertebra
The lateral view alone is inadequate and will miss up The lateral view alone is inadequate and will miss up to 15% of cervical spine injuries.to 15% of cervical spine injuries.

X-ray Guidelines (cervical)X-ray Guidelines (cervical)Adequacy, dequacy, AlignmentlignmentBBone abnormality, one abnormality, BBase of skullase of skullCCartilage, artilage, CContoursontoursDDisc spaceisc spaceSSoft tissueoft tissue

Interpreting Lateral Plain Interpreting Lateral Plain FilmFilm
AAdequacydequacyShould see C7-T1 Should see C7-T1
junctionjunctionIf not get If not get
swimmerswimmer’’s view or s view or CTCT

Swimmer’s View

Interpreting lateral Plain FilmInterpreting lateral Plain Film
AAlignmentlignmentAnterior vertebral lineAnterior vertebral line
• Formed by anterior borders of vertebral bodiesFormed by anterior borders of vertebral bodies
Posterior vertebral linePosterior vertebral line• Formed by posterior borders of vertebral bodiesFormed by posterior borders of vertebral bodies
Spino-laminar LineSpino-laminar Line• Formed by the junction of the spinous processes and the Formed by the junction of the spinous processes and the
laminaelaminae
Posterior Spinous LinePosterior Spinous Line• Formed by posterior aspect of the spinous processesFormed by posterior aspect of the spinous processes

AlignmentAlignment


BonesBones


CartilageCartilage Predental Space Predental Space
should be no more should be no more than 3 mm in adults than 3 mm in adults and 5 mm in and 5 mm in childrenchildren
Increased distance Increased distance may indicate may indicate fracture of odontoid fracture of odontoid or transverse or transverse ligament injuryligament injury

Cartilage Cont.Cartilage Cont. Disc SpacesDisc Spaces
Should be uniform Should be uniform
Assess spaces Assess spaces between the between the spinous processesspinous processes

Soft tissueSoft tissue
Nasopharyngeal Nasopharyngeal space (C1) - 10 mm space (C1) - 10 mm (adult)(adult)
Retropharyngeal Retropharyngeal space (C2-C4) - 5-7 space (C2-C4) - 5-7 mmmm
Retrotracheal space Retrotracheal space (C5-C7) - 14 mm (C5-C7) - 14 mm (children), 22 mm (children), 22 mm (adults)(adults)
Extremely variable Extremely variable and nonspecificand nonspecific
Measurements anterior to the mid-cervical spine up to 7 mm are common. > 7 mm,-a fracture is likely and the neck should be immobilized.

AP C-spine FilmsAP C-spine Films
Spinous processes Spinous processes should line up should line up
Disc space Disc space should be should be uniformuniform
Vertebral body Vertebral body height height should be uniform. should be uniform. Check for oblique Check for oblique fractures.fractures.

Open mouth viewOpen mouth view
AdequacyAdequacy: all of : all of the dens and the dens and lateral borders of lateral borders of C1 & C2C1 & C2
AlignmentAlignment: lateral : lateral masses of C1 and masses of C1 and C2C2
BoneBone: Inspect : Inspect dens for lucent dens for lucent fracture linesfracture lines

CT ScanCT Scan
Thin cut CT scan Thin cut CT scan should be used to should be used to evaluate abnormal, evaluate abnormal, suspicious or poorly suspicious or poorly visualized areas on visualized areas on plain filmplain film
The combination of The combination of plain film and directed plain film and directed CT scan provides a CT scan provides a false negative rate of false negative rate of less than 0.1%less than 0.1%

MRIMRI
Ideally all patients Ideally all patients with abnormal with abnormal neurological neurological examination should examination should be evaluated with be evaluated with MRI scanMRI scan

Management of SCIManagement of SCIPrimary GoalPrimary Goal
Prevent secondary injuryPrevent secondary injury
Immobilization of the spine begins in the Immobilization of the spine begins in the initial assessmentinitial assessmentTreat the spine as a long boneTreat the spine as a long bone
• Secure joint above and belowSecure joint above and below
Caution with “partial” spine splintingCaution with “partial” spine splinting

Management of SCIManagement of SCISpinal motion restriction: immobilization devicesSpinal motion restriction: immobilization devicesABCsABCs
Increase FiOIncrease FiO22
Assist ventilations as needed with c-spine controlAssist ventilations as needed with c-spine control Indications for intubation :Indications for intubation :
• Acute respiratory failureAcute respiratory failure• GCS <9GCS <9• Increased RR with hypoxiaIncreased RR with hypoxia• PCO2 > 50 PCO2 > 50 • VC < 10 mL/kg VC < 10 mL/kg
IV Access & fluids titrated to BP ~ 90-100 mmHgIV Access & fluids titrated to BP ~ 90-100 mmHg

Management of SCIManagement of SCILook for other injuries: “Life over Limb”Look for other injuries: “Life over Limb”Transport to appropriate SCI center once Transport to appropriate SCI center once
stabilizedstabilizedConsider high dose methylprednisoloneConsider high dose methylprednisolone
ControversialControversial as recent evidence questions benefit as recent evidence questions benefitMust be started < 8 hours of injuryMust be started < 8 hours of injuryDo not use for penetrating traumaDo not use for penetrating trauma30 mg/kg bolus over 15 minute 30 mg/kg bolus over 15 minute After bolus: infusion 5.4mg/kg IV for 23 hoursAfter bolus: infusion 5.4mg/kg IV for 23 hours

Principle of treatmentPrinciple of treatment
Spinal alignmentSpinal alignmentdeformity/subluxation/dislocation deformity/subluxation/dislocation
reductionreduction
Spinal column stabilitySpinal column stabilityunstable unstable stabilization stabilization
Neurological statusNeurological statusneurological deficit neurological deficit decompression decompression

CompleteComplete - Absence of sensory and - Absence of sensory and motor functions in the lowest sacral motor functions in the lowest sacral segments segments
IncompleteIncomplete - Preservation of sensory - Preservation of sensory or motor function below the level of or motor function below the level of injury, including the lowest sacral injury, including the lowest sacral segmentssegments

Frankel scaleFrankel scale
A complete paralysis A complete paralysis B sensory function only below the injury B sensory function only below the injury
level level C incomplete motor function below C incomplete motor function below
injury level injury level D fair to good motor function below D fair to good motor function below
injury level E normal function injury level E normal function

Treatment Treatment
SuportifSuportifNon OperativeNon OperativeSurgerySurgery

Steroid Protocol: for Spinal Steroid Protocol: for Spinal Cord InjuryCord Injury
Methylprednisolone given as bolus of 30 Methylprednisolone given as bolus of 30 mg / kg body wt - followed by infusion at mg / kg body wt - followed by infusion at 5.4 mg / kg / hour for 23 hours; 5.4 mg / kg / hour for 23 hours;
Excluded pts: - patients who are more Excluded pts: - patients who are more than 8 hours from injury (these patients than 8 hours from injury (these patients may actually do worse w/ steroids); may actually do worse w/ steroids);
Note: up to 40% of spine injured patients Note: up to 40% of spine injured patients who receive steroids can be expected to who receive steroids can be expected to develop some Gastrointenstinal bleedingdevelop some Gastrointenstinal bleeding

Non – Operative Treatment Non – Operative Treatment OptionsOptions
No treatmentNo treatment
advice / restrict activityadvice / restrict activity
Spinal ‘immobilisation’Spinal ‘immobilisation’
Bed restBed rest
Lumbar pillow / Log rollingLumbar pillow / Log rolling
TractionTraction
Casting / BracingCasting / Bracing
Combination treatmentCombination treatment


Guilford braceGuilford brace

Stable A3 FractureStable A3 Fracture
Bed Rest until Normal Trunk ControlBed Rest until Normal Trunk ControlStanding X RaysStanding X Rays? Use extension Brace or Cast? Use extension Brace or Cast

Indications for surgeryIndications for surgery
1.The spinal cord appears to be compressed 1.The spinal cord appears to be compressed 2.An progressive neurological deterioration. 2.An progressive neurological deterioration. 3.Dislocation with facet joint locking3.Dislocation with facet joint locking4.Unstable fracture of spine 4.Unstable fracture of spine

OccipitoatlantoaxiOccipitoatlantoaxial fusion with the al fusion with the Luque rectangleLuque rectangle

C Type Fracture L2C Type Fracture L2

USS2 Fracture Set – USS2 Fracture Set – Fixation of A3 FractureFixation of A3 Fracture


Complications Complications
A Infection of urinary and genital A Infection of urinary and genital tract tract
B. Pressure Sores : Prevention is B. Pressure Sores : Prevention is the most important treatment. the most important treatment.
C. Respiratory Complications : C. Respiratory Complications : respiratory infection respiratory infection
D. Disorder of D. Disorder of thermoregulation

PELVIC RING FRACTUREPELVIC RING FRACTURE

HermansyahHermansyah
Bag Bedah/ SMF Orthopedi Bag Bedah/ SMF Orthopedi
FK-Unand/ RSUP Dr. M.Djamil PadangFK-Unand/ RSUP Dr. M.Djamil Padang
PELVIC FRACTURES: CLASSIFICATION & PELVIC FRACTURES: CLASSIFICATION & MANAGEMENTMANAGEMENT

Pelvic fractures are caused by high energy blunt Pelvic fractures are caused by high energy blunt traumatrauma
Significant mortality and morbiditySignificant mortality and morbidity
Mortality 30% in unstable fracturesMortality 30% in unstable fractures
10 to 12% due to haemorrhage10 to 12% due to haemorrhage

ANATOMYANATOMY Sacrum and 2 Sacrum and 2
innominate bonesinnominate bones Innominate bones Innominate bones
articulate anteriorly articulate anteriorly at symphysis pubisat symphysis pubis
Sacrum articulates Sacrum articulates with the ilium with the ilium posteriorly through posteriorly through sacroiliac joints sacroiliac joints

ANATOMYANATOMYPelvic ring stability is Pelvic ring stability is
provided by:provided by: Iliolumbar ligs.Iliolumbar ligs. Dorsal sacroiliac Dorsal sacroiliac
ligamentsligaments Sacrotuberous ligsSacrotuberous ligs Ventral sacroiliac ligs.Ventral sacroiliac ligs. Sacrospinous ligsSacrospinous ligs Posterosuperior Posterosuperior
interosseous ligs.interosseous ligs.

ANATOMYANATOMYHighly vascularHighly vascular
Iliac vessels run Iliac vessels run along the inner along the inner wall of the pelviswall of the pelvis

Trauma MechanismTrauma Mechanism

YOUNG and BURGESSYOUNG and BURGESS










CLASSIFICATIONCLASSIFICATION
Tile’s classification Tile’s classification system uses radiographic system uses radiographic images to ascertain images to ascertain the degree of stability the degree of stability of the of the pelvis , and hence determine which pelvic injuries pelvis , and hence determine which pelvic injuries require stabilization and which can be managed require stabilization and which can be managed nonoperatively. nonoperatively.
Hence the classification by Tile is more relevant for Hence the classification by Tile is more relevant for formulating treatment, but does not give significant formulating treatment, but does not give significant information regarding the degree of damageinformation regarding the degree of damage

CLASSIFICATIONCLASSIFICATIONType A: Stable (Posterior Arch Intact)Type A: Stable (Posterior Arch Intact)
A1:Avulsion injuryA1:Avulsion injury
A2:Iliac wing or anterior arch fracture caused by A2:Iliac wing or anterior arch fracture caused by a direct blowa direct blow
A3: Transverse sacrococcygeal fractureA3: Transverse sacrococcygeal fracture
Type B: Partially Stable (Incomplete Type B: Partially Stable (Incomplete Disruption of Posterior Arch)Disruption of Posterior Arch)
B1:Open book injury (external rotation)B1:Open book injury (external rotation)
B2:Lateral compression injury (internal rotation)B2:Lateral compression injury (internal rotation)
B2-1:Ipsilateral anterior and posterior injuriesB2-1:Ipsilateral anterior and posterior injuries
B2-2:Contralateral (bucket-handle) injuriesB2-2:Contralateral (bucket-handle) injuries
B3:BilateralB3:Bilateral
Type C: Unstable (Complete Disruption of Type C: Unstable (Complete Disruption of Posterior Arch)Posterior Arch)
C1:UnilateralC1:Unilateral
C1-1:Iliac fractureC1-1:Iliac fracture
C1-2:Sacroiliac fracture-dislocationC1-2:Sacroiliac fracture-dislocation
C1-3:Sacral fractureC1-3:Sacral fracture
C2:Bilateral, with one side type B, one side type C2:Bilateral, with one side type B, one side type CC
C3:BilateralC3:Bilateral

TREATMENTTREATMENT
INITIAL MANAGEMENT:INITIAL MANAGEMENT:ATLS protocol: Primary surveyATLS protocol: Primary survey
IV fluids and blood transfusion with wide bore canulaIV fluids and blood transfusion with wide bore canula
A/P Xray of pelvis, L/S spine, Chest, Cervical spine (lat A/P Xray of pelvis, L/S spine, Chest, Cervical spine (lat view)view)
If blood is seen on external urethral meatus, suprapubic If blood is seen on external urethral meatus, suprapubic cystostomy is preferable to catheterization.cystostomy is preferable to catheterization.
Multidisciplinary approachMultidisciplinary approach

PrioritisingPrioritising
HEAD
PELVIS
ABDOMEN
CHEST

How to stabilise the PelvisHow to stabilise the Pelvis
Rotational instability – Binding – III – 3Rotational instability – Binding – III – 3Vertical instability – skeletal traction –Vertical instability – skeletal traction – III – 3 III – 3Non invasive external stabilisation devices Non invasive external stabilisation devices
or a bed sheet but allow access to or a bed sheet but allow access to laparotomy and femoral access for laparotomy and femoral access for angiographyangiography – IV – IV
If Non invasive fails invasive anterior If Non invasive fails invasive anterior external fixationexternal fixation - IV - IV
ITIM

Circumferential SheetingCircumferential Sheeting
SupineSupine
2 “Wrappers”2 “Wrappers”
PlacementPlacement
ApplyApply
““Clamper”Clamper”
30 Seconds30 Seconds
1
2
34
Routt et al, JOT, 2002



SAM SLINGSAM SLING

TREATMENTTREATMENT
HAEMODYNAMICALLY STABLEHAEMODYNAMICALLY STABLE::
Complete secondary surveyComplete secondary survey
Inlet and outlet views, Pelvic CT scanInlet and outlet views, Pelvic CT scan
Pelvic binder for unstable fracturesPelvic binder for unstable fractures
Definitive fixationDefinitive fixation

TREATMENTTREATMENT
HAEMODYNAMICALLY UNSTABLEHAEMODYNAMICALLY UNSTABLE

TREATMENTTREATMENT

TREATMENTTREATMENT

LAPAROTOMYLAPAROTOMY

PELVIC EXTERNAL FIXATOR PELVIC EXTERNAL FIXATOR Damage control Damage control
surgery, Minimally surgery, Minimally invasiveinvasive
Stabilizes rotationally Stabilizes rotationally unstable pelvis, in unstable pelvis, in patients with shockpatients with shock
Before laparotomy Before laparotomy

Immediate External FixationImmediate External FixationPelvic Pelvic ““clampsclamps””

Percutaneous fixationPercutaneous fixation Exposure not a Exposure not a
problemproblem Low complication rateLow complication rate Bio mechanically Bio mechanically
idealideal
Detailed anatomical Detailed anatomical knowledge requiredknowledge required
Technically Technically demandingdemanding

DEFINITIVE FRACTURE FIXATIONDEFINITIVE FRACTURE FIXATION
INDICATIONS:INDICATIONS:1.1.Symphyseal diastasis > 2cmSymphyseal diastasis > 2cm2.2.Contralateral bucket handle injury causing >1.5cm Contralateral bucket handle injury causing >1.5cm
limb length discrepancylimb length discrepancy3.3.Rotationally and vertically unstable fractures (Tiles Rotationally and vertically unstable fractures (Tiles
Type C)Type C)
TIMINGTIMING When patient is stabilized, and fit enough to When patient is stabilized, and fit enough to
undergo the definitive procedureundergo the definitive procedure

DEFINITIVE FRACTURE DEFINITIVE FRACTURE FIXATIONFIXATION
Lag screw, Lag screw, Neutralization platesNeutralization plates for for Iliac wing fracturesIliac wing fractures
Plate fixation Plate fixation for for Symphyseal diastasisSymphyseal diastasis

DEFINITIVE FRACTURE DEFINITIVE FRACTURE FIXATIONFIXATION
Plate fixation, Plate fixation, sacroiliac screw sacroiliac screw fixationfixation for Sacral for Sacral fracturesfractures
Cancellous screwCancellous screw or or Sacroiliac plate Sacroiliac plate fixation fixation for for Sacroiliac disruptionSacroiliac disruption

ANGIOGRAPHYANGIOGRAPHY

SUMMARYSUMMARY
Stabilization of a haemodynamically unstable patient Stabilization of a haemodynamically unstable patient is of paramount importance.is of paramount importance.
Unstable pelvic fractures should be stabilized Unstable pelvic fractures should be stabilized externally as soon as possible.externally as soon as possible.
For unresponsive patients, urgent laparotomy with For unresponsive patients, urgent laparotomy with angiography on stand by.angiography on stand by.
Not all pelvic fractures requires fixation.Not all pelvic fractures requires fixation.


















