
Joseph Gligorov : Lipegfilgrastim : A new long-ac,ng recombinant human G-CSF
Upload
olivia-hudsonCategory
view
216download
1
Soirée AERIO
23 novembre 2011
Joseph GLIGOROV
APHP Tenon

Conflict of interest
• Involved in past 2 years in clinical trials financially supported & medical advisory boards – Astra-Zeneca– Bristol Myers Squib– Eisai– Glaxo Smith Kline– Pfizer– Roche– Sanofi-Aventis

ADJUVANT TREATMENTpT1cpN0M0
luminal B
TAM vs AI vs NAT
Joseph GLIGOROV
APHP Tenon

LEVEL OF EVIDENCE: ?

DDFS by histological grade, ER content, erbB2 protein expression, and erbB2 amplification status.
Joensuu H et al. Clin Cancer Res 2003;9:923-930
©2003 by American Association for Cancer Research

Tumor Size for NN T1 and T2 Cases in SEER database
0
2
4
6
8
10
12
0 10 20 30 40 50
Tumor Size (mm)
% o
f cas
es

Influence des traitements systémiques…Données de registre

Survie globale et survie sans récidive durant les deux périodes

Survie sans récidive à distance durant les deux périodes en fonction du pT1


Survie sans récidive à distance durant les deux périodes
en fonction du statut RH et de la prolifération

AIs Are Now the Adjuvant Endocrine Therapy of Choice for Postmenopausal Women With Breast
Cancer• ASCO (2010)1 and NCCN (2011)2
– 5 years of endocrine therapy: Upfront AI or sequential TAM AI • St. Gallen Consensus Panel (2009)3
– In view of BIG 1-98 sequencing results,4 the majority of the panel preferred upfront AI, particularly for patients at higher risk of early relapse
• St. Gallen Consensus Panel (2011)5-6
– Panel was evenly divided regarding whether all patients should receive AI vs TAM therapy and if the AI should be upfront
• Regional guidelines in France and Germany support AI therapy7
• ESMO (2010)8
– Upfront AI for 5 years– For patients receiving TAM, switch to AI after 2 to 3 years– Total duration of therapy: 5 to 10 years
1. Burstein HJ, et al. JCO. 2010;28(23):3784-3796; 2. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. v.2.2011; 3. Goldhirsch A, et al. Ann Oncol. 2009;20(8):1319-1329; 4. Mouridsen H, et al. NEJM. 2009;361(8):766-776; 5. Goldhirsch A, et al. Ann Oncol. 2011; 22(8):1736-1747; 6. Gnant M, et al. Breast Care. 2011; 6:136-141; 7. Wolters R, et al. Eur J Cancer. 2011 July 7 Epub; 8. Aebi S, et al. Ann Oncol. 2010;21(suppl 5):v9-v14.

Adjuvant Therapy Trial Designs: Are Upfront AIs Superior to TAM?
a Note that some patients from the original newly diagnosed population are lost because of recurrence or adverse events before randomization.Abbreviations: AI, aromatase inhibitor; ANA, anastrozole; EXE, exemestane; LET, letrozole; TAM, tamoxifen.
1. Dowsett M, et al. JCO. 2010;28(3):509-518; 2. Ingle JN, et al. Ann Oncol. 2008;19(5):877-882; 3. Jakesz R, et al. JNCI. 2007;99(24):1845-1853.
Supporting Trials• ATAC (ANA vs TAM)• BIG 1-98 monotherapy arms (LET vs TAM)• TEAM (2.75-year follow-up; EXE vs TAM)
Upfront (early adjuvant at start)
Randomization
Supporting Trials• ABCSG-8 alone (arms A & C)• BIG 1-98 sequencing arms (arms C & D)• TEAM (5-year follow-up)
Sequencing
Randomization
ABCD
Supporting Trials• IES• ITA• ARNO/ABCSG-8 combined analysis
Switching
a
Randomization
Extended AdjuvantSupporting Trials• MA-17• ABCSG-6
a Randomization
All support switch to AI vs continued TAM1
All support extended AI vs no further therapy2,3
13

Patient Characteristics: BIG 1-98, ATAC, and TEAM
• Patient populations typical of PMW with early breast cancer in both trials• AI arms are well matched to TAM control arms in both trials• Patients with receptor-positive tumors
– BIG 1-98: 99.8% (study requirement)– TEAM: 100% (study requirement)– ATAC: 83.7%
Abbreviations: AI, aromatase inhibitor; ANA, anastrozole; CT, chemotherapy; ER, estrogen receptor; EXE, exemestane; LET, letrozole; PgR, progesterone receptor; PMW, postmenopausal women; TAM, tamoxifen.
1. Thürlimann B, et al. NEJM. 2005;353(26):2747-2757; 2. Baum M, et al. Lancet. 2002;359(9324):2131-2139; 3. van de Velde CJH, et al. Lancet. 2011;377(9762):321-331.
BIG 1-981 ATAC2 TEAM3
Characteristics LET TAM ANA TAM EXE TAMn 4,003 4,007 3,125 3,116 4,898 4,868Mean age, years 61 61
64.164.1 65 64
Tumor > 2 cm, % 36.5 37.735.3
36.4 40 40
Node+, % 41.5 41.234.9
33.5 47 47
ER+ and/or PgR+, % 99.8 99.783.7
83.4 100 100
Previous/adjuvant CT, % 25.3 25.322.3
20.8 36 36
14
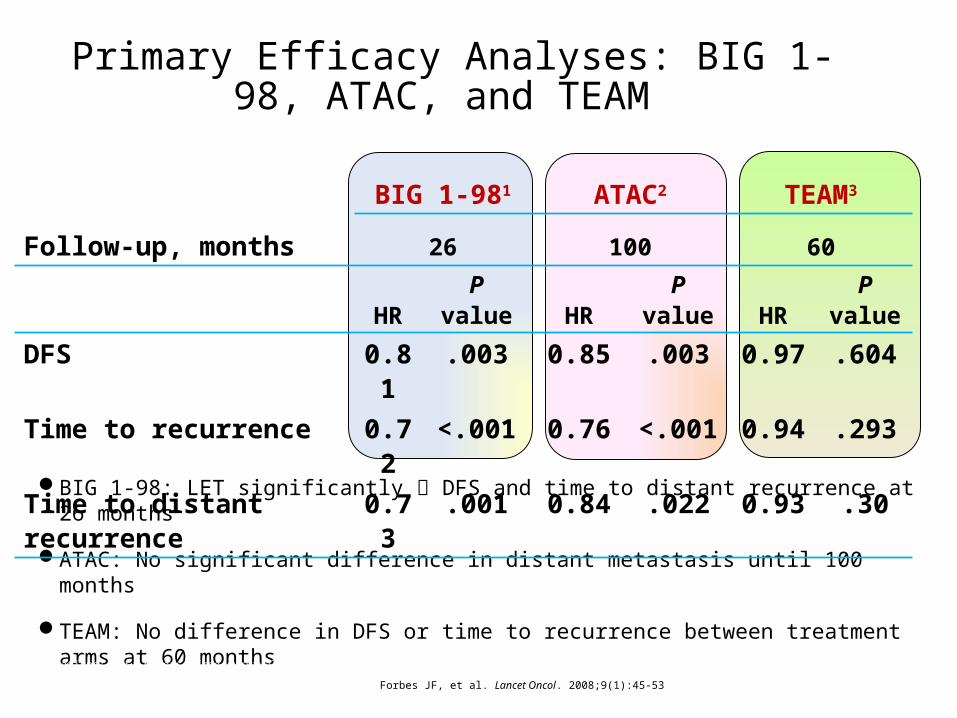
Primary Efficacy Analyses: BIG 1-98, ATAC, and TEAM
BIG 1-98: LET significantly DFS and time to distant recurrence at 26 months
ATAC: No significant difference in distant metastasis until 100 months
TEAM: No difference in DFS or time to recurrence between treatment arms at 60 months
Abbreviations: DFS, disease-free survival; HR, hazard ratio; LET, letrozole.
1. Thürlimann B, et al. NEJM. 2005;353(26):2747-2757; 2. Forbes JF, et al. Lancet Oncol. 2008;9(1):45-53; 3. van de Velde CJH, et al. Lancet. 2011;377(9762):321-331.
BIG 1-981 ATAC2 TEAM3
Follow-up, months 26 100 60
HR P value HR P value HR P valueDFS 0.81 .003 0.85 .003 0.97 .604
Time to recurrence 0.72 <.001 0.76 <.001 0.94 .293
Time to distant recurrence 0.73 .001 0.84 .022 0.93 .30
15






DDFS by histological grade, ER content, erbB2 protein expression, and erbB2 amplification status.
Joensuu H et al. Clin Cancer Res 2003;9:923-930
©2003 by American Association for Cancer Research
Is no adjuvant treatment a reasonable option ?

METASTATIC TREATMENTTriple negative disease
Joseph GLIGOROV
APHP Tenon

LEVEL OF EVIDENCE: ?


Natural Histoty & Prognosis
Prat A, Perou CM. Molecular Oncology 2011


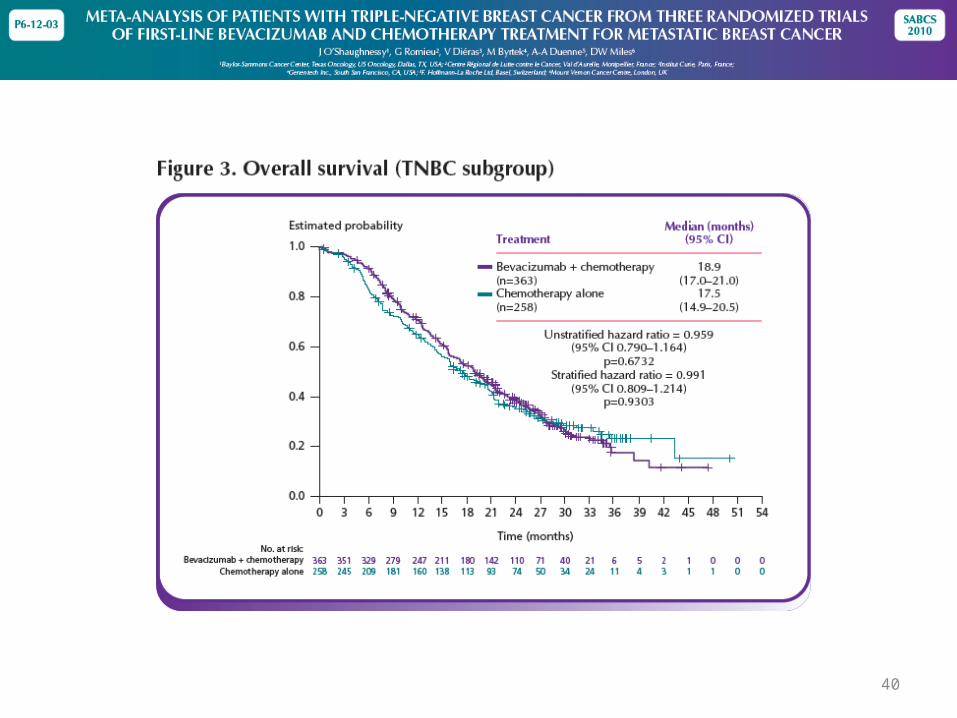
A Meta-Analysis of Overall Survival Data from Three Trials of Bevacizumab and First-Line
Chemotherapy as Treatment for Patients with Metastatic Breast Cancer
Baylor-Sammons Cancer Center, Texas Oncology, US Oncology, Dallas, TX; Mount Vernon Cancer Centre, London, England; Dana-Farber Cancer Institute, Boston, MA; Institut Curie, Paris, France; Mayo Clinic, Jacksonville, Florida; Michiana Hematology Oncology, South Bend, IN; Vall d'Hebron University Hospital, Barcelona, Spain; BioOncology, Genentech, S San Francisco, CA;
Indiana University Melvin and Bren Simon Cancer Center, Indianapolis, IN
Joyce O’Shaughnessy, David Miles, Robert Gray, Véronique Diéras, Edith A. Perez, Robin Zon, Javier Cortés,
Xian Zhou, See-Chun Phan, Kathy Miller
ASCO, 2010

30
Overall Survival, Pooled Population
Non-BV(n=1008)
BV(n=1439)
Median, mo 26.4 26.7
HR (95% CI) 0.97 (0.86–1.08)
1-yr survival rate (%)
77 82

31
Analysis of OS by Subgroups

32
Objective Response Rate*
*Includes only patients with measurable disease at baseline.
Non-BV(n=788)
BV(n=1105)
50
0
45
40
35
30
25
20
15
10
5
32
49
Ob
ject
ive
resp
on
se r
ate
(%)

33
Progression-Free Survival, Pooled Population
Non-BV(n=1008)
BV(n=1439)
Median, mo 6.7 9.2
HR (95% CI) 0.64 (0.57–0.71)

34
Analysis of PFS by Subgroups

35
Méta analyse bévacizumab 1ère ligne:
• Amélioration de la PFS dans la population- Triple négative (mais aussi RH+)
- Ayant reçu au préalable une chimiothérapie par taxanes en situation non métastatique
- Indépendament du type de chimiothérapie associée• Paclitaxel
• capécitabine

Comparison of Subgroup Analyses of PFS from Three Phase III Studies of Bevacizumab in Combination with
Chemotherapy in Patients with HER2-Negative Metastatic Breast Cancer
Joyce O’Shaughnessy,1 Véronique Diéras,2 John Glaspy,3 Adam Brufsky,4 Kathy D. Miller,5 David W. Miles,6 Piotr Koralewski,7
See-Ch un Phan,8 Suman Bhattacharya8
1Baylor-Sammons Cancer Center, Texas Oncology, U.S. Oncology, Dallas, TX; 2Institut Curie, Paris, France; 3UCLA TORI, Los Angeles, CA; 4University of Pittsburgh,
Pittsburgh, PA; 5Indiana University Melvin and Bren Simon Cancer Center, Indianapolis, IN; 6Mount Vernon Cancer Centre, London, England; 7Rydygiera
Hospital, Krakow, Poland; 8BioOncology, Genentech, South San Francisco, CA

Overall PFS Results

Neoadjuvant or Adjuvant Taxane Treatment

Triple Negative
40

41

42

Y A T’IL D’AUTRES ARGUMENTS CLINIQUES ?
Cancers du sein dit « Triple négatif »






ET EN DEHORS DES ESSAIS…DANS LA VRAI VIE…
Cancers du sein dit « Triple négatif »

ATHENAEfficacité d’Avastin / sous groupe TNBC
Thomssen et al. SABCS 2009

Miles D et al. ESMO 2010

Conclusion
• En attendant les résultats d’autres études comportant des thérapies ciblées:– l’association bévacizumab et chimiothérapie est la
seul ayant démontré un bénéfice en PFS sans majoration considérable de la toxicité dans la population dite « triple négative »
– Et plus particulièrement chez des patientes pré-exposées aux taxanes en situation (néo)adjuvante ce qui correspond aujourd’hui à nos pratiques les plus courantes

PersonalizingCancer Care

I Bergman The 7th Seal

Thanks
The complexity of TNBC treatment strategies


















