
Slides available at Bob Arnold, University of Pittsburgh School of Medicine James Tulsky, Duke...
126
Slides available at www.aahpm.org Bob Arnold, University of Pittsburgh School of Medicine James Tulsky, Duke University School of Medicine Sonni Mun, Mount Sinai School of Medicine Update in Hospice and Palliative Care
-
Upload
kristin-king -
Category
Documents
-
view
216 -
download
0
Transcript of Slides available at Bob Arnold, University of Pittsburgh School of Medicine James Tulsky, Duke...

Slides available at www.aahpm.org
Bob Arnold, University of Pittsburgh School of Medicine
James Tulsky, Duke University School of Medicine
Sonni Mun, Mount Sinai School of Medicine
Update in Hospice and Palliative Care

Slides available at www.aahpm.org
Acknowledgments
Daniel Fischberg
Karl Lorenz
Nathan Cherney
Rosanne Leipzig
Staff of AAHPM
Slides available at www.aahpm.org
2004: A Banner Year
• NIH State the Science– (http://consensus.nih.gov/ta/024/
endoflifeintro.html)
• National Consensus Project– (http://www.nationalconsensusproject.org)

Slides available at www.aahpm.org
2004: A Banner Year
• Review of Pediatric Palliative Care in NEJM– Himelstein B. P., Hilden J.M., Boldt A., Weissman
D., 350: 1752-1762, April 22, 204
• Review of Palliative Care in NEJM– Morrison, R.S., Meier, D., 350:2582-2590, June
17, 2004

Slides available at www.aahpm.org
Objectives
• Summarize seven important peer-reviewed articles from the last year
• Critically analyze their methodologies and understand their conclusions
• Determine if the findings are relevant to the care of your patients
Slides available at www.aahpm.org
Key Issues to Be Considered
• Is the question important?
• What are the results?
• Are the results valid?
• Can I apply the results to my patients
Slides available at www.aahpm.org
Methods
• Key Word search of evidence-based reviews– Nathan Cherney database
(www.cherneydatabase.org)– State of Science database

Slides available at www.aahpm.org
Methods
• Hand search of leading journals
• Selection criteria– Quality of science– Represent breadth of domains– Appeal to breadth of interest– Potential for impact
Slides available at www.aahpm.org
Relief of Suffering
One breakthrough of the last year stands out above all others….

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Case 1: Jerrold R
• Recently diagnosed stage IV lung cancer
• Presents to internist with chest wall pain
• Has not taken any analgesics as “not sure what to take?”

Slides available at www.aahpm.org
Is it appropriate to start with a strong opiate?
• WHO therapeutic ladder for the treatment of cancer pain
• Data supporting WHO guidelines are weak
Mild
Moderate
SevereStrong Opioid
Weak Opioid
Non-Opioid
Pain

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Starting With Strong Opioids
• Study Design: Randomized controlled trial• Source of funding: Unknown• Participants: 100 patients• Inclusion Criteria:
– Cancer– Not eligible for disease oriented treatment– Home palliative care– >6/10 on VAS for last week

Slides available at www.aahpm.org
Starting With Strong Opioids
• Exclusion Criteria:– Impaired sensory or cognitive function– Predominately neuropathic pain– Previous opiates
• Intervention:– Grp A: WHO pain ladder– Grp B: Start with strong opioids– Both groups can get adjuvants

Slides available at www.aahpm.org
Starting With Strong Opioids
• Measurement– Daily
• Pain diary-intensity, general condition, side effects
– Once a week• Pain relief• Satisfaction with pain relief Y/N• Quality of life• Side effects
• Analysis: chi-square and t-tests

Slides available at www.aahpm.org
Starting With Strong Opioids
Group A Group B(n = 48) (n = 44)
Age 61.3 + 20.3 63.9 + 20.0
Sex %Male 62.5 56.8Female 37.5 43.2
Karnofsky 58.92 + 5.56 58.01 + 8.04
VAS 4.03 + 1.36 4.13 + 1.36

Slides available at www.aahpm.org
Starting With Strong Opioids
QOL change Pain Score change Nausea
A -16.55 -1.92 315
B -16.05 -2.61 437
P ns p=0.041 p=0.0001
* There was no significant difference in vomiting, constipation, GI bleeding, or mental confusion

Slides available at www.aahpm.org
Starting With Strong Opioids

Slides available at www.aahpm.org
Key Issues
• Is the question important?– Common clinical problem
• What are the results?– All patients had significant pain
reduction– Quicker pain relief with starting with
non-opiates

Slides available at www.aahpm.org
Key Issues
• Are the results valid?– Small study– Unclear about analgesic use– No controlling for co-morbidities– Poor measures

Slides available at www.aahpm.org
Key Issues
• Can I apply the results to my patients?
– Non-neuropathic, cancer pain– Young

Slides available at www.aahpm.org
Bottom Line
• In selected cancer patients presenting with severe pain, starting with strong opioids will lead to better pain relief.

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Case 2: Jerrold R (continued)
• Stage IV lung cancer • Presents to internist six months later
with persistent left arm pain (4/10)• Has received radiation to the arm• Is currently on long acting morphine,
monthly bisphosphonates, steroids, and a NSAID
• What can you do?

Slides available at www.aahpm.org
Background
• What is the role of co-analgesics in pain relief?– NSAID– Steroids– Acetaminophen
• Does adding acetaminophen to opiates improve pain relief in cancer patients?

Slides available at www.aahpm.org

Slides available at www.aahpm.org
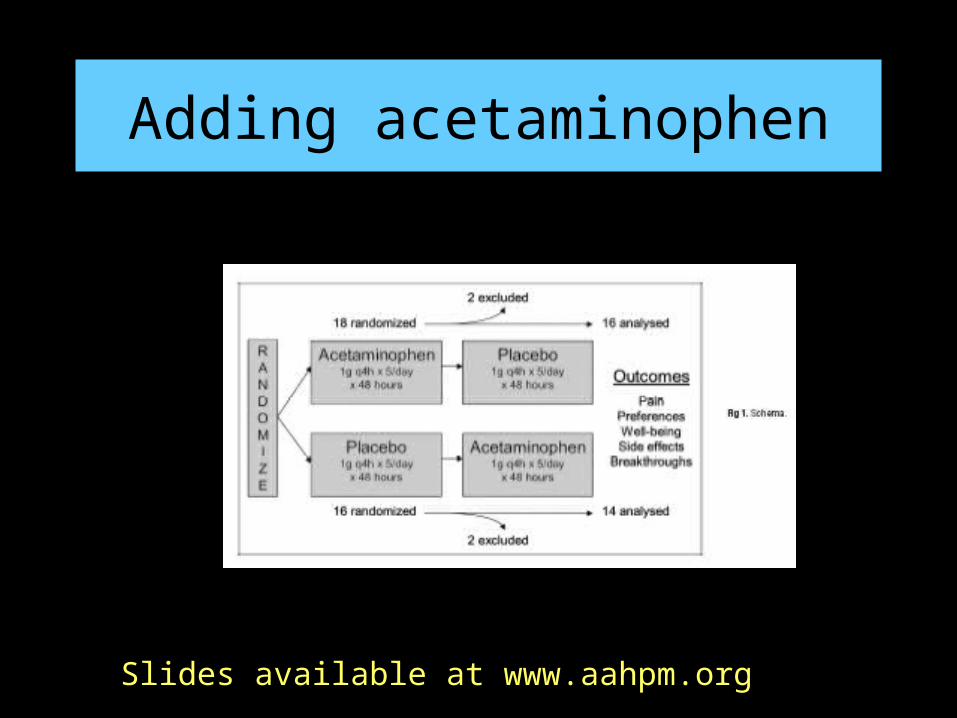
Adding Acetaminophen
• Study Design: RCT, placebo, crossover
• Source of Funding: Au Cancer Council Janssen
• Participants: 34 patients

Slides available at www.aahpm.org
Adding acetaminophen
• Exclusion Criteria:– Recent XRT– New chemotherapy– Neuropathic pain– Severe liver disease
.
Slides available at www.aahpm.org
Adding acetaminophen
.

Slides available at www.aahpm.org
Adding acetaminophen
• Primary outcome measure: – Pain as measured by 0-10 verbal scale and a 10-
cm VAS– Daily rating and at end of study preference
• Secondary measures– Breakthrough opiates– Well-being– Side effects

Slides available at www.aahpm.org
Adding acetaminophen
• Sample size• Analysis: ANOVA
– If not normal distribution then logit transformation

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Adding acetaminophen-Visual scale-pain

Slides available at www.aahpm.org
Adding acetaminophen-Verbal scale - pain

Slides available at www.aahpm.org
Adding acetaminophen-visual scale-well being

Slides available at www.aahpm.org
Key Issues
• Is the question important?– Common clinical problem
• What are the results?– Consistent decrease in pain and increase in
QOL if add acetaminophen– 30% had >1 point change on 0-10 scale for
both pain and well-being

Slides available at www.aahpm.org
Key Issues
• Are the results valid?– Small study– Problematic intervention– Short duration– Poor measures

Slides available at www.aahpm.org
Key Issues
• Can I apply the results to my patients?
– Consistent with other studies– Cheap and easy– Can stop if does not help

Slides available at www.aahpm.org
Clinical Bottom Line
“Acetaminophen improved pain and well-being without major side-effects in people with cancer and persistent pain despite a strong opioid regimen.”
It can be tried in patients with persistent pain

Slides available at www.aahpm.org“His final wish was that all his
medical bills be paid promptly.”

Slides available at www.aahpm.org
Case 3: Mary R
• 74 year old with severe COPD
• Has dyspnea at rest
• Current medications– Albuterol/Atrovent– Oxygen– Steroids

Slides available at www.aahpm.org
• Frustrated because dyspnea has made her life “miserable
• Is there anything else besides her current regimen that will help alleviate her dyspnea?
Mary R’s Case: continued
Slides available at www.aahpm.org
Opioids for Dyspnea: Background
• Dyspnea is a common symptom
• Dyspnea is subjective
• Can impair functional status
• Particularly difficult for caregivers to observe

Slides available at www.aahpm.org
Opioids for Dyspnea: Background
• Concern over adverse reactions
• Conflicting consensus guidelines
• Not enough good studies – Small sample numbers– Difficult to blind

Slides available at www.aahpm.org

Slides available at www.aahpm.org
• 8 day RCT crossover
• 20 mg of sustained release morphine versus placebo
• Primary outcome variable: dyspnea on day #4
Opioids for Dyspnea: Methods

Slides available at www.aahpm.org
Participants were recruited from outpatient clinics for respiratory, cardiac, general, and palliative medicine
Opioids for Dyspnea: Methods continued
Inclusion criteria
•Adults with dyspnea at rest despite “optimal treatment of reversible factors”
•Opioid naive
Exclusion criteria•Recent use of opioids
•Confusion
•Obtundation
•Adverse reactions to opioids
•History of substance misuse

Slides available at www.aahpm.org
Opioids for Dyspnea: Demographics

Slides available at www.aahpm.org
• 104 screened - 87 eligible
• 48 consented - 39 refused or too sick
• 10 withdrew - 5 in each group
Opioids for Dyspnea: Results

Slides available at www.aahpm.org
• Morphine better than placebo– Evening: Improvement of 9.5 mm (SD 19,
and P=0.006%)– Morning: Improvement of 6.6 mm (SD 15,
and P=0.011)
Opioids for Dyspnea: Results

Slides available at www.aahpm.org
Opioids for Dyspnea: Results continued
• No change in respiratory rates
• No difference in vomiting, confusion, sedation, or anorexia
• No sequence or period effects
• Sensitivity analysis showed benefit

Slides available at www.aahpm.org
Opioids for Dyspnea: Is this Question Important
• Yes, prevalence high and high level of suffering associated with this symptom. Suffocation difficult to tolerate for even short periods of time.

Slides available at www.aahpm.org
Opioids for Dyspnea:Are the results valid?
• Crossover design
• No washout period
• No blinding for constipation
• Blinding

Slides available at www.aahpm.org
Opioids for Dyspnea: Other supporting literature
• Meta analysis confirms that opioids are effective for dyspnea (Jennings et al, Thorax 2002; 57: 939-44).
• Cochran database systematic review again confirms that opioids are effective for treatment of dyspnea

Slides available at www.aahpm.org
Opioids for Dyspnea: Key issues
• Can I apply these results to my patient– Study included patients with dyspnea due
to many diseases– Included older patients– Dyspnea at rest

Slides available at www.aahpm.org
• Morphine is effective
• Small doses effective so concern over side effects may be exaggerated
Opioids for Dyspnea: Bottom line

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Case 4: Mary R. continued
• The patient did well after you started her on a low dose of sustained release morphine
• After about four months she is admitted with a COPD exacerbation
• While admitted she is found pulseless and the cardiac monitor indicates asystole and she is resuscitated for 15 minutes.

Slides available at www.aahpm.org
Mary R. continued
• She is “successfully” resuscitated and she regains her pulse and is sent to the intensive care unit
• You see her the next day and she is unresponsive and does not require any sedation on the ventilator
• The husband who is at the bedside asks you about her prognosis.
• What do you tell you the husband?

Slides available at www.aahpm.org
Prognosis after cardiac arrest: Background
• 500, 000 in hospital arrests• Public misunderstanding of hypoxic injury
after cardiac arrest (ER, Chicago Hope, Schiavo, fireman in Buffalo)
• Need information about expected level of recovery so appropriate decisions.
• The emotional, ethical, and financial aspects

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Cardiac arrest: Methods
• Study design: systematic review
• Source of funding: Griffen Rotman
• Outcome measures: precision and accuracy of physical findings to determine prognosis

Slides available at www.aahpm.org
Cardiac arrest: Methods
• Search strategy: Extensive MEDLINE, EMBASE, bibliography and abstracts from meetings search.
• Search terms: coma, cardiac arrest, prognosis, physical examination, sensitivity, specificity, and observer variation

Slides available at www.aahpm.org
Cardiac arrest: Methods
• Inclusion criteria for accuracy– Accuracy of physical exam – Outcome data for individual clinical
variables measured at discrete time intervals
• Exclusion criteria accuracy studies– Traumatic coma

Slides available at www.aahpm.org
Cardiac arrest: Methods
• Inclusion criteria for precision studies– Assessment of inter-observer agreement– Non-traumatic coma AND traumatic coma
• Exclusion criteria for precision studies– Not clear
Slides available at www.aahpm.org
Cardiac arrest: Methods
• Studies had outcome data for severe disability, vegetative state, and death
• Quality of study assessed by two “blinded” researchers– Level 1: Prospective with >100 subjects– Level 2: <100 subjects– Level 3: Retrospective chart reviews– Level 4: Non-consecutive patients

Slides available at www.aahpm.org
Table 2

Slides available at www.aahpm.org
Cardiac arrest: Methods
• Raw data used for positive and negative LR
• CPC 1 and 2 = good outcomes
• CPC 3, 4, and 5 = poor outcomes
• Summary LR if > 3 studies examined a clinical variable at same time after arrest

Slides available at www.aahpm.org
Cardiac Arrest: Results
• 5 articles of precision and 14 articles (11 studies) of accuracy – 11 accuracy studies
• 5 level 1• 3 level 2• 1 level 3• 2 level 4
– Heterogeneity in precision studies allowed only qualitative data

Slides available at www.aahpm.org
Cardiac Arrest: Results
• 5 studies of precision– Kappa: 0.36 -0.79– Variables
• GCS motor• GCS eye• GCS verbal• Pupil response• Oculo-cephalic response• Spontaneous Eye Movements• Brainstem reflexes

Slides available at www.aahpm.org
Cardiac Arrest: Results
• 1,914 survivors in accuracy studies
• Pre test probability of poor outcome = Percentage of the 1,914 that had bad outcome (self fulfilling prophesy)
• Random effects estimate of poor outcome was 77%

Slides available at www.aahpm.org
Cardiac Arrest: Results
Time Highest Pooled LR Clinical FindingOnset 1.7 no withdrawal to
pain
24 hr 12.9 no corneal reflex
72 hr 9.2 no motor
response

Slides available at www.aahpm.org
Cardiac Arrest: Are the results Valid
• Dichotomizing outcomes as good and poor
• Poor prognoses tend to be self fulfilling
• Diverse backgrounds in terms of demographics and co-morbidities

Slides available at www.aahpm.org
Cardiac Arrest: Key Issues
• Can I apply these results to my patients– High pooled LR from studies evaluating
accuracy– Non-traumatic coma

Slides available at www.aahpm.org
Is this Question Important?
• Yes– Families need accurate information to
make decisions especially when it revolves around discontinuation of therapies.

Slides available at www.aahpm.org
Clinical Bottom Line
• Immediately after arrest no clinical signs are helpful
• No clinical findings were found to have LR that predicted a good outcome
• Simple physical exam findings can strongly predict poor outcome in survivors of cardiac arrest

Slides available at www.aahpm.org

Slides available at www.aahpm.org
• Mary R dies
• Four weeks after Mary R’s death the husband is in your office
• Because you did such a great job in caring for her, her husband decides that you should be his primary care provider
Case 5: Mary R. continued

Slides available at www.aahpm.org
• The husband is clearly distraught and appears to have lost weight
• He says that this is the first time he has bothered to get dressed and leave his home since his wife’s death
• He wants to know if anything other than time will help him with the grieving process
Sonni M’s husband’s case

Slides available at www.aahpm.org
• Physicians may not be aware of the associated morbidity.
• Uncertainty on how to help grieving patients
• How much of the process is “normal” ?
• No consensus or guidelines on the many different techniques
Bereavement: Background

Slides available at www.aahpm.org

Slides available at www.aahpm.org
Bereavement Interventions: Methods
• Study Design: systematic review
• Source of Funding: CHOP and Agency for Health Care Research and Quality
• Intervention: Any study evaluating “bereavement care interventions”

Slides available at www.aahpm.org
Bereavement Interventions: Methods continued
• Search Strategy– Traditional as well as complementary and
alternative literature– Databases from many disciplines– Primary search terms: bereaved,
bereavement, and grief

Slides available at www.aahpm.org
Bereavement Interventions: Methods continued
• Inclusion Criteria: Treatment of bereaved individuals AND evaluation of the method used as the intervention– Initial search = 737 citations
• After title reviews: 243 citations• After abstract review: 87 articles• 87 articles were reviewed: 74 included in this
paper

Slides available at www.aahpm.org
Bereavement Interventions: Methods continued
• Review organized on the basis of the social framework used to implement the intervention

Slides available at www.aahpm.org
Bereavement Interventions: Methods continued
• Structured therapeutic relationship model– Pharmacotherapy– Support groups or counseling– Psychotherapy
• Cognitive-behavioral therapy• Psychodynamic therapy• Psychoanalysis• Behavioral therapy• Interpersonal therapy
• Systems-oriented interventions

Slides available at www.aahpm.org
Bereavement Interventions: Results
• Pharmacotherapy – Effective for insomnia and depression– Mixed effect on bereavement intensity

Slides available at www.aahpm.org
Bereavement Interventions: Results
• Support Groups– 39 studies
• 23 had controls and 15 had randomization• 29 were professionally led support groups• Great variation in number of sessions, targeted
population, and format

Slides available at www.aahpm.org
Bereavement Interventions: Results
• Support groups continued.– Spontaneous improvement noted in
several studies– No summary conclusion possible– No harm
Slides available at www.aahpm.org
Bereavement Interventions: Results
• Pharmacotherapy relieves depression and insomnia but not grief
• No conclusions regarding one type of intervention versus another

Slides available at www.aahpm.org
Bereavement Interventions: Are the results valid?
• Outcomes and measures to evaluate outcome heterogenous
• Internal and external validity poor
• Great variety in the treatments used (Apples versus promegranates)

Slides available at www.aahpm.org
Clinical Bottom line
• Highly prevalent and distressing
• There is lack of evidence to make recommendations
• More rigorous studies are needed

Slides available at www.aahpm.org
Bereavement: Key issues
• Can I apply these results to my patients– Unable to recommend one treatment
versus another– Pharmacotherapy can help with depression
and sleep disorders

Slides available at www.aahpm.org
“It’s a medical miracle you made it through that last medical miracle.”

Slides available at www.aahpm.org
Case 6
• Charlotte P is an 83 y/o retired lawyer with class IV CHF, moderate dementia and rapid functional decline.
• She was admitted with worsening dyspnea, narrowly avoiding intubation
• After one week, despite thorough testing and treatment trials, she feels no better.

Slides available at www.aahpm.org
Charlotte P. (Cont)
• The patient and her family recognize that she is at the end of her life.
• They want her to go home, yet she receives benefit from some treatments provided in the hospital.
• Everyone wonders what setting would be best for her.

Slides available at www.aahpm.org
Background
• Place of death has changed dramatically over the past century– All people used to die at home– Then shifted to most deaths in hospital– Now shifting back (dramatically in some states)
• 50% die in hospital, 2001 (range: 33-65%)
• Many people use place of death as a proxy for quality of death, but is it?

Slides available at www.aahpm.org
Background (cont.)
• One national study suggested that place of death less important than quality of death - having needs met
• Very little data on relationship between site of death and quality.

Slides available at www.aahpm.orgSlides available at www.aahpm.org

Slides available at www.aahpm.org
Family Perspectives:Methods
• Study Design: mortality follow-back survey• Source of Funding: RWJ Foundation• Participants:
– 1578 family members or close friends of decedents who died in 2000
• Inclusion Criteria– Identified through probability sampling of state death certificates
• Exclusion Criteria– States that would not allow sampling– Decedents under age 18– Death from trauma

Slides available at www.aahpm.org
Family Perspectives:Methods
• Measures– Telephone interview
• Quality of care in last place of life• Unmet needs for pain, dyspnea, emotional support• Shared decision-making• Treated with respect
• Analysis– Descriptive 2, logistic regression

Slides available at www.aahpm.org
Family Perspectives:Results
• Site of death– Hospital or nursing home 69%
• Nursing Services (of those at home)– No nursing services 36% (37% of these
functionally impaired)– Home nursing 12%– Home hospice 52%
• Cancer more likely hospice• Heart disease more likely no formal services

Slides available at www.aahpm.org
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Slides available at www.aahpm.org
Family Perspectives:Results• Not any or enough help with:
– Pain 24%– Dyspnea 22%– Emotional support 50%
• Recipients of home hospice care had lower rates of unmet needs compared with others
• Home with home health services did worse on several parameters c/w other settings

Slides available at www.aahpm.org
Family Perspectives:Results
• Nursing homes did worse on pain, being treated with respect (OR 1.6 and 2.6)
• Overall satisfaction highest in hospice (71% vs. 50% rated “excellent”

Slides available at www.aahpm.org
Key Issues: Is the Question Important?
• Remarkably little large scale data describing end of life experience
• Little rigorous data supporting/refuting value of hospice
• Significant implications for clinical decision-making and design of health care services

Slides available at www.aahpm.org
Key Issues: What are the Results? Are they valid?
• Increasing #’s of patients die in nursing homes, but quality is lacking in this setting
• Home death not a proxy for quality, unless hospice involved
• Limitations:– Non-randomized, selection bias (by state etc)– Non-response bias (favored Caucasians)– Family members may not be accurate observers

Slides available at www.aahpm.org
Key Issues:Can I Apply this to my Patients?
• Probably as generalizable data as we will get on a national scale
• Makes one aware of limitations in EOL care in nursing homes, home health nursing

Slides available at www.aahpm.org
Bottom Line
• Many dying patients have unmet needs
• Targeted systems of care for dying patients are necessary for highest quality care
• Mortality follow-back is a useful methodology in EOL research


Slides available at www.aahpm.org
Case 7
• Mike M is a 55 y/o social scientist with peritoneal mesothelioma
• He first presented with progressive ascites
• After surgical debulking and infusion of heated chemotherapy, he achieved complete symptom relief

Slides available at www.aahpm.org
Mike M. (Cont)
• One year later he had evidence of recurrence by CT/PET, but felt well, working out daily and traveling extensively
• In speaking with him, his physicians struggle with how much information about his prognosis to share….
Slides available at www.aahpm.org
Background
• Although we know something about preferences for bad news, much less data on prognosis
• MD’s tend not to communicate about prognosis, or to do so vaguely– And, have an optimistic bias
• Worried about balancing truth and hope

Slides available at www.aahpm.org
Background (cont.)
• Patients overestimate prognosis• Conflicting data on preferences for
information:– Clear majority want detailed info on
disease– But…not sure if want prognostic info
• Not clear what pts with advanced disease want to hear about prognosis

Slides available at www.aahpm.org
Slides available at www.aahpm.org
Patient Preferences for Communication:Methods
• Study Design: cross-sectional survey• Source of Funding: NSW Cancer Council• Participants:
– 126 Australian advanced cancer pts (from 218)– 30 oncologists (from 106)
• Inclusion Criteria– All oncologists in New South Wales– Patients > age 18
• Metastatic cancer diagnosed 6 wks to 6 mos earlier• English speaking
• Exclusion Criteria– Psychiatric disease

Slides available at www.aahpm.org
Patient Preferences for Communication:Methods
• Measures– Written survey
• 2 gender-specific hypothetical scenarios
• Prognostic information desired
• Pref presentation of survival stats (e.g., words, #’s)
• When to discuss, and who initiates
• Demographics and depression/anxiety scores
• Analysis– Descriptive 2, ANOVA, logistic regression

Slides available at www.aahpm.org
Patient Preferences for Communication:Results
• 54% Male
• 25% breast ca, 18% colorectal, 15% prostate, 10% lung, 30% other
• 95-99% wanted common information related to side effects, symptoms, treatment
• Most wanted info on survival duration– 65% 1-year survival; 80% 5-year survival
• Words/numbers > pie charts/graphs

Slides available at www.aahpm.org
Preferences for Communication - Results• 59% want to discuss survival when first learn
metastatic
• 1/3 wanted to discuss dying/pall care when diagnosed; 1/3 later– 24% only when they ask for it
– Patients with children more likely to want to wait
• More depressed more likely to want to discuss survival
• Worse prognosis less desiring to discuss

Slides available at www.aahpm.org
Key Issues: Is the Question Important?
• Clinicians face this issue frequently - much debate among them about what to say
• Patient experience and satisfaction can be dependent upon how information is shared

Slides available at www.aahpm.org
Key Issues: What are the Results? Are they valid?
• Most patients want information about symptoms and treatment; desire for prognostic information highly variable
• High refusal rate among both oncologists and patients threatens validity
• Do hypothetical scenarios mimic real life?

Slides available at www.aahpm.org
Key Issues:Can I Apply this to my Patients?
• Australian sample (85% Anglo-Saxon; remainder likely Asian/Aboriginal)
• Western, English-speaking healthcare system

Slides available at www.aahpm.org
Bottom Line
• Patient preferences for prognostic information are highly variable
• Cannot predict preferences
• Must negotiate the sharing of information– Ask first!– How much, and when to tell?

Slides available at www.aahpm.org
Pearls for Finding High Quality Evidence in Palliative Care
• Traditional randomized controlled trials– Look at the data differently– Study the survival curves
• Searching Medline– Keywords:
• Palliative care• Terminal Care• Attitude to death• Terminally ill• Life support care• Hospices

Slides available at www.aahpm.org
Conclusions
• Palliative Care is a growing field with a growing evidence base
• Although challenges exist, when faced with a clinical problem, first go to the literature
• Data is available from a variety of sources– Journals (J Pall Med, J Pain Sympt Man)– PC FACS, Cochrane Collaborative– Fast Facts– Textbooks (Oxford Textbook of Palliative Care)– Organizations (AAHPM)
















![1877.] Medicine. 241 MEDICINE.](https://static.fdocuments.in/doc/165x107/6248decce7f255195063a334/1877-medicine-241-medicine.jpg)
