slide AF.pptx
36
CASE REPORT APRIL 2015 By :Givaneshine Nadarajah Supervisor : dr.Akhtar Fajar M,Sp.JP.FIHA CHF NYHA II ec Atrial Fibrillation Medical Faculty of Hasanuddin University, Makassar 2015
-
Upload
gladys-ailing -
Category
Documents
-
view
213 -
download
1
Transcript of slide AF.pptx

CASE REPORTAPRIL 2015
By :Givaneshine Nadarajah
Supervisor : dr.Akhtar Fajar M,Sp.JP.FIHA
CHF NYHA II ec Atrial Fibrillation
Medical Faculty of Hasanuddin University, Makassar 2015

PATIENT IDENTITY
• Name : Madam ML• Sex : Female• Age : 68 y.o.• Address : Toraja• Job : Housewife• Status : Married• Date Administrated : 27th April 2015• MR : 709886• Room : Lontara 1 AB K4 B1

Chief complaint : Shortness of breath(SOB)History of present illness :• Suffered since 2 days before admitted. SOB is described as
feeling heavy while breathing. SOB worsen during activities(+) and while lying down(+). Patient have to sleep with more than 1 pillow(+). Patient had never woke up during the night because of thightness(-). Another current complaint is suddenly feeling palpitations since last year. Chest pain(-), fever(-), nausea(-), vomit(-), and heartburn(-). Defecation and urination within normal limits.

HISTORY TAKINGHistory of past/previous illness:• History of high blood pressure(+) since 5 years ago, irregular treatment• History of PND (-)• History of leg swelling (-)• History of diabetes(-)• History of smoking (-)• History of alcohol consumption (-)• History of lung disease (-)• History of cyanosis at birth denied• Family with the same disease (-)• History of hospital admission(-)

PHYSICAL EXAMINATION
• Moderate illness/ well-nourished/ conscious (GCS 15 : E4M6V5)General condition
• Blood pressure : 150/100 mmHg
• Heart rate : 114 x/min• Respiratory rate : 24 x/min• Temperature : 36,5oC
Vital Signs

HEAD AND NECK• No anemic, no icteric• No cyanosis • JVP R+2 cm H20
LUNG• Inspection : Symmetry left=right• Palpation : Mass (-), no tenderness• Percussion : Sonor• Auscultation : Vesicular
Rhonchi +/+ Mediobasal• Wheezing -/-

HEART• Inspection : Ictus cordis not visible• Palpation : Ictus cordis not palpable, thrill (-)• Percussion:
• Upper border 2nd ICS sinistra• Right border 4th ICS linea parasternalis dextra• Left border 5th ICS linea axillaris anterior sinistra
• Auscultation : Heart sound I/II irregular, murmur (-)
ABDOMEN• Inspection : Flat, follows breath movement• Auscultation : Peristaltic (+), normal• Palpation : Liver and spleen not palpable• Percussion : Tympani, ascites (-)
EXTREMITIES• No edema

RISK FACTORS
• Modified risk factor– Hypertension
• Non-modified risk factor– Female– Age 68 y.o

ELECTROCARDIOGRAPHY
o Sinus tachycardi, irregular.
o Heart rate:150 bpm
o PR interval : difficult to assess
o P Wave: difficult to assess
o QRS rate: 0.12s
o ST segment: no elevation
o T wave: Normal
Conclusion :– Atrial fibrillation– HR 110 bpm, normoaxis Atrial fibrillation Rapid Ventricular Response


LABORATORY FINDINGSRESULT NORMAL RESULT NORMAL
WBC 9,0 [10^3/uL] 4.0-10.0 TROPONIN-T <0,02 <0,05
RBC 5,23 [10^6/uL] 4.00-5.00 GDS 109 80-180
HGB 14,2 [g/dL] 12.0-16.0 ALBUMIN 3,4 3,5-5,0
HCT 38,1 [%] 37.0-48.0 UREUM 31 10-50
PLT 207 [10^3/uL] 150-400 CREATININE 0,52 L(<1.3), P(<1,1)
Na 140 136-145 SGOT 26 <38
K 3,7 3.5-5.1 SGPT 32 <41
Cl 108 97-111 HBsAG Non reaktif Non reaktif
CK 59 [U/L] L(<190), P(<167) Anti HCV Non reaktif Non reaktif

Chest X-ray
Conclusion: • Cardiomegaly with
signs of pulmonary edema
• Pleural effusion bilateral

DIAGNOSIS
Congestive Heart Failure NYHA Class II ec Atrial Fibrillation-CHF:
-major criteria: acute pulmonary edema, radiographic cardiomegaly,-minor criteria: dyspnea on ordinary exertion, tachicardia
-NYHA class 2:-Slight limitation of physical activity, in which ordinary physical activity leads to fatigue, palpitation, dyspnea or anginal pain, comfortable at rest
-Atrial Fibrillation:-Symptoms: palpitation-ECG: atrial fibrillation
Hypertension Grade I-BP: 150/100mmHg

• Bed rest• Fluid restriction• Low salt diet• Oxygen 2-4 lpm/ nasal kanul• Furosemide 40mg/24 jam/ Intravena• Digoxin 0.25/24 jam/oral• Captopril 12,5mg/8 jam/oral• Simarc 2mg/24jam/oral
Management

DEFINITION
• An irregular and often rapid heart rate• Commonly causes poor blood flow to the body. • The heart's two upper chambers (the atria) beat
chaotically and irregularly out of coordination with the two lower chambers (the ventricles) of the heart.

PREVALENCY
• Estimates of AF in Asia through 2014 suggest that 12,210,000 (0.4%) people in the Asia-Pacific have atrial fibrillation
• AF is most prevalent in South Korea, Philippines, Malaysia and Indonesia, affecting 0.7% of the populations
• Hypertension is the most common CV risk factor across the Asian region

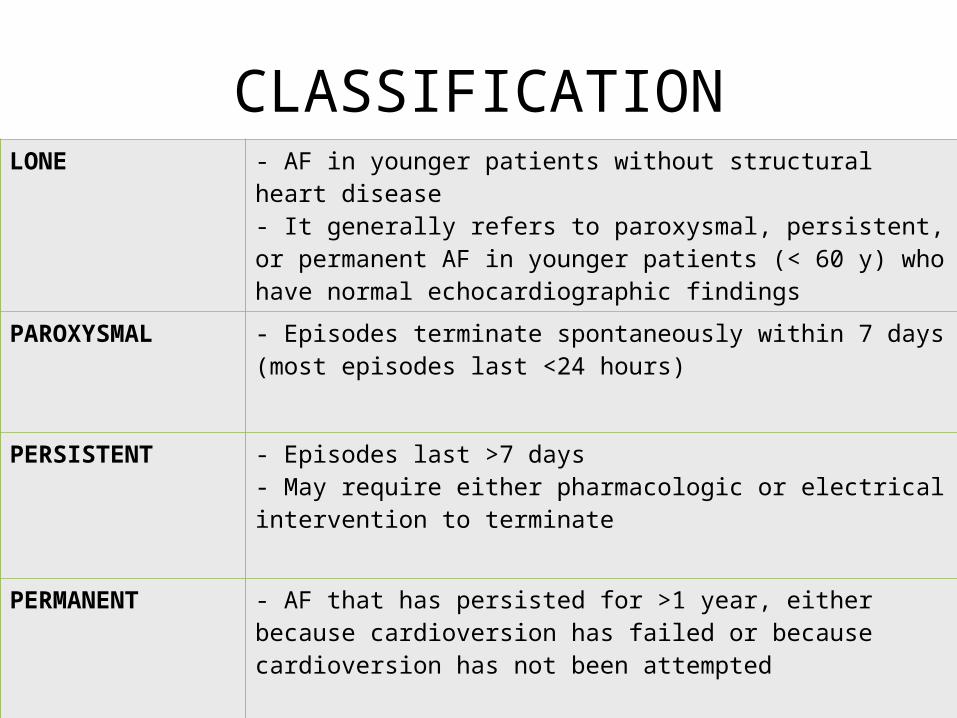
CLASSIFICATIONLONE - AF in younger patients without structural heart disease
- It generally refers to paroxysmal, persistent, or permanent AF in younger patients (< 60 y) who have normal echocardiographic findings
PAROXYSMAL - Episodes terminate spontaneously within 7 days (most episodes last <24 hours)
PERSISTENT - Episodes last >7 days- May require either pharmacologic or electrical intervention to terminate
PERMANENT - AF that has persisted for >1 year, either because cardioversion has failed or because cardioversion has not been attempted

ETIOLOGYCardiac causes of AF Non-cardiac causes of AF
Common cardiac causes- Ischemic heart disease- Rheumatic Heart Disease- Hypertension
Less common cardiac causes:- Cardiomyopathy or heart muscle disease- pericardial disease- Atrial septal defect-
- Acute infection especially pneumonia- Electrolyte depletion- Lung carcinoma- Pulmonary embolism- Thyrotoxicosis


PATHOPHYSIOLOGY

SIGN AND SYMPTOMS

PHYSICAL EXAMINATIONVital signs• irregularly irregular pulse and tachycardic (HR: 110-140) Head and neck• Examination of the head and neck may reveal exophthalmos, thyromegaly,
elevated jugular venous pressures, or cyanosis. Pulmonary• Evidence of heart failure (eg, rales, pleural effusion). • Wheezes or diminished breath sounds are suggestive of underlying
pulmonary disease (eg, COPD, asthma).

Cardiac• Thorough palpation and auscultation are necessary to
evaluate for valvular heart disease or cardiomyopathy. A displaced point of maximal impulse or S3suggests ventricular enlargement and elevated left ventricular pressure. A prominent P2 points to the presence of pulmonary hypertension.
Abdomen• The presence of ascites, hepatomegaly, or hepatic capsular
tenderness suggests right ventricular failure or intrinsic liver disease. Left upper quadrant pain may suggest splenic infarct from peripheral embolization.

Lower extremities• Examination of the lower extremities may reveal cyanosis,
clubbing, or edema. A cool or cold pulseless extremity may suggest peripheral embolization, and assessment of peripheral pulses may lead to the diagnosis of peripheral arterial disease or diminished cardiac output.
Neurologic• Signs of a transient ischemic attack or cerebrovascular
accident may be discovered. Evidence of prior stroke and increased reflexes is suggestive of hyperthyroidism.
• amined for carefully.

ADDITIONAL EXAMINATION
• Laboratorium– CBC count (looking for anemia, infection)
– Serum electrolytes and BUN/creatinine (looking for electrolyte disturbances or renal failure)
– Cardiac enzymes - CK and/or troponin level (to investigate myocardial infarction as a primary or secondary event)
– BNP (to evaluate for CHF)– D-dimer (if the patient has risk factors to merit a
pulmonary embolism workup)– Thyroid function studies (looking for thyrotoxicosis, a rare,
but not-to-be-missed, precipitant)

• Chest radiography– usually normal. – However, chest radiography may provide evidence
of CHF as well as signs of lung or vascular pathology (eg, pulmonary embolism, pneumonia).

ECG features of AF
• Irregularly irregular rhythm• Heart rate tachycardia• No P waves• Absence of an isoelectric baseline• Variable ventricular rate• QRS complexes usually <120ms unless pre-
existing bundle branch block, accessory pathway, or rate related aberrant conduction

MANAGEMENT
Therapeutic goals in patient with AF
Reduce thromboembolic
risk
Restore and maintain sinus
rhythm (Rhythm control)
Control ventricle rate during AF (Rate control)

Rate Control
• Target heart rate: 110 bpm• Beta blockers (preferably the "cardioselective"
beta blockers such as metoprolol, atenolol, bisoprolol, nebivolol)
• Non-dihydropyridine calcium channel blockers (e.g., diltiazem or verapamil)
• Cardiac glycosides (e.g., digoxin)
Rhytm Control
• Cardioversion is the attempt to switch an irregular heartbeat normal heartbeat– Electrical cardioversion involves the restoration of
normal heart rhythm through the application of a DC electrical shock
– Chemical cardioversion is performed with drugs:• Amiodarone, Dofetilide, Flecainide, Ibutilide,
Propafenone, Quinidine

Anti Coagulant
• Anticoagulants are used to prevent thromboembolic complications.– WarfarinReducing the risk of thrombus formation.

SURGERY
• Catheter Ablation– At the end of the catheter contain electode which
terminates ectopic focus.• Maze procedure– an effective invasive surgical treatment that is
designed to create electrical blocks or barriers in the atria of the heart, forcing electrical impulses that stimulate the heartbeat to travel down to the ventricles.
• Artificial pacemaker

PREVENTION
• Reduce risk by changing some behaviors(life style) – Cutting down intake of alcohol. – Stop smoking and using nicotine products, and
avoid over-the-counter medications that have stimulant properties.
– Make sure any health conditions are being properly treated.
– Work to reduce stress and maintain a healthy weight.

COMPLICATION
• Stroke• Heart failure
PROGNOSIS
• Treatment can often control this disorder. Many people with atrial fibrillation do very well.
• Atrial fibrillation tends to return and get worse. It may come back even with treatment.
• Clots that break off and travel to the brain can cause a stroke.