Slan 2007 survey of lifestyle attitudes and nutrition in ireland

Royal College of Surgeons in Irelande-publications@RCSI
Psychology Reports Department of Psychology
1-1-2009
SLAN 2007: Survey of Lifestyle, Attitudes andNutrition in Ireland. Smoking Patterns in Ireland:Implications for policy and servicesRuairi BrughaRoyal College of Surgeons in Ireland
Nuala TullyRoyal College of Surgeons in Ireland
Patrick DickerRoyal College of Surgeons in Ireland
Emer ShelleyRoyal College of Surgeons in Ireland
Mark WardRoyal College of Surgeons in Ireland
See next page for additional authors
This Report is brought to you for free and open access by the Departmentof Psychology at e-publications@RCSI. It has been accepted for inclusionin Psychology Reports by an authorized administrator of e-publications@RCSI. For more information, please contact [email protected].
CitationBrugha R, Tully N, Dicker P, Shelley E, Ward M, McGee H. SLAN 2007 : Survey of lifestyle, attitudes and nutrition in Ireland.Smoking patterns in Ireland : implications for policy and services. Commissioned by and copyright of the Department of Health andChildren. Conducted by the Royal College of Surgeons in Ireland, Economic and Social Research Institute, University College Corkand National University of Ireland Galway.
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by e-publications@RCSI

AuthorsRuairi Brugha, Nuala Tully, Patrick Dicker, Emer Shelley, Mark Ward, and Hannah McGee
This report is available at e-publications@RCSI: http://epubs.rcsi.ie/psycholrep/12

— Use Licence —
Attribution-Non-Commercial-ShareAlike 1.0You are free:• to copy, distribute, display, and perform the work.• to make derivative works.Under the following conditions:• Attribution — You must give the original author credit.• Non-Commercial — You may not use this work for commercial purposes.• Share Alike — If you alter, transform, or build upon this work, you may distribute the resulting work onlyunder a licence identical to this one.For any reuse or distribution, you must make clear to others the licence terms of this work. Any of theseconditions can be waived if you get permission from the author.Your fair use and other rights are in no way affected by the above.This work is licenced under the Creative Commons Attribution-Non-Commercial-ShareAlike License. Toview a copy of this licence, visit:URL (human-readable summary):• http://creativecommons.org/licenses/by-nc-sa/1.0/URL (legal code):• http://creativecommons.org/worldwide/uk/translated-license
This report is available at e-publications@RCSI: http://epubs.rcsi.ie/psycholrep/12

SLÁNSurvey of Lifestyle, Attitudes and Nutrition in IrelandSmoking Patterns in Ireland:Implications for policy and services
DEPARTMENT OF HEALTH AND CHILDREN, 2009
2007

This report should be cited as follows:
Brugha, R., Tully, N., Dicker, P., Shelley, E., Ward, M. and McGee, H. (2009) SLÁN 2007: Survey of
Lifestyle, Attitudes and Nutrition in Ireland. Smoking Patterns in Ireland: Implications for policy and
services, Department of Health and Children. Dublin: The Stationery Office.
Copyright © Minister for Health and Children, 2009
Department of Health and Children
Hawkins House
Hawkins Street
Dublin 2
Tel: +353 (0)1 635 4000
Fax: +353 (0)1 635 4001
E-mail: [email protected]
Web: www.dohc.gov.ie
Published by The Stationery Office, Dublin
All rights reserved. No part of this publication may be
reproduced, stored in a retrieval system, or transmitted,
in any form or by any means, electronic, mechanical,
photocopying, recording or otherwise, without the prior
permission in writing of the copyright holder.
For rights of translation or reproduction, applications should be
made to the Head of Communications, Department of Health and Children,
Hawkins House, Hawkins Street, Dublin 2, Ireland

The SLÁN 2007 ‘Smoking Patterns in Ireland’ Report is available to download from www.slan07.ie
The authors of this report are:
Ruairí Brugha, Nuala Tully, Patrick Dicker, Emer Shelley, Mark Ward and Hannah McGee
Royal College of Surgeons in IrelandEconomic and Social Research InstituteUniversity College, CorkNational University of Ireland, Galway
The SLÁN 2007 report is available to download as a PDF from www.slán07.ie
Karen Morgan, Hannah McGee, Dorothy Watson, Ivan Perry, Margaret Barry, Emer Shelley,
Janas Harrington, Michal Molcho, Richard Layte, Nuala Tully, Eric van Lente, Mark Ward,
Jennifer Lutomski, Ronan Conroy and Ruairí Brugha.
Royal College of Surgeons in Ireland
Economic and Social Research Institute
University College, Cork
National University of Ireland, Galway
Slan Report 07_FINAL ART4.indd Sec3:iii 28/04/2008 15:44:24
The SLÁN 2007 report is available to download as a PDF from www.slán07.ie
Karen Morgan, Hannah McGee, Dorothy Watson, Ivan Perry, Margaret Barry, Emer Shelley,
Janas Harrington, Michal Molcho, Richard Layte, Nuala Tully, Eric van Lente, Mark Ward,
Jennifer Lutomski, Ronan Conroy and Ruairí Brugha.
Royal College of Surgeons in Ireland
Economic and Social Research Institute
University College, Cork
National University of Ireland, Galway
Slan Report 07_FINAL ART4.indd Sec3:iii 28/04/2008 15:44:24

iv
Reports based on the SLÁN 2007 survey
Barry, M.M., Van Lente, E., Molcho, M., Morgan, K., McGee, H., Conroy, R., Watson, D., Shelley,
E. and Perry, I. (2009) SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland.
Mental Health and Social Well-being Report, Department of Health and Children. Dublin: The
Stationery Office.
Brugha, R., Tully, N., Dicker, P., Shelley, E., Ward, M. and McGee, H. (2009) SLÁN 2007: Survey
of Lifestyle, Attitudes and Nutrition in Ireland. Smoking Patterns in Ireland: Implications for
policy and services, Department of Health and Children. Dublin: The Stationery Office.
Harrington, J., Perry, I., Lutomski, J., Morgan, K., McGee, H., Shelley, E., Watson, D. and Barry,
M. (2008) SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. Dietary Habits of
the Irish Population, Department of Health and Children. Dublin: The Stationery Office.
Molcho, M., Barry, M., Van Lente, E., McGee, H., Watson, D. and Perry, I. (2009) SLÁN 2007:
Survey of Lifestyle, Attitudes and Nutrition in Ireland. Injuries in Ireland: An overview of
medically attended injuries, Department of Health and Children (forthcoming).
Morgan, K., McGee, H., Watson, D., Perry, I., Barry, M., Shelley, E., Harrington, J., Molcho, M.,
Layte, R., Tully, N., Van Lente, E., Ward, M., Lutomski, J., Conroy, R. and Brugha, R. (2008)
SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. Main Report, Department
of Health and Children. Dublin: The Stationery Office.
Morgan, K., McGee, H., Ward, M., Dicker, P., Brugha, R. and Shelley, E. (2009) SLÁN 2007:
Survey of Lifestyle, Attitudes and Nutrition in Ireland. Alcohol in Ireland: A profile of drinking
patterns, drinking-related harm and challenges of assessment from SLÁN 2007, Department
of Health and Children (forthcoming).
Ward, M., McGee, H., Morgan, K., Van Lente, E., Layte, R., Barry, M., Watson, D. and Perry, I.
(2009) SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. ‘One Island – One
Lifestyle?’ Health and lifestyles in the Republic of Ireland and Northern Ireland: Comparing
the population surveys SLÁN 2007 and NIHSWS 2005, Department of Health and Children.
Dublin: The Stationery Office.

v
CONTENTS
Reports based on the SLÁN 2007 survey iv
Acknowledgements vi
Executive Summary 1
Key findings on smoking 1
Policy Conclusions and Recommendations 2
1. Introduction 3
2. Smoking Patterns in Ireland 5
Overall smoking rates 5
Smoking rates among young women and by social class 6
Young people and smoking 6
Trends in smoking rates across SLÁN 1998, 2002 and 2007 8
Evidence of smoking trends from Office of Tobacco Control 9
Smoking and occupational categories 10
Smoking, social class and socio-economic effects 11
International comparisons 11
Exposure to smoking at home and at work 12
Attendance at primary care and smoking cessation advice from health professionals 12
GPs – An under-utilised resource for supporting smoking cessation 14
Smokers attending GPs – Opportunities for interventions 15
Attempts to quit 15
Quitting aids 16
Why quitting efforts fail, especially among women 16
Smoking – A multifaceted health issue 17
International efforts to tackle smoking: How is Ireland doing? 19
3. Conclusions 21
References 23

vi
ACkNOwLEDgEMENTS
We thank all who contributed to the 2007 Survey of Lifestyle, Attitudes and Nutrition (SLÁN) in Ireland. In particular, we are grateful to over 10,000 members of the public who gave of their time to complete the survey.
We acknowledge the SLÁN 2007 Consortium members and everybody who helped with survey planning, analysis and interpretation, together with interviewers from Amárach Consulting and interviewers, field support and data entry staff from the Economic and Social Research Institute’s Survey Unit who collected and processed the main survey information.
As a research team, we thank the Department of Health and Children in Dublin, particularly Mr. Brian Mullen and the staff of the Health Promotion and Policy Unit, for the opportunity to conduct the SLÁN 2007 survey. Input from the SLÁN 2007 Management and Advisory Groups was much appreciated during the project, in particular the coordinating role of Mr. Robbie Breen of the Health Promotion and Policy Unit.
Professor Hannah Mcgee (SLÁN 2007 Principal Investigator), and Professor Ruairí Brugha
Division of Population Health SciencesRoyal College of Surgeons in Ireland, Dublin
on behalf of the SLÁN 2007 Consortium

1
ExECuTIvE SuMMARy
kEy FINDINgS ON SMOkINg
• SLÁN 2007 findings are based on face-to-face interviews carried out with 10,364 randomly selected adults, aged 18 years and older, representative of the population of the Republic of Ireland (Morgan et al, 2008).
• Almost half of all respondents had smoked cigarettes at some point in their lives and 29% reported being current smokers. Smoking was more common among younger adults: 35% of those aged 18-29 and 37% among those in lower social class groups (SC 5-6).
• Overall, rates of smoking decreased from 33% in 1998 to 27% in 2002, with similar rates of reduction for men and women, across all ages and all social class groups. There was no significant change in smoking rates between 2002 and 2007 (29%).
• While more men than women smoked in 2007 (31% compared to 27%), more men than women had succeeded in quitting (23% compared to 16%). Lung cancer incidence rates continue to increase in women, while beginning to fall among men.
• Women were more likely than men to fear negative consequences of quitting smoking, such as gaining weight.
• A recent survey of Irish children aged 9-17 years – the Health Behaviour in School-aged Children (HBSC) Survey 2006 – showed a widening gap between 15-17 year-old boys and girls: girls were more likely to smoke than their male counterparts of similar age and this was apparent across social classes (girls SC 1-2: 24%; SC 3-4: 30%; SC 5-6: 28%; compared to boys SC 1-2: 18%; SC 3-4: 22%; SC 5-6: 23%).
• On the subject of giving up smoking, 9% of smokers were actively trying to quit; 17% were planning to quit; 33% were thinking about quitting but had no plans; and 41% were not thinking of quitting. Younger respondents and those in higher social class groups (SC 1-2) were most likely to have attempted to quit in the last year.
• Most respondents had some rules in their homes about smoking – almost 60% did not allow smoking anywhere inside their home, with an additional 23% reporting that smoking was only allowed in certain places or at certain times.
• Three-quarters of smokers and non-smokers had attended a GP in the previous year. Only 38% of current smokers who attended a GP or other health professional in the last year reported that the professional had discussed quitting smoking with them during the consultation. Smokers who had medical cards were more likely to have had such a discussion (45%) compared to smokers without medical cards (34%).
• There was a strong association between negative mental health and smoking. Those who smoked were 2-3 times more likely than those who did not smoke to report psychological distress or to be assessed as having a generalised anxiety disorder.
2
SLÁN 2007: Smoking Patterns in Ireland
POLICy CONCLuSIONS AND RECOMMENDATIONS
Success• Ireland's workplace smoking ban, introduced in 2004, has been successful in achieving
improved working conditions and significant reductions in the secondary damage caused to employees in the workplace due to passive smoking. SLÁN 2007 further confirms that the 'workplace rules' have been adopted by a majority of the population in their homes.
Challenge• While Ireland was rated 1st in Europe on a tobacco control scale in 2005, progress in
introducing further effective control measures and in sustaining downward smoking trends has since stalled.
Conclusions• Particular policy attention is warranted to combat higher rates of smoking among girls in their
late teenage years and among young women in lower social class groups.
• Smokers seeking employment and those in particular types of employment with high smoking rates could be targeted with location-specific smoking cessation supports and interventions. These approaches need to take into account that socio-economic deprivation may reinforce smoking.
• The finding that opportunities are missed for helping smokers to quit when they visit their GP, or other health professionals, warrants exploration. Incentives and support structures need to be in place to enable healthcare workers to deliver quitting interventions.
• Nicotine replacement aids should be freely available to all smokers on time-limited prescriptions as one component of a primary care-led smoking cessation strategy. Increasing taxes on cigarettes could make this a cost-free measure for Government if cigarette tax levels are harmonised with neighbouring jurisdictions.
• Smoking cessation interventions, as part of health promotion campaigns, need to build on an evidence base that points to the need for gender-sensitive approaches. Women are more vulnerable due to their fears of negative consequences from quitting, such as weight gain, and may be less likely to respond successfully to cessation interventions.
• Smoking is often one part of a constellation of behaviours and mental states. Smoking links with excess alcohol intake, lack of physical activity, mental health problems and poor quality of life. Multifaceted interventions to promote physical and mental health are thus needed.
• International experience highlights pricing as one of the most important factors for influencing and reducing smoking rates. Regular and significant increases in the price of cigarettes need to be continued by Government as one component in its efforts to decrease levels of smoking in the population.
• The impacts of recent changes in Irish legislation, notably the smoking ban, on smoking levels, smoking contexts and attitudes to smoking need to be further evaluated.
• There is a need for ongoing monitoring of population smoking patterns, notably in population sub-groups such as adolescents and young adults, so as to evaluate the effectiveness of specific smoking prevention and cessation strategies.

3
1. INTRODuCTION
Smoking is an important risk factor for six of the world’s eight leading causes of death and it causes about 1 in 10 adult deaths. This figure is expected to rise steeply worldwide as tobacco companies target new customers, particularly women and people living in low-income countries. Smoking is also the major preventable cause of death and chronic disability in Ireland today and a major cause of health inequality. Ireland ranks second highest for smoking-related deaths within the EU original group of 15 Member States. Action on Smoking and Health (ASH) Ireland and the Irish Cancer Society estimate that about 7,500 people in Ireland die every year from smoking-related illnesses. The causal association between lung cancer and smoking is very strong, with 90% of cases directly attributable to smoking (Kabir et al, 2007).
Lung cancer is currently the most common cancer in the world (Stewart et al, 2003). The National Cancer Registry reports that in Ireland in 2004, lung cancer accounted for over 1,600 deaths. Between 1994 and 2005, the age-standardised annual incidence rate of lung cancer in men was more than double that of women, at 63 compared to 30 per 100,000 persons per year (National Cancer Registry Ireland, 2006a). However, during the same period there was an annual increase of 2.3% in age-standardised lung cancer incidence rates reported for women and an annual decrease of 0.9% in men. This levelling off and fall in the incidence of lung cancer in men, coupled with an increasing rate in women, has also been found in other countries.
These temporal patterns reflect changes in smoking habits within the Irish population over the last 20 years (Kabir et al, 2007). The National Cancer Registry (2006b) estimates that, given current smoking rates and current risk, the number of new lung cancers in women will have increased by 136% by 2020. For men, the increase will be considerably lower, at 59%. An ageing population, which is paying the price for several decades of cigarette smoking exposure, will account for most of these increases.


5
2. SMOkINg PATTERNS IN IRELAND
SLÁN 2007 was the third national Survey of Lifestyle, Attitudes and Nutrition (SLÁN) in Ireland and followed previous surveys in 1998 and 2002. The 2007 survey was conducted through face-to-face interviews in the homes of 10,364 randomly selected adults, aged 18 years and older. There was a 62% response rate. The overall findings are contained in the SLÁN 2007: Main Report (Morgan et al, 2008) and a number of sub-reports on specific aspects (e.g. diet and nutrition, mental health and social well-being, alcohol, injuries, Northern Ireland comparisons) are also available or forthcoming (see www.slan07.ie).
As part of the SLÁN 2007 survey, respondents were asked about previous and current smoking behaviour, attempts to quit (current smokers only) and rules regarding smoking in the home. A ‘current smoker’ was defined as smoking ‘every day’ or ‘some days’, and ‘having smoked at least 100 cigarettes during my lifetime’. ‘Former smokers’ were current non-smokers who had smoked at least 100 cigarettes in the past.
Findings are analysed and presented here by gender, age, social class and occupation where differences within these categories are significant and important. Results comparing SLÁN 2007 with SLÁN 1998 and 2002 – and with the HBSC 2006 Survey of school-aged children – are highlighted where comparisons are possible.
OvERALL SMOkINg RATES
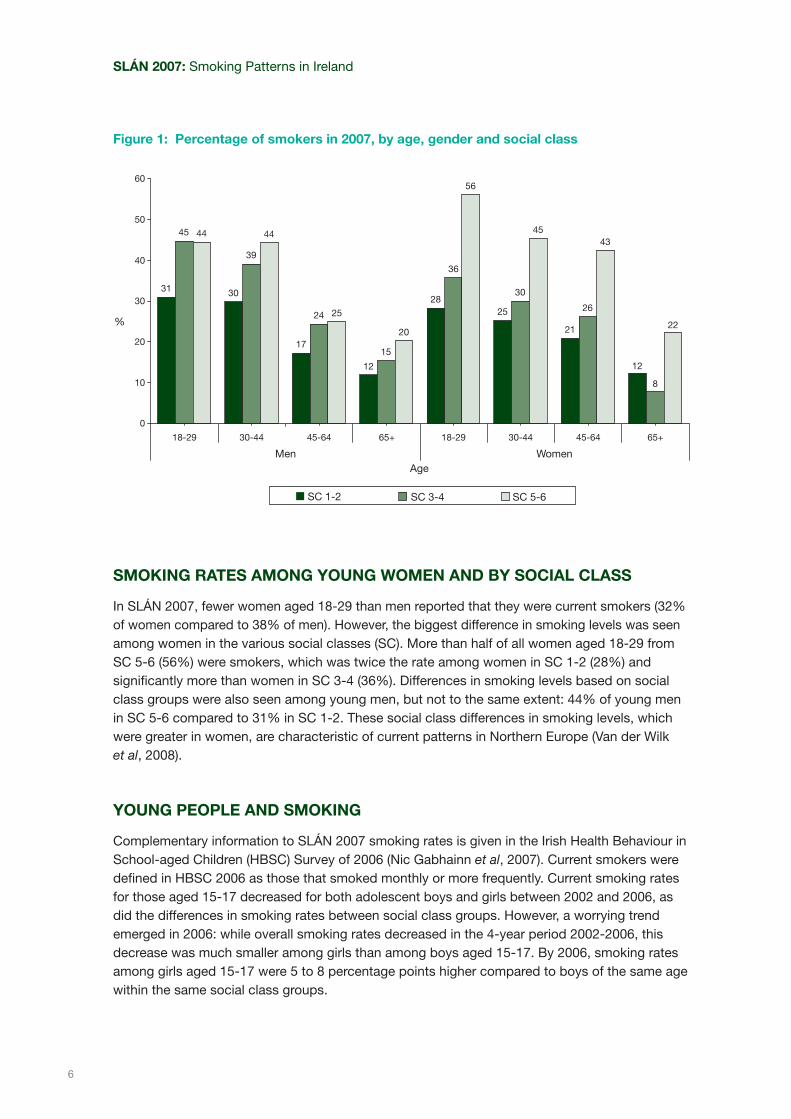
Almost half of SLÁN 2007 respondents (48%) reported that they were current or former cigarette smokers. Overall, 29% of respondents reported being current smokers, with higher rates for men (31%) than for women (27%). This pattern persisted across all age groups. Of those who were current smokers, 83% reported smoking on a daily basis and 17% reported smoking on ‘some days’. Higher rates of smoking were reported by younger respondents (age 18-29: 35%; 30-44: 34%; 45-64: 25%; 65+: 14%) and among respondents in lower social class groups (SC 1-2: 24%; SC 3-4: 30%; SC 5-6: 37%) (see Figure 1).
More men (54%) than women (42%) reported being current or former smokers, and more men (23%) than women (16%) reported having succeeded in quitting smoking. Higher rates of current and former smoking were reported within the two middle-age groups (30-44 and 45-64 years) and within the lowest social class groups (SC 5-6).
6
Figure 1: Percentage of smokers in 2007, by age, gender and social class
Age
SC 1-2 SC 3-4 SC 5-6
60
50
40
30
20
10
0
31
45 44
30
39
44
17
24 25
12
15
20
28
36
56
25
30
45
21
26
43
12
8
22
18-29 30-44 65+45-64 18-29 30-44 45-64 65+
Men Women
%
SMOkINg RATES AMONg yOuNg wOMEN AND By SOCIAL CLASS
In SLÁN 2007, fewer women aged 18-29 than men reported that they were current smokers (32% of women compared to 38% of men). However, the biggest difference in smoking levels was seen among women in the various social classes (SC). More than half of all women aged 18-29 from SC 5-6 (56%) were smokers, which was twice the rate among women in SC 1-2 (28%) and significantly more than women in SC 3-4 (36%). Differences in smoking levels based on social class groups were also seen among young men, but not to the same extent: 44% of young men in SC 5-6 compared to 31% in SC 1-2. These social class differences in smoking levels, which were greater in women, are characteristic of current patterns in Northern Europe (Van der Wilk et al, 2008).
yOuNg PEOPLE AND SMOkINg
Complementary information to SLÁN 2007 smoking rates is given in the Irish Health Behaviour in School-aged Children (HBSC) Survey of 2006 (Nic Gabhainn et al, 2007). Current smokers were defined in HBSC 2006 as those that smoked monthly or more frequently. Current smoking rates for those aged 15-17 decreased for both adolescent boys and girls between 2002 and 2006, as did the differences in smoking rates between social class groups. However, a worrying trend emerged in 2006: while overall smoking rates decreased in the 4-year period 2002-2006, this decrease was much smaller among girls than among boys aged 15-17. By 2006, smoking rates among girls aged 15-17 were 5 to 8 percentage points higher compared to boys of the same age within the same social class groups.
SLÁN 2007: Smoking Patterns in Ireland

7
Smoking initiation rates are also an important marker of smoking trends. Every 4 years, the HBSC survey looks at smoking initiation rates for those currently aged 15. Early smoking initiation (classified as smoking at or before 13 years of age) is linked to greater likelihood of continuing smoking into adulthood. In HBSC 2006, 31% of Irish 15-year-olds had initiated smoking at or before 13 years of age (29% boys and 33% girls). This trend – where young girls are increasingly more like to smoke than their male counterparts – has held true over the past 10-15 years in more than 15-20 countries, including almost all developed countries (Peto et al, 1996).
Figure 2: Rates of current smoking in SLÁN 2007 among young people aged 18-29, by social class (%)
Age
SC 1-2 SC 3-4 SC 5-6
60
50
40
30
20
10
0
Men Women
(%)
18-23 24-29 18-23 24-29
3437
39
30
47 47
24
40
55
30 31
56
The 36% of 15-17 year-old female adolescents in SC 5-6 who reported smoking in the HBSC 2002 survey correspond with the 55% of 18-23 year-old women in SC 5-6 who reported smoking in SLÁN 2007. While there may have been sampling differences (e.g. a greater percentage of those in SC 5-6 may have left school early, reducing smoking prevalence in the HBSC sample), this finding suggests that there may be a high level of smoking initiation among young women, especially in SC 5-6, soon after leaving school. Thus, it is essential to address the issue of young women and smoking in a more definitive way. If this trend continues, this age cohort will experience increased morbidity and mortality rates from chronic diseases associated with smoking.
High rates of smoking among young women, especially those in lower social classes, warrant particular policy attention. Over half of women aged 18-23 in social classes SC 5-6 were smokers. This corresponds with other Irish and international evidence that adolescent girls and young women are more likely to smoke than their male counterparts.
Smoking patterns in Ireland

8
TRENDS IN SMOkINg RATES ACROSS SLÁN 1998, 2002 AND 2007
Overall, 29% of respondents in SLÁN 2007 reported that they were current smokers. This was lower than in 1998 (33%) and a non-significant increase from 2002 (27%). The downward trend between 1998 and 2002 was seen in both men and women, and across all age groups and social classes (see Table 1). Progress then stalled in all these categories, with no significant change in smoking rates between 2002 and 2007.
The increase in smoking prevalence rates (2002: 27%; 2007: 29%) cannot be explained by the population increase in non-Irish nationals since SLÁN 2002. There were no significant differences in smoking rates between Irish nationals and non-Irish nationals, who formed 16% of the overall SLÁN 2007 sample.
Table 1: Percentages of respondents reporting smoking in SLÁN 1998, 2002 and 2007, by gender, age and social class
MEN wOMEN TOTAL
SLÁN 1998
(n = 2,981)
%
SLÁN 2002
(n = 2,787)
%
SLÁN 2007
(n = 5,074)
%
SLÁN 1998
(n = 3,300)
%
SLÁN 2002
(n = 3,048)
%
SLÁN 2007
(n = 5,177)
%
SLÁN 1998
(n = 6,293)
%
SLÁN 2002
(n = 5,835)
%
SLÁN 2007
(n = 10,251)
%
Total 34 27 31 32 27 27 33 27 29
Age group
18-29 42 29 38 44 31 32 43 30 35
30-44 38 33 37 34 32 29 36 33 34
45-64 29 23 23 26 25 27 28 24 25
65+ 19 20 17 16 14 13 17 17 14
Social class
SC 1-2 30 19 24 31 19 23 30 19 24
SC 3-4 36 27 33 37 27 28 36 27 30
SC 5-6 39 33 34 38 38 41 39 35 37
Unclassified 32 32 35 27 33 20 30 33 25
Note: The apparent increase in smoking rates between 2002 and 2007, notably in young men (aged 18-29)
– although to levels lower than in 1998 – needs to be treated with caution because this category had
been under-represented in respondents interviewed in SLÁN 2002.
SLÁN 2007: Smoking Patterns in Ireland

9
EvIDENCE OF SMOkINg TRENDS FROM OFFICE OF TOBACCO CONTROL
SLÁN 2007 smoking rates are complemented by other available evidence. Figures from the Office of Tobacco Control (2008) suggest a downward trend in smoking levels for one year after the introduction of the workplace smoking ban in Ireland in April 2004, followed by an upward rebound effect from April 2005 (see Figure 3). There was some early indication that rates may have begun to fall again from mid-2007, more so among women.
Figure 3: Monthly trends in smoking 2003-2008, by overall prevalence and gender (%)
30.0%
28.0%
26.0%
24.0%
22.0%
20.0%
Cigarette Smoking Prevalence within Gender12 month moving average trend ending March 2008
June 2003
March 2004
May 2004
July 2004
September 2004
November 2004
February 2007
February 2006
February 2005
February 2008
April 2006
April 2005
April 2007
June 2007
June 2006
June 2005
August 2003
August 2006
August 2005
August 2007
October 2003
October 2006
October 2005
October 2007
December 2006
December 2005
December 2007
January 2004
Overall PrevalenceMaleFemale
Source: Office of Tobacco Control
Notes:
• Caution is advised in interpreting Office of Tobacco Control (OTC) figures, which are based on
telephone surveys compared to SLÁN 2007 using household interviews. Under-representation of
certain groups in the OTC survey is likely to account for the overall reported lower rates of smoking
(about 24% compared to 29% in SLÁN 2007).
• It should be noted that the definitions used for smokers differ. The OTC survey defined a smoker as
someone who has smoked at least 1 cigarette within the previous 12 months, while SLÁN 2007 defines
a smoker as someone who has smoked at least 100 cigarettes in their lifetime and now smokes 'every
day' or 'some days'.
The success of Ireland’s smoking ban has primarily been in reduced risks from passive smoking. There is no evidence that Ireland has achieved a sustained downward trend in overall smoking rates.
Smoking patterns in Ireland

10
SLÁN 2007: Smoking Patterns in Ireland
SMOkINg AND OCCuPATIONAL CATEgORIES
In SLÁN 2007, smoking rates among people in employment, at 29%, were the same as the general population. These were lower compared with smoking rates of 49% among the 3% of respondents who were ‘unemployed and currently looking for work’ and 44% among the 4% who had ‘long-term sickness and disability’.
Figure 4 shows a range of occupational group categories where respondents had higher rates of smoking than were found in the general population. Almost one-quarter of male respondents (23%) were classified within the following 3 occupation categories: crafts and related trades workers; process, plant and machine operatives; and elementary occupations (i.e. elementary trades and plant and storage related occupations) (ONS, 2000). Smoking rates in these occupations averaged 38%, although only 50% of respondents provided a detailed description of their occupation. Unlike socio-economic categories, occupational groups are often visible or easily identifiable sub-groups, which could be targeted with smoking cessation interventions.
Figure 4: Occupational groups with smoking prevalence rates greater than 35% (%)
60
50
40
30
20
10
0
Service workers
Crafts
Elementary occupations
Plant and Machinery
State Training Schemes
Unemployed, currentlylooking for work
Long-term sicknessor disability
Occupational group
Cur
rent
Sm
oke
rs%
36
39
36
4243
49
44
Source: Adapted from Singh (2008)

11
SMOkINg, SOCIAL CLASS AND SOCIO-ECONOMIC EFFECTS
An analysis of US women smokers of lower socio-economic groups showed that the best predictors of quitting from smoking were active plans to quit, confidence and social pressure (Manfredi et al, 2006). Motivating factors included health concerns. A negative effect of daily stress on quitting was mediated through decreased self-efficacy.
However, an analysis of factors mediating the effects of social class in Ireland has suggested that social deprivation, rather than reduced self-efficacy, accounts for higher smoking levels and lower quitting rates (Layte and Whelan, 2008). This analysis of data from the Living in Ireland household survey, conducted in 2000 by the ESRI, explored three hypotheses to explain apparent socio-economic inequalities related to smoking, where higher smoking rates and lower quitting rates were found among lower socio-economic groups. The first hypothesis argued that socio-economic inequalities reflect differences across education groups in knowledge of the risks of smoking. The second hypothesis proposed that the living conditions of lower socio-economic groups lead to the development of lower self-efficacy and a lower propensity to quit smoking. The third hypothesis was that smoking has a functional use among poorer individuals.
The study concluded that self-efficacy played almost no part in social class differences, that education played a small part, and that ‘measures of economic resources and enduring economic and social difficulties’ accounted for the largest part of the differential (Layte and Whelan, 2008).
Targeted approaches with particular occupational groups and the unemployed need to avoid stigmatising these groups and should also take account of how the ‘lived experience of socio-economic deprivation’ reinforces and sustains smoking behaviour.
INTERNATIONAL COMPARISONS
The UK introduced a similar workplace smoking ban on 1st July 2007 as that introduced in Ireland 3 years earlier, on 1st April 2004. The 2008 report by the UK Department of Health, Smokefree England: One Year On, stated that nearly 234,060 people quit smoking with the help of local NHS Stop Smoking Services between April and December 2007, a 22% increase in the number of successful quitters and a 23% increase in the number of people setting a quit date, compared to the same period in 2006/07.
The Smoking Toolkit Study by West (2006) found that smoking prevalence rates in England have declined at an average rate of 0.61 percentage points per month since smoke-free legislation came into effect in July 2007, compared with 0.18 percentage points a month before the legislation. By April 2008, it was estimated that the effect of the legislation was a total fall in prevalence rates of 4.3 percentage points. This equates to at least 400,000 people stopping smoking, which would lead to about 40,000 fewer premature deaths in the longer term. Long-term monitoring of smoking prevalence rates is needed to identify what combinations of interventions lead to sustained downward trends.
Smoking patterns in Ireland

12
SLÁN 2007: Smoking Patterns in Ireland
The Tobacco Control Scale survey, carried out by the World Health Organization, examines tobacco control policy within 30 European countries. The scale is based on the six strategic policies described by the WHO under its MPOWER package (WHO, 2008) (see p. 19 for details). The 2007 survey ranked Ireland as 2nd overall for adhering to these important control measures. In the previous 2005 survey, Ireland was ranked in 1st place, but was overtaken by the UK in 2007 due to its increases in tobacco taxation and prices, investment in interventions and increased spending on public information campaigns. Ireland may have missed an opportunity after 2004 to reinforce the early success of the smoking ban by the introduction of such additional smoking control measures.
Ireland’s fall from 1st to 2nd place – behind the uk – in European rankings for its tobacco control policies points to lack of investment in tobacco control interventions and too modest tobacco tax and price increases.
ExPOSuRE TO SMOkINg AT HOME AND AT wORk
Most respondents in SLÁN 2007 reported being unwilling to allow smoking in their own homes – 59% never allowed it and a further 23% only allowed it at certain times and in certain places in the home.
While the workplace smoking ban introduced in 2004 has not been shown by SLÁN 2007 data to have had a positive impact on overall smoking rates, it can still be considered a success through having improved working conditions and significantly reducing the damage caused to employees in the workplace by passive smoking (Allwright et al, 2005). Irish bar workers, for example, have been found to have better respiratory function following introduction of the workplace smoking ban.
ATTENDANCE AT PRIMARy CARE AND SMOkINg CESSATION ADvICE FROM HEALTH PROFESSIONALS
Overall, 74% of SLÁN 2007 respondents had attended a general practitioner (GP) within the previous 12 months (26% in the previous 4 weeks and 48% between 1 and 12 months previously). A similar proportion of current smokers (72%) also reported attending their GP within the previous 12 months. Smokers with a medical card (82%) were more likely than smokers without a medical card (68%) to have attended a GP within the past year, which reflects similar overall GP attendance rates for medical card holders and non-holders.
A notably low percentage of current smokers (38%) reported that ‘a doctor or health professional’ had discussed ways of giving up smoking with them during the previous 12 months (see Table 2).1
*
Those most likely to have had such a discussion were:
1
* The question did not specify the type of health professional.
13
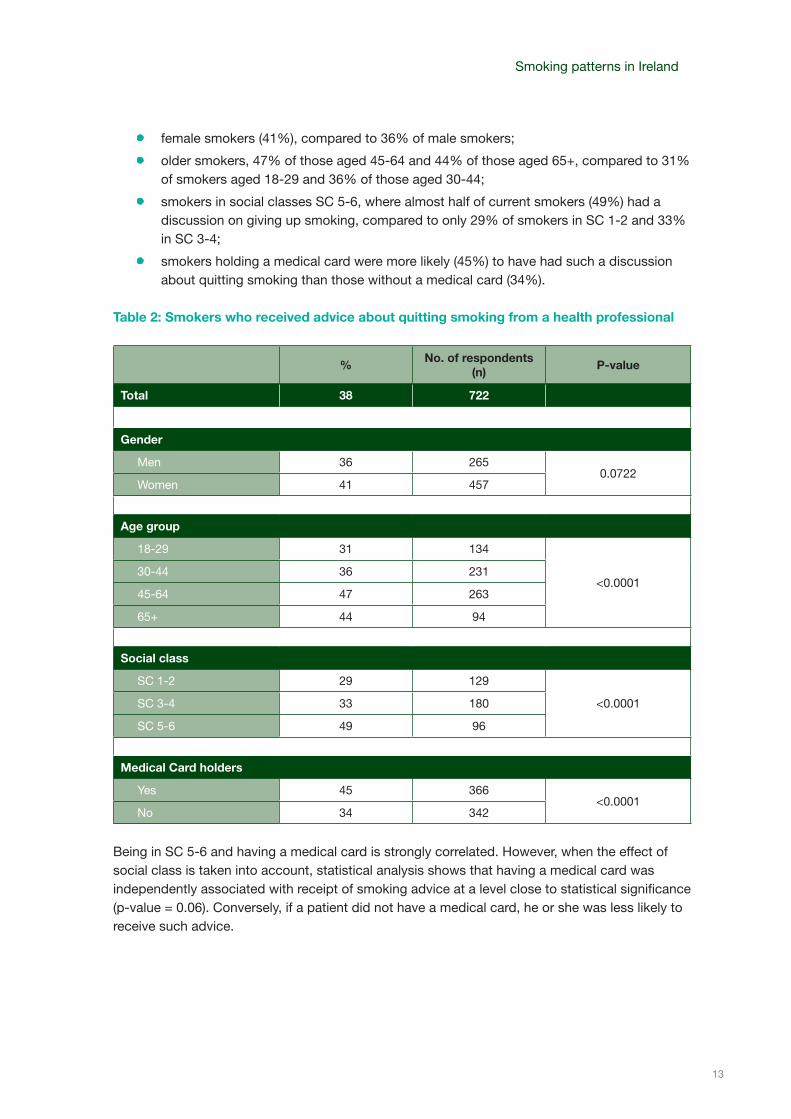
• female smokers (41%), compared to 36% of male smokers;
• older smokers, 47% of those aged 45-64 and 44% of those aged 65+, compared to 31% of smokers aged 18-29 and 36% of those aged 30-44;
• smokers in social classes SC 5-6, where almost half of current smokers (49%) had a discussion on giving up smoking, compared to only 29% of smokers in SC 1-2 and 33% in SC 3-4;
• smokers holding a medical card were more likely (45%) to have had such a discussion about quitting smoking than those without a medical card (34%).
Table 2: Smokers who received advice about quitting smoking from a health professional
%No. of respondents
(n)P-value
Total 38 722
gender
Men 36 2650.0722
Women 41 457
Age group
18-29 31 134
<0.0001 30-44 36 231
45-64 47 263
65+ 44 94
Social class
SC 1-2 29 129
<0.0001 SC 3-4 33 180
SC 5-6 49 96
Medical Card holders
Yes 45 366<0.0001
No 34 342
Being in SC 5-6 and having a medical card is strongly correlated. However, when the effect of social class is taken into account, statistical analysis shows that having a medical card was independently associated with receipt of smoking advice at a level close to statistical significance (p-value = 0.06). Conversely, if a patient did not have a medical card, he or she was less likely to receive such advice.
Smoking patterns in Ireland

14
SLÁN 2007: Smoking Patterns in Ireland
Almost three-quarters of Irish smokers had attended a gP in the previous year, which could provide an opportunity for gP-mediated smoking cessation interventions. Therefore, high reported rates of missed opportunities for helping smokers quit when they visit health professionals warrant exploration.
gPs – AN uNDER-uTILISED RESOuRCE FOR SuPPORTINg SMOkINg CESSATION
Smoking cessation at any age is associated with risk reduction. GP-mediated interventions are an effective way of helping smokers to quit (Campbell, 1994). A Cochrane review conducted in 2008 showed that even when doctors gave brief simple advice to their patients about quitting smoking, this increased the likelihood that a smoker would successfully quit and remain a non-smoker 12 months later (Stead et al, 2008a). More intensive advice may result in slightly higher rates of quitting.
In addition to GP interventions, nursing staff also play an important role in smoking cessation. Rice and Stead (2008) found that advice and support from nurses could increase people’s success in quitting smoking. This was particularly evident within the hospital setting. Similar advice and encouragement given by community-based nurses, however, at health checks or prevention activities seemed to be less effective.
An international literature review conducted in 2008 as part of the PESCE Project (an EU-funded study of GPs and the economics of smoking cessation in Europe) showed that most GPs asked new patients if they smoked; fewer GPs routinely asked all regular patients about their smoking status and fewer still routinely advised all patients who were smokers to quit (PESCE, 2008). Factors that influenced GPs’ active intervention to assist patients to stop smoking included:
• gPs' own smoking behaviour: Generally, GPs who smoke give cessation advice less frequently than GPs who do not smoke.
• gPs' attitudes towards and interest in smoking cessation: Some GPs feel that it is not part of their job to give smoking cessation advice; some feel uncomfortable or embarrassed to give such advice; some find it unrewarding and consider it is ineffective.
• Concern for doctor–patient relationship: There is a concern that asking about smoking habits could harm the doctor–patient relationship and be associated with less frequent consultations.
• Factors related to patients: GPs are more likely to advise quitting where symptoms are seen as being smoking-related; they are therefore more likely to intervene with heavier smokers and those with a longer history of smoking.
• Structural factors: GPs perceive that giving advice on smoking cessation is too time-consuming and is not adequately reimbursed.
• gPs' skills and knowledge: GPs sometimes lack knowledge of counselling techniques, treatments and skills in delivering smoking cessation interventions. The willingness to use them may depend on perceptions of the efficacy of treatment options.

15
The challenge is to incorporate smoking behaviour monitoring and smoking cessation interventions into standard practice so all patients are given the opportunity to discuss their smoking behaviour and be given advice or counselling to quit, along with follow-up after a certain period of time. A study conducted by Currie et al (2008) for the Research Institute for a Tobaccofree Society (RIFTFS) investigated the range and availability of smoking cessation services in Ireland. It found that while cessation services were available in each of the four HSE regions, there were regional differences in resource allocation, with HSE South and HSE Dublin Mid-Leinster being relatively under-served. There was also little consistency in the delivery of these services nationwide and no systematic follow-up from service providers.
SMOkERS ATTENDINg gPs – OPPORTuNITIES FOR INTERvENTIONS
The reported low levels of advice received from doctors and other health professionals by smokers in SLÁN 2007 suggest that an important opportunity for delivering smoking cessation advice and support is being missed. The questions asked in SLÁN 2007 regarding GP attendance and advice on smoking from GPs or other health professionals do not categorically point to missed opportunities by GPs. However, the findings do raise questions, including: What are the factors that determine GP health promotion practices in Ireland? Why, for example, do respondents from social classes SC 1-2 and those without medical cards report lower rates of GP-initiated (and other health professional) discussions on smoking cessation? To what extent do the factors identified in the PESCE Project as influencing GPs’ willingness to intervene (see p. 14) account for these differences?
The nature of reporting complaints may be one factor, in that holders of medical cards in Ireland may report smoking-related symptoms to their GPs more frequently than do non-holders, thereby eliciting smoking cessation advice. However, the absence of smoking-related targets for Irish GPs, compared to their UK counterparts (NICE, 2007a and 2008), and the lack of incentives to underpin these targets warrant exploration and structured engagement and discussion by health service managers with primary care professional groups in Ireland.
Incentive and support structures need to be in place to enable gPs and other health professionals to actively engage in smoking cessation interventions.
ATTEMPTS TO quIT
In SLÁN 2007, almost half of both male and female smokers (46%) reported attempting to quit within the previous 12 months. Reported attempts to quit fell gradually with age, from 54% of smokers at age 18-29 down to 30% of smokers at 65+ years. Women aged 18-29 from SC 1-2, who were the social class group least likely within this age category to smoke, were also the group most likely (65%) to report attempting to quit smoking in the previous 12 months.
Smoking patterns in Ireland

16
SLÁN 2007: Smoking Patterns in Ireland
quITTINg AIDS
SLÁN 2007 respondents who had attempted to quit smoking were asked whether they had used any form of nicotine replacement therapy (NRT) or any other aid to help them. (The aim of NRT is to temporarily replace much of the nicotine obtained from cigarettes, so as to reduce nicotine withdrawal symptoms and their association with smoking cigarettes, thus easing the transition from cigarette smoking to complete abstinence.) Just under 60% of respondents who had tried to quit in the previous 12 months reported using an aid in their attempt.
Overall, women were more likely (46%) than men (36%) to report using some form of cessation aid. The most popular aids used were NRT in the form of patches (29%), followed by nicotine gum or lozenges (10%). Few respondents had used methods other than NRT: just 2% had used acupuncture, while 1% used a smoking cessation helpline.
A Cochrane review, conducted in 2008, evaluated whether NRT is effective at assisting people to quit smoking (Stead et al, 2008b). The study considered 132 trials with over 40,000 people in the main analysis. It concluded that all forms of NRT (patches, gum, nasal spray, inhalers and lozenges) increase the success of attempts to quit smoking by 50%-70%. There was no evidence to suggest an overall difference of effectiveness between the different forms of NRT or any benefit in using patches beyond 8 weeks.
NRT has been available on prescription free of charge to medical card holders in Ireland (29% of the population) since April 2001 (Tilson et al, 2004). Almost 50,000 patients availed of this in 2002. The 2007 report by the Primary Care Reimbursement Service (formerly known as the General Medical Services Payment Board), entitled Statistical Analysis of Claims and Payments, 2007 (HSE, 2008), places NRT as 58th in a list of expenditure for the top 100 products. In 2007, there were 103,607 prescriptions for NRT. This cost €3,282,024 and accounted for 0.39% of total expenditure for the scheme in 2007. However, those without medical cards have to pay for prescription items up to a total of €100 per month, in addition to fees for attending GPs to obtain a prescription.
Nicotine replacement aids have been shown to be effective and are available on prescription and free to medical card holders. Prescription charges incurred by the majority of the population may be a disincentive to their incorporation and use as one component of a smoking cessation package.
wHy quITTINg EFFORTS FAIL, ESPECIALLy AMONg wOMEN
There is evidence that women and men respond somewhat differently to nicotine. For example, female addiction may be reinforced more by the sensory and social context of smoking rather than by nicotine itself (Brigham, 2001). This being the case, nicotine replacement therapy in the form of patches and gum/lozenges may be less effective in women.

17
SLÁN 2007, like other surveys, found that women were less likely (16%) than men (23%) to report successfully quitting smoking. Findings in SLÁN 2007 pointed to factors that could account for this: 36% of female smokers (compared to 27% of men) expected that they would put on weight if they stopped smoking, suggesting that some women may be using smoking as a method of controlling their weight.
When asked if giving up smoking would make it harder to deal with stress in their lives, 33% of smokers from lower social classes (SC 5-6) and 33% of women overall agreed that it would make it harder, compared to 22% of smokers from higher social classes (SC 1-2) and 23% of men overall. The likelihood of stress was reported by half of female respondents from SC 5-6, but the numbers were small. This may indicate that smoking is used as a form of stress management by some women, and more so among those in lower social classes.
Smoking cessation interventions that are sensitive to gender and social class are required.
SMOkINg – A MuLTIFACETED HEALTH ISSuE
The health impact of various lifestyle behavioural factors, such as smoking, diet, physical activity and alcohol consumption, is well-documented. However, their combined impact on the general population is less well-known. Khaw et al (2008) identified 4 positive lifestyle behaviours:
• consuming 5 or more daily servings of fruit and vegetables; • being a non-smoker; • having a moderate alcohol intake; • being physically active.
In a study of a UK population, the EPIC-Norfolk Prospective Population Study (Khaw et al, 2008), research found a 14-year difference in life expectancy between individuals practising none of these behaviours relative to those practicing all 4 of them – the equivalent of a 4-fold difference in total mortality in men and women. Thus, small differences in lifestyle may make a big difference to the health of the population.
Respondents in SLÁN 2007 were asked to report on important health-related behaviours, specifically the frequency and intensity of their physical activity, their alcohol consumption and whether they smoked. Respondents were then classified into different health behaviour categories depending on their responses. Physical activity levels were classified into three separate groups (low, moderate and high); alcohol consumption was divided into two risk level groups (low risk and increased risk); and smoking status was recorded (current smoker, former smoker and never smoked).
Smoking patterns in Ireland
18
SLÁN 2007: Smoking Patterns in Ireland
The positive lifestyle behaviours chosen for this analysis of SLÁN 2007 data were similar to those selected by Khaw et al (2008), namely:
• Consuming 5 or more daily servings of fruit and vegetables. Servings were calculated from the Food Frequency Questionnaire.
• Being a non-smoker, as defined by the question 'Have you yourself smoked at least 100 cigarettes in your entire life?' If a respondent answered 'No' to this question, they were defined as a non-smoker for this analysis.
• Being physically active. Physically active respondents were those with International Physical Activity Questionnaire (IPAQ) scores that categorised them as having either moderate or high activity levels.
• Being a moderate drinker of alcohol. Moderate drinkers were defined as those respondents who drank up to 14 units in the previous 7 days.
Overall, 1% of SLÁN 2007 respondents reported none of the 4 positive lifestyle behaviours, while 10% reported one behaviour, 27% reported 2 behaviours, 39% reported 3 behaviours and 23% reported 4 behaviours (Harrington et al, 2008).
The food frequency component of SLÁN 2007 was used to calculate the level of vitamin C intake among respondents. Measurement of vitamin C gives a good indication of an individual’s fruit and vegetable intake. The recommended daily allowance (RDA) for vitamin C is 60mg/day. Analysis of the SLÁN 2007 Food Frequency Questionnaire data found that 90% of non-smokers reach this RDA, compared to 83% of smokers. The difference in vitamin C intake between smokers and non-smokers is statistically significant.
Previous studies have attributed lower ‘quitting smoking’ success rates in women to depression (which is more common in women than in men) and to sex-linked differences in hormonal levels, as well as to lack of social supports (Ernster, 2001; Perkins, 2001; Piper et al, 2001). SLÁN 2007 also asked respondents about aspects of their mental health and well-being. Findings showed a strong association between negative mental health and smoking and not exercising. Respondents who smoked (compared to those who never smoked) were 2-3 times more likely to report psychological distress or a generalised anxiety disorder. Also, current and former smokers were less likely than those who had never smoked to report that their health was ‘excellent’ or ‘very good’ – 51% of current smokers and 56% of former smokers, compared to 63% of those who never smoked. Indeed, current and former smokers were more likely (15%) to rate their health as ‘fair’ or ‘poor’ compared to those who had never smoked (10%).
Further analysis on links between smoking and mental health are available in the SLÁN 2007: Mental Health and Social Well-being Report by Barry et al (2009).
Smoking is often one component of a constellation of unhealthy behaviours and mental states, linking smoking with excess alcohol intake, overweight or obesity, lack of physical activity, mental health problems and poor quality of life. Multifaceted interventions to promote physical and mental health are therefore needed.

19
INTERNATIONAL EFFORTS TO TACkLE SMOkINg: HOw IS IRELAND DOINg?
The 2008 report by the World Health Organization entitled MPOWER: A Policy Package to reverse the Tobacco Epidemic provides a comprehensive analysis of tobacco use, smoking control and taxation policies in 179 countries worldwide (WHO, 2008). It sets out 6 MPOWER strategies to reduce tobacco use. SLÁN 2007 provides evidence of Ireland’s progress in these strategy areas and offers guidance on what further actions can be taken in 4 areas.
• Monitor tobacco use and prevention policies• The SLÁN surveys of 1998, 2002 and 2007, and the HBSC 2006 Survey have measured
and tracked trends in smoking prevalence in Ireland over the last 10 years by gender, age and social class.
• The forthcoming National Cardiovascular Health Policy (Department of Health and Children, 2009) will set 10-year targets – to reduce the overall prevalence of smoking by 1% per annum (from 29% to 19%) and to reduce smoking initiation rates by 1% per annum (from 31% to 21%) by 2018.
• Ongoing monitoring of population and target group trends – through periodic national health and lifestyle surveys and/or as components in more frequent household surveys – will be essential for guiding and evaluating control efforts.
• Protect people from tobacco smoke• The first total workplace smoking ban in Europe was launched in Ireland in April 2004.
Other evidence points to its effectiveness in reducing risks to employees from passive smoking in the workplace (Allwright et al, 2005).
• SLÁN 2007 also shows that the majority of the public have adopted the smoking restriction rules in their own homes, thus significantly increasing the impact of protection from passive smoking.
• Offer help to quit tobacco use• Helplines and media campaigns have been implemented to assist people in quitting
smoking.
• However, the low levels of smoking cessation advice given by health professionals to smokers in Ireland, as reported in SLÁN 2007, suggest that GPs and primary care settings are a neglected resource for helping people to quit smoking. The cost of nicotine replacement therapies to most smokers may also be a disincentive.
• SLÁN 2007 provides evidence of population sub-groups that need to be targeted with smoking cessation supports, particularly young women in lower social classes and those in particular employment categories, as is now done in the UK (NICE, 2007b).
Smoking patterns in Ireland

20
SLÁN 2007: Smoking Patterns in Ireland
• warn about the dangers of tobacco• Media campaigns warn about the dangers of smoking and there are plans to include the
use of graphic images of smoking-related illnesses on cigarette packets. Further legislative restrictions on advertising and cigarette displays are imminent (see below).
• SLÁN 2007 has identified several high-risk groups, especially women in their late teens and early 20s, for whom campaigns and messages need to be tailored.
• Enforce bans on tobacco advertising, promotion and sponsorship• The Public Health (Tobacco) Acts 2002 and 2004 are in place, with further provisions to
commence on 1st July 2009. These provisions will include:
• a ban on all in-store/point-of-sale advertising of tobacco products;
• a ban on the display of tobacco products in retail premises;
• introduction of a closed container/dispenser provision;
• tighter controls on the location and operation of tobacco vending machines;
• introduction of a retail register for tobacco retailers.
• Raise taxes on tobacco• Governments can use budgetary tax increases to control tobacco consumption. The 2008
WHO report on the global tobacco epidemic states that increasing tobacco taxes by 10% generally decreases tobacco consumption by 4% in high-income countries (WHO, 2008). In Ireland, the price of tobacco products has increased by less than 10% in annual budgets between 1999 and 2009. It is highly likely that the stalling in the reduction of smoking prevalence rates in Ireland despite the introduction of the smoking ban, as seen in SLÁN 2007, is attributable, at least to some extent, to a failure to sufficiently raise cigarette taxes and prices.
Ireland has –
• shown leadership internationally in pioneering the introduction of one important component of a national tobacco control strategy – the ban on smoking in enclosed public spaces;
• missed an opportunity to build on this success and introduce what is considered the most important component of a tobacco control strategy – tax and price measures;
• been collecting population-based data to enable it to target and monitor the effectiveness of national tobacco control strategies. Ongoing monitoring and evaluation of strategies is essential.

21
3. CONCLuSIONS
The evidence from SLÁN 2007 points to the risk of Ireland becoming complacent about smoking cessation achievements, following the credits it deservedly received for the introduction of the 2004 workplace smoking ban – the first country in Europe to do so. The most effective smoking control approaches apply multifaceted comprehensive packages of measures. The 2004 smoking ban was both a success and a missed opportunity. It was highly successful in reducing exposure to smoking. It established and ensured adherence to legal prohibitions to smoking in workplace settings, resulting in improvements in staff health. SLÁN 2007 reports that similar controls are now implemented in private homes by the majority of the public. However, the findings show that the ban has had no effect on overall smoking rates.
The World Bank, WHO and expert consensus in Europe have concluded that price and taxation measures are the cornerstone of tobacco control. According to the World Bank, such measures are particularly effective among lower income groups and young people who are more sensitive than other groups to price increases (Ranson et al, 2000). A price rise of 10% decreases overall consumption in high-income countries by 4% and in young people by 8%, according to WHO (2008). The European Network on Smoking Prevention, using an expert consensus approach, scored ‘price/tax’ policy as the most effective measure, at 30 points; a ‘workplace smoking ban’ scored 2nd, at 22 points (Van der Wilk et al, 2008).
The optimal direction for Ireland to take now is to shift the cost-benefit balance of smoking, especially among those who are most vulnerable. Such a strategy could be cost-neutral, by increasing revenue through large price increases in the region of 25% to 30% for a packet of cigarettes, signalled well in advance of such a change. An amount equivalent to the increase in revenue could then be invested in prevention and quitting interventions, tailored and targeted to those at highest risk of starting smoking and least likely to otherwise quit. If such a pricing tool mechanism is planned, discussions should be held with the relevant authorities in Northern Ireland so as to ensure comparable pricing policies that dissuade cross-border flows of cigarettes.
Discussions with professional groups responsible for the delivery of primary care services – doctors, nurses, pharmacists – could identify acceptable mechanisms for encouraging and making better use of what are currently missed primary care opportunities for delivering smoking cessation interventions.
Ireland has been successful in enforcing behaviour change in the workplace and promoting behaviour change at home, based on the evidence of the dangers of passive smoking. Now that most of the population do not smoke, we need to avoid becoming complacent just because smoking is a hazard we experience less due to the success of the smoking ban. Out of sight (or outside the building) should not mean out of mind.


23
REFERENCES
Allwright, S., Paul, G., Greiner, B., Mullally, B.J., Pursell, L., Kelly, A., Bonner, B., D’eath, M., McConnell, C., McLaughlin, J.P., O’Donovan, D., O’Kane, E. and Perry, I. (2005) ‘Legislation for smoke-free workplaces and health of bar workers in Ireland: Before and after study’, British Medical Journal, Vol. 331, pp. 1117-23.
Barry, M.M., Van Lente, E., Molcho, M., Morgan, K., McGee, H., Conroy, R., Watson, D., Shelley, E. and Perry, I. (2009) SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. Mental Health and Social Well-being Report, Department of Health and Children. Dublin: The Stationery Office.
Brigham, J. (2001) ‘The addiction model’. In: J. Samet and Soon-Young Yoon (eds.), Women and the Tobacco Epidemic: Challenges for the 21st Century. Geneva: World Health Organization, pp. 99-118.
Campbell, I. (1994) ‘Nicotine patches in general practice’, British Medical Journal, Vol. 308, pp. 1476-77.
Currie, L., Keogan, S., Campbell, P., Gunning, M., Kabir, Z., Clarke, V. and Clancy, L. (2008) ‘The range and availability of smoking cessation services in Ireland’, The International Journal of Tuberculosis and Lung Disease, Vol. 12, No. 11 (Supplement 2), pp. 222-23. Available at: www.tri.ie (Research Institute for a Tobaccofree Society, Dublin).
Department of Health and Children (2009) Changing Cardiovascular Health. The National Cardiovascular Policy 2009-2018. Dublin: The Stationery Office (forthcoming).
Department of Health, UK (2008) Smokefree England: One Year On. London: Department of Health.
Ernster, V.L. (2001) ‘Impact of tobacco use on women’s health’. In: J. Samet and Soon-Young Yoon (eds.), Women and the Tobacco Epidemic: Challenges for the 21st Century. Geneva: World Health Organization, pp. 1-16.
Harrington, J., Perry, I., Lutomski, J., Morgan, K., McGee, H., Shelley, E., Watson, D. and Barry, M. (2008) SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. Dietary Habits of the Irish Population, Department of Health and Children. Dublin: The Stationery Office.
HSE (2008) Finance Shared Services. Primary Care Reimbursement Service: Statistical Analysis of Claims and Payments, 2007. Dublin: Health Service Executive.
Kabir, Z., Connolly, G.N. and Clancy, L. (2007) ‘Temporal patterns in lung cancer deaths in Ireland’, Irish Journal of Medical Science, Vol. 176, No. 2, pp. 81-85.
Khaw, K.T., Wareham, N., Bingham, S., Welch, A., Luben, R. and Day, N. (2008) ‘Combined Impact of Health Behaviours and Mortality in Men and Women. The EPIC-Norfolk Prospective Population Study’. Available at: www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.0050012 (accessed May 2009)
Layte, R. and Whelan, C. (2008) ‘Explaining social class inequalities in smoking: The role of education, self-efficacy and deprivation’, European Sociological Review, DOI: 10.1093/esr/jcn022, Published online 25th March 2008.
Manfredi, C., Ik Cho, Y., Crittenden, K.S. and Dolecek, T.A. (2006) ‘A path model of smoking cessation in women smokers of low socio-economic status’, Health Education Research, Vol. 22, pp. 747-56.

24
Morgan, K., McGee, H., Watson, D., Perry, I., Barry, M., Shelley, E., Harrington, J., Molcho, M., Layte, R., Tully, N., Van Lente, E., Ward, M., Lutomski, J., Conroy, R. and Brugha, R. (2008) SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. Main Report, Department of Health and Children. Dublin: The Stationery Office.
National Cancer Registry Ireland (2006a) Cancer in Ireland 1994-2005: A summary. Dublin: National Cancer Registry. Available at: www.ncri.ie/pubs/pubfiles/summary2007.pdf (accessed May 2009)
National Cancer Registry Ireland (2006b) Trends in Irish cancer incidence 1994-2002, with projections to 2020. Cork: National Cancer Registry. Available at: www.ncri.ie/pubs/pubfiles/proj_2020.pdf (accessed May 2009)
NICE (2008). Smoking cessation services. London: National Institute for Health and Clinical Excellence. Available at: www.nice.org.uk (accessed May 2009)
NICE (2007a) NICE advice on the best way to quit smoking. London: National Institute for Health and Clinical Excellence. Available at: www.nice.org.uk (accessed May 2009)
NICE (2007b) Workplace interventions to promote smoking cessation. London: National Institute for Health and Clinical Excellence. Available at: www.nice.org.uk (accessed May 2009)
Nic Gabhainn, S., Kelly, C. and Molcho, M. (2007) HBSC Ireland 2006: National Report of the 2006 Health Behaviour in School-aged Children in Ireland, Department of Health and Children. Dublin: The Stationery Office.
Office of Tobacco Control. Research Programmes. Available at: www.otc.ie/research_programmes.asp (accessed May 2009)
ONS (2000) Standard Occupational Classification 2000, Volume 1. Newport, South Wales: Office for National Statistics. Available at: www.ons.gov.uk/about-statistics/classifications/current/SOC2000/ (accessed May 2009)
Perkins, K.A. (2001) ‘Smoking cessation in women. Special considerations’, CNS Drugs, Vol. 15, No. 5, pp. 391-411.
PESCE Report (2008) Available at: www.ensp.org/files/pesce_executive_summary_20080602.doc (accessed May 2009)
Peto, R., Lopez, A.D., Boreham, J., Thun, M., Heath, C. Jnr. and Doll, R. (1996) ‘Mortality from Smoking Worldwide’, British Medical Bulletin, Vol. 52, pp. 12-21.
Piper, M.E., Fox, B.J., Welsch, S.K., Fiore, M.C. and Baker, T.B. (2001) ‘Gender and racial/ethnic differences in tobacco-dependence treatment: A commentary and research recommendations’, Nicotine and Tobacco Research, Vol. 3, pp. 291-97.
Ranson, K., Jha, P., Chaloupka, F.J. and Yurekli, A. (2000) ‘Effectiveness and cost-effectiveness of price increases and other tobacco control policies’. In: P. Jha and F.J. Chaloupka (eds.), Tobacco Control in Developing Countries. Oxford: Oxford University Press, pp. 427-47.
Rice, V.H. and Stead, L.F. (2008) ‘Nursing interventions for smoking cessation’, Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD001188. DOI: 10.1002/14651858.CD001188.pub3.
Singh, J. (2008) Prevalence of Smoking by Occupation in Ireland: An analysis of SLÁN 2007, Boulos Hanna Summer Studentship Report. Dublin: Royal College of Surgeons in Ireland.
SLÁN 2007: Smoking Patterns in Ireland

25
Stead, L.F., Bergson, G. and Lancaster, T. (2008a) ‘Does advice from doctors encourage people who smoke to quit’, Cochrane Database of Systematic Reviews, Issue 2. Art. No.: CD000165. DOI: 10.1002/14651858.CD000146.pub3.
Stead, L.F., Perera, R., Bullen, C., Mant, D. and Lancaster, T. (2008b) ‘Nicotine replacement therapy for smoking cessation’, Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD000146. DOI: 10.1002/14651858.CD000146.pub3.
Stewart, B.W., Kleihues, P. (eds.) (2003) World Cancer Report. Lyon: International Agency for Research on Cancer.
Tilson, L., Bennett, K. and Barry, M. (2004) ‘Prescribing trends for nicotine replacement therapy in primary care’, Irish Medical Journal, Vol. 97, pp. 270-73.
Van der Wilk, E.A., Melse, J.M., Den Broeder, J.M. and Achterberg, P.A. (2008) Learning from our Neighbours. Cross-national inspiration for Dutch public health policies: Smoking, alcohol, overweight, depression, health inequalities, youth, screening, RIVM Report 270626001/2008 Netherlands. Bilthoven, The Netherlands: National Institute for Public Health and the Environment. Available at: www.rivm.nl/bibliotheek/rapporten/270626001.pdf (accessed May 2009)
West, R. (2006) Smoking Toolkit Study. London: University College London. Available at: www.smokinginengland.info (accessed May 2009)
WHO (2008). MPOWER: A Policy Package to reverse the Global Tobacco Epidemic. Geneva: World Health Organization. Available at: www.who.int/tobacco/mpower/mpower_english.pdf (accessed May 2009)
References
26
NOTES