Simplifying neurologic assessmentdownloads.lww.com/wolterskluwer_vitalstream_com/...cle twitching....
4
www.NursingMadeIncrediblyEasy.com March/April 2010 Nursing made Incredibly Easy! 15 peak technique Neurologic assessment doesn’t just take place in neuro units and the ED. A patient who doesn’t have a neurologic diagnosis may also require a neuro assessment; for example, a patient with pneumonia can develop neuro- logic changes due to hypoxia or a post-op pa- tient may have a neurologic deficit due to blood loss. No matter what setting you work in, you’ll have to perform a neurologic as- sessment at some point. The value of a solid neurologic assessment can’t be overstated—a small change in the assessment is indicative of a neurologic injury, and early intervention can prevent permanent damage. Performing a neurologic assessment sends many of us into a panic. Fortunately, it doesn’t have to be that way. In this article, I’ll review not only how to perform a solid neurologic assessment, but also how you can tailor your assessment to the situa- tion. I’ll also give you some helpful tips to make your assessment as smooth as possible. The comprehensive assessment A thorough neurologic assessment will include assessing mental status, cranial nerves, motor and sensory function, pupillary response, reflexes, the cerebel- lum, and vital signs. However, unless you work in a neuro unit, you won’t typically need to perform a sensory and cerebellar assessment. Also, most vital sign changes are a sign of end-stage neurologic injury. Therefore, we’ll look at assessment of mental status, cranial nerves, motor function, and pupillary response. Although this isn’t a compre- hensive neurologic exam, it will yield valuable clinical information. Let’s get started with mental status. Assessing mental status Evaluating a patient’s mental status in- cludes level of consciousness (LOC), orien- tation, and memory. To assess LOC, you’ll use the Glasgow Coma Scale (see Glasgow Coma Scale). LOC is crucial to test because it’s the first assessment to change when there’s neurologic injury. You should always elicit your patient’s best level of response for an accurate assessment of LOC. Begin with speaking your patient’s name in a normal tone. If he doesn’t respond, say his name again in a louder tone. (If your patient is hearing-impaired, you’ll need to document this; it shouldn’t change his score.) If there’s still no response, gently shake your patient. If you still can’t get a reaction, you’ll need to use painful Simplifying neurologic assessment By Wendi Rank, CNRN, CRNP Board Member • American Association of Neuroscience Nurses • Philadelphia, Pa. Glasgow Coma Scale A decreased score in one or more of the following categories may signal an impending neurologic crisis. Add the scores for the best response in each category to achieve the total score. A total score of less than 9 indicates severe brain injury. Test EYE OPENING Spontaneously To speech To pain None MOTOR RESPONSE Obeys Localizes Withdraws Abnormal flexion Abnormal extension None VERBAL RESPONSE Oriented Confused Inappropriate words Incomprehensible None Score 4 3 2 1 6 5 4 3 2 1 5 4 3 2 1 Patient’s response Opens eyes spontaneously Opens eyes to verbal command Opens eyes to painful stimulus Doesn’t open eyes in response to stimulus Reacts to verbal command Identifies localized pain Flexes and withdraws from painful stimulus Assumes a decorticate position Assumes a decerebrate position No response; lies flaccid Is oriented and converses Is disoriented and confused Replies randomly with incorrect words Moans or screams No response
Transcript of Simplifying neurologic assessmentdownloads.lww.com/wolterskluwer_vitalstream_com/...cle twitching....

www.NursingMadeIncrediblyEasy.com March/April 2010 Nursing made Incredibly Easy! 15
peak technique
Neurologic assessment doesn’t just take placein neuro units and the ED. A patient whodoesn’t have a neurologic diagnosis may alsorequire a neuro assessment; for example, apatient with pneumonia can develop neuro-logic changes due to hypoxia or a post-op pa-tient may have a neurologic deficit due toblood loss. No matter what setting you workin, you’ll have to perform a neurologic as-sessment at some point. The value of a solidneurologic assessment can’t be overstated—asmall change in the assessment is indicativeof a neurologic injury, and early interventioncan prevent permanent damage.
Performing a neurologic assessment sendsmany of us into a panic. Fortunately, itdoesn’t have to be that way. In this article,I’ll review not only how to perform a solidneurologic assessment, but also how youcan tailor your assessment to the situa-tion. I’ll also give you some helpful tipsto make your assessment as smooth aspossible.
The comprehensiveassessmentA thorough neurologic assessment willinclude assessing mental status, cranialnerves, motor and sensory function,pupillary response, reflexes, the cerebel-lum, and vital signs. However, unlessyou work in a neuro unit, you won’ttypically need to perform a sensory andcerebellar assessment. Also, most vitalsign changes are a sign of end-stageneurologic injury. Therefore, we’ll lookat assessment of mental status, cranialnerves, motor function, and pupillaryresponse. Although this isn’t a compre-hensive neurologic exam, it will yieldvaluable clinical information. Let’s getstarted with mental status.
Assessing mental statusEvaluating a patient’s mental status in-cludes level of consciousness (LOC), orien-tation, and memory.
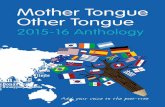
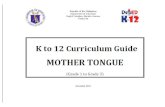
To assess LOC, you’ll use the GlasgowComa Scale (see Glasgow Coma Scale). LOC iscrucial to test because it’s the first assessmentto change when there’s neurologic injury.You should always elicit your patient’s bestlevel of response for an accurate assessmentof LOC. Begin with speaking your patient’sname in a normal tone. If he doesn’trespond, say his name again in a loudertone. (If your patient is hearing-impaired,you’ll need to document this; it shouldn’tchange his score.) If there’s still no response,gently shake your patient. If you still can’tget a reaction, you’ll need to use painful
Simplifying neurologic assessmentBy Wendi Rank, CNRN, CRNPBoard Member • American Association of Neuroscience Nurses • Philadelphia, Pa.
Glasgow Coma ScaleA decreased score in one or more of the following categories may signal an impendingneurologic crisis. Add the scores for the best response in each category to achieve thetotal score. A total score of less than 9 indicates severe brain injury.
TestEYE OPENING
SpontaneouslyTo speechTo painNone
MOTOR RESPONSE
ObeysLocalizesWithdrawsAbnormal flexionAbnormal extensionNone
VERBAL RESPONSE
OrientedConfusedInappropriate wordsIncomprehensibleNone
Score
4321
654321
54321
Patient’s response
Opens eyes spontaneouslyOpens eyes to verbal commandOpens eyes to painful stimulusDoesn’t open eyes in response to stimulus
Reacts to verbal commandIdentifies localized painFlexes and withdraws from painful stimulusAssumes a decorticate positionAssumes a decerebrate positionNo response; lies flaccid
Is oriented and conversesIs disoriented and confusedReplies randomly with incorrect wordsMoans or screamsNo response

stimulation. To do this, you can use one thefollowing techniques:• trapezius squeeze. Grasp and twist themuscle that runs from the back of the neckto the shoulder.• sternal rub. Make a fist, then push thebroad side of your fist into the sternum andpress hard enough to leave a mark on yourpatient’s skin.• supraorbital pressure. Along the bone be-neath the eyebrow you’ll find an indentationnear the nose. Press it with your thumbs.
If these techniques elicit a reaction, it comesfrom the brain. But there’s one more tech-nique you’ll need in your repertoire. Thepatient who requires painful stimuli isn’t fol-lowing commands; therefore, if he reacts tothe painful stimuli with only one side of hisbody, you’ll need to assess the nonreactiveside. This can be done by pressing a pencilinto the cuticle of one of your patient’s fin-gers. The response you’ll see will be purpose-ful, occurring when your patient pulls awayfrom the pain; nonpurposeful, occurringwhen he moves in response to the pain butnot in any meaningful way (including flexionposturing [arms bent up toward the trunkwith legs extended] and extension posturing[arms extend down and legs extended], for-merly called decorticate and decerebrate pos-turing); or no response at all. All painful stim-uli should be applied for 15 to 30 seconds.
To determine orientation, ask detailedquestions about your patient’s name, wherehe is, and the date. Obtain as much informa-tion as you can from the question; for exam-ple, when asking the date, also ask for themonth and year. Keep in mind that hospital-ized patients often know the month but notthe date or day of the week. Evaluate yourpatient’s knowledge of date and time care-fully; patients who are confused may stillanswer correctly enough that a disorder goesunnoticed. I once had a patient who wasclearly confused in conversation but confi-dently stated the name of the hospital eachtime I asked where we were. Halfwaythrough my shift, I realized he was readingthe hospital’s name off his roommate’ssheets, which were emblazoned with ourlogo. For the same reason, alternate yourquestions with each assessment. It’s impor-
tant to note that when you’re assessing ori-entation, you’re also evaluating yourpatient’s speech.
Memory is divided into three abilities:immediate memory, short-term memory,and remote memory. To assess immediatememory, give your patient three unrelatedwords to remember, such as pencil, grape,and car. Have him repeat the words and askhim to remember them. After 5 minutes, askhim to repeat the words back to you.
To assess short-term memory, ask yourpatient to describe something that happenedin the last few days. The classic example is toask him what he had for breakfast, but you’llwant to be able to verify his response. Youmay choose to ask about a recent significantnews event or a recent holiday.
Remote memory also commonly requiresverification from another party. Weddingdates or children’s birth dates are testsof remote memory but if you can’t get confir-mation, you can again try to use a news event.
Assessing the cranial nervesThe next component of the neurologic as-sessment is cranial nerve testing. Test thecranial nerves as follows:• CN I (olfactory). Ask your patient toidentify at least two common substancessuch as coffee and cinnamon. Make sure hisnostrils are patent before performing thistest. (Note: CN I testing is usually deferred.)• CN II (optic). Test visual acuity with aSnellen chart and the Rosenbaum near-vision card.
• CN III (oculomotor), CN IV (trochlear),and CN VI (abducens). Assess these nerves
www.NursingMadeIncrediblyEasy.com March/April 2010 Nursing made Incredibly Easy! 17
peak technique

together using the corneal light reflextest, the six cardinal positions of gaze,and the cover-uncover test. Also, inspect thesize, shape, and symmetry of your patient’spupils and papillary reactions to light.• CN V (trigeminal). To assess the sensorycomponent of the trigeminal nerve, ask yourpatient to close his eyes and then touch himwith a wisp of cotton on his forehead, cheek,
and jaw on each side (see photo atleft). Next, test pain perception bytouching the tip of a safety pin tothe same three areas. Ask him todescribe and compare both sensa-tions. To test the motor compo-nent, ask him to clench his teethwhile you palpate the temporaland masseter muscles (see photosat bottom of page 17). Note thestrength of the muscle contraction;it should be equal bilaterally. Ifyour patient isn’t alert, test hiscorneal reflex by lightly touchingthe cornea with a fine wisp of cot-
ton. Look for the normal reaction of blinkingof the eyes. (Note: Corneal reflex testing isn’tdone on an alert patient.)• CN VII (facial). To assess the sensorycomponent, test taste by placing items with
various tastes on the anterior por-tion of your patient’s tongue, forexample, sweet, sour, and bitter.To test motor function, observehis face for symmetry at rest andwhile he smiles, frowns, andraises his eyebrows. Then havehim close both eyes tightly. Testmuscle strength by attempting toopen his eyes (see photo at left).• CN VIII (acoustic). To assessthis nerve, use Weber’s test—
strike a tuning fork lightly against yourhand and place the vibrating fork on yourpatient’s forehead at the midline or on thetop of his head—and the Rinne test—strikethe tuning fork against your hand and placethe vibrating fork over his mastoid process.• CN IX (glossopharyngeal) and CN X (vagus). Test these nerves together becausetheir innervation overlaps in the pharynx.Listen to your patient’s voice. Then checkhis gag reflex by touching the tip of a
tongue blade against his posterior pharynxand asking him to open wide and say “ah.”Watch for symmetrical upward movementof the soft palate and uvula and for themidline position of the uvula.• CN XI (spinal accessory). Assessthis nerve by testing the strength of the sternocleidomastoid muscles and the upper
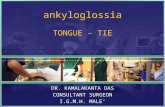
portion of the trapezius muscle (see photoabove).• CN XII (hypoglossal). Observe yourpatient’s tongue for symmetry. Histongue should bemidline withouttremors or mus-cle twitching.Test tonguestrength by asking him topush his tongueaga inst his cheekas you apply resistance (seephoto at right).
Assessing motor functionWhen assessing motor function, you’llwant to look at both sides of your patient’sbody simultaneously. On inspection, noteany asymmetry of muscle; unilateral atrophy will often indicate weakness.To assess the upper extremities, haveyour patient raise his arms parallel tothe floor or bed, and then have him re-sist when you try to push them down.You’ll do the same for the lower extremi-ties, having him raise his legs and resistwhen you push them down. You can alsohave him grasp your fingers in his fist,and then ask him to let go. If he can’t letgo on command, it’s indicative of neuro-logic injury.
18 Nursing made Incredibly Easy! March/April 2010 www.NursingMadeIncrediblyEasy.com
peak technique

To test for pronator drift, have yourpatient close his eyes so he can’t compen-sate and extend his arms, palms up, infront of him. Look for one arm to swayfrom its original position: a subtle indica-tor of weakness.
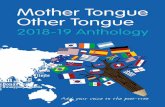
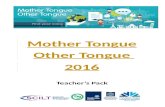
Assessing pupillary responseNow, we’ll move on to pupillary response.Along with eye motion, pupillary responseis controlled by cranial nerves III, IV, andVI. Normal pupils are of the same size bilaterally, about 2 to 6 mm and round (see Visualizing pupil size). About 15% of peoplehave one pupil up to 1 mm smaller than theother; this is a normal variant known asanisocoria.
To check pupil reactivity, bring a smallbeam of light in from the outer canthus ofone eye; the normal response is for bothpupils to react equally and briskly. Keep inmind that medications, surgery, and blind-ness can affect pupil size, shape, and reactiv-ity. The hallmark sign of severe neurologicinjury is a change in pupil size and reactivi-ty. Eye motion is tested by asking yourpatient to follow your finger as you trace theletter H in front of him. This is known asextraocular movement, or EOM. Documentany inability to follow your finger.
The focused assessmentAlthough a thorough neurologic assessmentyields valuable information, at times you’llneed to perform a focused neurologic as-sessment. You may have a patient with aneurologic diagnosis who develops achange. More likely, you may have a pa-tient with another diagnosis who developsa neurologic deficit. In these cases, it isn’tnecessary to perform the entire assessmentas previously described. Limit your exami-nation to LOC, motor strength, and pupil-lary reactivity. You’ll also want to includeother assessments you feel may yield im-
portant data. For example, if your patientdevelops slurred speech, you’ll want to in-clude an examination of the cranial nervesinvolved with speech.
Helpful tipsIn performing frequent neurologic assess-ments, I’ve found the following informationto be helpful.
Keep a cheat sheet. Remembering thefunction of each cranial nerve or the termi-nology to describe deficits is overwhelm-ing. Consult your cheat sheet for accu-rate documentation or when dis-cussing your findings with thehealthcare provider, as well as todetermine what additions youneed if you perform a focusedneurologic assessment.
Explain the assessment toyour patient and his familybefore you begin. Many peopleare frightened when they, or aloved one, develop a neurologicinjury, so they can becomefrustrated when you askthem to do such seeming-ly silly things as stick-ing out their tongues. Explain to your patientupfront that you’ll be asking him to answer aseries of questions and perform commandsthat may seem frivolous but are importantindicators of brain function. I also instructfamily members not to answer questions forthe patient, even if he seems to be strugglingto respond.
Peak performancePerforming a neurologic assessment canbe scary. But if you take your time anduse the proper resources, you can performa solid neurologic assessment no matterwhat. ■
Learn more about itBickley LS, Szilagyi PG. Bates’ Guide to Physical Examina-tion and History Taking. 10th ed. Philadelphia, PA: Lippin-cott Williams & Wilkins; 2009:671-689.
Health Assessment Made Incredibly Visual! Philadelphia, PA:Lippincott Williams & Wilkins; 2007:177-189.
Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Brunner &Suddarth’s Textbook of Medical-Surgical Nursing. 11th ed.Philadelphia, PA: Lippincott Williams & Wilkins;2008:2143-2152.
www.NursingMadeIncrediblyEasy.com March/April 2010 Nursing made Incredibly Easy! 19
Visualizing pupil size
1 2 3 4 5 6 7 mm
Follow thesesteps to perform
a successfulneurologic
assessment.