
Tongue Tie
37
ankyloglossia TONGUE – TIE DR. KAMALAKANTA DAS CONSULTANT SURGEON I.G.M.H. MALE’
-
Upload
kamalakanta-das -
Category
Documents
-
view
65 -
download
3
Transcript of Tongue Tie

ankyloglossia
TONGUE – TIE
DR. KAMALAKANTA DASCONSULTANT SURGEON
I.G.M.H. MALE’

What is tongue-tie?
• Tongue-tie (ankyloglossia) is a birth defect in which the tissue that attaches the tongue to the bottom of the mouth (lingual frenulum) is abnormally short.
• Movements of the tongue may be restricted, depending on the degree of attachment to the mouth.
• occurs more frequently in babies whose mothers abused cocaine during pregnancy

Lingual frenulum
The lingual frenulum is a band of tissue connecting the tongue to the bottom of the mouth.
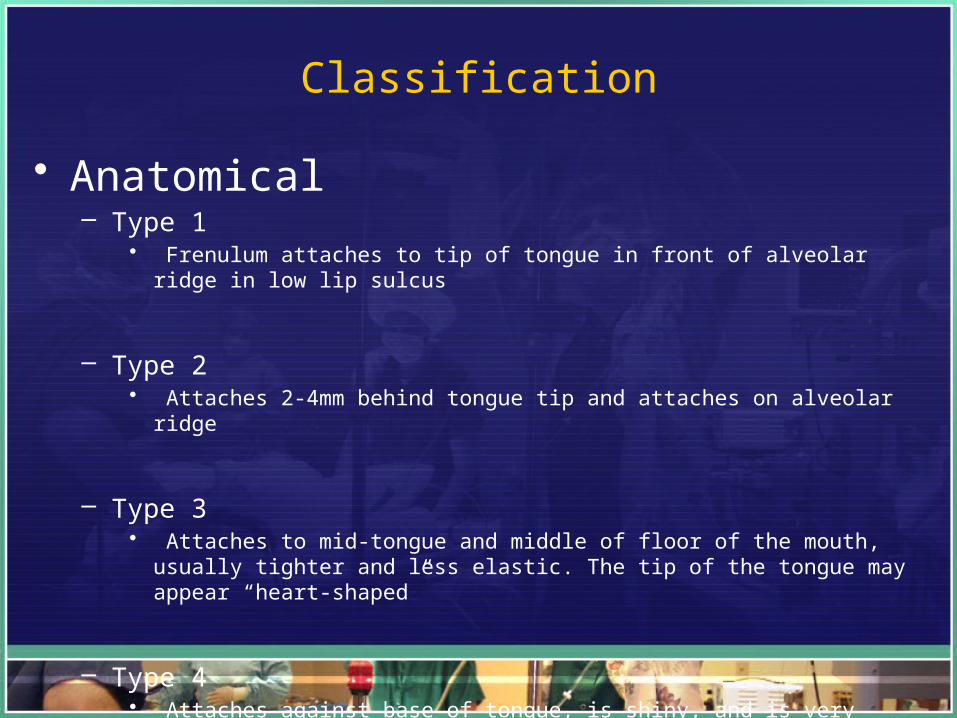
Classification
• Anatomical– Type 1
• Frenulum attaches to tip of tongue in front of alveolar ridge in low lip sulcus
– Type 2• Attaches 2-4mm behind tongue tip and attaches on alveolar ridge
– Type 3• Attaches to mid-tongue and middle of floor of the mouth, usually tighter and less
elastic. The tip of the tongue may appear “heart-shaped”
– Type 4• Attaches against base of tongue, is shiny, and is very inelastic

Symptoms
• 10% of babies born with some degree of tongue tie• Males to Females ratio 3:1• Babies :-
– Difficulty or inability to latch on– Constantly slipping off the breast– Excessive weight loss– Slow or no weight gain– Constant or very frequent feeding– Unsettled baby

At the start of each suck cycle the jaws compress the lactiferous sinus (A) tapping a bolus of milk. The tongue walls up at the top (B) and a wave of compression moves back along the tongue (C, D) compressing the nipple and breast tissue against the hard palate. The milk is swept towards the end of the nipple (E) and beyond to be swallowed.
• Mothers often complain of:-– Sore nipples– Pain during feeds– Engorgement or mastitis– Poor milk supply
• Older children :-– Speech problems
• the tip of the tongue cannot rise high enough to make (articulate) some sounds clearly
• such as t, d, z, s, th, n, and l.– Personal or social problems
• A child with tongue-tie may be ridiculed by peers
– Heart shape of tongue when raised.
– Cannot extend tongue out to a point.
– Tongue curves down when extended..
– Usually leads to a deviate swallow.

Downward protrusion shows deep notching and midline groove.

Diastema between lower incisors caused by frenum pulling on teeth.

Heart-shaped tongue, attempting protrusion.

Cup shaped tongue when attempting intra-oral elevation.

Trying to talk, eat, or swallow with a tight lingual frenum is like trying to run a marathon with your shoes
tied. together.
You will NEVER win a race until you are told about your problem!

Diagnosis
• Babies– Lift baby's tongue and examine lingual frenulum. The lingual
frenulum may be thick or thin and may extend to the tip of the tongue.
– Measure the strength of baby's suck by inserting a finger into the baby's mouth and noting how hard he or she sucks on it.
– Weigh baby and determine whether he or she weighs less than expected.
– Ask whether mother have sore nipples.– Watch mother breast-feed to see how well the baby latches on and
sucks.

• Older children or adults– Examine the mouth for:
• Restricted tongue movement : – Measure the tongue's protrusion beyond the lower teeth. – This measurement may be used as a comparison after tongue-tie surgery. – Looks for difficulty lifting the tongue to the upper teeth and upper lip – Look for limited side-to-side tongue movement.
• Abnormal spacing between the front lower teeth.– Caused by rubbing of the lingual frenulum during protrusion of the tongue.
• A notched or heart-shaped tongue when protruded. • The tongue may roll or curl when the person tries to protrude it.
• Other tests– Lactation consultant
• If primarily having breast-feeding difficulties• May be able to help teach the mother how to assist her baby in latching on and sucking effectively.
– Speech therapist • If speech problems• To rule out other conditions that could be causing the speech problem.

Management
Conservative• Breast feeding advice and counselling
Division of tongue tie• Evidence suggests that this procedure can improve breast
feeding (NICE). • One randomised controlled trial compared division of
tongue-tie with 48 hours of intensive support from a lactation consultant.
• 95% (19/20) of babies had improved breastfeeding 48 hours after tongue-tie division,
• compared with 5% (1/20) of babies in the control group (p < 0.001).

Surgical Indications
• Breastfeeding difficulties.• Speech impediments• Dental problems• Medical problems
— Indigestion — Snoring and sleep apnea
• Personal / Social reasons— Licking ice-cream cones— Kissing

Appropriate age for surgery
• Controversial.• Some experts believe that surgery should be done before
speech problems develop.• Others believe that surgery should be delayed until the child
is 4 years old and should be done only on children with speech difficulties.
• But delaying surgery may result in the child needing speech therapy after surgery to correct any altered speech patterns.

Surgery Options
• Frenotomy— No anesthetic needed— No suturing
• Frenectomy— Local or general anesthetic used— Sutures placed
• Z-plasty— More complex— Sutures placed

Frenotomy technique
• Done in the hospital's new-born nursery or in a doctor's office without anaesthesia or with a local anaesthetic
• Parent holds and stabilizes head• Stabilize and elevate tongue• Clip center of frenum (1 cm)
— Frenum is poorly vascularized.— Frenum is poorly innervated
• Infant can breastfeed immediately

Frenotomy
During a Frenotomy to repair tongue-tie, the doctor clips (cuts) the lingual frenulum. The frenulum is the tissue that attaches the tongue to the floor of the mouth. Most babies don't need stitches afterward.

Tongue ready for Frenotomy

Approximate area of snip for Frenotomy

Frenectomy
• It is the preferred surgery for child over the age of 1 or 2 years .
• General Anaesthesia for younger children and Local anaesthetics for older children and adults.
• Clipping the lingual frenulum to release the tongue and then suturing the resulting triangular-shaped wound.
• Pressure may be applied to stop any bleeding that occurs.

Frenectomy for tongue-tie
Frenectomy is a procedure in which a health professional clips the tissue (lingual frenulum) that attaches the tongue to the floor of the mouth. Stitches are used to close the resulting triangular-shaped wound, and pressure may be applied to stop any bleeding that occurs.

Frenectomy

Area of tongue that would be incised (yellow)

Area of sutures (green)

Z-Plasty

Area of Incision for Z-plasty

Placement of Z-plasty sutures

Z-plasty : sutures elevate tongue

Multiple small Z-plasty incisions

Sutures being placed

10 day healing can elevate tongue higher now

Things to remember….
• All babies should have had Vitamin K administered at birth or at least 1 day prior to the procedure.
• Post-operatively, babies will require a period of observation for at least 4 hours. – Ex-premature infants should have a longer observation
period in view of the increased risk of apnoea.
• Paracetamol may be given as needed. • If mothers are Hepatitis C positive, breast feeding
should be postponed until the wound has healed.

Complications
• Infection at the site.• Excessive bleeding.• Recurrent tongue-tie from scar tissue formation.
– Tongue-tie may be more likely to recur after a simple release of the tissue (Frenotomy) than after Frenectomy / frenuloplasty. If tongue-tie recurs, it is generally less severe than it was before the surgery.
• Tongue exercises several times daily for about 4 to 6 weeks after the surgery. – strengthen the tongue muscle– improve mobility of the tongue– reduce the chances of scar tissue formation.
Thank you !!


















