Sileshi prematurity and lbw
61
UNIVERSTY OF Gondar COLLEGE OF MEDICINE and HEALTH SCIENCE PREMATURITY AND LOW BIRTH WEIGHT SILESHI MULATU (2 nd YEAR MSc, PEDIATRICS NURSE STUDENT) E-mail- [email protected]
-
Upload
sileshi-mulatu -
Category
Healthcare
-
view
35 -
download
3
Transcript of Sileshi prematurity and lbw

1
UNIVERSTY OF Gondar COLLEGE OF
MEDICINE and HEALTH SCIENCE
PREMATURITY AND LOW BIRTH WEIGHT
SILESHI MULATU (2nd
YEAR MSc, PEDIATRICS NURSE STUDENT)
E-mail- [email protected]

Presentation outline
• Introduction
• Definitions
• Cause
• Epidemiology
• Complications
• Management
• Intervention
• Evidence
• Reference
2

IntroductionNewborn death and illness• The fourth Millennium Development Goal (MDG 4) aims to
reduce the 1990 mortality rate among under-five children by two thirds.
• Child mortality is also closely linked to MDG 5- to improvematernal health.
• Since more than one third of all child deaths occur within thefirst month of life, providing skilled care to mothers duringpregnancy, as well as during and after birth, greatly contributesto child survival.
3

Newborn death and illness• World wide about 4 million newborn babies die each year
• Another 4 million babies each year are stillborn;
• Most newborn deaths occur in developing countries.
• The same statistics show that about two-thirds of deaths in the first year of life occur in the first month of life; of those who die in the first month, about two-thirds die in the first week of life and of those who die in the first week, two-thirds die in the first 24 hours of life.
• Eighty-five percent of newborn deaths are due to the following main causes: infection, birth asphyxia, and complications of prematurity and low birth weight (LBW).
4
Causes of newborn death
• The three major causes of neonatal deaths worldwideare infections (36%, which includes sepsis/pneumonia,tetanus and diarrhea), pre-term (28%), and birthasphyxia (23%).
• There is some variation between countries dependingon their care configurations
2005 World Health Report
5

6

What is prematurity ? 7

What do the terms prematurity mean ?
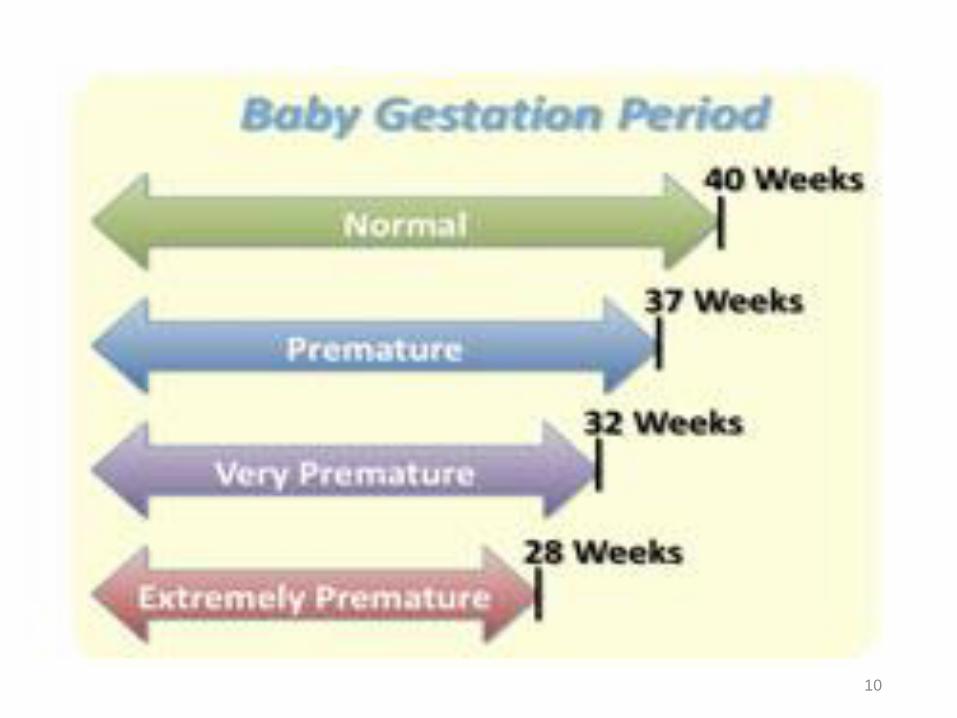
• Normally, babies are born at approximately 40 weeks’ gestation.
• Preterm birth is defined by WHO as all births before 37 completedweeks of gestation or fewer than 259 days since the first day of awoman’s last menstrual period
• Very premature babies are those born before 32 weeks’ gestation,and extremely premature babies are those born before 28 weeks’gestation
WHO, 2005
8
What do the terms “premature…….Premature 32-36 weeks
Feeding and temperature problems, some have immaturelungs
Moderate 28-31 weeksImmature lungs, poor temperature control, feeding
problems, apneas
Severe < 28 weeksImmature organ systems, intensive care
9
10

prematurity• More than 1 in 10 of the world’s babies born in 2010
were born prematurely, making an estimated 15 millionpreterm births, of which more than 1 million died asa result of their prematurity (Blencowe et al, 2012)
• Prematurity is now the second leading cause of death inchildren under 5 years and the single most importantcause of death in the first month of life (Liu et al., 2012).
11

prematurity• Preterm birth is a major cause of death and a significant
cause of long-term loss of human potential amongst
survivors all around the world.
• Complications of preterm birth are the single largest direct
cause of neonatal deaths, responsible for 35% of the world’s
3.1 million deaths a year, and the second most common
cause of under-5 deaths after pneumonia
12

prematurity• In almost all high- and middle income countries of the
world, preterm birth is the leading cause of child death (Liuet al., 2012).
• Being born preterm also increases a baby’s risk of dying dueto other causes, especially from neonatal infections withpreterm birth estimated to be a risk factor in at least 50% ofall neonatal deaths
Lawn et al., 201013

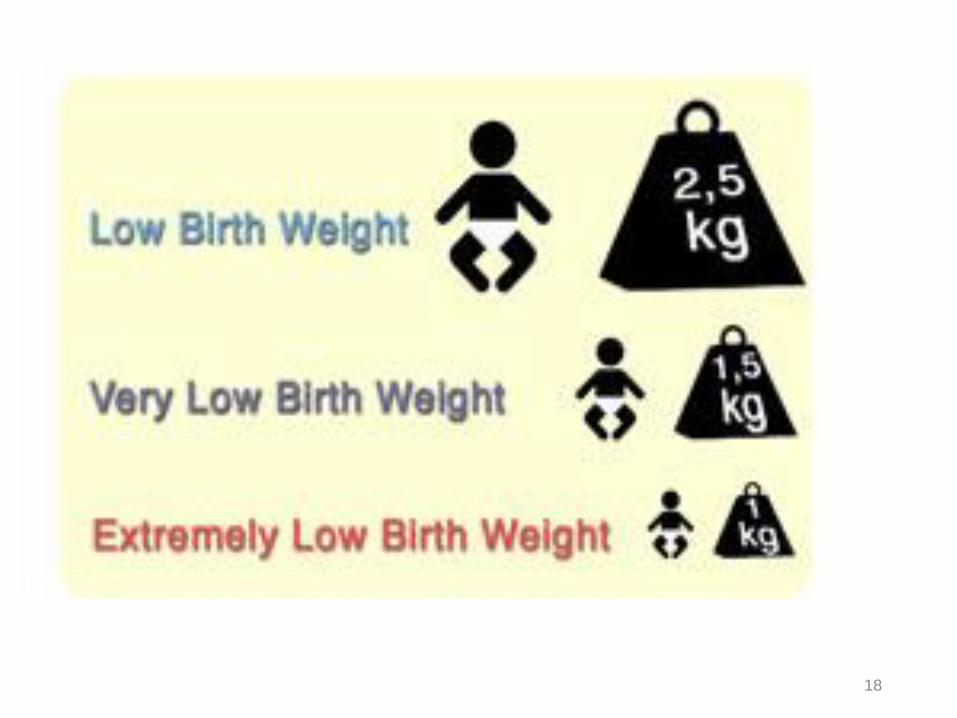
What is low birth weight ?• Babies who weigh less than 2500 grams are considered low birth
weight (LBW).
• Globally, more than 20 million infants are born with Low BirthWeight (LBW) and a larger proportion of these concentrating inAsia and Africa
• Most of LBW babies are premature. However, other conditions cancause LBW in a baby born after s full-term pregnancy, such assmoking during pregnancy.
14

What is low birth weight 2• Weight at birth is an important determinant of the
newborn to survive and experience healthy growthand development.
• Fetal growth and birth weight are influenced by avariety of factors racial, social, and economic amongothers, as well as specific medical conditions that maybe present or may develop during pregnancy
East African Medical Journal, 7 July 2006
15

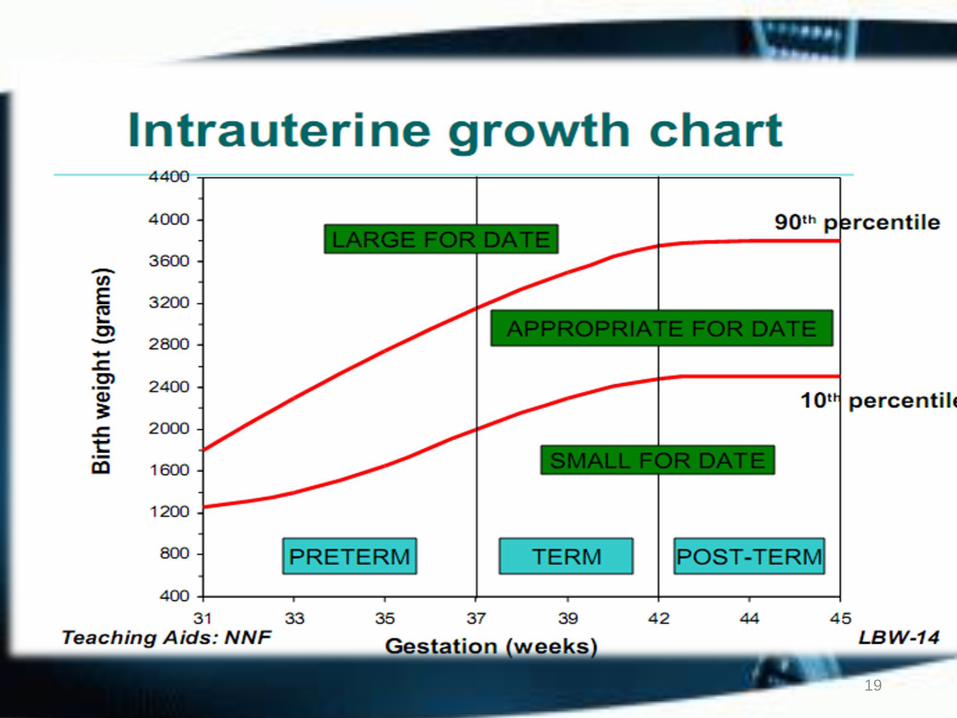
What is low birth weight..... 3• Some babies with LBW are full term but underweight
• Others are premature and weight less than they should
• These infants are called intrauterine growth restriction (IUGR)
or small for gestational age (SGA).
• Data on the incidence of LBW world wide regularly collected
by WHO revealed the incidence of LBW range from 7% in
Ethiopia to 14% in Africa and 31% in middle South Asia
• East African Medical Journal
16
What is low birth weight..... 4• Although LBW is generally linked to prematurity.
• In fact, only 70% of low birth weight babies were bornpremature
• Low birth weight is defined as less than 2,500 grams,very low birth weight as less than 1,500 grams andextremely low birth weight as less than 1,000 grams
17
18
19

Cause of prematurity• Preterm birth is a syndrome with a variety of causes which can be
classified into two broad subtypes:1. spontaneous preterm birth (spontaneous onset of labor or following
prelabor premature rupture of membranes and2. provider-initiated preterm birth (defined as induction of labor or
elective caesarian birth before 37 completed weeks of gestation formaternal or fetal indications or other non-medical reasons)
• Most preterm births happen spontaneously
• Common causes include multiple pregnancies, infections andchronic conditions, such as diabetes and high blood pressure
• There is also a genetic influence.
Goldenberg et al., 201220

Cause of prematurity• Spontaneous preterm birth is a multi-factorial process
• The precursors to spontaneous preterm birth vary by
environmental factors, but the cause of spontaneous preterm
labor remains unidentified in up to half of all cases
(Menon, 2008)
• Maternal history of preterm birth is a strong risk factor and
most likely driven by the interaction of genetic and
environmental risk factors (Plunkett and Muglia, 2008)21
Cause of prematurity• Age of the mothers also the risk, a study in Ireland women who gave
birth during the teenage years were at increased risk of preterm andvery preterm delivery.
• This risk was higher for younger teenager mothers (14-17 yrs.) than forolder teenagers (18-19 yrs.) and in the 14-17 yrs.
• old group the risk was greater in second pregnancies than in first in asimilar cross sectional study from the UK, Smith and Pell described anincreased risk of both preterm and very preterm birth in teenage womenand this risk was greatest for second births.
Khashan et al, 2010
22

Cause of prematurity• Adolescent pregnancy, short time gaps between births,
unhealthy pre-pregnancy weight (underweight orobesity), chronic disease (e.g. diabetes), infectiousdiseases (e.g. HIV), substance abuse (e.g. tobacco use andheavy alcohol use) and poor psychological health arerisk factors for preterm birth.
23

Clinical Manifestation of premature
• Body hair (lanugo)
• Abnormal breathing patterns (shallow, irregularpauses in breathing called apnea)
• Enlarged clitoris (female infant)
• Problems breathing due to immature lungs (neonatalrespiratory distress syndrome) or pneumonia

Clinical Manifestation• Lower muscle tone and less activity than full-term infants
• Problems feeding due to difficulty sucking or coordinatingswallowing and breathing
• Less body fat Small scrotum, smooth without ridges, andundescended testicles (male infant)
• Soft, flexible ear cartilage
• Thin, smooth, shiny skin, which is often transparent (can seeveins under skin)
25

Epidemiology of prematurity …...1• Over 60% of preterm births occur in Africa and South
Asia
• Of the 11 countries with preterm birth rates of over 15%, all but two are in sub-Saharan Africa.
• In the poorest countries, on average, 12% of babies are born too soon compared with 9% in higher-income countries.
• Within countries, poorer families are at higher risk.26

27
Epidemiology of prematurity …..2

28
Epidemiology of prematurity ……3

Preterm babies face specific risks…...1• Feeding difficulties since the coordinated suck and swallow
process only starts at 34 weeks gestation.
• Preterm babies need help to feed and are more likely to aspirate.
• Severe infections are more common, and premature babies are athigher risk of dying once they get an infection.
• The majority of babies who die from neonatal sepsis are preterm.
• Respiratory Distress Syndrome due to lung immaturity and lackof surfactant in the alveoli, resulting in collapsing lungs that takeextra pressure to inflate.
29

Preterm babies face specific risks ….2• Jaundice is more common in premature babies since the
immature liver cannot easily metabolize bilirubin, and oncejaundiced, the preterm baby’s brain is at higher risk since theirblood-brain barrier is less well developed to protect the brain
• Brain injury it is most commonly intraventricular hemorrhage,occurring in the first few days after birth
• Low blood sugar (hypoglycemia) or hypocalcemia.
• Heart problems, A common condition is PDA
30

Preterm babies face specific risks…..3• Preterm babies may have hypoxic brain injury with white matter
loss which differs from that seen in the brain of term babies
• Retinopathy of prematurity due to abnormal proliferation of theblood vessels around the retina of the eye, which is more severe ifthe baby is given too high levels of oxygen.
• Anemia of prematurity, which often becomes apparent at a fewweeks of age due to delay in producing RBCs as the bone marrowis immature.
31

Preterm babies face specific risks …4• In addition to its significant contribution to mortality, the effect of
preterm birth may continue throughout life,
impairing neurodevelopmental functioning through increasing
the risk of cerebral palsy,
learning impairment and visual disorders and
affecting long-term physical health with a higher risk of non-
communicable disease
Rogers and Velten, 2011
32

33

Management of premature baby• Each year 15 million babies are born preterm and their
survival chances vary dramatically around the world(Blencowe et al., 2012)
• Worldwide, almost half of preterm babies are born athome, and even for those born in facilities, essentialnewborn care is often lacking.
• Most premature babies (>80%) are born between 32 and37 weeks of gestation (moderate/late preterm), and dieneedlessly for lack of simple, essential care such aswarmth and feeding support.
34

Management…..• All newborn babies are vulnerable given that birth
and the following few days hold the highestconcentrated risk of death of any time in thehuman lifespan.
• Every baby needs essential newborn care, ideallywith their mothers providing warmth, breastfeeding and a clean environment.
35

1. Essential and extra newborn careA. Thermal care: Simple methods to maintain a baby’s
temperature after birth include drying and wrapping, increasedenvironmental temperature, covering the baby’s head (e.g., with aknitted cap), skin-to-skin contact with the mother and coveringboth with a blanket (McCall et al, 2005) (WHO, 1997a).
• Delaying the first bath is promoted
• Kangaroo Mother Care (KMC) has decreased mortality effect forbabies <2,000 g
36

• Equipment-dependent warming techniques includewarming pads or warm cots, radiant heaters orincubators and these also require additional nursingskills and careful monitoring (WHO, 1997a).
37

B. Feeding support• Early initiation of breastfeeding within one hour after
birth has been shown to reduce neonatal mortality(Bhutta et al., 2008; Mullany et al., 2008).
• Premature babies benefit from breast milknutritionally, immunologically and developmentallythe short-term and long-term benefits compared withformula feeding are well
(Callen and Pinelli, 2005). 38

• Extremely preterm babies under about 1,000 g and babies who arevery unwell may require intravenous fluids or even totalparenteral nutrition, but this requires meticulous attention tovolume and flow rates.
• Total parenteral nutrition, or intravenous (IV) feeding, is neededfor some very small or sick infants who can’t be fed any other way.
• Tis advanced care that requires very careful monitoring.
39
B. Feeding support

C. Infection prevention• Clean birth practices reduce maternal and neonatal mortality
and morbidity from infection-related causes, including tetanus(Blencowe et al., 2011).
• Premature babies have a higher risk of bacterial sepsis.
• Hand cleansing is especially critical in neonatal care units.
• However basic hygienic practices such as hand washing andmaintaining a clean environment are well known but poorlydone
40

Infection : • Antibiotics• supporting treatment :
nutrition oxygenation warmth
• immunotherapy ; if it is needed
41

2. Neonatal resuscitation• Between 5 to 10% of all newborns and a greater percentage of
premature babies require assistance to begin breathing at birth(Wall et al., 2009).
• Basic resuscitation through use of a bag-and-mask or mouth-to-mask (tube and mask) will save four out of every five babies whoneed resuscitation
• More complex procedures, such as endotracheal intubation, arerequired only for a minority of babies who do not breathe atbirth and who are also likely to need ongoing ventilation.
42

3. Kangaroo Mother Care• KMC was developed in the 1970s by a Colombian pediatrician,
Edgar Rey, who sought a solution to incubator shortages, highinfection rates and abandonment among preterm births in hishospital (Charpak et al., 2005; Rey and Martinez, 1983).
• The premature baby is put in early, prolonged and continuousdirect skin-to-skin contact with her mother or another familymember to provide stable warmth and to encourage frequentand exclusive breastfeeding.
43

Special care and neonatal intensive care• Moderately-premature babies without complications
can be cared for with their mothers on normal postnatalwards or at home, but babies under 32 weeks gestationare at greater risk of developing complications and willusually require hospital admission.
• Fewer babies are born under 28 weeks of gestation andmost of these will require intensive care.
44

45

46

Interventions during pregnancy1. Services delivered during antenatal care:
• Situational interventions (identification and treatment of malaria, TB and HIV)
• Additional interventions as needed (e.g., behavioral, social support andfinancial interventions, nutritional interventions including calciumsupplementation)
2. Management of pregnant women at higher risk of preterm birth including:
• Identification and treatment of hypertensive disease in pregnancy
• Monitoring multiple pregnancies
• Administration of progesterone to prolong pregnancy
• Identification and treatment of structural abnormalities (e.g., cervical CA)
47

Interventions3. Management of women in preterm labor including:
Tocolytics to slow down labor
Antenatal corticosteroids to reduce mortality in the newborn
Antibiotics for PPROM to prevent infection
Provision of magnesium sulphate for neuro-protection of the newborn
4. Community interventions:
Promote antenatal and skilled delivery care for all women
Smoking cessation and reducing exposure to secondhand smoke and
other pollutants
48

5. Policy interventions:• Policies to support safe motherhood and universal
access to antenatal care
• Workplace policies regulating working hours andstrenuous working conditions
• Professional and hospital policies to regulateinfertility treatments and to reduce cesarean birthrates and early induction of labor
49

prevention• Good prenatal care is the best way to reduce your baby’s
risk of premature birth.
• Not smoking during pregnancy can reduce the risk of
having a LBW baby.
50

prevention• Despite all the preventive measures and available information, not
all cases of prematurity and low birth weight can be prevented.
• This is because the main causes of prematurity and low birthweight include preeclampsia, infection, multiple pregnancy (e.g.,twins), high blood pressure, and drug and alcohol abuse.
• In fact, the rate of preterm births has been increasing for almosttwenty years. So what happens to babies who are bornprematurely?
51

Evidence• Multiple pregnancies (twins, triplets, etc.) carry nearly 10 times the risk of
preterm birth compared to single births
• Mehdi Ranjbaran, 2015
• In the study systematic review and meta-analyses, underweight women havehigher risks of overall, spontaneous and induced premature <37 weeks andLBW <2500 g.
International Journal of Epidemiology 2011
• Study that conducted in University of Gondar, on birth outcome 11% ofparticipants had history of fever of 2 weeks or more during pregnancy and 10%had been diagnosed anemic during the current pregnancy.
Adane et al, 201452

Evidence• Women who develop anemia and not attending ANC during
pregnancy, had 15% and 41% added risk of having small sizebabies than their counterparts
Taddese Alemu, 2015
• Studies shows that conditions including gestational age, maternalage, regular antenatal checkup, mother’s height, mother’s weight,anemia, physical work, tobacco chewing, and history of abortionare significant determinants of LBW
Agarwal A, 2011
53

Evidence• Multiple birth, gestational weight gain and gestational age has
significant relationship with LBW.Mehdi Ranjbaran, 2015
• Many factors affect LBW among which the most important onesare genetic, environmental, fetal, placental gestational andmaternal factors
Singh, G, R, 2009
• Women who had history of either preterm delivery or LBW were3.1 more like to have preterm birth than their counter parts.
Adane et al, 201454

EvidenceSmall size neonates at birth were 2 times more likely to diecompared with medium sized ones.
Bekana Kebede, Abebaw Gebeyehu, Hardeep Rai Sharma, Sisay Yifru
55

Evidence• Study conducted on BW by GA Birth weights were 700-1,000
grams between 26 and 36 weeks of pregnancy.
• 35 and 54% of neonates were very-low and low birth weight,respectively, without sex difference.
Mekonen et al, 2015
• In the LBW group, 87.3% (n = 453) were singleton, while 12.1%(n = 63) were twin and 0.6% (n = 3) were triple pregnancies.
Golestan M, 2011
56

Evidence• The study conducted in Axum show that the burden of
low birth weight deliveries is associated withinadequate ANC service utilization and unwantedpregnancy which deserve goal oriented prenatal careand choice based family planning service provision bythe respective health facilities
Negassi Teklehaimanot et al,2014
57

Summary• Premature birth and low birth weight (LBW) still a health problem
with high Morbidity and mortality • The survival at high risk of LBW for long term neurocognitive
deficits • Three types of LBW and premature • Problems accordingly to the type
• Management consist of : warmth, feeding, management of complication
• Breast feeding is prioritized, in case of breastmilk is not available, consider milk formula
58

Reference1. Young P.N. Birth weight in 60 hospital delivered infants in Addis Ababa and
Gondar. Ethiopia Med. J. 1967; 6: 15-17.
2. Agrawal V, Agrawal P, Chaudhary V, Agarwal K, Agarwal A (2011) Prevalenceand determinants of “low birth weight” among institutional eliveries. Ann NigerMed 5: 48.
3. Singh, G, R. Chouhan and K. Sidhu, 2009. Maternal factors for low birth weightbabies, Medical Journal Armed Forces India, 65(1): 10-12.
4. Negassi Teklehaimanot, Tesfay Hailu, Huruy Assefa. Prevalence and FactorsAssociated with Low Birth Weight in Axum and Laelay Maichew Districts,North Ethiopia: A Comparative Cross Sectional Study. International Journal ofNutrition and Food Sciences. Vol. 3, No. 6, 2014, pp. 560-566. doi:10.11648/j.ijnfs.20140306.21 59

Reference1. Zhen Han, et al. (2011) Knowledge Synthesis Groupy Maternal underweight
and the risk of preterm birth and low birth weight: a systematic review andmeta-analyses
2. Adane et al. Adverse birth outcomes among deliveries at Gondar UniversityHospital, Northwest Ethiopia. BMC Pregnancy and Childbirth 2014 14:90.
3. Bekana Kebede1et al, Prevalence and associated factors of neonatal mortalityin North Gondar Zone, Northwest Ethiopia
60

Thanks to watching my story