
Seventh International Symposium in Continuing Nursing Education/March 2014 Donald W. McLaren, MD.
75
TYPHOID FEVER Seventh International Symposium in Continuing Nursing Education/March 2014 Donald W. McLaren, MD
-
Upload
sheila-turner -
Category
Documents
-
view
222 -
download
1
Transcript of Seventh International Symposium in Continuing Nursing Education/March 2014 Donald W. McLaren, MD.

TYPHOID FEVER
Seventh International Symposium in Continuing Nursing Education/March
2014
Donald W. McLaren, MD

PURPOSE OF TALK To discuss epidemiology of typhoid To discuss myriad of ways Typhoid can
present To discuss challenges in diagnosis and
give some guidelines for diagnosis To discuss antibiotic resistance patterns
and treatment recommendations for Typhoid


INTRODUCTION Typhoid or Enteric fever is a systemic
illness with fever and abdominal symptoms
Caused by S. Typhi & paratyphi A, B, and C
Now known as Salmonella enterica serotypes Typhi and Paratyphi A,B and C
Typhi meaning “typhus like” according to one source. From Greek typhos - an ethereal smoke or cloud that was believed to cause illness and madness
SHORT HISTORY OF TYPHOID Known 2000 years ago - may have been cause
of Great Plague of Athens at end of Pelopennesian War 431-404 B.C.
1659 First description of epidemic typhoid 1837 first differentiated from typhus 1880 Carl Eberth discovered typhoid bacillus 1896 Widal test described by George Widal 1948 Antibiotic treatment became available Increasing drug resistance since emergence of
Multidrug resistance (MDR) 1984-1989

© Homeschool Freebie of the Day. .

http://quigleyscabinet.blogspot.com/2010/07/typhoid-mary.html

“TYPHOID MARY” Mary Mallon (born 1869)
Emigrated from Ireland at about age 15First healthy carrier identified in the U.S.Unfortunately worked as a cookHired by Charles Warren, investment
banker6 of 11 in his household became infectedHired civil engineer George Soper to
investigateSuspected Ms. Mallon but getting stool
and blood specimen proved to be a real challenge

“TYPHOID MARY” CONTINUED
She with knife in hand put up resistanceAfter unsuccessful attempts, 5 police officers
took 5 hours to find her hiding in a closetKnown infected 47 – maybe many more – 3
died Initially quarantined 3 years but released
upon promise never to cook again for othersReleased once but started cooking againLived in enforced quarantine for 23 more
yearsWas demonized and butt of jokesBecame term for disease carrier

ETIOLOGY/BACTERIOLOGY Salmonella species – Typhi, Paratyphi A,B,C. Typhi > Paratyphi: equal in severity now Highly specific to humans - infection means
contact with infected individual, chronic carrier or contaminated food or water
3 common antigens – O (body), H (flagella), Vi (virulence antigen – lacking in about 10%)
Resistance to Amp, chloramphenicol (CMP), TMP/SMX (Multidrug resistance or MDR) a worldwide problem since 1989; increasing resistance to fluoroquinolones (FLQ)

EPIDEMIOLOGY 200-300 cases / year in U.S. 314 in 2006
– about 0.42/100,000 travelers 80% have travelled (< 20% traced to
carrier) – 2/3 to India Almost none had gotten the vaccine. Most cases from India (47%), Pakistan,
Mexico, Bangladesh India area travel (>100 case / million
travelers); SE Asia and Africa 5-14/million Highest rate if visiting friends, relatives

© 2014 Top-10-List.com. All Rights Reserved. http://top-10-list.org/2010/02/27/top-10-epidemics-list/2/

EPIDEMIOLOGY Infects > 21 mil/yr, kills >200,000 worldwide Most prevalent in impoverished areas with
overcrowding and poor access to sanitation. Mortality 9-13% pre antibiotics – now < 1% Incidence
South-central and SE Asia, Southern Africa > 100 cases / 100,000 person years
Rest of Asia, Africa, Latin America, Oceana 10-100 cases/ 100,000 person years (but poor reporting)
Percentage of paratyphi rising Resistance increasing from <1% 1986-89 to
>12% Children < 1 more susceptible, more severe

© Society for Science & the Public 2000 - 2013. All rights reserved. https://www.sciencenews.org/article/cheap-shots-%E2%80%94-typhoid-vaccine-shows-broad-coverage


PATHOPHYSIOLOGY Greater dose - higher attack rate, shorter
incubation. About 30% of volunteers given 105 CFU, 10-20% with 103 CFU develop illness
Most cases get low dose with low attack rate and long incubation of 2-3 weeks.
Ingested - pass stomach to SB. Doesn’t tend to cause fulminant enteritis as do non–typhi salmonella; 10-20% get D at some point.
Phagocytic cells take to sub-mucosal region and proliferate – primarily at terminal ileum

PATHOPHYSIOLOGY Enter Peyer’s patches which hypertrophy -
lymphs and mononuclear cells recruited. Necrosis of sub-mucosal tissue leads to
abdominal pain, sometimes ileal perforation.
Dissemination from Peyer’s patches through lymphatic system, blood to replicate in the reticuloendothelial system
This is a major part of Typhoid which can leads to prostration, sepsis, H-S megaly. (Primary bacteremia often silent)

PATHOPHYSIOLOGY Remain in mononuclear cells in the liver,
spleen, LNs, bone marrow (Source of relapse, late complications)
Proliferate then break into bloodstream Need Fe for growth. Hemochromatosis carriers
and carriers of cystic fibrosis gene have decreased susceptibility (and to cholera and Tb)
Low stomach acid (PPIs) - more susceptibile
Evidence mixed whether immune def (HIV) leads to more severe or complicated typhoid as it does for other salmonella organisms, but fare worse
CLINICAL – GREAT IMITATOR HTTP://WWW.WORLDORTHO.COM/DEV/INDEX.PHP?OPTION=COM_CONTENT&TASK=VIEW&ID=1778&ITEMID=420
“A case of typhoid fever may present as a disease clinically indistinguishable from malaria, progress to a bacillary dysentery, mimic a case of acute bronchitis, simulate a fully fledged lobar pneumonia, cause an acute abdomen with perforation, and then finally in convalescence, with its evil spent, linger on as an orchitis, a myocarditis or a peripheral neuritis. The Seven Ages of Man are scarcely greater, or more diverse in their span, or the stage more prone to variety.”

CLINICAL – GREAT IMITATOR* “Typhoid fever usually presents
nonspecifically with abdominal pain, fever, chills and constitutional symptoms; as a result many other diagnoses may be entertained”
Hohmann EL. Epidemiology, microbiology, clinical manifestations, and diagnosis of typhoid fever. UpToDate 2010. UpToDate.com
CLINICAL Personal experience: one of hardest
common tropical diseases to dx early and accurately
Highly variable presentation Often nonspecific symptoms Many organs can be effected Can mimic many other diseases No good quick accurate test to diagnose Test most often used to diagnose in
third world is totally unreliable

CLASSIC PRESENTATION IF NOT TREATED
Starts 7-14 (5-21) days after ingestion Week 1 - stepwise fever increase. Chills
common. Abdominal pain. Bacteremia. (Constipation in some - Dry cough, HA, delirium and malaise)
Week 2 Fever plateaus: 103-4. Rose spots, abdominal pain. Relative bradycardia and dicrotic pulse. (abdominal distension and splenomegaly)
Week 3 – More toxic, anorexic. Tachycardia. Bowel perforation, other complications, death possible.
Week 4 Slow improvement/resolution over weeks-months, but can still get neuro, GI complications. Weight loss and debilitation can last for months.

CLINICAL HISTORY Can vary a lot from classic presentation. Tends to be insidious onset Only 12% have classic stepwise fever Can develop D instead of constipation
(especially in AIDS, children, but in 1/3 of normal persons, specific to some outbreaks)
Non-localizing abdominal pain Non specific flu like symptoms Many atypical presentations

CLINICAL HISTORY
Strickland, GT (ed). Hunter’s Tropical Medicine and Emerging Infectious Diseases, Eight Edition. Philadelphia: W. B. Saunders Company, 2000. p 477

CLINICAL FEATURES Fever most prominent feature and lasts
3-4 weeks untreated. Tends not to be sudden and high (unlike
Dengue or Malaria) Tends to be stepwise (think 2 steps
forward, and 1 step back each day) Relative bradycardia common – slower
than would be expected for degree of fever but not very helpful sign

17Strickland, GT (ed). Hunter’s Tropical Medicine and Emerging Infectious Diseases, Eight Edition. Philadelphia: W. B. Saunders Company, 2000. p 477

Magill AJ, et. Al. Hunter’s Tropical Medicine and Emerging Infectious Diseases. China: Saunders Elsevier, 2013. pp 568-576

CLINICAL – USEFUL PHYSICAL SIGNS Rose spots – small blanching 2-4
salmon-pink colored macules or M-P rash mainly on chest, abdomen and back. 30% at end of first week. Lasts 2-5 days. Organism grows from lesions which are clumps of bacteria, cells.
Coated tongue – varies from 50-95%. White, yellow or brown sparing edge of tongue.
Stepwise rise in temperature

ROSE SPOTS (HTTP://EN.WIKIPEDIA.ORG/WIKI/FILE:SALMONELLA_TYPHI_TYPHOID_FEVER_PHIL_2215_LORES.JPG

http://www.zipheal.com/typhoid/typhoid-fever-symptoms/3761

Copyright ©2004 Canadian Medical Association or its licensors
Bal, S. K. et al. CMAJ 2004;170:1095
Figure 1

CLINICAL – CLASSIC FEVER CURVE HTTP://WWW.WORLDORTHO.COM/DEV/INDEX.PHP?
OPTION=COM_CONTENT&TASK=VIEW&ID=1786&ITEMID=420

http://www.henriettes-herb.com - Copyright 1995-2014 Henriette Kress.

USEFUL S/S POINTING TO TYPHOID Must have high index of suspicion Insidious onset – not sudden high
fever If present classic fever curve Coated tongue Rose spots Often have abdominal findings. If malaria ruled out or already
treated, and fever continues > 1 week must consider typhoid.

FROM HUNTER’S – IN ENDEMIC AREA:
Must have high index suspicion Consider if > 3 days non-focal fever. Good hx, px, lab can R/O other
conditions Increased suspicion if: young age, T > 39oC,
ill appearance and any abdominal symptoms. Consider W/U if >3 days non-localizing fever
+ any of these features Likelihood this is typhoid increases with
length of fever: If > 7 days should be evaluated and treated
(Magill AJ, et. Al. Hunter’s Tropical Medicine and Emerging Infectious Diseases. China: Saunders Elsevier, 2013. pp 568-576

OTHER PRESENTATIONS Can present as pneumonia Massive rectal bleeding Delirium and coma Uncommon: hepato-biliary, CNS, CVS,
Respiratory, GU, MS system complications.
Severe presentation ill or toxic appearing, febrile > 1 week, moderate abdominal pain, constipation or diarrhea.
Death most likely from GI perf, hemorrhage, encephalopathy, seizures or pneumonia
OTHER USEFUL SIGNS Malaise, anorexia and lassitude are
prominent in many cases. HA is common Dry cough is common as is vague
abdominal discomfort is common, constipation
Less common in antibiotic era Much less splenomegaly (60 to 10%) Fewer have rose spots (30 to 1.5%) Much lower mortality (15 to < 1%) Diarrhea now more common than constipation
especially in children and varies with location.

LAB Not real helpful but Anemia (normocytic) common WBC normal or decreased (15-30%) but Tends to be increased in children, or if
perforation. Increased ESR Thrombocytopenia common LFTs (ALT, AST, bili) about double in
90+% LDH, CPK often elevated; Na, K can be
low

DIAGNOSIS Definitive diagnosis a + culture
Positive from different places at different timesBone marrow most consistently +
throughout disease – 90% sensitive up to 5 days after antibiotics started
Stool + 30-50% early; 20% 2nd week; higher with later increased shedding from GB. Urine less.
Blood 90% week 1, but less after first weekBlood overall 40-80%. Can increase with high
volume culture (10-15 cc) and multiple culturesRose spots – about 60% positive culture

DIAGNOSIS – SEROLOGICAL TESTING Widal - measures agglutinating antibodies
to H, O antigens of S. Typhi. Not specific, sensitive enough – no
longer considered acceptable for diagnosis.
Positive if prior infection or immunization.
Great lab to lab variability – most not reliable
O titer more specific, H more sensitive – > 1:160 (O titer) positive + in non-endemic area but 1:640 in endemic

DIAGNOSIS CONTINUED Fourfold increase in paired titers 2
weeks apart helpful in half of cases. Really not positive till 6-8 days (O)
and 10-12 days (H) and negative in up to 30% of culture proven cases. Peaks week 3-5
Newer tests probably not available on field; not that helpful acutely since antibodies not present at beginning of illness, not very available. Includes PCR

COMPLICATIONS Gross intestinal hemorrhage 21% Relapse 12.5% Pneumonia 11.4% Intestinal perforation 1.9% Psychosis 1.9% UTI 1.9% Toxic myocarditis 1.7% Transient deafness 1.4% Toxic hepatitis 0.6% Meningitis 0.3% Endocarditis 0.3% Transient paralysis – LE 0.3%Hegazi AM. An update on: Typhoid Fever. http://www. imbabafevers.com/.../An%20update
%20on%20typhoid%20fever/Epidemiology%20of%20typhoid%20fever.ppt
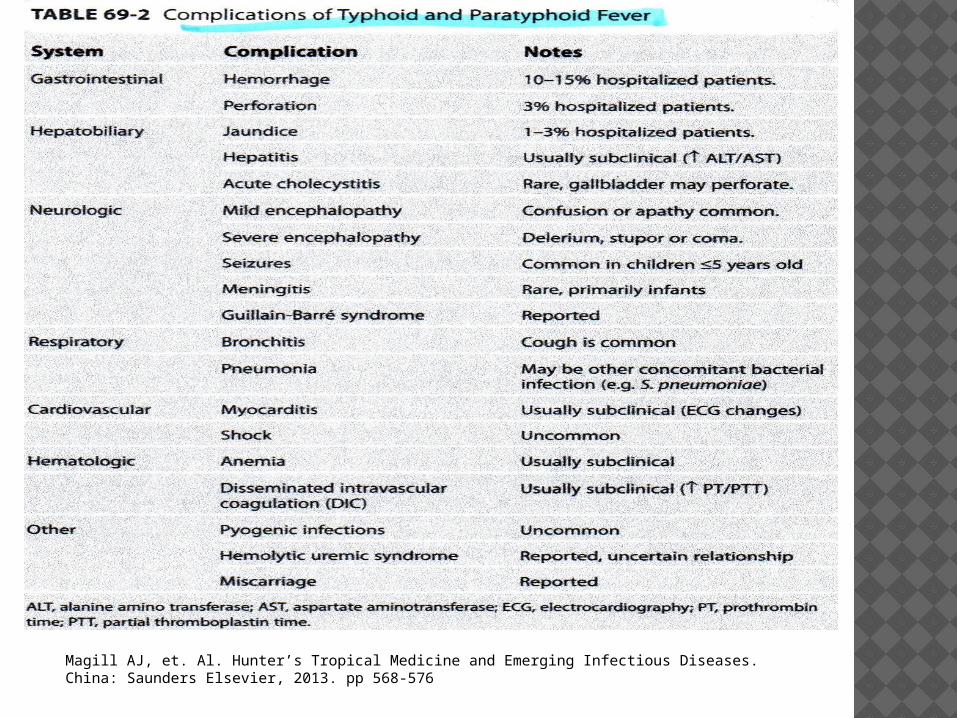
Magill AJ, et. Al. Hunter’s Tropical Medicine and Emerging Infectious Diseases. China: Saunders Elsevier, 2013. pp 568-576
COMPLICATIONS – MANY OTHERS Pancreatitis or abscess Empyema Renal complications Focal infections in many places Post salmonella enteritis reactive arthritis
3.4% Bed sores CNS and neuritis (even psychosis) Dehydration Muscle degeneration and DVT Hemolytic anemia Acute cholecystitis

INTESTINAL PERFORATION Rare in children but as high as 25% in
adults Classically in 3rd week (1-22 days) median 9 days Up to 3% in developing countries (1% in U.S.) Sx: worsening, sudden onset increased RLQ pain,
tachycardia, rebound fever, abdominal distention tenderness or rigidity, leukocytosis in 3rd week
80% single perforation May be masked by steroids Tx: Surgery and broaden antibiotic
coverage High mortality

ENCEPHALOPATHY AND PNEUMONIA Delirium, stupor and confusion Sometimes altered consciousness or coma Seizures most common in children with
increased mortality (usually < 35 cells in CSF)
Has been reported in up to 17% of patients. High mortality around 50%. Decreased
mortality to 10% if treated with dexamethasone in study out of Indonesia.
Pneumonia serious complication of severe typhoid more common in children

DIFFERENTIAL DIAGNOSIS Other salmonella species Malaria Influenza Shigella and other bacterial enteritis Dengue Typhus, Rickettsial infections Pulmonary or abdominal Tb Brucellosis Many others: Trypanosomiasis,
Leptospirosis, Amebic liver abscess, Acute HIV infections, Toxoplasmosis, Tularemia, leishmaniasis

PROGNOSIS 10-15% (as high as 30%) mortality prior to
CMP Now < 1%; 0.2% in U.S.; higher in developing
countries – 2% in hospitalized patients Higher in infants and elderly Higher if antibiotics delayed (3) Causes of death
Early shock, ARDS 27.4% Late perforation 14.1 Intestinal hemorrhage 25.9 Pneumonia 12.6 Other (myocarditis 4.4%) Hegazi AM. An update on: Typhoid Fever. http://www.
imbabafevers.com/.../An%20update%20on%20typhoid%20fever/Epidemiology%20of%20typhoid%20fever.ppt

TREATMENT - RESISTANCE Emergence of resistance to all first line drugs
(MDR) began late 1980s – Amp, TMX/SMX, CMP (plasmid mediated)
Subsequently nalidixic acid resistance (NARST) which is followed by FLQ (single point mutations)
NARST (NaR) considered marker for decreased fluoroquinolone susceptibility.
FLQ resistance common from India In 1996-1997 CDC reported 17% resistant to 5
drugs. (Now 13% MDR) Sporadic ceftriaxone resistance but not clinically
much of a problem anywhere yet (MIC creep)

TREATMENT - RESISTANCE U.S. 1999-2006 43% resistant to at least 1
antibiotic Resistance patterns change quickly –
Asia: increase NaR resistance from 5-50% (1993 – 2004) 2009 from Central India 98% NaR resistant Full quinolone resistance India, Korea Nepal from 0-13%
In Africa only about 5% resistant to FLQs. 3.7% Americas, 10.8% Middle East
(When not resistant to CMP – very good drug despite 1:20,000 aplastic anemia – quick response (3-5 days), inexpensive, widely available, broad spectrum)
With decreased usage, some reemergence sensitivity to older first line drugs – 2001-4 67% typhi and 80% paratyphi sensitive to CMP

TREATMENT - RESISTANCE Resistance has lead to favoring FLQs,
ceftriaxone, over 1st line drugs for initial treatment
NARST especially problem in Asia – 70-90% in some parts of India, Nepal and Vietnam.
Nalidixic acid resistant S. Typhi harbinger of fully quinolone – resistant S. Typhi.
NaR resistant typhoid have slower and less reliable response to quinolones.
Avoid FLQs as first line drugs in most of Asia and especially India

TREATMENT RESISTANCE Even if “sensitive” to FLQ, tx of NARST
with FLQ less effective especially for short course tx of 3-5 days. Defervesce slower (> 10 days vs. 3.5 days) and > rate of treatment failure
Better options Azithromycin, 3rd generation cephalosporins
Alternatives being investigated – include imipenen, newer or higher doses of old fluoroquinolones, combinations.
TREATMENT IF susceptible, Fluoroquinolones drug of
choice for fully susceptible organisms High levels in GI tract after oral treatment Bactericidal with good IC (intracellular)
penetration Oral and IV available; Not expensive Acts rapidly - Defervesce 3-4 days High cure rate; low failure rate with relapse rate
< 2% Concentrated in biliary tract – decreasing carrier
rate Cipro, ofloxacin, levofloxacin good – Not
Norfloxacin – poorly absorbed Several studies show safety in children

If resistant, Azithromycin also gets good intra-cellular levels (IC levels 50-100X > blood levels)
Azithromax as effective as FLQ and have lower failure rate and relapse rate than 3rd generation cephalosporins
3rd generation cephalosporins (i.e. Ceftriaxone or cefixime) compared to FLQs - longer to defervescence and higher relapse rate

ADULT TREATMENT EXCEPT FOR SOUTH (AND POSSIBLY SE) ASIA Ciprofloxacin 500 mg BID or Ofloxacin
400 mg BID po or IV X 7-10 days. Ceftriaxone 2-3 gm IV, IM daily or
Cefixime 20-30 mg/kg/day po divided BID X 7-14 days.
Alternatives if can’t take, resistant to FQsAzithromycin 1 gm orally then 500 daily for
5-7 days OR 1 gm po daily X 5 daysCMP 2-3 gm/day divided q6hr for 14 days
Hohmann EL. Treatment and prevention of typhoid fever. UpToDate 2010. UpToDate.com

TREATMENT IN CHILDREN (IN U.S.) A beta lactam
Ceftriaxone 100 mg/kg/day max 4 gm/day for 10-14 days (qD or BID)
Cefotaxime 150-200 mg/kg/day q6-8 hr max 12 g for 10-14 days
Cefixime 20 mg/kg/day q12 hours max 400 mg/day 10-14 days (po)
Fluoroquinolones Ciprofloxacin or Ofloxacin 30 mg/kg/day BID
max 1000 mg/day oral or IV for 7-10 days Ofloxacin 30 mg/kg daily max 800 mg/day po
or iv X 7-10 days
Hohmann EL. Treatment and prevention of typhoid fever. UpToDate 2010. UpToDate.com

TREATMENT (CHILDREN) CONT 10
Azithromycin 10-20 mg/kg to 1 g maximum once daily for 5-7 days
If fully susceptibleAmox 100 mg/kg/d q8hr max 4 g/day for 14
daysTMP-SMX 8-12 mg/kg TMP 40-60 mg/kg
SMX / day divided every 6 hours max 320 mg TMP/1600 mg SMX/day for 14 days.
CMP 75 mg/kg/d po q6hr max 3g/day: 14-21 days
Hohmann EL. Treatment and prevention of typhoid fever. UpToDate 2010. UpToDate.com

TREATMENT Outside U.S. Fluoroquinolones 1st
line in children and studies support they are ok if fluoroquinolones-sensitive.
Treat at least 5 days after fever resolution
If susceptible usually defervesce 3-5 days So much resistance from parts of S, SE
Asia fluoroquinolone should not be 1st choice– use Azithromax or 3rd generation cephalosporin
CMP, Amp, TMP-SMX ok if not resistant

CHILDREN CONTINUED FLQ – cartilage toxicity in immature
animals Large series show no evidence acute
adverse bone or joint events in humans. For serious infection if no other
options they are ok for children Optimal duration of cephalosporin
treatment not established – but need > 7 days
Ceftriaxone may be superior to cefotaxime so give ceftriaxone or cefixime 10-14 days

http://thedhakaproject.blogspot.com/2011/02/treatment-of-typhoid-fever.html

TREATMENT - OTHER Pay attention to nutrition, fluid and
electrolytes and monitor closely In complicated typhoid (critically ill -
shock, obtundation, delirium, stupor, coma) studies with CMP in past show 80% reduced mortality from 55% to 10% with corticosteroids.
Dexamethasone 3 mg/kg then 1 mg/kg q6hr for 48 hours.
Perforation (most - 80% single – ileum) – primary repair. Sometimes needs segmental resection and appropriate antibiotics. 14-34% mortality.

RELAPSE Common 2-3 wks after fever resolution
(1-10 weeks) after antibiotics stopped. Relapse usually milder than initial
infection. In past 10-25% but more recently 1-
6% - newer antibiotics seem to be more effective
Usually can treat with same drug vs. longer course with third generation cephalosporin. But culture to be sure sensitive.
CARRIER STATE Can shed normally up to 3 months in 10% Can be in stool or less commonly urine Chronic carrier = Excretion in stool (or
urine) > 12 months (Typhoid > Paratyphoid)
Incidence after Typhoid about 4 % (1-6%)
Increased with cholelithiasis Urine carriage more common with kidney
stones, urinary schistosomiasis or BPH Well but risk to others – esp. food preparers

TREATMENT OF CARRIER STATE In past Ampicillin for 6-12 weeks +
cholecystectomy. Now can treat try FLQ for 4 wks for
near 90% cure rate. If FLQ treatment fails, cholecystectomy
(for food handlers, day care workers, health care workers)Ciprofloxacin 500-750 mg BID for 4 weeksOfloxacin 400 mg BID for 4 weeks

CARRIERS Missouri: after typhoid 3 stool cultures
needed for (child care, food handlers, medical personnel) 24 hrs apart to see if carrier - If so repeat every month till 3 consecutive negative cultures.
For chronic carrier (> 1 year) must have 6 consecutive negative cultures collected 1 month apart to go back to work.
Missouri Depart. Of Health and senior Services Communicable Disease Investigation and Reference Manual. Typhoid fever. 7/03.

http://www.docstoc.com/docs/11383809/Spots-Typhoid-Fever © Docstoc® 2013. All rights reserved.

PREVENTION/VACCINATION CDC: “Boil it, cook it, peel it, or forget it” 2 vaccines – 50% effective at 3 years (85%
initially) Parenteral Vi polysaccharide vaccine (efficacy 55%) (>
2 yoa. Repeat 2 yrs); Oral S. Typhi vaccine strain Ty21a (efficacy 51%) (> 6
yoa. Repeat 5 years) About 1/6 of cases in travelers came after < 2 weeks
travel so recommended even for short travel. Neither 100% effective – no good against paratyphoid In U.S. 1994-99, ¾ of U.S. cases from travel; but only
4% vaccinated Though only approved for > 6, studies show 57%
protection with oral vaccine in ages 2-5 Others on horizon

http://talesfromindonesia.wordpress.com/2012/06/22/of-typhoid-pills-and-crazy-prices-or-the-things-we-do-for-immunity/

SUMMARY Typhoid is a serious illness caused by S. Typhi Typhoid can present many ways and mimic
many other diseases. Diagnosis requires a high index of suspicion
The most common test for Typhoid, the Widal test, is not reliable, is positive after one has a vaccine, and should not be relied on
There is considerable drug resistance in typhoid. FLQs are the DOC except in S, SE Asia. Due to FLQ resistance, better choices there are Azithromax or a 3rd generation cephalosporin

SOURCES/CREDITS 1Brusch JL, Garvey T. Typhoid Fever. Emedicine
medscape.com 2010. http://emedicine.medscape.com/article/231135-print.
Brusch JL. “Typhoid Fever.” Medscape Reference. Accessed 1/22/2014 at http://emedicine.medscape.com/article/231135-overview
Burkholder-Allen K, Rega P. “’Typhoid’” Mary Mallon. Accessed 1/22/2014 at http://www.docstoc.com/docs/161918129/%E2%80%9CTyphoid%E2%80%9D-Mary-Mallon---errata-llc www.errata-llc.com/blog/files/Typhoid_Mary.ppt
Christenson JC. “Salmonella Infections.” Pediatrics in Review accessed online in 11/2014. @ http://pedsinreview.aappublications.org/content/34/9/375

SOURCES/CREDITS Division of Environmental Health and Communicable
Disease Prevention. Missouri Department of Health and Senior services Communicable Disease Investigation Reference Manual . http://www.dhss.mo.gov/CDManual/Typhoidfever.pdf
Ekdahl K, de Song, B, Andersson Y. Travel Associated Typhoid and Paratyphoid Fever. Medscape.com 2005. http://www.medscape.com/viewarticle/511056_print
Harrison’s Practice. Typhoid Fever. http://www.harrisonspractice.com/practice/ub/view/Harrisons%20Practice/141051/0/enteric_fever
Hegazi AM. An update on: Typhoid Fever. http://www.imbabafevers.com/.../An%20update%20on%20typhoid%20fever/Epidemiology%20of%20typhoid%20fever.ppt

7Hohmann EL. Epidemiology, microbiology, clinical manifestations, and diagnosis of typhoid fever. UpToDate 2010. UpToDate reaccessed 1/22/2014 @ http://www.uptodate.com/contents/epidemiology-microbiology-clinical-manifestations-and-diagnosis-of-typhoid-fever?source=search_result&search=typhoid&selectedTitle=1%7E77
Hohmann EL. Microbiology and epidemiology of Salmonellosis. UpToDate 2010. UpToDate reaccessed 1/22/2014 @ www.worldortho.com/dev/index.php?option=com_content&task=view&id=1778&Itemid=420
Hohmann EL. Pathogenesis of typhoid fever. UpToDate 2010. UpToDate reaccessed 1/22/2014 at http://www.uptodate.com/contents/pathogenesis-of-typhoid-fever?source=search_result&search=typhoid&selectedTitle=3%7E77
Hohmann EL. Treatment and prevention of typhoid fever. UpToDate 2010. UpToDate reaccessed 1/22/2014 @ http://www.uptodate.com/contents/treatment-and-prevention-of-typhoid-fever?source=search_result&search=typhoid&selectedTitle=2%7E77

SOURCES CONTINUED Kadhiravan, T. Drug-resistant Typhoid Fever – Implications
for Clinical practice. Medicine Update 2007; pp. 584-586. http://www.apiindia.org/medicine_update_2007/98.pdf
Kalra SP, Naithani N, Mehta SR, Swamy AJ. Current trends in the Management of Typhoid Fever. MJAFI 2003; 59:130-135.
Kumar R. Typhoid Fever. Power Point referencing World Health Organization 2003. N Engl. J Med, Vol 347,No.22. 11/28/2002.
Magill AJ, et. Al. Hunter’s Tropical Medicine and Emerging Infectious Diseases. China: Saunders Elsevier, 2013. pp 568-576
Mirza, SH. Multi-drug resistant Typhoid – A Global Review. Infections Disease Journal of Pakistan. Jan – March 2005: pp; 17-20. http://www.idspak.org/journal/2005/Jan-March/page17-20.pdf

Missouri Depart. Of Health and senior Services Communicable Disease Investigation and Reference Manual. Typhoid fever. 7/03.
Zahran RF. Typhoid Fever. http://www.slideworld.org/slideshow.aspx/Typhoid-Fever-ppt-2844722
Rosenberg J. “Typhoid Mary: The sad story of a woman responsible for several typhoid outbreaks. About.com accessed on 1/22/2014 at http://history1900s.about.com/od/1900s/a/typhoidmary.htm
Strickland, GT (ed). Hunter’s Tropical Medicine and Emerging Infectious Diseases, Eight Edition. Philadelphia: W. B. Saunders Company, 2000. p 477


















