
September 2008 Partnership for Health and Accountability The PHA: Where to Next? Vi Naylor Executive...
35
September 2008 Partnership for Health and Accountability The PHA: Where to Next? Vi Naylor Executive Vice President Georgia Hospital Association
-
Upload
marian-morton -
Category
Documents
-
view
213 -
download
0
Transcript of September 2008 Partnership for Health and Accountability The PHA: Where to Next? Vi Naylor Executive...

September 2008 Partnership for Health and Accountability
The PHA:Where to Next?
Vi NaylorExecutive Vice President
Georgia Hospital Association

September 2008 Partnership for Health and Accountability
The PHA Roadmap to Success

September 2008 Partnership for Health and Accountability
Once upon a time….
Georgia Hospital Association established the Partnership for Health and Accountability
Purpose: To promote: Accountability, Best practices, Patient safety and To improve quality of care statewide
Vision:"Stakeholders collaboratively use data to proactively improve quality, patient safety and health, and effectively communicate results across the publics served."

September 2008 Partnership for Health and Accountability
Critical Success Factors
• Long standing good relationships among partners
• Built on existing programs• Involved all from the beginning• Full authority for committees• Utilized provider-driven, non-
punitive public/private effort that fostered learning
• Addressed public and provider needs
• Public recognition

September 2008 Partnership for Health and Accountability
Addressed Public and Provider Needs
Public
Health Education and Public Reports User friendly and readable• State of the Health of Georgia•Hospital Specific Reports: Quality Insights
Provider
Accountability for Patient Safety:
Sharing of Sensitive confidential data
Shared learning opportunities:•Toolkits•Technical Assistance

September 2008 Partnership for Health and Accountability
Positive Recognition

September 2008 Partnership for Health and Accountability
The End Result?
• Award program with recognition from the Governor
• Public Website for consumer information
• Significant reduction in medication errors
• Improved in adherence to evidence-based guidelines
• Sentinel Event Reporting with related Safety Alerts
• Shared Learning

September 2008 Partnership for Health and Accountability
Whew!

September 2008 Partnership for Health and Accountability
Is the Party Over?
The program is now institutionalized – Give us a break!

September 2008 Partnership for Health and Accountability
Now What?
• GHA board agreed to fund on-going PHA initiatives
• We switched focus to the Community Side while maintaining Quality and Safety Initiatives
• Strategically sought grants
September 2008 Partnership for Health and Accountability
Community Outreach
• Grant funding to develop a community based program in chronic care management
• Grant to develop a tobacco-free hospital campus toolkit
• Created Center for Rural Health• Library initiative: “connected the dots” between
the public and their local hospitals• Diabetes and VTE Special Interest Groups

September 2008 Partnership for Health and Accountability
Quality and Patient Safety
• Continued Event Reporting and Safety Alerts and Safe Medication Audio Conferences
• Expanded the Quality and Patient Safety Award program• Created the Hospital Mentor Program• Responded to environmental forces:
– Transparency website– Teams for Infection Prevention Success (TIPS)
• Best Practices PowerHour Plus telnets held monthly• Added resources/toolkits
September 2008 Partnership for Health and Accountability
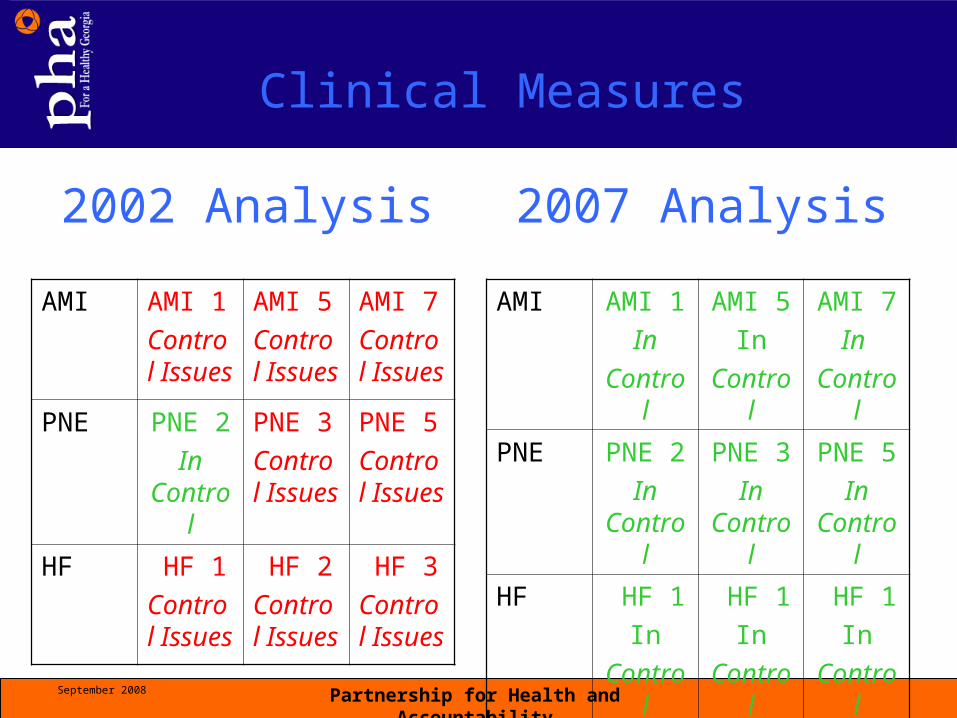
Clinical Measures
AMI AMI 1
Control Issues
AMI 5
Control Issues
AMI 7
Control Issues
PNE PNE 2
In Control
PNE 3
Control Issues
PNE 5
Control Issues
HF HF 1
Control Issues
HF 2
Control Issues
HF 3
Control Issues
2002 Analysis 2007 Analysis
AMI AMI 1
In
Control
AMI 5
In
Control
AMI 7
In
Control
PNE PNE 2
In Control
PNE 3
In Control
PNE 5
In Control
HF HF 1
In
Control
HF 1
In
Control
HF 1
In
Control

September 2008 Partnership for Health and Accountability
Georgia Progress Lags National Progress
0%10%20%30%40%50%60%70%
80%90%
100%
PN 4 PN 2 HF 4 HF 1 AMI 4 AMI 2
Q3 2003 RateQ1 2008 Rate Q1 2008 Nation

September 2008 Partnership for Health and Accountability
Our Wake-up Call
• US Averages *• National = 84.5%• Top State = 92.9%• Top 10th State =
88.1%
Georgia Status• Average = 81.4% *• Georgia Rank = 46
Georgia Now = 87.1%
Right care every time for targeted core measures: AMI, CHF, PN

September 2008 Partnership for Health and Accountability
Moving Georgia to the Top Ten
What Can Hospitals Do to
Improve?Participate! Participate! Participate!

September 2008 Partnership for Health and Accountability
Increased Participation = Better ResultsParticipation vs. Performance
-2
0
2
4
6
8
10
12
14
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50% 55% 60% 65% 70% 75% 80% 85% 90% 95% 100%
Performance in ACM and Index
Par
ticip
atio
n (#
Mea
sure
Set
s x
#Qtr
s)
CompositeScore Index Score
Correlation: 0.59Correlation: 0.69

September 2008 Partnership for Health and Accountability
Original Guiding Principles Revisited
• Accountability to the public• Physician is responsible for medical treatment decisions*• Physician performance should be reviewed by physician peers*• Proactive and voluntary• Public and private stakeholders• Continuous improvement rather than a punitive, “name, blame, shame”*• Provides for trust• Resources and buy-in to support a long term commitment – with QI staff• Repository for confidential peer review protected information*• User-friendly feedback reports, but not for CEOs, MDs and Trustees
• Promotes best practices• Educational
*Crucial!

September 2008 Partnership for Health and Accountability
Return to Prior Success
• Build on existing programs
• Involve all from the beginning
• Full authority to committees
• Foster collaboration and shared learning/education
• Public recognition

September 2008 Partnership for Health and Accountability
Moving to the Next Level Top Ten Program
• Step up Trustee Education• Communicate Board’s action• Increase physician and CEO engagement• Invitational Conference: From Worst to First• Create infrastructure to implement Conference
recommendations• Make Quality a standing Board agenda item.• Increase public recognition
September 2008 Partnership for Health and Accountability
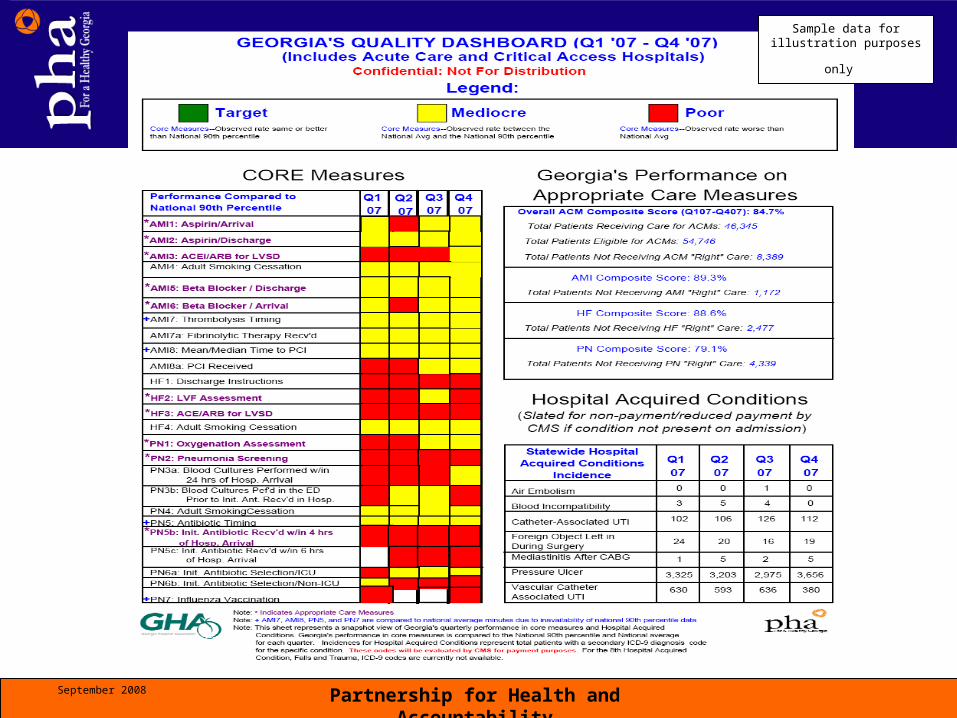
Sample data for illustration
purposes only

September 2008 Partnership for Health and Accountability
Change in Reporting
September 2008 Partnership for Health and Accountability
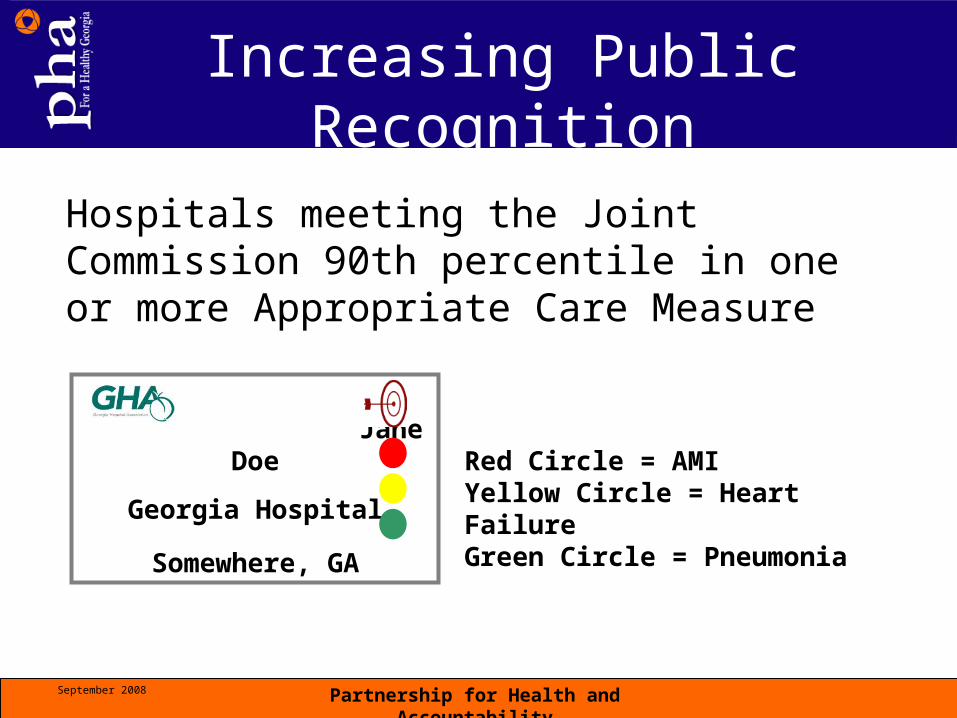
Hospitals meeting the Joint Commission 90th percentile in one or more Appropriate Care Measure
Increasing Public Recognition
JANE JANE Jane Doe
Georgia Hospital
Somewhere, GA
Red Circle = AMIYellow Circle = Heart FailureGreen Circle = Pneumonia

September 2008 Partnership for Health and Accountability
Quality Honor Roll

September 2008 Partnership for Health and Accountability
Engaging Physicians and CEOs
From Worse to First ConferenceRecurring Theme:
Incentivize acceptance and promote implementation of evidence-based practice among the hospital board, CEO, medical and hospital staffs
September 2008 Partnership for Health and Accountability
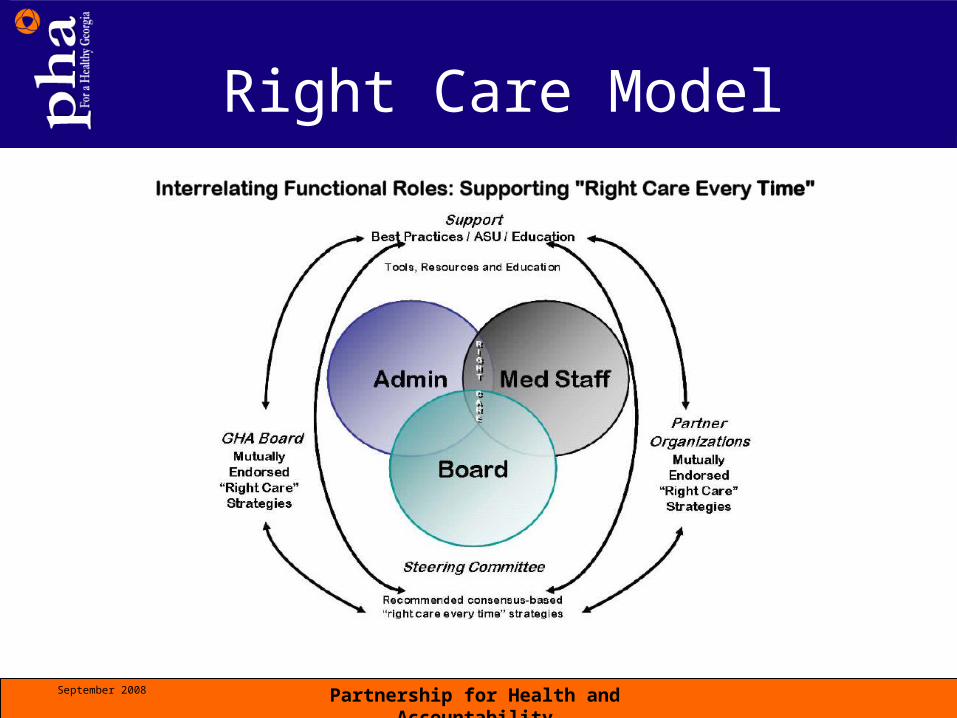
Right Care Model

September 2008 Partnership for Health and Accountability
Top Ten Organizational Structure

September 2008 Partnership for Health and Accountability
Purpose
Work together in partnership with physicians, hospitals, trustees, and CEOs/Executive Leadership/Front line staff to determine and promote mutually endorsed reliable, systematic processes of care that support “right care every time.”

September 2008 Partnership for Health and Accountability
Physician-Directed “Right Care Every Time”
Use of evidence-based practice to support “right care, every time”
• Systematic reliable process of care such as Medical staff-approved order sets and nurse initiated protocols
• Strategies to recognize and promote physicians’ investment of time in developing processes for outstanding performance.
• Identify obstacles to providing “right care every time”

September 2008 Partnership for Health and Accountability
Physician-Directed “Right Care Every Time”
• Strengthen physicians’ role as the captain of the ship as related to accountability for “right care every time”
• Identify system supports such as “redundancy” and “forcing”
• Provide physician specific real-time data
• Promote the use of performance data in re-credentialing; set targets

September 2008 Partnership for Health and Accountability
Physician-Directed “Right Care Every Time”
Integrate activities and recommendations in partnership with hospital trustee and executive leadership activities
• Promote local Top Ten infrastructure
• Strategies for active engagement of local “voluntary” physicians
• Provide regular CME to address Top 10 strategies through “Physician Power Hour”
September 2008 Partnership for Health and Accountability
Trustees: Institutional Policies/Statements
Assure visibility of the board’s ultimate responsibility for evidence-based practice
• Include adherence to evidence-based practice in contracts
Reinforce physician accountability for evidence-based practice
• Institutional adoption of evidence-based practices
• Performance data for re-credentialing• Recognition program related to evidence-
based practice

September 2008 Partnership for Health and Accountability
Executive Leadership
• Facilitate evidence-based practices
• Multi-disciplinary discussions to determine obstacles and identify supportive system functions to facilitate “right care every time”
• Employ forcing and redundancy strategies

September 2008 Partnership for Health and Accountability
Executive Leadership
• Enhance ability for physician to participate in recommending reliable systematic processes of care
• Concurrent monitoring for real time assessment and completion of missing elements of “right care every time”.
• Physicians real-time feedback data

September 2008 Partnership for Health and Accountability
The Future
QUARTER GA GA NATIONAL TOP STATE RANK RATE RATE RATE_____
Q4 2010 1 95.5 90.2 95.5
Our Vision - 2010


















