
SEPSIS BIO-MARKERS AFTER CARDIAC SURGERY · SEPSIS BIO-MARKERS AFTER CARDIAC SURGERY Dr/ Sameh R...
46
SEPSIS BIO SEPSIS BIO- -MARKERS MARKERS SEPSIS BIO SEPSIS BIO- -MARKERS MARKERS AFTER CARDIAC AFTER CARDIAC SURGERY SURGERY Dr/ Dr/ Sameh Sameh R Ismail R Ismail Dr/ Dr/ Sameh Sameh R Ismail R Ismail Consultant Consultant Pediatric Cardiac Intensive Care Pediatric Cardiac Intensive Care King Abdulaziz Medical City for National Guard
Transcript of SEPSIS BIO-MARKERS AFTER CARDIAC SURGERY · SEPSIS BIO-MARKERS AFTER CARDIAC SURGERY Dr/ Sameh R...
SEPSIS BIOSEPSIS BIO--MARKERS MARKERS SEPSIS BIOSEPSIS BIO--MARKERS MARKERS AFTER CARDIAC AFTER CARDIAC
SURGERYSURGERYDr/ Dr/ SamehSameh R IsmailR IsmailDr/ Dr/ SamehSameh R IsmailR Ismail
Consultant Consultant Pediatric Cardiac Intensive CarePediatric Cardiac Intensive CareKing Abdulaziz Medical City for National Guard
IntroductionIntroductionIntroductionIntroduction•• ““SEPSIS AT ITS INCEPTION SEPSIS AT ITS INCEPTION
Is Is DIFFICULT TO RECOGNIZE DIFFICULT TO RECOGNIZE BUT BUT EASY TO TREATEASY TO TREAT; AND IF ; AND IF BUT BUT EASY TO TREATEASY TO TREAT; AND IF ; AND IF LEFT UNATTENDED It LEFT UNATTENDED It BECOMESBECOMES EASY TO EASY TO RECOGNIZE BUT DIFFICULT RECOGNIZE BUT DIFFICULT RECOGNIZE BUT DIFFICULT RECOGNIZE BUT DIFFICULT TO TREATTO TREAT” ”
MachiavelliMachiavelli
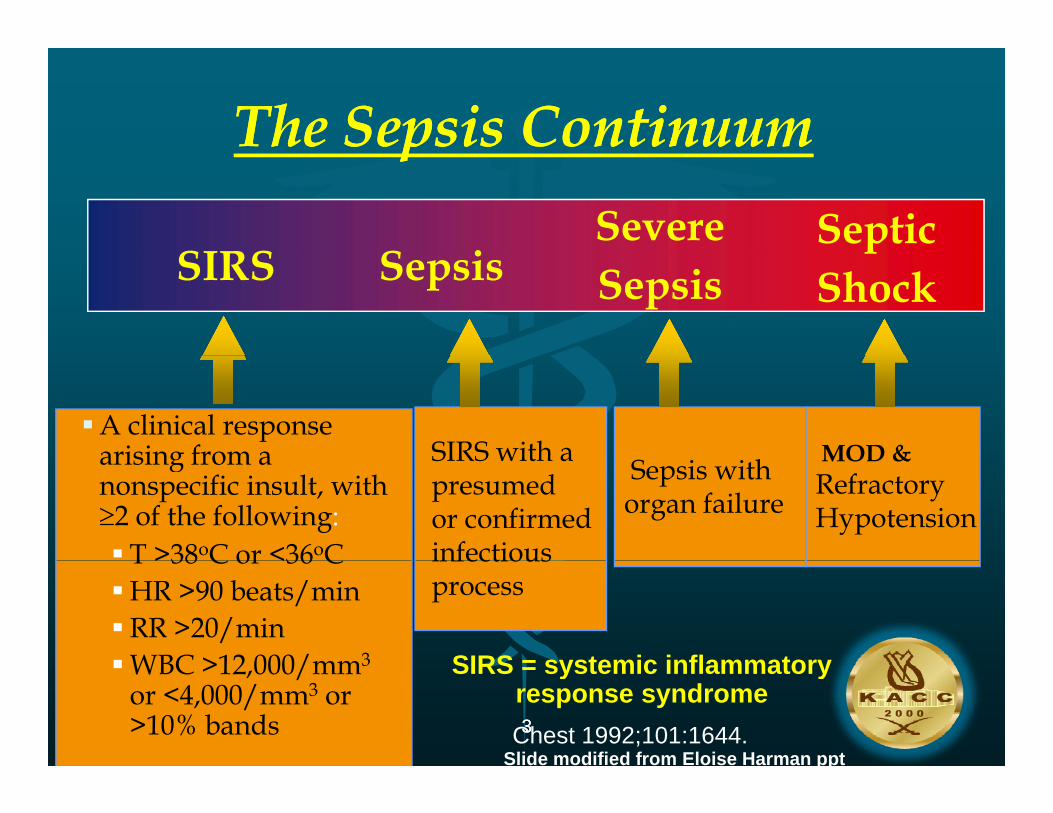
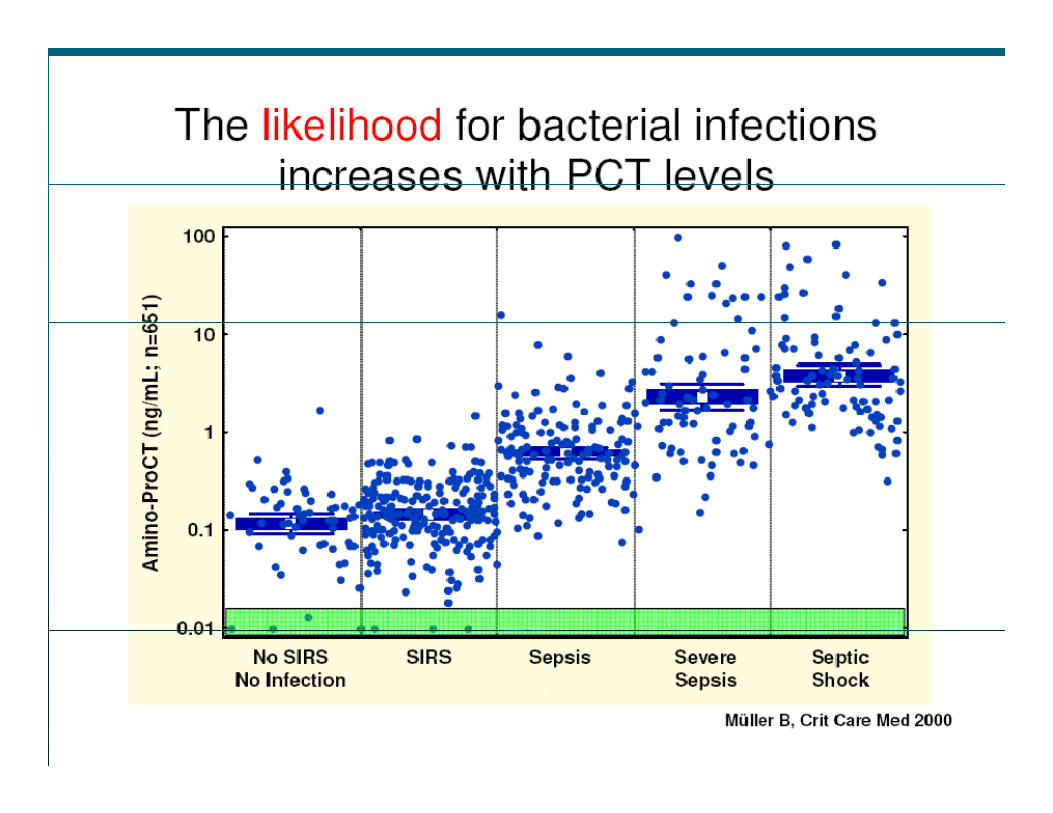
The Sepsis ContinuumThe Sepsis Continuumpp
S iSIRSSevere Septic
SepsisSIRS Sepsisp
Shock
A clinical response arising from a SIRS with a MOD & arising from a nonspecific insult, with 2 of the following: T >38oC or <36oC
SIRS with apresumedor confirmed infectious
Sepsis with organ failure
MOD & RefractoryHypotension
T >38 C or <36 CHR >90 beats/minRR >20/minWBC >12 000/mm3 SIRS = systemic inflammatory
infectiousprocess
33
WBC >12,000/mm3
or <4,000/mm3 or >10% bands
SIRS = systemic inflammatory response syndromeChest 1992;101:1644.
Slide modified from Eloise Harman ppt
IntroductionIntroductionIntroductionIntroduction
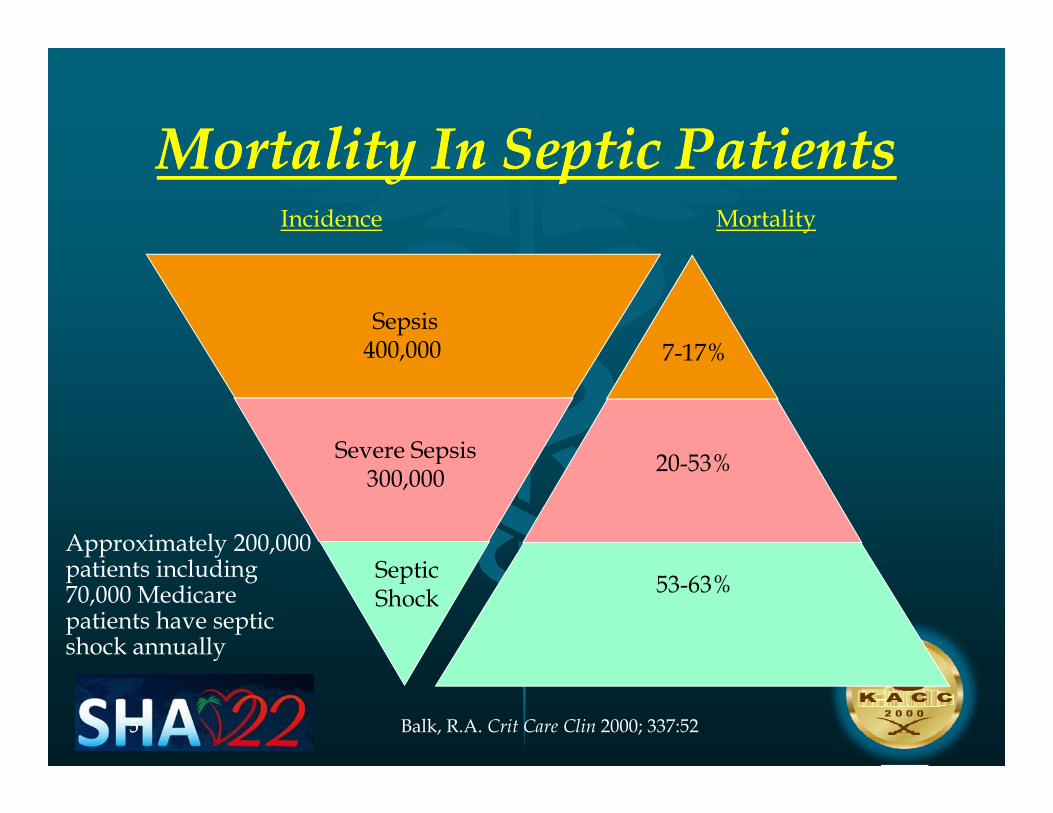
Mortality In Septic PatientsMortality In Septic PatientsMortality In Septic PatientsMortality In Septic PatientsMortalityIncidence
7-17%Sepsis
400,000
20 53%Severe Sepsis
7-17%400,000
20-53%Seve e Seps s300,000
Approximately 200,000 i i l di Septic
Shock 53-63%patients including 70,000 Medicare patients have septic shock annually
55 Balk, R.A. Crit Care Clin 2000; 337:52
Ch lCh lChalengesChalenges
CHALLENGES :
Sepsis Major cause of morbidity and mortality
Clinical presentation is often similar as with viral or i f t noninfectous causes
Anti – Biotic Treatment of viral infections /noninfectious causes is not only ineffective ,but
-Costs Ri k f t i it -Risk of toxicity
-Resistance
77
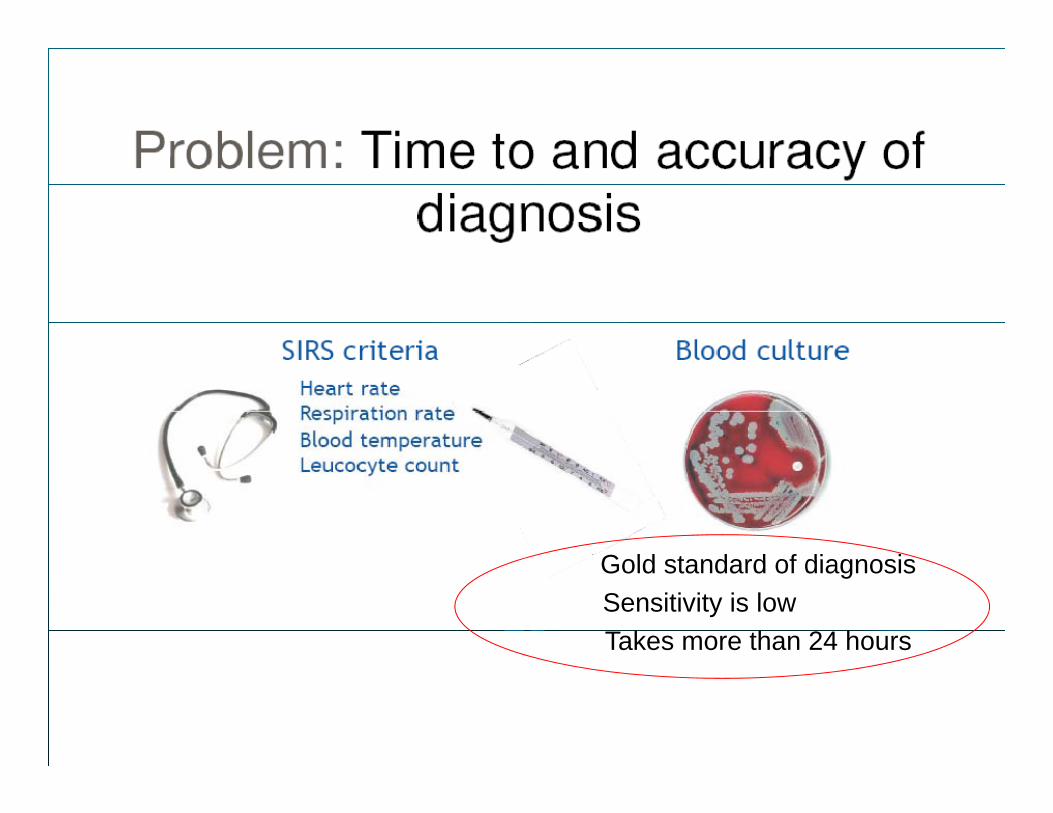
Gold standard of diagnosisGold standard of diagnosisSensitivity is low Takes more than 24 hours
88
Gold standard of diagnosisSensitivity is low
Takes more than 24 hours
Treating Sepsis Treating Sepsis Current practiceCurrent practice
•• Clinical diagnosis supported by Clinical diagnosis supported by nonnon specificspecific &tests &tests •• Clinical diagnosis supported by Clinical diagnosis supported by nonnon--specificspecific &tests &tests egeg: WBC, CRP, radiology : WBC, CRP, radiology
•• GuessGuess what is the likely infecting organismwhat is the likely infecting organism•• GuessGuess what antibiotic to usewhat antibiotic to use•• WaitWait to see if it works….?to see if it works….?•• If it doesn't have If it doesn't have another guessanother guessIf it doesn t ….have If it doesn t ….have another guessanother guess•• add/upgrade/change add/upgrade/change abxabx•• If it still doesn’t work ask micro/ID/If it still doesn’t work ask micro/ID/pharmapharma
llll•• to to guessguess as wellas well•• The treating physician The treating physician somtimessomtimes cannot decide cannot decide
which direction to gowhich direction to go
1010
1111
NEED :something that help………………g p
E l t di i ????•Early correct diagnosis ????•Infection vs non=inf????•Bacterial vs non-bact??????? •Bacterial vs non-bact??????? •Use of antibiotics only when needed??? •De-escalate??? •Use short course of therapy ??•Risk stratification??
1212
What is the SOLUTION?
1313
The ideal biomarkerThe ideal biomarker1.1. Does not increase in the absence of the disease Does not increase in the absence of the disease
(high (high specificityspecificity))2.2. increases pathologically in the presence of disease increases pathologically in the presence of disease p g y pp g y p
(high (high sensitivity)sensitivity)3.3. Relates to the Relates to the disease burden and extentdisease burden and extent44 Changes in accordance with the clinical evolutionChanges in accordance with the clinical evolution4.4. Changes in accordance with the clinical evolution,Changes in accordance with the clinical evolution,5.5. reflecting the current status of diseasereflecting the current status of disease6.6. anticipatesanticipates clinical changes before it happensclinical changes before it happenspp g ppg pp7.7. shows no major fluctuation in serum levelsshows no major fluctuation in serum levels8.8. Adds independent information about the Adds independent information about the risk or prognosisrisk or prognosis99 R d iblR d ibl9.9. ReproducibleReproducible10.10. Easy and cheapEasy and cheap
1414
1515
C Reactive Protein (CRP)C Reactive Protein (CRP)
1616
CRPCRPCRPCRP•• acute phase protein; synthesised in liveracute phase protein; synthesised in liver•• ILIL--6 6 (and IL(and IL--1 1 and TNFa) stimulate synthesis and TNFa) stimulate synthesis
via action on promotervia action on promoter
•• binds bacterial polysaccharide, chromatinbinds bacterial polysaccharide, chromatin
•• activates the classical complement pathwayactivates the classical complement pathway
•• increased in the immune inflammatory increased in the immune inflammatory response; especially in bacterial (vs viral) response; especially in bacterial (vs viral) infectioninfection
1717
Diseases associated with only minor Diseases associated with only minor l ti f Cl ti f C ti t iti t ielevations of Celevations of C--reactive proteinreactive protein
S t i l th tS t i l th t•• Systemic lupus erythematosusSystemic lupus erythematosus•• Systemic sclerosisSystemic sclerosis•• DermatomyositisDermatomyositis•• Sjögren’s diseaseSjögren’s diseaseSjögren s diseaseSjögren s disease•• Ulcerative colitisUlcerative colitis
L k iL k i•• LeukaemiaLeukaemia•• GraftGraft--versusversus--host diseasehost disease
1818
PROPRO CALCITONIN PCTCALCITONIN PCTPROPRO--CALCITONIN PCTCALCITONIN PCT
1919
2020
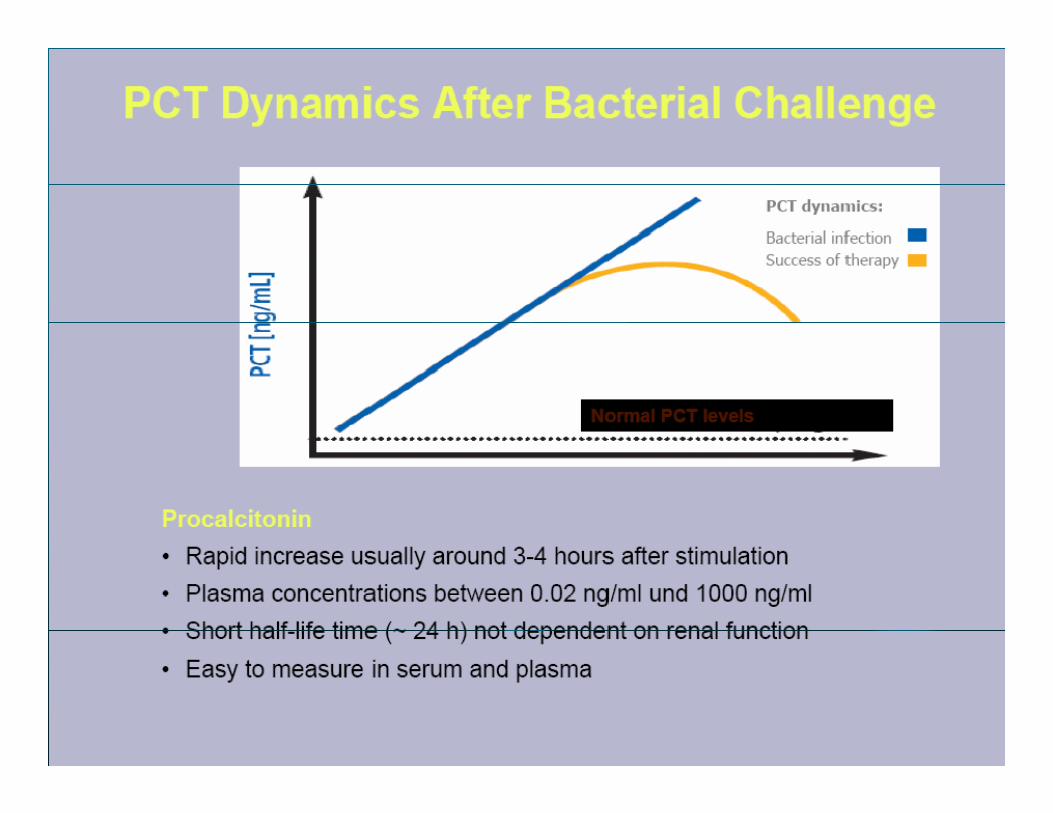
ProPro--calcitonincalcitonin PCT is the PCT is the 116116--amino acid amino acid prohormoneprohormone of calcitoninof calcitonin
In healthy individuals, PCT is produced by C cells of thyroid glandIn healthy individuals, PCT is produced by C cells of thyroid glandy , p y y gy , p y y g
IncresedIncresed markedly in septic statesmarkedly in septic states
•• stimulation by sepsisstimulation by sepsis--related cytokines and has bactericidal effect.related cytokines and has bactericidal effect. Approved by FDA as a diagnostic tool Approved by FDA as a diagnostic tool
Easy to measure in serum and plasma by immunoassay Easy to measure in serum and plasma by immunoassay
Its Its level not only correlates level not only correlates with the with the severityseverity of infection but also of infection but also acts as acts as Its Its level not only correlates level not only correlates with the with the severityseverity of infection but also of infection but also acts as acts as a prognostic marker a prognostic marker
2121
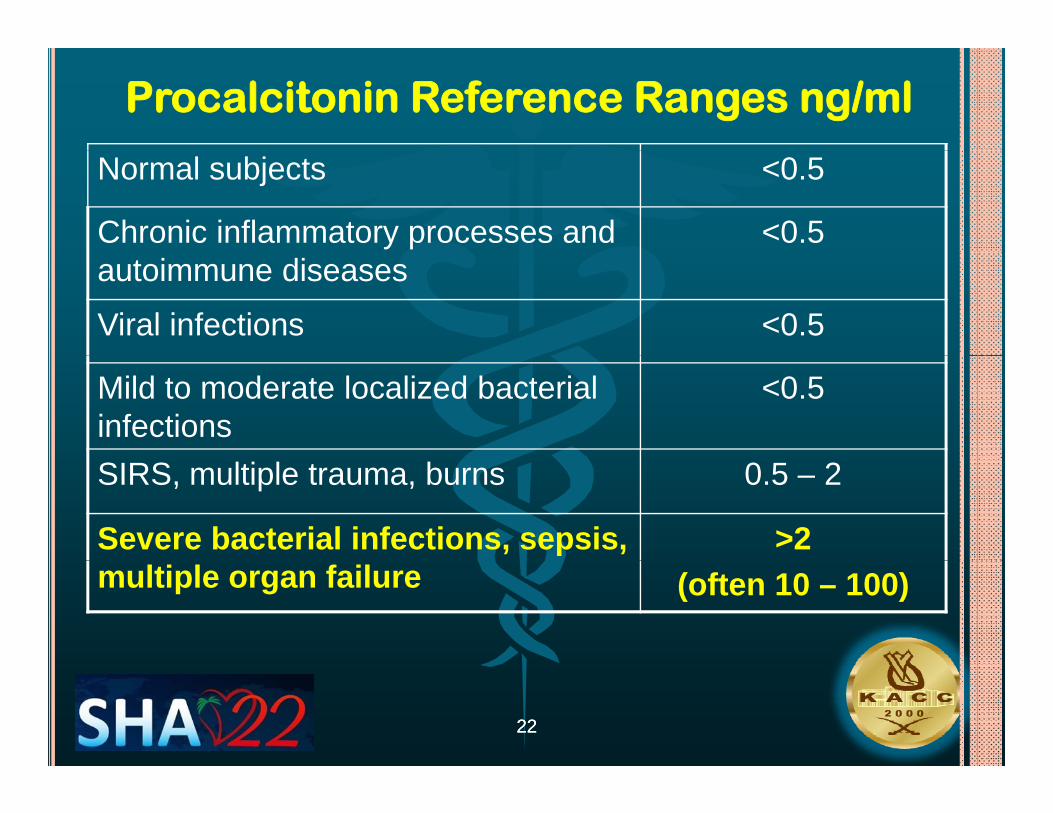
Procalcitonin Reference Ranges ng/ml
Normal subjects <0.5
Chronic inflammatory processes and <0.5autoimmune diseases
Viral infections <0.5
Mild to moderate localized bacterial infections
<0.5
SIRS, multiple trauma, burns 0.5 – 2
Severe bacterial infections, sepsis, >2 multiple organ failure (often 10 – 100)
2222
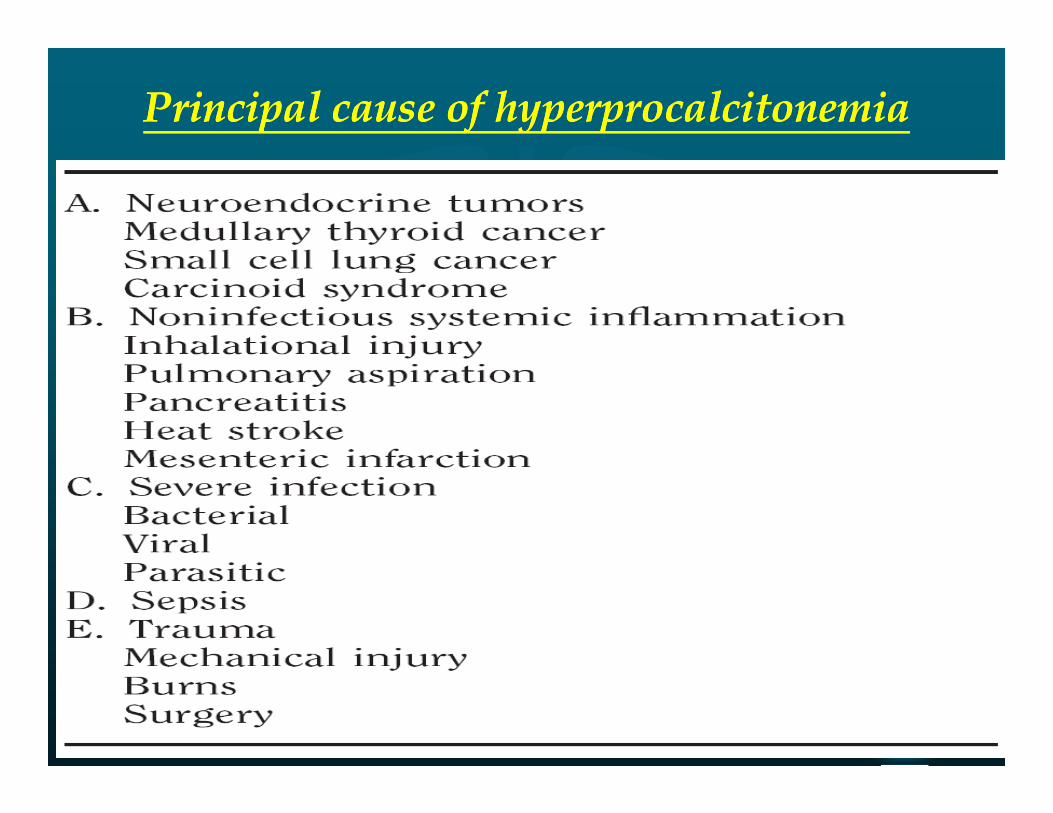
Principal cause of Principal cause of hyperprocalcitonemiahyperprocalcitonemia
2323
Nonbacterial infection: Viruses, Fungi, Nonbacterial infection: Viruses, Fungi, ParasitesParasites
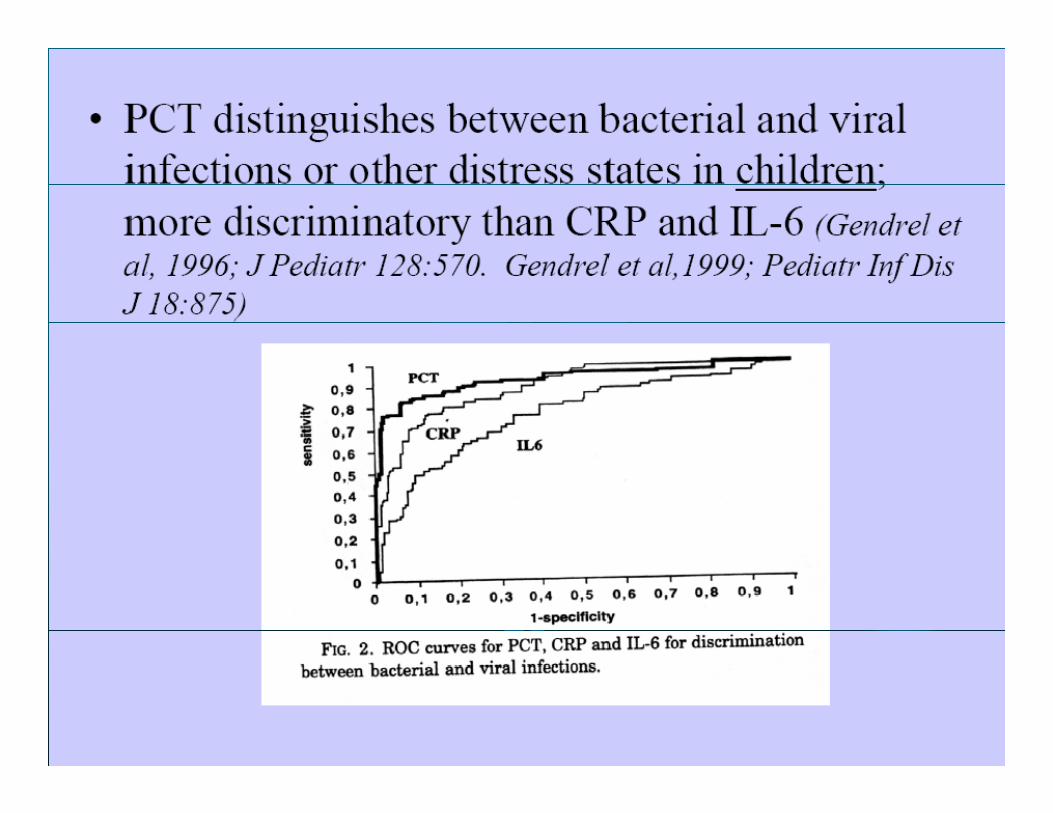
•• PCTPCT tend to be low in viral infectiontend to be low in viral infection•• However, in systemic viral infection, PCT value can be as high as 16 However, in systemic viral infection, PCT value can be as high as 16
ngng/ml/mlgg
•• A low serum PCT cannot be used to exclude bacterial from A low serum PCT cannot be used to exclude bacterial from viral infections but that a combination of PCT, CRP, white viral infections but that a combination of PCT, CRP, white bl d ll d li i l ill i i h b bl d ll d li i l ill i i h b blood cell count, and clinical illness scoring might be more blood cell count, and clinical illness scoring might be more usefuluseful
•• In patients with In patients with fungal infectionsfungal infections, results have been , results have been variablevariable
•• Infection with the Infection with the malariamalaria parasite often leads to very parasite often leads to very high high levels of serum, as high as 662 levels of serum, as high as 662 ngng/mL/mL
2424
2525
2626
2727
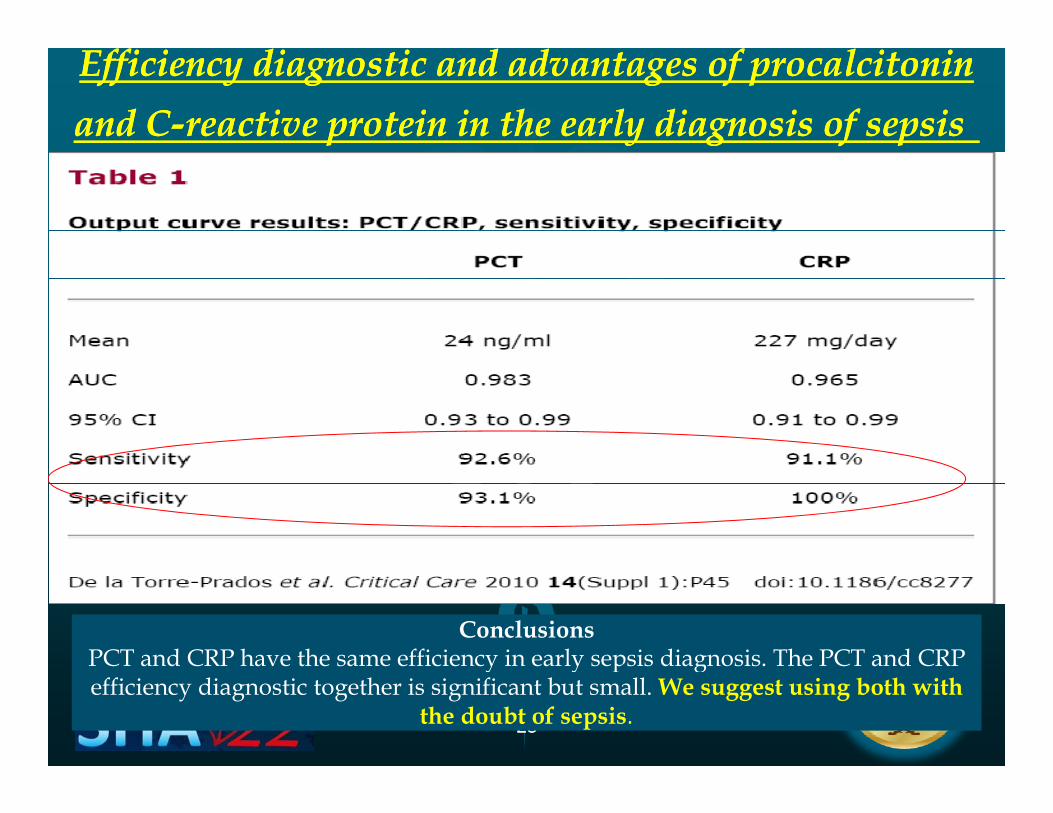
Efficiency diagnostic and advantages of Efficiency diagnostic and advantages of procalcitoninprocalcitoninand Cand C--reactive protein in the early diagnosis of sepsisreactive protein in the early diagnosis of sepsis
ConclusionsPCT and CRP have the same efficiency in early sepsis diagnosis The PCT and CRP
2828
PCT and CRP have the same efficiency in early sepsis diagnosis. The PCT and CRP efficiency diagnostic together is significant but small. We suggest using both with
the doubt of sepsis.
2929
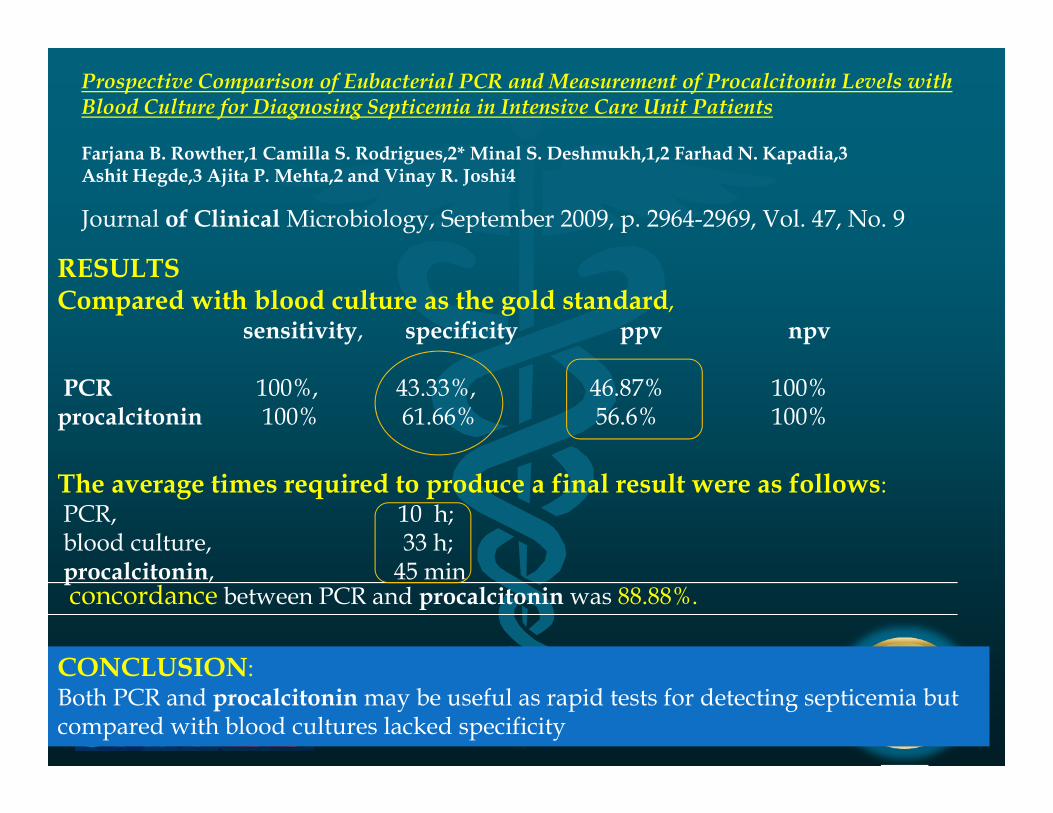
Prospective Comparison of Eubacterial PCR and Measurement of Procalcitonin Levels with Blood Culture for Diagnosing Septicemia in Intensive Care Unit Patients
F j B R th 1 C ill S R d i 2* Mi l S D h kh 1 2 F h d N K di 3
Journal of Clinical Microbiology, September 2009, p. 2964-2969, Vol. 47, No. 9
Farjana B. Rowther,1 Camilla S. Rodrigues,2* Minal S. Deshmukh,1,2 Farhad N. Kapadia,3Ashit Hegde,3 Ajita P. Mehta,2 and Vinay R. Joshi4
RESULTSCompared with blood culture as the gold standard,
sensitivity, specificity ppv npv
PCR 100%, 43.33%, 46.87% 100%procalcitonin 100% 61.66% 56.6% 100%
The average times required to produce a final result were as follows:PCR, 10 h;blood culture, 33 h;procalcitonin, 45 minconcordance between PCR and procalcitonin was 88.88%.
CONCLUSION
3030
CONCLUSION:Both PCR and procalcitonin may be useful as rapid tests for detecting septicemia but compared with blood cultures lacked specificity
PCT GUIDES ANTIBIOTICS USEPCT GUIDES ANTIBIOTICS USE
3333
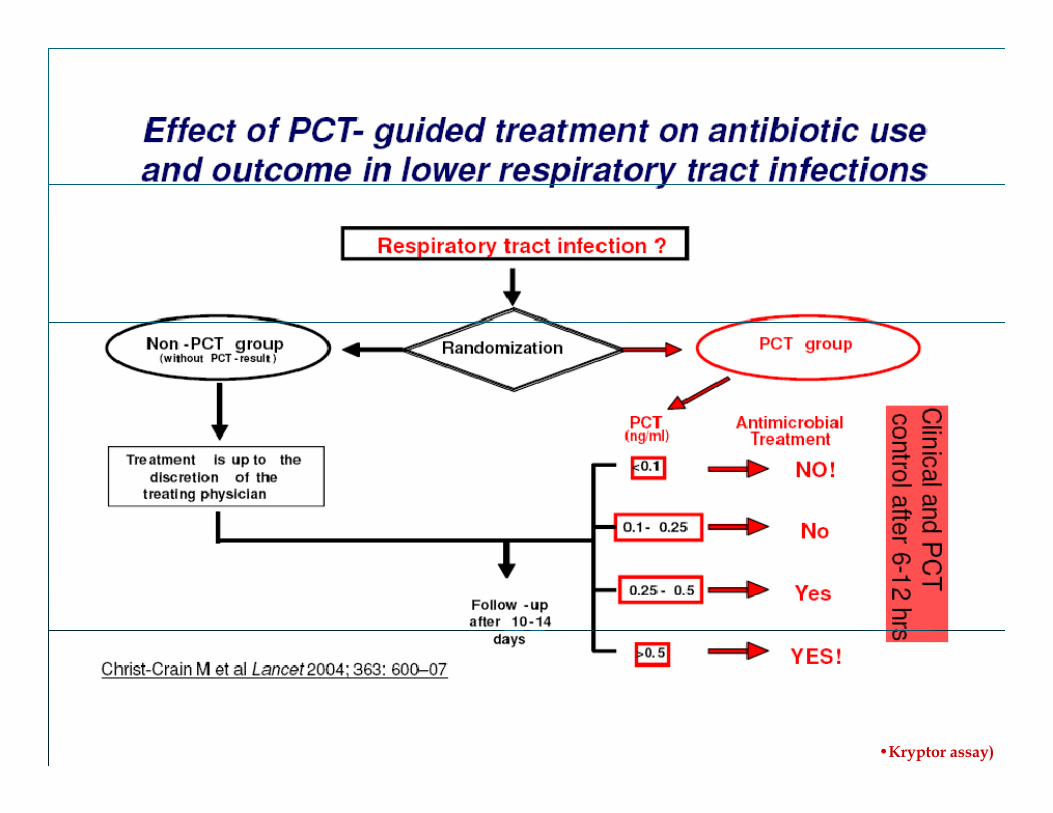
3434Pro Resp: Patients with LRTI in the ED (Lancet 2004, N=243)
•Kryptor assay)119 randomised to standard care 124 to PCT-guided treatment
(52%)
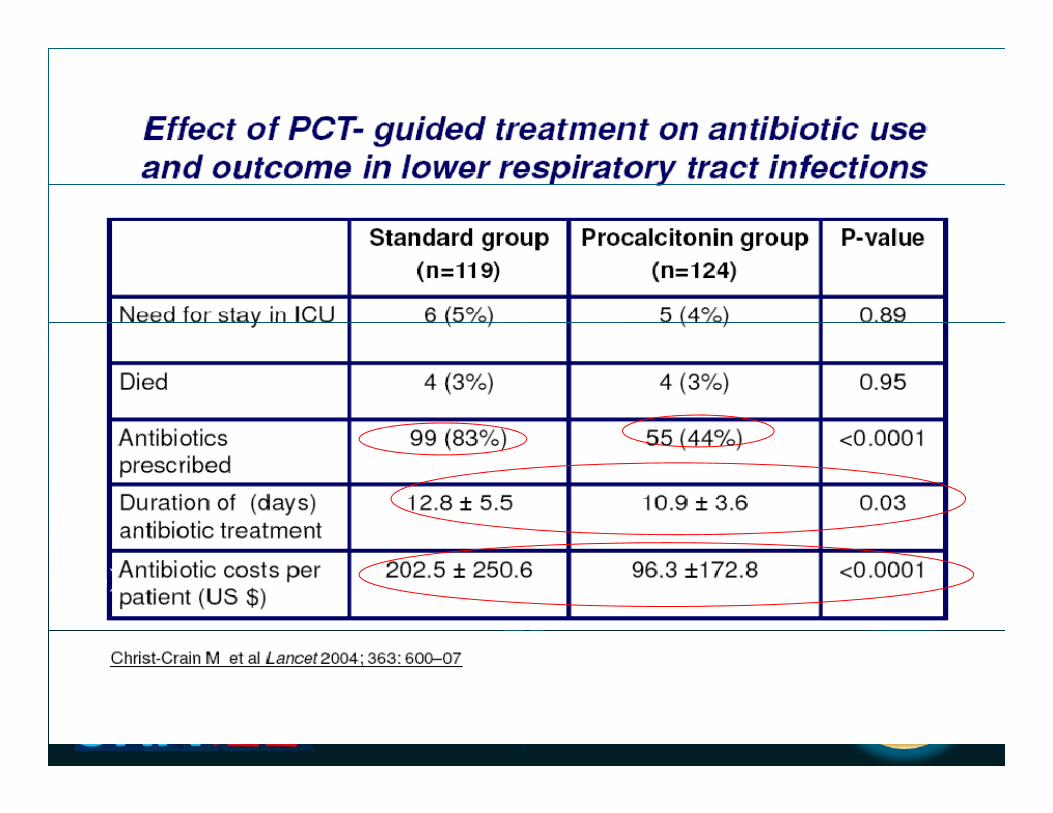
3535ProResp: Patients with LRTI in the ED (Lancet 2004, N=243)
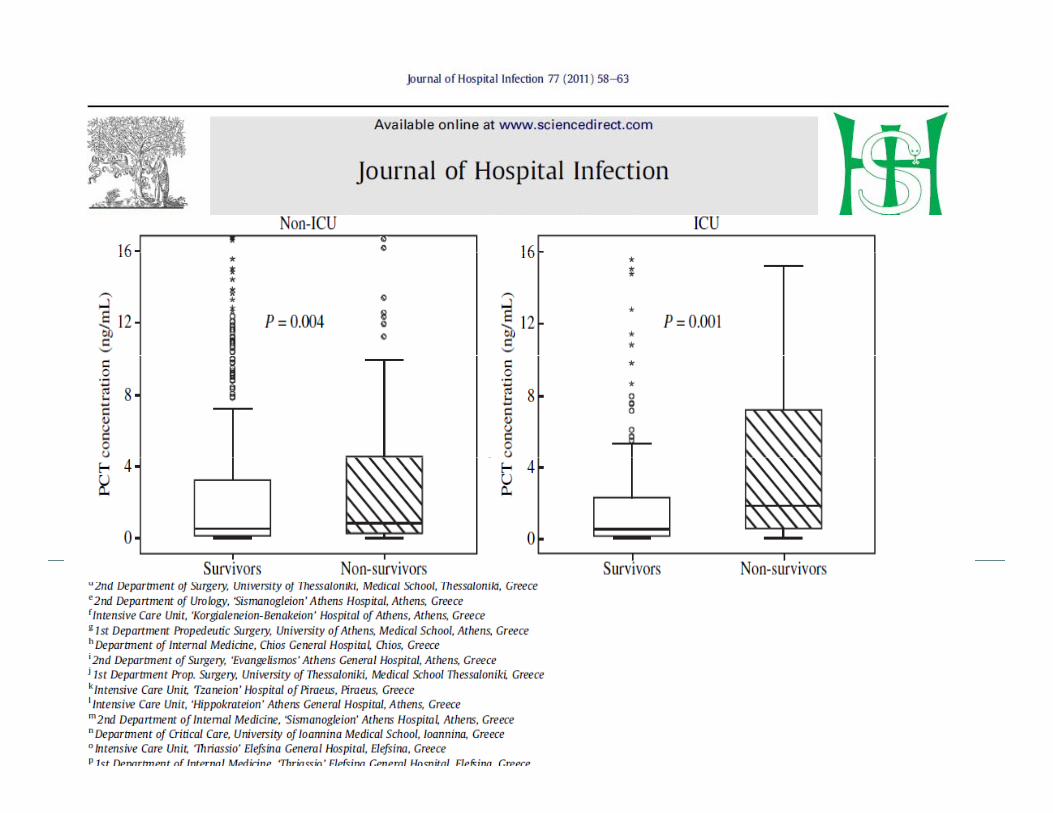
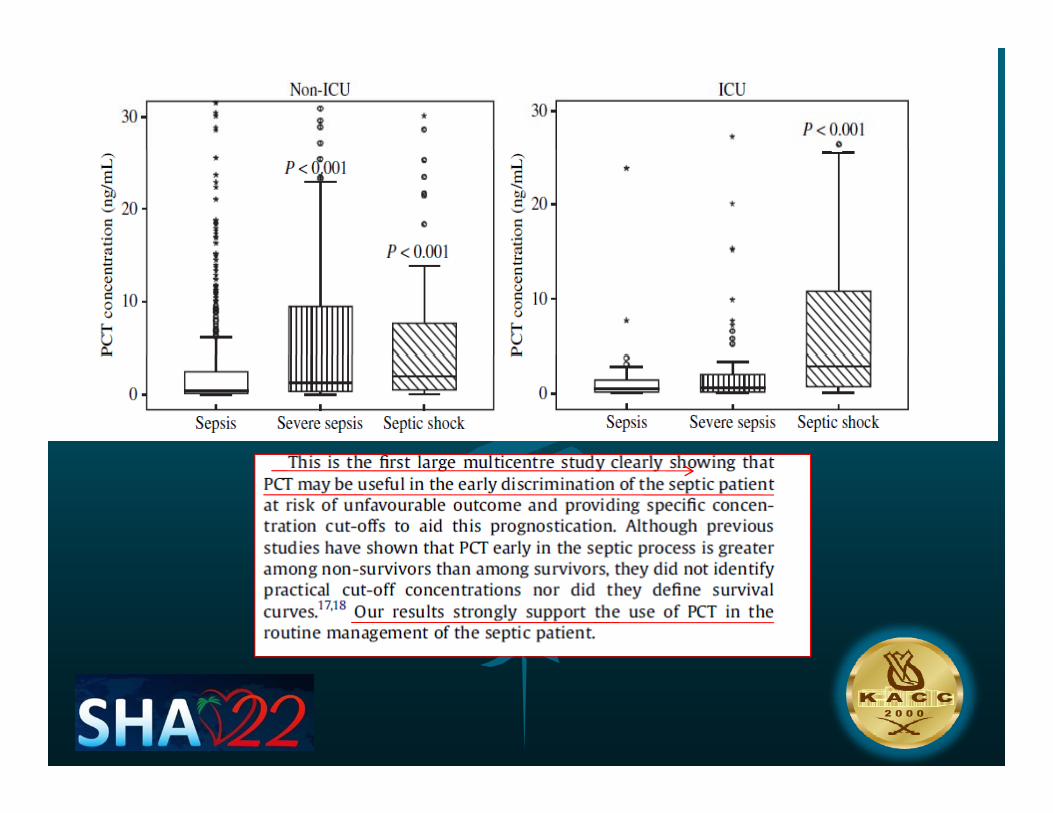
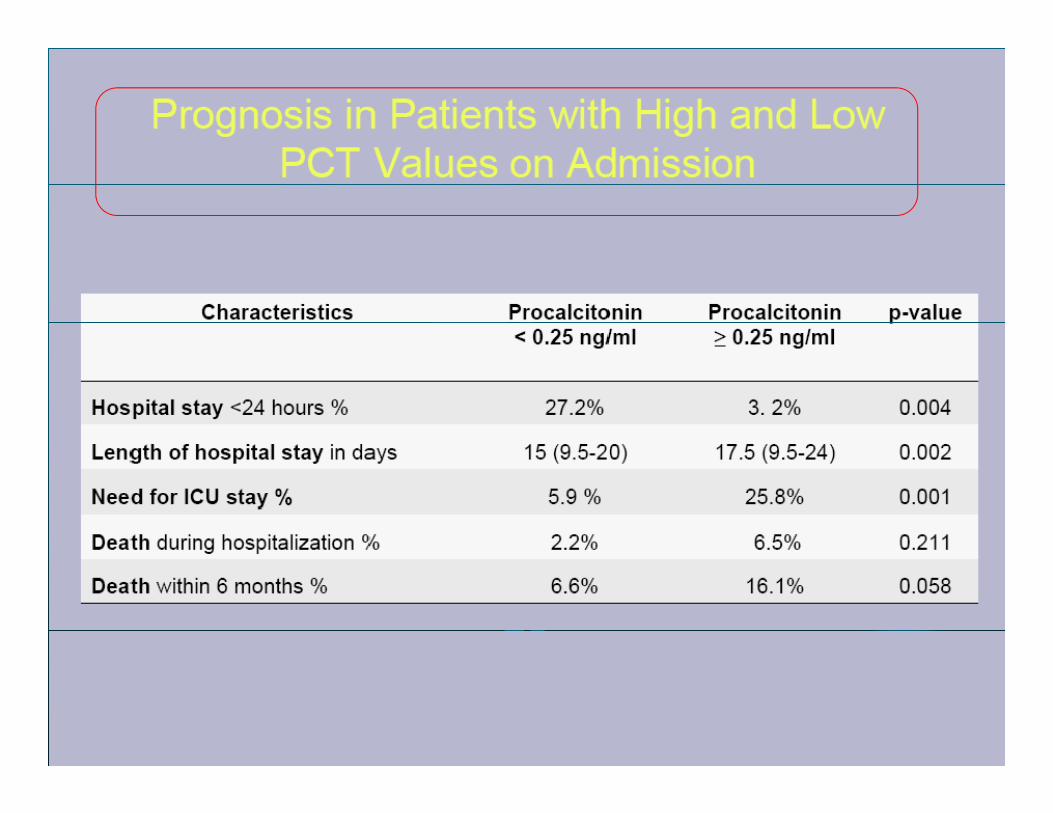
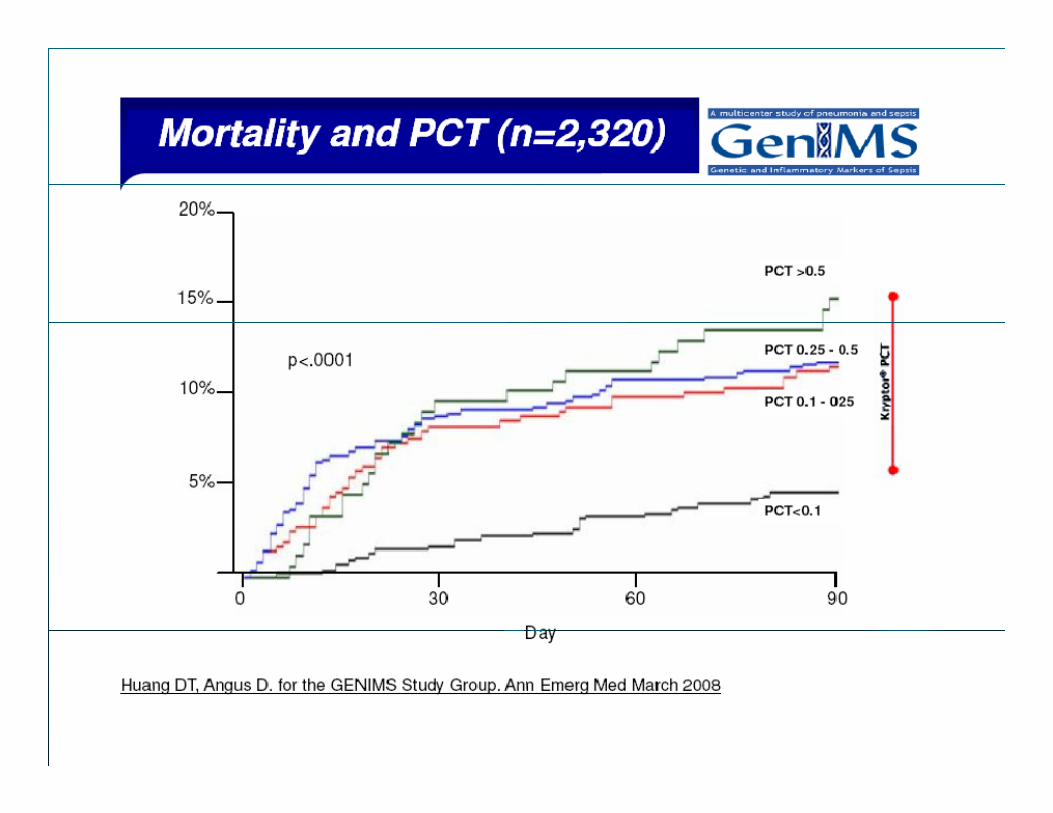
PCT PREDECT OUTCOMEPCT PREDECT OUTCOMEPCT PREDECT OUTCOMEPCT PREDECT OUTCOME
3636
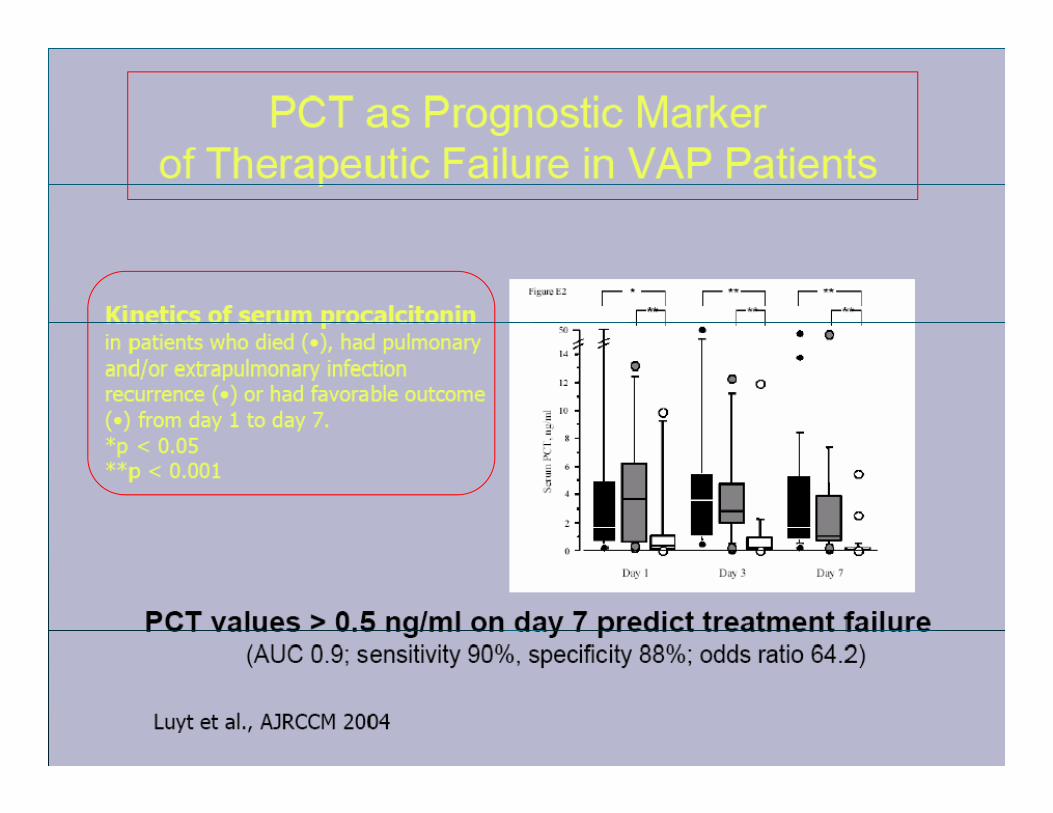
3737
3838
3939
PCT and severity of illness scoringPCT and severity of illness scoring
Moderate to fairly strong statistical correlationModerate to fairly strong statistical correlation•• Acute Physiology and Chronic Health Evaluation Acute Physiology and Chronic Health Evaluation •• Acute Physiology and Chronic Health Evaluation Acute Physiology and Chronic Health Evaluation
(APACHE III) scores(APACHE III) scores•• Simplified Acute Physiology Score (SAPS II)Simplified Acute Physiology Score (SAPS II)y gyy gy•• Pediatric Risk of Mortality scoresPediatric Risk of Mortality scores•• APACHE II and the Multiple Organ Dysfunction APACHE II and the Multiple Organ Dysfunction
S (MODS)S (MODS)Score (MODS)Score (MODS)•• Sequential Organ Failure Assessment (SOFA) Sequential Organ Failure Assessment (SOFA)
scoresscoresscoresscores•• Baltimore Sepsis Scale (BSS)Baltimore Sepsis Scale (BSS)
4040
The future ??The future ??The future ??The future ??
P t iP t i•• ProteomicsProteomics•• Detect specific bacterial protein signaturesDetect specific bacterial protein signatures•• Detect biological response markersDetect biological response markers
•• Protein microarraysProtein microarraysyy
ConclusionConclusionConclusionConclusion
AA i li l dd li ili i•• AA moremore rationalrational andand explicitexplicitincorporationincorporation ofof biomarkersbiomarkers intointofuturefuture researchresearch designsdesigns maymay wellwellaidaid inin addressingaddressing thisthis challengechallenge..gg gg

ThanksThanksThanksThanks

4646


















