
SECTION TWO GENERALIZED IDIOPATHIC …akbraincenter.com/wp-content/uploads/2015/12/Book...Werz,...
4
Werz, 978-1-4160-4833-6 SECTION TWO GENERALIZED IDIOPATHIC SEIZURES Jeffrey L. Sponsler Juvenile absence epilepsy is a type of idiopathic generalized epi- lepsy recognized by the International League Against Epilepsy. 1 Onset is from age 8 to age 16 years, with a peak occurrence at 10 to 12 years of age. The frequency of absence seizures in juve- nile absence epilepsy is lower than that in childhood absence epi- lepsy. A higher frequency of generalized tonic-clonic seizures is seen, compared with childhood absence epilepsy, and there is an increased probability of epilepsy continuing into the adult years. 2 The precise incidence and prevalence of juvenile absence epilepsy are not known. Wolf and Inoue report that, typi- cally, patients with juvenile absence epilepsy are physically and neurodevelopmentally normal. They also notes that 11% of patients with the disorder report a family history of epilepsy. 3 CLINICAL PRESENTATION Absence seizures are predominant. The impairment of con- sciousness in juvenile absence epilepsy is moderate and not gen- erally as severe as in childhood absence epilepsy. The level of retained consciousness may vary significantly from seizure to seizure in the same patients. Absence attacks have been termed spanioleptic, meaning “scarce.” Unlike childhood absence epi- lepsy they may occur once a day or in a cluster in the hour after awakening. The duration of absence seizures is probably simi- lar to that in childhood absence epilepsy at 4 to 20 seconds. The classic clinical feature is “simple absence” with staring and altered alertness (sometimes “complex absence” with blinking or head nodding). 2 A large majority of patients will have expe- rienced at least one generalized tonic-clonic seizure, and this may lead to the diagnosis. Myoclonic seizures associated with juvenile absence epilepsy occur in a minority of cases. 4 Seizures are typically triggered by hyperventilation or sleep deprivation. A photoparoxysmal response is described in a minority of chil- dren. However, some experts view the presence of a photopar- oxysmal response as excluding a diagnosis of juvenile absence epilepsy. Tovia and associates 5 studied 17 patients with juvenile absence epilepsy retrospectively and found that the outcome of patients with the disorder is less favorable than in children with childhood absence epilepsy and that the presence of generalized tonic-clonic seizures is a predictor for poorer outcome, that is, fewer such patients were seizure free when treated. EEG FINDINGS Interictal background activity is usual normal in juvenile absence epilepsy. 6 Posterior bilateral delta activity has been described as an interictal phenomenon in children with absence epilepsy more commonly in childhood absence epilepsy and less com- monly in juvenile absence epilepsy. 6 Absence seizures demon- strate generalized “surface negative spikes” seen predominately in the frontocentral head regions, followed by a surface negative slow wave discharge with frequency often faster than 3 Hz (3.5– 4.0 Hz). 6 Overall, the ictal discharges are similar to those in child- hood absence epilepsy, although polyspikes on the slow wave are common. MRI FINDINGS Betting and colleagues 7 report, in a study of 124 patients with idiopathic generalized epilepsy, that 24% of patients had non- specific MRI abnormalities. Woermann and coworkers 8 note that microdysgenesis in gray and white matter has been found in cases of idiopathic generalized epilepsy; their group performed MRI studies of patients with idiopathic generalized epilepsy and found that 4 of 10 patients with juvenile absence epilepsy demonstrated significant abnormalities of the regional distribution of cerebral gray and subcortical matter. GENETICS Heron and colleagues 9 report that in a study of 100 patients with a generalized epilepsy syndrome, including juvenile absence epilepsy, variants in the T-type calcium channel gene CACNA1H, which alters channel properties, are present. In a study of 55 families with idiopathic generalized epilepsy, no mutation of sodium, calcium, or γ-aminobenzoic acid (GABA) channels was found. In this study, phenotypic concordance Juvenile Absence Epilepsy CHAPTER FOUR B978-1-4160-4833-6.00004-6, 00004 c0020 P P S P P S P S P S P
Transcript of SECTION TWO GENERALIZED IDIOPATHIC …akbraincenter.com/wp-content/uploads/2015/12/Book...Werz,...

Werz, 978-1-4160-4833-6
B978-1-4160-4833-6.00004-6, 00004
SECTION TWO GENERALIZED IDIOPATHIC SEIZURES
Jeffrey L. Sponsler
Juvenile absence epilepsy is a type of idiopathic generalized epi-lepsy recognized by the International League Against Epilepsy. 1 Onset is from age 8 to age 16 years, with a peak occurrence at 10 to 12 years of age. The frequency of absence seizures in juve-nile absence epilepsy is lower than that in childhood absence epi-lepsy. A higher frequency of generalized tonic-clonic seizures is seen, compared with childhood absence epilepsy, and there is an increased probability of epilepsy continuing into the adult years. 2
The precise incidence and prevalence of juvenile absence epilepsy are not known. Wolf and Inoue report that, typi-cally, patients with juvenile absence epilepsy are physically and neurodevelopmentally normal. They also notes that 11% of patients with the disorder report a family history of epilepsy. 3
CLINICAL PRESENTATION
Absence seizures are predominant. The impairment of con-sciousness in juvenile absence epilepsy is moderate and not gen-erally as severe as in childhood absence epilepsy. The level of retained consciousness may vary significantly from seizure to seizure in the same patients. Absence attacks have been termed spanioleptic, meaning “scarce.” Unlike childhood absence epi-lepsy they may occur once a day or in a cluster in the hour after awakening. The duration of absence seizures is probably simi-lar to that in childhood absence epilepsy at 4 to 20 seconds. The classic clinical feature is “simple absence” with staring and altered alertness (sometimes “complex absence” with blinking or head nodding). 2 A large majority of patients will have expe-rienced at least one generalized tonic-clonic seizure, and this may lead to the diagnosis. Myoclonic seizures associated with juvenile absence epilepsy occur in a minority of cases. 4 Seizures are typically triggered by hyperventilation or sleep deprivation. A photoparoxysmal response is described in a minority of chil-dren. However, some experts view the presence of a photopar-oxysmal response as excluding a diagnosis of juvenile absence epilepsy.
Tovia and associates 5 studied 17 patients with juvenile absence epilepsy retrospectively and found that the outcome of patients
with the disorder is less favorable than in children with childhood absence epilepsy and that the presence of generalized tonic-clonic seizures is a predictor for poorer outcome, that is, fewer such patients were seizure free when treated.
EEG FINDINGS
Interictal background activity is usual normal in juvenile absence epilepsy. 6 Posterior bilateral delta activity has been described as an interictal phenomenon in children with absence epilepsy more commonly in childhood absence epilepsy and less com-monly in juvenile absence epilepsy. 6 Absence seizures demon-strate generalized “surface negative spikes” seen predominately in the frontocentral head regions, followed by a surface negative slow wave discharge with frequency often faster than 3 Hz (3.5–4.0 Hz). 6 Overall, the ictal discharges are similar to those in child-hood absence epilepsy, although polyspikes on the slow wave are common.
MRI FINDINGS
Betting and colleagues 7 report, in a study of 124 patients with idiopathic generalized epilepsy, that 24% of patients had non-specific MRI abnormalities. Woermann and coworkers 8 note that microdysgenesis in gray and white matter has been found in cases of idiopathic generalized epilepsy; their group performed MRI studies of patients with idiopathic generalized epilepsy and found that 4 of 10 patients with juvenile absence epilepsy demonstrated significant abnormalities of the regional distribution of cerebral gray and subcortical matter.
GENETICS
Heron and colleagues 9 report that in a study of 100 patients with a generalized epilepsy syndrome, including juvenile absence epilepsy, variants in the T-type calcium channel gene CACNA1H, which alters channel properties, are present. In a study of 55 families with idiopathic generalized epilepsy, no mutation of sodium, calcium, or γ -aminobenzoic acid (GABA) channels was found. In this study, phenotypic concordance
Juvenile Absence Epilepsy
CHAPTER FOUR
B978-1-4160-4833-6.00004-6, 00004
c0020
p0040
p0045
s0010
p0050
p0055
s0015
p0060
s0020
p0065
s0025
p0070

B978-1-4160-4833-6.00004-6, 00004
Werz, 978-1-4160-4833-6
16
Juve
nile
Abs
ence
Epi
leps
y within families of juvenile absence epilepsy probands was 10%. 10 In a genetic survey of families with the four most com-mon subtypes of idiopathic generalized epilepsy (e.g., childhood absence epilepsy, juvenile absence epilepsy, juvenile myoclonic epilepsy, and epilepsy with grand mal seizures on awakening), three different heterozygous mutations in the chloride-channel gene CLCN2 in three unrelated families were found. 11 Durner and coworkers 12 report strong evidence for a genetic locus com-mon to most idiopathic generalized epilepsies on chromosome 18. Sander and associates 13 report that allelic variants of the kainate-selective GluR5 receptor gene ( GRIK1 ) on chromosome
21q22.1 are a factor in the pathogenesis of juvenile absence epilepsy–related phenotypes.
TREATMENT AND PROGNOSIS
Wolf and Inoue 4 report that 82% of patients with juvenile absence epilepsy will be seizure free when treated with ethosux-imide or valproic acid. Newer-generation agents have shown effi-cacy, although usually in noncontrolled open-label studies. The seizures of juvenile absence epilepsy may also be worsened by certain antiepileptic drugs. 14
CASE 4-1: Juvenile Absence Epilepsy
Patient History : A 12-year-old boy with diagnoses of atten-tion-deficit disorder and hyperactivity was noted to have “staring episodes” beginning over 1 year before this evaluation. About 6 months earlier, the staring episodes became accompanied by some eye blinking and mouth twitching.
Seizure Risk Factors : He had a fraternal twin without clinical evidence of epilepsy. He was born at 34 weeks’ gestational age. A family history of epilepsy was reported in a paternal aunt and paternal cousin.
Medications : • Methylphenidate extended-release tablets • Clonidine
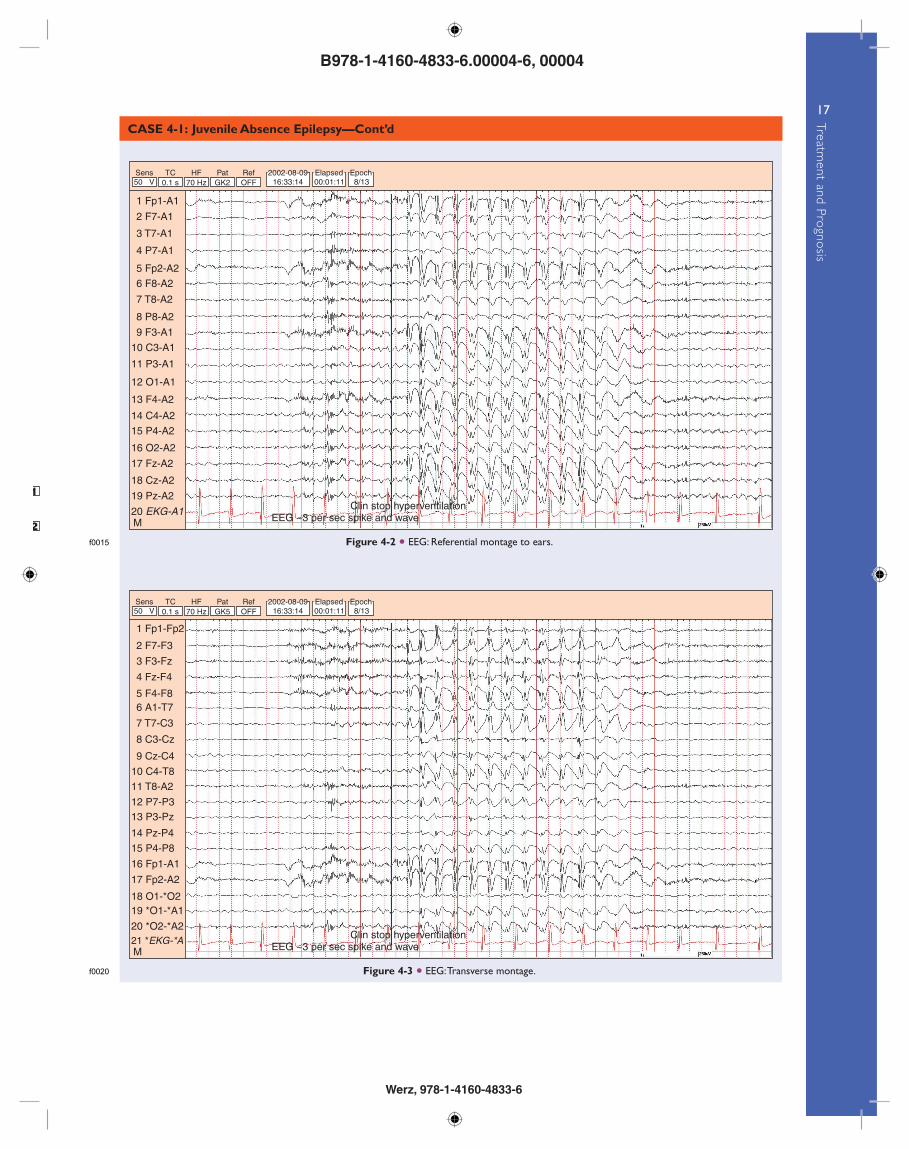
Video-EEG : Normal physiologic rhythms were seen. Approxi-mately 3-Hz spike and wave discharges lasting 4 to 6 seconds were associated with behavioral arrest. Two- to 3-Hz spikes were seen associated with some slow waves ( Figs. 4-1 to 4-3 ).
Outcome : The patient was discharged on lamotrigine.
AU1
AU2
Figure 4-1 • EEG: Longitudinal bipolar montage.
EEG ~3 per sec spike and waveClin stop hyperventilation
1 Fp1-F7
2 F7-T7
3 T7-P7
4 P7-O1
5 Fp2-F8
6 F8-T8
7 T8-P8
8 P8-O2
9 Fp1-F3
10 F3-C3
15 C4-P4
14 F4-C4
13 Fp2-F4
12 P3-O1
11 C3-P3
18 Cz-Pz
17 Fz-Cz
16 P4-O2
19 EKG-A1M
Sens TC HF Pat Ref30 µV 0.1 s 70 Hz GK1 OFF
2002-08-09 Elapsed Epoch16:33:14 00:01:11 8/13
s0030
p0075
b0010
s0035p0080
s0040p0085
s0045
u0040
u0045
s0050 p0105
s0055 p0110
f0010
B978-1-4160-4833-6.00004-6, 00004
Werz, 978-1-4160-4833-6
17
Treatment and Prognosis
CASE 4-1: Juvenile Absence Epilepsy—Cont’d
1
2 Figure 4-2 • EEG: Referential montage to ears.
EEG ~3 per sec spike and waveClin stop hyperventilation
1 Fp1-A1
2 F7-A1
3 T7-A1
4 P7-A1
5 Fp2-A2
6 F8-A2
7 T8-A2
8 P8-A2
9 F3-A1
10 C3-A1
15 P4-A2
14 C4-A2
13 F4-A2
12 O1-A1
11 P3-A1
18 Cz-A2
19 Pz-A2
17 Fz-A2
16 O2-A2
20 EKG-A1M
Sens TC HF Pat Ref50 µV 0.1 s 70 Hz GK2 OFF
2002-08-09 Elapsed Epoch16:33:14 00:01:11 8/13
Figure 4-3 • EEG: Transverse montage.
EEG ~3 per sec spike and waveClin stop hyperventilation
1 Fp1-Fp2
2 F7-F3
3 F3-Fz
4 Fz-F4
5 F4-F86 A1-T7
7 T7-C3
8 C3-Cz
9 Cz-C4
10 C4-T8
15 P4-P8
14 Pz-P4
13 P3-Pz12 P7-P3
11 T8-A2
18 O1-*O219 *O1-*A1
20 *O2-*A2
17 Fp2-A2
16 Fp1-A1
21 *EKG-*AM
Sens TC HF Pat Ref50 µV 0.1 s 70 Hz GK5 OFF
2002-08-09 Elapsed Epoch16:33:14 00:01:11 8/13
f0015
f0020

B978-1-4160-4833-6.00004-6, 00004
Werz, 978-1-4160-4833-6
18
Juve
nile
Abs
ence
Epi
leps
y References
[1] Nordli Jr DR . Idiopathic generalized epilepsies recognized by the International League Against Epilepsy . Epilepsia 2005 ; 46 (Suppl. 9) : 48 – 56 .
[2] Fenichel G . Clinical Pediatric Neurology . Philadelphia : WB Saunders ; 2001 .
[3] Wolf P . Juvenile absence epilepsy . In: Roger J , Bureau M , Dravet C , et al., editors. Epileptic Syndromes in Infancy, Childhood and Adolescence . 3rd ed London : John Libbey ; 1992 . p. 307 – 12 .
[4] Wolf P , Inoue Y . Therapeutic response of absence seizures in patients of an epilepsy clinic for adolescents and adults . J Neurol 1984 ; 231 : 225 – 9 .
[5] Tovia E , Goldberg-Stern H , Shahar E , Kramer U . Outcome of children with juvenile absence epilepsy . J Child Neurol 2006 ; 21 : 766 – 8 .
[6] Ebersole J , Pedley T . Current Practice of Clinical Electroencephalography . Philadelphia : Lippincott Williams & Wilkins ; 2003 . p. 518 – 25 .
[7] Betting LE , Mory SB , Lopes-Cendes I , et al . MRI reveals structural abnormalities in patients with idiopathic generalized epilepsy . Neurology 2006 ; 67 : 848 – 52 .
[8] Woermann FG , Sisodiya SM , Free SL , Duncan JS . Quantitative MRI in patients with idiopathic generalized epilepsy: Evidence of widespread cerebral structural changes . Brain 1998 ; 121 : 1661 – 7 .
[9] Heron SE , Khosravani H , Varela D , et al . Extended spectrum of idiopathic generalized epilepsies associated with CACNA1H functional variants . Ann Neurol 2007 ; 62 : 549 – 50 .
[10] Marini C , Scheffer IE , Crossland KM , et al . Genetic architecture of idiopathic generalized epilepsy: Clinical genetic analysis of 55 multiplex families . Epilepsia 2004 ; 45 : 467 – 78 .
[11] Haug K , Warnstedt M , Alekov AK , et al . Mutations in CLCN2 encoding a voltage-gated chloride channel are associated with idiopathic generalized epilepsies . Nat Genet 2003 ; 33 : 527 – 32 .
[12] Durner M , Keddache MA , Tomasini L , et al . Genome scan of idiopathic generalized epilepsy: Evidence for major susceptibility gene and modifying genes influencing the seizure type . Ann Neurol 2001 ; 49 : 328 – 35 .
[13] Sander T , Hildmann T , Kretz R , et al . Allelic association of juvenile absence epilepsy with a GluR5 kainate receptor gene (GRIK1) polymorphism . Am J Med Genet 1997 ; 74 : 416 – 21 .
[14] Murphy K , Delanty N . Primary generalized epilepsies . Curr Treat Options Neurol 2000 ; 2 : 527 – 42 .


















