Scd after stemi
20
SCD after STEMI- Prediction & Prevention
-
Upload
please-hit-like-if-you-really-liked-my-ppts -
Category
Health & Medicine
-
view
220 -
download
0
Transcript of Scd after stemi

SCD after STEMI- Prediction & Prevention

Introduction• Sudden cardiac death is one of the causes of death in
a patient of myocardial infarction
• In observational studies the incidence of SCD after MI has ranged from 2% to 4%
• In the VALIANT trial, SCD rate was found to be 1.4%/month in the first 30 days, which decreased exponentially over time

Time periods after MI• On the basis of literature, we can consider 3 distinct time periods
after MI: Early (≥48 hours–40 days), subacute (41 days–6 months), and remote (>6 months to many years)
• Current data suggests the following:• First 48 hrs: Life threatening VAs that occur during the first 24–48
h of ACS do not imply the risk for SCD over time• Early Phase (also called as ‘48-h and 40-day Rule’): most
controversial as data not clear whether ICD implantation is beneficial or not
• Subacute & Remote Phase: ACC/AHA/ESC & HRS guidelines state that ICDs should be implanted for the primary prevention of SCD in patients at least 40 days after MI, with an EF of 30–40% and NYHA class II–III, who are on optimal pharmacotherapy and have a reasonable expectation of survival, with a good functional status for at least 1 year (Class 1, Level of Evidence A)

Risk Factors• Reduced LV ejection fraction (LVEF) or history of heart failure• Ventricular tachycardia (VT) induced by electrophysiologic
study (EPS)• Spontaneous ventricular premature beats (VPBs) and
nonsustained ventricular tachycardia (NSVT) documented on 24hour ambulatory monitoring
• Late potentials on a signal averaged ECG (SAECG)• Reduced heart rate variability (HRV) assessed by ambulatory
monitoring• T wave (repolarization) alternans (TWA)
Sustained arrhythmias that occur in the early postMI phase (usually defined as the first 48 hours) are generally considered epiphenomena of the MI and are not consistently associated with long term prognosis

ICD Studies in the Early Phase of MI
• Both DINAMIT & IRIS showed fewer SCD deaths
• However, an increase in non-arrythmic deaths and non-significant benefit of ICD implantation in the early phase of MI was observed

• The BEST multicenter investigation comprised 143 survivors of acute MI and patients were stratified to a conventional strategy or Electrophysiology Pacing Study (EPS) – a guided strategy for ICD implantation
• In the follow-up of 2 years, a trend towards lower mortality in the EPS-guided/ICD arm was observed in comparison with the conventional arm: 20 versus 29.5%, respectively


Study details• In this study by Zaman et al in STEMI patients, EF was
assessed for more than 2 days of coronary intervention• If EF> 40% : Patients discharged• If EF< 40%: EPS was done• No inducible patients were discharged and those with
inducible monomorphic ventricular tachycardia lasting more than 10 s had ICDs implanted before discharge.
• At the median of 12 months of followup, the mortality rate in all subgroups was low: 3, 3 and 6%, respectively.
• This suggests that early ICD implantation limited to patients with inducible ventricular tachycardia results in low mortality in the population treated with coronary intervention due to Stelevation MI

Possible Reasons for discrepancy between SCD susceptibility in the early phase of MI
& the lack of benefit from ICD therapy
• ICD shock therapies (adequate and inappropriate) lead to a two or threefold increase in total mortality, respectively, probably due to heart failure progression over longterm followup
• Right ventricular pacing has a detrimental effect
• 'Inappropriate' protocols are followed, with regard to inclusion criteria (too high cutoff value of ejection fraction in patients qualifying for ICD therapy).

Optimizing ICD therapyIt can be done by:
• Implantation of dual chamber ICDs, which seem to be superior to single chamber ICDs.
• Reprogramming of the device settings (enhanced programming).
• Programming ventricular tachycardia or fibrillation at longer detection intervals (i.e., number of intervals detected: 30/40).
• Applying ventricular tachycardia or fibrillation detection zones at higher rates (i.e., fast ventricular tachycardia up to 250 bpm).
• Introducing new technological tools (i.e., enabling the monitoring of the patients' fluid status).

Future ICD perspectives in post-MIpatients
• Better selection of high risk MI survivors using the microvolt T-wave alternans and electrophysiological pacing studies
• Biventricular cardioverter defibrillator in the early phase of MI to prevent both heart failure progression and SCD episodes.
• Blood pressure monitoring detector to deliver shock therapy in hemodynamically unstable patients only.
• Wearable cardioverter defibrillators.
• Miniature, portable, easily attached and removable automated external defibrillators for the crucial '48h and 40day‘ period

Does EPS play a role in stratification?
• Objective: The purpose of this study was to evaluate outcomes of electrophysiology (EP)-guided defibrillatorimplantation early after ST-elevation MI in patients with ejection fraction ≤40%
• Methods: EP study was performed 9 days after MI (n = 360). Predischarge defibrillator was recommended if VT with cycle length ≥200 ms was induced with ≤4 extrastimuli (EP-positive [EP(pos)], n = 142). EP-negative (EP(neg)) patients were discharged without a defibrillator
• Primary Endpoint: Either sudden death or spontaneous ventricular arrhythmia
Kumar S et al. Heart Rhythm. 2010 Nov;7(11):1589-97

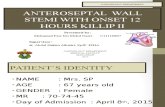
Results
71
6
Defibrillator implantation (in % of patients) as per study
groups
EP PositiveEP Negative

Incidence of primary endpoint at 2 years
Category 1 Category 20
5
10
15
20
25
Primary endpoint
Primary endpoint
22%
4.3%
p=0.035

Lack of a defibrillator in EP positive patients conferred them with a 4 fold increased risk of sudden death (p=0.014)
EP(neg) patients without a defibrillator were at significantly lower risk for the primary endpoint than were EP(pos) patients without a defibrillator (adjusted HR 0.34, P = .011).
Short inducible VT cycle length (200-230 ms) and use of the fourth extrastimulus identified patients at significant arrhythmic risk.

Conclusions
• EP study performed early after MI identified patients at significant long-term arrhythmic risk at a critical time after MI in whom defibrillator implantation was protective
• EP testing might be a promising means of risk stratification in early post-MI patients

Current Recommendations of major societies
• The evidence was less well established to support the routine use of Holter monitoring, SAECG, or HRV for arrhythmia risk stratification after an MI
2004 American College of
Cardiology/American Heart Association
(ACC/AHA) guidelines on STEMI
• The routine use of SAECG, HRV, and T wave alternans (TWA) for risk stratification is not adequately supported at this time
2008 AHA/ACC/Heart Rhythm Society (HRS) scientific statement on
noninvasive risk stratification

Conclusions• With regard to primary prevention of sudden cardiac
death (SCD), the most important initial parameter is left ventricular ejection fraction (LVEF)
• LV function should be assessed in the time period when an ICD may be indicated (ie, after 40 days). If a low LVEF was documented earlier, it should be reassessed at this time.
http://www.uptodate.com/contents/incidence-of-and-risk-stratification-for-sudden-cardiac-death-after-acute-myocardial-infarction

Further risk stratification is largely based upon the LVEF:• No further risk stratification is required for patients in whom an ICD
is indicated for primary prevention of SCD: those with an LVEF ≤30 percent (MADIT II criteria) or those who satisfy SCD-HEFT criteria (ischemic cardiomyopathy, LVEF ≤35 percent, NYHA II or III HF)
• For patients with an LVEF >40 percent, we recommend no further risk stratification, since such patients are unlikely to meet indications for an ICD
• For patients with an LVEF of 31 to 40 percent, we do not routinely proceed with further risk stratification. However, periodic Holter monitoring (once or twice a year) is a reasonable approach, with the understanding that patients found to have nonsustained ventricular tachycardia should be referred for invasive electrophysiology (EP) study
http://www.uptodate.com/contents/incidence-of-and-risk-stratification-for-sudden-cardiac-death-after-acute-myocardial-infarction

References• Sredniawa B et al. Early therapy following myocardial infarction:
arguments for and against implantable cardioverter-defibrillators. Future Cardiol. 2010;6(3):315323
• Zaman S, Kovoor P. Sudden cardiac death early after myocardial infarction: pathogenesis, risk stratification, and primary prevention. Circulation. 2014 Jun 10;129(23):2426-35
• Estes NA 3rd. The challenge of predicting and preventing sudden cardiac death immediately after myocardial infarction. Circulation. 2009 Jul 21;120(3):185-7
• Podrid PJ et al. Incidence of and risk stratification for sudden cardiac death after acute myocardial infarction. Accessed from: http://www.uptodate.com/contents/incidence-of-and-risk-stratification-for-sudden-cardiac-death-after-acute-myocardial-infarction















![Impact of Bleeding on Mortality After Percutaneous ... · female sex, presentation (by normal biomarkers [elective/ ACS], raised biomarkers [non-STEMI], and STEMI), elevated white](https://static.fdocuments.in/doc/165x107/5ed7f9dfc64afa2ac7587d50/impact-of-bleeding-on-mortality-after-percutaneous-female-sex-presentation.jpg)