Stemi: Guides

of 44
-
Upload
adeline-n-omene -
Category
Documents
-
view
239 -
download
0
Transcript of Stemi: Guides
-
7/27/2019 Stemi: Guides
1/44
1
ACC/AHA 2009 STEMI Guideline
Focused Update and
Whats New in 2012 Guideline
David Zhao, MD, FACC, FSCAI
Professor of Medicine and Cardiac Surgery
Harry and Shelley Page Professor in Interventional Cardiology
Director, Cardiac Catheterization Laboratories
& Interventional Cardiology
Vanderbilt University Medical Center
Nashville TN, USA
-
7/27/2019 Stemi: Guides
2/44
2
1990 1992 1994 1996 1998 2000 20021990
ACC/AHAAMI
R. Gunnar1994
AHCPR/NHLBIUA
E. Braunwald 1996 1999Rev UpdACC/AHA AMIT. Ryan
2004 2007Rev UpdACC/AHA STEMI
E. Antman
2000 2002 2007Rev Upd RevACC/AHA UA/NSTEMIE. Braunwald; J. Anderson
2004 2007
Evolution of Guidelines for ACS
2009
2009Upd
ACC/AHA STEMI/PCIF. Kushner
-
7/27/2019 Stemi: Guides
3/44
3
Hospitalizations in the U.S. Due to Acute
Coronary Syndromes (ACS)
Acute Coronary
Syndromes*
1.57 Million Hospital Admissions - ACS
UA/NSTEMI STEMI
1.24 millionAdmissions per year
.33 millionAdmissions per year
Heart Disease and Stroke Statistics 2007 Update. Circulation 2007; 115:69-171.
*Primary and secondary diagnoses. About 0.57 million NSTEMI and 0.67 million UA.
-
7/27/2019 Stemi: Guides
4/44
4
Class I
Benefit >>> Risk
Procedure/ Treatment
SHOULD be
performed/
administered
Class IIa
Benefit >> Risk
Additional studies with
focused objectives
neededIT IS REASONABLE
to perform
procedure/administer
treatment
Class IIb
Benefit Risk
Additional studies with
broad objectives
needed; Additional
registry data would behelpful
Procedure/Treatment
MAY BE CONSIDERED
Class III
Risk Benefit
No additional studies
neededProcedure/Treatmentshould NOT be
performed/administered
SINCE IT IS NOT
HELPFUL AND MAY BE
HARMFUL
shouldis recommendedis indicatedis useful/effective/
beneficial
is reasonablecan be useful/effective/
beneficialis probably recommended
or indicated
may/might be consideredmay/might be reasonableusefulness/effectiveness is
unknown /unclear/uncertain
or not well established
is not recommendedis not indicatedshould notis not
useful/effective/beneficialmay be harmful
Applying Classification of Recommendations
and Level of Evidence
-
7/27/2019 Stemi: Guides
5/44
Class I
Benefit >>> Risk
Procedure/ Treatment
SHOULD be
performed/
administered
Class IIa
Benefit >> Risk
Additional studies with
focused objectives
neededIT IS REASONABLE to
perform
procedure/administer
treatment
Class IIb
Benefit Risk
Additional studies with
broad objectives needed;
Additional registry data
would be helpful
Procedure/Treatment
MAY BE CONSIDERED
Class III
Risk Benefit
No additional studies
neededProcedure/Treatment
should NOT be
performed/administered
SINCE IT IS NOT
HELPFUL AND MAY
BE HARMFUL
Applying Classification of Recommendations
and Level of Evidence
Level A: Multiple populations evaluated; Data derived from multiple randomized clinical trials or meta-analyses
Level B: Limited populations evaluated. Data derived from a single randomized trial or non-randomized studies
Level C: Very limited populations evaluated. Only consensus opinion of experts, case studies, or standard-of-care.
-
7/27/2019 Stemi: Guides
6/44
6
Recommendations for the use ofThienopyridines
-
7/27/2019 Stemi: Guides
7/447
Recommendations for the use of
Thienopyridines
A loading dose of thienopyridine is recommended for
STEMI patients for whom PCI is planned. Regimens shouldbe one of the following:
MODIFIED
Recommendat ion
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Clopidogrel at least 300 mg to 600mg should
be given as early as possible before or at the
time of primary or non-primary PCI.
-
7/27/2019 Stemi: Guides
8/44
Optimal Plavix Loading Dose:
ISAR CHOICE
-
7/27/2019 Stemi: Guides
9/449
Recommendations for the use of
Thienopyridines
Prasugrel 60 mg should be given as soon aspossible for primary PCI.
MODIFIED
Recommendat ion
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
-
7/27/2019 Stemi: Guides
10/4410
0
5
10
15
0 30 60 90 180 270 360 450
Percent(%)
Days From Randomization
9.5%6.5%
HR 0.68(0.54-0.87)
P=0.002
12.4%10.0%
HR 0.79
(0.65-0.97)P=0.02
Clopidogrel
PrasugrelNNT = 42
CV Death / MI / Stroke
TIMI MajorNonCABG Bleeds
ClopidogrelPrasugrel 2.4
2.1
STEMI Cohort
N=3534
Montalescot et al Lancet 2008.Adapted withpermiss ion from Antman EM.
TRITON TIMI-38
-
7/27/2019 Stemi: Guides
11/44
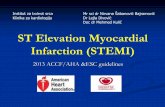
PLATO (The Study of Platelet Inhibition andPatient Outcomes)
Cumulative Incidence of Primary Endpoint* and Major Bleeding
Adapted from: Wallentin L et al.
N Engl J Med. 2009; Available at: http://www.nejm.org.
Ticagrelor
Clopidogrel
HR=0.84 (0.77 0.92)
P
-
7/27/2019 Stemi: Guides
12/4412
Recommendations for the use of
Thienopyridines
For STEMI patients undergoing non-pr imaryPCI, the
following regimens are recommended:
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII a. and has been given clopidogrel, it should be
continued as the thienopyridine of choice.b. without a thienopyridine, a loading dose of 300-600
mg of clopidogrel should be given as the
thienopyridine of choice.
If the patient did not receive fibrinolytic therapyc. either a loading dose of 300-600 mg of clopidogrel
should be given or, once the coronary anatomy is
known and PCI is planned, a loading dose of 60 mg of
prasugrel should be given promptly and no later than 1
hour after the PCI.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
If the patient has received fibrinolytic therapy
MODIFIED
Rec
-
7/27/2019 Stemi: Guides
13/4413
Thienopyridines
The duration of thienopyridine therapyshould be as follows:MODIFIED
Recommendat ion
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII a. In patients receiving a stent (BMS or DES)
during PCI for ACS, clopidogrel 75 mg daily
or prasugrel 10 mg daily should be given
for at least 12 months;
b. If the risk of morbidity from bleeding
outweighs the anticipated benefit affordedby thienopyridine therapy, earlier
discontinuation should be considered.
-
7/27/2019 Stemi: Guides
14/4414
Thienopyridines
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
In patients taking a thienopyridine in whom coronary
artery bypass surgery (CABG) is planned and can be
delayed, it is recommended that the drug be discontinued
to allow for dissipation of the antiplatelet effect.
The period of withdrawal should be at least 5 days in
patients receiving clopidogrel
and at least 7 days in patients receiving prasugrel,
unless the need for revascularization and/or the net
benefit of the thienopyridine outweighs the potential risks
of excess bleeding.
MODIFIED
Recommendat ion (prasugrel added)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
-
7/27/2019 Stemi: Guides
15/4415
Thienopyridines
NEW
Recommendat ion
In STEMI patients with a prior
history of stroke and transientischemic attack for whom primary
PCI is planned, prasugrel is not
recommended as part of a dual
antiplatelet therapy regimen
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
-
7/27/2019 Stemi: Guides
16/44
TRITON TIMI-38 Net Clinical BenefitBleeding Risk Subgroups
Overall
60 kg
-
7/27/2019 Stemi: Guides
17/4417
Recommendations for the Use of
Glycoprotein IIb/IIIa Receptor
Antagonists in STEMI
-
7/27/2019 Stemi: Guides
18/4418
It is reasonable to start treatment with glycoprotein
IIb/IIIa receptor antagonists at the time of primaryPCI (with or without stenting) in selected patients
with STEMI:
abciximab
tirofiban and eptifibatide
Use of Glycoprotein IIb/IIIa Receptor
Antagonists in STEMI
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Modif ied
Recommendat ion
-
7/27/2019 Stemi: Guides
19/4419
Use of Glycoprotein IIb/IIIa Receptor
Antagonists in STEMI
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIIIThe usefulness of glycoprotein IIb/IIIa receptorantagonists (as part of a preparatory
pharmacologic strategy for patients with STEMI
prior to arrival in the cardiac catheterizationlaboratory for angiography and PCI) is uncertain.
Modif ied
Recommendat ion
-
7/27/2019 Stemi: Guides
20/4420
BRAVE 3: Effects of Abciximab
Mehilli et al. Circ. 2009;119:1933-1940
No significant difference in infarct
size or major bleeding
Patient received Plavix 600mg
loading
P= 0.47
P= 0.40
-
7/27/2019 Stemi: Guides
21/4421
Recommendations for
Use of Parenteral
Anticoagulants in Patients
with STEMI
-
7/27/2019 Stemi: Guides
22/44
22
Use of Parenteral Anticoagulants
in STEMI(cont.)
Modif ied
Recommendat ion
b. Bivalirudin is useful as support for primary PCI with orwithout prior treatment with heparin.
For patients proceeding to primary
PCI, who have been treated with
ASA and a thienopyridine,
recommended supportive
anticoagulant regimens include:
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
-
7/27/2019 Stemi: Guides
23/44
23
Bilvalirudin added as an acceptable anticoagulant for
primary PCI
Unfractionated heparin (UFH) administration guided
by: Therapeutic activated clotting time (ACT) levels
Prior administration of GP IIb/IIIa receptor
antagonists
Enoxaparin and fondaparinux unchanged from 2007STEMI Focused Update
Use of Parenteral Anticoagulants in STEMI
Patients Proceeding to Primary PCI:
Modified Class I Recommendations
-
7/27/2019 Stemi: Guides
24/44
24
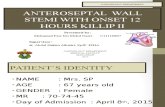
HORIZONS-AMI: Time-to-Event Curves
through 30 days: Net Adverse Clinical Events
Treatment with bivalirudin alone compared with UFH + GP IIb/IIIa
Inhibitors resulted in reduced 30-day rates of net adverse
clinical events
[HR=0.75, (0.62-0.92); p=0.006]Stone et al. N Eng J Med. 2008;358:2218-30.
-
7/27/2019 Stemi: Guides
25/44
25
HORIZONS-AMI: Time-to-Event Curves
through 30 days: Major Bleeding
HR=0.59 (0.45-0.76); p
-
7/27/2019 Stemi: Guides
26/44
26
Recommendations for triage and
transfer for PercutaneousCoronary Intervention for Patients
with STEMI
-
7/27/2019 Stemi: Guides
27/44
27
Recommendations for Triage and
Transfer for PCI (for STEMI)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
NEW
Recommendat ion
Each community should develop aSTEMI system of care following the
standards developed forMission
Lifeline including:
Ongoing multidisciplinary team
meetings with EMS, non-PCI-
capable hospitals (STEMI Referral
Centers), & PCI-capable hospitals
(STEMI Receiving Centers)
-
7/27/2019 Stemi: Guides
28/44
28
Recommendations for Triage and
Transfer for PCI (for STEMI) (cont.)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
NEW
Recommendat ion
STEMI system of care standards incommunities should also include:
Process for prehospital
identification & activation
Destination protocols to STEMIReceiving Centers
Transfer protocols for patients
who arrive at STEMI Referral
Centers and are primary PCI
candidates, and/or are fibrinolytic
ineligible and/or in cardiogenic
shock
-
7/27/2019 Stemi: Guides
29/44
7
2.5
1
0.05
9
6.8
21.1
0
1
2
3
4
5
6
7
8
9
10
Death Re-MI CVA Hemo CVA
%P
atients
PCI Thrombolytics
p=0.0002
P
-
7/27/2019 Stemi: Guides
30/44
Stenestrand, U. et al. JAMA 2006;296:1749-1756.
Age-Adjusted and Propensity Score-Adjusted MortalityAccording to Time to Reperfusion and Type of Therapy
-
7/27/2019 Stemi: Guides
31/44
31
Recommendations for Triage and
Transfer for PCI (for STEMI)(cont.)
NEW
Recommendat ion
I IIaIaIa IIbIbIb IIIIIIIIIaIaIa IIbIbIb IIIIIIIIIaIaIa IIbIbIb IIIIIIIIaIaIa IIbIbIb IIIIIII
It is reasonable to transfer high
risk patients who receive fibrinolytic
therapy as primary reperfusiontherapy at a non-PCI capable facility
to a PCI-capable facility as soon as
possible where either PCI can be
performed when needed or as apharmacoinvasive strategy.
-
7/27/2019 Stemi: Guides
32/44
32
CARESS-IN-AMI:Primary Outcomeprimary outcome (composite of all cause mortality, reinfarction, & refractory MI within 30 days)
occurred significantly less often in the immediate PCI group vs. standard care/rescue PCI group
10.7%
4.4%
HR=0.40 (0.21-0.76)
Di Mario et al. Lancet 2008;371.
TRANSFER AMI Effi
-
7/27/2019 Stemi: Guides
33/44
33
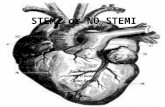
TRANSFER-AMI: Efficacy
Kaplan Meier Curves for Primary Endpoint
17.2%
11.0%
primary end point: composite of death, reinfarction, recurrent ischemia, new
or worsening CHF, or shock within 30 dayspharmaco-invasive group=11.0% vs. standard treatment group=17.2%
RR= 0.64, 95 CI% (0.47-0.87)
C
umulativeIncidence
Days
p=0.004
Cantor et al. N Engl J Med 2009;360:26
-
7/27/2019 Stemi: Guides
34/44
34
Recommendations for Triage and
Transfer for PCI (for STEMI)(cont.)
NEW
Recommendat ion
I IIaIaIa IIbIbIb IIIIIIIIIaIaIa IIbIbIb IIIIIIIIIaIaIa IIbIbIb IIIIIIIIaIaIa IIbIbIb IIIIIII
Consideration should be given
to initiating a preparatory
antithrombotic (anticoagulant
plus antiplatelet) regimen prior
to and during patient transfer
to the catheterizationlaboratory.
-
7/27/2019 Stemi: Guides
35/44
35
Triage and Transfer for PCI (in STEMI)
2009 STEMI Focused Update. Appendix 5
Each community and each facility in thatcommunity should have an agreed-upon planfor how STEMI patients are to be treated,including:
which hospitals should receive STEMI patientsfrom EMS units capable of obtaining diagnosticECGs
management at the initial receiving hospital, and
written criteria & agreements for expeditioustransfer of patients from non-PCI-capable to PCI-capable facilities
-
7/27/2019 Stemi: Guides
36/44
36
Triage and Transfer for PCI (in STEMI)
Need for the development of regionalsystems of STEMI care through stakeholderefforts to evaluate ACS care using: standardized performance & quality improvement
measures, (e.g., endorsed by the ACC, AHA, JointCommission, Centers for Medicare and MedicaidServices)
standardized quality-of-care data registriesdesigned to track and measure outcomes,complications and adherence to evidence-based
processes of care NCDR ACTION Registry
American Heart Association Get With the Guidelines
-
7/27/2019 Stemi: Guides
37/44
37
Triage and Transfer for PCI (in STEMI)
American Heart Associations Mission
Lifel ineis an initiative to encourage
closer cooperation and trust amongst
prehospital care providers, and cardiaccare professionals.
-
7/27/2019 Stemi: Guides
38/44
Whats New in 2012
STEMI Guideline
-
7/27/2019 Stemi: Guides
39/44
Whats New in 2012
STEMI Guideline
39
-
7/27/2019 Stemi: Guides
40/44
Whats New in 2012
STEMI Guideline
40
-
7/27/2019 Stemi: Guides
41/44
Whats New in 2012
STEMI Guideline
41
-
7/27/2019 Stemi: Guides
42/44
Whats New in 2012
STEMI Guideline
42
-
7/27/2019 Stemi: Guides
43/44
Whats New in 2012
STEMI Guideline
43
-
7/27/2019 Stemi: Guides
44/44
Whats New in 2012
STEMI Guideline