Gurunanak & Chandraketu Pandya English Medium School with ...

Sample Copy. Not for Distribution.

i
Oral Carriage & Suffering of
Staphylococcus Aureus
Sample Copy. Not for Distribution.
ii
Publishing-in-support-of,
EDUCREATION PUBLISHING
RZ 94, Sector - 6, Dwarka, New Delhi - 110075
Shubham Vihar, Mangla, Bilaspur, Chhattisgarh - 495001
Website: www.educreation.in
________________________________________________________________
© Copyright, Authors
All rights reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form by any means, electronic, mechanical, magnetic, optical, chemical, manual, photocopying, recording or otherwise, without the prior written consent of its writer.
ISBN: 978-1-61813-887-3
Price: ` 2565.00
The opinions/ contents expressed in this book are solely of the authors and do not represent the opinions/ standings/ thoughts of Educreation or the Editors . The book is released by using the services of self-publishing house.
Printed in India
Sample Copy. Not for Distribution.

iii
Oral Carriage & Suffering
of Staphylococcus Aureus Oral Infection & Staph.Aureus
AUTHOR
Dr. Biswajit Batabyal
EDUCREATION PUBLISHING (Since 2011)
www.educreation.in
Sample Copy. Not for Distribution.

iv
Sample Copy. Not for Distribution.

v
Content List ______________________________________________________
S. No. Content Page
Abbreviations
Abstract
1. Introduction 1
1.1. Microbiology 2
1.2. Role in disease 3
1.3. Atopic dermatitis 4
1.4. Toxic shock syndrome and food
poisoning
4
1.5. Mastitis in cows 4
1.6. Reproduction 4
1.7. Virulence factors 5
1.8. Role of pigment in virulence 6
1.9. Classical diagnosis 7
1.10. Rapid diagnosis and typin 7
1.11. Treatment and antibiotic resistance 8
1.12. Antibiotics 9
1.13. Penicillin Group 9
1.14. Cephalosporins Group 15
1.15. Macrolide Antibiotics Group 16
1.16. Lincosamides Group 18
1.17. Rifamycins 19
1.18. Linezolid 20
Sample Copy. Not for Distribution.

vi
1.19. Quinolones (Fluoroquinolones) 21
1.20. Vancomycin 22
1.21. Carbapenems Group 23
1.22. Mechanisms of antibiotic resistance 24
1.23. MRSA in oral cavity 27
2. Literature Review 30
3. Aims & Objectives 43
3.1. Importance of the Study 43
3.2. Aims of the Study 43
3.3. Objectives of the Study 44
4. Research Methodology 45
4.1. Study Period & Study Setting 45
4.2. Study patients and participants 45
4.3. Collection and processing of the samples 46
4.4. Identification of isolates 48
4.5. Mannitol salt agar 48
4.6. Gram Technique 50
4.7. Catalase test 52
4.8. Coagulase test 53
4.9. DNase test 56
4.10. Sensitivity testing using Disc Diffusion
technique
58
4.11. Tryptone soya broth 63
4.12. Mueller Hinton agar 63
4.13. Methicillin Resistant Staph. aureus
detection
64
4.14. List of materials used for the study 65
4.15. Control strain 68
4.16. Maintenance of isolated strains 69
5. Results 70
Sample Copy. Not for Distribution.

vii
6. Statistical Analysis 84
7. Discussion 92
8. Conclusion 105
9. Bibliography 108
Sample Copy. Not for Distribution.

viii
Sample Copy. Not for Distribution.
ix
ABBREVIATIONS ______________________________________________________
AMX : Amoxicillin
AMP : Ampicillin
AMC : Amoxicillin/clavulanic acid
AS : Ampicillin/sulbactam
ABST : Antibiotic sensitivity test
ATCC : American Type Culture Collection °C : Degree centigrade
CPS : Coagulase positive Staphylococcus
CLSI : Clinical Laboratory Standard Institute
CPD : Cefpodoxime
CD : Clindamycin
CIP : Ciprofloxacin
CV : Crystal violet
DNA : Deoxyribonucleic acid
DNase : Deoxiribonuclease
EF : Exfoliative
E : Erythromycin
EDTA : Ethylenediaminetetraacetic acid
Gm : Gram
GPC : Gram positive cocci
GNB : Gram negative bacilli
GDA : Group-D Assistant
H2O2 : Hydrogen per oxide
HCl : Hydrochloric acid
hr : Hour
Ig : Immunoglobulin
Sample Copy. Not for Distribution.

x
IPM : Imipenem
IS : Intermediate Sensitive
LZ : Linezolid
MRSA : Methicillin resistant Staphylococcus aureus
MSSA : Methicillin sensitive Staphylococcus aureus
MDR : Multi drug resistant
mg : Milligram
MW : Molecular weight
MRP : Meropenem
MSA : Mannitol salt agar
MHA : Mueller Hinton agar
mm : Millimeter
ml : Milli litre
mcg : Microgram
min : Minute
NEG : Negative
Nacl : Sodium chloride
NCCLS : National committee for clinical laboratory
standards
OX : Oxacillin
OF : Ofloxacin
OS : Oral Surgery
OPD : Outdoor patients department
OP &
OM
: Oral Pathology & Microbiology
OT : Operation theater
ORSA : Oxacillin resistant Staphylococcus aureus
OSSA : Oxacillin sensitive Staphylococcus aureus
PI : Piperacillin
PIT : Piperacillin/Tazobactam
POS : Positive
PBP : Penicillin-binding protein
PCR : Polymerase chain reaction
Sample Copy. Not for Distribution.

xi
PVL : Panton-valentine leukocidin
R : Resistant
RNA : Ribonucleic acid
rRNA : Ribosomal Ribonucleic acid
RIF : Rifampicin
S : Sensitive
SA : Staphylococcus aureus
SSSS : Staphylococcal scalded skin syndrome
Scc mec : Staphylococcal cassette chromosome mec
Sec : Second
SSIs : Surgical Site infections
TSS : Toxic shock syndrome
TI : Ticarcillin
TCC : Ticarcillin/clavulanic acid
TSB : Tryptone soya broth
V : Volume
VA : Vancomycin
VRSA : Vancomycin-resistant Staphylococcus aureus
VISA : Vancomycin Intermediate Staphylococcus
aureus
W : Weight
WHO : World Health Oraganisation
μg : Microgram
μl : Micro liter
*****
Sample Copy. Not for Distribution.

xii
Sample Copy. Not for Distribution.

xiii
ABSTRACT ______________________________________________________
The oral cavity carriage and antibiotic susceptibility patterns of
Staphylococcus aureus in Dental hospital staff and healthy general
population were determined. Oral cavity swabs were taken from
113 healthy general population and 90 health care workers.
Antibiotic disc susceptibility testing was conducted following the
CLSI method. Staphylococcus aureus carriage was noted in 28.3%
of healthy general population and 38.9% of health care workers.
Resistance to commonly used oral antibiotics of healthy general
population & health care workers, ampicillin 93.8% & 97.2%,
amoxicillin/clavulanic acid 84.4% & 77.2%, amoxicillin 43.8% &
57.2%, ciprofloxacin 53.2% & 57.2% and ofloxacin 37.5% &
42.9%, respectively. 5.7% methicillin resistant Staphylococcus
aureus was detected among the hospital personnel from isolated
strain. The MRSA isolates showed multiple drug resistance
(MDR), except imipenem. Hospitals should assess the advantages
and disadvantages of routinely culturing personnel, however, in
outbreak situation hospital personnel especially young persons
may be sources of nosocomial infection.
Staphylococcus aureus is a well recognized pathogen
associated with a variety of clinical syndrome. The role of Staph.
aureus in some types of oral disease may be more important than
previously recognized. The present study was designed to
investigate the prevalence of Staphylococcus aureus, MRSA and
their rate of resistance to different anti staphylococcal antibiotics.
For this study, Gurunanak Institute of Dental Science & Research
(Kolkata), selected patients who were suffering from
Staphylococcus aureus oral infection. Isolated Staphylococcus
aureus was tested for Oxacillin (1 mcg) sensitivity and their
antibiotic susceptibility was investigated by using eighteen
antibiotics followed by Disk diffusion technique following CLSI
method. Out of the 223 specimens collected, 109 (48.8%) were
Sample Copy. Not for Distribution.

xiv
isolated. All the 109 (48.8%) specimens were studied in detail.
5.5% of the isolates were shown to be methicillin resistant Staph.
aureus (MRSA). Percentage (%) of resistance in commonly used
oral antibiotics are ampicillin 98.1%, amoxycillin/clavulanic acid
73.3%, amoxycillin 44.9%, ofloxacin 48.6% and ciprofloxacin
41.2%. The MRSA isolates showed multiple drug resistance
(MDR), except linezolid and imipenem. In line with more recent
surveys, this retrospective study suggests that Staph. aureus may
be more frequent isolate from the oral cavity than hitherto
suspected. The role of Staph. aureus in several diseases of the oral
mucosa merits further investigation.
The problem of infection has been persistent in the surgical
world even after the introduction of antibiotics. Pathogens that
infect surgical site can be acquired from the hospital environment
or other infected patients. A total of 66 pus samples from post-
operative oral & maxillofacial surgical infections were received in
the Department of Microbiology, Gurunanak Institute of Dental
Science & Research, Panihati, Kolkata, over a period of one year.
The isolates were identified using standard laboratory procedures.
All the isolates were tested for susceptibility to various commonly
used antibiotics and screened for oxacillin susceptibility according
to CLSI guidelines. Out of 66 pus samples received, 34(51.5%)
were culture positive for Staph. aureus. Methicillin resistance was
documented in 14 (41.2%) of the Staph. aureus isolates. Highest
efficacy was observed with linezolid (97.0%). All MRSA isolates
were 100% sensitive to linezolid. The hospital acquired surgical
site infection is alarming. Hospital disinfection and treatment
protocols should be practiced.
*****
Sample Copy. Not for Distribution.

Oral Carriage & Suffering of Staphylococcus Aureus
1
INTRODUCTION ______________________________________________________
Staphylococcus aureus literally the “golden cluster seed” or “the
seed gold” and also known as golden staph and Oro staphira is a
facultative anaerobic, Gram-positive coccus and is the most
common cause of staph infections. It is frequently part of the skin
flora found in the nose and on skin. About 20% of the human
populations are long term carriers of Staph. aureus [1]. The
carotenoid pigment staphyloxanthin is responsible for Staph.
aureus characteristic golden color, which may be seen in colonies
of the organism. This pigment acts as a virulence factor with an
antioxidant action that helps the microbe evade death by reactive
oxygen species used by the host immune system. Staph organisms
which lack the pigment are more easily killed by host defenses.
Staph. aureus can cause a range of illnesses from minor skin
infection, such as pimples, impetigo, boils (furuncles), cellulitis
folliculitis, carbuncles, scalded skin syndrome, and abscesses, to
life-threatening diseases such as pneumonia, meningitis,
osteomyelitis, endocarditis, toxic shock syndrome (TSS), chest
pain, bacteremia, and sepsis. Its incidence is from skin, soft tissue,
respiratory, bone, joint, endovascular to wound infections. It is still
one of the five most common causes of nosocomial infections,
often causing postsurgical wound infections. Abbreviated to Staph.
aureus or Staph. aureus in medical literature, Staph. aureus should
not be confused with the similarly named and similarly dangerous
(and also medically relevant) species of the genus Streptococcus.
Staph. aureus was discovered in Aberdeen, Scotland in 1880
by the surgeon Sir Alexander Ogston in pus from surgical
1
Sample Copy. Not for Distribution.

Dr. Biswajit Batabyal
2
abscesses [2]. Each year, some 500,000 patients in American
hospitals contract a staphylococcal infection [3].
1.1. Microbiology
Staph. aureus is a facultative anaerobic, Gram-positive coccus,
which appears as grape-like clusters when viewed through a
microscope and has large, round, golden-yellow colonies, often
with hemolysis, when grown on blood agar plates [4]. The golden
appearance is the etymological root of the bacteria’s name;
“golden” in Latin. Staph. aureus is catalase-positive (meaning that
it can produce the enzyme, “catalase”) and able to convert
hydrogen peroxide (H2O2) to water and oxygen, which makes the
catalase test useful to distinguish staphylococci from enterococci
and streptococci. A small percentage of Staph. aureus can be
differentiated from most other staphylococci by the coagulase test:
Staph. aureus is primarily coagulase positive (meaning that it can
produce the enzyme “coagulase”) that causes clot formation,
whereas most other Staphylococcus species are coagulase-negative
[4]. However, while the majority of Staph. aureus are coagulase-
positive, some may be atypical in that they do not produce
coagulase(the most common organism in patients with nosocomial
bacteremia is coagulase-negative staphylococcus) [5]. Incorrect
identification of an isolate can impact implementation of effective
treatment and /or control measures [6].
Fig.1.1.Grampositive cocci in cluster
Sample Copy. Not for Distribution.

Oral Carriage & Suffering of Staphylococcus Aureus
3
Fig.1.2. Staph. aureus Electron micrograph
1.2. Role In Disease
Staph. aureus are responsible for food poisoning through the
production of an enterotoxin and pathogenicity is also associated
with coagulase positivity. Staph. aureus may occur as a
commensal on skin; it also occurs in the nose frequently (in about a
third of the population) [7] and throat less commonly. The
occurrence of Staph. aureus under these circumstances does not
always indicate infection and, therefore, does not always require
treatment (indeed, treatment may be ineffective and re-colonization
may occur). It can survive on domesticated animals such as dogs,
cats, and horses, and can cause bumble foot in chickens. It can
survive for hours to days, weeks, or even months on dry
environmental surfaces depending on strain [8]. It can host phages,
such as Panton-Valentine leukocidin, that increase its virulence.
Staph. aureus can infect other tissues when barriers have been
breached (e.g. skin or mucosal lining). This leads to furuncles
(boils) and carbuncles (a collection of furuncles). In infants Staph.
aureus infection can cause a severe disease staphylococcal scalded
skin syndrome (SSSS) [9].
Staph. aureus alv infections can be spread through contact
with pus from an infected wound, skin-to-skin contact with an
infected person by producing hyaluronidase that destroys tissues,
and contact with objects such as towels, sheets, clothing, or athletic
equipment used by an infected person. Deeply penetrating Staph.
aureus infections can be severe. Prosthetic joints put a person at
particular risk for septic arthritis, and staphylococcal endocarditis
Sample Copy. Not for Distribution.

Dr. Biswajit Batabyal
4
(infection of the heart valves) and pneumonia, which may be
rapidly spread.
1.3. Atopic Dermatitis
Staph. aureus is extremely prevalent in atopic dermatitis patients,
who are less resistant to it than other people. It often causes
complications. The disease is most likely found in fertile active
places including, the armpits, hair, and scalp. The large pimples
that appear in those areas may cause the worst of the infection if
popped. This can lead to scaled skin syndrome. A severe form of
this is Ritter’s disease seen in neonates.
1.4. Toxic Shock Syndrome And Food Poisoning
Some strains of Staph. aureus, which produce the exotoxin TSST-
1, are the causative agents of toxic shock syndrome. Some strains
of Staph. aureus also produce an enterotoxin that is the causative
agent of Staph. aureus gastroenteritis. The gastroenteritis is self-
limiting, with the person recovering in 8-24 hours. Symptoms
include nausea, vomiting, diarrhea, and abdominal pain.
1.5. Mastitis In Cows
Staph. aureus is one of the causal agents of mastitis in dairy cows.
Its large polysaccharide capsule protects the organism from
recognition by the cow’s immune defenses [10].
1.6. Reproduction
Staph. aureus reproduces asexually. It starts this process by
reproducing its DNA. The membrane stretches out and separates
the DNA molecules. The cells from a hollow space that eventually
divides out into two new cells. The new cell wall does not fully
separate from the existing cell wall, which is why the cells are
Sample Copy. Not for Distribution.

Oral Carriage & Suffering of Staphylococcus Aureus
5
observed in clusters. This cell will eventually reproduce and cells
will attach onto it [11].
1.7. Virulence Factors
Toxins
Depending on the strains, Staph. aureus is capable of secreting
several toxins, which can be categorized into three groups. Many
of these toxins are associated with specific diseases.
Super antigens
PTSAgs have super antigen activities that induce toxic shock
syndrome (TSS). This group includes the toxin TSST-1, which
causes TSS associated with tampon use. The staphylococcal
enterotoxins, which cause a form of food poisoning, are included
in this group.
Exfoliative toxins
EF toxins are implicated in the disease staphylococcal scalded-skin
syndrome (SSSS), which occurs most commonly in infants and
young children. It also may occur as epidemics in hospital
nurseries. The protease activity of the exofoliative toxins causes
peeling of the skin observed with SSSS.
Other toxins
Staphylococcal toxins that act on cell membranes include alpha-
toxin, beta-toxin, delta-toxin, and several bicomponent toxins. The
bicomponent toxin Panton-Valentine leukocidin (PVL) is
associated with severe necrotizing pneumonia in children. The
genes encoding the components of PVL are encoded on a
bacteriophage found in community-associated methicillin-resistant
Staph. aureus (MRSA) strains.
Protein A
Protein A is a protein that is anchored to staphylococcal
peptidoglycan pentaglycine bridges (chains of five glycine
residues) by the transpeptidase Sortase A [12]. Protein A is an IgG-
binding protein that binds to the Fc region of an antibody. In fact,
Sample Copy. Not for Distribution.

Dr. Biswajit Batabyal
6
studies involving mutation of genes coding for protein A resulted
in a lowered virulence of S. aureus as measured by survival in
blood, which has led to speculation that Protein A contributed
virulence requires binding of antibody Fc regions[13]. Protein A in
various recombinant forms has been used for decades to bind and
purify a wide range of antibodies by immune affinity
chromatography. Transpeptidases such as the sortases that are
responsible foranchorning factors like Protein A to the
staphylococcal peptidoglycan are being studied in hopes of
developing new antibiotics to target MRSA infections [14].
1.8. Role Of Pigment In Virulence
Some strains of Staph. aureus are capable of producing
staphyloxanthin-a carotenoid pigment that acts as a virulence
factor. It has an antioxidant action that helps the microbe evade
death by reactive oxygen species used by the host immune system.
Staphyloxanthin is responsible for Staph. aureus characteristic
golden color [15]. When comparing a normal strain of Staph.
aureus with a strain modified to lack staphyloxanthin, the wild
type pigmented strain was more likely to survive incubation with
an oxidizing chemical such as hydrogen peroxide than the mutant
strain was. Colonies of the two strains were also exposed to human
neutrophils. The mutant colonies quickly succumbed while many
of the pigmented colonies survived. Wounds on mice were
inoculated with the two strains. The pigmented strains created
lingering abscesses. Wounds with the unpigmented strains healed
quickly.
These tests suggest that the staphyloxanthin may be key to the
ability of Staph. aureus to survive immune system stacks. Drugs
designed to inhibit the bacterium’s production of the
staphyloxanthin may weaken it and renew its susceptibility to
antibiotics [16]. In fact, because of similarities in the pathways for
biosynthesis of staphyloxanthin and human cholesterol, a drug
developed in the context of cholesterol-lowering therapy was
shown to block Staph. aureus pigmentation and disease
progression in a mouse infection model [17].
Sample Copy. Not for Distribution.
Oral Carriage & Suffering of Staphylococcus Aureus
7
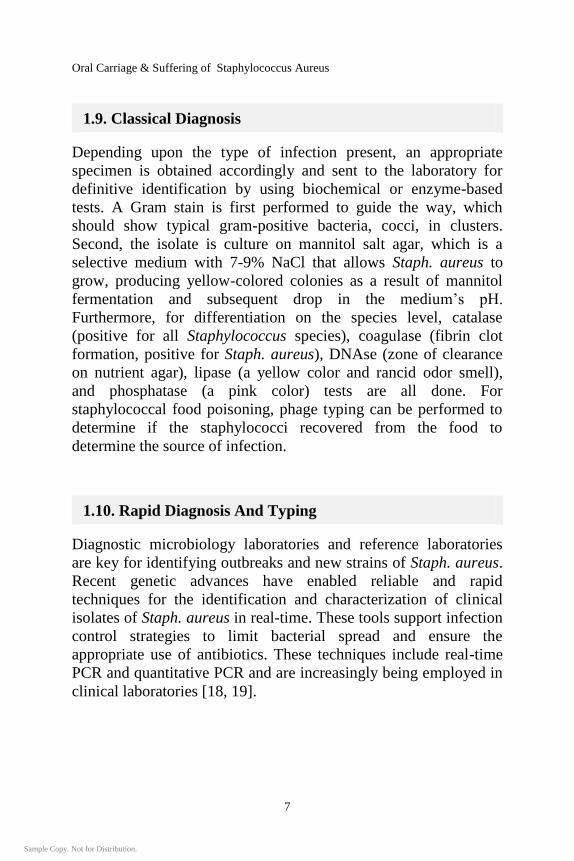
1.9. Classical Diagnosis
Depending upon the type of infection present, an appropriate
specimen is obtained accordingly and sent to the laboratory for
definitive identification by using biochemical or enzyme-based
tests. A Gram stain is first performed to guide the way, which
should show typical gram-positive bacteria, cocci, in clusters.
Second, the isolate is culture on mannitol salt agar, which is a
selective medium with 7-9% NaCl that allows Staph. aureus to
grow, producing yellow-colored colonies as a result of mannitol
fermentation and subsequent drop in the medium’s pH.
Furthermore, for differentiation on the species level, catalase
(positive for all Staphylococcus species), coagulase (fibrin clot
formation, positive for Staph. aureus), DNAse (zone of clearance
on nutrient agar), lipase (a yellow color and rancid odor smell),
and phosphatase (a pink color) tests are all done. For
staphylococcal food poisoning, phage typing can be performed to
determine if the staphylococci recovered from the food to
determine the source of infection.
1.10. Rapid Diagnosis And Typing
Diagnostic microbiology laboratories and reference laboratories
are key for identifying outbreaks and new strains of Staph. aureus.
Recent genetic advances have enabled reliable and rapid
techniques for the identification and characterization of clinical
isolates of Staph. aureus in real-time. These tools support infection
control strategies to limit bacterial spread and ensure the
appropriate use of antibiotics. These techniques include real-time
PCR and quantitative PCR and are increasingly being employed in
clinical laboratories [18, 19].
Sample Copy. Not for Distribution.

Dr. Biswajit Batabyal
8
1.11. Treatment And Antibiotic Resistance
The treatment of choice for Staph. aureus infection is penicillin;
but, in most countries, penicillin-resistance is extremely common
and first-line therapy is most commonly a penicillinase-resistant
beta-lactam antibiotic (for example, oxacillin or flucloxacillin).
Combination therapy with gentamicin may be used to treat serious
infections like endocarditis [20, 21], but its use is controversial
because of the high risk of damage to the kidneys [22]. The
duration of treatment depends on the site of infection and on
severity.
Antibiotic resistance in Staph. aureus was uncommon when
penicillin was first introduced in 1943. Indeed, the original petri
dish on which Alexander Fleming of Imperial College London
observed the antibacterial activity of the penicillium fungus was
growing a culture of Staph. aureus. By 1950, 40% of hospital
Staph. aureus isolates were penicillin-resistant; and, by 1960,this
had risen to 80% [23]. Researchers from Italy have identified a
bacteriophage active against Staphylococcus aureus, including
methicillin-resistant strains (MRSA), in mice and possibly humans
[24].
Methicillin-resistant Staphylococcus aureus (MRSA) is a
bacterium responsible for several difficult-to-treat infections in
humans. It is also called multidrug-resistant Staphylococcus aureus
and oxacillin-resistant Staphylococcus aureus (ORSA). MRSA is
any strain of Staphylococcus aureus that has developed resistance
to beta-lactam antibiotics, which include the penicillins
(methicillin, dicloxacillin, nafcillin, oxacillin, etc.) and the
cephalosporins. Strains unable to resist these antibiotics are
classified as methicillin-sensitive Staphylococcus aureus, or
MSSA. The development of such resistance does not cause the
organism to be more intrinsically virulent than strains of
Staphylococcus aureus that have no antibiotic resistance, but
resistance does make MRSA infection more difficult to treat with
standard types of antibiotics and thus more dangerous. MRSA is
especially troublesome in hospitals and nursing homes, where
patients with open wounds, invasive devices, and weakened
Sample Copy. Not for Distribution.

Oral Carriage & Suffering of Staphylococcus Aureus
9
immune systems are at greater risk of infection than the general
public.
1.12. Antibiotics
The word antibiotic [25] is derived from Greek stems that mean
“against life”. In 1889, the French researcher Paul Vuillemin
coined the term to describe a substance he isolated some years
earlier from Pseudomonas aeruginosa. The substance, called
pyocyanin, inhibits the growth of other bacteria in test tubes, but it
was too toxic to be useful in disease therapy. Vuillemin’s term has
survived to the current era. Antibiotics are now considered to be
chemical products or derivatives of microorganisms that are
inhibitory to other microorganisms.
Scientists
are uncertain as to how the ability to produce
antibiotics arose in living things, but it is conceivable that random
genetic mutations were responsible. Clearly, the ability to produce
an antibiotic conferred an extraordinary evolutionary advantage on
the processor in the struggle for survival. In this section we shall
discuss the sources of antibiotics-which are used in this study, their
modes of action, and side effects, and how they are used by
physicians to control infections disease.
1.13. Penicillin
Since the 1940s, Penicillin [25] has remained the most widely
used antibiotic because of its low cost and thousands of
derivatives. Penicillin G, or Benzyl penicillin, is currently the
most popular penicillin antibiotic and is usually the one intended
when doctor prescribe “Penicillin”. Other types are Penicillin F
and Penicillin V, all with the same basic structure of a beta-lactam
nucleus and several attached groups.
The Penicillins are active against a variety of Gram-positive
bacteria, including Staphylococci, Streptococci, Clostridia, and
Pneumococci. In higher concentrations, they are also inhibitory to
the Gram-negative diplococci that cause gonorrhea and
meningitis, and they are useful against syphilis spirochetes.
Sample Copy. Not for Distribution.

Dr. Biswajit Batabyal
10
Penicillin functions during the synthesis of the bacterial cell wall.
It blocks the cross-linking of carbohydrates in the peptidoglycan
layer during wall formation.
Antimicrobial Activity [26]:
The initial step in Penicillin action is binding of the drug to cell
receptors. These receptors are PBPs, at least some of which are
enzymes involved in transpeptidation reactions. From three to six
(or more) PBPs per cell can be present. After penicillin molecules
have attached to the receptors, peptidoglycan synthesis is
inhibited as final transpeptidation is blocked. A final
bacterialcidal event is the removal or inactivation of an inhibitor
of autolytic enzymes in the cell wall. This activates the autolytic
enzymes and results in cell lysis. Organisms with defective
autolysin function are inhibited but not killed by Beta-lactam
drugs, and they are said to be “tolerant”.
Since active cell wall synthesis is required for penicillin
action, metabolically inactive microorganisms are not susceptible.
Penicillin G and Penicillin V are often measured in unit (1 million
Units=0.6 gm), but the semi synthetic penicillins are measured in
grams. Whereas 0.002-1microgm/ml of Penicillin G is lethal for a
majority of susceptible gram positive organisms, 10-100 times
more is required to kill gram negative bacteria(except Neisseriae).
Resistance
Resistance to penicillins falls into several categories:
1. Production of Beta-lactamases by Staphylococci, gram
negative bacteria, haemophili, gonococci, and others. More
than 50 different Beta-lactamases are known, most of them
produced under the control of bacterial plasmids. Some Beta-
lactamases are inducible by the new cephalosporins.
2. Lack of penicillin receptors (PBPs) or altered PBPs (e.g.,
Pneumococci, enterococci) or inaccessibility of receptors
because of permeability barriers of bacterial outer membranes.
These are often under chromosomal control.
Sample Copy. Not for Distribution.

Oral Carriage & Suffering of Staphylococcus Aureus
11
Get Complete Book At Educreation Store
www.educreation.in
Sample Copy. Not for Distribution.

Sample Copy. Not for Distribution.