SAMHSA Primary and Behavioral Health Care Integration ... · Health Care Integration (PBHCI)...
30
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 3 Freddie Smith, MPH, Project Director Alameda County Behavioral Health Care Services Faith Elizabeth Fuller, MBA, Project Evaluator ILC Meeting #41 February 25, 2015 1
Transcript of SAMHSA Primary and Behavioral Health Care Integration ... · Health Care Integration (PBHCI)...
SAMHSA Primary and Behavioral Health Care Integration (PBHCI)
Program Grantees: Part 3
Freddie Smith, MPH, Project Director Alameda County Behavioral Health Care Services
Faith Elizabeth Fuller, MBA, Project Evaluator
ILC Meeting #41 February 25, 2015
1
Housekeeping This webinar is being recorded.
Feel free to type questions into the chat box at any time during the presentation.
Questions will also be taken via phone at the end of the presentation.
During this Q&A session, please mute your phone line by pressing *6. You can un-mute yourself for questions by pressing *7.
2
SAMHSA PBHCI Program
SAMHSA’s Primary and Behavioral Health Care Integration program (PBHCI) provides federal grant funding to promote the integration of primary care services for adults with serious mental illness (SMI) into community-based behavioral health settings, to increase access to care and improve consumer health through better coordination of care.
http://www.integration.samhsa.gov/pbhci-learning-community
3
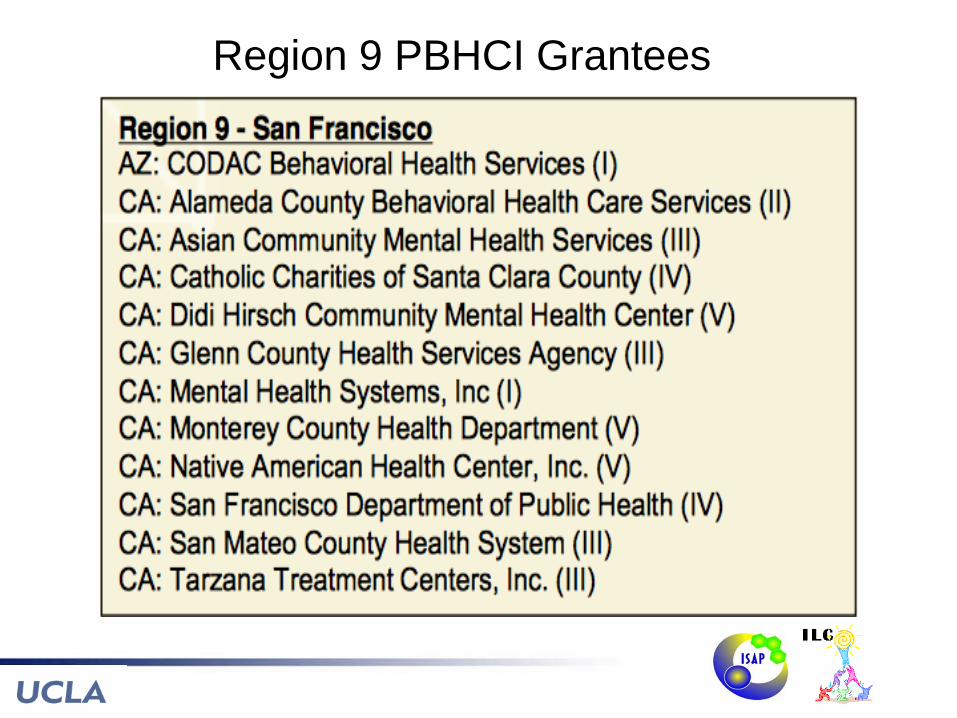
Region 9 PBHCI Grantees

Poll Question
We are/I am: 1. A current PBHCI grantee 2. Applying for a PBHCI grant Feb 2015 3. Exploring PBHCI funding for 2016 4. Not applicable, or none of the above
5
PATH Project (Promoting Access to Health)
)
SAMHSA/PBHCI Cohort 2 Alameda County Behavioral Health Care
Services, Northern California Manuel Jimenez, Director
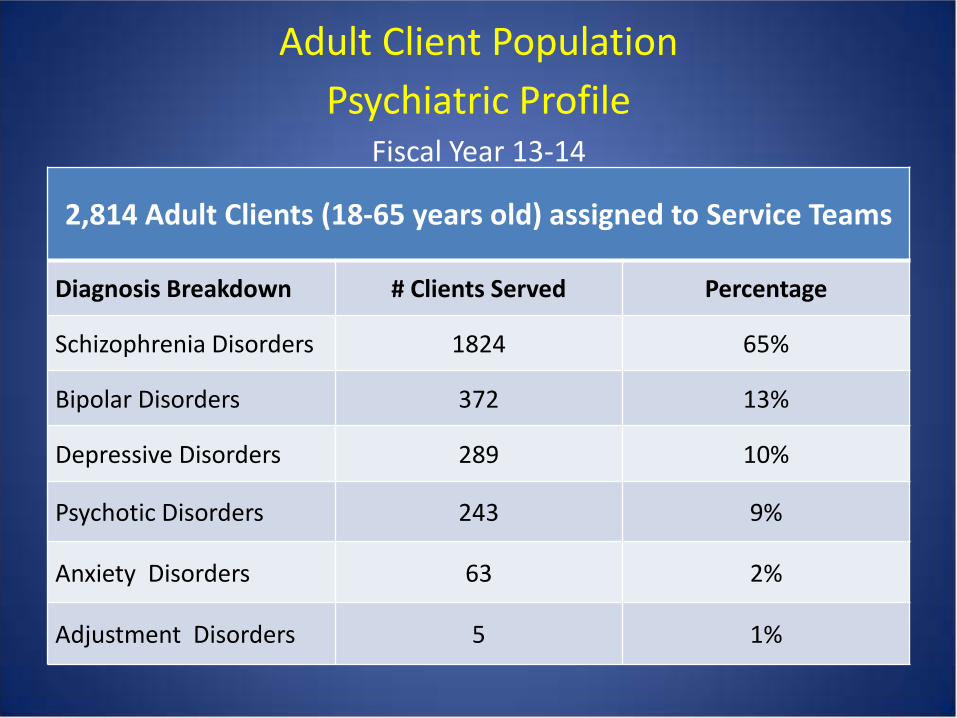
Adult Client Population Psychiatric Profile
Fiscal Year 13-14
2,814 Adult Clients (18-65 years old) assigned to Service Teams
Diagnosis Breakdown # Clients Served Percentage
Schizophrenia Disorders 1824 65%
Bipolar Disorders 372 13%
Depressive Disorders 289 10%
Psychotic Disorders 243 9%
Anxiety Disorders 63 2%
Adjustment Disorders 5 1%

Health Characteristics of BH Clients served by Service Teams
1. 228% more likely to be diagnosed with diabetes
2. 62% more likely to be diagnosed with hypertension
3. 61% more likely to be diagnosed with asthma
4. 53% more likely to be diagnosed with heart disease
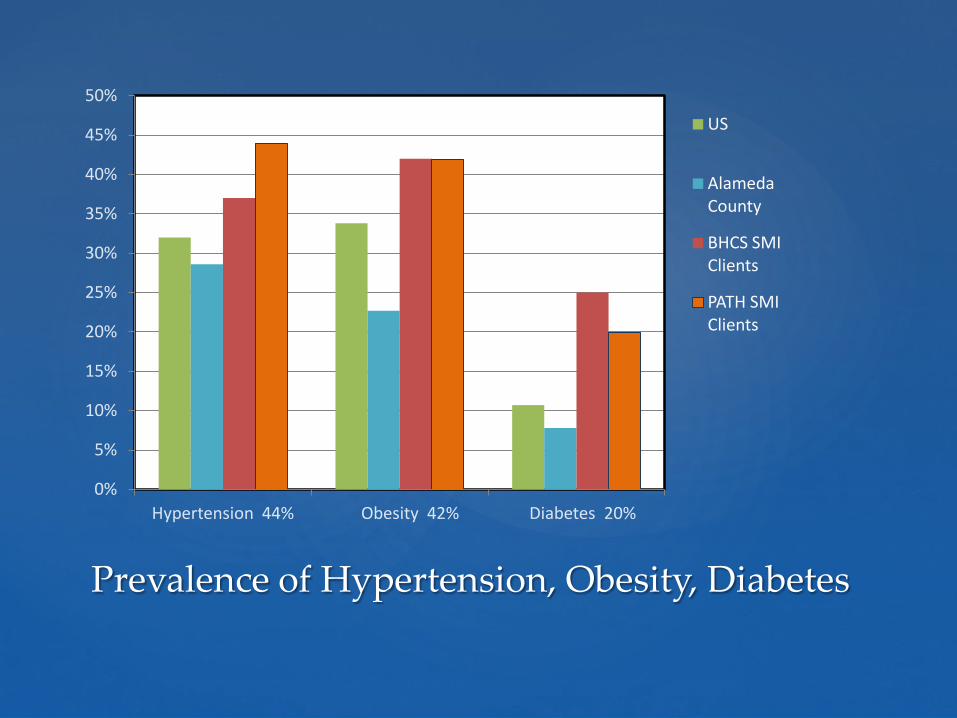
Prevalence of Hypertension, Obesity, Diabetes
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Hypertension 44% Obesity 42% Diabetes 20%
US
Alameda County
BHCS SMI Clients
PATH SMI Clients

Federally Qualified Health Center(s) co-locate a satellite primary care clinic
in a county-operated mental health center. The site becomes the “Medical Home” for seriously mentally ill
adults in the county’s Adult System of Care. Oakland, CA Fremont, CA
LIFELONG MEDICAL CARE:
“Safety net” primary care provider since 1976 for uninsured residents with complex health needs in Berkeley, Oakland, Albany, and Emeryville, California
TRI-CITY HEALTH CENTER:
“Safety net” primary care provider since 1970 for uninsured and under-served residents in Fremont and Union City, California
September 2011: LifeLong Medical Care PATH Clinic opens at the Oakland Adult Community Support Center (200 participants)
August 2012: Tri-City Health Center PATH clinic opens at the Tri-City Adult Community Support Center / Fremont (50 participants)
Goals of PATH Project
1. Improve Access to primary care services for SMI clients
2. Create a “Medical Home” for SMI clients served in County Mental Health Centers, with the goal of improving health outcomes 3. Develop a “Sustainable Financial Model” to expand PATH Clinics and integrated care to additional Centers
A PATH Clinical Team
From the FQHC: • Primary Care Providers
(Physicians or NP’s) .4 FTE • Medical Assistant .5 FTE • Clinic Coordinator 1 FTE
manages clinic operations • Care Assistant 1 FTE
coordinates appointments, schedules, and enters patient information into health information systems
From the Mental Health Center: • BHCS Psychiatrists provide
consultation to primary care providers as needed
• Nurse Care Coordinator 1 FTE • Peer Support Counselor 1 FTE
facilitates wellness activities, assists with care coordination
• Case Managers assist getting clients to appointments and referrals to specialty care

• Average visit with the Primary Care Provider takes 30 minutes (after relationship is established)
• Care Assistant makes reminder calls & covers “no shows” with walk-ins
• Peer Support helps clients get to their appointments, interprets, plans wellness activities
• The Team meets at the end of each half -day clinic for a 30 minute “debrief” to discuss care for each client seen that day
• Nurse coordinates referrals and follow ups, medication refills, blood draws, triage
How the PATH Clinic Works

Health and Wellness Activities Led by peers or student interns, provide socialization, education, engagement,
inclusion; a colorful calendar is posted monthly on the bulletin board
Community Connections, field trips to farmer’s markets, bowling, movies
Cooking Class, teaching nutrition, self sufficiency, healthy eating (free lunch!)
Living Well Class, participants set health goals based on Whole Health Action
Management plan (WHAM) developed by SAMHSA-HRSA
Tobacco Cessation, group and one-on-one coaching (“Bye Bye Butts”)
Meditation/ Movement, yoga, walking, for exercise, stress reduction (“Fun and Games”
and “Feel Good Fridays”)
Lunch and Learns, medical staff present a topic and answer questions
The PATH Café for socialization and relaxation for clients to use before or after receiving
primary care or wellness services
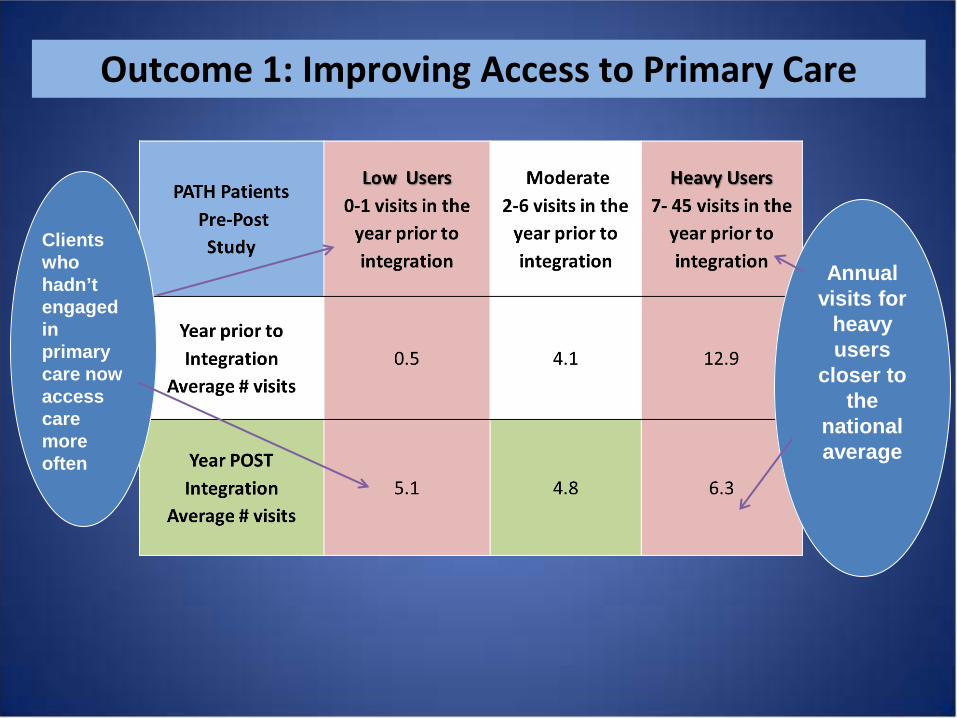
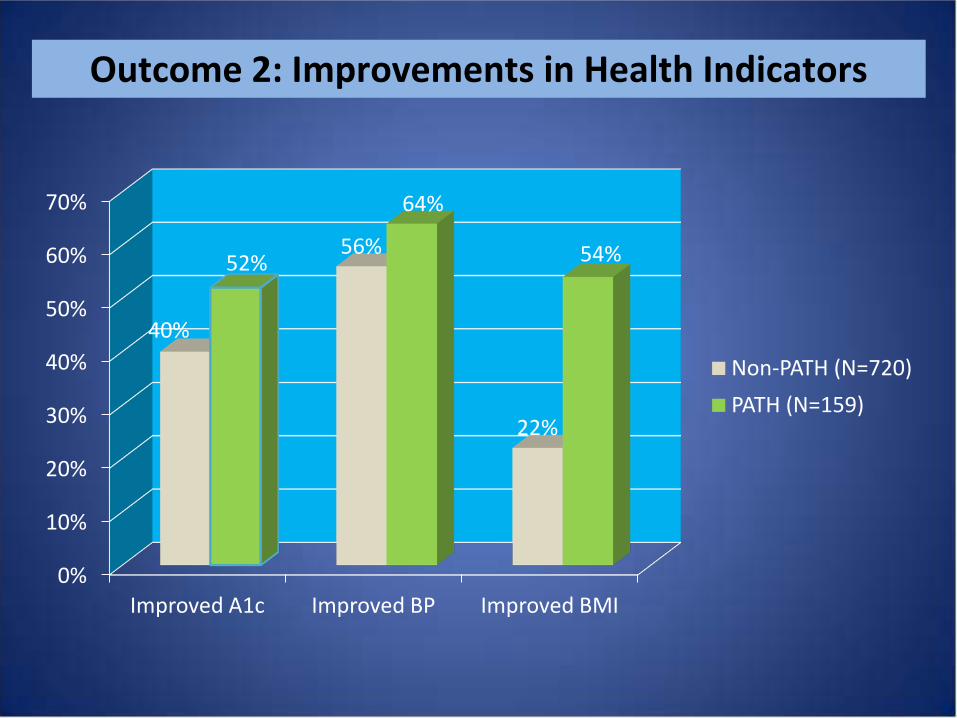
Outcome 1: Improving Access to Primary Care
Clients who hadn’t engaged in primary care now access care more often
Annual visits for
heavy users
closer to the
national average
0%
10%
20%
30%
40%
50%
60%
70%
Improved A1c Improved BP Improved BMI
40%
56%
22%
52%
64%
54%
Non-PATH (N=720) PATH (N=159)
Outcome 2: Improvements in Health Indicators
1. Plan to document outcomes for charts, graphs, presentations, and grant applications and proposals 2. Prepare a Financial Plan and Service Model to show how implementation and operating costs can be covered 3. Develop strong collaborative Partnerships with primary care partners (data sharing, transparency, for a win-win) 4. Build Support from BH Executive Staff, elected officials, and community and consumer groups
Outcome 3: Sustainability Focus
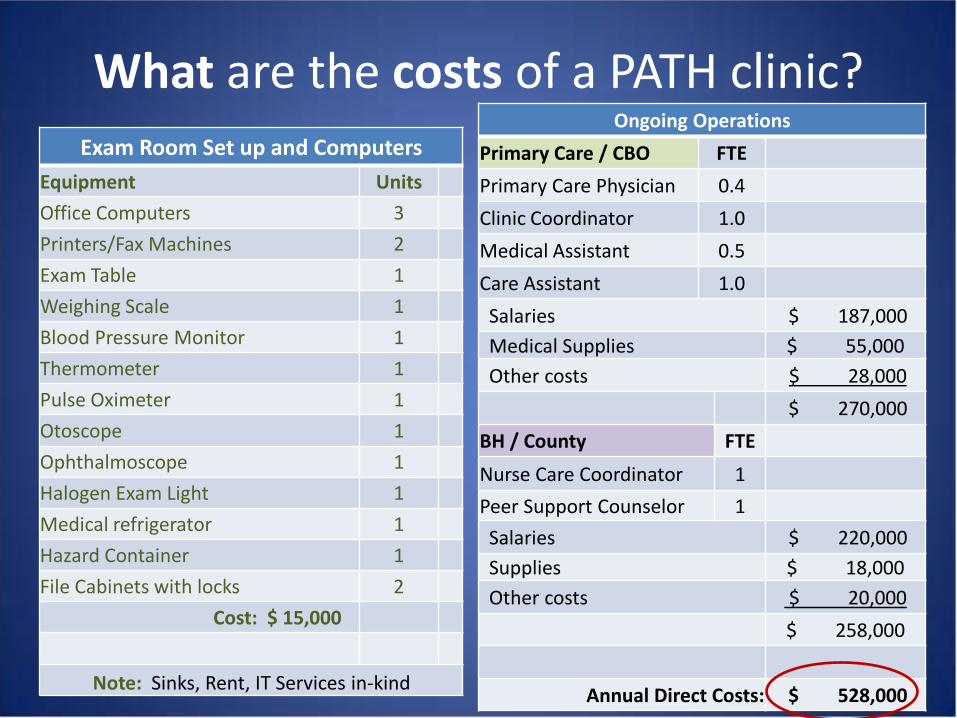
What are the costs of a PATH clinic? Ongoing Operations
Primary Care / CBO FTE Primary Care Physician 0.4 Clinic Coordinator 1.0 Medical Assistant 0.5 Care Assistant 1.0 Salaries $ 187,000 Medical Supplies $ 55,000 Other costs $ 28,000
$ 270,000 BH / County FTE Nurse Care Coordinator 1 Peer Support Counselor 1 Salaries $ 220,000 Supplies $ 18,000 Other costs $ 20,000
$ 258,000
Annual Direct Costs: $ 528,000
Exam Room Set up and Computers Equipment Units Office Computers 3 Printers/Fax Machines 2 Exam Table 1 Weighing Scale 1 Blood Pressure Monitor 1 Thermometer 1 Pulse Oximeter 1 Otoscope 1 Ophthalmoscope 1 Halogen Exam Light 1 Medical refrigerator 1 Hazard Container 1 File Cabinets with locks 2 Cost: $ 15,000
Note: Sinks, Rent, IT Services in-kind
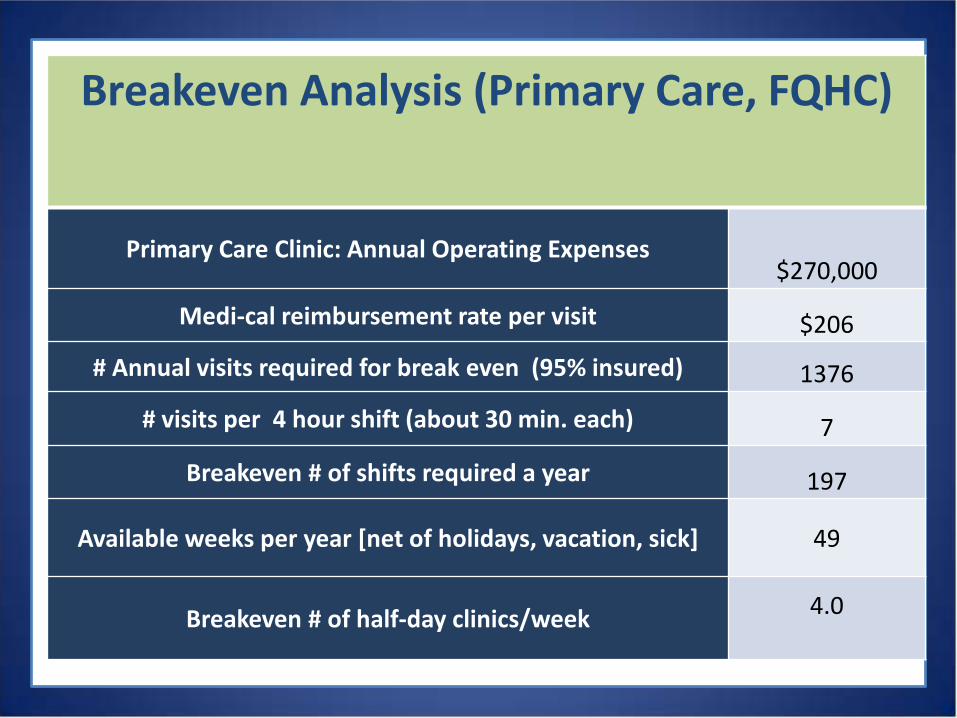
Breakeven Analysis (Primary Care, FQHC)
Primary Care Clinic: Annual Operating Expenses $270,000
Medi-cal reimbursement rate per visit $206
# Annual visits required for break even (95% insured) 1376
# visits per 4 hour shift (about 30 min. each) 7
Breakeven # of shifts required a year 197
Available weeks per year [net of holidays, vacation, sick] 49
Breakeven # of half-day clinics/week 4.0

Can BH find ways to Cover Costs? Setting up MAA and TCM billing to help cover operating costs of approx.
$250,000 a year per clinic (200 participants) County Leadership approved allocation of California Mental Health
Services Act funds to sustain PATH and expand to 2 new sites San Francisco Foundation grant for sustainability planning and data
analysis Tobacco Cessation grants (MHSA) Blue Shield Foundation grant to improve county-wide interagency data
sharing USC/Cal State University Schools of Social Work Integrated Health Interns
(in-kind donation of services) UC Berkeley collaborative proposal to NIMH for SMI sleep improvement
study begins next month

Challenges For the organizations: • The bureaucratic processes (everything takes time); hiring, purchasing,
MOU’s • Primary Care has “productivity” targets (different from BH) • Getting “billing” up and running on the Behavioral Health side • Challenges in data sharing, 3 systems that don’t talk to each other, and
getting data for comparison groups .. And we have all of these reassessment interviews! For the consumers: • Staff changes can be upsetting • Substance use can affect engagement and compliance • Challenges with transportation; limited access to healthy food • Some consumers prefer one-on-one and do not like group activities

Tips (Clinical Team)
Schedule a team “de-brief” after each clinic day to share information and problem solve (improves care coordination and helps build relationships)
Convene “Lunch and Learns” so providers can introduce themselves to consumers, present different health topics, and encourage discussion (consumers feel less isolated)
Orient consumers on “how to be an effective patient” Get Peers involved early on, to help design service delivery,
communication, and educational materials that makes sense to your consumers
Tips (Data and Outreach) Work with your Evaluator and clinical team to plan what data to
collect, when, how, and why. Measure blood pressure, weight, breath CO, blood sugar, cholesterol
levels (for example). Track number of primary care visits, before and after integration. Make charts and graphs for a “data wall” and disseminate your
successes widely; integration is a hot topic! A weekly cooking class attracted participants, as did outings and
events, and created a “culture” of wellness The “PATH Café” created a welcoming, colorful environment Consumers contributed artwork, provided input into outreach
materials and a colorful monthly calendar

Annual Visioning Retreats Ask Stakeholders “IS IT WORKING?” TOPIC: “Strategies for improvement” • Health Education/Wellness Activities • Recruitment/Enrollment/Outreach • Clinic Operations and Communication • Information Sharing and Data Utilization
Consumers, PATH Staff & Family Members

Collaborative Leadership
Take ownership of your partner’s measures of success
Build trusting, dependable working relationships with all project staff
Always be willing to listen, and help solve issues that might impact the collaboration
Be willing to think “outside the box”
Goals for the Future Open primary care clinics at additional MH sites
Integrate Substance Abuse Treatment
Continue to collect and analyze data to identify the benefits of integration / added value to the system, i.e. measure impacts on Emergency Room visits Hospitalizations (psychiatric and medical) Criminal Justice System Contacts Cost savings to the public health care system
QUESTION & ANSWER
28
Reminder: Please mute your phone line by pressing *6. You may ask a question by pressing *7 on your phone to un-mute yourself.

CONTACT
Freddie Smith, Alameda County BHCS [email protected]
Faith Elizabeth Fuller, FAS Services
29

For more information on the ILC…
Meeting Summaries http://uclaisap.org/integration/html/learning-collaborative/ Archived Recordings http://vimeo.com/channels/ilcintegration Mailing List http://lists.ucla.edu/cgi-bin/mailman/listinfo/ilc E-mail [email protected] with additional questions!
30