SAÚDE NA FAMÍLIA - South-East Asia Regional Office the domiciliary visits under the “Programa...
102
1 Saúde na Família SAÚDE NA FAMÍLIA Part of Comprehensive Primary Healthcare Package Success stories from the field INDONESIA
Transcript of SAÚDE NA FAMÍLIA - South-East Asia Regional Office the domiciliary visits under the “Programa...

1
Saúd
e na
Fam
ília
SAÚDE NA FAMÍLIAPart of Comprehensive PrimaryHealthcare Package
Success stories from the fieldINDONESIA




INDONESIA
SAÚDE NA FAMÍLIAPart of Comprehensive PrimaryHealthcare Package
Success stories from the field

A Programme of Ministry of Health,Democratic Republic of Timor-Leste
Programme FacilitatorMr Pedro Canisio da Costa Amaral, SKM, National Director, Public HealthDr Noel Gama Soares, National Coordinator for Saúde na FamíliaDr Marcelo Amaral Mali, Regional Coordinator for Saúde na FamíliaDr Carlos José Lay Guterres, Regional Coordinator for Saúde na FamíliaDr Adelia M.M Barreto, Regional Coordinator for Saúde na FamíliaDr Ramila F.P. Paiva, Regional Coordinator for Saúde na FamíliaDr Josefina Clarinha João, Regional Coordinator for Saúde na FamíliaMs Norberta Belo, Public Health Advisor
Design Concept byShobhan and Seday Ganefabra
Designed atseday design
Photos byShobhan
The printing of this book is supported by the World Health Organisation (WHO) Country Office for Timor-Leste as part of the European Union (EU) - Luxembourg - WHO Universal Health Coverage Partnership in Timor-Leste.

SAÚDE NA FAMÍLIAPart of Comprehensive PrimaryHealthcare Package
Success Stories from the field

8

9
Saúd
e na
Fam
íliaContent
i Foreword
vii Introduction
01 Aileu
05 Ainaro
11 Baucau
15 Bobonaro
23 Covalima
27 Dili
33 Ermera
39 Lautem
43 Liquiça
49 Manatuto
63 Manufahi
69 Oecusse
75 Viqueque
i
Fore
wor
d
The Government of the Democratic Republic of Timor-Leste is committed to fulfil the right to free universal health care of its People through a decentralized public health care system as enshrined in the Constitution. As part of this commitment much of the health infrastructure destroyed in the wake of the 1999 independence vote was rebuilt, new health care facilities have been put in place, and health care workers were being deployed throughout the country to provide primary and hospital care to the communities.
The launching of “Programa Nasional Saúde na Família” on 22nd July 2015 has galvanized the continuing efforts to provide free universal health care to the people of Timor-Leste. Modelled on the Cuban primary health-care system, this program is designed to bring a “Comprehensive Service Package of Primary Health Care” to the household level through domiciliary visits, clinical consultation, treatment and referrals by team of health professionals, as well as recording the household’s and each of its member’s clinical profiles, which are then being entered into an integrated digitalized medical record system.
First and foremost, this programme is a testament to the universal values and principles of equality and justice, and underscores the responsibility of the government to guarantee health care for all its citizens. Secondly it recognizes that primary health care is the best strategy to achieve health for all, and is the foundation for health system strengthening through provision of quality and comprehensive health care in a cost-effective and equitable manner. And lastly it is in line with the spirit of the Sustainable Development Goals of “leaving no one behind” by reaching out to a large number of people who are still being ‘left behind’ in Timor-Leste in terms of access to health care.

The cases documented in this book underline the need and the benefits of this programme. There is no doubt that many of these cases would have never come to light had it not been for the domiciliary visits under the “Programa Nasional Saude na Familia” and that it will prevent such cases recurring in the future.
I congratulate the Ministry of Health for implementing the programme and appreciate the efforts of all the health professionals of this country without whose commitment and dedication this program would not become a reality. I also would like to thank the World Health Organization and UNICEF for their continued commitment to support locally identified and locally owned strategies to achieve health for all in Timor-Leste.
Dr Rui Maria de AraújoPrime Minister,Democratic Republic of Timor-Leste
ii
Saúd
e na
Fam
ília

iii
Fore
wor
d
The Government of Timor-Leste has taken another step forward to reaffirm its commitment to active improvement of access and quality of health care services to all Timorese people, by introducing Programa Nacional Saúde na Família.
Programa Saúde na Família is a new approach to health services delivery embraced by the Ministry of Health’s Comprehensive Packages of Primary Health Care Services, which was launched in April 2015, with the objective of delivering family health care services to each family member throughout Timor-Leste.
The implementation of Programa Saúde na Família consists of two (2) stages of home visits in the form of “Dispensarization” as well as in the form of Regular Home Visits, as to fully identify family health profiles, environmental and other social determinant factors affecting the health conditions of each family, in order to allow for appropriate direct and indirect interventions that can best respond to the needs of each family member.
In its first year of implementation, Saúde na Família is already showing its intended purpose by bridging existing gaps between the health professionals and the people they intend to care for. In this regard, dedicated health professionals testify their experience in rolling-out this important programme amidst high expectations.
Now, I think it is a suitable time to pause for a moment and take a look back on the stumbling stones and challenges we have experienced together in order to move forward and celebrate the milestones we have achieved so far.
I truly hope this book serves not only as an inspiring collection of real experiences through the journey of implementing Saúde na Família, but also as a reminder of the potential benefits of Saúde na Família to help reduce the morbidity and mortality rates among children and pregnant mothers, increase immunization coverage, improve malnutrition

iv
Saúd
e na
Fam
ília
rates, reduce communicable diseases as well as prevent the social and economic risks associated with non-communicable diseases, in order to improve the health status of the Timorese people.
I thank the Honorable Prime Minister, Dr. Rui Maria de Araújo, for supporting this important policy initiative towards for a stronger National Healthcare System in Timor-Leste.
I also would like to extend my sincere gratitude to “Brigada Medica Cubana” for the assisting the Ministry of Health in developing Programa Saúde na Família, and to Sra. Maria Diaz, from Clinica Prontu Atu Servi (PAS), for facilitating and implementing the Dispensarization model in the area of Remarik, Becori.
Lastly, but not least, my sincere appreciation goes to WHO and UNICEF for their support to the Ministry of Health and in help making Programa Saúde na Família a reality.
Dr. Maria do Céu Sarmento Pina da CostaMinister of Health,Democratic Republic of Timor-Leste

v
Fore
wor
d
The Constitution of the Democratic Republic of Timor-Leste protects the right to health, medical care and a healthy environment. According to Article 57 of the constitution the State has the responsibility to provide free universal health care through a decentralized public health care system. In accordance with the Constitutional provision, public health care is provided free of charge to all citizens of the country.
Since the restoration of independence in 2002, all successive Governments of Timor-Leste have been committed to providing universal health care. The launching of the Comprehensive Service Package for Primary Health Care which includes “Saúde na Família” in 2015 constitutes an important milestone to strengthen the primary health care services at the community level through domiciliary visits by health professional teams. This is also in line with the Sustainable Development Goal 3: “Ensure healthy lives and promote well-being for all at all ages.” By taking primary health care directly to the people and identifying those requiring follow-up care, the “Saúde na Família” Programme aims to overcome barriers of access to health care especially for the vulnerable, poor, marginalized, and disabled.
This book documents a few stories from the first year of the implementation of the Programme. These offer hope that although in its nascent stages, “Saúde na Família”, once fully implemented, should have a significant impact on reducing maternal and child mortality, getting people with communicable and non-communicable diseases on to treatment, and improving the overall health status of the population.
We reiterate our commitment to support the Ministry of Health in every step towards achieving the vision of “Healthy Timorese in Healthy Timor-Leste”.
Dr Rajesh Pandav Desiree JongsmaWHO Representative, UNICEF Representative,Timor-Leste Timor-Leste


n July 22, 2015 H.E Prime Minister and the head of the VI Constitutional Government of
Democratic Republic of Timor-Leste, Dr Rui Maria de Araujo launched the ‘Health in the Family’ programme called Saúde na Família, the comprehensive package of primary healthcare. The implementation of the programme began in July 2015, in the municipality of Dili and it continues throughout the other 11 municipalities and the autonomous region of Oecusse-Ambeno. As per the 2015 national census there are 206,483 households in Timor-Leste and 2,225 villages (aldeias). Saúde na Família programme is meant to ensure that each of these households are visited by a dedicated team of healthcare professionals.
An integrated medical team including a doctor, a midwife, and a nurse conduct the domiciliary visits. The advantage of this programme is that it brings services close to the families and communities living in the rural areas, promote and educate individuals, families and communities and to better understand their condition and enhance their access to health, to information for early prevention.
The programme adheres to the five fundamental principles of primary healthcare, (a) universal: all populations will have access to, and actively participate
OIntroduction
viii
Saúd
e na
Fam
ília
in primary healthcare activities from health promotion, disease prevention, early diagnosis, early treatment and rehabilitation using standard and scientific practices for the individual, family and the community; (b) basic right: everyone has the same right for health care and should be guaranteed health services of good quality;(c) equity: everyone will receive health care according to their necessity; (d) integrated: to take into account bio-physio-social perspectives, regarding the health problems and in the delivery of healthcare with assurance good quality; (e) continuity: to provide continuing health care for everyone in all levels of health facilities over the long term and in accordance with the needs of the individuals and the community.
The programme requires a sizeable human resource and expertise. Even though the country’s infrastructure was in the ruins when the independence was restored in 2002 but it rose from the ashes admirably. In the rebuilding of the healthcare system particularly international and non-governmental organizations played a supportive and important role. The Cuban Medical Brigade has been one of the cornerstones in strengthening the health systems in Timor-Leste. The World Health Organisation, UNICEF and other health development partners have played a vital role. In the context of Saúde na Família, World Health Organization support provided basic equipment that contributed to the successful implementation of the programme.

ix
Intr
oduc
tion

x
Saúd
e na
Fam
ília
On July 22, 2015 H.E. Prime Minister, Dr Rui Maria de Ara’ujo launched the Sa’ude na Fam’ilia programme in presence of several national and international health development partners.

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
INDONESIA
48554
4
26
46
37
26
3731
Aileu

2
Saúd
e na
Fam
ília
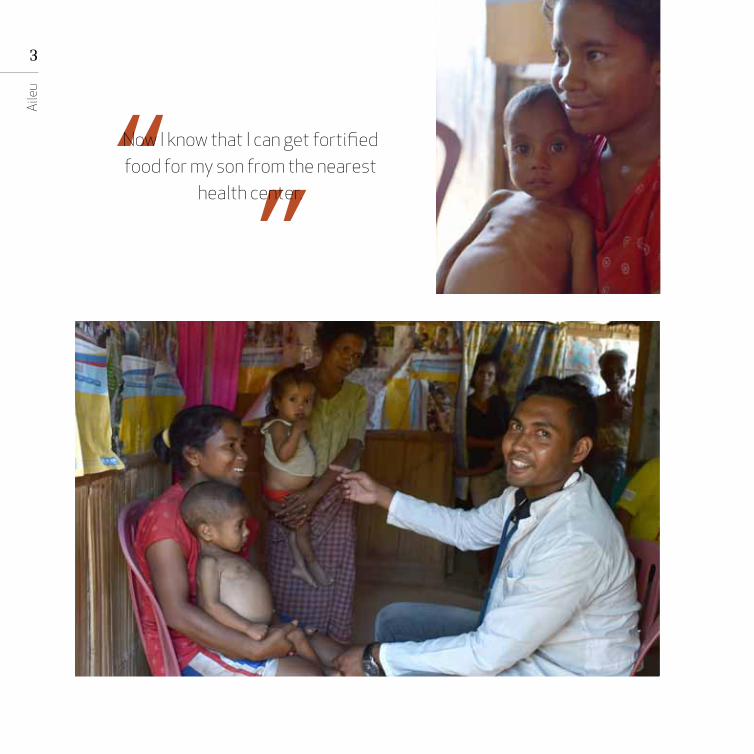
orentina Amaral’s house is atop a hill, where the 21-year-old lives with her husband, three children, and
extended family. The home isn’t easy to reach by car; the best and safest way is to walk, as the locals will tell you. Two of Amaral’s children are as healthy as any parent could hope for. But the third — Interfenia da Costa, now three-years old— had health issues she couldn’t understand. Or at least not until a doctor, nurse and midwife came calling at her house as a part of the Saúde na Família programme’s domiciliary visit. Amaral says, “My third son was born healthy. He weighed a good 3 kg at birth. But the problems started when he was six months old. He developed fever and diarrhea-like symptoms. We tried some treatment that seemed best to our mind, but his condition didn’t improve. When he turned one, his stomach started to bloat. Since then it hasn’t gone down. I didn’t know what to make of it till the doctor and a team came home in July this year. They explained to me that Interfenia is malnourished and that’s why his growth is hampered and stomach bloated. At least, I know the problem now. They explained to me the things I need to be careful about, and I know that I can get fortified food for my son from the nearest health center.”
L
3
Aile
u
Now I know that I can get fortified food for my son from the nearest
health center.

4
Saúd
e na
Fam
ília
Saúde na Família programme is immensely gratifying as a doctor.
It allows me an opportunity to make some kind of medical intervention for cases which otherwise would have never been identified. People in the rural community do not seek healthcare services proactively because of lack of awareness and the reluctance to visit a health center. It is also because of the long distance sometimes.
Dr Estanislau Amaral,Faturasa Health Post, Aileu
Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
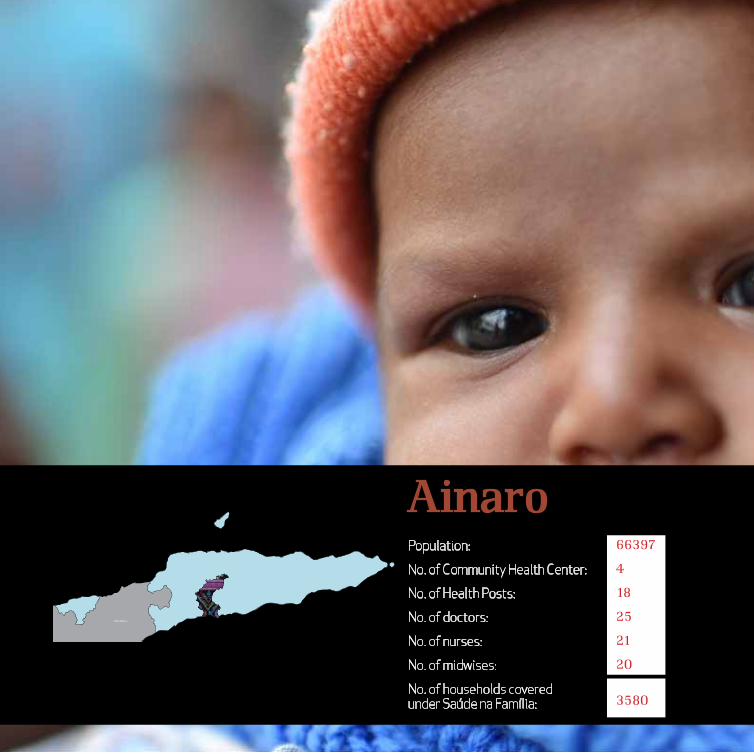
66397
4
18
25
21
20
3580
INDONESIA
Ainaro

6
Saúd
e na
Fam
ília
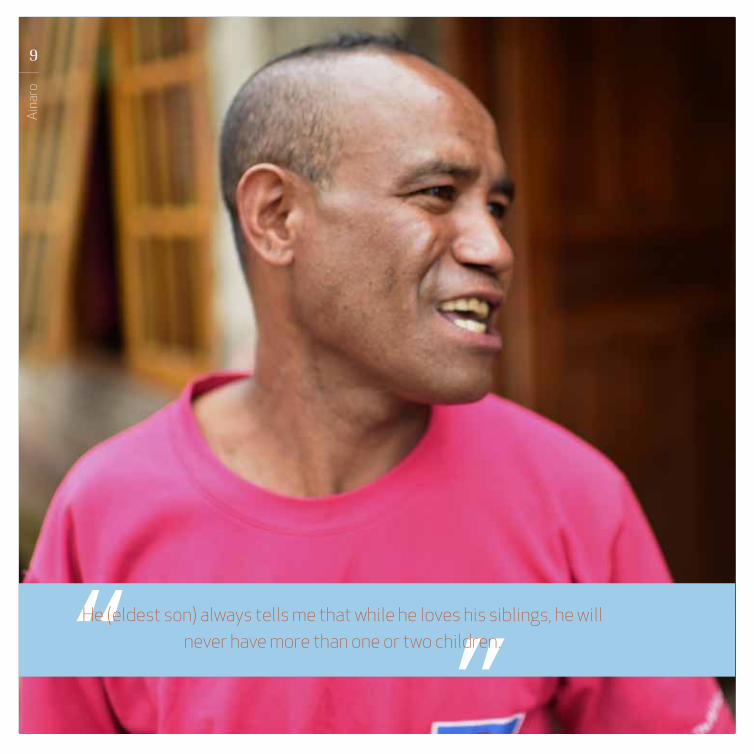
arlos Pereira Tilman, 42, and Nepolina da S. Conscesan, 31, along with their eight children, make
for one, big, happy family. But unfortunately, two babies were lost during childbirth. The couple doesn’t intend to have any more children; albeit a little late, they have understood the importance of family planning. Their eldest son’s resolve has had some bearing on the couple’s decision. Tilman says, “He (eldest son) always tells me that while he loves his siblings, he will never have more than one or two children.” Encouragingly, their youngest child was delivered by a nurse from the nearest Community Health Center (CHC). In addition to visits by the healthcare providers, the family also accesses the health posts and the monthly mobile health clinic, SISCa, in their neighbourhood.
C

7
Aina
ro
8
Saúd
e na
Fam
ília
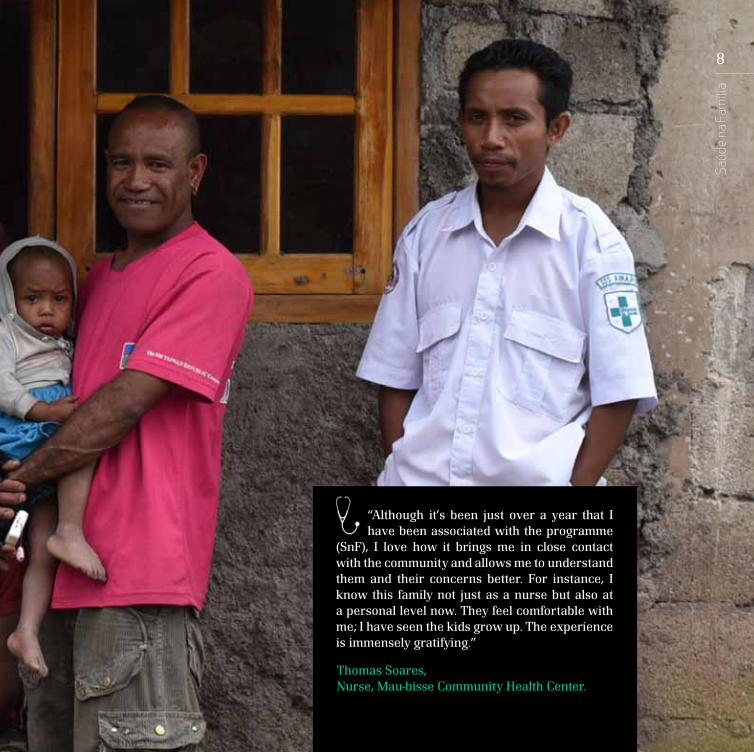
“Although it’s been just over a year that I have been associated with the programme
(SnF), I love how it brings me in close contact with the community and allows me to understand them and their concerns better. For instance, I know this family not just as a nurse but also at a personal level now. They feel comfortable with me; I have seen the kids grow up. The experience is immensely gratifying.”
Thomas Soares,Nurse, Mau-bisse Community Health Center.
9
Aina
ro
He (eldest son) always tells me that while he loves his siblings, he will never have more than one or two children.

10
Saúd
e na
Fam
ília
Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
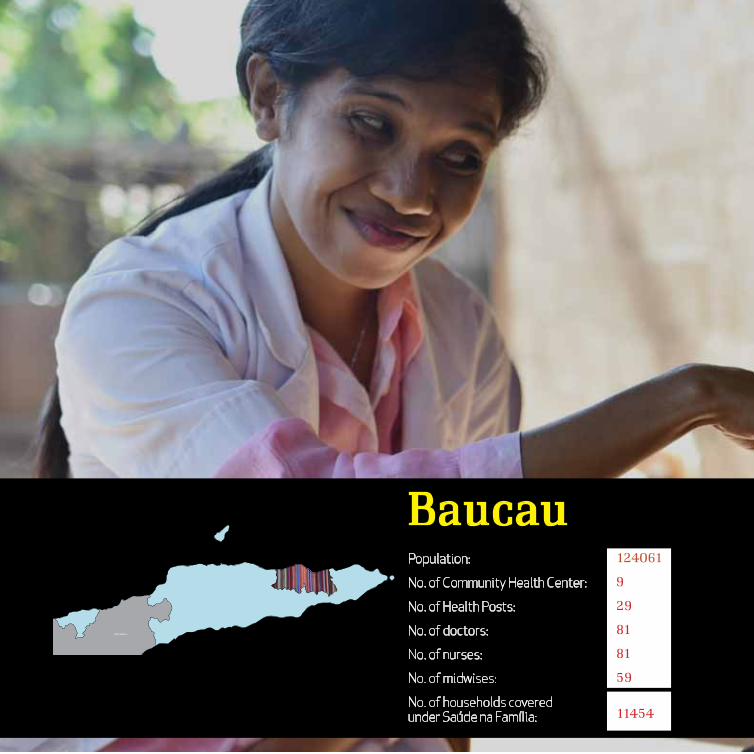
124061
9
29
81
81
59
11454
INDONESIA
Baucau

12
Saúd
e na
Fam
ília
elsia Bonita Fatima, all of three years and eight months, will charm you the moment you see her. But
if you look carefully, you will notice that the beautiful toddler has Down syndrome — a condition that was largely undiagnosed when her parents started frequenting clinics after Nelsia’s health turned delicate when she was just four months old. Nelsia’s parents — Domingus Bonita, 38, and Terezina Fatima, 32 — are relatively affording but it was of little help. It was in July 2016 that a team of healthcare workers visited their house. “They counselled us and explained at length what the problem with my child is,” says Terezina. “I do appreciate this idea – healthcare workers coming to the house, who wouldn’t? It’s one thing less to worry about. It is reassuring.”
N

13
Bauc
au
Dr Augusta da Costa,Bucoli, Baucau Community Health Center
“Ever since I have been associated with this programme, I have learnt
so much more about the problems that the communities in rural areas face. I have a better understanding of our people, their problems and their needs. It is also an opportunity to bring change, at least in a small way, by helping people in leading a healthier life.”

14
Saúd
e na
Fam
ília
They counselled us and explained at length what the problem with my child is. I do appreciate this idea –
healthcare workers coming to the house, who wouldn’t? It’s one thing less to worry about. It is reassuring.

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households covered
under Saúde na Família:
98932
6
21
46
37
26
12490
INDONESIAONESIA
Bobonaro

16
Saúd
e na
Fam
ília
aria da Silva’s third child, Jacques, was born perfectly healthy. He stayed
that way till he was five months old. Then, Maria, 40, noticed that he wasn’t growing like his other siblings. Maia and Manuel Talo, 41 (Jacques’ father), started frequenting clinics. “We were given medicine and sent back. His condition would improve only temporarily but I could see that my son wasn’t growing like his other two siblings. We went back again but doctors said there’s nothing wrong with him. Tests also revealed nothing except that he had malaria for which he was treated. We stopped seeing doctors thereafter.”
Jacques had developed certain undiagnosed complications following malaria that impacted his growth almost irreversibly. “When the doctors came home and recorded our family’s health details, it was then that my son’s condition was explained to me at length. At least, now I know what happened. It brought a sense of closure. The doctors also informed me what kind of care my son will require going forward. While it remains to be seen whether or not his condition will improve, but now I know what I can do for my son,” says Maria. Jacques has been referred to the nutrition centre in the district and also receives free nutrition support every month.
M

17
“The programme gives us an opportunity to establish direct
contact with the families. The most noble aspect of the domiciliary visit is that it strengthens the chances of reaching every Timorese — truly capable of attaining the idea of reaching the unreachable.
Dr Mateus Cardoso, Atabae, Bobonaro Community Health Center
Bobo
naro

18
Saúd
e na
Fam
ília
Dr Mateus Cardoso, Atabae, Bobonaro Community Health Center
When the doctors came home andrecorded our family’s health details, itwas then that my son’s condition was
explained to me at length. At least,now I know what happened. It brought
a sense of closure. The doctors alsoinformed me what kind of care my son
will require going forward. While itremains to be seen whether or not hiscondition will improve, but now I know
what I can do for my son.
19
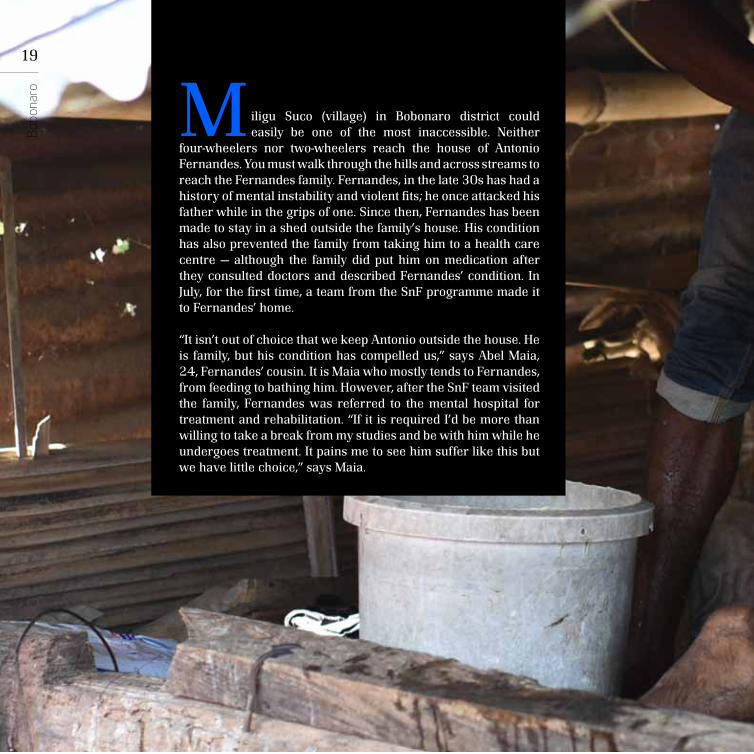
iligu Suco (village) in Bobonaro district could easily be one of the most inaccessible. Neither
four-wheelers nor two-wheelers reach the house of Antonio Fernandes. You must walk through the hills and across streams to reach the Fernandes family. Fernandes, in the late 30s has had a history of mental instability and violent fits; he once attacked his father while in the grips of one. Since then, Fernandes has been made to stay in a shed outside the family’s house. His condition has also prevented the family from taking him to a health care centre — although the family did put him on medication after they consulted doctors and described Fernandes’ condition. In July, for the first time, a team from the SnF programme made it to Fernandes’ home.
“It isn’t out of choice that we keep Antonio outside the house. He is family, but his condition has compelled us,” says Abel Maia, 24, Fernandes’ cousin. It is Maia who mostly tends to Fernandes, from feeding to bathing him. However, after the SnF team visited the family, Fernandes was referred to the mental hospital for treatment and rehabilitation. “If it is required I’d be more than willing to take a break from my studies and be with him while he undergoes treatment. It pains me to see him suffer like this but we have little choice,” says Maia.
MBobo
naro

20
Saúd
e na
Fam
ília

21
“We find cases like Fernandes, which perhaps could have never
come to light otherwise. Experiences like these make me feel strongly about the programme. This also makes you feel good as a doctor and as a human being too; I can go to bed knowing that I have changed someone’s life in some small way.”
Dr Sidonio Amaral,Cailaco, Community Health Center
Bobo
naro

22
Saúd
e na
Fam
ília
I am glad and so is therest of the family thatdoctors actualy came
all the way to our house,which is difficult to reach.But what is more relieving
is that António is beingreferred to the mentalhospital for treatment.We now look forward tothe day when he will bebetter and live with usunder the same roof.

INDONESIAONESIA
Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
64550
7
14
32
38
23
9734
Covalima

24
Saúd
e na
Fam
ília
aninito Lopez, three, is like any other kid his age: curious, inquisitive, sometimes bemused — just as he was to see
doctors, nurses and healthcare workers at his home. The doctors spoke to his parents and to him, then measured Lpoez’s height, weight etc. The purpose of it all escaped his curious eyes.
There’s one thing that sets Lopez apart: he’s visibly and starkly malnourished, weak. His protruding belly and skeletal arms bear testimony to his malnourishment. When the team of Saúde na Família doctors recorded Janinito’s anthropometric measurements, their preliminary clinical diagnosis was of ‘marasmus’, one of the three forms of serious protein-energy malnutrition (PEM).
There is hope, however. Lopez’s house has been marked for a nutritionist’s visit at the earliest. The nutritionist will counsel the parents on what kind of food he needs to have and more importantly, the family will get free nutrition supplements and fortified food that are tailor-made for children like Lopez. “It is now that I realise what a huge mistake it was on our part not to have taken our son to a healthcare centre. But I’m surprised and glad that the doctors have come home today and my son has a chance at healthier life,” says Julian Lopez Amaral, 32, Janinito’s father.
JIt is now that I realisethat a huge mistake itwas on our part to not
have taken our son to ahealthcare center. ButI’m surprised and gladthat the doctors havecome home today andmy son has a chance at
healthier life.

25
Cova
lima
In contrast to the preconceived notion that it is the communities in the rural areas and
inaccessible terrains that do not go to health centers, it is also families like these that are sometimes reluctant. It is only because of the Saúde na Família programme and the domiciliary visit that such families can be tapped. Of course, one of the challenges is the poor health awareness in the communities, but that can be addressed too, by this programme.
Dr. Rosita Martins,Suai (Covalima) City Health Post

26
Saúd
e na
Fam
ília

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
252854
6
22
87
96
99
23212
INDONESIAONESIA
Dili

28
Saúd
e na
Fam
ília
lexanderinho Xavier, 66, and Adelede de Santos, 65, are the kind of tuberculosis (TB) patients whom
doctors would term as difficult cases to treat. It is not because their TB is incurable but because they are irregular; not just in seeing a doctor but even in adhering to the medication and treatment. The couple cannot exactly recall how many years ago they were diagnosed with TB but they recall going to a doctor “now and then” — which essentially meant when their condition worsened. In doing so, the husband and wife also risked the health and thus the life, of the six children in the family. The Saúde na Família team visited the family in July 2016 and recorded the couple’s condition and that of the children. Alexanderinho and Adelede cited compelling reasons as to why they couldn’t adhere to the treatment cycle. They have now been referred to a TB hospital and will also receive subsistence support from the Ministry of Social Solidarity. “When I was first diagnosed I did not fully grasp the complexity of the disease, but I do now. After the doctors came home the first time, they explained to the children in the family as well — the precautions that they need to take and we need to take too, so that we don’t put anyone at risk. I am more than willing to see through my treatment,” says Xavier.
A
When I was first diagnosed I did not fully grasp the complexity of the disease,but I do now. After the doctors came home the first time, they explained tothe children in the family as well — the precautions that they need to takeand we need to take too, so that we don’t put anyone a risk . I am more than
willing to see through my treatment.
29
Dili
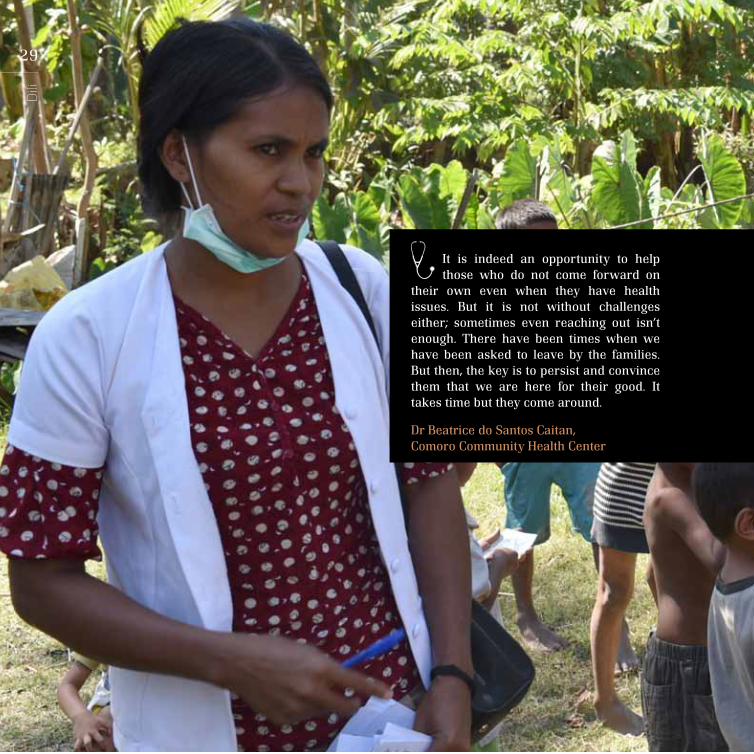
It is indeed an opportunity to help those who do not come forward on
their own even when they have health issues. But it is not without challenges either; sometimes even reaching out isn’t enough. There have been times when we have been asked to leave by the families. But then, the key is to persist and convince them that we are here for their good. It takes time but they come around.
Dr Beatrice do Santos Caitan,Comoro Community Health Center

30
Saúd
e na
Fam
ília

31
Dili

32
Saúd
e na
Fam
ília

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
127283
6
28
51
49
29
13068
INDONESIAONESIA
Ermera

34
Saúd
e na
Fam
ília
amilo Alves is 17, but has the frame of a nine or 10-year-old. A closer look at his face, uncovered arms and feet reveal that he possibly has some kind
of skin disease too, which is confirmed by the doctor who visited him earlier in the day as a part of the domiciliary visit of the Saúde na Família programme. Alves’ body is also ravaged by tuberculosis. Alves’ mother, Olga de Jesus, 44, the doctors find, suffers from TB too. The last time that the family ever visited a health facility was in 2003. “I took my son to the hospital in Ermera. They admitted him for a week. He improved somewhat and then we came back home. Since then he has been sick like this,” says Olga. Alves, given his illness, has never been to a school. “But I’m glad that the doctors came today and assured (us) that my son can receive not just treatment but also the needed nutritional supplements and fortified food,” Olga adds.
C

35
Erm
era

36
Saúd
e na
Fam
ília
“There are terrains and areas that make it difficult for families, especially the sick to travel to the nearest
health centre. People often say, how can we help if people do not come forward? I have always maintained that if the communities cannot come to the health centres then you need to take health to their doorstep. And this is the best way of doing just that.”
Dr Marcos Gomes,Gleno Community Health Center
37
Erm
era
…I’m glad that the doctors came today and assured (us) that my son can receive not just treatment but also the needed nutritional supplements
and fortified food.

38
Saúd
e na
Fam
ília

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
64135
5
32
54
44
26
4774
INDONESIAONESIA
Lautem
40
Saúd
e na
Fam
ília
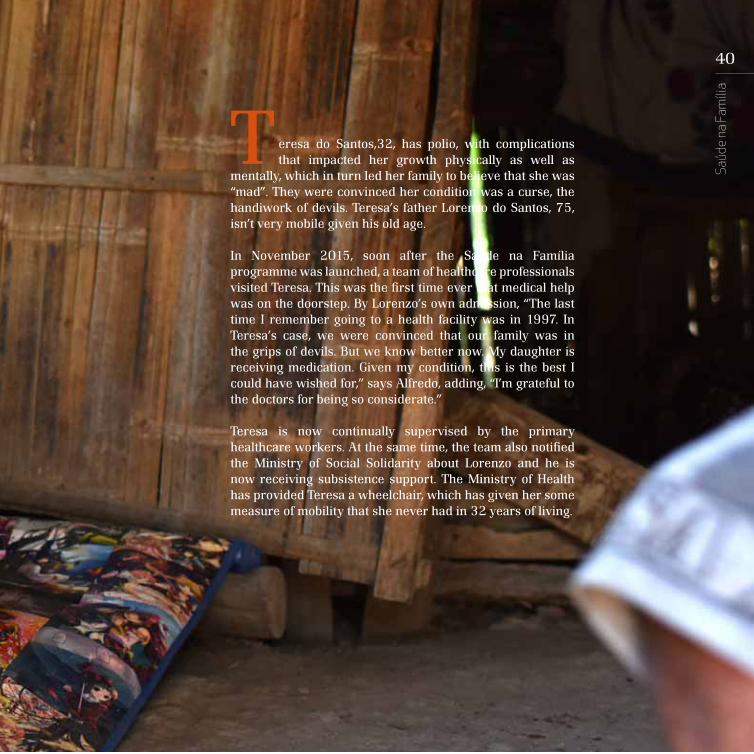
eresa do Santos,32, has polio, with complications that impacted her growth physically as well as
mentally, which in turn led her family to believe that she was “mad”. They were convinced her condition was a curse, the handiwork of devils. Teresa’s father Lorenzo do Santos, 75, isn’t very mobile given his old age.
In November 2015, soon after the Saúde na Família programme was launched, a team of healthcare professionals visited Teresa. This was the first time ever that medical help was on the doorstep. By Lorenzo’s own admission, “The last time I remember going to a health facility was in 1997. In Teresa’s case, we were convinced that our family was in the grips of devils. But we know better now. My daughter is receiving medication. Given my condition, this is the best I could have wished for,” says Alfredo, adding, “I’m grateful to the doctors for being so considerate.”
Teresa is now continually supervised by the primary healthcare workers. At the same time, the team also notified the Ministry of Social Solidarity about Lorenzo and he is now receiving subsistence support. The Ministry of Health has provided Teresa a wheelchair, which has given her some measure of mobility that she never had in 32 years of living.
T

41
Laut
em
If you are in the space of public health then it is
important that you know your village/hamlet/— basically the area that falls under your health post. You have to know each and every household, the living condition, the environment. It can happen only when you go out on the field. And Saúde na Família helps us do just that.
Dr Sonia Maria Gusmão,Lautem, District Health Centre

42
Saúd
e na
Fam
ília
The last time I remember going to a healthfacility was in 1997. In Teresa’s case, we were
convinced that our family was in the grips of adevil. But we know better now. My daughter isreceiving some kind of medication. Given my
condition, this is the best I could have wished for.

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
73027
3
21
46
37
26
14064
INDONESIAONESIA
Liquiça

44
Saúd
e na
Fam
ília
he story of Jaimito Gonsalves is both heart wrenching and heartwarming. It also epitomises the
transformative potential of the SnF programme. Gonsalves, 23, has polio with complications that impacted his mental growth too. However, his family did not seek medical help; his father subjected Gonsalves to some indiscriminate medication instead.
A team of Saúde na Família health professionals visited the family in January 2016 and noticed that the son was kept in a separate shed outside the house. The doctors immediately contacted a rehabilitation centre for the differently abled. The following day Gonsalves was in the centre, and under supervised medical care and rehabilitation therapy. After six months of treatment, Gonsalves is now reunited with his family and lives in the same house as the rest of the family members. “What we did was because of our limited understanding of what he suffered from. But the doctors and team who visited us have helped us understand. He shares the same roof as us now and I want to make up for all the painful times he had to endure because of our lack of knowledge,” says Pedro Gonsalves, 63, the father.
T

45
Liqu
iça

46
Saúd
e na
Fam
ília
“A programme like this makes you realise that your medical education can’t and should not end in the four
walls of the medical school. For instance, in this particular case, the challenge wasn’t to treat Jaimito as such; we know his condition, we know the treatment. It was taught to us. But what stumped us was the treatment that he was subjected to by the family. So, the challenge was to make the family understand, to counsel them. The programme teaches you to engage with the community, it is one of the most — if not the most — important tool(s) of public health and primary health care according to me.”
Dr Alfarobino do Santos Ques, Coordinator for Primary Healthcare Programme for Liquica

47
Liqu
iça
What we did was because of our limited understanding of what he suffered from. But the doctor and team who visited us have helped us understand. He shares the same roof as us now and I want to make up for all the difficult times he had to endure because of our lack of knowledge.

48
Saúd
e na
Fam
ília
What we did was because of our limited understanding of what he suffered from. But the doctor and team who visited us have helped us understand. He shares the same roof as us now and I want to make up for all the difficult times he had to endure because of our lack of knowledge.

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
45541
6
21
55
41
26
7443
INDONESIAONESIA
Manatuto

50
Saúd
e na
Fam
ília
rancisa Soares, 65, has been bed-ridden for nearly three years now. During this time, she has never
been taken to a doctor or a health facility. She has gangrene on the right foot; the festering wound she has was never tended to. The kids in the family, all teenagers, hovered around when the doctor was inquiring after Fracisca. “She’s our grandmother. Father is in the fields most of the time and mother too... It is also almost impossible to carry her anywhere. We have tried some traditional treatment but that doesn’t seem to have helped Avo (grandmother),” says Julia Soares, 17. In June 2016, a team of Saúde na Família came to Soares’ house the first time. They explained the situation to the family members and insisted that she be taken to a health centre. The team also emphasised the need and importance of cleanliness and hygiene. However, Francisca was never taken to a health facility. Instead, the team went out of their turn and visited her twice to clean and bandage her wound. The team also notified the Ministry of Health about the severity of the case and indicated that Francisca is in need of urgent surgical intervention.
F

51
Man
atut
o
In August, an ambulance from the Ministry of Health was sent to Francisca’s house and she was admitted to the national hospital, Hospital Nacional Guido Valadares (HNGV) in Dili. The doctors at the hospital, after assessing the condition, amputated her foot, thereby saving the rest of her leg. Francisca remained in the hospital for the duration of her recovery and has since been successfully rehabilitated with her family.

52
Saúd
e na
Fam
ília
©WHO/SHOBHAN

53
We all have a firm belief in the programme. Moreover, after having worked on the field for a while now, we know its potential and the change it can make. But like
anything in life, this programme too has its challenges. Sometimes the community is the challenge itself — their reluctance to change certain ways and methods to ensure better hygiene and health etc. But then, had all been so easy then the programme wouldn’t have been as interesting either perhaps.”
Dr Rina de Araújo de Franco,Laclubar Community Health Center
Man
atut
o

54
Saúd
e na
Fam
ília

55
On September 8, 2016 H.E. Primer Minister Dr Rui Maria de Araújo joined the team of Saúde na Família healthcare professionals in Manatuto for domiciliary visit. Dr Araújo who is a doctor himself and the brain behind the programme examined Esperança da Costa and recorded the details of the visit online.
Man
atut
o

56
Saúd
e na
Fam
ília

57
Man
atut
o

58
Saúd
e na
Fam
ília

59
Man
atut
o

60
Saúd
e na
Fam
ília
Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
52246
4
21
42
36
25
4438
INDONESIAONESIA
Manufahi
62
Saúd
e na
Fam
ília
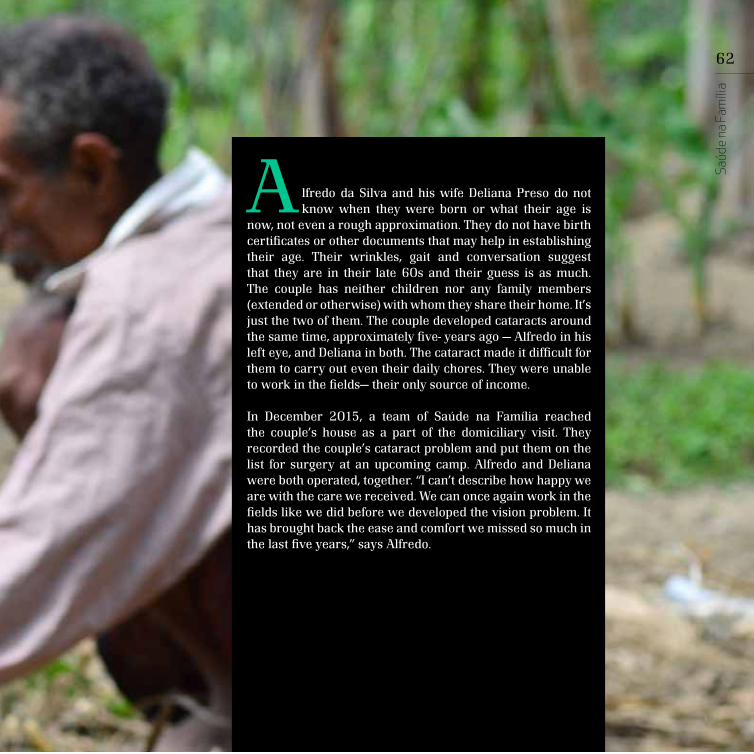
lfredo da Silva and his wife Deliana Preso do not know when they were born or what their age is
now, not even a rough approximation. They do not have birth certificates or other documents that may help in establishing their age. Their wrinkles, gait and conversation suggest that they are in their late 60s and their guess is as much. The couple has neither children nor any family members (extended or otherwise) with whom they share their home. It’s just the two of them. The couple developed cataracts around the same time, approximately five- years ago — Alfredo in his left eye, and Deliana in both. The cataract made it difficult for them to carry out even their daily chores. They were unable to work in the fields— their only source of income.
In December 2015, a team of Saúde na Família reached the couple’s house as a part of the domiciliary visit. They recorded the couple’s cataract problem and put them on the list for surgery at an upcoming camp. Alfredo and Deliana were both operated, together. “I can’t describe how happy we are with the care we received. We can once again work in the fields like we did before we developed the vision problem. It has brought back the ease and comfort we missed so much in the last five years,” says Alfredo.
A

63
Man
ufah
i
“The programme is a powerful public health intervention mechanism. There is so much built into the programme
that it can potentially direct the entire healthcare system from curative care to preventive, which is how it should be in an ideal world.
The biggest challenge we face is access to some remote areas, especially in the rains. There’s no way that certain areas can be accessed in the rains.”
Dr Samuel Magno da Silva,Same Community Health Centre

64
Saúd
e na
Fam
ília

65
Man
ufah
i

66
Saúd
e na
Fam
ília
I can’t describe how happy we are with the care we received. Wecan once again work in the field like we did before we developedthe vision problem. It has brought back the ease and comfort we
missed so much in the last five years.

Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
72230
4
17
33
15
15
1637
INDONESIAONESIA
Oecusse

68
Saúd
e na
Fam
ília
argareta Oqui, 25, is in the third trimester of her first pregnancy. Her husband Abilio Sun, 29, is
both excited and anxious. The couple lives in a joint family setting, which includes Abilio’s mother and the family of his elder brother, Martinho Nuno, 37. Martinho’s wife Julian Oqui gave birth to her second child just in August 2016. The family’s house is a stone’s throw away from the Community Health Centre (CHC), and the family accesses it often. It was the midwife, nutritionist, the nurse and the doctor from the CHC who saw Julian through her second pregnancy and the Saúde na Família team assisted did the delivery.
The Saúde na Família team is almost like family for Margareta and Julian especially Imaculada Pereira, the midwife. “She delivered my second child and she had been following up on my second pregnancy throughout, with her colleagues who told me about diet, precautions, dos and don’ts etc. Now she is looking after my sister-in-law. They have become the constant in our lives. It is very reassuring and comforting for a pregnant woman,” says Julian.
M

69
Oec
usse
Imaculada Pereira, Midwife, Baki Community Health Centre, Oecusse on challenges of working with the community
“As a midwife, my job is to best help the community, especially women. That’s what I’m trained for.
However, sometimes you come across families that do not want to work with you in order to help them live better. They do not cooperate or just do not follow your advice. It’s not every day that you come across a family like this.”
70
Saúd
e na
Fam
ília
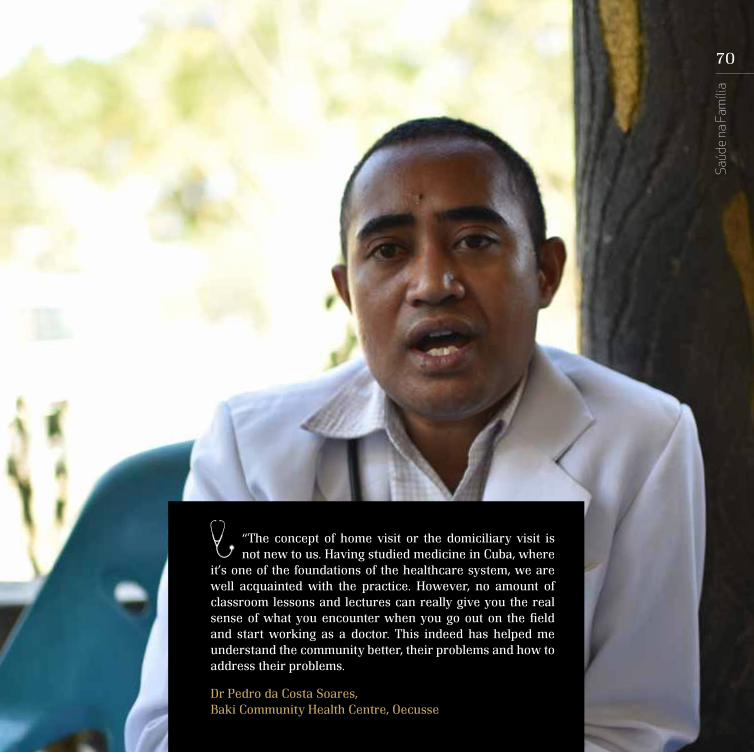
“The concept of home visit or the domiciliary visit is not new to us. Having studied medicine in Cuba, where
it’s one of the foundations of the healthcare system, we are well acquainted with the practice. However, no amount of classroom lessons and lectures can really give you the real sense of what you encounter when you go out on the field and start working as a doctor. This indeed has helped me understand the community better, their problems and how to address their problems.
Dr Pedro da Costa Soares, Baki Community Health Centre, Oecusse

71
Oec
usse
She delivered my secondchild and she had been
following up on my secondpregnancy throughout,
with her colleagueswho told me about diet,
precautions, dos anddon’ts etc. Now she is
looking after my sister-in-law. They have become
the constant in our lives.It is very reassuring and
comforting for a pregnantwoman.

72
Saúd
e na
Fam
ília
Population:
No. of Community Health Center:
No. of Health Posts:
No. of doctors:
No. of nurses:
No. of midwises:
No. of households coveredunder Saúde na Família:
77402
5
43
52
88
35
6521
INDONESIAONESIA
Viqueque

74
Saúd
e na
Fam
ília
hen he was born, we didn’t think he would survive. But thanks to some traditional
healers, he did. However, his disability is crippling. I don’t think his condition is going to improve. However, if you tell me otherwise, I’m willing to give it a try,” says Luis Ornei, 55 — of his grandson Elizario Pereira Monteiro, 13, who suffers from polio and associated complications.
Elizario’s polio has not just rendered him immobile but also with left him with a cognitive disability. He cannot speak but does understand just little when spoken to. Luis says he took his grandson to clinics and doctors a couple of times when he seemed unwell but he is almost convinced that his grandson can never hope for a better life. The Saúde na Família team visited the family in May 2016. The team has already made a referral request for the rehabilitation therapy. “I’d be more than happy to take Elizario if it means a shot at a better life for him. But what we need is a wheelchair for him so that he can at least move around the house by himself. It will be a relief for not just him but us too,” says Luis. Luis’ request was immediately escalated to the Ministry of Health and the Municipal Administrator and the needful was done for Luis on an urgent basis.
“W

75
Viqu
eque

76
Saúd
e na
Fam
ília
“The opportunity to make a difference to someone’s life
by means of a simple home visit is absolutely wonderful. In that moment you feel so satisfied that your work is of some consequence in the larger scheme of things. But then, there are also times when you find cases, where there is little or no scope of intervention because we found them late. It breaks you to realise that you are helpless; all that you have studied and worked for so many years is of little use because you just can’t undo what has already happened to a person.”
Dr. Isaias Renaldo Monteiro Gueterrs, Ossu, Community Health Centre

77
Viqu
eque
I’d be more than happy to takeElizario if it means a shot at
better life for him. But what weneed is a wheelchair for him so
that he can at least move aroundthe house by himself.

78
Saúd
e na
Fam
ília

79







![ISSN 1519-339X / [ISSN 2447-2034] V. On-line Revista · com foco na Estratégia Saúde da Família ... Alexandra de Freitas Teixeira, Thayane Cristine Ribeiro de Sousa Bomfim ...](https://static.fdocuments.in/doc/165x107/5bfc464b09d3f297368b48d1/issn-1519-339x-issn-2447-2034-v-on-line-revista-com-foco-na-estrategia.jpg)