Evaluation of Clinical Benefit in Sarcomas: Modern Imaging Modalities
Upload
cristian-yanezCategory
view
330download
0
114
The incidence of nonvisualization of the vestibularaqueduct and the endolymphatic duct–endolym-phatic sac (ED-ES) complex as well as the type ofperiaqueductal pneumatization were evaluated in23 patients with definite Meniere’s disease (MD) byhigh-resolution CT and by MRI. Fifty subjects with noprevious history of any ear disease were used as acontrol group. High-resolution CT results disclosedthat in the control group the percentage of nonvi-sualized vestibular aqueduct (3.4%) was statisticallysignificantly lower than in the MD group, wheneither the diseased ear (27.8%) or the nondiseasedear of the same group (22.2%) was examined. Inaddition, no differences were observed betweenthe diseased and nondiseased ears of the patientswith MD. The periaqueductal pneumatization wasalso found to be statistically significantly lower inthe MD group. As regards the MRI examination, theresults of the analysis showed that the ED-ES com-plex was visualized more frequently in the ears ofthe control subjects (64.1%) than in the diseasedears of the patients with Meniere’s disease (39.1%).This difference had a marginal statistical signifi-cance (P ~ 0.05). We discussed the results in relationto possible underlying pathophysiologic mecha-nisms involving the flow of endolymph toward the ESduring the different stages of the disease. (Oto-laryngol Head Neck Surg 2000;123:114-9.)
Meniere’s disease (MD) is a well-established clini-cal entity; patients with the definite type have all of thefollowing symptoms: vertigo, hearing loss, and tinni-tus or ear pressure.1 Since MD’s description by ProsperMeniere,2 the scientific community has tried to discoverthe underlying etiopathophysiologic factors responsiblefor the characteristic vestibulocochlear dysfunction.
Today it is widely accepted that the histopathologicsubstrate of the disease is endolymphatic hydrops (EH)because of the disruption of the balance between pro-duction and absorption of the endolymph.3
A key role in the pathogenesis of the EH is attributedto impaired function of endolymphatic duct (ED) andendolymphatic sac (ES).4 The ED-ES system lies partlywithin, partly through, and partly outside of the vestibu-lar aqueduct (VA), which is a bony channel of the oticcapsule.
In the literature concerning MD, there are somereports of a high incidence of radiologic nonvisualiza-tion of the VA5,6 and poor pneumatization of the sur-rounding mastoid air cells in the diseased ears.6,7 How-ever, other authors8,9 consider these observations asnonspecific diagnostic signs seen in a variety of ear dis-eases.
In this study we analyzed our findings after exami-nation of the VA, ED-ES complex, and periaqueductalpneumatization with high-resolution (HRCT) and MRIof 23 temporal bones from 23 patients with definite uni-lateral MD. We also attempted to delineate the possibleimplications of these findings on the normal function ofthe inner ear.
ANATOMY OF THE VA AND THE ED-ES COMPLEX
The VA is a bony canal that contains the ED and theproximal part of the ES. It extends from the medial wallof the vestibule to the posterior surface of the petrouspyramid, where it terminates in a bony cleft called theendolymphatic meatus, which contains the ES. Inadults, as the VA traverses the temporal bone, it isshaped like an inverted J. The short limb and the bend
INTERNATIONAL ORIGINAL ARTICLESEUGENE N. MYERS, MDInternational Editor
Role of the new imaging modalities in the investigation ofMeniere’s diseaseJOHN XENELLIS, MD, LAMBROS VLAHOS, MD, ANDREAS PAPADOPOULOS, MD, PERICLES NOMICOS, MD,KONSTANTINOS PAPAFRAGOS, MD, and GEORGE ADAMOPOULOS, MD, Athens, Greece
From the Departments of ENT (Drs Xenellis, Nomicos, Papafragos,and Adamopoulos) and Radiology (Drs Vlahos and Papadopoulos),University of Athens Medical School.
Reprint requests: J. Xenellis, MD, Sarantapichou 35, GR-114 72Athens, Greece.
Copyright © 2000 by the American Academy of Otolaryngology–Head and Neck Surgery Foundation, Inc.
0194-5998/2000/$12.00 + 0 23/77/102113doi:10.1067/mhn.2000.102113

Otolaryngology–Head and Neck SurgeryVolume 123 Number 1 Part 1 XENELLIS et al 115
of the VA together are called the isthmus, and this is themost narrow part of it.
The distal end of the VA expands to accommodatethe terminal enlargement of the ED, the ES. Lund-quist10 divided the ES into 3 parts: (1) a proximal partlocated within the VA, (2) an intermediate part locatedpartially within the VA and partially between the layersof dura mater outside the VA, and (3) a distal part rest-ing completely within layers of dura mater.
The dimensions of the VA and the ED-ES complexrender visualization of these structures by radiologicmethods technically feasible. The VA can be visualizedon CT, and the postisthmic part of the ED and the ES,along with their stroma, can be visualized on MRI. Inthis context, the degree and type of periaqueductalpneumatization is crucial because it seems to have adirect influence on the appearance and the length of theVA.6
In our study we classified the type of pneumatizationof our patients according to the proposed scheme byStahle and Wilbrand.6 They considered 3 types ofpneumatization: type I, with large-cell pneumatization;type II, with small air cells or bone marrow spaces; andtype III, with a complete absence of air cells. In type Ithe VA is longer, and its external aperture is wider.Contrary to type I, type III is compatible with a shorter
VA, which also shows a narrow external aperture. InMD there is a high incidence of type III pneumatiza-tion.6,7
METHODS AND MATERIAL
Between 1994 and 1996, 23 patients with definite unilateralMD were evaluated in the ENT Department of the Universityof Athens. This group of patients constitutes the source of thisstudy. The selection criteria for these patients conformed tothose proposed by the Committee on Hearing and Equilibriumof the American Academy of Otolaryngology–Head and NeckSurgery.1 None of the patients expressed the so-calledcochlear or vestibular types of MD.
The patient group included 10 men and 13 women. Theright ear was involved in 12 patients, and the left ear wasinvolved in 11. The mean age of the patients was 48.6 years(range 19-72 years). In 12 patients (52%) the disease durationranged between 4 and 9 years, in 4 (17.4%) it was more than9 years, and in the remaining 7 (30.6%) it was less than 4years. The mean duration of symptoms was 5.3 years (range0.3-24 years).
The mean value of the pure-tone audiograms (500, 1000,2000, and 4000 Hz) was 48.2 dB, and the type of hearing losswas flat in 14 patients (60.9%), downward sloping in 6 (26%),and upward sloping in 3 (13%). At the time of HRCT andMRI, the disease in all 23 patients was in an inactive phase,and none of them reported vertigo.
As a control group, we used 50 patients who had no previ-
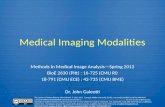
Fig 1. Transaxial HRCT of a normal VA (arrow).
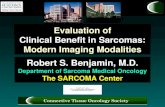
Fig 2. MRI of a normal ED-ES complex (arrow).

Otolaryngology–Head and Neck Surgery
116 XENELLIS et al July 2000
ous history of any ear disease and had CT and MRI examina-tion of the brain for other reasons. More precisely, 29 of themhad HRCT and the other 21 had MRI.
HRCT of the petrous bone was performed on a 9800 GEscanner with the following technical characteristics: 1.5-mmslice thickness, 1-mm table increment, 200 mA, 3 seconds,120 kV, 10-cm field of view (FOV), and bone algorithm. Thesection plane was 30° above the anthropologic line.11 Forimproved demonstration of the VA, reformed images wereobtained in the sagittal plane parallel to a line connecting theexternal aperture of the VA and the common crus of the pos-terior and superior semicircular canals (Fig 1).
Measurements of the VA were made by one radiologistblinded to any clinical information. Images were magnified by2, and the anteroposterior diameter of the VA was manually cal-culated at the midpoint of the postisthmic segment of the VA.
MRI was performed on a Phillips 0.5-T Gyroscan unit.Two-dimensional Fourier transform images of the membra-nous labyrinth were obtained with an SE T1-weighted pulsesequence (recovery time, 700 ms; echo time, 15 ms; FOV, 20cm; matrix, 192 × 256) and a GRE pulse sequence (recoverytime, 40 ms; echo time, 17 ms; flip angle, 90°; FOV, 16 cm;matrix, 205 × 256). The section plane was 30° to the anthro-pologic line. Slice thickness was 3 mm, and interslice gap was0.3 mm for both sequences. All examinations were performedwith a head coil (Fig 2).
RESULTS
Table 1 shows the HRCT findings regarding thepneumatization of the temporal bones in the diseasedand control groups. We did not consider separately the2 ears of the patients with MD because we found thatthe pneumatization was similar between the two sites.From the univariate analysis and the χ2 test from trend,we found that there was statistically significant differ-ence in the type of pneumatization between the controlgroup and the MD group. Type I pneumatization wasfound in 41.4% of the control group and only 11.1% ofthe MD group. On the other hand, type III pneumatiza-tion was found in 55.5% of patients with MD and onlyin 24.1% of control patients. Type II pneumatizationwas similar in both groups.
Table 2 shows the percentage of visualization of VAin the various groups after the tomographic examinationof the temporal bone with HRCT. In the control groupboth ears were considered together, whereas in the MDgroup the two ears were evaluated separately.
The VA was not visualized in 3.4% of the controlgroup. In the MD group it was not visualized in theaffected ears in 27.8% and in the ears on the oppositeside in 22.2%.
Both differences, between the control group and thediseased and nondiseased ears of the MD group, were
Table 1. Frequency distribution of the pneumatiza-tion type among control and MD groups
Control group MD group
Pneumatizationtype n % n % P value
I 12 41.4 2 11.1 0.01II 10 34.5 6 33.3III 7 24.1 10 55.5
Table 2. Frequency distribution of the visualizationof the HRCT examination among control and MDgroups
MD group
Control Diseased Nondiseasedgroup* ear† ear‡
HRCT result n % n % n %
Visualized 56 96.6 13 72.2 14 77.8Nonvisualized 2 3.4 5 27.8 4 22.2
*P = 0.007 for control group versus diseased ear (Fisher exact test).†P = 0.02 for control group versus nondiseased ear (Fisher exact test).‡P = 0.78 for diseased versus nondiseased ear (Fisher exact test).
Table 3. Descriptive characteristics of the width ofthe VA among control and MD groups
Average Minimum MaximumGroup n (mm) (mm) (mm)
Control patient 56 1.08 0.50 2.00Diseased ear 13 0.63 0.40 1.00Nondiseased ear 14 0.83 0.60 1.20
Table 4. Frequency distribution of the visualizationof the MR examination among control group, dis-eased and nondiseased ears from MD groups
MD group
Control Diseased Nondiseasedgroup* ear† ear‡
HRCT result n % n % n %
Visualized 25 64.1 9 39.1 14 63.6Nonvisualized 14 35.9 14 60.9 8 36.4
*P = 0.05 for control group versus diseased ear (Fisher exact test).†P = 0.59 for control group versus nondiseased ear (Fisher exact test).‡P = 0.08 for diseased versus nondiseased ear (Fisher exact test).

Otolaryngology–Head and Neck SurgeryVolume 123 Number 1 Part 1 XENELLIS et al 117
found to be statistically significant. On the contrary,examining the affected and nonaffected ears of the MDgroup, no statistically significant differences wereobserved.
Performing the Mann-Whitney U and the Wilcoxonnonparametric tests, we compared also the width of thevisualized VA between the control and the MD groups.More precisely, as shown in Table 3, the average widthof the VAs in the control group was 1.08 mm (range0.50-2.0 mm), whereas it was only 0.63 mm (range0.40-1.0 mm) in the diseased ears (P < 0.001) and 0.83mm (range 0.60-1.2 mm) in the nondiseased ears (P <0.01) in the MD group.
Table 4 depicts the percentages of visualized andnonvisualized ED-ES complex with MRI in the con-trol and the MD group. In the latter group the dis-eased and nondiseased ears were also considered sep-arately.
The ED-ES complex was visualized in 64.1% of thecontrol group and only in 39.1% of the diseased ears.This difference was proved to have a marginally statis-tical significance (P ~ 0.05). The visualization of theED-ES complex in the nondiseased ears of the MDgroup was almost similar to that of the control group(63.6%), without any statistical significance.
DISCUSSION
The ED-ES complex has long been recognized as apossible explanation of the pathogenesis of EH, whichis the histopathologic substrate of MD.4,12 Studies sug-gest that the ED and ES are both actively involved inendolymph regulation. In experimental animals it wasproved that the destruction of the ES or obstruction ofthe ED resulted regularly in progressive EH.4
Clemis and Valvassori5 first reported that there is ahigher incidence of nonvisualization of the VA inpatients with MD on conventional tomography. Theirobservation was criticized by Yuen and Schuknecht,13
who reported that measurements of VAs in histologicsections of temporal bones of patients with MD failed toestablish any statistical evidence of narrowing, in com-parison with measurements in normal temporal bones.However, these authors measured the isthmic and notthe postisthmic part of the VA, as was recommended byClemis and Valvassori. Sando and Ikeda14 investigatingthis controversy confirmed the finding of Clemis andValvassori of hypoplasia of the postisthmic segment ofthe VAs in histologic examinations of temporal bones ofpatients with MD. Absence and morphologic abnormal-ities of the VA-ES complex, along with poor pneumati-zation of the periaqueductal mastoid air cells, have been
Fig 3. HRCT of a patient with MD: VA is not visualized. Poorperiaqueductal pneumatization (arrow).
Fig 4. MRI of a patient with MD: ED-ES system is not visual-ized.

Otolaryngology–Head and Neck Surgery
118 XENELLIS et al July 2000
correlated with ES fibrosis, which is one of the pro-posed causes of MD.7
There is no universally accepted classification of thedifferent morphology types of VAs, nor is there a stan-dard point where measurements should be taken. In thisstudy we measured the width of the VA at the midpointof the postisthmic segment.
Valvassori and Dobben15 classified the VA into 5types, based on measurements at the anteroposteriordiameter of the midpoint of the postisthmic segment, asfollow: (1) normal, 0.5 to 1 mm; (2) filiform, less than0.3 mm; (3) large, 1.5 cm or more; and (4) obliterated,when a portion of the postisthmic segment is not visu-alized; and (5) nonvisualized.
Our data are in accordance with those of others,6,7
who found that MD is associated with an increased inci-dence of abnormally decreased periaqueductal pneuma-tization and small or nonvisualized VA (Fig 3). Moreprecisely, type III was found in 55.5% of ears ofpatients with MD and only 24.1% of the ears of controlsubjects (Table 1). Likewise the VA was not visualizedin 27.8% in the diseased ears and only 3.4% in the con-trol group ears (Table 2). Table 3 displays 2 moreimportant findings. First, in the studied group the aver-age width of the VA is obviously smaller than in thehealthy subjects, and second, the nondiseased ears inthe MD group show the same abnormalities as theaffected ones. This evidence supports the opinion thatthe disease is bilateral and there is a progressivelyincreasing incidence of involvement of the second ear ifthe patients with MD are followed up for many years.9
Preliminary studies using MRI suggest that patientswith MD often have a small or nonvisualized ED-EScomplex.16 Results of this study confirm the aboveobservation (Fig 4). Visualization of the ED-ES systembetween diseased ears and ears from the control groupindicated a marginally statistically significant differ-ence (P ~ 0.05). On the contrary, the visualization of theED-ES in nondiseased ears of patients with MD was notstatistically different from that in ears of control sub-jects.
It is probable that an adequately visible ED-ES com-plex with MRI has to do with the stage and phase(active-nonactive) of the disease.17 Linthicum andXenellis18 disclosed that the temporal bones of patientswith MD with hearing loss (0.5, 1.0, and 2.0 kHz) of 65dB or greater showed small or obliterated ES and a faradvanced EH with a severe deformation of the normalhistoanatomic architecture of the membranous innerear. Accordingly, the passage of endolymph from thepars superior and inferior to the ES in cases such isprobably obstructed. Schuknecht and Ruther19 describedthe possible areas of blockage of the longitudinal flow
of endolymph in cases of advanced EH. MRI when theendolymph has no access to the ES may fail to depictthe ED-ES complex. However, the physician mustalways keep in mind the small possibility of an anatomicaberration of the ES20 as a cause of a failure in visual-ization of the ED-ES complex. In our study we did notfind any statistically significant difference (P ~ 0.1) invisualization of ES between the diseased and nondis-eased ears and only a marginally statistical differencebetween the diseased ears of the MD group and those ofthe control group. In this particular group of patients,the disease was in an inactive phase, and no patientsshowed hearing loss of more than 65 dB (mean value48.2 dB). In this context it is important to note theobservation of Tanioka et al,17 who found that inpatients having acute episodes of MD, the ED-ES com-plex was not adequately visible in the affected ear butwas seen well in the unaffected ear; Tanioka et al alsofound that during remission the ED-ES complex wasnot visible in patients with clinically advanced diseasebut was seen well during the early-to-moderate stagesof disease.
CONCLUSIONS
1. HRCT findings in our group of patients with defi-nite MD are in accordance with those of others,who found that MD is associated with an in-creased incidence of abnormally decreased peri-aqueductal pneumatization and small or nonvisu-alized VA.
2. MRI is a sensitive examination of the membra-nous labyrinth and may contribute to better under-standing of the pathophysiology of the differentstages and phases of MD.
3. HRCT and MRI may be used as confirmatoryexamination techniques when the diagnosis of MDis in question.
4. Further studies are necessary to confirm the abili-ty of MRI to depict and differentiate the differentstages of MD. If this proves to be true, MRI maybecome a useful means for planning individuallythe best therapeutical approach for each patient.
REFERENCES
1. Committee on Hearing and Equilibrium guidelines for the diag-nosis and evaluation of therapy in Meniere’s disease. OtolaryngolHead Neck Surg 1995;113:181-5.
2. Meniere P. Sur une form de surdite grave dependant d’une lesionde l’oreille interne. Gar Med Paris 1861;16:29.
3. Schuknecht HF. Disorders of unknown or multiple causes. In:Schuknecht HF, editor. Pathology of the ear. 2nd ed. Philadel-phia: Lea and Febiger; 1993. p. 499-519.
4. Kimura RS. Experimental blockage of the endolymphatic duct andsac and its effect on the inner ear of the guinea pig. A study onendolymphatic hydrops. Ann Otol Rhinol Laryngol 1967;76:664-87.
5. Clemis SD, Valvassori GE. Recent radiographic and clinical

Otolaryngology–Head and Neck SurgeryVolume 123 Number 1 Part 1 XENELLIS et al 119
observations on the vestibular aqueduct (a preliminary report).Otolaryngol Clin North Am 1968;1:339-46.
6. Stahle J, Wilbrand H. The vestibular aqueduct in patients withMeniere’s disease. A tomographic and clinical investigation. ActaOtolaryngol (Stockh) 1974;78:36-48.
7. Stephen FH, Fitzgerald O’Connor, et al. Significance of tomog-raphy in Meniere’s disease: periaqueductal pneumatization.Laryngoscope 1983;93:1551-3.
8. Kraus EM, Dubois PJ. Tomography of the vestibular aqueduct inear disease. Arch Otolaryngol 1979;105:91-8.
9. Sackett JF, Korareck JA, Arenberg IK. The clinical significanceof tomographic visualization or nonvisualization of the vestibularaqueduct. Otolaryngol Clin North Am 1980;13:657-64.
10. Lundquist PG. The endolymphatic duct and sac in the guinea pig.An electron microscopic and experimental investigation. ActaOtolaryngol (Stockh) 1965;Suppl 201:1.
11. Brogan M, Chakeres DN, Schmalbrock P. High resolution 3DFMR imaging of the endolymphatic duct and soft tissues of oticcapsule. AJNR Am J Neuroradiol 1991;12:1-11.
12. Egami T, Sando I. Pathology of the vestibular aqueduct andendolymphatic sac in temporal bones with endolymphatic hy-drops. In: Hood JD, editor. Vestibular mechanisms in health anddisease. London: Academic Press; 1978. p. 122-8.
13. Yuen SS, Schuknecht H. Vestibular aqueduct and endolymphaticduct in Meniere’s disease. Arch Otolaryngol 1972;96:553-5.
14. Sando J, Ikeda M. The vestibular aqueduct in patients withMeniere’s disease: a temporal bone histopathological investiga-tion. Acta Otolaryngol (Stockh) 1984;97:558-70.
15. Valvassori G, Dobben G. Multidirectional and CT of the vestibu-lar aqueduct in Meniere’s disease. Ann Otol Rhinol Laryngol1983;93:547-50.
16. Tanioka H, Zusho H, Machida T et al. High resolution MR imag-ing of the inner ear: findings in Meniere’s disease. Eur J Radiol1992;15:83-8.
17. Tanioka H, Kimitaka K, Zusho H, et al. MR of the endolymphat-ic duct and sac: findings in Meniere disease. AJNR Am JNeuroradiol 1997;18:45-51.
18. Linthicum FH Jr, Xenellis JE. Pathophysiological mechanisms toMeniere’s syndrome based on infrared oculography andhistopathology. Proceedings of the 4th International Symposiumon Meniere’s disease.
19. Schuknecht HF, Ruther A. Blockage of longitudinal flow inendolymphatic hydrops. Eur Arch Otorhinolaryngol 1991;248:209-17.
20. Feghali JG, Linthicum FH Jr, Xenellis SE. Is the endolymphatic sacalways accessible? Otolaryngol Head Neck Surg 1985;93:21-4.
Brachytherapy Workshop
The 3rd Workshop on Brachytherapy in Head and Neck Cancer will be held August27-29, 2000, in Kiel, Germany. Chairmen are Prof Dr H. Rudert and Prof Dr G.Kovács.
For further information, contact S. Gottschlich, MD, Department of Otorhino-laryngology–Head and Neck Surgery, University of Kiel, Arnold-Heller-Strasse 14, D-24105 Kiel, Germany; phone, 49-431-5972321; fax, 49-431-5972272; e-mail, [email protected].