Role of persistent amenorrhea in bone mineral metabolism of young hemodialyzed women
5
Kidney International, Vol. 58 (2000), pp. 331–335 Role of persistent amenorrhea in bone mineral metabolism of young hemodialyzed women JOSE ´ R. WEISINGER,LEYDA GONZALEZ,HECTOR ALVAREZ,EDDY HERNANDEZ, RAU ´ L G. CARLINI,FREYA CAPRILES,MERCEDES CERVIN ˜ O,RUBY MARTINIS, VIRGILIO PAZ-MARTI ´ NEZ, and EZEQUIEL BELLORI ´ N-FONT Division of Nephrology, Hospital Universitario de Caracas, Universidad Central de Venezuela and Fresenius Medical Care of Venezuela, Caracas, Venezuela with normal menstruating women on dialysis. The possible Role of persistent amenorrhea in bone mineral metabolism of impact of these results in the natural history of the uremic young hemodialyzed women. osteodystrophy remains to be determined. Background. Chronic renal failure in women is frequently associated with endocrine disturbances leading to menstrual disorders. However, most studies on renal osteodystrophy have not taken into account the possible role of these hormonal The term renal osteodystrophy has been widely ac- disturbances on the pathogenesis of bone alterations seen in cepted to define the bone lesions associated with chronic these patients. In the present study, we evaluated bone mineral metabolism in a group of young hemodialyzed women with renal failure. It includes diseases that affect the control persistent amenorrhea and compared them with similar women of bone remodeling, such as high turnover bone disease with regular menstruation. caused basically by secondary hyperparathyroidism or Methods. We studied 74 women who were further subdi- low turnover in the form of adynamic bone disease and vided into 43 women with regular menstrual periods and 31 women with persistent amenorrhea, defined as the absence of osteomalacia, usually associated to vitamin D deficiency menstrual bleeding for more than six months. In all patients, or aluminum toxicity [1]. However, little concern has we performed a bone mineral density (BMD) analysis and been given to the possible role of estrogen deficiency in simultaneously evaluated different biochemical parameters, in- the pathogenesis of uremic bone disease. Indeed, since tact parathyroid hormone (iPTH), sexual hormone determina- renal osteodystrophy develops at a faster rate and repre- tions that included total estradiol, follicle-stimulating (FSH), and luteinizing hormone and markers of bone resorption such sents a major clinical problem, it has dominated the as the procollagen type 1 cross-linked carboxy-terminal telo- contribution that postmenopausal osteoporosis could peptide (ICTP). have in the bone alterations observed in the female ure- Results. Serum calcium, phosphorus, and iPTH were similar mic patient. This is particularly important since uremic in both groups. Serum alkaline phosphatase was higher in women frequently have early menopause or anovulatory amenorrheic women. Although the total serum estradiol con- centration was normal in the amenorrheic women when com- cycles with hypoestrogenism, an important hormonal al- pared with nonuremic women, the values were significantly teration frequently associated with osteoporosis [2]. lower than those in regularly menstruating women. Serum FSH As shown by several authors, the number of patients and ICTP values were significantly higher in the amenorrheic with adynamic bone disease as a form of uremic osteo- women. Trabecular BMD in the lumbar spine was also signifi- cantly lower in the amenorrheic women compared with regu- dystrophy has increased during the recent years [3]. At larly menstruating dialysis patients. Lumbar spine BMD and the same time, similarities between postmenopausal os- total estradiol levels correlated significantly in the amenorrheic teoporosis and adynamic bone disease of uremia have group. been suggested [4]. Increased plasma levels of bone re- Conclusions. These studies show that persistent amenor- sorpting cytokines [interleukin-1 (IL-1), IL-6, IL-11, and rheic young women on dialysis have lower trabecular BMD and evidence of increased bone resorption when compared tumor necrosis factor-a (TNF-a)] as well as naturally occurring inhibitors of IL-1 and TNF-a have been found in estrogen deficiency and uremic patients undergoing Key words: bone mineral density, osteoporosis, menopause, anovolua- tory cycles, estrogen replacement. hemodialysis or continuous ambulatory peritoneal dial- ysis [5–12]. In addition, sex steroids act directly on the Received for publication September 8, 1999 parathyroid gland to increase parathyroid hormone and in revised form December 30, 1999 Accepted for publication January 24, 2000 (PTH) mRNA at physiological relevant doses [13]. Therefore, women on dialysis could have an increased 2000 by the International Society of Nephrology 331
Transcript of Role of persistent amenorrhea in bone mineral metabolism of young hemodialyzed women

Kidney International, Vol. 58 (2000), pp. 331–335
Role of persistent amenorrhea in bone mineral metabolism ofyoung hemodialyzed women
JOSE R. WEISINGER, LEYDA GONZALEZ, HECTOR ALVAREZ, EDDY HERNANDEZ,RAUL G. CARLINI, FREYA CAPRILES, MERCEDES CERVINO, RUBY MARTINIS,VIRGILIO PAZ-MARTINEZ, and EZEQUIEL BELLORIN-FONT
Division of Nephrology, Hospital Universitario de Caracas, Universidad Central de Venezuela and Fresenius Medical Care ofVenezuela, Caracas, Venezuela
with normal menstruating women on dialysis. The possibleRole of persistent amenorrhea in bone mineral metabolism ofimpact of these results in the natural history of the uremicyoung hemodialyzed women.osteodystrophy remains to be determined.Background. Chronic renal failure in women is frequently
associated with endocrine disturbances leading to menstrualdisorders. However, most studies on renal osteodystrophy havenot taken into account the possible role of these hormonal
The term renal osteodystrophy has been widely ac-disturbances on the pathogenesis of bone alterations seen incepted to define the bone lesions associated with chronicthese patients. In the present study, we evaluated bone mineral
metabolism in a group of young hemodialyzed women with renal failure. It includes diseases that affect the controlpersistent amenorrhea and compared them with similar women of bone remodeling, such as high turnover bone diseasewith regular menstruation. caused basically by secondary hyperparathyroidism orMethods. We studied 74 women who were further subdi-
low turnover in the form of adynamic bone disease andvided into 43 women with regular menstrual periods and 31women with persistent amenorrhea, defined as the absence of osteomalacia, usually associated to vitamin D deficiencymenstrual bleeding for more than six months. In all patients, or aluminum toxicity [1]. However, little concern haswe performed a bone mineral density (BMD) analysis and been given to the possible role of estrogen deficiency insimultaneously evaluated different biochemical parameters, in-
the pathogenesis of uremic bone disease. Indeed, sincetact parathyroid hormone (iPTH), sexual hormone determina-renal osteodystrophy develops at a faster rate and repre-tions that included total estradiol, follicle-stimulating (FSH),
and luteinizing hormone and markers of bone resorption such sents a major clinical problem, it has dominated theas the procollagen type 1 cross-linked carboxy-terminal telo- contribution that postmenopausal osteoporosis couldpeptide (ICTP). have in the bone alterations observed in the female ure-Results. Serum calcium, phosphorus, and iPTH were similar
mic patient. This is particularly important since uremicin both groups. Serum alkaline phosphatase was higher inwomen frequently have early menopause or anovulatoryamenorrheic women. Although the total serum estradiol con-
centration was normal in the amenorrheic women when com- cycles with hypoestrogenism, an important hormonal al-pared with nonuremic women, the values were significantly teration frequently associated with osteoporosis [2].lower than those in regularly menstruating women. Serum FSH
As shown by several authors, the number of patientsand ICTP values were significantly higher in the amenorrheicwith adynamic bone disease as a form of uremic osteo-women. Trabecular BMD in the lumbar spine was also signifi-
cantly lower in the amenorrheic women compared with regu- dystrophy has increased during the recent years [3]. Atlarly menstruating dialysis patients. Lumbar spine BMD and the same time, similarities between postmenopausal os-total estradiol levels correlated significantly in the amenorrheic teoporosis and adynamic bone disease of uremia havegroup.
been suggested [4]. Increased plasma levels of bone re-Conclusions. These studies show that persistent amenor-sorpting cytokines [interleukin-1 (IL-1), IL-6, IL-11, andrheic young women on dialysis have lower trabecular BMD
and evidence of increased bone resorption when compared tumor necrosis factor-a (TNF-a)] as well as naturallyoccurring inhibitors of IL-1 and TNF-a have been foundin estrogen deficiency and uremic patients undergoingKey words: bone mineral density, osteoporosis, menopause, anovolua-
tory cycles, estrogen replacement. hemodialysis or continuous ambulatory peritoneal dial-ysis [5–12]. In addition, sex steroids act directly on the
Received for publication September 8, 1999parathyroid gland to increase parathyroid hormoneand in revised form December 30, 1999
Accepted for publication January 24, 2000 (PTH) mRNA at physiological relevant doses [13].Therefore, women on dialysis could have an increased 2000 by the International Society of Nephrology
331

Weisinger et al: Early amenorrhea and bone in hemodialysis332
Table 1. Age, time on dialysis, and duration of renal disease inrisk for renal bone disease and postmenopausal osteopo-normal menstruating and persistent amenorrheic women
rosis. To further evaluate the possible relationship be-Menstruating Persistenttween estrogen levels and changes in bone mass in hemo-
women amenorrheadialyzed women, we compared a group women withNumber of patients 43 31persistent early amenorrhea with aged-matched men-Age years 35.469.2 38.268.9
struating women under similar conditions of dialysis Time on dialysis months 59.1646.3 53.8639.1Duration of renal diseasetreatment.
months 87.7671.4 85.77666.7Duration of amenorrhea
months — 48.4638.9METHODS
Patients
One hundred twenty-seven women were evaluatedTable 2. Serum biochemical parameters in menstruating andfrom a total of 276 patients under treatment in the dial-
persistent amenorrheic womenysis units of the University Hospital of Caracas and Fre-senius Medical Care of Venezuela. Of these, 74 (58.3%) Menstruating Persistent
Serum values women amenorrheawere younger than 50 years and were subdivided in twoCreatinine mg/dL 13.763.2 10.364.1groups: one with regular menstrual periods (N 5 43)Calcium mg/dL 9.1660.78 9.3561.23and the other with persistent amenorrhea, defined as thePhosphorus mg/dL 5.861.9 5.361.8
absence of menstrual bleeding exceeding a period of Alkaline phosphatase IU/L 136.56128 321.26112a
Estradiol pg/mL 315.4641.8 98.25624.1btime of six months (N 5 31). None of the patients hadFSH mL U/mL 12.7627.3 29.7632.4cprevious evidence of diseases, other than chronic renalLuteinizing Hormone mL U/mL 21.03641.9 30.1633.8
failure, that could affect bone metabolism. Patients who iPTH pg/dL 582.86387 5216465ICTP lg/L 50.1569.4 72.52614.8drecently had been treated with estrogen, progesterone,
corticosteroids, anticonvulsants, fluoride, bisphospho- Abbreviations are: FSH, follicle stimulating hormone; iPTH, intact parathy-roid hormone; ICTP, procollagen type-1 cross-linked carboxy terminal telopep-nates, or calcitonin were excluded from the study. Antide.
informed consent was obtained from all subjects. aP , 0.01; bP , 0.001; cP , 0.01; dP , 0.05
Biochemical assays
Serum levels of total calcium, phosphorus, alkalineStatistical analysisphosphatase, blood urea nitrogen, and creatinine were
analyzed by standard photometric methods. Hormone Results are presented as mean 6 SD. Comparisonsbetween two groups of data were performed by Student’slevels of total estradiol, follicle-stimulating hormone
(FSH), and luteinizing hormone (LH) were assayed by t-test for unpaired observations (two-tailed). Compari-chemiluminescence with an Elecsys 1010 (Boehringer sons between two variables were performed by linearMannheim GmbH Diagnostic, Mannheim, Germany). regression analysis. A P value of , 0.05 was consideredIntact PTH was determined by an immunoradiometric significant.assay (Nichols Institute Diagnostics, San Juan Capis-trano, CA, USA). A serum marker of bone resorption,
RESULTSprocollagen type 1 cross-linked carboxy-terminal telo-From 127 women on dialysis, 53 were postmenopausalpeptide (ICTP), was analyzed by radioimmunoassay
and older than 50 years of age (61.7 6 7.9 years). The(Orion Diagnostica, Espoo, Finland).duration of amenorrhea of these women was 174 6 103.9
Bone density measurements months, and only six of them were on regular hormonereplacement therapy (11.3%). All of them were excludedBone mineral density (BMD) of lumbar spine andfrom the study. The remaining 74 women with a meanfemur were performed by dual x-ray absorptiometryage of 36.5 6 9.1 years were included in the study. Pa-(DEXA), with a DPX-L densitometer (Lunar Corpora-tients were separated into two groups: one with regulartion, Madison, WI, USA). The results were expressedmenstrual periods (N 5 43) and the other with persistentin grams and were divided by the projected area of theamenorrhea (N 5 31).bone to derive the BMD in grams per square centimeter.
Mean age, duration of renal disease, time on dialysis,To evaluate patients of different ages, we used the Zand management of renal osteodystrophy were similarscore, which compares the value of every patient within the normal menstruating and amenorrheic womenan age- and gender-matched control population. The(Table 1). The time of untreated amenorrhea in theprecision error of the BMD analysis in our laboratoryamenorrheic group was 48.4 6 38.9 months.was 0.7% for the whole body, 1% for anteroposterior
spine, and 1.7% for the femoral neck. Blood biochemical parameters are shown in Table 2.

Weisinger et al: Early amenorrhea and bone in hemodialysis 333
Table 3. Bone mineral density in lumbar spine (L2-L4) and femoralneck in menstruating and persistent amenorrheic women
Menstruating PersistentBMD women amenorrhea
L2-L4g/cm2 1.16360.07 0.99760.16a
Z score (SD) 0.1260.81 21.1461.2b
Femoral neckg/cm2 0.87960.106 0.82260.124Z score (SD) 20.4560.82 20.7560.99aP , 0.002; bP , 0.006
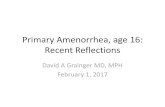
Fig. 2. Bone mineral density (BMD) expressed as the Z score of lumbarspine (L2-L4) and femoral neck in persistent young amenorrheic women( ) and normal menstruating women in dialysis (h).
As shown in Figure 2, there was a significant correla-tion between total serum estradiol and the Z score oflumbar spine BMD in the amenorrheic women (r 5 0.45,P , 0.01). A similar positive correlation was obtainedbetween total serum estradiol and absolute BMD valuesexpressed as g/cm2 (r 5 0.51, P , 0.01).
DISCUSSION
Our results demonstrate that young persistent amen-orrheic women on dialysis have significantly lower tra-
Fig. 1. Correlation between serum concentrations of total estradiol becular BMD and increased bone resorption comparedand BMD expressed as the Z score of lumbar spine (L2-L4) in young
with regular menstruating women under similar condi-women in dialysis (r 5 0.45; P , 0.01).tions of dialysis. The lower levels of estrogens in amenor-rheic women and the correlation between estradiol andlumbar spine BMD suggest that estrogen status may play
Serum creatinine, calcium, and phosphorus were similar an important role in bone mass conservation in uremicin both groups. Serum alkaline phosphatase was higher women.in the amenorrheic women (P , 0.01). The analysis of Most of the gynecological interest in women withthe hormone levels demonstrated lower total estradiol chronic renal failure on dialysis has been related to the(P , 0.001) and higher FSH (P , 0.01) in the amenor- markedly reduced fertility observed in these patients.rheic group when compared with the normal menstruat- Chronic renal failure in women is frequently accompa-ing women, whereas LH was similar in both groups. nied by endocrine disturbances that could lead to men-iPTH values were increased but were nonsignificantly strual, fertility, and other disorders. The postulated causedifferent between groups. Serum levels of ICTP were for these alterations appears to be a defect in the hypo-significantly elevated in the amenorrheic group when thalamic regulation of gonadotrophin secretion, result-compared with the normal menstruating women. ing in lower estradiol peaks, lower FSH/LH ratios, and
Table 3 shows the absolute values of BMD in amenor- a higher prolactin concentration [14]. This could lead torheic and menstruating women. BMD at the lumbar anovulatory cycles and persistent amenorrhea. At thespine was significantly lower in the amenorrheic group same time, hyperprolactinemia has been associated withcompared with menstruating women (0.997 6 0.16 vs. infertility and reduced sexual desire [15]. Dialysis treat-1.163 6 0.07 g/cm2, P , 0.002). Likewise, as illustrated ment does not improve ovarian function, but after ain Figure 1, the Z score that compares BMD in patients successful renal transplant, ovarian function and fertilitywith age- and gender-matched controls was also lower are usually restored.in the amenorrheic group (21.14 6 1.2 vs. 0.12 6 0.81, Women with chronic renal disease are frequently hy-P , 0.006). In contrast, no differences in femoral neck poestrogenic as a result of the disease or its treatment.BMD or Z score between both groups were observed In a recent study, Cochrane and Regan questioned 100
women with chronic renal failure (26 of them on chronic(Table 3).

Weisinger et al: Early amenorrhea and bone in hemodialysis334
dialysis) about different gynecological aspects [16]. Men- effect of hyperparathyroidism [22–24]. The fact thatamenorrheic women had also lower BMD may suggeststrual disorders were present in 85% of the patients.
Menopause was found in one third of the patients, but that the lower estrogen levels may influence bone cellactivity. The adverse effects of hypoestrogenism on boneonly two of these women (6%) were offered hormonal
replacement therapy. This situation was not perceived have been widely recognized. The lack of estrogens isassociated with increased osteoclastic bone resorptionto be a problem by the treating nephrologists. Another
study evaluated 76 women on dialysis who were less probably by a direct effect, as well as by stimulating theproduction of bone resorpting cytokines such as IL-1,than 55 years of age (68% on hemodialysis and 32% on
continuous ambulatory peritoneal dialysis). Of these, 44 IL-6, IL-11, and TNF-a [5–9]. In addition, estrogens mayaffect PTH action by increasing PTH mRNA at the para-women (58%) were amenorrheic, and 21 (28%) were
postmenopausal. In the postmenopausal women group, thyroid gland [13] and modulating the PTH action onbone. Indeed, studies in vitro have demonstrated thatonly one (4.8%) was receiving hormone replacement
therapy [17]. Thus, menopause in women on dialysis estrogen inhibits PTH-stimulated osteoclast formationby directly affecting hemopoietic blast cell precursors byis not managed in the same way as in normal women,
and few postmenopausal women are being offered hor- a cAMP-mediated mechanism [25].Clinical evidence in favor of a role of estrogen inmone replacement therapy. In our group of 53 postmeno-
pausal women, only 6 (11.3%) were on regular hormone uremic bone disease in women has been recently ad-vanced by Matuszkiewicz-Rowinska et al [26]. In theirreplacement therapy. Besides the lack of attention of
the treating physicians, women with end-stage renal fail- controlled study of a small group of postmenopausaldialysis women, the treatment with transdermal estradiolure are usually stoical and rarely complain about gyneco-
logical problems that may seem trivial compared with and cyclic addition of norestisterone acetate significantlyincreased lumbar spine BMD after one year.their renal disease.
Previous studies performed in nonuremic women with Another aspect in which estrogen deficiency couldplay a role is the excessive cardiovascular morbidity andanovulatory cycles demonstrated lower bone mass than
regularly menstruating women [18, 19]. Our young amen- mortality observed in uremic patients. In a recent article,Ginsburg et al demonstrated that hormone replacementorrheic dialysis patients demonstrated significant lower
BMD compared with similar patients with normal men- therapy in 11 postmenopausal women with end-stagerenal disease increased high-density lipoprotein choles-struation, suggesting that estrogen levels could be in part
responsible for the maintenance of the bone metabolism terol significantly to an extent that would be expectedto improve cardiovascular risk profile [27]. The role ofin these subjects. This could be one of the potential
explanations of why women on dialysis had proportion- estrogen replacement therapy in other comorbid condi-tions observed in postmenopausal should be also ad-ately significantly lower BMD when compared with male
patients on dialysis [20]. dressed in women on dialysis.Estrogen therapy in postmenopausal women couldAlthough the levels of estradiol in our young amenor-
rheic women were significantly lower than in normal have several beneficial effects as well as potentially seri-ous risks. Currently, there are no long-term studies inmenstruating patients, they were within normal limits
for normal women. Previous studies have found that uremic women on hemodialysis or continuous ambula-tory peritoneal dialysis that support the recommendationtotal and free estradiol levels are higher at baseline and
after estradiol administration in patients with end-stage of hormone replacement therapy to all postmenopausalwomen. The decision to treat a postmenopausal womanrenal disease when compared with the control popula-
tion, suggesting that renal failure may decrease estradiol on dialysis with estrogens should be based on assessmentof the benefits and risks for that woman and their fullcatabolism and affect the pharmacokinetics of exogenous
estradiol [21]. The role of uremia in the peripheral action disclosure and discussion with her. Women taking long-term unopposed estrogen therapy have an increased riskof this hormone has not been completely defined.
In our patients, serum iPTH was similarly elevated for endometrial carcinoma. As a result, nearly all womenwho have not had a hysterectomy should be treated within both groups. Nevertheless, serum levels of alkaline
phosphatase and ICTP, markers of bone formation and estrogen and progestin.Recent data suggest that as in the case of the femaleresorption, respectively, were significantly greater in the
amenorrheic women, suggesting a higher bone turnover skeleton, estrogens have more relevance than testoster-one in the development or maintenance of the malein these patients. Although there has been demonstra-
tion of a good correlation between ICTP values and skeleton [28]. The role of estrogens in the bone alter-ations of the male dialysis patients remains to be ex-histomorphometric parameters of bone resorption in dif-
ferent metabolic bone diseases, their values could have amined.In summary, the role of persistent amenorrhea on thediurnal variations and in these patients could reflect cer-
tain serum accumulation with renal insufficiency or the bone alterations of young uremic patients should not be

Weisinger et al: Early amenorrhea and bone in hemodialysis 335
tors in undialyzed chronic renal failure, CAPD and hemodialysisoverlooked. Instead, female postmenopausal patients onpatients. Kidney Int 45:890–896, 1993
dialysis should be offered similar treatment opportuni- 12. Kitazawa R, Kimble RB, Vannice JL, Kung VL, Pacifici R:Interleukin-1 receptor antagonist and tumor necrosis factor bind-ties than normal women. More prospective and con-ing protein decrease osteoclast formation and bone resorption introlled studies are needed in this area. The potential ovariectomized mice. J Clin Invest 94:2397–2406, 1994
role of these alterations in the natural history of uremic 13. Naveh-Many T, Almogi G, Livni N, Silver J: Estrogen receptors,and biologic response in rat parathyroid tissue and C-cells. J Clinosteodystrophy should be also clarified in the near future.Invest 90:2434–2438, 1992
14. Lim VS, Henriquez C, Sieversten G, Frohman LA: Ovarian func-tion in chronic renal failure: Evidence of hypothalamic anovula-ACKNOWLEDGMENTStion. Ann Intern Med 92:21–27, 1980
This study was supported by grant G-97-000808 of the Consejo 15. Lim VS, Kathpalia SC, Frohman LA: Hyperprolactinemia andNacional de Investigaciones Cientıficas y Tecnologicas de Venezuela impaired pituitary response to suppression and stimulation inand Fundarenal-HUC. The help of the physicians, nurses, and secre- chronic renal failure: Reversal after transplantation. J Clin Endo-tarial staff of our dialysis units is fully appreciated. crinol Metab 48:101–107, 1979
16. Cochrane R, Regan L: Undetected gynecological disorders inwomen with renal disease. Hum Reprod 12:667–670, 1997Reprint request to Jose R. Weisinger, M.D., Hospital Universitario
17. Holley JL, Schmidt RJ, Bender FH, Dumier F, Schiff M: Gyne-de Caracas, Division of Nephrology, Apartado Postal 47365, Los Cha-cological and reproductive issues in women on dialysis. Am J Kid-guaramos, Caracas, Venezuela 1040.ney Dis 29:685–690, 1997E-mail: [email protected]
18. Prior JC, Vigna YM, Schechter MT, Burgess AE: Spinal boneloss and anovulatory disturbances. N Engl J Med 323:1221–1227,1990REFERENCES
19. Schachter M, Shoham Z: Amenorrhea during the reproductive1. Goodman WG, Coburn JW, Slatopolsky E, Salusky IB: Renal years: Is it safe? Fertil Steril 62:1–16, 1994
osteodystrophy in adults and children, in Primer on the Metabolic 20. Russo CR, Taccetti G, Caneva P, Mannarino A, Maranghi P,Bone Diseases and Disorders of Mineral Metabolism (3rd ed), Ricca M: Volumetric bone density and geometric assessed byedited by Favus MJ, Philadelphia, New York, Lippincott-Raven, peripheral quantitative computed tomography in uremic patients
on maintenance hemodialysis. Osteoporos Int 8:443–448, 19981996, pp 324–36021. Ginsburg ES, Owen WF Jr, Greenberg L, Shea BF, Lazarus2. Lindberg JS, Moe SM: Osteoporosis in end stage renal disease.
M, Walsh BW: Estrogen absorption and metabolism in postmeno-Semin Nephrol 19:115–122, 1999pausal women with end-stage renal disease. J Clin Endocrinol3. Cannata-Andia JB: Hypokinetic azotemic osteodystrophy. Kid-Metab 81:4414–4417, 1996ney Int 54:1000–1016, 1998
22. Garnero P, Shih W, Gineyts E, Karpf D, Delmas P: Comparison4. Silver J, Epstein E, Naveh-Many T: Estrogen deficiency: Doesof new biochemical markers of bone turnover in late post-meno-it have a role in the genesis of skeletal problems in dialyzed women?pausal osteoportic women in response to alendronate treatment.Nephrol Dial Transplant 11:565–566, 1996 J Clin Endocrinol Metab 79:1693–1700, 1994
5. Pacifici R, Rifas L, McCracken R, Vered I, McMurtry C, Avioli 23. Panteghini M, Pagani F: Biological variation in bone-derivedLV, Peck WA: Ovarian steroid treatment blocks a postmenopausal biochemical markers in serum. Scand J Clin Lab Invest 55:609–616,increase in blood monocyte interleukin 1 release. Proc Natl Acad 1995Sci USA 86:2398–2402, 1989 24. Urena P, Vernejoul MC: Circulating biochemical markers of
6. Ralston SH: Analysis of gene expression in human bone biopsies bone remodeling in uremic patients. Kidney Int 55:2141–2156, 1999by polymerese chain reaction: Evidence for enhanced cytokine 25. Kanatani M, Sugimoto T, Takahashi Y, Kaji H, Kitazawa R,
Chichahara K: Estrogen via the estrogen receptor blocks cAMP-expression in postmenopausal osteoporosis. J Bone Miner Res 9:mediated parathyroid hormone (PTH)-stimulated osteoclast for-883–890, 1994mation. J Bone Miner Res 13:854–862, 19987. Jones TH: Interleukin-6 an endocrine cytokine. Clin Endocrinol
26. Matuszkiewicz-Rowinska J, Skorzewska K, Radowicki S, So-40:703–713, 1994kalski A, Przedlacki J, Niemczyk S, Wlodarczyk D, Puka J,8. Jilka RL, Hangoc G, Girasole G, Passeri G, Williams DC,Switalski M: The benefits of hormone replacement therapy in pre-Abrams JS, Boyce B, Broxmeyer H, Manolagas SC: Increasedmenopausal women with oestrogen deficiency on haemodialysis.osteoclast development after estrogen loss: Mediation by inter-Nephrol Dial Transplant 14:1238–1243, 1999leukin-6. Science 257:88–91, 1992 27. Ginsburg ES, Walsh B, Greenberg L, Price D, Chertow GM,
9. Horowitz M: Cytokines and estrogen in bone: Anti-osteoporotic Owen WF Jr: Effect of estrogen replacement therapy on the lipo-effects. Science 260:626–627, 1993 protein profile in postmenopausal women with ESRD. Kidney Int
10. Luger A, Kovarik J, Stummvoll HK, Urbanska A, Luger T: 54:1344–1350, 1998Blood membrane interaction in hemodialysis leads to increased 28. Slemenda CW, Longcope C, Zhou L, Hui SL, Peackock M, John-cytokine production. Kidney Int 32:84–88, 1987 ston CC: Sex steroids and bone mass in older men: Positive associa-
11. Pereira BJG, Shapiro L, King AJ, Falagas ME, Strom JA, Dina- tions with serum estrogens and negative associations with andro-rello CA: Plasma levels of IL-1b, TNFa and their specific inhibi- gens. J Clin Invest 100:1755–1759, 1997