Amenorrhea Mayurasakorn N.. Not physiologic Primary amenorrhea Normal secondary sex characteristic ...
54
Amenorrhea Mayurasakorn N.
-
Upload
henry-blankenship -
Category
Documents
-
view
218 -
download
2
Transcript of Amenorrhea Mayurasakorn N.. Not physiologic Primary amenorrhea Normal secondary sex characteristic ...

Amenorrhea
Mayurasakorn N.
Not physiologic
Primary amenorrheaNormal secondary sex characteristic
no manarche by 16 yearsno periods by 2 years after
start of secondary sex changesIf No secodary sex characteristic
14 years
Secondary amenorrhea
Definitions and EpidemiologyDefinitions and Epidemiology
If regular menstruation : 3 cyclesIf irregular mrnstruation : 6 months
PregnancyBreast feedingMenopause

Hypothalamic causesPituitary causes
Premature ovarian failure(<40 years)
Outflow tractHyperandrogenic anovulation
EtiologyEtiologyHypergonadotropic
hypogonadism
Hypogonadotropic hypogonadism
Normogonadotropic hypogonadism
Secondary AmenorrheaSecondary Amenorrhea

Ovary Pituitary Hypothalamus
Infection /infiltration
Mump Oophoritis
TB,syphilis,Encephalitis/menigitis,Sarcoidosis
Tumor Ovarian tumor
HyperprolactinPituitary tumorEmpty sella
Craniopharyngioma, Germinoma,Hamartoma,Teratoma,Metastasis
Trauma Irradiation Chemotherapy
SurgeryIrradiationSheehan sd
Metabolic Autoimmune AutoimmuneHemochromatosisLymphocytic hypophysis
Anorexia nervosaStressExercise Nutrition-related
Hypergonadotropic hypogonadismHypergonadotropic hypogonadismHypogonadotropic hypogonadismHypogonadotropic hypogonadism
Hyperandrogenic anovulationPCOSAndrogen-secreting tumorCushing’s sdNonclassical congenital adrenal hyperplasiaThyroid
Outflow tractAsherman syndromecervical stenosis
Normogonadotropic hypogonadismNormogonadotropic hypogonadism

Hypothalamus :25-35%
PCOS: 20-25%
Ovarian : 12%
Hyperprolactinemia : 13%
Pituitary : 7-16%
Uterine : 7%
other
Most common causesMost common causes

Hypothalamus
Stress, wt loss, diet ,exercise, illnessChemotherapy,radiation
GalactorrheaDrugs( metoclopramide,
anti-psychotics?)
Headaches, visual field defects, fatigue, polyuria, polydipsia
Chemotherapy,radiation
Hot flashes, vaginal dryness, poor sleep,decreased libido
Hyperprolactinemia
Ovary
History & Physical examinationsHistory & Physical examinations
Pituitary

Hypothalamus
Hyperprolactinemia
Ovary
History & Physical examinationsHistory & Physical examinations
Pituitary
Signs of systemic illness ,cachexia
Breast : galactorrhea
Bitemporal hemianopia

PCOS
History & Physical examinationsHistory & Physical examinations
Hirsutism, acne, history of irregular menses
Obstetrical catastrophe, severe bleeding, dilatation and curettage, endometritisBMI,hirsutism, acne, striae, acanthosis nigricans, vitiligo
Virilization, clitorial hypertrophy

PCOS
History & Physical examinationsHistory & Physical examinations
Hirsutism, acne, history of irregular menses
Obstetrical catastrophe, severe bleeding, dilatation and curettage, endometritis

PRL FBSProgesterone estrogen challengeUrine BhCG KaryotypeAntithyroid antibody FSHProgesterone challengeDHEA-S and testosterone TSH
ข้�อใดไม่�ใช่� Investigations ข้อง Amenorrheaข้�อใดไม่�ใช่� Investigations ข้อง Amenorrhea

HypothalamusHyperprolactinemia
Ovary
Pituitary
PCOS
Outflow tract
Cushing’s sd
Thyroid
MRI hypothalamus, pituitary
FSH,LH, autoimmune
MRI pituitary
U/S ovary,testosterone
Dexamethasone supression testThyroid function test
prolactin
Hysterosalpingogram,hysteroscopy
InvestigationsInvestigations

Pregnancy test
TSH ,PRL,FSH
TSH
Hypothyroid
PRL
Hyperpro-lactinemia
FSH
Premature
ovarian failure
Hypogonadotropic Normogonadotropic PCOS
Outflow
Clinical
PRL > 40 mg/dL
FSH > 40 mIU/mL

High false positive, false negativeDelay diagnosis
Primolut-N (Norethisterone acetate) 5-10 mg ODProvera (Medroxyprogesterone acetate) 10 mg OD 5 days
withdrawal bleed within 2 weeks
Progesterone challenge test
Estrogen progesterone challenge test
Premarin (conjugated E)1.25 mg OD Progynova(Estradial) 21 days followed by provera as above

Prog.challenge test
Withdrawal bleeding
No withdrawal bleeding
Chronic anovulation
Testosterone, DHEA-S,17 hydroxyprogesteroneTestosterone, DHEA-S,17 hydroxyprogesterone
T,DHEA-S,LH
mild
PCOS
T,DHEA-S
marked
Androgen-secreting
tumor
17-hydroxyprogesterone
CAH Idiopathic anovulation

No withdrawal bleeding
Est,progest.challenge test
Hypothalamic-
pituitary failure
Hypothalamic-
pituitary failure
hypoestrogenic
outflow tract .
Withdrawal bleeding
No
Prog.challenge test

1% population40% autoimmune ass autoimmune
Autoimmune thyroiditisIDDMParathyroid diseaseMGAddison’s disease(1:million)
Polyglandular sd20-40% develop other autoimmune disease
Premature ovarian failurePremature ovarian failure
TSH, thyroid autoAb FBS Ca,PO4
Karyotype : if < 30 for Y chromosome remove gonad
HyperprolactinemiaHyperprolactinemia< 100 ng/mL(µg/L)
Altered metabolism: liver failure, renal failureEctopic production : BCA,renal cell CA , ovarian dermoid cyst,teratomaHypothyroidDrugs: OC,antipsychotic, antidepressant,antihypertensive,opiate,cocain,H2 blokerPituitary stalk irritability
> 100 ng/mL(µg/L)Empty sella syndromeProlactinoma

Discovery and treatment of underlying disorderHormone replacement
for maintain secondary sex characteristic Normal menses every 1-3 months
reduce risk of osteoporosis
Adequate caloric intake
Calcium 1200 to 1500 mg/D
Vitamin D (400 IU daily)Pregnancy
Ovulation inductionGnRH pumpFSH/LH
Treatment GoalsTreatment Goals

Chromosomal abnormality:20%Ovarian failure: 15%
46 XY :5%
Mullerian agenesis : 10%
Androgen insensitivity : 9%
Constitutional delay: 8%
Constitutional delay
Prolactinoma: 5%
Kallman, Stress, PCOS
Breast
30%
High FSH
40%
Low FSH
30%
Primary AmenorrheaPrimary Amenorrhea
HistoryHistoryNormal physical & pubertal development?
Family history of delayed/absent menarche?Short stature compared to family members?
Neonatal/childhood health normal? any recent increase in stress, or change in weight, diet, or exercise habits?
Hypothalamic-pituitary disease (headaches, visual field defects, fatigue, polyuria or polydipsia?)
Drugs?

Physical examinationPhysical examination
Height, weight
Secondary sex characteristic (Tanner staging)
PV for cervix, uterus, ovaries (may need ultrasound)
Androgen excess (acanthosis nigras, hirsutism, acne, & striae)
Turner syndrome (low hair line, web neck, shield chest, and widelyspaced nipples)
Galactorrhea?

Secondary sex characteristicSecondary sex characteristic
Thelarche (breast devel): average age 10.8 yrs estrogen exposure
Adrenarche (pubic/axillary hair development): average 11 yrs ovarian,adrenal androgen
production ,end organ responseDecreased breast size or vaginal dryness
decreasing estrogen exposure (or increasing androgens)

Tanner StagingTanner Staging
Stage 1 : prepubertal
Stage 2 : breast bud
Stage 3 : further enlarge of breast
& areolar ,no seperation
Stage 4: areolar & papilla form
second mound
Stage 5 : mature, only projection of
papilla
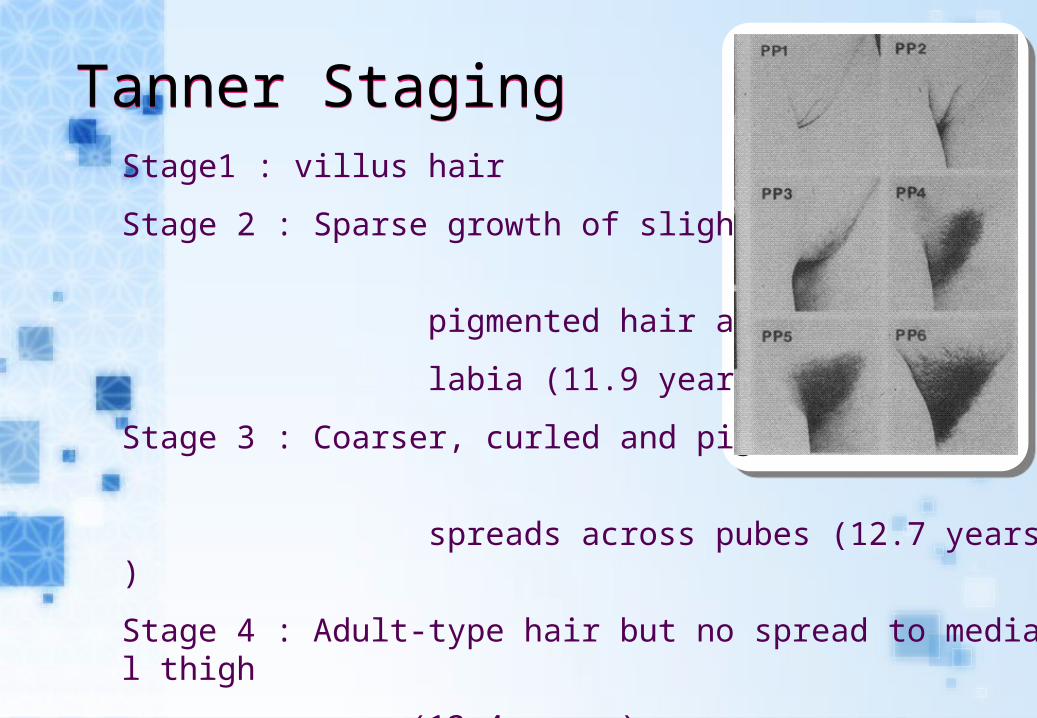
Tanner StagingTanner StagingStage1 : villus hair
Stage 2 : Sparse growth of slightly
pigmented hair along
labia (11.9 years)
Stage 3 : C oarser, curled and pigmented;
spreads across pubes (12.7 years)
Stage 4 : - Adult type hair but no spread to medial thigh
(1 3 .4 years)
Stage 5 : - Adult type hair with spread to medial thigh but not up linea alba (14.6 years)

Secondary sex characteristic
No Yes
Pubic hair
Yes
Uterus
No
Androgen insentivity syndrome
Androgen insentivity syndrome
Imperforate hymen
Imperforate hymen
Yes NoMullerian agenesis
Mullerian agenesisAs secondary
amenorrhea
PV

Secondary sex characteristic
No ( normal cervix and uterus
not include ambiguous )FSH
E
Primary Gonodal failure
Primary Gonodal failure
Constitutional delay
Kallman sd
Hypothalamus-pituitary
Hypothalamus-pituitary
Karyotype
XX,XY,XO

Primary gonodal failurePrimary gonodal failure
Gonodal dysgenesis
less than 30ykaryotypeif Y chromosome exists, excise gonadsif 46XX, r/o 17a-hydroxylase deficiencyIf XOTurner sd
Premature ovarian failure
Time Before thelarche Before menarche After menopause
AutoimmnueLaboratory evidence of autoimmune is much more prevalent than clinically significant disease

CNS, hypothalamic, or pituitary failureConstitutional delayHypothalamic dysfunction
Kallmann syndromeAnorexia nervosa, exercise induced; Space-occupying lesion of CNS
Pituitary damage (surgery/radiation)Hyperprolactinemia
Hypogonadotropic hypogonadismHypogonadotropic hypogonadism

Mullerian agenesisMullerian agenesisnormal gonad hormone
but no uterus and upper vagina
Embryonal activation of antimullerian hormone
15-30% ass. urogenital malformation : unilateral renal agenesis, pelvic kidney, horseshoe kidney, hydronephrosisIVP
Cyclic breast tenderness or pain in rudimentary uterus
karyotype R/O male pseudohermaphrodism

1:60,000, XR mutation of androgen receptorKaryotype 46, XYMale range testosterone levelNormal breasts but no sexual hairNormal looking female external genitaliaOccasional present of inguinal massAbsent uterus and upper vagina by AMHRisk gonodal malignancy 20%Raised as girls (XY)
remove gonads after breast development and epiphyseal closurereplace estrogen
Complete androgen insensitivity syndromeComplete androgen insensitivity syndrome

Imperforate hymenImperforate hymen

Discovery and treatment of underlying disorderRemove gonadal streaks if XY or mosaic
Increased (52%) risk of gonadoblastomas, dysgerminomas, and yolk sac tumors
Hormone replacement for maintain secondary sex characteristic and reduce risk of osteoporosis
adolescent: low dose E breast augmentationThen progestin normal menses every 1-3 monthsPregnancy
Ovulation inductionPulsatile GnRH FSH/LH
Treatment GoalsTreatment Goals

17 yo female with primary amenorrhea
Normal pubertal development
Normal health
No family history of delayed puberty
Not involved in athletics
Does well in school
Not taking any meds
Case 1:Case 1:

Physical Examination
Thin young woman )10% below IBW)
Normal genitalia
No galactorrhea
Tanner stage 4
Laboratory values
Urine and serum B-HCG negative
Prolactin, FSH, TSH all normal

Further history
Patient’s parents concerned about her eating habits (very low fat intake and restricting calories)
Diagnosis : hypothalamic amenorrhea
Etiology is most likely inadequate caloric and fat intake.
referred for evaluation for an eating disorder.

Psychological stress, weight changes,exerciseChronic debilitating diseaseCompetitive sport : 3-fold risk of amenorrhea
Esp: long distance runnersRx
correct causesAdequate intakeLess exerciseOC???
Hypothalamic amenorrheaHypothalamic amenorrhea

24 yo woman with secondary amenorrhea
Menarche at age 12
Periods have always been irregular
Now amenorrhea x 10 months
Overweight
Wants to get pregnant
Case 2:Case 2:

Physical Examination
Obese femaleAcneNormal genitaliaMild hirsutism

Urine B-HCG negativeTSH, FSH and Prolactin : WNL Testosterone 180 ng/dLPelvic U/S
Laboratory findings

PCOS : Polycystic Ovarian SyndormePCOS : Polycystic Ovarian Syndorme
Etiology unknown Reduce insulin sensitivity 30-40% : Increase secretion LH
Hyperinsulin or LH Theca cell androgen disturb hypothalamus& ovary anovulation

PCOS : Polycystic Ovarian SyndormePCOS : Polycystic Ovarian Syndorme

Menstrual disturbance (DUB,oligomenorrhea (76%), amenorrhea(24%)
Symptom onset at menarche but sign androgen excess obvious several years laterDifferential diagnosis :
Androgen-secreting tumor(ovarian or adrenal)Cushing’s sdNonclassical congenital adrenal hyperplasia
Thyroid Excess estrogen
Increased risk endometrial cancer threefold
Hyperandrogenic anovalationHyperandrogenic anovalation

Metabolic complicationMetabolic complication
Impaired glucose tolerance:31%Impaired fasting glucose 7.5%DM : 2-5 folds test OGTTCardiovascular risk 2 folds Metabolic syndrome 43%

2/3Chronic anovulation HyperandrogenismU/S : polycystic ovaries
Exclude other causes20% of woman with regular menses have polycystic ovaryLH/FSH> 2 , not useful in diagnosis
NIH criteriaNIH criteria

TreatmentTreatmentShort-term management
InfertilityHirsutismAcneObesityMiscarriage
Long-term managementCardiovascular risks
CholesterolDiabetesblood pressure
Endometrial Cancer

weight reductionlower androgen level , improve hersutism, normalize menses , decrease insulin resistance
Anovulation & Infertility: Clomiphene , GnRH, Metformin
RCOG guidline 2003
Protection endometrial CA: Oral contraceptive or Cyclic progestin to prevent : monthly 10-14 day regimen
AntiandrogenCyproterone acetate (Diane-35)Drospirenone ( Yasmin)

34 Years with secondary amenorrhea 19 years
Menarche at age 15
Only 2 cycles
Short stature
Case 3:Case 3:


Turner SyndromeTurner Syndrome

Classic 45,X other :
46,X ,i(Xq)46,X,Xq-46,X,Xp-46,X,r(X)45,X/46,XX
Time of diagnosis

Ischemic heart diseaseType 2 DMosteoporosisCirrhosisType 1 DMDilated ascending aortaThyroiditis
ข้�อใดไม่�ใช่� Risks ข้องผู้��ป่�วย turner syndromeข้�อใดไม่�ใช่� Risks ข้องผู้��ป่�วย turner syndrome
HypothyroidismCoartation of aortaFracture Type 1 CA colonHypertensionHorseshoe kidney
CardiovascularRecord BP, BMIEchocardiogram q 3-5 yearsFBSFasting lipid
Renal ultrasoundRenal and liver functionThyroid status & antibodyBMDAortogram

TreatmentTreatmentChildren : Growth hormone
adequate height, phychological demand, may spontaneous menseEstrogen maintian secondary sex characteristicBone massCycle progesteroneFertility
Oocyte donationOocyte implantation from cryopreservation