
Foods or Bioactive Constituents of Foods as Chemopreventives in Cell Lines After Simulated
Upload
drshifaya-nasrinCategory
view
56download
1
BIOMARKERSAND
CHEMOPREVENTIVES IN ORAL CARCINOGENESIS
Presented by
SHIFAYA NASRIN.S
INTRODUCTION
Oral carcinogenesis is a multi factorial and complex process related
to the sequential occurrence of alterations in genetic structures,
promoting inhibitory or excitatory effects of the tumor on and gene
suppressors, compromising the histophysiology of the division
,differentiation and cell death; and therefore, methods to prevent,
detect, or treat it in the best way is constantly being searched for.
Biomarkers reveal the genetic and molecular changes related to
early, intermediate and late endpoints in the process of oral
carcinogenesis
BIOMARKERS,……
• The national cancer institute defines biomarker as a : A biological
molecule found in blood ,other body fluids or tissues that is a sign of a
normal or abnormal processor of a condition or disease
• A biomarker may be used to how well the body responds to a
treatmentfor a disease or condition
• Also called molecular marker and signature molecule
WHERE DOES THIS TUMOUR MARKERS SEEN…….?
Cells
Tissue
Body fluids
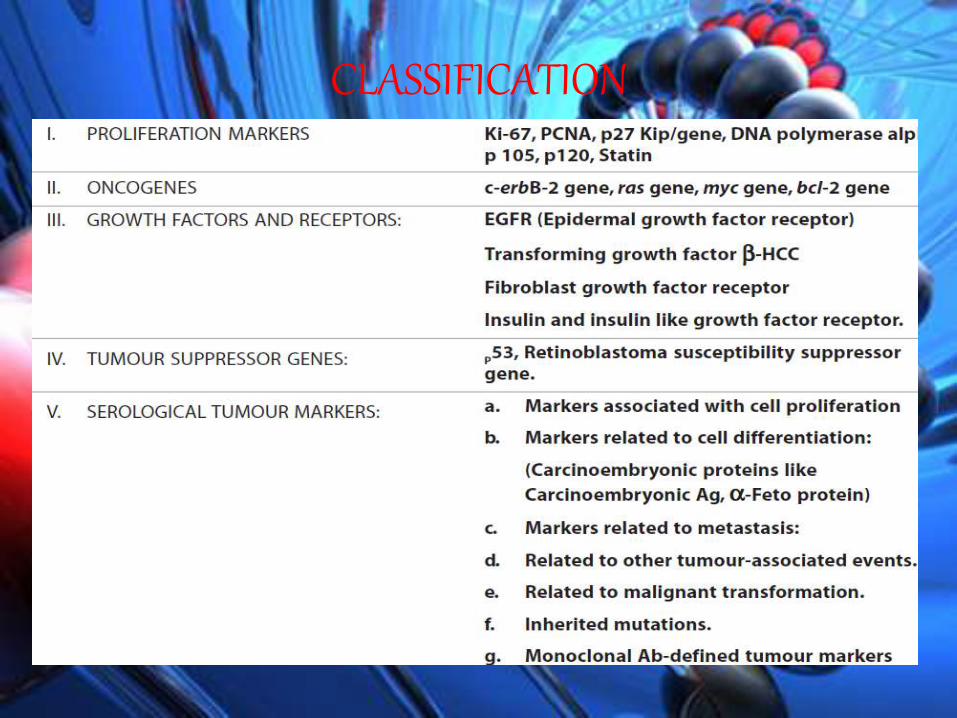
CLASSIFICATION
CONCEPT OF IDEAL TUMOUR MARKER
• Be easy and and inexpensive to measure
• Readily available in body fluids
• Be specific to tumour being studied and commonly
associated with it
• They should change as current state of tumour changes
• Precede and predict recurrence before clinically
detectable
USES OF BIOMARKERS
DIAGNOSTIC
PROGNOSTIC PREDICTIVE

ROLES OF CELLULAR BIOMARKERS
Indicators of deoxyribonucleic acid (DNA) repair
mechanisms
Indicators of programmed cell
death (PCD)
Indicators of tumor
development and growth
Indicators of genetic markers of oral cancer.
INDICATOR OF DNA REPAIR
• Cancer cell require high level of DNA repair
• Repair of the telomeric ends of chromosomes produced
through the action of telomerase and repair of
nucleotide sequences, exemplified by mismatch repair
and nucleotide excision repair (NER).
• In human oral carcinomas, telomerase is elevated in the
proliferative areas of the carcinoma
• DNA repair influence the
progression of oral
carcinogenesis through the
regulation of various growth
factors .e.g; transforming growth
factor -Β3
• Development of DNA repair
defect and development of
mutated TGF-Β3
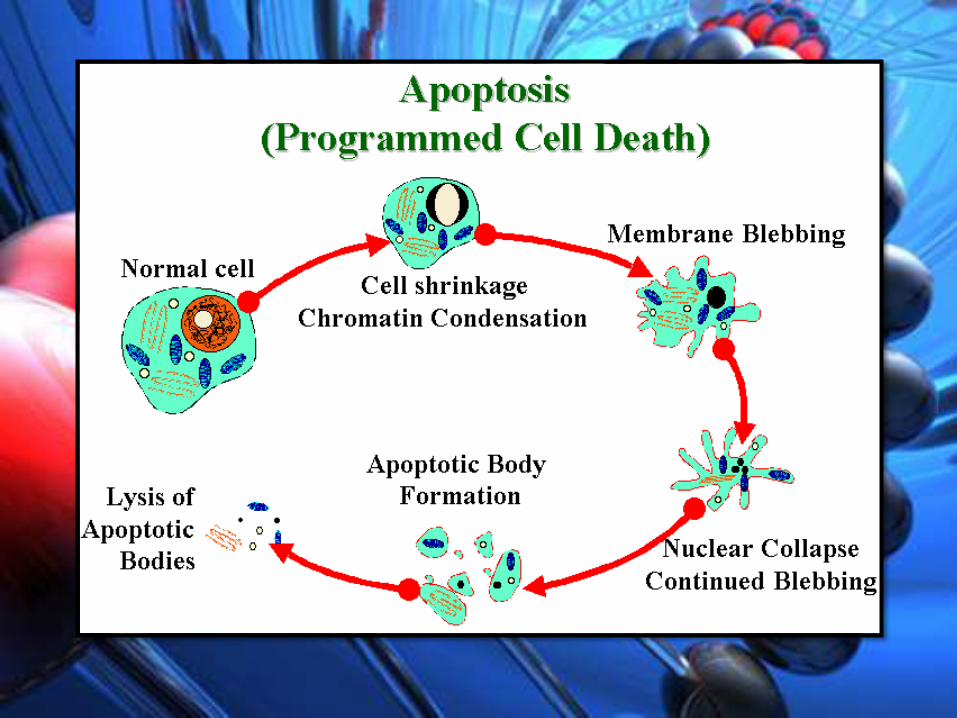
INDICATOR OF PCD
• PCD gene directed apoptosis- remove unwanted cells
• Plays an important screening role in cancer formation.
• It results in the modification of surviving cell population in
transforming clones by altering the number and type of cell
in a tumor
• Surviving transforming cells :
suppresed PCD
high rate of proliferation
Elevated level of DNA repair
OXIDATION AND EFFECT ON PCD
• ORAL MALIGNANT TRANSFORMATION, a product of
oxidising change
• Oxidative change result in changes in DNA repair and PCD
• Cellular manifestation of this processs :
Loss of cell growth control
modification in cell to cell interaction
enhance tumor metastasis.

CHEMOPREVENTIVE AND PCD
This alter the oxidative state of oral transforming cells as
reducing agent( antioxidant)
Oxidising agent(prooxidant)
These agent induce PCD by there oxygen responding charateristic which
trigger such as
Tumor suppressor gene p53
Modifiers of PCD –BCL2 family,
gene immune derived cytokins( TNF)
Examples of chemopreventive : retinoids , carotinoids, tocopherols,
bioflavonoids , isothia cyanates, indole, poly phenol
INDICATORS OF TUMOR DEVELOPMENT AND GROWTH
• Biomarkers establish the level of risk for individuals in a
target group of patients and provide information
concerning the etiology and the process of
carcinogenesis.
• The primary goal for the use of early, intermediate and
late biomarkers is to identify individuals at risk of
developing malignancy and indicate their level of risk.
INDICATORS OF GENETIC MARKERS OF ORAL CANCER
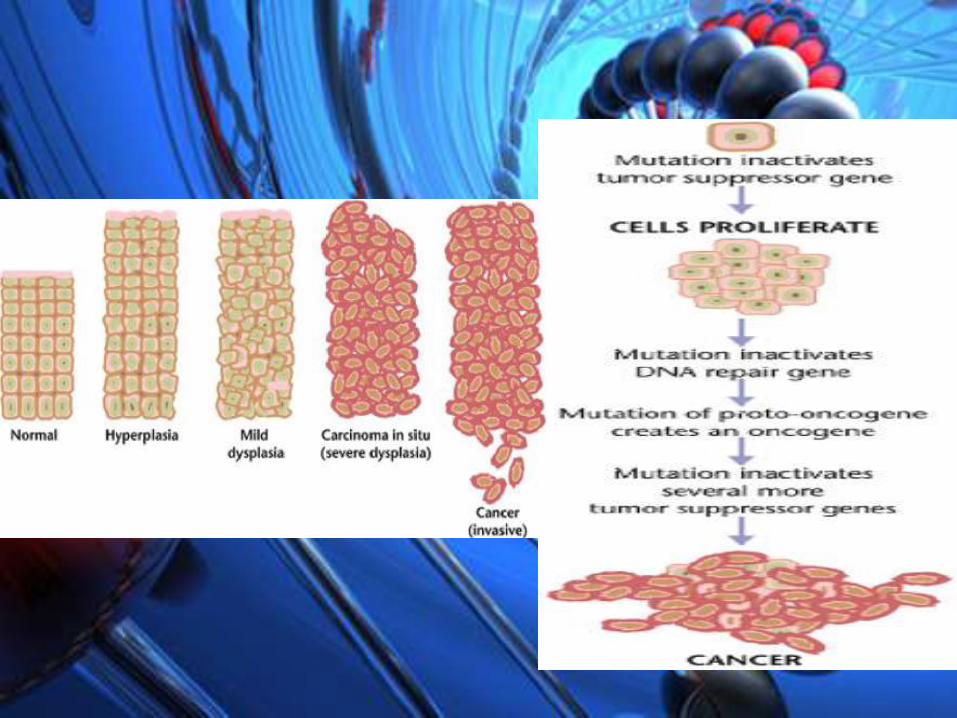
• A developing solid clone of transforming cells found in an
oral carcinoma arrives at the state of malignancy by
proceeding through stages of transformation
• The transformation rate is dependent on the location of the
clone in the spherical tumor mass and the oxygen states of
the cells
Specific tumourmarkers implicated in oral neoplasms
Alpha-1-antichymotrypsin (1-ACT) & factor XIIIa antibodies:
giant cell lesions of the oral cavity may arise from
precursor cells that express markers for both
macrophages and osteoclasts
BCL2
• Squamous Cell Carcinoma of head and neck.
• The predictive role in terms of pathological response and prognostic role of biomarkers such as
GST-pi,(glutathione-s-transferace)
p53,
bcl-2 and bax expression,
• immune-histochemically detection of the S-phase cell fraction,
Beta 2-Microglobulin
• increase in the level of beta 2- microglobulin -oral submucous fibrosis and oral cancer.
CD44, CD80, CD105 (ENDOGLIN):
• HA and CD44 among different types of salivary gland
tumours,
• In oral SCC’s decreased expression of CD80 may increased
tumourigenicity during early development
• decreased expression of CD44 -decreased survival rate.
• endoglin (CD105) - neovascularization in solid malignancies
• positive CD105 - vessels in Adenoid cystic carcinomas -
increases risk of metastasis.
Cytokeratins:
• useful for evaluation of epithelial differentiation changes in
oral dysplasia’s and oral SCC.
• CK19 and CK8 - premalignant changes in head and neck
carcinogenesis.
• Non expression of CK5 -tobacco-associated
pathological changes in the buccal mucosa.
• CK filaments -reflect the biological behavior and
aggressiveness of tongue SCCs
Cathepsin-d
• promote tumour invasion and metastasis.
• predictor of cervical lymph node metastasis in
Head and Neck SCC.
CEA, CA19-9, CA125, SCC-Ag:
• oral squamous cell carcinoma (OSCC) patients- increase in
Cyfra 21-1, tissue polypeptide antigen, and CA125
Carbohydrate associated antigens
• regarded as markers of glandular differentiation
pattern in salivary gland carcinomas
Calretinin
• Immunohistochemical marker for neoplastic
ameloblastic epithelium
• diagnostic aid in the differential diagnosis of cystic
odontogenic lesions and ameloblastic tumours
Growth factors
• Vascular endothelial growth factor (VEGF) -angiogenic factor
associated with cancer cells and endothelial cells in SCCHN
• VEGF-C or LVD (lymphatic vesseldensity)-lymphatic
metastasis of oral SCC.
• Basic Fibroblast growth factor (FGF) has relevance for
advanced head and neck cancer
cyclins and Mib
• Proliferation markers cyclins and Mib - basal and
superficial cells of premalignant lesions serve as
surrogate end point biomarkers for chemoprevention
trials
P53
• p53 -high risk of developing recurrence of primary disease69 and
second primary tumours of SCCHN who may benefit from
adjuvant therapy and chemoprevention after definitive local
therapy.
• predict radioresistance of the tumours.
• Preoperative serum p53 antibody is a significant
prognostic factor for nodal metastasis of SCCHN

CHEMOPREVENTIVES
• CHEMOPREVENTIVES are chemicals of natural or
synthetic origin which unlike other drugs do not
prevent disease but reduce incidience of disease
such as cancer before clinical syndromes occur
• High dose retinoids- active against oral premalignant
lesions and in prevention of second primary tumor
in head and neck
Rationale for pharmacological prevention of in patients risk
for development of invasive cancer based on
• Field canceirzation
• multi step carcinogenesis.
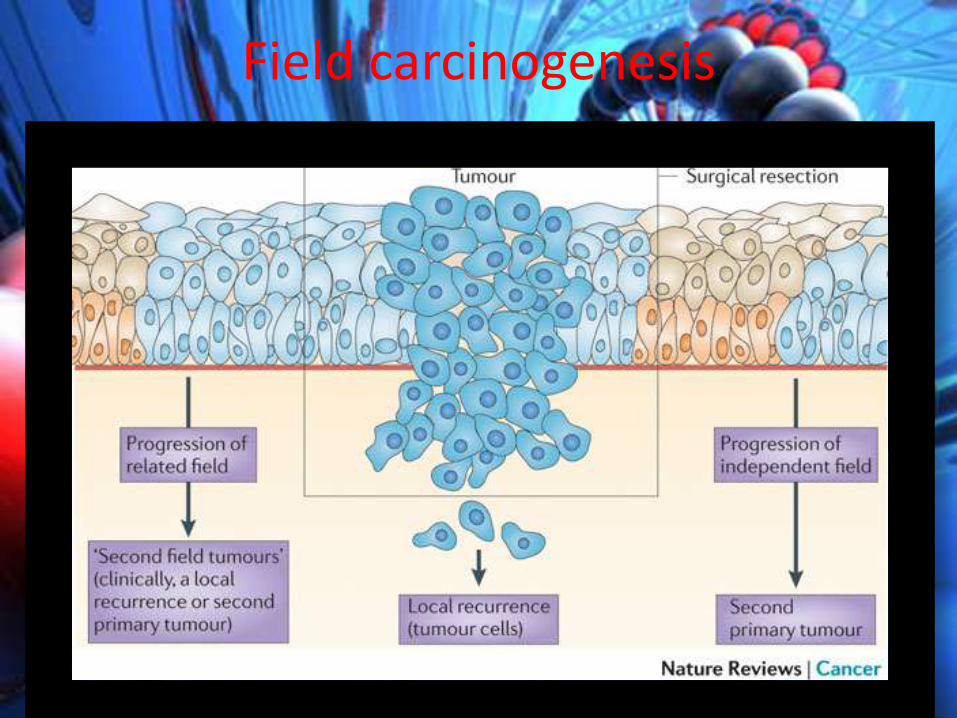
Field carcinogenesis
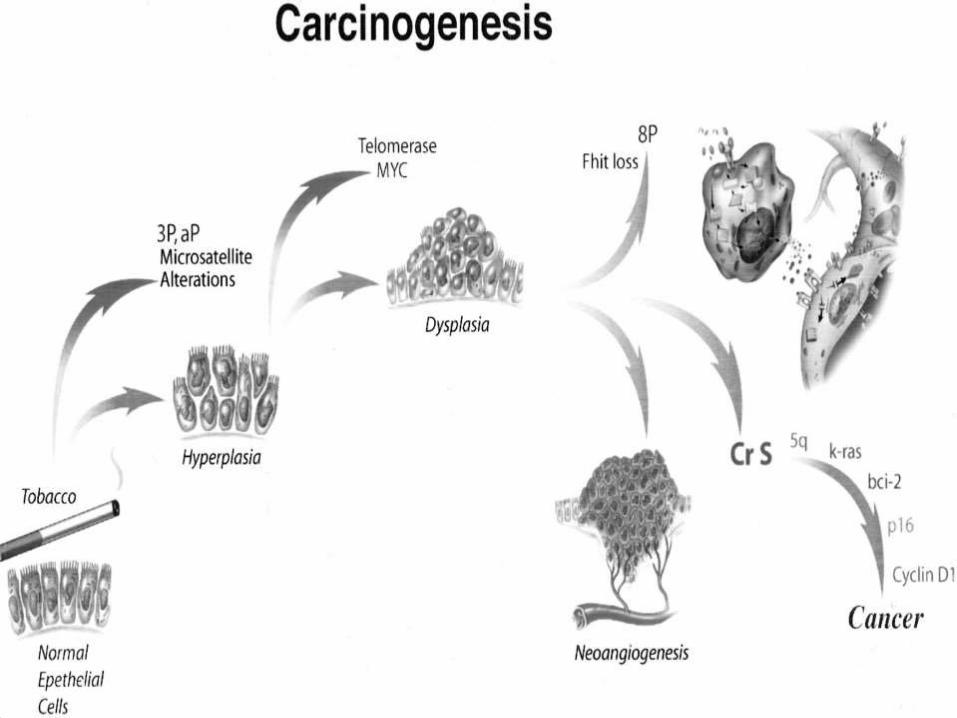
Multistep carcinogenesis
CLASSIFICATION OF CHEMOPREVENTIVE AGENTS
1. Antimutagens/Carcinogen Blocking Agents• Phase II metabolic enzyme inducers• N-acetyl L-cysteine• Polyphenols• Curcumin and dehydroepiendrosterone (DHEA).
2. Antiproliferatives• Retinoids/caretinoids: β-carotene, 13-cis-retinoic acid,
vitamin-A• Glucose-6-phosphate dehydrogenase inhibitors• Aspirin.[11]
3. Antioxidants.

COMMONLY TRIED CHEMOPREVENTIVE AGENTS IN ORAL
CANCER• Vitamin A and other retinoids
• β-carotene
• Vitamin E
• Dietary agents
• Other agents
…Β-CAROTENE• carotenoid, acts as an antioxidant,• also act as a pro-oxidant, depending on the oxygen
state of the cell.• β-carotene as well as ellagic acid (from garlic) are
carcinogen-blocking agents that either suppress promotion or act as antioxidants, which are reducing agents.
• mechanism of action - prevent carcinogenic compounds from reacting with critical target sites of DNA by inhibiting the metabolic activation of carcinogens catalyzed by cytochrome P450 (Phase I enzymes
δλ -ALPHA-TOCOPHEROL (VITAMIN E):
• are strong antioxidants that enhance the cellular
detoxification system by increasing the levels of
glutathione-S-transferases (GSTs; Phase II enzymes).
• The activation of these enzymes may also lead to
the trapping of reactive carcinogen metabolites or
the triggering of apoptosis
THE TERPENES,
Inhibit:
• oncogenic expression ,
• cell proliferation,
• reducing dedifferentiation.
INDOMETHACIN,
• an anti-inflammatory drug, blocks prostaglandin
synthesis
• reduces tumor development, resulting in a normal
differentiation pattern.

ENZYMES………
• Cells protect themselves from reactive oxygen substances
(ROSs) by activating antioxidant pathways and molecular
systems that use enzymes
• Examples are superoxide dismutase, which controls the level
of the superoxide anion (e.g., O2−);
• catalase modifies the levels of hydroxyl radicals (e.g., OH−)
• Glutathione- s-transferase (GSTs) alters the level of the
intracellular antioxidant glutathione
PROTEINS…..
• cellular antioxidants are proteins such as Bcl-2 - a family of
proteins that modifies PCD.
• several protein families that function as redox,
antioxidant/pro-oxidant molecules that also regulate PCD
(e.g., p53).
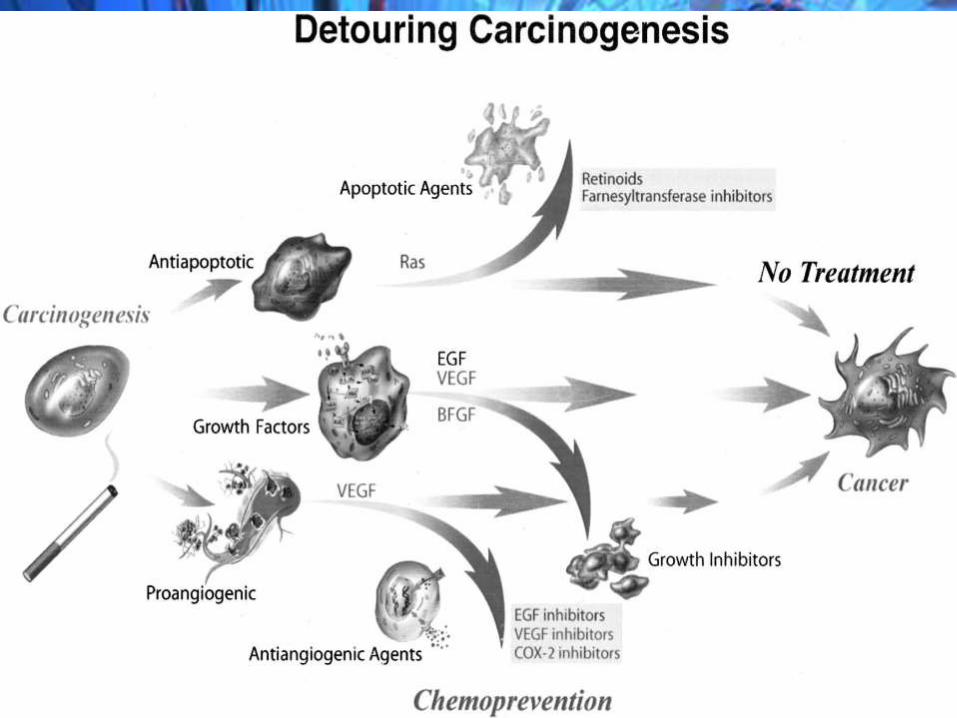
It is thought that patients with head and neck premalignant changes consist of a
diverse population and should be treated differently depending on their
molecular genotype. Patients with minimal genetic changes may be treated with
single-agent retinoids or other agents. Those with more accumulated genetic
changes will require combination of chemoprevention therapies. Lesions that
have advanced genetic changes with mutant p53 may benefi t from targeted p53
therapy and those lesions that express EGFR and COX-2 may require inhibitors of
EFGR and COX-2 However, the challenge today is achieving long-lasting efficacy
with retinoids and/or new agents and determining the optimal dose and duration
of therapy while maintaining acceptable toxicities
conclusion

References
• Journal of Oral and Maxillofacial Pathology: Biomarkers and
chemopreventives in oral carcinogenesis and its prevention
Sonalee Shah, Manpreet Kaur Vol. 18 Issue 1 Jan - Apr 2014
• CA A Cancer Journal for Clinicians Anne S. Tsao, MD; Edward
S. Kim, MD; Waun Ki Hong, MD Volume :54 Number: 3
May/June 2004
• Tumour marker an over view : journal of indian academy of
medicine and radiology, july –september 2010



















